ARTICLE IN PRESSG ModelESPOL-3232; No. of Pages 16
Research Policy xxx (2016) xxx–xxx
Contents lists available at ScienceDirect
Research Policy
jo ur nal ho me page: www.elsev ier .com/ locate / respol
he revolution re-visited: Clinical and genetics research paradigmsnd the productivity paradox in drug discovery
ichelle Gittelmanutgers Business School, Department of Management and Global Business, Newark-New Brunswick, New Jersey, United States
r t i c l e i n f o
rticle history:eceived 12 January 2016ccepted 12 January 2016vailable online xxx
eywords:&D productivityrug discoveryasic and applied researchcience-technology linkagesharmaceuticalsiotechnology
a b s t r a c t
Breakthroughs in genetics and molecular biology in the 1970s and 1980s were heralded as a major tech-nological revolution in medicine that would yield a wave of new drug discoveries. However, some fortyyears later the expected benefits have not materialized. I question the narrative of biotechnology as aSchumpeterian revolution by comparing it to the academic research paradigm that preceded it, clinicalresearch in hospitals. I analyze these as distinct research paradigms that involve different epistemolo-gies, practices, and institutional loci. I develop the claim that the complexity of biological systems meansthat clinical research was well adapted to medical innovation, and that the genetics/molecular biologyparadigm imposed a predictive logic to search that was less effective at finding new drugs. The paperdescribes how drug discovery unfolds in each paradigm: in clinical research, discovery originates withobservations of human subjects and proceeds through feedback-based learning, whereas in the geneticsmodel, discovery originates with a precisely-defined molecular target; feedback from patients enters latein the process. The paper reviews the post-War institutional history that witnessed the relative decline ofclinical research and the rise of genetics and molecular science in the United States bio-medical research
landscape. The history provides a contextual narrative to illustrate that, in contrast to the framing ofbiotechnology as a Schumpeterian revolution, the adoption of biotechnology as a core drug discoveryplatform was propelled by institutional changes that were largely disconnected from processes of sci-entific or technological selection. Implications for current medical policy initiatives and translationalscience are discussed.
The past forty years have witnessed significant changes in theandscape of bio-medical research. Breakthroughs in genetics and
olecular biology in the 1970s and 1980s made possible thepplication of basic science to medical discovery, and innovativeio-informatics techniques vastly increased the analytical powerhat could be harnessed to the complex task of finding new drugsScannell et al., 2012). These developments transformed the pro-ess of drug discovery as well as the institutional landscape ofio-medical research.
The new biotechnologies were framed in the popular press asell as the scholarly literature as a revolutionary technology inrug discovery (Cockburn, 2006; Henderson et al., 1999; Hopkins
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
t al., 2007; Rosenberg, 2009). Biotechnology was characterizeds a rational, science-driven approach to discovery, in contrasto the trial-and-error, chemical-based research platforms of the
pharmaceutical industry. This framing was a powerful force in itsadoption by both firms as well public sector policies. Billions ofdollars and a great deal of scientific resources were invested inrapidly sequencing the human genome, fuelled by the promise ofradical progress in medical innovation. Changes in policy to allowpatenting of genetic material facilitated commercialization andprivate-sector adoption of the new technologies. The Schumpete-rian character of the technology was exemplified by a US model ofcommercialization that centered on entrepreneurial start-up firmsfounded by university scientists and backed by venture capital(Gittelman, 2006; Kenney, 1986; Zucker et al., 2002).
Some forty years have passed since the initial discoveries weremade, yet the expected benefits in medical discovery have notmaterialized (LeFanu, 2012). It is estimated that in real terms, thenumber of new drugs approved in the US per billion dollars of R&Dspending has declined by half every nine years since 1950, with the
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
steepest declines in the 1980s and 2000s – precisely the era that thenew scientific paradigm emerged (Scannell et al., 2012). As block-buster drugs lose patent protection, the rate of discovery of newdrugs has not been sufficient to maintain a robust R&D pipeline
Kola and Landis, 2004). In the face of a perceived R&D productiv-ty crisis, many large pharmaceutical firms are reducing R&D andhuttering entire branches of research (Jack, 2011).
The problem of declining productivity of discovery is puzzling, paradox even: why have scientific breakthroughs in biology,s well as vastly improved analytical techniques, failed to yieldhe expected gains in medical innovation? Current medical policyddresses this question by pointing to institutional failures, as wells time lags, in the translation of basic science to clinical settingsCockburn, 2006; Collins, 2011; Mullard, 2011). This paper devel-ps a different perspective, to consider the role of different scientificesearch paradigms in the productivity of drug discovery. I contrastwo distinct paradigm in medical research: patient-oriented clin-cal research and discovery based on the science of genetics and
olecular biology. The former was central in the post-war insti-utional landscape, whereas the latter emerged as important inhe 1980s and 1990s. The two paradigms represent distinct andompeting logics of discovery: genetics-based approaches repre-ent a predictive, theory-driven search logic that abstracts fromatural complexity, whereas clinical research is an experiential,
eedback-based search process using study objects as they exist inhe natural world. They are distinguished by an epistemic divide inheir beliefs about the usefulness of understanding disease causal-ty as a starting point of discovery. As a result, the origin points andubsequent search unfold differently in each of the two paradigms.
core argument is that these practices have implications forhe relative performance of each search paradigm in medicaliscovery.
The comparison of the two paradigms is guided by the largerebate about the relative merits of predictive and experientialearch and learning routines for technological innovation. Prioresearch in the management literature has stressed the power ofredictive science and analytics for innovation when technologicalroblems are complex (e.g., Arora and Gambardella, 1994; Flemingnd Sorenson, 2004). However, the idea that more science yieldsetter technology has been challenged by the claim that the logic ofasic science is fundamentally ill-equipped to solve many complexechnological problems, and indeed may conflict with techno-ogical learning. This perspective stresses different evolutionaryogics of scientific and technological knowledge, such that discov-ry in each unfolds largely independently of the other (Nelson,003; Nightingale, 1998; Pavitt, 1998; Gittelman and Kogut, 2003;incenti, 1993). In line with this perspective, many in the medicalolicy literature have pointed out that most major medical discov-ries originated at the bedside rather than the bench, and that thepplication of genetics and molecular science to medical discov-ry could hinder, rather than accelerate, progress (LeFanu, 2012;elijns and Rosenberg, 1994; Gelijns et al., 1998; Rees, 2002a; Vos,991). This claim partly reflects the remarkable postwar recordf clinical research: the period following World War II has beenalled the “Golden Age of Clinical Research” because of the unprece-ented wave of treatments and health-enabling technologies that
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
ere developed by scientists working in clinical research settingsAhrens, 1992; Mitra, 2009; Swazey and Fox, 2004).1
1 Mitra (2009) details the unprecedented wave of drugs and other innovations dis-overed in clinical settings in the post-war period: penicillin and other antibiotics;treptomycin for tuberculosis; cortisone for immune system disorders; chlorpro-azine, which changed understanding and treatment of psychiatric disorders and
aid the basis for modern psychiatry; chemotherapy drugs; immune-suppressantsor organ transplantation; polio vaccine; and contraceptive medications. Treatmentsnd devices included cardio-pulmonary bypass and open heart surgery, cardiacatheterization, organ transplantation, joint replacement, renal dialysis, intra-ocularens implant, cochlear implant, in vitro fertilization; the invention of the ventila-or and intensive care of infants; the operating microscope, fiber-optic endoscope,
PRESScy xxx (2016) xxx–xxx
The historical centrality of clinical research in medical discov-ery and its subsequent decline raises the question of how and whya new scientific paradigm emerged in the research landscape. Didclinical research face diminishing returns, with the low-hangingfruits of discovery already picked, such that the emergence ofgenetics and molecular-based approaches represented a radicalshift toward a new and more productive research paradigm? Or wasits role in medical research diminished by changing institutionalforces that were largely independent of technological selection(Ahrens, 1992; Nathan, 2002)? Understanding the answer to thisquestion is important for an effective diagnosis of the productiv-ity decline in drug discovery, as well as the design of effectiveorganizational and public policies to address it.
This paper tackles the link between research paradigms anddiscovery by analyzing the two paradigms from both a con-ceptual as well as a historical perspective. I describe how theprocess of drug discovery unfolds in the genetics and clinicalresearch paradigms. The two paradigms are distinguished by dif-ferences in their origin points and the types and timing of feedbackthat guide sequential decision-making: in the clinical researchparadigm, observation from humans forms the starting point ofinvestigation, and feedback from patients is used to guide fur-ther investigations. In the genetics model, models of interactionsat the sub-cellular/molecular level form the initial point of dis-covery, with information from intact human subjects entering atthe testing stages. A central claim is that the highly uncertain andvariable nature of human biology means that early feedback fromhuman subjects is important in the discovery process, such thatmodels of fundamental causality at the molecular level – whilevaluable for further scientific research – are of limited utility inas guides to technological search. The implication is that the clini-cal research paradigm is comparatively advantaged at discoveringdrugs that will operate effectively in humans, and that this advan-tage is robust to advances in fundamental biological science. In thisperspective, the historically central role of doctors in medical dis-covery does not reflect a lag in basic science, but the persistentlimitations of basic science and predictive theory to develop tech-nologies that will be effective in highly complex, variable naturalphenomena.
The second part of the paper questions the dominant narrativeof biotechnology as a Schumpeterian revolution that emerged toovertake a largely exhausted research trajectory based on random,trial-and-error discovery. This framing neglects the substantialUS investment in the postwar period to build an institutionalinfrastructure that would provide support for academic cliniciansworking in a network of Academic Medical Centers, in close col-laboration with chemists in pharmaceutical firms. I describe themultiple factors that, following the rise of the clinical paradigmin biomedical research in the 1950s and 1960s, led to its weaken-ing in the 1970s and 1980s: changes in healthcare and insuranceand policies that put budgetary pressure on teaching hospitals andshortened in-patient care cycles; increased bureaucratization ofacademic hospitals; and declining career opportunities for youngphysician-researchers. Concurrent with these changes, recombi-nant DNA and related techniques were discovered in universitylaboratories which previously had little or no application to medicalresearch. In the US, translation of the basic science to medical appli-cations was propelled by a Silicon Valley model adapted from thetechnology sector, characterized by venture-capital backed firms
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
spun off from university research.The history reveals the decline of support for clinical research
can be tied to institutional and policy shifts that were largely
cardiac pacemaker, laser, ultrasound, isotope scan, CT, MRI, and PET scans, and thelinear accelerator.
with other knowledge across a broad range of problems (Flemingand Sorenson, 2004) and is helpful in narrowing down the rangeof options for further testing (Nelson, 1982; Thomke et al., 1998).
ARTICLEESPOL-3232; No. of Pages 16
M. Gittelman / Researc
ecoupled from evolutionary processes of scientific or technologi-al selection. I argue that the decline of clinical research and the risef genetics-based discovery techniques were not causally related,ut their temporal coincidence, and the framing of genetics as
revolutionary technology in medicine, meant they were jointlynstrumental in shifts in the centrality of research paradigms in theiomedical landscape.
The organization of the paper is as follows. In Section 2, I con-rast experiential and theory-drive research paradigms (2.1), andow institutional arrangements accommodate learning in each2.2). Section 2.3 lays out the theoretical debate about the rela-ive performance of these different search logics in solving complexechnological problems. The general discussion about search andomplexity in Section 2 is then applied to the specific case of drugiscovery in Section 3. The challenge of complexity in biology isiscussed (3.1), followed by the application of the framework devel-ped in Section 2 to drug discovery (3.2). Sections 4 and 5 lay outhe comparison of the clinical research paradigm (Section 4) and theenetics paradigm (Section 5) in drug discovery, from an epistemics well as historical/institutional perspective. Section 4.2 describesn some detail the history of the clinical paradigm in the postwareriod and the reasons for its decline. There have been many insti-utional histories of biotechnology; therefore, Section 5 emphaseshe importance of predictive models in this paradigm, the framingf the technology as a rational, science-driven approach to dis-overy, and the entrepreneurial model that emerged in the US toommercialize the science. Section 6 reviews secondary evidenceo evaluate the central claim that the clinical research paradigms relatively advantaged in discovery as compared to the genet-cs paradigm. Section 7 concludes with a discussion of the currentranslational science model as a useful framework in diagnosinghe productivity paradox in medical discovery.
The relative merits of theoretical and practical knowledge haveeen debated since ancient times. Plato and Aristotle – both believ-rs in the universal laws of nature – differed over the roles ofbstract reason (logos) and observation of things in nature (nomos)n discovery. Victorian-era historians resisted the role played byccidental discovery in scientific experimentation, arguing that sci-ntific principles provided for a rational and planned method fordvancing knowledge (Merton and Barber, 2004). Post WWII sci-nce policy was framed around the idea that government-fundedasic science is an engine for industrial R&D (Stokes, 1997), andurrent medical policy similarly conceives of basic research as anngine of technological innovation.
