Fungi Linking thePathophysiology of ChronicRhinosinusitis with Nasal Polypsand Allergic Asthma
Michael N. Pakdaman, MD,1 David B. Corry, MD,2,3
and Amber Luong, MD, PhD1
1Department of Otorhinolaryngology-Head & Neck Surgery and Texas Sinus Institute,University of Texas Medical School at Houston, Houston, Texas, USA2Department of Medicine, Baylor College of Medicine, One Baylor Plaza, Houston,Texas, USA3Departments of Pathology and Immunology, Baylor College of Medicine, One BaylorPlaza, Houston, Texas, USA
The immunologic reaction to fungal stimuli has long been thought to be a contributor tothe development of sinonasal disease. We aim to review the role of fungi in upper andlower airway inflammatory diseases. The immune response to fungi in the pathogenic-ity of specific respiratory inflammatory diseases such as allergic bronchopulmonaryaspergillosis and a subtype of CRS known as allergic fungal rhinosinusitis has beenrelatively well described. Fungi are thought to serve both as immunogenic antigens andas adjuncts to inflammation through protease activity. Development of a recent murinemouse model of asthma bypassing the pre-sensitization of allergen further suggests abroader role for fungi in allergic asthma. The literature is lacking in defining a clearpresence of fungi within the inflamed sinus cavity of CRS patients and its potentialimmunologic effects, as well as the utility of antifungal therapy for CRS management.We will review these data and potential common molecular mechanisms activated byfungi in the common pathway toward upper and lower airway inflammatory pathology.
Financial Disclosures: Supported by NIH grants HL75243, AI057696 and AI070973(D.B.C.)Address correspondence to Amber Luong, MD, PhD, 6431 Fannin Street, MSB 5.036,Houston, Texas 77030. E-mail: [email protected]
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
768 M. N. Pakdaman et al.
INTRODUCTION
Rhinosinusitis is defined as symptomatic inflammation of the paranasalsinuses and nasal cavities. It is characterized by two or more major symptoms(mucopurulent drainage, nasal obstruction or congestion, facial pain-pressure-fullness, or decreased sense of smell) in conjunction with objective evidenceof inflammation on nasal endoscopy or computerized tomography (CT) scan(Rosenfeld et al., 2007). The condition is further sub-classified into chronic rhi-nosinusitis (CRS) when the duration of symptoms is longer than 12 weeks.Rhinosinusitis is one of the most common chronic conditions, affecting upto 16% of the US population, representing 32 million Americans annually(Fokkens et al. 2007; Hsiao et al., 2010).
Asthma is an inflammatory disease of the lower airways characterized byairway hyperresponsiveness and airflow limitation with resultant character-istic symptoms such as chest tightness, dyspnea, cough, and wheezing. It isdescribed as a disorder of variable expiratory airflow obstruction arising inassociation with these episodic symptoms (Gibson, et al., 2010). The conditionaffects 5–30% of children and 2–30% of adults (Annesi-Maesano 1999), withsevere asthma affecting 5–10% of this group (Reddy, 2008).
Asthma and CRS have been known to coexist since the 1950s, withasthma being diagnosed in up to 50% of CRS patients, generally patientswith nasal polyps, (Annesi-Maesano,1999; Staikuniene et al., 2008) andabnormal sinus CT scans being found in over 80% of patients with severeasthma (Bresciani et al., 2001; Ragab et al., 2006; ten Brinke et al., 2002).Staikuniene et al. (2008) found 91% of patients with asthma to have nasalpolyps.
This relationship between CRS and asthma has classically been describedas resulting from a common allergic upper and lower airway response, knownas the “united airways disease” (Newman et al., 1994). Recently, attentionhas been directed at further understanding this complex relationship. Theimmunologic reaction to fungal stimuli has long been thought to be a contrib-utor to the development of sinonasal disease. In this article, we will reviewthe evidence supporting a role of fungi in certain forms of chronic respiratoryinflammatory diseases.
Allergic Asthma and Nasal Polyps – A Common Cytokine ProfileChronic rhinosinusitis represents a diverse array of clinical conditions
with a variety of clinical presentations. CRS is a sinonasal inflammatory con-dition that can be described as with (CRSwNP) or without (CRSsNP) nasalpolyps (Bachert et al., 2010a; Gliklich and Metson, 1995, 1997; Pearlman et al.,2009; Staikuniene et al., 2008). CRS is accompanied by polyps in 19%–36% of
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 769
patients (Dykewicz and Hamilos, 2010; Rosenfeld et al., 2007) and the major-ity of clinicians and scientists use CRSwNP and CRSsNP as the primaryclassification of this heterogeneous disease.
The classification scheme based on the absence and presence of nasalpolyps is supported by immunological markers. CRSwNP is characterized bythe presence of polyps in the nasal cavity and paranasal sinuses (Bachertet al., 2009; Zhang et al., 2006). Immunologically, CRSsNP involves a predomi-nantly neutrophilic response moderated by T helper cell type 1 (Th1) responsescharacterized by IL-12 and IFN-γ , whereas CRSwNP is characterized by aneosinophilic response predominated by Th2 cytokines such as IL-5, IL-4 andIL-13.
Consequently, eosinophils and their related inflammatory products areconsidered the hallmark of polypoid inflammation, thus sharing a commonpathway with the inflammatory response described in asthma. Histologically,elevated expression of cytokines IL-4, IL-5, and IL-13 are found to be involvedin the Th2 cascades of both asthma and CRSwNP pathophysiology (Bachertet al., 2000; Chan and Kuhn, 2009; Eloy et al., 2011; Fokkens et al., 2009;Pawankar, 2003; Staikuniene et al., 2008; Van Zele et al., 2006). Staikuniene(2008) prospectively followed 144 patients, 121 with CRS and 23 controls. Datawere collected on the presence of asthma per history and pulmonary func-tion testing as well as presence of polyposis per imaging and endoscopy andallergic rhinitis per skin-prick testing to common inhalant allergens. Patientswith both nasal polyps and asthma had significantly higher blood leukocyte,eosinophila, and IgE levels as well as increased sensitivity to mold allergenscompared with patients with nasal polyps alone. Van Zele et al. describe IL-5as the predominant cytokine in the Th2 response of both asthma and nasalpolyposis (Van Zele et al., 2006).
Interestingly, while allergic asthma and CRSwNP share a common Th2cytokine profile, there exists a population of CRSwNP associated with non-allergic asthma (Eloy et al., 2011). Nasal polyposis has been described to affectup to 40% of patients with nonallergic asthma (Eloy et al., 2011). Studies havedemonstrated the relationship between CRS and asthma among non-atopicpatients. Leynaert et al. (1999) collected data on over 1,400 patients withperennial rhinitis and compared them to over 5,000 normal controls. Theyfound the odds ratio for asthma to be higher among nonatopic patients withIgE levels <= 80 kIU/L (OR = 13.3) compared to atopic patients (OR = 8.1).Rashid et al. (2007) retrospectively reviewed 1,026 charts of patients with CRSand found no relationship to any inflammatory disease with a Th2 cytokineprofile other than asthma. These results lead us to question whether atopyalone can explain the complex relationship between these CRS and asthmapatients. This surprising relationship may be explained by the increased
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
770 M. N. Pakdaman et al.
prevalence of nonallergic disease in severe asthma patients coupled with theincreased severity of asthma in patients with polyposis (Craig, 2010).
