56
GENEAL ANESTHETICS
| Date post: | 31-Dec-2015 |
| Category: |
Documents |
| Upload: | sharon-joseph |
| View: | 233 times |
| Download: | 2 times |
GENEAL ANESTHETICS

GENERAL ANESTHETICS INTRODUCTION
The physiologic state induced by general
anesthetics typically includes:
Analgesia Amnesia Loss of consciousness Inhibition of sensory reflexes Inhibition of autonomic reflexes Skeletal muscle relaxation
GENERAL ANESTHETICS INTRODUCTION
An ideal anesthetic drug: Induce a smooth and rapid loss of consciousness Allowing a prompt recovery after discontinuation
of its administration Possess a wide margin of safety Devoid of adverse effects
For many years, inhalation anesthesia was used for all types of surgical procedures.
Recently, intravenous anesthesia has become a more widely used technique around the world.
GENERAL ANESTHETICS INTRODUCTION The extent of anesthesia in producing these
effects depends on: Specific drug Dosage Clinical situation.
The choice of anesthetic technique will vary according to: Proposed type of diagnostic Therapeutic intervention to be performed Surgical intervention to be performed

GENERAL ANESTHETICS INTRODUCTION
Used AS A SOLE AGENT, none of the currently available anesthetic agents is capable of achieving all of these desirable effects
Most commonly the use of
COMBINATIONS OF INTRAVENOUS AND INHALED DRUGS (so-called balanced anesthesia techniques)
Advantage of the favorable properties of each agent while minimizing the adverse reactions.
OTHER AGENTS IN COMBINATION
Muscle relaxants used to facilitate tracheal intubation and optimize surgical conditions during the operation
Local anesthetics administered by tissue infiltration and peripheral nerve blocks to provide perioperative analgesia
Opioid analgesics
Cardiovascular drugs (eg, β blockers, α2 agonists, calcium channel blockers) to control transient autonomic responses to noxious (painful) surgical stimuli.
STAGES OF ANESTHESIA
The traditional description of the various stages of anesthesia
effects of inhaled diethyl ether slow onset of central action owing to its high solubility in blood
Using these signs, anesthetic effects on the brain divided into 4 stages of increasing depth of CNS depression
STAGES OF ANESTHESIA
I. Stage of analgesia:
analgesia without amnesia. Later, both analgesia and amnesia
II. Stage of excitement:
delirious amnesic. irregular Respiration in both volume and rate, retching and vomiting ends with the reestablishment of regular breathing.
STAGES OF ANESTHESIA
III. Stage of surgical anesthesia:
recurrence of regular respiration cessation of spontaneous respiration (apnea).
IV. Stage of medullary depression:
severe depression of the CNS, the vasomotor center in the medulla, the respiratory center in the brain stem.
TYPES OF GENERAL ANESTHESIA
For extensive surgical procedures:
Preoperative benzodiazepines
Induction of anesthesia with an intravenous anesthetic (eg, thiopental or propofol)
Maintenance of anesthesia with a combination of inhaled (eg, volatile agents, nitrous oxide) and intravenous (eg, propofol, opioid analgesics) drugs
TYPES OF GENERAL ANESTHESIA administered by intravenous injection
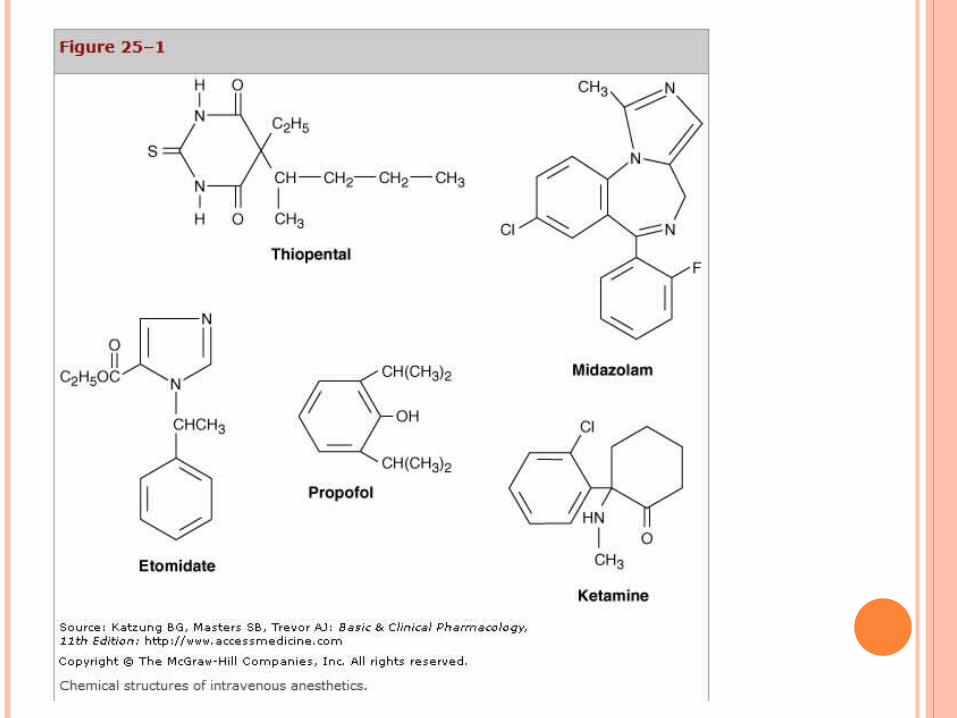
1. barbiturates (eg, thiopental, methohexital)2. benzodiazepines (eg, midazolam, diazepam)3. propofol4. Ketamine5. opioid analgesics (morphine, fentanyl, sufentanil,
alfentanil, remifentanil)6. miscellaneous sedative-hypnotics (eg, etomidate,
dexmedetomidine)
administered by inhalation. 1. Isoflurane2. Desflurane3. Sevoflurane 4. Nitrous oxide