The major paradigms that have characterized bio-medicalesearch in the postwar period, clinical research and genetics, cor-espond to these broad categories of knowledge. Clinical researchs oriented to generating practical knowledge that can be appliedo alleviate human suffering, and genetics/molecular biology buildspon fundamental knowledge of biological processes.
Rather than categorize these fields as “basic” and “applied”esearch, it is useful to conceive of them as sets of beliefs andnternally consistent practices that set in motion distinctive log-cs of search. Doing so allows an analysis of specific search routinesnd their approach to complex problems, such as encountered in
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
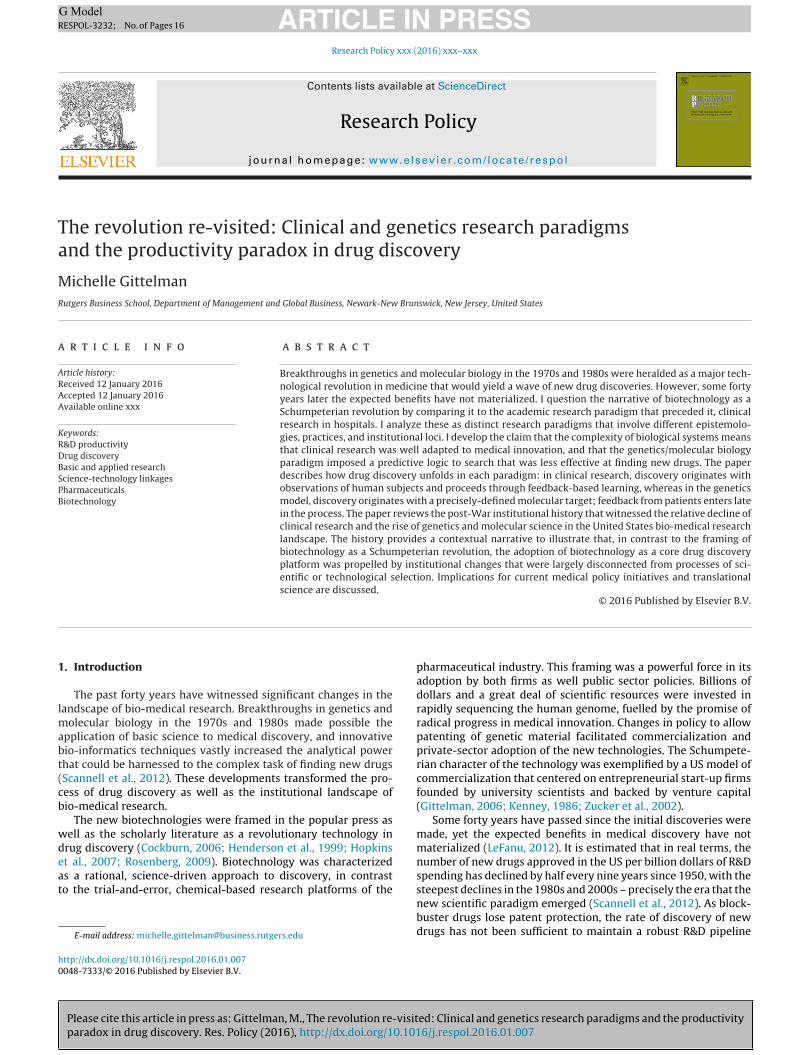
edicine. Fig. 1 provides a representation of two dimensions alonghich search paradigms may vary. The horizontal axis represents
he routines, empirical methods, and tools that are employed in theearch process. The vertical axis shows the type of knowledge that
Fig. 1. Search logics.
emerges from search, whether intentionally or as a byproduct.2 Iconsider each in turn.
On the left side of the horizontal axis is experiential search.Experiments reproduce, to varying degrees, real-world conditionsand utilize objects that resemble phenomena as they exist in theirnatural states. Learning is thus conducted “online” and is “back-wards looking” in the sense that it proceeds sequentially, throughfeedback gained from experiments designed to mimic real-worldcontexts (Dougherty and Dunne, 2011; Gavetti and Levinthal, 2000;Thomke et al., 1998). Experimentation accommodates the com-plexity of the problem being studied rather than reducing objects totheir essential properties (Nightingale, 1998). For instance, admin-istering an experimental blood pressure drug to rats in a controlledsetting uses real-world analogs – animals and drugs – that simu-late the intended objects of study, and generates feedback aboutwhether to proceed to further testing in closer analogs, such as ina human clinical trial.
Toward the right end of the horizontal axis is theory-drivensearch. Whereas experiential search is based on post hoc learn-ing from experimental feedback, theory-driven search follows apredictive, forward-looking logic (Gavetti and Levinthal, 2000).Theories of cause-effect relationships guide experimental design.Theory-driven search is reductionist, simplifying phenomena asthey exist in nature to their essential properties. Validation andtesting occur “offline”, utilizing simulations, models and instru-ments that are abstractions of complex, real-world settings (Aroraand Gambardella, 1994).
Along the vertical axis are the types of knowledge that emergefrom the search process. Abstract knowledge relates to principles,causal relationships, universal laws, frameworks and understand-ings that are stripped of the details describing the operation of realobjects in specific contexts. Abstract knowledge can be recombined
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
2 While similar to Stokes’ (1997) diagram showing Pasteur’s Quadrant, this frame-work does not impose a priori motives – e.g. quest for fundamental understanding –on post hoc outcomes; it shows research strategies and knowledge as independentdimensions, though as discussed, strong complementarities in the upper right andlower left quadrants.
general theory of the causes of high blood pressure may be use-ul in narrowing down predictions about the classes of drugs mostikely to be effective in treating the disease.
Contextualized knowledge relates to understandings of howeal objects function in the real world. Unlike abstract knowledge,ontextualized knowledge is wedded to the myriad unexplainedetails that attend to the functioning of objects in action. Contextu-lized knowledge may be useful even if the functions and actions ofhe underlying relationships are not be fully characterized nor wellnderstood. Moreover, contextualized knowledge is of limited useor problems outside the range of experimental search. Feedbackbout a drug’s effect on lowering the blood pressure of a group ofatients is useful for further testing of that drug, but may not shed
ight on the causes of high blood pressure, nor how well the drugill work on people outside of the experimental setting.
.2. Search logics and institutional complementarities
There is a natural complementarity in the upper right and lowereft quadrants of Figure 1: theory-driven search is generally aimedt producing deeper theoretical understandings, and experientialearch seeks to produce objects that function reliably in real-worldettings. These complementarities mean that specialized institu-ional settings can be designed to accommodate and incentivizeach kind of search. In the upper right quadrant, universities adhereo the norms of “open science”, rewarding faculty for producingnd sharing theoretical knowledge. Scientists working in universityabs, institutionally freed from the constraint of having to imple-
ent their ideas into functioning objects, can apply theoreticalnowledge to produce findings that yield new knowledge whoserimary or sole utility is to test and advance theory. Firms seek arepecialized to search in the lower left quadrant, and seek to developseful products; their incentives reward research that yields prod-cts that can be sold in a market.
The lower right and upper left quadrants lack these natural com-lementarities between search routines and knowledge. In theseuadrants, hybrid organizational forms and institutional arrange-ents have emerged to accommodate these mixed-mode search
aradigms. Nelson and Rosenberg (1994) describe how the jointperation of experiential learning and fundamental insights (uppereft quadrant) have been institutionalized in numerous new disci-linary initiatives. Indeed, many applied fields such as chemicalnd electrical engineering, aeronautics and computer science wereounded by practitioners or academics seeking to fill gaps leftetween basic science and technological research. They are notbridges” in the sense of applying basic understandings to prac-ical applications, but have emerged as distinct and independentelds of inquiry in their own right. Specialized biotechnology firmsre examples of hybrid institutions in the lower right quadrant;hey aim to develop practical technologies from basic science, andften employ a mix of incentives and practices from universitiesnd firms.
.3. Search paradigms and complexity
The relative performance of experiential and theory-drivenearch has recently been explored in the context of innovation inomplex technological fields. Gavetti and Levinthal (2000) defineomplex fields as systems of variables characterized by a high den-ity of inter-relationships; using the metaphor of a landscape, theyhow that as these relationships multiply, localized peaks emergen the search space, and these may confound attempts to find
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
lobally-optimal solutions using feedback-based learning routines. hiker in the Alps who, lacking a map, uses gravitational pull as therimary guide to search would not necessarily know, upon arriv-
ng at a mountaintop, whether she had arrived at a low-level peak
PRESScy xxx (2016) xxx–xxx
or whether higher peaks lay beyond. They claim that in such com-plex landscapes, predictive theory can be a useful guide to searchfor globally optimal solutions. Fleming and Sorenson, building onthat work, propose that scientific knowledge provides a map fortechnological innovation, such that when technological problemsare complex, scientific research guides technological researcherstoward important discoveries (Fleming and Sorenson, 2004). Aroraand Gambardella (1994) similarly propose that scientific methodsand advanced computing power allow for knowledge to be cast inuniversal frameworks and categories, which can be usefully appliedto solve complex technological problems.
This claim that science provides a useful guide to technologi-cal search has been challenged by the argument that is preciselywhen problems are complex that predictive search and scientificknowledge are unlikely to be applied to technological discovery(Nightingale, 1998, 2004; Pavitt, 1998; Nelson, 2003; Vincenti,1993). Rejecting the idea that complexity is an exogenous prop-erty of a technological field, complexity is viewed as a symptomof an underdeveloped understanding of variables and their inter-relationships. When natural phenomena are highly complex andvariable, there is a considerable distance between the power ofpredictive rules and the unpredictable outcomes that emerge invariable states of nature (Nightingale, 1998). Reframing complex-ity as endogenous to the extant state of knowledge suggests thatit is a tautology to state that causal theories are useful in solvingcomplex problems: problems appear complex when researchers donot understand them, not the other way around (Rees, 2002a).
If complexity is understood as endogenous to knowledge, thengeneral theories are lacking; instead, experiments using closeanalogs to the objects of study can generate important cluesabout key variables and their interactions (Dougherty and Dunne,2011; Nightingale, 1998; Vincenti, 1993). Online experimentationprovides “sharp feedback” about system-wide performance andfunctional relationships about study phenomena as they operatein natural settings. Observation of these patterns can help developrobust design principles that are based on mechanistic interven-tions, rather than fundamental causal relationships, which mayremain obscure (Nelson, 2003; Vincenti, 1993). Search is cumu-lative, advancing by recognizing similarities across a range ofproblems that may have no apparent causal explanation connect-ing them; serendipity plays a particularly salient role in this type ofexploration (Nightingale, 1998; Merton and Barber, 2004). Discov-ery happens when the searcher understands how a given outcomefits with a stream of prior, similar patterns and is able to hypothe-size a common solution (though not necessarily a common cause)for these functionally related events. In this way, insights into com-plex phenomena may emerge largely independent of predictivetheory, and attempts to enforce predictability and strip out contex-tualized variability in an experimental setting may actually reduceopportunities for discovery (Nightingale, 1998, 2004; Vincenti,1993). Indeed, in many technological fields (including medicine),feedback-based search using real-world objects triggers subse-quent theorizing of underlying causal mechanisms, rather than theother way around (Nightingale, 2004; Pavitt, 1998; Nelson, 2003).
In Section 3 below, I describe how the general frameworkdescribed above can be applied to research paradigms in drug dis-covery.