Fungi have been argued to serve as pathogenic mediators of CRS. A subsetof CRSwNP patients can produce copious amounts of mucin containing highnumbers of eosinophils and fungi. The term “eosinophilic mucin,” or “allergicmucin,” describes a thick, tenacious, dark-colored mucus on the mucosal sur-faces of the upper airway (Katzenstein et al., 1983). Microscopic evaluationof this mucin reveals a significant concurrent presence of bacteria and fungi.In 55 specimens analyzed, 22 had microscopic evidence of fungi of which 17(77%) had concurrent bacterial presence (Ferguson et al., 2007). Similarly, fun-gal exposure in fungal sensitized allergic asthmatic patients elicits a robusteosinophilic Th2-type immune response (Porter et al., 2009; Vicencio et al.,2010). Although the data are insufficient to confirm a causal role for fungiin CRS, they do suggest that sinus cavity fungi can contribute to diseaseexpression in a subset of CRSwNP patients.
In addition to fungi, Staphylococcus aureus has been cultured from manydiseased sinuses of CRS patients. Some studies have shown the immuneresponse to S. aureus to be a contributor to the inflammatory pathogenesisof asthma and CRS. Rates of S. aureus colonization in up to 50% of patientswith CRS have been described (Corriveau et al., 2009; Foreman and Wormald,2010; Sachse et al., 2010a; Van Zele et al., 2004), as well as increased sen-sitization to S. aureus antigens among patients with CRS (Cho et al., 2010;Krysko et al., 2010; Sachse et al., 2010b). It is unclear whether this antigenicresponse is specific to CRSwNP or if it is evident in all forms of CRS. Also,given the frequent co-presence of S. aureus and fungi in CRSwNP patients, itis unclear how this relationship contributes to the Th2 immune response andoverall disease pathophysiology. Bachert et. al. (2010b) analyzed nasal polypsfrom 70 Belgian patients and found that mucosal inflammation was amplifiedby S. aureus, and IL-5 and IgE above certain threshold levels were associatedwith co-morbid asthma.
These studies reveal a common Th2 cytokine profile within the diseasedtissue of patients with CRSwNP and asthma. The presence of fungi in diseasedTh2 characterized sinuses and lungs further raises the question of their abilityto elicit common cytokine expression profiles and potentially play a role incertain types of both asthma and CRS.
Fungi and Chronic Allergic Respiratory Inflammatory DiseasesOne of the earliest descriptions of fungal etiology for airway inflammation
is in the pathophysiology of allergic bronchopulmonary aspergillosis (ABPA).It is described as an allergic pulmonary disorder caused by hypersensitivityto Aspergillus fumigatus. The disease is characterized clinically by chronicasthma, recurring pulmonary infiltrates, and bronchiectasis (Soubani and
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 771
Chandrasekar, 2002). The condition is found in 1–2% of asthmatics (Agarwal,2009), and up to 39% of asthmatic patients admitted to the ICU (Agarwal,2009). Patients will commonly present with low-grade fever, wheezing, andproductive cough. Hemoptysis and expectoration of brownish-black mucusharboring fungi are highly suggestive (Agarwal, 2009).
Clinical criteria for diagnosis includes the presence of asthma, pulmonaryopacities on imaging, eosinophilia, elevated IgE, central bronchiectasis, andA.fumigatus-specific serum IgE and IgG (Patterson et al., 1986). The cytokineprofile of ABPA is grossly similar to that of CRSwNP and asthma, as it isthought to be a Th1/Th2 dysregulation with shift toward Th2 (Bozza et al.,2002). A common thought is that once the conida are inhaled, they germi-nate into hyphae and express antigens that impair mucociliary clearance, thusallowing for invasion of airway epithelium and activation of innate immu-nity and subsequent Th2-moderated inflammatory reaction (Agarwal, 2009;Patterson et al., 1986).
The role of T regulatory cells in ABPA was suggested in a recent studyby Kreindler et al. (2010) comparing cystic fibrosis patients who did and didnot develop concurrent ABPA. Those developing ABPA were found to have asignificantly lower vitamin D serum level and suppressed T regulatory cellnumber and function. They also demonstrated that peripheral blood T cellsisolated from patients with ABPA stimulated IL-5 and IL-13 production whenchallenged in vitro with A. fumigatus and these levels were attenuated withthe addition of 1,25 OH-vitamin D3. The exact molecular mechanism elicitedby fungi, however, remains unclear.
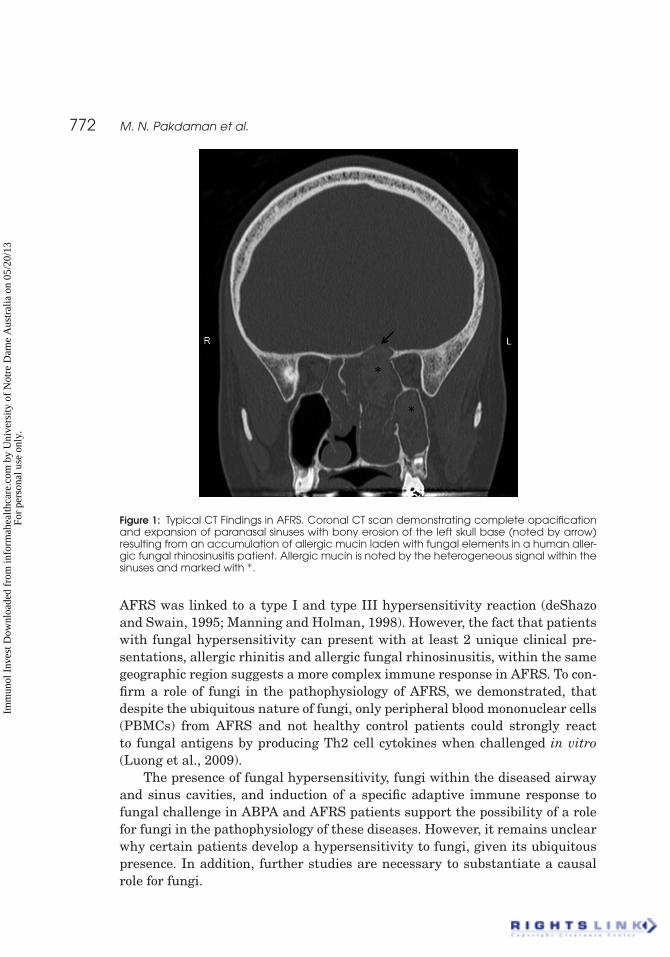
Sharing clinical similarities to ABPA, fungal pathology in the upperairways has also been demonstrated through allergic fungal rhinosinusitis(AFRS). AFRS is a distinct subset of chronic rhinosinusitis representing upto 12% (Chan and Kuhn, 2009). Regionally, it is predominantly found in theSouthern and Southwestern United States (Schubert, 2009). The role of fungiin AFRS is highly suggested by the clinical accumulation of eosinophilic mucinladen with fungal hyphae which can cause expansion and bony erosion ofparanasal sinuses (Figure 1). Dematiaceous fungi are most commonly asso-ciated with AFRS, but other fungal species including Aspergillus have alsobeen linked to the pathophysiology of this disease(Schubert, 2009). Diagnosisof AFRS is based primarily on histologic evaluation of mucin obtained dur-ing surgery. Most investigators agree on a positive fungal histology or culture,eosinophilic mucin, and CT or MRI findings consistent with accumulation ofmucinous debris resulting in expansion of involved sinuses (Figure 1), and evi-dence of fungal hypersensitivity as criteria for diagnosis (deShazo and Swain1995; Fokkens et al. 2009; Schubert, 2009).