INHALED ANESTHETICS
isoflurane, desflurane, and sevoflurane volatile liquids aerosolized in specialized vaporizer delivery
systems.
Nitrous oxide a gas at ambient temperature and pressure an important adjuvant to the volatile agents Concerns about environmental pollution Increase the incidence of postoperative nausea
and vomiting (PONV) a significant decrease in its use.
INHALED ANESTHETICSPHARMACOKINETICS
Adequate depth of anesthesia depends on a therapeutic concentration of the anesthetic in the CNS.
The concentration of an inhaled anesthetic in a mixture of gases is proportional to its partial pressure (or tension)
Transfer of the anesthetic from the alveolar air to the blood
Transfer from the blood to the brain.
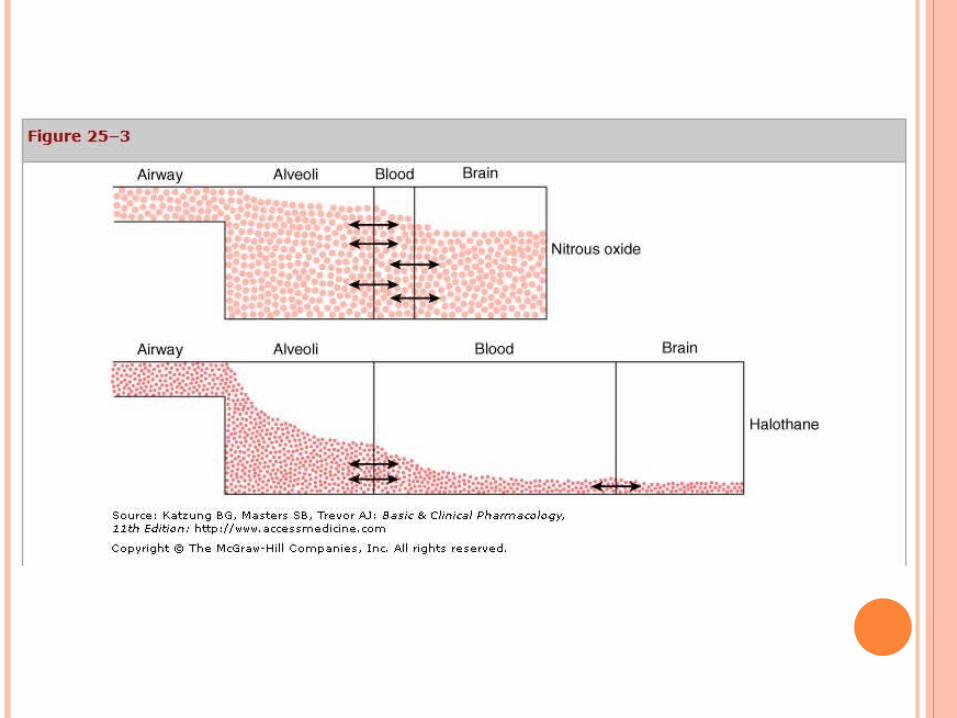
THE BLOOD: GAS PARTITION COEFFICIENT
A useful index of solubility
Defines the inverse relationship between the blood solubility and the rate of rise of its tension in arterial blood
Blood Solubility: Nitrous oxide < desflurane < sevoflurane < isoflurane < halothane < methoxyflurane
Arterial tensions results in equilibration with the brain and onset of action
Nitrous oxide > desflurane > sevoflurane > isoflurane > halothane > methoxyflurane