3. Search paradigms in drug discovery
3.1. The challenge of drug discovery: the body as a complex
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
system
The central challenge of drug discovery is the profound com-plexity of human physiology. The human body represents a
Medicinal and synthe�c chemistry; chemical libraries
Large pharmaceu�cal firms
Target-based drug discovery High throughput screening
Biotechnology firms
DrivenTheoryExperien�al
1950s-1970s
1980s-2000s
Type of search
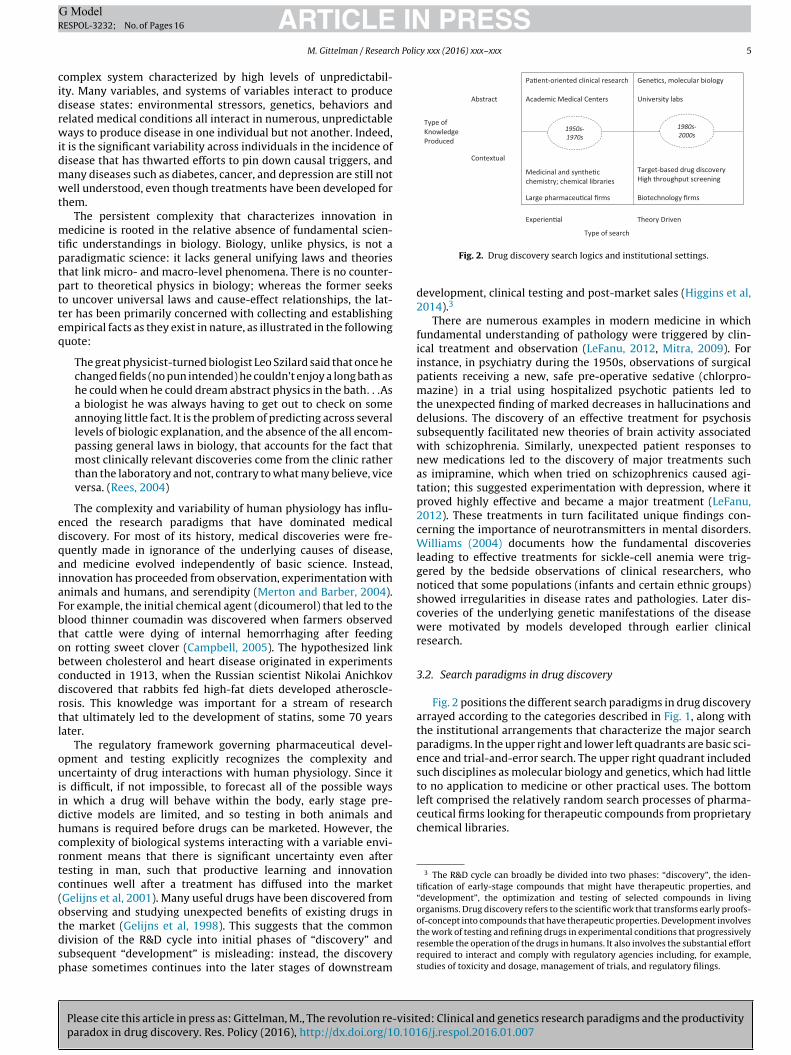
left comprised the relatively random search processes of pharma-ceutical firms looking for therapeutic compounds from proprietarychemical libraries.
3 The R&D cycle can broadly be divided into two phases: “discovery”, the iden-tification of early-stage compounds that might have therapeutic properties, and“development”, the optimization and testing of selected compounds in livingorganisms. Drug discovery refers to the scientific work that transforms early proofs-of-concept into compounds that have therapeutic properties. Development involves
ARTICLEESPOL-3232; No. of Pages 16
M. Gittelman / Researc
omplex system characterized by high levels of unpredictabil-ty. Many variables, and systems of variables interact to produceisease states: environmental stressors, genetics, behaviors andelated medical conditions all interact in numerous, unpredictableays to produce disease in one individual but not another. Indeed,
t is the significant variability across individuals in the incidence ofisease that has thwarted efforts to pin down causal triggers, andany diseases such as diabetes, cancer, and depression are still notell understood, even though treatments have been developed for
hem.The persistent complexity that characterizes innovation in
edicine is rooted in the relative absence of fundamental scien-ific understandings in biology. Biology, unlike physics, is not aaradigmatic science: it lacks general unifying laws and theorieshat link micro- and macro-level phenomena. There is no counter-art to theoretical physics in biology; whereas the former seekso uncover universal laws and cause-effect relationships, the lat-er has been primarily concerned with collecting and establishingmpirical facts as they exist in nature, as illustrated in the followinguote:
The great physicist-turned biologist Leo Szilard said that once hechanged fields (no pun intended) he couldn’t enjoy a long bath ashe could when he could dream abstract physics in the bath. . .Asa biologist he was always having to get out to check on someannoying little fact. It is the problem of predicting across severallevels of biologic explanation, and the absence of the all encom-passing general laws in biology, that accounts for the fact thatmost clinically relevant discoveries come from the clinic ratherthan the laboratory and not, contrary to what many believe, viceversa. (Rees, 2004)
The complexity and variability of human physiology has influ-nced the research paradigms that have dominated medicaliscovery. For most of its history, medical discoveries were fre-uently made in ignorance of the underlying causes of disease,nd medicine evolved independently of basic science. Instead,nnovation has proceeded from observation, experimentation withnimals and humans, and serendipity (Merton and Barber, 2004).or example, the initial chemical agent (dicoumerol) that led to thelood thinner coumadin was discovered when farmers observedhat cattle were dying of internal hemorrhaging after feedingn rotting sweet clover (Campbell, 2005). The hypothesized linketween cholesterol and heart disease originated in experimentsonducted in 1913, when the Russian scientist Nikolai Anichkoviscovered that rabbits fed high-fat diets developed atheroscle-osis. This knowledge was important for a stream of researchhat ultimately led to the development of statins, some 70 yearsater.
The regulatory framework governing pharmaceutical devel-pment and testing explicitly recognizes the complexity andncertainty of drug interactions with human physiology. Since it
s difficult, if not impossible, to forecast all of the possible waysn which a drug will behave within the body, early stage pre-ictive models are limited, and so testing in both animals andumans is required before drugs can be marketed. However, theomplexity of biological systems interacting with a variable envi-onment means that there is significant uncertainty even afteresting in man, such that productive learning and innovationontinues well after a treatment has diffused into the marketGelijns et al, 2001). Many useful drugs have been discovered frombserving and studying unexpected benefits of existing drugs inhe market (Gelijns et al, 1998). This suggests that the common
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
ivision of the R&D cycle into initial phases of “discovery” andubsequent “development” is misleading: instead, the discoveryhase sometimes continues into the later stages of downstream
Fig. 2. Drug discovery search logics and institutional settings.
development, clinical testing and post-market sales (Higgins et al,2014).3
There are numerous examples in modern medicine in whichfundamental understanding of pathology were triggered by clin-ical treatment and observation (LeFanu, 2012, Mitra, 2009). Forinstance, in psychiatry during the 1950s, observations of surgicalpatients receiving a new, safe pre-operative sedative (chlorpro-mazine) in a trial using hospitalized psychotic patients led tothe unexpected finding of marked decreases in hallucinations anddelusions. The discovery of an effective treatment for psychosissubsequently facilitated new theories of brain activity associatedwith schizophrenia. Similarly, unexpected patient responses tonew medications led to the discovery of major treatments suchas imipramine, which when tried on schizophrenics caused agi-tation; this suggested experimentation with depression, where itproved highly effective and became a major treatment (LeFanu,2012). These treatments in turn facilitated unique findings con-cerning the importance of neurotransmitters in mental disorders.Williams (2004) documents how the fundamental discoveriesleading to effective treatments for sickle-cell anemia were trig-gered by the bedside observations of clinical researchers, whonoticed that some populations (infants and certain ethnic groups)showed irregularities in disease rates and pathologies. Later dis-coveries of the underlying genetic manifestations of the diseasewere motivated by models developed through earlier clinicalresearch.
3.2. Search paradigms in drug discovery
Fig. 2 positions the different search paradigms in drug discoveryarrayed according to the categories described in Fig. 1, along withthe institutional arrangements that characterize the major searchparadigms. In the upper right and lower left quadrants are basic sci-ence and trial-and-error search. The upper right quadrant includedsuch disciplines as molecular biology and genetics, which had littleto no application to medicine or other practical uses. The bottom
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
the work of testing and refining drugs in experimental conditions that progressivelyresemble the operation of the drugs in humans. It also involves the substantial effortrequired to interact and comply with regulatory agencies including, for example,studies of toxicity and dosage, management of trials, and regulatory filings.
pronethalol, fuelling the emergence of a new field of cardiovascularresearch.
ARTICLEESPOL-3232; No. of Pages 16
M. Gittelman / Researc
Bio-medicine is a hybrid search process in that it relies heavilyn scientific understandings, but also seeks to produce functionalolutions that are effective, safe, and reliable in highly complexnd variable natural contexts (human organisms). In the post-wareriod, hybrid institutional arrangements emerged to accommo-ate learning in both the upper left and lower right quadrants. In the940s, the clinical sciences and bio-statistics, that allowed for con-rolled clinical trials, emerged as important new fields in medicalesearch. In the 1950s, US Federal policy encouraged the creation ofcademic Medical Centers that were designed as hybrids betweenospitals, medical training schools and university research labs,o integrate the skills of physicians and laboratory researchers inhe search for new treatments. Clinical researchers collaboratedlosely with pharmaceutical firms to explore and develop new com-ounds.
In the 1970s and early 1980s, breakthroughs in the sciencef genetics and molecular biology occurred in basic science labsf universities and introduced a new paradigm to drug discoveryocused on the manipulation and analysis of genetic information.his shifted the locus of innovation from academic hospitals andhysician-researchers to PhD scientists working in basic science
abs. In order to effectively commercialize their discoveries, univer-ity scientists formed start-up firms that were hybrids in the sensehat they engaged in both commercial innovation and engagedn “open science”, adopting many of the scientific practices andeward systems of universities (Gittelman and Kogut, 2003). Theseew firms, represented in the lower right quadrant, served as aridge between the discoveries made in basic science and a marketor new medical treatments.
Thus, the post-war period in medicine was characterized by twoistinct paradigms of search, accompanied by important changes inhe institutional locus of innovation and patterns of collaboration.n the following two sections (4 and 5) I describe each in detail. Eachection discusses the epistemic foundations of search and the waysn which drug discovery unfolds within that paradigm, as well ashe institutional and organizational arrangements that emerged toccommodate these distinctive approaches to drug discovery.
. The clinical research paradigm
.1. The drug discovery process
Modern clinical research encompasses a wide range of medicalpecialties (biochemistry, pathology, pharmacology, epidemiol-gy), but the unifying theme, as defined by leading NIH researchers,s “research performed by a scientist and a human subject work-ng together, both being warm and alive” (Schechter, 1998). Thelinical research paradigm is thus intimately connected to theractice of medicine and the delivery of healthcare in hospital set-ings.
The clinical research paradigm rejects disease causality as aseful starting point in the drug discovery process. In the clinicalaradigm, causes and solutions can be cast as two different, discon-ected endpoints. Causal explanations of disease, while potentiallyseful understanding initial triggers, are seen as secondary tohe task of finding solutions: variables that initiate perturbationsuch as disease states may be far removed from the variableshat will be successful in reversing them. Mechanistic insights,s opposed to fundamental understandings, are used to guideearch for medical interventions (Carlsson, 2003; Rees, 2002a,b,004). Research originates with observations of patients or near
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
nalogs of patients (clinical subjects or animals). Because causesre de-coupled from solutions, search for interventions is targetedt the localized site of the perturbation – expressed symptoms –ather that initial causes (Carlsson, 2003).
PRESScy xxx (2016) xxx–xxx
An example of the role of experimental observation of patientsymptoms in developing solutions is given by the case of per-nicious anemia, a complex, inheritable autoimmune disease thatis usually fatal. In that case, an initial understanding of causalitywas not the key to finding a treatment; it hinged on experimentsin which patients were fed different foods, until one – liver –caused the symptoms to subside. This mechanistic insight, madein the 1920s, was a first step in developing a treatment; how-ever, it took decades before the active ingredient, vitamin B12,was isolated. While addressing this deficit cured the disease, thevitamin deficiency was not the main cause of the disease, but wasmerely one of many complex symptoms and causal factors (Rees,2002b).
