on fetus during pregnancy Discuss physiological impact of alcohol on fetus Describe clinical manifestations of FASD at birth Discuss diagnostic evaluation of the neonate Discuss therapeutic approach and treatment
options Define economic, emotional and social
implications of FASD
Introduction
Approximately 12% of women in the United States and over 20% worldwide drink alcohol during pregnancy.
Many women are not aware they are pregnant until 4-6 weeks into pregnancy; consequently those women have been drinking alcohol during the critical time of development in the first trimester.
As a result fetus may experience detrimental effects of alcohol.
(Balachova et al., 2013)
Fetal Alcohol Spectrum Disorders (FASD)
Consumption of alcohol during any gestation of pregnancy = alcohol fetal consumption; consequently, it causes detrimental physical & neurological defects, which can be lead to any one of the array of disorders which are described as Fetal Alcohol Spectrum Disorders [FASD].
Alcohol easily crosses placenta and reaches fetus.
Amniotic fluid acts as a reservoir for alcohol, prolonging fetal exposure.
Ethanol and its metabolite, acetyldehydrate (the placenta deoxidizes ethanol to this substance) alters fetal development by:
(Blackburn, 2013) (Vaux, 2012)
Pathophysiology
1) disrupting cellular differentiation & growth
2) disrupting DNA & protein synthesis
3) inhibiting cell migration due to the fact it reaches 50% of maternal levels
4) modifies the metabolism of carbohydrates, proteins, & fats
(Blackburn, 2013) (Vaux, 2012)
Pathophysiology
5) interferes and decreases the transfer of amino acids, glucose, folic acid, zinc & other nutrients across placental barrier disrupting fetal growth due to intrauterine nutrient deprivation
6) interferes with the incorporation of amino acids into proteins
this may limit the number of fetal cells and lead to fetal growth restriction
8) decreased placental transfer of linoleic & docosahexanoic acid may also alter fetal growth & development
(Blackburn, 2013) (Vaux, 2012)
Physiological Impact
Physiological impact on fetus development depends on the time of gestation & amount of alcohol consumption
Heavy drinking (four or more drinks in a day at least occasionally) throughout pregnancy can cause major structural defects to the fetus.
These include defects in several major organ systems, growth retardation, and brain abnormalities. However, different systems are more vulnerable at different times. (Sadler & Langman, 2012)
(Paoletti et al., 2013)
Physiological Impact
Alcohol related birth defects
(NOFAS, n.d.)
Clinical Manifestations of FASD at birth and up to 36 hours post birth
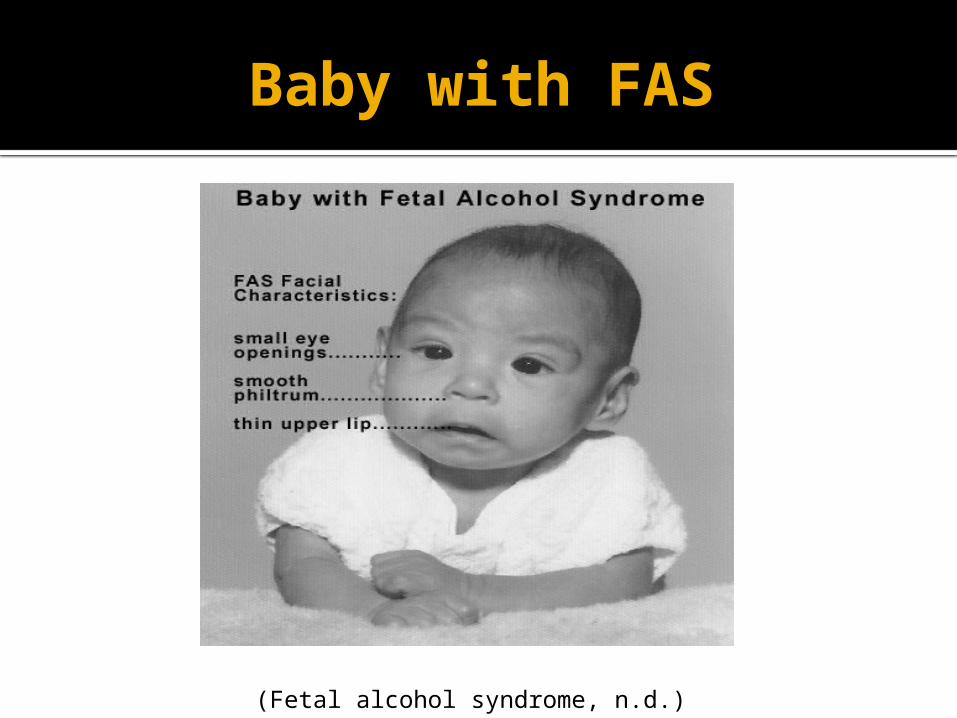
Upon birth there are distinct set of facial anomalies seen when a fetus is exposed to
alcohol in utero.