Based on this clinical similarity to ABPA and the identification of elevatedfungal specific serum IgE and IgG levels to the same fungal species presentwithin the diseased sinuses, it was postulated that the pathophysiology of
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
772 M. N. Pakdaman et al.
Figure 1: Typical CT Findings in AFRS. Coronal CT scan demonstrating complete opacificationand expansion of paranasal sinuses with bony erosion of the left skull base (noted by arrow)resulting from an accumulation of allergic mucin laden with fungal elements in a human aller-gic fungal rhinosinusitis patient. Allergic mucin is noted by the heterogeneous signal within thesinuses and marked with ∗.
AFRS was linked to a type I and type III hypersensitivity reaction (deShazoand Swain, 1995; Manning and Holman, 1998). However, the fact that patientswith fungal hypersensitivity can present with at least 2 unique clinical pre-sentations, allergic rhinitis and allergic fungal rhinosinusitis, within the samegeographic region suggests a more complex immune response in AFRS. To con-firm a role of fungi in the pathophysiology of AFRS, we demonstrated, thatdespite the ubiquitous nature of fungi, only peripheral blood mononuclear cells(PBMCs) from AFRS and not healthy control patients could strongly reactto fungal antigens by producing Th2 cell cytokines when challenged in vitro(Luong et al., 2009).
The presence of fungal hypersensitivity, fungi within the diseased airwayand sinus cavities, and induction of a specific adaptive immune response tofungal challenge in ABPA and AFRS patients support the possibility of a rolefor fungi in the pathophysiology of these diseases. However, it remains unclearwhy certain patients develop a hypersensitivity to fungi, given its ubiquitouspresence. In addition, further studies are necessary to substantiate a causalrole for fungi.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 773
Role of Fungi in Non-Allergic Chronic RhinosinusitisThe immunologic reaction to fungal stimuli playing a role in the patho-
physiology of sinonasal disease is evidenced in AFRS. Ponikau et al. (1999)after identifying fungi within the nasal cavity of 96% of CRS patients sug-gested a broader role of fungi in more generalized CRS. Utilizing a reducingagent to treat the collected mucin, they found positive fungal cultures fromnasal lavage in 96% of 210 CRS patients and 100% of healthy controls, andidentified fungal elements in 81% of 101 surgically obtained mucin from CRSpatients (Ponikau et al., 1999).
Prior to this study, fungi within mucin were rarely identified and servedas an essential element in the diagnosis of AFRS. A follow-up study isolatedPBMCs from 18 patients with CRS and 15 healthy individuals and challengedthese cells in vitro with 4 common fungal antigens. Fungi and most convinc-ingly Alternaria incited a Th1 and Th2 immune response from PBMCs onlyfrom CRS and not healthy controls (Shin et al., 2004). Based on these data,they suggested that fungi may play a role in all types of CRS.
This hypothesis that fungi play a role in all forms of CRS has been hotlydebated for over a decade (Orlandi and Marple, 2010). Examining a hetero-geneous group of CRS patients including with and without nasal polyps from2 geographically unique areas, a dry climate of Utah where AFRS is uncom-mon and a humid area of Texas where AFRS is present in up to 15% of CRSpatients, investigators found no consistent increase in secretion of the Th2cytokines IL-4, IL-5 and IL-13 after in vitro challenge of PBMCs with fungalantigens. The clinically heterogeneous CRS group did show a greater range ofcytokine expression as compared to healthy controls arguing that certain sub-types of CRS may have an immune response to the fungi. However, the samplesize of 10 CRS patients, 4 categorized as CRS without nasal polyps, 5 as AFRSand only 1 CRS with nasal polyps, limited the ability to draw more contrast inthe subgroup analysis of these categories. (Orlandi et al., 2009).
AFRS is clinically separated from other types of CRSwNP by the presenceof eosinophilic mucin characterized by a heavy fungal and eosinophil presenceand fungal hypersensitivity as noted by either a positive skin reaction whenchallenged with fungal antigen or elevated serum fungal specific IgE levels.Otherwise both AFRS and CRSwNP are characterized by a chronic inflamma-tion of the sinonasal mucosa with nasal polyps. Unlike CRS without nasalpolyps, cytokine analysis of the inflamed mucosa from both CRSwNP andAFRS reveal elevated Th2 cytokines and significant presence of eosinophils(Van Zele et al., 2006).
With new sensitive techniques to identify fungal presence such as quan-titative polymerase chain reaction, multiple studies have now described thepresence of fungal elements in the nasal respiratory tract to be a common phe-nomenon (Catten et al., 2001; Lackner et al., 2005; Rao et al., 2006). However,the presence of fungi limited to the paranasal sinuses, which is anatomically
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
774 M. N. Pakdaman et al.
much less accessible to the environment than the nasal cavity, has not beenclosely examined. So, it remains unclear if CRSwNP and AFRS are distinctclinical entities or the same disease of varying severity sharing a similarpathophysiology.
Proteases – The Missing Link?Much of the recent discussion regarding the role of fungi in CRS patho-
physiology has centered on fungal proteases. Proteases are a class of enzymescapable of hydrolyzing peptide bonds. They play functional roles such asmobilization of storage proteins, normal protein turnover and degradation, reg-ulatory function, and post-translational modification (Yike, 2011). Similarly,proteases may serve a pathologic role. Protease activity has been shown toaccompany the antigenic activity of many allergens derived from dust mites,ragweed and fungi (Kheradmand et al., 2002; Porter et al., 2009). For thepurposes of this review, we will focus on the immunogenic role of fungalproteases.
Protease exposure and human allergic respiratory disease was first rec-ognized in occupational exposure to microbial and plant proteinases. Thepresence of proteases such as Bacillus subtilis-derived proteinases added todetergents has been known dating back to the 1960s (Flindt, 1969). Van Rooyet al. (2009) found a 14% risk of developing sensitization and respiratoryallergy among workers exposed to detergent proteases. Brant et. al examineda cohort of employees and estimated protease exposure using a job expo-sure matrix from over 12,000 measurements taken from the factory between1989 and 2002. They found clear relationships between protease exposure andlower and upper respiratory disease after controlling for age, sex, and smoking(Brant et al., 2009).