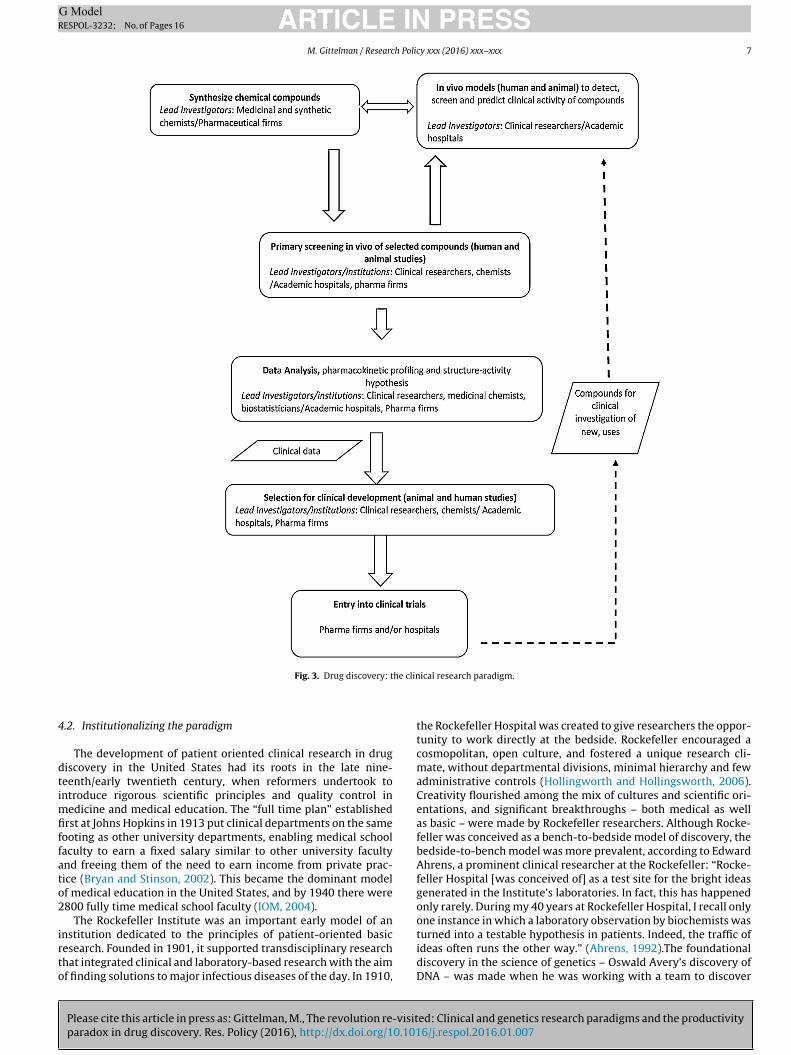
Fig. 3 depicts the main stages involved in discovery as prac-ticed in the modern (post-War) clinical paradigm. The processcentered on collaborations between clinical investigators, usuallyworking in academic hospitals, and medicinal chemists, usuallyworking in pharmaceutical companies (Lombardino and Lowe,2004). Industrial chemists in large pharmaceutical firms createdand maintained proprietary libraries of synthesized compoundsthat could be screened for therapeutic properties, a slow, expen-sive and labor-intensive process. Clinical researchers workingwith patient populations helped shape and guide that work, pro-viding hypotheses about new indications for drugs. In return,medicinal chemists supplied synthesized compounds in quanti-ties sufficient for clinical research (Lombardino and Lowe, 2004;Vos, 1991). In these close-knit (and largely unregulated) rela-tionships, clinicians had access to proprietary compounds toexperiment with and explore new uses in their patients (LeFanu,2012).
As discussed above, researchers generally begin with mecha-nistic theories of effective interventions rather the fundamentalcauses of disease (Vos, 1991). With chemical synthesis a time-consuming and laborious process, the creativity of the medicinalchemist was important in carefully synthesizing new compoundsthat were likely have the expected properties (Scannell et al.,2012). A benefit of what was effectively phenotypic screening(in humans) was that real data about a drug’s properties in manwere obtained very early in the process. Drawbacks were that itwas a slow, costly and time-consuming process, and early com-pound libraries and clinical populations provided limited samplesizes.
Collaborative, iterative exploration between industrial medic-inal chemists and academic clinical researchers frequently led tounexpected discoveries as well as new theoretical models of dis-eases. Vos (1991) describes how this process led to the rapidbranching of new indications for beta blockers in the mid-1960s.According to James Black, the famed pharmacologist/chemist whodeveloped the beta blocker propranolol while working for Britishchemical firm ICI: “When a drug with a new pharmacological actionbecomes available it is liable to be tried clinically in disorderswhich were not foreseen during its laboratory development. Theumbilical connexion with the laboratory has been cut and wemust rely on the vision of the clinician and be grateful for this.”(Vos, p. 91).4 As a result of explorations in clinical settings, rep-resented by the arrow going up the right side of Fig. 3, sevennew indications emerged within a few years for the beta blocker
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
4 Black’s discovery of propranolol represented one of the rare “science-driven”drug development projects of the era with discovery focused on a specified receptor;it is noteworthy that he nonetheless made this remark about the value of clinicalexploration.
ARTICLE IN PRESSG ModelRESPOL-3232; No. of Pages 16
M. Gittelman / Research Policy xxx (2016) xxx–xxx 7
he clin
4
dtimfiffato2
irto
Fig. 3. Drug discovery: t
.2. Institutionalizing the paradigm
The development of patient oriented clinical research in drugiscovery in the United States had its roots in the late nine-eenth/early twentieth century, when reformers undertook tontroduce rigorous scientific principles and quality control in
edicine and medical education. The “full time plan” establishedrst at Johns Hopkins in 1913 put clinical departments on the same
ooting as other university departments, enabling medical schoolaculty to earn a fixed salary similar to other university facultynd freeing them of the need to earn income from private prac-ice (Bryan and Stinson, 2002). This became the dominant modelf medical education in the United States, and by 1940 there were800 fully time medical school faculty (IOM, 2004).
The Rockefeller Institute was an important early model of an
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
nstitution dedicated to the principles of patient-oriented basicesearch. Founded in 1901, it supported transdisciplinary researchhat integrated clinical and laboratory-based research with the aimf finding solutions to major infectious diseases of the day. In 1910,
ical research paradigm.
the Rockefeller Hospital was created to give researchers the oppor-tunity to work directly at the bedside. Rockefeller encouraged acosmopolitan, open culture, and fostered a unique research cli-mate, without departmental divisions, minimal hierarchy and fewadministrative controls (Hollingworth and Hollingsworth, 2006).Creativity flourished among the mix of cultures and scientific ori-entations, and significant breakthroughs – both medical as wellas basic – were made by Rockefeller researchers. Although Rocke-feller was conceived as a bench-to-bedside model of discovery, thebedside-to-bench model was more prevalent, according to EdwardAhrens, a prominent clinical researcher at the Rockefeller: “Rocke-feller Hospital [was conceived of] as a test site for the bright ideasgenerated in the Institute’s laboratories. In fact, this has happenedonly rarely. During my 40 years at Rockefeller Hospital, I recall onlyone instance in which a laboratory observation by biochemists was
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
turned into a testable hypothesis in patients. Indeed, the traffic ofideas often runs the other way.” (Ahrens, 1992).The foundationaldiscovery in the science of genetics – Oswald Avery’s discovery ofDNA – was made when he was working with a team to discover
golden opportunity it provides for medical investigators andtheir staffs to watch carefully and to think deeply about themedical challenges posed by their patients; this forces them
5 The plan was not uncontroversial. It was opposed by science policy architectVannevar Bush who promoted government funding of basic, not applied, research,and the NIH was focused on biology and chemistry without direct clinical relevance(Chung, 2007). Despite Bush’s opposition, those who favored a strong medical anddisease-management orientation at the NIH prevailed (Nathan and Schechter, 2006;Schechter, 1998). The debate over NIH investment in basic and applied R&D was notpurely philosophical: Rasmussen (2002) points out that Bush’s advocacy of govern-
ARTICLEESPOL-3232; No. of Pages 16
M. Gittelman / Researc
cure for pneumonia. Josh Lederberg, the Nobel-prize winningeneticist wrote: “[Avery’s] discovery [of DNA] is an outstandingxample of the feedback of clinically motivated inquiry to the mostasic issues of fundamental biomedical science” (Lederberg, 1994).
At the same time, clinical sciences were emerging as a scholarlyiscipline: the first randomized clinical trials were conducted in theK in 1948, and statistical methods were developed for large-scalelinical studies that could validate small differences between treat-ent regimens. Advances in medical technologies opened up new
venues of investigation. Major advances in quelling human diseaseere being made at the time through breakthroughs in physiol-
gy, biochemistry, and pharmacology, and a host of new drugsere developed to treat infectious disease, particularly antibiotics.
rapid period of growth in training of researchers followed theecond World War, and by 1960 there were 11,300 medical schoolaculty (IOM, 2004).
The period witnessed the growth of investment in new Aca-emic Medical Centers attached to universities (IOM, 2004). These
nstitutions, which delivered hospital care in a research setting,ere characterized by a close interaction between scientists of dif-
erent disciplines and an integration of experimental work withlinical activity, a novel combination that set the US medicalesearch system apart from the more discipline-based Europeanystem. Trainees described a “milieu of inquiry and freedom” thatncouraged risk-taking and curiousity-driven science (Swazey andox, 2004).
The physician-scientist (MD/PhD) became a central, high-tatus professional career track in the rapidly growing biomedicalesearch infrastructure. These investigators were trained to betriple threats” with skills in medical practice, research, andeaching. At the center of their clinical training was systems phys-ology, an integrative discipline that grounded their knowledgen human disease (Swazey and Fox, 2004). A position at one ofhe top AMCs, the Rockefeller Institute, or the newly-founded NIHas considered a prestigious and desirable position for a younghysician-investigator. The small size of the institutions enabled
unior investigators to be trained by or work alongside the influ-ntial scientists working in those institutions. Contrasting withuropean labs, in which senior directors acted as patrons of junioresearchers and careers advanced in more hierarchical structures,he more open environment of medical research in the US helped tottract talent from Europe and elsewhere to the US research systemSwazey and Fox, 2004).
The centrality of clinical facilities in US medical researcheflected both the important role of hospitals in the healthcareystem, as well as the federalization of research in the post-wareriod. Long-term hospitalization was a common practice, and wasn invaluable resource for both medical training and for clinicalesearch, affording clinical investigator access to patients on a long-erm basis (Bloom, 2003). Teaching hospitals were sites where bothesearchers and patients had access to advanced medical technol-gy. Lab technicians mentored early-career physician-researchers,raining them in basic science, statistics and the application of newechnologies to clinical research. Hospital stays were reimbursedy third-party insurance and, after the mid-1960s, by Federally-unded programs Medicare and Medicaid. This meant that indigentatients could be hospitalized in research hospitals, at no cost to theospitals, and revenues from patient care could be made availableo fund research. Experimentation with human subjects was unfet-ered by ethical and administrative controls, and some researchxposed patients to dangerous and risky experiments (Swazey andox, 2004).
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
.2.1. The role of the NIH and the Clinical CentersA central event in the institutionalization of clinical research
as the creation of the NIH in 1930, founded to administer a federal
PRESScy xxx (2016) xxx–xxx
grant-system on a wide range of health-related fields (Luft, 1997).The Cold War spurred rapid growth in Congressional funding formedical research: funding for the NIH grew from $700,000 in 1940to $28.5 million in 1950, to $292 million in 1959 (NIH Office ofthe Budget). The level of investment and the standard of researchin academic medical centers were far ‘higher in the US than inother countries, following a model of peer review, competitionfor grants, and a high standard of research excellence. NIH grantsfor disease-specific research in the 1950s and 1960s spurred thegrowth of clinical programs at such institutions as the Brigham,Johns Hopkins, Yale, and Duke (Swazey and Fox, 2004).
In the 1950s Initiatives were taken within the NIH to createa federally-funded institutional infrastructure to support patient-oriented research. The intention was to emulate the institutionalmodel of the Rockefeller Institute, but on a much larger scale.5 Aclinical research leg at the NIH was established, and the ClinicalCenter was founded in 1955. Based in Bethesda, the Clinical Cen-ter served as a model of patient-oriented research, and was thelargest hospital devoted to patient-oriented clinical research (Luft,1997; Nathan, 2002). Following on its success, in 1959 Congressauthorized the formation of a network of clinical centers based inacademic medical centers around the country. These centers, calledGCRC (General Clinical Research Centers), coordinated their workwith the NIH but were funded through the extramural grant systemfunding (Luft, 1997). By 1960 there were 8 centers and 133 beds; atits peak the GCRC comprised 93 centers and over a thousand bedsin 1969 (IOM, 2004). The operation of the clinical centers reflectedthe prevailing practices of healthcare delivery in the United Statesin the postwar period: long-term hospitalization, and close doctor-patient interactions (Robertson and Tung, 2001).
Each center resembled a mini-hospital that was equipped withample resources for patient care and research. The goal was to pro-vide an optimal setting for scientifically controlled clinical research.The centers were fully staffed with dedicated, full-time personnel,including specially trained nurses, medical fellows and students.Resources also included laboratory facilities and biostatistical sup-port. They were intentionally small, with no more than about 30beds, in order to foster close interaction between doctors andpatients and allow for ongoing observation of patients over a longstretch of time, an important element in a clinically-motivated dis-covery paradigm (Luft, 1997). Major clinical initiatives involvingmultiple sites and population-level data were launched, includingthe Framingham Heart Study as well as collaborative clinical trialsprogram, notably in oncology (Schechter, 1998).
Close observation of patients is an essential aspect of the PORdiscovery paradigm, as investigators look for unexpected changesthat provide important clues to pathology. Ahrens (1992) describesthis process in the context of a specially designed hospital-basedresearch lab:
Scientifically, the most important asset of a POR facility is the
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
ment funding of basic research favored large firms, which could afford in-houseR&D labs, over small ones, which could not, and therefore could benefit less frombasic science. The medical activists, including philanthropist Mary Lasker, arguedstrongly and ultimately successfully for a strong medical research orientation at theNIH.
to formulate new hypotheses and to devise new stratagemsfor attacking unsolved problems. There is time to ponder anunexpected event – an unexplained turn in the course of the dis-ease or a puzzling response to a medication – and thus to obtainfresh insights into a disease or a manipulation under study.