INHALED ANESTHETICS -UPTAKE & DISTRIBUTION
Rate of induction and recovery depends on:
The physicochemical properties (solubility properties)
Brain uptake Tissue distribution Concentration in the inspired air Volume of pulmonary ventilation Pulmonary blood flow
INHALED ANESTHETICSELIMINATION
The time to recovery from inhalation anesthesia depends on the rate of elimination from the brain.
simply the reverse of the introduction of the anesthetic agent:
blood:gas partition coefficient magnitude of ventilation tissue solubility of the anesthetic

PHARMACODYNAMICSMECHANISM OF ACTION
Depress spontaneous and evoked activity of neurons
Older concepts:
Nonspecific interactions with the lipid matrix of the nerve membrane
Secondary changes in ion flux.
PHARMACODYNAMICS MECHANISM OF ACTION OF GENERAL ANESTHETICS
Primary molecular target: GABA A receptor-chloride channel, a major
mediator of inhibitory synaptic transmission.
Inhaled anesthetics, barbiturates, benzodiazepines, etomidate, and propofol facilitate GABA-mediated inhibition at GABAA receptor sites.
OTHER MECHANISM OF ACTION OF GENERAL ANESTHETICS
Membrane hyperpolarization via activation of potassium channels.
These channels linked to neurotransmitters, including acetylcholine, dopamine, norepinephrine, and serotonin.
Decrease the duration of opening of nicotinic receptor-activated cation channels
Activation of the strychnine-sensitive glycinereceptor
ORGAN SYSTEM EFFECTS OF INHALED ANESTHETICS
Effects on the Cardiovascular System
Halothane, desflurane, enflurane, sevoflurane, and isoflurane decrease mean arterial pressure in direct proportion to their alveolar concentration.
Change heart rate Bradycardia with halothane, probably because of
direct vagal stimulation Desflurane and isoflurane increase heart rate and
blood pressure via transient sympathetic activation with elevations in catecholamine levels
ORGAN SYSTEM EFFECTS OF INHALED ANESTHETICS
Effects on the Respiratory System A dose-dependent decrease in tidal volume
and an increase in respiratory rate, with the exception of nitrous oxide
Respiratory depressants, a reduced response to
increased levels of carbon dioxide.
Decrease the ventilatory response to hypoxia.
Depress mucociliary function in the airway

ORGAN SYSTEM EFFECTS OF INHALED ANESTHETICS
Effects on the Brain Decrease the metabolic rate of the brain. Increase cerebral blood flow (except nitrous
oxide) because the decrease in cerebral vascular resistance;
Clinically undesirable in patients who have increased intracranial pressure because of a brain tumor or head injury.
Depressant effects at lower doses and at higher doses, the cerebral irritant effects, generalized muscle twitching (ie, myoclonic activity), seizure-like activity by enflurane and sevoflurane, but not desflurane.

ORGAN SYSTEM EFFECTS OF INHALED ANESTHETICS
Effects on the Kidney
Decrease the glomerular filtration rate and renal blood flow
Autoregulation of renal flow may be impaired by these drugs.
ORGAN SYSTEM EFFECTS OF INHALED ANESTHETICS
Effects on the Liver
A concentration-dependent decrease in hepatic blood flow
Despite transient intraoperative changes in liver function tests, Permanent changes in liver enzyme function are rare except following repeated exposures to halothane.