Many of the common allergens such as Der p 1 (Schulz et al., 1998), themajor dust mite allergen, Per a 10 antigen from cockroach (Sudha et al., 2009),and Cur 11 antigen from fungi Curvularia lunata (Tripathi, et al. 2009) areproteases. Of these common allergens, the most studied relevant to chronicrhinosinusitis are from fungi (Shin and Lee, 2010; Shin et al., 2006). The majorsource of fungal protease is hyphae; spores are specifically devoid of proteaseactivity.
Microscopic aerosolized particles that contain fungal proteinase activitymost likely contain hyphal fragments (Green, et al. 2006). In addition, CRSpatients often have elevated levels of specific IgE antibodies to other non-fungal allergens with protease activity (Reed and Kita, 2004; Rudack et al.,2007; Sookrung and Chaicumpa, 2010). The presence of systemic immuneresponses to protease activity in CRS suggests a possible role in its patho-physiology, but more direct experimentation is required to illustrate a truerelationship.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 775
Direct Fungal Protease Exposure Can Overcome TolerogenicMechanisms in the Lungs
The classic mouse model of asthma requires pre-sensitization of BALB/cmice to ovalbumin (OVA), applied via an intraperitoneal (IP) injection, fol-lowed by a course of exposure to aerosolized OVA. With this protocol, themice demonstrate chronic inflammation of airway lamina propria, intraep-ithelial eosinophil accumulation with Th2 responses, and marked airwayhyperreactivity to methacholine when compared with controls (Temelkovskiet al., 1998). The responsiveness to stimulation by OVA requires that themice be primed through intraperitoneal or subcutaneous administrationto overcome the increased Treg function inducing tolerance in the lungsto OVA.
Unlike OVA, proteases derived from ragweed and multiple fungi directlyapplied to the mouse lung via intranasal application can overcome the lungtolerogenic mechanisms and incite lower airway Th2 response and hyperre-sponsiveness without an intraperitoneal pre-sensitization (Kheradmand et al.,2002; Porter et al., 2009; Porter et al., 2011). Using this more physiologic pro-tocol, a murine model for asthma could be established using various differentproteases, not restricted to one class (cysteine, serine, metallo, etc.), such asDer p 1, papain, and proteases derived from human rhinovirus and A. oryzae(Chen et al., 2006; Singh et al., 2010; Sokol et al., 2008). Notably, the allergenicability of the protease derived from A. oryzae required fully intact proteaseactivity, indicating that it is the enzymatic activity that is the essential allergicproperty of these proteases (Kheradmand et al., 2002).
Proteases can also serve as an adjuvant to allow antigens that would haveotherwise caused no harm to induce an immunogenic response (Kheradmandet al., 2002; Yike, 2011). The broad sensitivity to diverse antigens that is com-mon to many allergic asthmatic patients may be supportive of this adjuvantrole. Thus, experimental studies of fungal proteases in rodents provide thefirst molecular insight into the association between human allergic disease,allergens and allergenic organisms such as fungi. Nonetheless, much furtherwork is required to clarify how proteases derived from fungi and potentiallyother organisms contribute to human CRS and asthma.
A murine model for CRS currently exists utilizing the classic protocol inBALB/c mice. This model of CRS, demonstrating chronic eosinophilia in thesinonasal mucosa, was established with an initial intraperitoneal injection ofwhole-organism derived fungal antigen for sensitization and recurrent nasalchallenge with this fungal antigen over 1 month (Lindsay et al., 2006). Basedon the recent models for asthma utilizing only intranasal challenge with fungalprotease antigen, similar sinonasal mucosal inflammation may be found inthese mice.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
776 M. N. Pakdaman et al.
The Questionable Role of Protease Activated Receptors in ofFungal Protease Activity Responsible for Inciting RespiratoryInflammatory Disease
The mechanism by which respiratory Th2 inflammation is incited byproteases remains a mystery. One popular hypothesis suggests that theseproteases activate protease-activated-receptors (PAR) leading to release ofproinflammatory cytokines (Kauffman et al., 2000; Yike, 2011). Shin et al.(2006) obtained nasal polyp epithelial cells from patients with CRS. Thesecells were stimulated with Aspergillus, Alternaria, and Cladosporum in vitroand showed increased PAR-2 and PAR-3 mRNA, as well as increased expres-sion of proinflammatory cytokines IL-8 and RANTES. Kauffman et. al suggestthe role of proteases in the Th2 response involves fungal activation of nasalepithelial cells with upregulation of PAR2, PAR3 mRNA (Shin et al. 2006),leading to morphologic changes, cell desquamation, and release of proinflam-matory cytokines (IL-6, IL-8) (Kauffman et al. 2000), resulting in eosinophilicinflammation (Rudack et al. 2007).
However, protease-activated receptors have been linked to anti-inflammatory as well as pro-inflammatory responses. To clarify the role ofPAR2 in the murine asthma model incited by protease-containing Asperillus,one of us (DBC), challenged wild-type and PAR2 −/− mice every 4 days for2 weeks intranasally with a protease-containing allergen derived from theculture filtrate of A. fumigatus (Calvanico et al., 1981). Although the PAR 2−/− mice had reduced airway hyperreactivity as compared to WT as noted byhigher PC200 values with fungal antigen challenge, the inflammatory cell com-position within the bronchoalveolar lavage fluid was identical between bothgroups (Figure 2) suggesting that PAR-2 is not essential for the recruitment ofeosinophils, a key indicator of Th2 cell-driven allergic inflammation, in allergicasthma. However, the specific roles of PARs in CRS remain less clear.
Antifungal Therapy in Management of CRS and AsthmaShould fungi play a key role in the pathophysiology of chronic respira-
tory inflammatory disease, one would expect patients to respond to antifungaltherapy. Despite earlier studies that suggested symptomatic and objectiveimprovement with topical amphotericin, later studies found no differencebetween patients treated with topical Amphotericin B versus saline (Bentand Kuhn, 1994; Ebbens et al., 2006; Gerlinger et al., 2009; Helbling et al.,2006; Liang et al., 2008; Ponikau et al., 1999, 2002, 2005; Ricchetti et al.,2002; Weschta et al., 2004). Liang et al. (2008) performed nasal irrigationwith Amphotericin B versus normal saline in 64 CRS without polyps (CRSsNP)patients and found no change in subjective scores, endoscopic exam, or fungalcultures. Ebbens et al. performed a multi-center randomized controlled trial
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 777
Figure 2: PAR-2 is not necessary in the recruitment of inflammatory cells in response to pro-tease containing A. fumigatus. Allergic lung disease phenotype of PAR2–/– mice challengedwith a proteinase-active allergen. Par2–/– mice were challenged intranasally every other dayfor 14 days with either physiological saline or a culture filtrate allergen derived from A. fumi-gatus (AFA) and compared to genotype matched wild-type mice. On day 16, (A) airwayhyperresponsiveness as assessed by the provocative concentration of acetylcholine (Ach) toinduce a 200% increase in respiratory system resistance from baseline (PC200; expressed asμg Ach/gram body weight) was determined by interpolation of Ach dose-response curvesand (B) the percentage of macrophages (Mac), eosinophils (Eos), neutrophils (Neu) andlymphocytes (Lym) from bronchoalveolar lavage fluid (BALF) was determined by standardcytological criteria [6]. BALF from saline-challenged mice of both genotypes contained >95%macrophages. ∗: P < 0.05 relative to saline-challenged mice as assessed by the Mann-Whitneytest.
of topical Amphotericin B. A total of 166 patients were randomized to eitheran experimental arm that included nasal irrigation with Amphotericin B or acontrol arm of saline irrigation. After 13 weeks of treatment, the group foundno significant changes in the major inflammatory cytokines and chemokinestypically recognized to be involved in CRS pathogenesis (Ebbens et al.,2009).