The NIH clinical research network played an important role inostering careers in patient-oriented clinical research. The NIH clin-cal center itself trained some 300 investigators between 1960 and980, most continuing on to research careers at AMCs (Nathan,002). To expand the ranks of researchers trained in patient-riented research an NIH training program was initiated in 1974.he CAP, Clinical Associate Physician program, provided up to threeears of salary support to junior faculty taking clinical research jobs.n addition to financial support, the program provided an opportu-ity for young investigators to advance her research to point wherehe could independently apply for NIH grant funding (Luft, 1997).
.2.2. Challenges to the clinical research paradigmBy the 1980s, the institutional infrastructure supporting POR
as in severe decline, and the population of investigators trainedn POR was stagnating. By 1979, the clinical scientist was declared toe “an endangered species” (Wyngaarden, 1981). Indeed, the num-er of physicians whose primary activity was research declinedrom about 5% of all physicians in the early 1980s to less than 2%n the mid-1990s (Ley and Rosenberg, 2005). After a rapid rise inhe number of funded beds in the GCRC system, the rate of fundingeclined, such that the number of new patient beds in the 1980sas about half of what it had been in the 1960s (Ahrens, 1992).n analysis of R01 (primary research) grants in 1991 showed thatnly 30% of grants involved the use of humans or human materials,nd of those only one third (a tenth of the total) actually involveduman subjects (IOM, 2004).
Several factors have been identified as contributing to theecline in patient oriented research: eroding institutional andnancial support for patient-oriented research; declining num-er of young investigators choosing a clinical research career; andhe rise of genetics and other reductionist methods as a dominant
odel of disease research (Ahrens, 1992). Since the practice of clini-al research is intimately tied to medical care, changes in the overallealthcare system had direct consequences for patient-orientedlinical research. The rise of managed care in reimbursements had
major impact on the sources of funding and opportunities foratient-oriented clinical research. Managed care meant that long-erm hospitalization – a cornerstone of the clinical paradigm – waso longer reimbursed, giving way to shorter stays and outpatientare. Increasing revenue pressures also encouraged the growth ofcademic Medical Centers into larger, more bureaucratic organi-ations, controlled by administrative guidelines and managerialrofessionals; the proliferation of hierarchy and administrativeontrols has been associated with a dampening of the curiousity-riven research culture that characterized AMCs in the post-wareriod. At the same time, clinical research was also made moreifficult by increasing regulation of research involving humanubjects, and the introduction of IRBs, reflecting ethical con-erns.
As a result of these changes, the optimal conditions for clinicalesearch that had been created in the postwar period deteriorated.n the late 1960s, all GCRC studies were conducted on an in-patientasis, but by 1999 only 18% of studies were conducted on an in-atient basis, with the remainder consisting of outpatient studies.ithin the GCRC system, average hospital stays in GCRCs decreased
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
rom sixteen days in the 1970s to four to six days in 1990, and theotal number of inpatient days fell from 200,000 in 1978 to 100,000n 1996, with the number of outpatient visits growing from 75,000o 300,000 in the same time period (Robertson and Tung, 2001).
PRESSy xxx (2016) xxx–xxx 9
The unique working conditions that fostered close patient-physician interaction also eroded. A greater emphasis on costcontainment in AMCs entailed greater bureaucratization; with thegrowth in size and complexity of AMCs, the physical distancebetween investigator and the clinical centers also grew. Robertsonand Tung (2001) document how investigators had been physicallylocated adjacent to the clinic in the late 1960s, effectively makingthe clinical unit a “personal research laboratory”; as AMCs grew andnew buildings were constructed, that distance increased markedly,to roughly a long city block, making close and frequent bedsideinteraction and close observation more difficult.
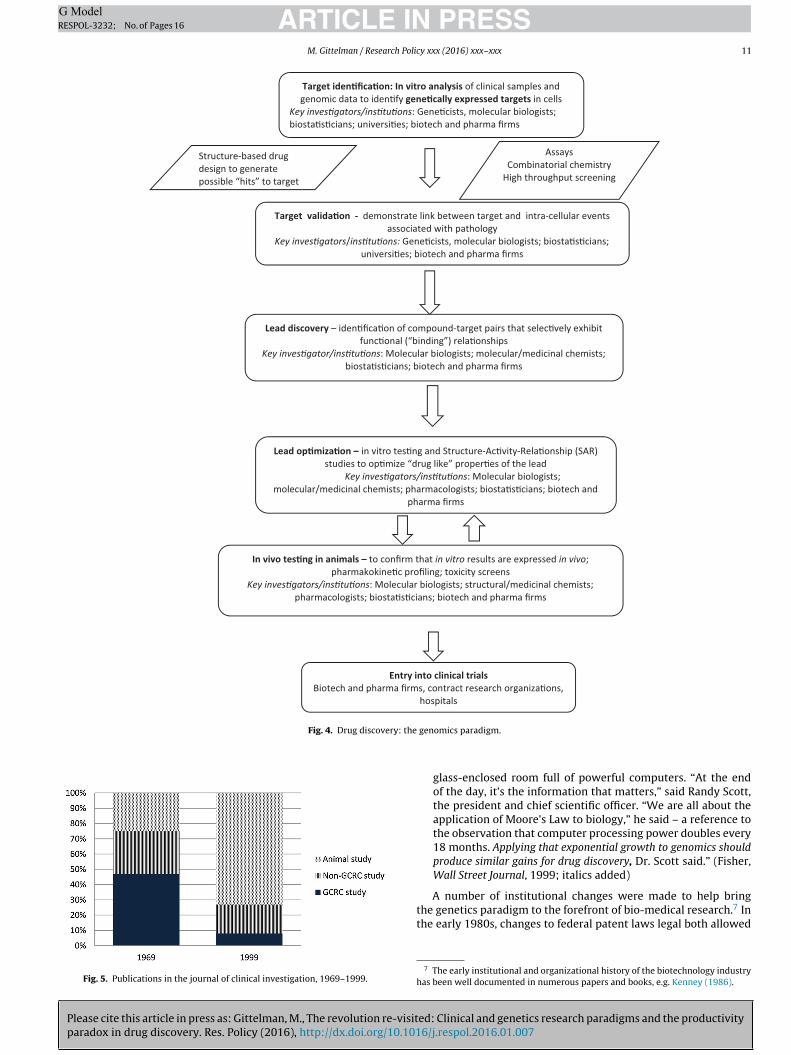
Career pressures contributed to the decline in clinical research,as fewer talented young scientists were attracted to the clinicalinvestigator career path. Faced with mounting student debt, fewermedical students chose to pursue research careers that would pro-long their training and lower wages. In the 1960s, most medicalschools revenues came from government research funds; by the1990s, medical care and private medical funds provided the lions’share, lowering incentives to train students in research (IOM, 2004).An important deterrent to a career in patient-oriented research isthe difficulty in establishing a strong publication record early ina young investigators’ career, as compared to lab-based research,animal models, and other reductionist methods. Patient-orientedresearch is slow, complex and uncertain; it is among the most costlytypes of medical research (Luft, 1997). As stricter ethical guidelineswere imposed, significant administrative functions were imposed.Moreover, the demands of patient care and teaching leave littletime for research as compared to junior scientists pursuing pureresearch (PhD) tracks. As a career path, POR grew less attractive inthe 1970s when reductionist techniques – which allow for morerapid, cheaper studies and higher number of publications – werebecoming more important. Fig. 5 shows the decline in GCRC publi-cations in a leading clinical research journal, and the marked rise instudies using animal models. Whereas clinical research had been ahigh status career, many MD-PhDs junior researchers were “stuckin the middle” of the academic hierarchy, between practitionerswith little taste for research and looked up as unscientific by purelylab-based researchers, as well as by (IOM, 2004). By the 1980s,high-status career tracks in biomedicine shifted into basic research,particularly university departments of genetics and molecular biol-ogy as well as pre-clinical departments of medical schools.
Moreover, the close personal working relationships betweenindividual investigators and pharmaceutical companies that char-acterized the earlier era were challenged by the increasingregulatory burden, as well as organizational complexity. It wasno longer possible to experiment with new compounds withoutsignificant regulatory hurdles; increasing emphasis on academicscience as a team sport – partly a reflection of increased specializa-tion of disciplines – also frayed those bonds. The role of clinicalresearch shifted from upstream discovery to downstream test-ing: while pharmaceutical companies remained important in thefunding of academic research, the character of the relationshipchanged, from one in which clinicians hypothesized and advisedcompanies on new ideas for compounds (Vos, 1991) to a model inwhich drug companies were more likely to sponsor clinical teststo be performed on their compounds, such as comparative stud-ies to show efficacy over competing treatments (Angell, 2000).There was a perception in the pharmaceutical industry that the“low hanging fruit” of medical discovery had been picked, andthat paradigm of screening chemical libraries for “hits” was facingsteep diminishing returns. Thus, the period of institutional declineof clinical research coincided with weakening ties between aca-
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
demic clinicians and the pharmaceutical industry, and pessimismin the pharmaceutical industry about the future opportunities for aresearch paradigm centered on its expertise in medicinal chemistry(LeFanu, 2012).
In contrast to the clinical paradigm, fundamental causality isentral to the genetics paradigm of drug discovery: the processs organized around the theory of a causal linkage between anrganism’s genetic makeup and pathology at the system level.he general model embedded in the paradigm – “genes causeisease” – yields the specific prediction that valuable clues inrug discovery can be found in observed correlations betweenenetically-expressed proteins within cells and disease states inrganisms (the genome-phenome linkage). Reflecting this coreausal model, genetic and molecular information provides the ini-ial starting point for new drug discovery projects, from whichcientists build theorize of macro-scale disease processes in intactrganisms.
This shift in epistemology yields differences in the ways in whichesearchers conduct their work. Dougherty and Dunne (2011)ncover sharp differences in the practices of scientists working inhe genetic paradigm from those working in the clinical model:he former frames problems and products using abstract, system-tic maps, based on identifying and following “knowns”, e.g., geneaps, to identify well-specified molecular targets for drug discov-
ry projects, while the latter group studies “unknowns”, emergentrocesses as they occur in the human body.
Fig. 4 shows the discovery process as it unfolds in the geneticsiscovery paradigm. Geneticists and molecular biologists work-
ng in university labs or private firms manipulate and analyzeenetic information to identify targets, which become the basisor “offline” drug development projects.6 Identified targets formhe starting point of the drug discovery process. Search involvesarge scale analysis and screening of data about genomic structurend function. New analytical tools and techniques, such as HTShigh throughput screening) and combinatorial chemistry, X-rayrystallography were developed in the 1980s and 1990s to pro-ess the copious amounts of data generated in genomic compoundcreening (Scannell et al., 2012). Because drugs discovered usinghe target-based approach are tailored to the molecular target, theyere expected to be much more effective and specific (affecting
nly the targeted molecules) than drugs developed through syn-hetic chemistry, which were less specific, had more actions in cells,nd therefore more side effects in humans.
An advantage of this method is that many more compoundsould be screened, at a lower cost, and knowledge of molecularnd chemical structure guides the search for compounds (Swinneynd Anthony, 2011; Eder et al., 2014). Discovery became a moreinear process, as shown in Fig. 5, with the expectation that higherhroughput would increase the productivity of finding validatedeads (Eder et al., 2014). Because compounds are tailored to bind tohe target, they were also expected to be much more effective andpecific (affecting only the targeted molecules) than drugs devel-ped through synthetic chemistry, which were less specific, hadore actions in cells, and therefore more side effects in humans.
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
s shown in Fig. 4, a drawback of this approach is that in vivo feed-ack about toxicology, efficacy and other pharmacokinetic activity
n animals and in particular, humans., arrives relatively late in the
6 Targets are molecules (mostly proteins and enzymes) that exist in the body, areroduced by DNA, and are active in metabolic processes and signaling pathwayshat, when disrupted, can trigger pathological states in an organism. Targets aredruggable” when a drug molecule can bind to a target molecule and interfere withts functioning: drugs work by interacting with targets in the cells of living organ-sms. The ability of targets to bind with drug molecules make them critical elementsy which medicines work in the human body.
PRESScy xxx (2016) xxx–xxx
discovery process. As described in Section 6 below, the timing ofclinical feedback has implications for the success and attrition ofdrugs developed through the genetic paradigm as compared to theclinical paradigm.