ORGAN SYSTEM EFFECTS OF INHALED ANESTHETICS
Effects on Uterine Smooth Muscle
Nitrous oxide have little effect on uterine musculature.
Halogenated anesthetics are potent uterine muscle relaxants
Advantage when profound uterine relaxation is required for an intrauterine fetal manipulation or manual extraction of a retained placenta during delivery.
TOXICITY OF INHALED ANESTHETICS
Hepatotoxicity (Halothane)
Nephrotoxicity (Metabolism of methoxyflurane, enflurane, and sevoflurane leads to the formation of fluoride ions)
Malignant Hyperthermia (tachycardia and hypertension, severe muscle rigidity, hyperthermia, hyperkalemia, and acid-base imbalance with acidosis)
Chronic Toxicity Mutagenicity Carcinogenicity Hematotoxicity

INTRAVENOUS ANESTHETICS
Used alone or in combination with other anesthetic and analgesic drugs
Used to achieve the fast induction of desired anesthetic state.
Recovery is sufficiently rapid
Used to sedate ventilator-dependent patients in intensive care units (ICUs)
PHARMACODYNAMICSMECHANISM OF ACTION
Depress spontaneous and evoked activity of neurons
Like inhaled anesthetics, those with sedative-hypnotic properties directly activate GABAA receptors,
At low concentrations facilitate the action of GABA to increase chloride ion flux.
INTRAVENOUS ANESTHETICS
lack of antinociceptive (analgesic) properties,
combined with nitrous oxide or local anesthetics, or both.
Adjunctive use of potent opioids (eg, fentanyl, sufentanil or remifentanil) to improves cardiovascular stability, enhanced sedation, and perioperative analgesia. But, opioids enhance the ventilatory depressant and increase postoperative emesis.

BARBITURATES - THIOPENTAL
For induction of anesthesia.
Rapidly crosses the blood-brain barrier
Rapidly diffuses out of the brain and other highly vascular tissues and is redistributed to muscle and fat
Sufficient dosage produces loss of consciousness
Plasma:brain equilibrium occurs rapidly (< 1 minute) because of their high lipid solubility.
BARBITURATES
Thiamylal almost identical to thiopental and the same pharmacokinetic and pharmacodynamic profile.
Similar effects with the shorter-acting barbiturate, methohexital.
BARBITURATES – ADVERSE EFFECTS
Decreases in arterial blood pressure, stroke volume, and cardiac output, myocardial depressive effect and increased venous capacitance
Potent respiratory depressant, producing transient apnea and lowering the sensitivity of the medullary respiratory center to carbon dioxide.
No increase in Intracranial pressure and blood volume, thiopental is a desirable drug for patients with cerebral swelling (eg, head trauma, brain tumors).
no adverse effects on hepatic or renal function.
BARBITURATES – ADVERSE EFFECTS
Methohexital has antiseizure activity and the drug of choice for providing anesthesia in patients undergoing electroconvulsive therapy (ECT).
Given its more rapid elimination, methohexital is also preferred over thiopental for short procedures.
BENZODIAZEPINES
Lack general anesthetic properties (eg, diazepam, lorazepam)
Facilitate GABA action but have no direct actions on GABAA receptors
Slower onset and slower recovery than the barbiturates or propofol
Diazepam, lorazepam, and midazolam are preanesthetic medication