A meta-analysis of these studies with topical Amphoterecin B in CRSshowed no significant improvement in objective (CT or nasal endoscopy exam)or subjective symptoms (Isaacs, Fakhri, Luong, Citardi, in press). Although theresults of these studies are discouraging for generalized use of topical antifun-gals, these studies included all CRS types rather than a specific subset suchas AFRS or CRSwNP group with elevated fungal load and known immuneresponses to detected fungi. Thus, additional studies of topical antifungals insubsets of CRS patients are warranted.
A small number of non-controlled studies focusing on antifungals in AFRS,a subset of CRS, have demonstrated more positive response (Chan et al.,2008; Erwin and Fitzgerald, 2007; Seiberling and Wormald, 2009). Chan et al.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
778 M. N. Pakdaman et al.
(2008) treated a group of 32 patients with AFRS who were refractory to tradi-tional treatment (steroids, surgery, and Amphotericin B) with itraconazole for3 months, with 12 cases showing endoscopic improvement. Similarly, Seiber-ling and Wormald (2009) noted improvement in 19 of 23 patients with 6months of itraconazole who recurred after failing traditional medical and sinussurgery.
Data for management of asthma is more established. A recent randomizedcontrolled Fungal Asthma Sensitization Trial (FAST) by Denning et al. appliedoral itraconazole in the management of 58 severe asthmatics with fungal sen-sitivity to 1 or more of 7 fungi tested. Patients treated with itraconazole for32 weeks had significant changes in a validated Asthma Quality of Life Ques-tionnaire, as well as improved rhinitis scores and morning peak flow (Denninget al., 2009).
Interpreting the clinical studies utilizing itraconazole for treatment ofeither asthma or CRS is confounded by the anti-inflammatory properties ofthe azole class of antifungal agents and cellular effects (Steel et al., 2007,2008). These effects are less potent with other imidazole antimycotics, suchas voriconazole. Although making it difficult to isolate the effects of theseantifungals, it may be the combined anti-inflammatory and antifungal effectsthat explain the effectiveness of these agents in the treatment of these chronicinflammatory airway diseases. The rudimentary understanding of the relation-ship of fungi in asthma and CRS along with limited analysis of antifungalsin the management of subsets of CRS and asthma patients warrant futurestudies.
CONCLUSION
Abundant evidence has now emerged that support a role for fungi in thepathophysiology of chronic respiratory diseases. Many studies have now inde-pendently described the presence of fungi in the airways of patients with CRSand asthma. Recently, proteases have been identified as one of the key contrib-utors to the immunogenic response to fungal antigens. Data on the presenceof an increased population of fungal hyphae in patients with chronic airwayinflammation is not yet definitive, and the same is true for outcome data ontreatment with antifungal medications. However, the exact role of fungi aseither a principle immunogenic agent or an adjuvant to another immunogenicfactor remains unclear.
Nonetheless, the studies reviewed here suggest at least in outline forma common pathophysiologic mechanism that is capable of explaining a sub-stantial fraction of Th2-mediated disease of both the upper and lower airways.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 779
Inhalation of protease alone is sufficient to induce both human and experimen-tal asthma, but the relevance of this finding to human disease is likely confinedto occupational settings involving unnaturally high exposures to proteases.
In contrast, conventional Th2-mediated upper and lower respiratory tractdisease is more likely caused by mucosal immune response to locally producedfungal proteases within the airway. Concomitant bacterial infection almostcertainly contributes to the severity of fungal sinusitis, but seems to repre-sent a secondary process as demonstrated experimentally by the ability offungi alone to induce profound Th2-mediated airway disease in the normalairway. This pathogenic sequence is remarkably similar to another allergicmucosal inflammatory syndrome, eczema (atopic dermatitis), in which superfi-cial infection with fungi, especially Malassezia spp., is linked to uncomplicateddisease, but may become secondarily involved with staphylococci leading tomore complex disease syndromes including impetigo (Noble, 1998; Scheyniuset al., 2002). Although the possibility of fungi being the sole etiology of all CRSand asthma is unlikely, further studies will reveal the true role that fungi playin inflammatory airway diseases.
Declaration of interest: The authors report no conflicts of interest. Theauthors alone are responsible for the content and writing of the paper.
REFERENCES
Agarwal, R. (2009). Allergic bronchopulmonary aspergillosis. Chest 135:805–826.
Annesi-Maesano, I. (1999). Epidemiological evidence of the occurrence of rhinitis andsinusitis in asthmatics. Allergy 54 (Suppl 57):7–13.
Bachert, C., Claeys, S.E., Tomassen, P., van Zele, T., Zhang, N. (2010a). Rhinosinusitisand asthma: a link for asthma severity. Curr. Allergy Asthma Rep. 10:194–201.
Bachert, C., Gevaert, P., Holtappels, G., Cuvelier, C., van Cauwenberge, P. (2000). Nasalpolyposis: from cytokines to growth. Am. J. Rhinol. 14:279–290.
Bachert, C., Van Bruaene, N., Toskala, E., Zhang, N., Olze, H., Scadding, G., VanDrunen, C.M., Mullol, J., Cardell, L., Gevaert, P., et al. (2009). Important researchquestions in allergy and related diseases: 3-chronic rhinosinusitis and nasalpolyposis —A GALEN study. Allergy 64:520–533.
Bachert, C., Zhang, N., Holtappels, G., De Lobel, L., van Cauwenberge, P., Liu, S., Lin,P., Bousquet, J., Van Steen, K. (2010b). Presence of IL-5 protein and IgE antibodiesto staphylococcal enterotoxins in nasal polyps is associated with co-morbid asthma.J. Allergy Clin. Immunol. 2010 Nov;126(5):962–8, 968.e1–6
Bozza, S., Gaziano, R., Spreca, A., Bacci, A., Montagnoli, C., di Francesco, P., Romani,L. (2002). Dendritic cells transport conidia and hyphae of Aspergillus fumigatusfrom the airways to the draining lymph nodes and initiate disparate Th responsesto the fungus. J. Immunol. 168:1362–1371.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
780 M. N. Pakdaman et al.
Brant, A., Upchurch, S., van Tongeren, M., Zekveld, C., Helm, J., Barnes, F., NewmanTaylor, A.J., Cullinan, P. (2009). Detergent protease exposure and respiratorydisease: Case-referent analysis of a retrospective cohort. Occup. Environ. Med.66:754–758.