5.2. Institutionalizing the paradigm
The genetics paradigm represented a powerful cognitive fram-ing device that applied a forward-looking, predictive, and scientificlogic to drug discovery. The causal model linking targets to dis-eases implied a scientifically planned approach as contrasted to theprior paradigm in which discovery relied on mechanistic insightsderived from known analogs and observational data, rather than aprecisely hypothesized mechanism. As such, prior methods wereframed as unpredictable, driven by blind, trial-and-error searchrather than scientific knowledge. Indeed, the ability to specify theprecise molecular structure of targets and the molecules that mightbind to them gave rise to the phrases “rational discovery” and“designer drugs” that captured the scientific promise of the newparadigm in the early 1990s. Arora and Gambardella (1994) wrote:
Rational design of molecules is gradually replacing ran-dom, trial-and-error experiments. . .The drug industry isone where the rise of the new approach has been mostapparent. . .Growth of scientific understanding in molecularbiology and genetic engineering has clarified important aspectsof human metabolism and the chemical and biological actionof drugs. . .For instance, cell receptors in the human body haveparticular geometrical structures, and the drug molecule has tobind to them just as a key fits into a lock. By studying the struc-ture of receptors, scientists can design (typically on computer)a theoretical compound that matches a given receptor site, andis expected to counter a certain pathology. (p. 526).
The new paradigm was promoted as simultaneously a scien-tific and technological revolution, expected to yield an entirely newparadigm for discovery of new, and more effective, medicines. Asexpressed by William Haseltine, the Nobel-prize winning founderof an early genomics firm Human Genome Science: “Death is aseries of preventable diseases” (Fisher, 1999). Below are two exam-ples of the framing of the genetics paradigm as a rational approach,using advanced computational methods. The first is excerpted froma textbook on drug development (Ng, 2004), the second from a newsarticle describing a genomics-based start-up:
“The approach to drug discovery and development can generallybe classified into the following areas:
Irrational approachRational Approach
Irrational approach: This approach is the historical method ofdiscovering and developing drugs. It involves empirical obser-vations of the pharmacological effects from screening of manycompounds, mainly those from natural products. The activecomponent that gives rise to the observed effects is isolated. Thechemical formula is determined, and modifications are made toimprove its properties. This approach has yielded most drugsavailable today.
Rational Approach: This approach requires three-dimensionalknowledge of the target structure involved in the disease. Drugsare designed to interact with this target structure to create abeneficial response. This is an emerging field in drug discovery.”
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
(Ng, 2004)
“Incyte is based in Palo Alto, Calif., deep in Silicon Valley, andit is no coincidence that the heart of its headquarters is a vast,
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
ARTICLE IN PRESSG ModelRESPOL-3232; No. of Pages 16
M. Gittelman / Research Policy xxx (2016) xxx–xxx 11
Target iden� fica�on: In vit ro analy sis of cli nica l samp les an d genomic data to iden�fy gene�cally expressed targets in cells
Key inves�gato rs/ ins�tu�on s: Ge ne�cis ts, mol ecular biologists; biost a�s�cians; universi�es; biotec h and pharma firms
Assays Combinatorial chemistry
High throughput screening
Target valida�on - demonstrate link between target and intra-cellular eventsassociated with pathology
Key inves�gators/ins�tu�ons: Gene�cists, molecular biologists; biosta�s�cians; univers i�e s; biotech and pharma firm s
Lead discovery – iden�fica�on of compound-target pairs that se lec�vely exhibit func�onal (“bind ing”) re la�onships
Key inves�gator/ins�tu�ons: Molecular biologists; molecular/medicinal chemists; biosta�s�cians; biotech an d pharma firms
Structure-based drug design to generate possible “hits” to target
Lead op�miza �on – in vit ro tes�ng an d Struc ture-Ac �vity- Rela�onsh ip (SAR) studies to op �miz e “d rug li ke” proper �es of the lead
Key inve s�gators/ins�t u�on s: Mo lec ular biologists; molecular/medicinal chemists; pharmacologists; biosta�s�cians; biotech and
pharma firms
In vivo tes�ng in animal s – to confirm that in vitr o resu lts are expressed in vivo; pharma kokine�c pro filing; toxicity screen s
Key in ves�gators/ins�tu�o ns: Mol ecul ar biolo gists; st ructural/me dicin al chem ists; pharm acolo gists; biosta�s�cians; biotech and pharma firms
Entry in to cli nical trialsBiot ech and pharma firm s, co ntract research organi za�ons,
hospitals
Fig. 4. Drug discovery: the
Fig. 5. Publications in the journal of clinical investigation, 1969–1999.
genomics paradigm.
glass-enclosed room full of powerful computers. “At the endof the day, it’s the information that matters,” said Randy Scott,the president and chief scientific officer. “We are all about theapplication of Moore’s Law to biology,” he said – a reference tothe observation that computer processing power doubles every18 months. Applying that exponential growth to genomics shouldproduce similar gains for drug discovery, Dr. Scott said.” (Fisher,Wall Street Journal, 1999; italics added)
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
A number of institutional changes were made to help bringthe genetics paradigm to the forefront of bio-medical research.7 Inthe early 1980s, changes to federal patent laws legal both allowed
7 The early institutional and organizational history of the biotechnology industryhas been well documented in numerous papers and books, e.g. Kenney (1986).
did not emerge from the target-based approach shown in Fig. 4, andtheir clinical success can be traced to solving complex optimizationproblems.8
ARTICLEESPOL-3232; No. of Pages 16
2 M. Gittelman / Researc
or patenting of biological inventions and strengthened intellec-ual property rights; these were instrumental in the formation ofew companies in biotechnology. Strengthened intellectual prop-rty rights on genomic information created opportunities for entryy new firms into drug discovery with the aim of developingarly-stage research findings. Drug companies, whose discoverynd development functions were organized around traditional ana-ytical and synthetic chemistry techniques, were ill-equipped tongage in in-house development programs based on the new bio-ogical approaches.
The 1980s and 1990s were a period in which thousands ofntrepreneurial firms were founded to commercialize the new sci-ntific breakthroughs. Many founders were prominent scientistst the forefront of the genetics reolution in biology (Zucker andarby, 2002). The location of early scientific discoveries in the Sanranscisco Bay area was significant. Recombinant DNA was dis-overed at the University of San Francisco in the mid-1970s. Theegion had a history of active university technology transfer andpin-offs, and during the 1980s had witnessed a period of the flour-shing of start-ups in technology sector. The region thus embodied
culture and institutional orientation to the entrepreneurial start-p model, which was adapted by venture capitalists to the newusiness of biotechnology (Kenney, 1986). The “Silicon Valley”odel of entrepreneurship became a hallmark of the biotechnol-
gy revolution in the United States (Gittelman, 2006). Academicntrepreneurship was a defining characteristic of the new tech-ological possibilities, and many new firms were clustered nearbyhe university labs of their founders which was outside the geo-raphic footprint of the established pharmaceutical industry. “Bigharma” was perceived as overly bureaucratic and lacking innova-ive capacity as compared to the new start-ups. The latters’ focusn upstream discovery, coupled with stronger intellectual prop-rty rights, allowed them to broker knowledge between universityesearch and pharmaceutical firms (Gittelman, 2006, Stuart et al,007). The latter, in turn, adapted to the change by investing inew screening technologies and licensing targets and other proofsf concepts from small firms for downstream development andesting (Arora and Gambardella, 1991).
The Human Genome Project was an important policy mile-tone in the linking of genetic science to medical discovery. It wasaunched in the mid-1980s and created a global network of sci-ntific teams working to sequence the human genome; Congresspproved spending of $3 billion for the project. The justification forhis expensive investment (for what had recently been a relativelynderfunded basic science) was that the understanding of the mostasic elements of life would lead to enormous social gains in theorm of new drugs. In 2000 Francis X Collins, who led the Humanenome Project in the United States, declared that “Over the longer
erm, perhaps in another 15 or 20 years, you will see a completeransformation in therapeutic medicine.” (Wade, 2010).
Reflecting this belief, the genetics-based approach to drugiscovery found expression in firms founded by leading geneticists
n the 1990s: Human Genome Sciences, Celera, Incyte, Mille-ium, Myriad and DeCode possessed advanced capabilities toequence genetic information and deep reservoirs of patentedene sequences as their primary resource. At the core of theirusiness model was the promise of downstream rights to theew drugs that were expected to be developed based on theenetic information they were producing and patenting. The980s and 1990s thus witnessed a period of significant organiza-ional change, characterized by dense collaborations and marketsor technology, a deepening division of labor between small
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
iotechnology focused on transforming university research intoarly-stage proofs-of-concept for drug discovery (e.g., targets andeads), and large pharmaceutical firms who opened their doorso collaboration with these firms to develop their discoveries
PRESScy xxx (2016) xxx–xxx
into commercial drugs. Indeed, pharmaceutical firms became lessvertically integrated than in prior periods, and outsourced morefunctions, some to overseas locations, including research as wellas clinical trials and medicinal and analytical chemistry (Thierset al., 2008). The role of large pharmaceutical firms increasinglybecame one of coordinating complex collaborative network withless emphasis on in-house, proprietary R&D. (Rafols et al., 2014).
6. The revolution revisited: evidence of the relativeperformance of search paradigms and medical discovery
While the science of genetics has flourished, it is now widelyacknowledged in the scientific community that the target-basedapproach did not deliver on its early promise (Hamilton, 2004;Hopkins et al., 2007; Wade, 2010). The models of single targetsproviding a “magic bullet” to finding effective drugs has given wayto an understanding that the problem of linking genetic informa-tion to pathology in whole organisms is much more complex; itis now believed that most diseases are triggered by multiple tar-gets operating in unknown (and possible unpredictable) sequences,and that the identification of a single target through a genetic assayfails to capture these events (Sams-Dodd, 2005). As such, the earlytarget-based approach to drug discovery is now perceived as beinginsufficient to tackle the full complexity of disease.
The limitations of the target-based model as a useful guide fortechnological discovery is illustrated by the example of leptin. Inthe 1990s scientific experiments with genetically engineered micedemonstrated that leptin was implicated in appetite regulation.When a correlation was found between the genetic expression ofleptin and obesity in mice, the prediction that “deficits in leptincause obesity” was important to Amgen’s decision to invest in lep-tin to search for an obesity drug (Goozner, 2004). However, twomore decades of research revealed that a host of other complexfactors were important in appetite regulation and that leptin wasonly one of several complex triggers; the leptin-based drug wasnot effective. In this case, the initial finding was useful in guidingsubsequent scientific research; however, the full complexity of theproblem defied the utility of the simple predictive model for findinga technological solution to the problem.
Indeed, the primacy of the early target-based models has beenchallenged by cases where treatments have failed to emerge foreven single-gene diseases, such as Huntington’s disease and cys-tic fibrosis, for which the genetic mechanisms have been wellunderstood for a long period of time. For more complex diseases,and those with significant environmental triggers, the genome-phenome link remains elusive: in a recent study at Brigham andWomen’s Hospital, 101 genetic markers that have been statisticallylinked to heart disease were shown to have no value in forecastingdisease among 19,000 subjects followed for 12 years; a more validpredictor was the old-fashioned method of a family history (Wade,2010).
There are few available metrics by which to compare andevaluate the contribution of different search paradigms to theproductivity of discovery. That the new wave of protein-based bio-logics has not emerged, as initially promised, can be traced to theexaggerated promises that were made in the early days of therevolution. An exception are several highly successful monoclonalantibodies, including Herceptin and Rituxan. However, these drugs
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
8 Instead of starting from a theory of structure-action and working forward todiscover a drug, development of MaBs involves identification of known antigensand designing molecules to bind to them to neutralize their activity. These drugs,
There is evidence that shows that while new analytical tech-iques allow for the launch of many more drug candidates intohe testing pipeline, they have not yielded more approved drugs.cannell et al. (2012) propose that, contrary to initial expectations,he ability to screen millions of compounds has proven to be annefficient way of selecting drugs that will be effective in humans,nd that feedback-based exploration by medicinal chemists is likelyo yield more hits, despite a much smaller search space. In recentears, there has been a shift in clinical trials from failure in earlytages to a period in which the majority of compounds fail inate stage trials, when most of the development expense has beenncurred (Hopkins et al., 2007; Kola and Landis, 2004; Wade, 2010).ola and Landis (2004) find that, across all disease areas, the majorause of attrition (40%) in 1991 was adverse pharmacokinetic andioavailability results, which generally occur in Phase 1 or test-
ng. By 2000, these factors accounted for less than 10% of attritionhich had shifted to failures due to toxicology (30%) and lack of
fficacy (30%), which occur in Phase II and III. Bains (2004) sim-larly finds very high rates of attrition occuring in late stages ofrials, and several biologically-derived drugs that were discoveredhrough target affinity were found to have little efficacy in humansLeFanu, 2012). The data on the increase in late-stage failure sug-ests that technological uncertainty has not declined but has shiftedo later stages, when significant development costs have been sunk.his shift corresponds to the fact that in the target-based approach,eedback a drug’s operation in humans arrives relatively late in theiscovery process. In this regard, naturally derived substances andompounds discovered through phenotypic screening are advan-aged, insofar as they have been optimized through evolution orave been tested in man early in the discovery process (Swinneynd Anthony, 2011).