BENZODIAZEPINES
preanesthetic administration of benzodiazepines (eg, midazolam) provides: Anxiolysis, Sedation Amnesia Control acute agitation
Diazepam and lorazepam are not water-soluble, and their intravenous use cause pain and local irritation.
Midazolam is water-soluble and is the choice for parenteral administration.
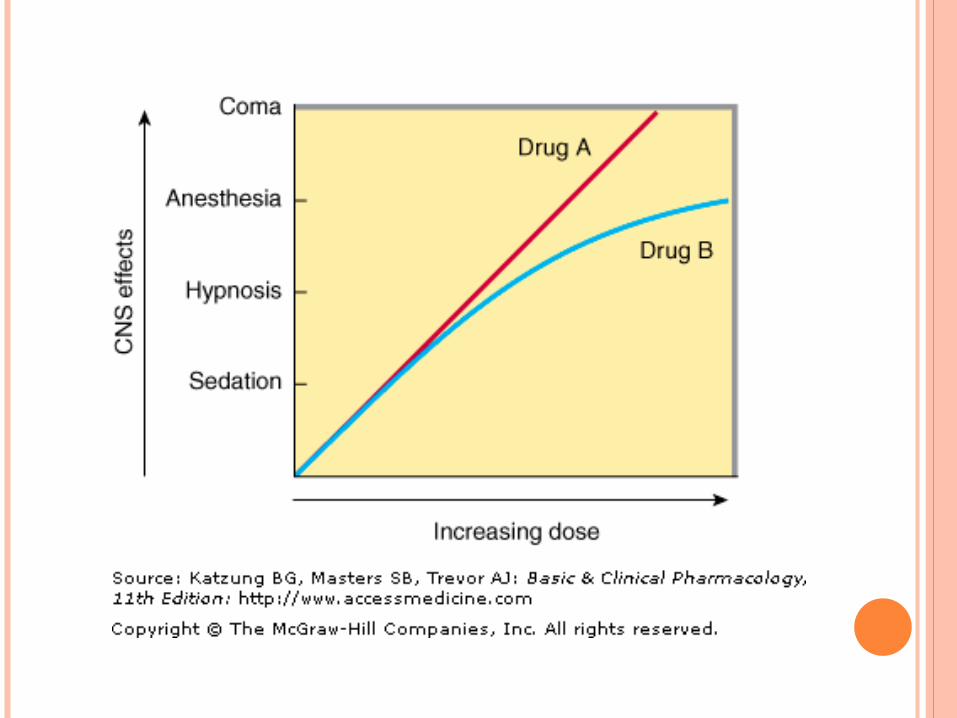
BENZODIAZEPINES - MIDAZOLAM
sedative-anxiolytic properties
high incidence of amnesia
More rapid onset, a shorter elimination half-life (2–4 hours), a steeper dose-response curve than the other BZs
The BZ antagonist, flumazenil, accelerate recovery when excessive doses of intravenous BZs are administered
The short duration of action (< 90 minutes) of flumazenil necessitate multiple doses to prevent recurrence of the CNS depressant effects of the longer-acting BZs (eg, lorazepam, diazepam).
OPIOID ANALGESICS
in combination with BZs to achieve a general anesthetic state,
intravenous morphine (1–3 mg/kg)
fentanyl
sufentanil (IV)
remifentanil, a potent and extremely short-acting opioid, to minimize ventilatory depression.
OPIOID ANALGESICS awareness during anesthesia
unpleasant postoperative recall
chest wall (and laryngeal) rigidity
acutely impairing ventilation
increasing postoperative opioid requirements owing to the development of acute tolerance.
increased postoperative morbidity (eg, prolonged ventilatory support, gastrointestinal and bladder complications)
lower doses of fentanyl and sufentanil as an adjunct to both intravenous and inhaled anesthetics to provide perioperative analgesia.
OPIOID ANALGESICS The shorter-acting alfentanil and remifentanil have
a rapid onset of action.
Remifentanil is rapidly metabolized by esterases in the blood (not plasma cholinesterase) and muscle tissues
not interfere with the clearance of other compounds metabolized by plasma cholinesterase (eg, esmolol, mivacurium, or succinylcholine).
Opioid analgesics are administered in very low doses by the epidural and subarachnoid (spinal) routes of administration to produce postoperative analgesia.
Fentanyl and droperidol administered together produce analgesia and amnesia and combined with nitrous oxide provide a state referred to as neuroleptanesthesia.

PROPOFOL
most popular intravenous anesthetic.
rate of onset of action is similar to the intravenous barbiturates
recovery is more rapid
the reduction in postoperative nausea and vomiting and a sense of well-being.
used for both induction and maintenance of anesthesia
the agent of choice for ambulatory surgery.
PROPOFOL
popular for intravenous sedation in the operating room
effective in producing prolonged sedation in patients in critical care settings
elevate serum lipid levels.

PROPOFOL
rapidly metabolized in the liver faster than of thiopental.
excreted in the urine as glucuronide and sulfate conjugates, with less than 1% of the parent drug excreted unchanged.