Bresciani, M., Paradis, L., Des Roches, A., Vernhet, H., Vachier, I., Godard, P., Bousquet,J., Chanez, P. (2001). Rhinosinusitis in severe asthma. J. Allergy Clin. Immunol.107:73–80.
Calvanico, N.J., Du Pont, B.L., Huang, C.J., Patterson, R., Fink, J.N., Kurup, V.P. (1981).Antigens of Aspergillus fumigatus. 1. Purification of a cytoplasmic antigen reac-tive with sera of patients with Aspergillus-related disease. Clin. Exp. Immunol. 45:662–671.
Catten, M.D., Murr, A.H., Goldstein, J.A., Mhatre, A.N., Lalwani, A.K. (2001). Detec-tion of fungi in the nasal mucosa using polymerase chain reaction. Laryngoscope111:399–403.
Chan, K.O., Genoway, K.A., Javer, A.R. (2008). Effectiveness of itraconazole in themanagement of refractory allergic fungal rhinosinusitis. J. Otolaryngol. Head NeckSurg. 37:870–874.
Chan, Y., Kuhn, F.A. (2009). An update on the classifications, diagnosis, and treatmentof rhinosinusitis. Curr. Opin. Otolaryngol. Head Neck Surg. 17:204–208.
Chen, C.L., Wang, S.D., Zeng, Z.Y., Lin, K.J., Kao, S.T., Tani, T., Yu, C.K., Wang,J.Y. (2006). Serine protease inhibitors nafamostat mesilate and gabexate mesi-late attenuate allergen-induced airway inflammation and eosinophilia in a murinemodel of asthma. J. Allergy Clin. Immunol. 118: 105–112.
Cho, K.S., Kim, C.S., Lee, H.S., Seo, S.K., Park, H.Y., Roh, H.J. (2010). Role of interferon-gamma-producing t cells in the pathogenesis of chronic rhinosinusitis with nasalpolyps associated with staphylococcal superantigen. J. Otolaryngol. Head NeckSurg. 39:600–605.
Corriveau, M.N., Zhang, N., Holtappels, G., Van Roy, N., Bachert, C. (2009). Detectionof Staphylococcus aureus in nasal tissue with peptide nucleic acid-fluorescence insitu hybridization. Am. J. Rhinol. Allergy 23:461–465.
Craig, T.J. (2010). Aeroallergen sensitization in asthma: prevalence and correlationwith severity. Allergy Asthma Proc. 31:96–102.
Denning, D.W., O’Driscoll, B.R., Powell, G., Chew, F., Atherton, G.T., Vyas, A., Miles,J., Morris, J., Niven, R.M. (2009). Randomized controlled trial of oral antifun-gal treatment for severe asthma with fungal sensitization: The Fungal AsthmaSensitization Trial (FAST) study. Am. J. Respir. Crit. Care Med. 179:11–18.
Dykewicz, M.S., Hamilos, D.L. (2010). Rhinitis and sinusitis. J. Allergy Clin. Immunol.125:S103–115.
Ebbens, F.A., Georgalas, C., Luiten, S., van Drunen, C.M., Badia, L., Scadding, G.K.,Hellings, P.W., Jorissen, M., Mullol, J., Cardesin, A., et al. (2009). The effect oftopical amphotericin B on inflammatory markers in patients with chronic rhinosi-nusitis: A multicenter randomized controlled study. Laryngoscope 119:401–408.
Ebbens, F.A., Scadding, G.K., Badia, L., Hellings, P.W., Jorissen, M., Mullol, J.,Cardesin, A., Bachert, C., van Zele, T.P., Dijkgraaf, M.G., et al. (2006). Ampho-tericin B nasal lavages: not a solution for patients with chronic rhinosinusitis. J.Allergy Clin. Immunol. 118:1149–1156.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 781
Eloy, P., Poirrier, A.L., De Dorlodot, C., Van Zele, T., Watelet, J.B., Bertrand, B. (2011).Actual concepts in rhinosinusitis: A review of clinical presentations, inflammatorypathways, cytokine profiles, remodeling, and management. Curr. Allergy AsthmaRep. 2011 Apr;11(2):146–62.
Erwin, G.E., Fitzgerald, J.E. (2007). Case report: Allergic bronchopulmonary aspergillo-sis and allergic fungal sinusitis successfully treated with voriconazole. J. Asthma44:891–895.
Flindt, M.L. (1969). Pulmonary disease due to inhalation of derivatives of Bacillussubtilis containing proteolytic enzyme. Lancet 1:1177–1181.
Fokkens, W.J., Ebbens, F., van Drunen, C.M. (2009). Fungus: A role in pathophysiologyof chronic rhinosinusitis, disease modifier, a treatment target, or no role at all?Immunol. Allergy Clin. North Am. 29:677–688.
Fokkens, W.J., Lund, V., Mullol, J. (2007). European position paper on rhinosinusitisand nasal polyps. Rhinol. Suppl. 2007 Jun;45(2):97–101.
Foreman, A., Wormald, P.J. (2010). Different biofilms, different disease? A clinicaloutcomes study. Laryngoscope 120:1701–1706.
Gerlinger, I., Fittler, A., Fonai, F., Patzko, A., Mayer, A., Botz, L. (2009). Postopera-tive application of amphotericin B nasal spray in chronic rhinosinusitis with nasalpolyposis, with a review of the antifungal therapy. Eur. Arch. Otorhinolaryngol.266:847–855.
Helbling, A., Baumann, A., Hanni, C., Caversaccio, M. (2006). Amphotericin B nasalspray has no effect on nasal polyps. J. Laryngol. Otol. 120:1023–1025.
Hsiao, C.J., Cherry, D.K., Beatty, P.C., Rechtsteiner, E.A. (2010). National AmbulatoryMedical Care Survey: 2007 summary. Natl Health Stat Report, 2010 Nov 3;(27):1–32.
Katzenstein, A.L., Sale, S.R., Greenberger, P.A. (1983). Pathologic findings in allergicaspergillus sinusitis. A newly recognized form of sinusitis. Am. J. Surg. Pathol.7:439–443.
Kauffman, H.F., Tomee, J.F., van de Riet, M.A., Timmerman, A.J., Borger, P. (2000).Protease-dependent activation of epithelial cells by fungal allergens leads tomorphologic changes and cytokine production. J. Allergy Clin. Immunol. 105:1185–1193.
Kheradmand, F., Kiss, A., Xu, J., Lee, S.H., Kolattukudy, P.E., Corry, D.B. (2002). Aprotease-activated pathway underlying Th cell type 2 activation and allergic lungdisease. J. Immunol. 169: 5904–5911.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
782 M. N. Pakdaman et al.
Kreindler, J.L., Steele, C., Nguyen, N., Chan, Y.R., Pilewski, J.M., Alcorn, J.F., Vyas,Y.M., Aujla, S.J., Finelli, P., Blanchard, M., et al. 2010 Vitamin D3 attenuatesTh2 responses to Aspergillus fumigatus mounted by CD4+ T cells from cysticfibrosis patients with allergic bronchopulmonary aspergillosis. J. Clin. Invest. 120:3242–3254.