A recent study by Swinney and Anthony (2011) provides evi-ence that the target-based approach drug discovery as shown inig. 4 has been less productive of innovative new drugs than thecreening methods described in Fig. 3. Of all 259 NME (New Molec-lar Entities) approved by the FDA over the period 1999–2008,early 50% of the approved phenotypically screened drugs (28)ere first in class, or innovative medications, while only 27′%
f the target-based drugs fell into that category; the remaining3% were follower (“me too”) drugs (and for only target-basedmall molecule drugs, 83% in the “follower” category).9 This evi-ence suggests that the complexity of most diseases defies theimple predictive model. Instead, phenotypic search techniques
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
hat provide closer analogs to disease states in their naturalomplexity appears to be more productive of innovative newrugs.
temming from the seminal Kohler Millstein discovery in the UK in the mid-1970s,tilize genetic technologies to develop drugs that to attack antigens with a very highegree of specificity. Their clinical success was unexpected: in the 1980s and 1990s,
t was widely believed that drugs based on recombinant protein technology wouldepresent the major therapeutic breakthroughs stemming from biotechnology, andhat mAbs were not likely to succeed as therapeutics. Skepticism was based onhe difficulty of producing mAbs that were nontoxic to humans. Breakthroughs inhe engineering and manufacturing of mAbs have rendered them safe for humans,nd mAbs are now by far the most important technology driving the biotechnologyherapeutic pipeline (Gittelman, 2007).
9 A more recent analysis (Eder et al., 2014) looks at similar data for 1999–2013,nd finds that 71% of all approved First In Class drugs were target based, an increasever the proportion in the earlier study. However, it is difficult to evaluate thisgure without knowing how many were approved overall, since during the period auch higher number of drugs were developed using target-based approaches than
henotypic (or chemocentric) approaches; without data on the proportions of theseroups in both First in Class it cannot be known the probability of phenotypic andarget-based drugs of falling into First in Class or Me Too drugs. In fact, both studiesnly report data are for approved drugs; without knowing how many were rejectede do know the unconditional probability of falling into the innovative and follower
roups.
PRESSy xxx (2016) xxx–xxx 13
A handful of studies provide evidence that the clinical paradigmremains important in medical innovation. An early, well-knownstudy by Comroe and Dripps (1976) analyzed the sources of majordiscoveries in pulmonary and cardiac medicine. Overall, they foundthat in 4 out of 10 subfields, over 75% of articles were clinically ori-ented. They also found that 62% of articles involved “basic” research,defined as research that was directly concerned with identifyinga causal mechanism. A follow-on study of major advances in neo-natal care (Grant et al., 2003) identified the most highly cited paperscontributing to the field over 17 years, and found that in all sub-fields over 80% were clinically oriented; interestingly, between 26and 55% of the research was conducted in hospitals.
The role of medically trained researchers and downstreamdevelopment as a source of new, unexpected uses has been high-lighted in recent research. In a study of inventions at leadingAcademic Medical Centers, we found evidence that even whenMDs and PhDs collaborated on inventions, those that were com-posed of MDs or had MDs as team leaders were more likely tobe licensed than teams led by PhD researchers (Ali and Gittelman,2016). Gelijns et al. (1998) find that nearly all the blockbuster drugsapproved in 1993 had secondary, unexpected uses, and that salesfrom these unexpected uses amounted to 40% of total sales. Muchof these discoveries are made by practicing doctors: a 2006 studyexamined the sources of discovery of new off-label uses for drugs,and found that 59% of innovations came from clinicians practic-ing in the field rather than from universities and drug companies(DeMonaco et al., 2006). Higgins et al (2014) analyzed a set of 342university discoveries licensed to biotechnology firms, and foundthat nearly one third were subsequently re-licensed to other firms;of those, 81% showed a change in the original indication. The resultsunderscore the uncertain nature of early predictive models in drugdiscovery.
7. Discussion: the challenge of translation
The declining rate of discovery of new medicines is a centralconcern in current medical policy debates. Policy makers haveattributed the problem to failure in markets for ideas, and haveembraced the concept of translation as a central tool in address-ing the productivity paradox. The NIH defines the problem oftranslation as “taking basic discoveries about the causes of a dis-ease and transforming this knowledge into a new treatment anddemonstrating that it tangibly improves human health”.10 In thisperspective, advances from scientific research (the bench) are fail-ing to be translated to practical applications. Reflecting this view,The President’s Scientific Advisory Committee wrote in its 2012report to the President:
“While biomedical research has experienced a golden ageof progress over the past 25 years, there has been growingconcern about the pace of translating scientific insight intopublic health impact. The many remarkable advances in basicbiomedical research over the past quarter-century have not yetled to significant increase in the flow of new medicines to theAmerican public” (President’s Council on Science and Technol-ogy, 2012, p. vi)
In this perspective, the problem stems from institutional andmarket failures that impose frictions on the translation of advances
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
made at the bench to the bedside. The current Director of the NIH,Francis Collins – the geneticist who led the Human Genome Project– frames the issue as follows:
in what is increasingly a team-driven enterprise. While scientificteams helps bring varied specialized resources to a project, a divi-sion of labor among specialists might also overburden research in
ARTICLEESPOL-3232; No. of Pages 16
4 M. Gittelman / Researc
“We have seen a deluge of new discoveries in the last few yearson the molecular basis of disease. That’s the good news. Butthere is bad news too. Despite increasing investments by theprivate sector, there has been a downturn in the number ofapproved new molecular entities over the last few years. Also,drug development research remains very expensive and the fail-ure rate is extremely high. . . pharmaceutical companies havecut back their investments in research and development. Wecan’t count on the biotech community to step in and fill that voideither, because they are hurting from an absence of long-termventure capital support. So, we have this paradox: we have agreat opportunity to develop truly new therapeutic approaches,but are undergoing a real constriction of the pipeline. One solu-tion is to come up with a non-traditional way of fostering drugdevelopment — through increased NIH involvement.” (Mullard,2011)
Recent institutional and policy has been motivated by this modelf translational, “gap filling” research. In 2005 the NIH issued itsoadmap for the future, with stronger integration of basic and clin-
cal sciences at its core; in 2011, it founded the National Center fordvancing Translational Sciences (NCATS) – the first new Center at
he NIH in many decades – to implement this vision (Collins, 2011).he institute is specifically involved in validating leads discoveredy academia to be translated to the private sector. The NIH haslso stressed the importance of teams and collaborative researchn medical research, reflecting the increasing specialization andnter-disciplinary nature of the field (Collins, 2010). Several Euro-ean policy initiatives similarly seek to foster integration of basiccience to clinical applications through translational research.
Many writers in the medical policy literature have criticizedhe translational model as flawed (LeFanu, 2012; Gelijns andosenberg, 1994; Mitra, 2009; Rees, 2004; Scannell et al., 2012;illiams, 2004). First, it adheres to a linear model of bench-to-
edside learning, with genetic science providing initial discoverieshat are refined by the clinical sciences and can flow into theipelines of the pharmaceutical industry. The discussion herend elsewhere (e.g. Gelijns and Rosenberg, 1994) underscores themportance of clinical data and phenotyping screening as a startingoint in discovery, as well as the importance of close interactionsetween academic clinicians and medicinal chemists early in theiscovery phase.
The diagnosis of a gap in the research landscape between “basiccience” and “the market” is problematic insofar as entrepreneurialiotechnology firms were expected to fill a gap between upstream,niversity inventions and the pharmaceutical industry, and spe-ialized in the role of translating early stage discoveries toractical, downstream applications (Arora and Gambardella, 1991;ittelman and Kogut, 2003; Kenney, 1986; Zucker et al., 2002).hese firms were founded by highly trained university scientistsho were positioned to broker between patented university dis-
overies and the pharmaceutical industry (Gittelman, 2006; Stuartt al., 2007). If the biotech industry, which received billions of dol-ars of private sector investment and was specialized in the role ofranslation, has failed to “fill the gap” in the market for ideas, thenhere is reason to suppose that government may not succeed at thisask, and indeed to suspect that the diagnosis of an unfilled “gap”s itself incorrect.
A further problem with the translational model is that it pre-umes that integrating different types of knowledge will help speediffusion and application; the emphasis on inter-disciplinary teamseflects this orientation. While integrating specialized knowledge
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
s important, it is also important to understand that teams are noterely combinations of the diverse skills and knowledge of theirembers; they are collections of individuals who may adhere to
ifferent research paradigms that shape their beliefs about how the
PRESScy xxx (2016) xxx–xxx
discovery process should unfold. As discussed in this paper, clini-cal and basic research represent distinct research paradigms thatembody fundamentally different epistemic cultures of research.Indeed, beliefs about the very nature of medical discovery are dif-ferent, and sometimes conflicting, in the logics of the basic andclinical research paradigms. In related research (Ali and Gittelman,2016) we show that inventions by teams of scientists at AcademicMedical Centers are more likely to be licensed to firms when theyare led by clinicians, over and above the composition of the team;we propose that this finding provides evidence for the effect of theclinical research paradigm on translation. The finding suggests thatthe problem of translation is much more complex than a simplearithmetic of combining diverse specializations within and acrossorganizations or teams; it involves understanding, integrating andtranscending differences that embody distinct professional identi-ties, epistemic cultures, and norms and practices of search.
Although this paper does not focus on drug discovery insidefirms, I attempt to show that as new paradigms emerge in the sci-entific landscape, the menu of research options available to firmschanges in ways that might impact their own productivity. Morespecifically, firms rely on external knowledge to help guide theirsearch, and the subfields they select for collaboration matter. Aca-demic science is particularly useful in guiding industrial search bygenerating well-supported hypotheses about promising avenuesof inquiry, improving the efficiency and lowering the cost of R&D(Nelson, 1982; Vos, 1991). In medicine, pharmaceutical firms lookto academic science to hypothesize pathways and mechanisms thatpoint in certain directions as promising avenues of discovery. Theproduction of validated hypotheses is thus a key role of academicscience in the discovery process; and these are sensitive to thetraining and research paradigms of collaborating scientists.
While many in the medical community decry the decline ofthe “golden age” of clinical research, they readily acknowledgethat the paradigm as it once existed cannot, nor should be, re-created. However, the history is instructive in terms of providinginsights for the future. Several points suggest themselves as impor-tant in this regard. First, clinical data plays a critical role in the earlystages of a drug discovery project, in terms of generating insightsinto innovative treatments, efficacy and safety. There are currentlyuntapped stores of clinical data (for instance from unpublishedclinical trials and abandoned projects) that are not made availableto the research community; making this data compulsorily avail-able would help accelerate discovery of promising new drugs.11
Drug companies would also collectively benefit from opening theirsubstantial vaults of clinical data to the research community. Theevidence strongly suggests that the thousands of compounds thathave failed in clinical trials would be fruitful platforms for newdiscovery projects.
The role of the clinical investigator in the innovation landscaperequires renewed institutional support. Current efforts to foster asystems biology approach in medical research represents a recogni-tion of the central importance of studying complex phenomena asthey exist in nature, and trained clinicians play a central role in thatendeavor. (LeFanu, 2012). Renewed institutional support for clini-cal research in hospitals remains important. This likely entails theisolation of budgeting-oriented missions from medical research inAcademic Medical Centers. It also entails a recognition of the impor-tant role of “curiousity-driven science” and individual investigators
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
11 The initiative to publish clinical trials data on clinicaltrials.gov is a step in thisdirection, though the requirements are non-binding.
way as to drown out the spark of creativity of the individualnvestigator working closely with patients in experimental settings.
Lastly, industry plays an important role in spurring renewedlinical research in drug discovery. The early close collabora-ions between academic clinicians and large pharmaceutical firmsas weakened and shifted toward a sponsorship relationship; re-reating collaborative relationships in which clinicians provide keyntellectual guidance and creative inputs for early-stage drug dis-overy would yield both support for clinical research as well asseful ideas for pipeline development.