PROPOFOL on respiratory function are similar to those of
thiopental. dose-related depression of central ventilatory
drive and transient apnea. marked decrease in blood pressure through
decrease in peripheral arterial resistance and venodilation.
direct negative inotropic effects than other intravenous anesthetics.
Pain at the site of injection after bolus administration.
Muscle movements, hypotonus, and (rarely) tremors
Newer formulations of propofol contain less lipid for prolonged administration (eg, Ampofol).
A water-soluble prodrug of propofol, fospropofol, ameliorate the problems associated with administration of propofol.
ETOMIDATE
For induction of anesthesia in patients with limited cardiovascular reserve.
Causes minimal cardiovascular and respiratory depression.
Produces a rapid loss of consciousness, with minimal hypotension
Heart rate usually unchanged, Incidence of apnea low No analgesic effects, and coadministration of
opioid analgesics is required Recovery from etomidate is less rapid (< 10
minutes) compared with propofol.
ETOMIDATE
Relatively short duration of anesthetic effects. Extensively metabolized in the liver and plasma
to inactive metabolites, with only 2% of the drug excreted unchanged in the urine.
High incidence of pain on injection and postoperative nausea and vomiting.
Cause adrenocortical suppression via inhibitory effects on steroidogenesis, with decreased plasma levels of cortisol after a single dose.
Prolonged infusion of etomidate in critically ill patients result in hypotension, electrolyte imbalance, because of its adrenal suppressive effects.
KETAMINE
a unique dissociate anesthetic
characterized by amnesia and analgesia, with or without loss of consciousness
possesses both anesthetic and analgesic properties
No facilitation GABAA receptor functions
Rather antagonizes the action of the excitatory neurotransmitter glutamic acid on the N -methyl-D -apartate (NMDA) channel receptor.
KETAMINE
Chemically related to phencyclidine (PCP), a drug with a high abuse potential owing to its psychoactive properties.
Highly lipophilic drug and is rapidly distributed into the brain, liver, and kidney.
cardiovascular stimulant, increase Heart rate, arterial blood pressure, and cardiac output by: stimulating the central sympathetic nervous
system to a lesser extent, inhibiting the reuptake of
norepinephrine at sympathetic nerve terminals
KETAMINE
Increases cerebral blood flow, oxygen consumption, and intracranial pressure.
Dangerous when intracranial pressure is elevated.
Upper airway muscle tone is well maintained and airway reflexes are usually preserved.
Use of low doses of ketamine (0.1–0.25 mg/kg IV) in combination with other intravenous and inhaled anesthetics is an alternative to opioid analgesics to minimize ventilatory depression.
KETAMINE
Associated with postoperative disorientation, illusions and dreams (so-called emergence phenomena).
Diazepam or midazolam, as well as propofol, given before ketamine to reduce these adverse effects.
High incidence of postoperative psychic phenomena
Useful for high-risk patients in cardiogenic or septic shock because of its cardiostimulatory properties.
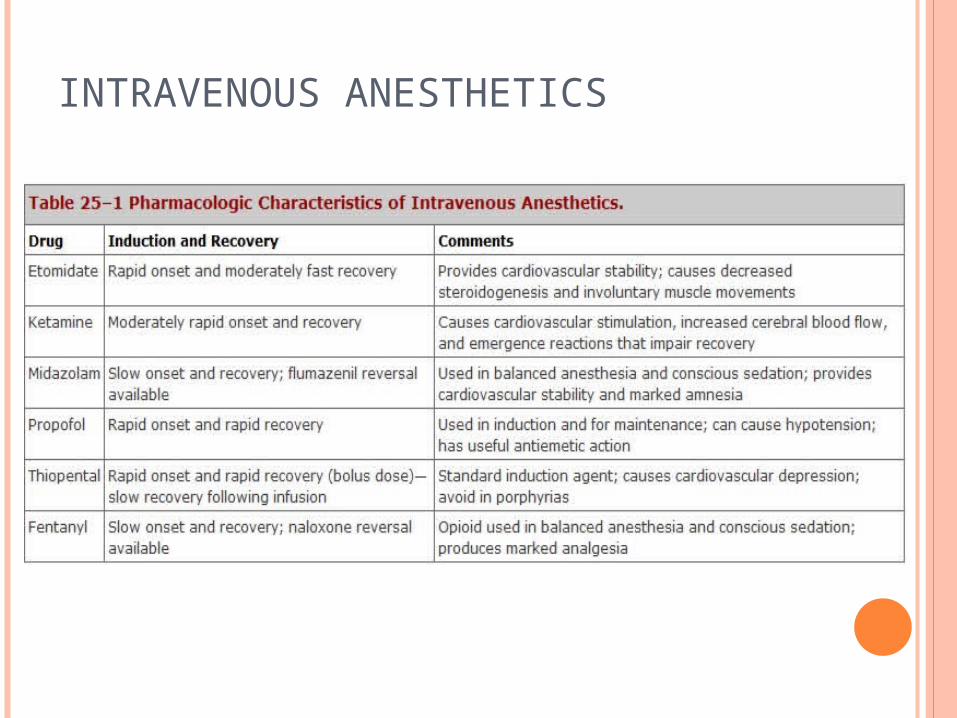
INTRAVENOUS ANESTHETICS

