Krysko, O., Holtappels, G., Zhang, N., Kubica, M., Deswarte, K., Derycke, L., Claeys,S., Hammad, H., Brusselle, G.G., Vandenabeele, P., et al. (2010). Alternativelyactivated macrophages and impaired phagocytosis of S. aureus in chronic rhinosi-nusitis. Allergy. 2011 Mar;66(3):396–403.
Lackner, A., Stammberger, H., Buzina, W., Freudenschuss, K., Panzitt, T., Schoster-itsch, S., Braun, H. (2005). Fungi: A normal content of human nasal mucus. Am. J.Rhinol. 19:125–129.
Leynaert, B., Bousquet, J., Neukirch, C., Liard, R., Neukirch, F. (1999). Perennial rhini-tis: An independent risk factor for asthma in nonatopic subjects: results fromthe European Community Respiratory Health Survey. J. Allergy Clin. Immunol.104:301–304.
Liang, K.L., Su, M.C., Shiao, J.Y., Tseng, H.C., Hsin, C.H., Lin, J.F., Jiang, R.S. (2008).Amphotericin B irrigation for the treatment of chronic rhinosinusitis without nasalpolyps: A randomized, placebo-controlled, double-blind study. Am. J. Rhinol. 22:52–58.
Lindsay, R., Slaughter, T., Britton-Webb, J., Mog, S.R., Conran, R., Tadros, M., Earl, N.,Fox, D., Roberts, J., Bolger, W.E. (2006). Development of a murine model of chronicrhinosinusitis. Otolaryngol. Head Neck Surg. 134:724–730; discussion 731–722.
Luong, A., Davis, L.S., Marple, B.F. (2009). Peripheral blood mononuclear cells fromallergic fungal rhinosinusitis adults express a Th2 cytokine response to fungalantigens. Am. J. Rhinol. Allergy 23:281–287.
Manning, S.C., Holman, M. (1998). Further evidence for allergic pathophysiology inallergic fungal sinusitis. Laryngoscope 108:1485–1496.
Newman, L.J., Platts-Mills, T.A., Phillips, C.D., Hazen, K.C., Gross, C.W. (1994).Chronic sinusitis. Relationship of computed tomographic findings to allergy,asthma, and eosinophilia. JAMA 271: 363–367.
Noble, W.C. (1998). Skin bacteriology and the role of Staphylococcus aureus in infection.Br. J. Dermatol. 139 (Suppl):539–512.
Orlandi, R.R., Marple, B.F. (2010). The role of fungus in chronic rhinosinusitis.Otolaryngol Clin. North Am. 43:531–537, viii.
Orlandi, R.R., Marple, B.F., Georgelas, A., Durtschi, D., Barr, L. (2009). Immunologicresponse to fungus is not universally associated with rhinosinusitis. Otolaryngol.Head Neck Surg. 141:750–756. e751–752.
Patterson, R., Greenberger, P.A., Halwig, J.M., Liotta, J.L., Roberts, M. (1986). Allergicbronchopulmonary aspergillosis. Natural history and classification of early diseaseby serologic and roentgenographic studies. Arch. Intern. Med. 146:916–918.
Pawankar, R. (2003). Allergic rhinitis and asthma: From the link to emerging therapies.Ind. J. Chest Dis.Allied Sci. 45:179–189.
Pearlman, A.N., Chandra, R.K., Chang, D., Conley, D.B.S, Tripathi-Peters, A., Gram-mer, L.C., Schleimer, R.T., Kern, R.C. (2009). Relationships between severity ofchronic rhinosinusitis and nasal polyposis, asthma, and atopy. Am. J. Rhinol.Allergy 23:145–148.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 783
Ponikau, J.U., Sherris, D.A., Kern, E.B., Homburger, H.A., Frigas, E., Gaffey, T.A.,Roberts, G.D. (1999). The diagnosis and incidence of allergic fungal sinusitis. MayoClin. Proc. 74:877–884.
Ponikau, J.U., Sherris, D.A., Kita, H., Kern, E.B. (2002). Intranasal antifungaltreatment in 51 patients with chronic rhinosinusitis. J. Allergy Clin. Immunol.110:862–866.
Ponikau, J.U., Sherris, D.A., Weaver, A., Kita, H. (2005). Treatment of chronic rhi-nosinusitis with intranasal amphotericin B: A randomized, placebo-controlled,double-blind pilot trial. J. Allergy Clin. Immunol. 115:125–131.
Porter, P.C., Ongeri, V., Luong, A., Kheradmand, F., Corry, D.B. (2011). Seeking commonpathophysiology in asthma, atopy and sinusitis. Trends Immunol. 32:43–49.
Porter, P.C, Susarla, S.C., Polikepahad, S., Qian, Y., Hampton, J., Kiss, A., Vaidya, S.,Sur, S., Ongeri, V., Yang, T., et al. (2009). Link between allergic asthma and air-way mucosal infection suggested by proteinase-secreting household fungi. MucosalImmunol. 2:504–517.
Ragab, S.M., Lund, V.J., Saleh, H.A., Scadding, G. (2006). Nasal nitric oxide in objectiveevaluation of chronic rhinosinusitis therapy. Allergy 61:717–724.
Rao, A.K., Mathers, P.H., Ramadan, H.H. (2006). Detection of fungi in the sinus mucosausing polymerase chain reaction. Otolaryngol. Head Neck Surg. 134:581–585.
Rashid, R.M., Miller, A., Scianna, J.M., Stankiewicz, J.A. (2007). Chronic rhinosinusitisand psoriasis: Do mutually exclusive systemic Th1 and Th2 disease patterns exist?Acta Otolaryngol. 127:780–783.
Reddy, R.C. (2008). Severe asthma: Approach and management. Postgrad. Med. J.84:115–120; quiz 119.
Reed, C.E., Kita, H. (2004). The role of protease activation of inflammation in allergicrespiratory diseases. J. Allergy Clin. Immunol. 114:997–1008; quiz 1009.
Ricchetti, A., Landis, B.N., Maffioli, A., Giger, R., Zeng, C., Lacroix, J.S. (2002). Effect ofanti-fungal nasal lavage with amphotericin B on nasal polyposis. J. Laryngol. Otol.116:261–263.
Rosenfeld, R.M., Andes, D., Bhattacharyya, N., Cheung, D., Eisenberg, S., Ganiats, T.G.,Gelzer, A., Hamilos D, Haydon RC, 3rd, Hudgins PA, et al. (2007). Clinical practiceguideline: adult sinusitis. Otolaryngol. Head Neck Surg. 137:S1–31.