This paper suggests that the productivity paradox in drug dis-overy is not really a paradox. The discussion presented in thisaper suggests that the biotechnology revolution was bound to fail,iven the limits of predictive science to solve problems in complexatural phenomena, as well as the hype that surrounded it in thearly decades. The history documents a period in which Federalolicy expressly supported experiential research that proved diffi-ult to maintain over time. The institutional conditions that gaveise to the clinical paradigm cannot be replicated. In hindsight, thexperience of genetics in medical research has demonstrated that
moving frontier in scientific knowledge does not translate to aorresponding advance in technological innovation. The broaderesson from the history is that basic science and technological inno-ation are distinct sets of practices, and while each may benefitrom advances in the other, they evolve independently. Medicalesearch closely utilizes scientific knowledge but requires institu-ional and organizational arrangements that support, rather thanonflict with, its own distinct logic of discovery.
cknowledgements
The author would like to thank Magnus Galbrundson and theditors of the Special Issue as well as three anonymous reviewersor providing excellent feedback throughout the review process.he paper benefited from useful discussions with numerous indi-iduals, including Ayfer Ali, Linda Asher, Iain Cockburn, Deborahougherty, Annetine Gelijns, Martin Kenney, Dan Levinthal, Don-ld F. Klein, Christopher Molloy, Richard R. Nelson, Bhaven Sampat,aniel Sarewitz, Alan Schechter, Judith Rapoport, and Finn Valetin,s well as seminar participants at Bocconi University, Drexel Uni-ersity, National Institutes of Health, University of Connecticut,openhagen Business School, Georgia Tech, and the Lerner Center
or Pharmaceutical Research at Rutgers Business School.
eferences
hrens, E., 1992. The Crisis in Clinical Research. Oxford University Press, Oxford.li, A., Gittelman, M., 2016. Research Paradigms and Useful Inventions in
Medicine: Patents and licensing by clinical and basic scientists in AcademicMedical Centers.
ngell, M., 2000. Is academic medicine for sale? N. Engl. J. Med. 342, 1516–1518.rora, A., Gambardella, A., 1990. Complementarity and external linkages: the
strategies of the large firm in biotechnology. J. Ind. Econ. 38 (4), 361–379.rora, A., Gambardella, A., 1994. The changing technology of technological change:
general and abstract knowledge and the division of innovative labour. Res.Policy 23, 523–532.
ains, W., 2004. Failure rates in drug discovery and development: will we ever getany better? Drug Discov. World (Fall).
loom, F., 2003. Science as a way of life: perplexities of a physician-scientist.Science 300 (June), 1680–1682.
ryan, C.M., Stinson, S., 2002. The choice: Lewellys F. Barker and the full-time plan.Ann. Intern. Med. 137 (6), 521–525.
ampbell, W., 2005. Serendipity and new drugs for infectious disease’. ILAR J. 46(4), 352–356.
arlsson, A., 2003. Questions and answers following the talks of Paul Greengardand Arvid Carlsson. CINP Newsl. (March).
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
hung, K., 2007. Revitalizing the training of clinical scientists in surgery. Plast.Reconstr. Surg. 120 (7), 2066–2072.
ockburn, I., 2006. Is the pharmaceutical industry in a productivity crisis? In:Innovation Policy and the Economy. NBER, Cambridge.
ollins, F.X., 2010. Opportunities for research and NIH. Science, 327.
PRESSy xxx (2016) xxx–xxx 15
Collins, F.X., 2011. Reengineering translational science: the time is right. Sci.Transl. Med. 3, 90.
Comroe, J., Dripps, R., 1976. The scientific basis for the support of biomedicalscience. Science 192, 105–111.
DeMonaco, H., Ali, A., von Hippel, E., 2006. The major role of clinicians in thediscovery of off-label drug therapies. Pharmacotherapy 26 (3),323–332.
Dougherty, D., Dunne, D., 2012. Digital science and knowledge boundaries incomplex innovations. Org. Sci. 23 (5), 1467–1484.
Eder, J., Sedrani, R., Wiesmann, C., 2014. The discovery of first-in-class drugs:origins and evolution. Nat. Drug Discov. 13, 577–587.
Fisher, L., 1999. The race to cash in on the genetic code. New York Times, August 29.Fleming, L., Sorenson, O., 2004. Science as a map in technological search. Strateg.
Manag. J. 25, 909–928.Gavetti, G., Levinthal, D., 2000. Looking forward and looking back: cognitive and
experiential search. Adm. Sci. Q. 45, 113–137.Gelijns, A., Rosenberg, N., 1994. The dynamics of technological change in medicine.
Health Aff. (Millwood) 13, 28–46.Gelijns, A., Rosenberg, N., Moskowitz, A., 1998. Capturing the unexpected benefits
of medical research. N. Engl. J. Med. 339 (10), 693–698.Gelijns, A.C., Zivin, J.G., Nelson, R.R., 2001. Uncertainty and technological change in
medicine. J. Health Polit. Policy Law 26 (5), 913–924.Gittelman, M., 2006. National institutions, public-private knowledge flows, and
innovation performance: a comparative study of the biotechnology industry inthe United States and France. Res. Policy 35 (7), 1052–1068.
Gittelman, M., 2007. Analytical Report on the Uptake and Diffusion ofHealth-Related Biotechnologies OECD Working Group on BiotechnologyReport, DSTI/ISP/BIO(2006)/50.
Gittelman, M., Kogut, B., 2003. Does good science lead to valuable knowledge?Biotechnology firms and the evolutionary logic of citation patterns. Manag. Sci.49 (4), 366–382.
Goozner, M., 2004. The $800 Million Pill: The Trust Behind the Cost of New Drugs.University of California Press, Berkeley.
Grant, J., Green, L., Mason, B., 2003. From Bedside to Bench: Comroe and DrippsRevisited. GERG Research Report Number 30 (August). Brunel University,Middlesex, UK.
Hamilton, D., 2004. Dose of reality – biotech’s dismal bottom line: more than $40billion in losses. Wall Street J., May 20.
Henderson, R., Pisano, G., Orsenigo, L., 1999. The pharmaceutical industry and therevolution in molecular biology: interactions among scientific, institutional,and organizational change. In: Mowery, D., Nelson, R. (Eds.), Sources ofIndustrial Leadership: Studies of Seven Industries. Cambridge University Press,Cambridge.
Higgins, M., Thursby, M., Thursby, J., 2014. Bench-to-bench bottlenecks intranslation. Sci. Transl. Med. 6 (250).
Hollingsworth, R., Hollingsworth, E.J., 2006. Major Discoveries and BiomedicalResearch Organizations: Perspectives on Interdisciplinarity. NurturingLeadership, and Integrated Structure and Cultures Workingpaper.
Hopkins, M., Martin, P., Nightingale, P., Kraft, A., Mahdi, S., 2007. The myth of thebiotech revolution: an assessment of technological, clinical, and organizationalchange. Res. Policy 36, 566–589.
Institute of Medicine, 2004. Careers in Clinical Medicine. IOM, New York.Jack, A., 2011. Drugs: supply running low. Financial Times of London, February 9.Kenney, M., 1986. Biotechnology: The University-Industrial Complex. Yale
University Press, New Haven.Kola, I., Landis, J., 2004. Can the pharmaceutical industry reduce attrition rates?
Nat. Drug Discov. 3 (August).Lederberg, J., 1994. The transformation of genetics by DNA: an anniverary
celebration of Avery, MacLeod and McCarty. Nat. Genet. 136, 423–426.LeFanu, J., 2012. The Rise and Fall of Modern Medicine. Basic Books, New York.Ley, T., Rosenberg, L., 2005. The physician-scientist career pipeline in 2005. J. Am.
Med. Assoc. 294, 1343–1351.Lombardino, J.G., Lowe, J.A., 2004. The role of the medicinal chemist in drug
discovery – then and now. Nat. Rev. Drug Discov. 2, 853–862.Luft, F., 1997. The role of the general clinical research center in promoting
patient-oriented research into the mechanisms of disease. J. Mol. Med. 75,345–350.
Merton, R., Barber, E., 2004. The Travels and Adventures of Serendipity. PrincetonUniversity Press.
Mitra, I., 2009. Why is modern medicine stuck in a rut? Perspect. Biol. Med. 52,500–517.
Mullard, A., 2011. An interview with Francis Collins. Nat. Rev. Drug Discov. 10, 14.Nathan, D., Schechter, A., 2006. NIH support for basic and clinical research. J. Am.
Med. Assoc. 295, 2656–2658.Nathan, David, 2002. Careers in translational clinical research – historical
perspectives, future challenges. J. Am. Med. Assoc. 287, 2424–2427.National Institutes of Health, Office of the Budget, 2015. NIH Research Portfolio
Online Reporting Tools, http://report.nih.gov/frrs/index.aspx.Nelson, R.R., 1982. The role of knowledge in R&D efficiency. Q. J. Econ. 97 (3),
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
453–470.Nelson, R.R., 2003. On the uneven evolution of human know-how. Res. Policy 32,
909–922.Rosenberg, N., Nelson, R.R., 1994. American universities and technical advance in
ightingale, P., 1998. A cognitive model of innovation. Res. Policy 27,689–709.
ightingale, P., 2004. Technological capabilities, invisible infrastructure, and theunsocial construction of predictability: the overlooked fixed cost of usefulresearch. Res. Policy 33, 1259–1284.
g, R., 2004. Drugs: From Discovery to Approval. John Wiley, New Jersey.avitt, K., 1998. The social shaping of the national science base. Res. Policy 27,
793–805.012. Report to the President on Propelling Innovation in Drug Discovery,
Development, and Evaluation. President’s Council of Advisors on Science andTechnology, Washington, DC.
afols, I., Hopkin, M., Hoekman, J., Siegel, J., Perianes-Rodríguez, A., Nightingale, P.,2014. Big Pharma, little science? A bibliometric perspective on Big Pharma’sR&D decline. Technol. Forecast. Soc. 81, 22–38.
asmussen, N., 2002. Steroids in arms: science, government, industry and thehormones of the adrenal cortex in the United States: 1930–1950. Med. Hist. 46,299–324.ef.
ees, J., 2002a. Complex disease and the new clinical sciences. Science 295,698–701.
ees, J., 2002b. Two cultures? J. Am. Acad. Dermatol. 46, 313–316.ees, J., 2004. The fundamentals of clinical discovery. Perspect. Biol. Med. 47 (4),
597–607.obertson, D., Tung, C., 2001. Linking molecular and bedside research: designing a
clinical research infrastructure. J. Mol. Med. 79 (12), 686–694.osenberg, N., 2009. Some critical episodes in the progress of medical innovation:
Please cite this article in press as: Gittelman, M., The revolution re-visitparadox in drug discovery. Res. Policy (2016), http://dx.doi.org/10.101
an Anglo-American perspective. Res. Policy 38, 234–242.ams-Dodd, F., 2005. Target based drug discovery: is something wrong? Drug
Discov. Today 10 (January (2)).cannell, J., Blanckley, A., Boldon, H., Warrington, B., 2012. Diagnosing the decline
in pharmaceutical R&D efficiency. Nat. Rev. Drug Discov. 11 (March).
PRESScy xxx (2016) xxx–xxx
Schechter, A., 1998. The crisis in clinical research: Endangering the half-century.National Institutes of Health, Consensus, Commentary. J. Am. Med. Assoc. 280(16.).
Stokes, D., 1997. Pasteur’s Quadrant: Basic Science and Technological Innovation.Brookings Institute, Washington, DC.
Swazey, J., Fox, R., 2004. Remember the golden years of patient-oriented clinicalresearch. Perspect. Biol. Med. 47 (4.).
Swinney, D., Anthony, J., 2011. How were new medicines discovered? Nat. DrugRev. Discov. 10, 507–519.
Thiers, F., Sinskey, A., Berndt, E., 2008. Trends in the globalization of clinical trials.Nat. Rev. Drug Discov. 7, 13–14.
Thomke, S., von Hippel, E., Franke, R., 1998. Modes of experimentation: aninnovation process – and competitive – variable. Res. Policy 27, 315–332.
Vincenti, W., 1993. What Engineers Know and How they Know It. Johns HopkinsUniversity Press.
Vos, R., 1991. Drugs Looking for Diseases: Innovative Drug Research and theDevelopment of the Beta Blockers and the Calcium Antagonists. Developmentsin Cardiovascular Medicine, vol. 120. Springer.
Wade, N., 2010. A decade later, human gene maps few new cures. New York Times,June 12.
Williams, V., 2004. Pathways of innovation: a history of the first effectivetreatment for sickle cell anemia. Perspect. Biol. Med. 47 (4), 552–563.
ed: Clinical and genetics research paradigms and the productivity6/j.respol.2016.01.007
Wyngaarden, J.M., 1981. The clinical investigator as an endangered species. Bull. N.Y. Acad. Med. 57 (6), 415–426.
Zucker, L., Darby, M., Armstrong, J., 2002. Commercializing knowledge: universityscience, knowledge capture, and firm performance in biotechnology. Manag.Sci. 48 (1), 138–153.