Rudack, C., Steinhoff, M., Mooren, F., Buddenkotte, J., Becker, K., von Eiff, C., Sachse,F. (2007). PAR-2 activation regulates IL-8 and GRO-alpha synthesis by NF-kappaB,but not RANTES, IL-6, eotaxin or TARC expression in nasal epithelium. Clin. Exp.Allergy 37:1009–1022.
Sachse, F., Becker, K., Rudack, C. (2010a). Incidence of staphylococcal colonization andof the 753Q Toll-like receptor 2 variant in nasal polyposis. Am. J. Rhinol. Allergy24:e10–13.
Sachse, F., Becker, K., von Eiff, C., Metze, D., Rudack, C. (2010b). Staphylococcus aureusinvades the epithelium in nasal polyposis and induces IL-6 in nasal epithelial cellsin vitro. Allergy 65:1430–1437.
Scheynius, A., Johansson, C., Buentke, E., Zargari, A., Linder, M.T. (2002). Atopiceczema/dermatitis syndrome and Malassezia. Int. Arch. Allergy Immunol. 127:161–169.
Schubert, M.S. (2009). Allergic fungal sinusitis: Pathophysiology, diagnosis and man-agement. Med. Mycol. 47 (Suppl 1):S324–330.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
784 M. N. Pakdaman et al.
Schulz, O., Sewell, H.F., Shakib, F. (1998). Proteolytic cleavage of CD25, the alpha sub-unit of the human T cell interleukin 2 receptor, by Der p 1, a major mite allergenwith cysteine protease activity. J. Exp. Med. 187:271–275.
Seiberling, K., Wormald, P.J. (2009). The role of itraconazole in recalcitrant fungalsinusitis. Am. J. Rhinol. Allergy 23:303–306.
Shin, S.H., Lee, Y.H., Jeon, C.H. (2006). Protease-dependent activation of nasal polypepithelial cells by airborne fungi leads to migration of eosinophils and neutrophils.Acta Otolaryngol. 126: 1286–1294.
Shin, S.H., Ponikau, J.U., Sherris, D.A., Congdon, D., Frigas, E., Homburger,H.A., Swanson, M.C., Gleich, G.J., Kita, H. (2004). Chronic rhinosinusitis: Anenhanced immune response to ubiquitous airborne fungi. J. Allergy Clin. Immunol.114:1369–1375.
Singh, M., Lee, S.H., Porter, P., Xu, C., Ohno, A., Atmar, R.L., Greenberg, S.B., Bandi,V., Gern, J., Amineva, S., et al. (2010). Human rhinovirus proteinase 2A inducesTH1 and TH2 immunity in patients with chronic obstructive pulmonary disease. J.Allergy Clin. Immunol. 125:1369–1378 e1362.
Sokol, C.L., Barton, G.M., Farr, A.G., Medzhitov, R. (2008). A mechanism for theinitiation of allergen-induced T helper type 2 responses. Nat. Immunol. 9:310–318.
Sookrung, N., Chaicumpa, W. (2010). A revisit to cockroach allergens. Asian Pac. J.Allergy Immunol. 28:95–106.
Soubani, A.O., Chandrasekar, P.H. (2002). The clinical spectrum of pulmonaryaspergillosis. Chest 121:1988–1999.
Staikuniene, J., Vaitkus, S., Japertiene, L.M., Ryskiene, S. (2008). Association of chronicrhinosinusitis with nasal polyps and asthma: clinical and radiological features,allergy and inflammation markers. Medicina (Kaunas) 44:257–265.
Steel, H.C, Tintinger, G.R., Anderson, R. (2008). Comparison of the anti-inflammatoryactivities of imidazole antimycotics in relation to molecular structure. Chem. Biol.Drug Des. 72:225–228.
Steel, H.C., Tintinger, G.R., Theron, A.J., Anderson, R. (2007). Itraconazole-mediatedinhibition of calcium entry into platelet-activating factor-stimulated humanneutrophils is due to interference with production of leukotriene B4. Clin. Exp.Immunol. 150:144–150.
Sudha, V.T., Arora, N., Singh, B.P. (2009). Serine protease activity of Per a 10 aug-ments allergen-induced airway inflammation in a mouse model. Eur. J. Clin. Invest.39:507–516.
Temelkovski, J., Hogan, S.P., Shepherd, D.P., Foster, P.S., Kumar, R.K. (1998). Animproved murine model of asthma: Selective airway inflammation, epitheliallesions and increased methacholine responsiveness following chronic exposure toaerosolised allergen. Thorax 53:849–856.
ten Brinke, A., Grootendorst, D.C., Schmidt, J.T., De Bruine, F.T., van Buchem, M.A.,Sterk, P.J., Rabe, K.F., Bel, E.H. (2002). Chronic sinusitis in severe asthma isrelated to sputum eosinophilia. J. Allergy Clin. Immunol. 109:621–626.
Tripathi, P., Kukreja, N., Singh, B.P., Arora, N. (2009). Serine protease activity of Curl 1 from Curvularia lunata augments Th2 response in mice. J. Clin. Immunol. 29:292–302.
Imm
unol
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Not
re D
ame
Aus
tral
ia o
n 05
/20/
13Fo
r pe
rson
al u
se o
nly.
Fungi Linking Chronic Rhinosinusitis and Asthma 785
van Rooy, F.G., Houba, R., Palmen, N., Zengeni, M.M., Sander, I., Spithoven, J.,Rooyackers, J.M., Heederik, D.J. (2009). A cross-sectional study among detergentworkers exposed to liquid detergent enzymes. Occup. Environ. Med. 66:759–765.
Van Zele, T., Claeys, S., Gevaert, P., Van Maele, G., Holtappels, G., Van Cauwenberge,P., Bachert, C. (2006). Differentiation of chronic sinus diseases by measurement ofinflammatory mediators. Allergy 61:1280–1289.
Van Zele, T., Gevaert, P., Watelet, J.B., Claeys, G., Holtappels, G., Claeys, C., vanCauwenberge, P., Bachert, C. (2004). Staphylococcus aureus colonization and IgEantibody formation to enterotoxins is increased in nasal polyposis. J. Allergy Clin.Immunol. 114:981–983.
Vicencio, A.G., Muzumdar, H., Tsirilakis, K., Kessel, A., Nandalike, K., Goldman, D.L.(2010). Severe asthma with fungal sensitization in a child: Response to itraconazoletherapy. Pediatrics 125: e1255–1258.
Weschta, M., Rimek, D., Formanek, M., Polzehl, D., Podbielski, A., Riechelmann, H.(2004). Topical antifungal treatment of chronic rhinosinusitis with nasal polyps: Arandomized, double-blind clinical trial. J. Allergy Clin. Immunol. 113:1122–1128.
Yike, I. (2011). Fungal proteases and their pathophysiological effects. Mycopathologia,in press.
Zhang, N., Holtappels, G., Claeys, C., Huang, G., van Cauwenberge, P., Bachert, C.(2006). Pattern of inflammation and impact of Staphylococcus aureus enterotoxinsin nasal polyps from southern China. Am. J. Rhinol. 20:445–450.