(NOFAS, n.d.) (Vaux, 2012)
Baby with FAS
(Fetal alcohol syndrome, n.d.)
Clinical Manifestations continued
The infant may also have decreased muscle tone, poor coordination and heart defects such as ventricular septal defect (VSD) or atrial septal defect (ASD).
Central nervous symptoms seen within 24 hours after delivery are tremors, irritability, twitching, hyperacusis(decreased tolerance to noise), hyperventilation, hypertonicity, opisthotonos, and seizures.
(Gomella et al., 2013)
Diagnostic Evaluation
When a diagnosis of FASD is considered, there are three major factors that must be addressed in the individual:
(1) physical growth, development, and structural defects (for example, dysmorphology)
(2) cognitive and neurobehavioral function; and
(3) maternal exposure and risk (Douzgou et al., 2012)(May & Gossage, 2011)
Diagnostic Evaluation continued
In 1996, the Institute of Medicine published specific diagnostic criteria for FAS with confirmed maternal alcohol exposure, FAS without confirmed maternal alcohol exposure, partial FAS with confirmed alcohol exposure, alcohol related birth defects (ARBD), and alcohol-related neurodevelopmental disorders [ARND]. (Douzgou et al., 2012)
Diagnostic Classification of Fetal Alcohol Syndrome (FAS) and Alcohol-Related Effects
(CDC, 2011)
Diagnostic Evaluation continued…
(Martin et al., 2011)
A new test capable of detecting fetal fatty acid ethyl esters in the meconium of newborns of heavy alcohol users may be useful for identification of infants in need of early health, developmental and psychosocial intervention and may enhance clinical research involving prenatal drug and alcohol exposure .
There is no cure for FASD. Main focus of treatment is ultimately
prevention, education & early intervention. Abstinence from alcohol preconceptually
and during pregnancy. Guidelines for screening and management
of FASD include universal screening of pregnant women for alcohol use, so that appropriate management can be provided.
Treatment Options
(Martin et al., 2011)
Treatment options
It is imperative to identify possible diagnosis of one of the FASD because early intervention is associated with better outcomes.
Prompt referrals and enrollment in indicated services are required to achieve best outcomes.
(CDC, 2011)(Schaefer & Deere, 2011)
Economic Implications of FASD
Due to possibility of wide array of disabilities, patients with FASD may have special needs that require lifelong help.
FASD costs $6 billion annually in the United States.
It costs $1.4 million to treat one person with FAS over their lifetime. (This estimates medical treatment, home and residential care, special educational services and productivity losses with patients with FASD of all ages . (NOFAS, n.d.)
(Popova et al., 2011)
Emotional/Social Implications of FASD
These children often come from unstable families and are at higher risk for physical, sexual abuse and neglect.
As many as 85% of children with FASD are raised by grandparents, other relatives, foster parents, or adoptive parents.
They are at increased risk for negative attachment & reactive attachment disorder.
(NOFAS, n.d.)
Emotional/Social Implications of FASD
The mother may feel guilty upon learning of infants diagnosis; counseling should be recommended to deal with life-long behavioral and learning problems the child will have.
This can be extremely stressful and overwhelming for the family.
These children may require a range of specialized medical, social , educational, and legal services.(NOFAS, n.d.)
Conclusion
Worldwide rate of FAS has been estimated to be 1.9 per 1,000 in the United States.
Alcohol is now recognized as the leading of preventable cause of birth defects and developmental disorders in the United States.
The national Organization of Fetal Alcohol Syndrome best sums up the relationship of alcohol and pregnancy by stating, ““Alcohol and Pregnancy. No safe amount. No safe time. No safe alcohol. Period.” (Belachova et al.,
2013) (NOFAS, n.d.)
References
Balachova, T., Bonner, B. L., Chaffin, M., Isurina, G., Shapkaitz, V., Tsvetkova, L., ... & Knowlton, N. (2013). Brief FASD prevention intervention: physicians’ skills demonstrated in a clinical trial in Russia. Addiction science & clinical practice, 8(1), 1-10.
Blackburn, S. T. (2013). Pharmacology and pharmacokinetics during the perinatal period. Maternal, fetal, & neonatal physiology: a clinical perspective (4th ed., pp. 183-213). Maryland Heights, MO: Elsevier Saunders.
Brocardo, P. S., Gil-Mohapel, J., & Christie, B. R. (2011). The role of oxidative stress in fetal alcohol spectrum disorders. Brain research reviews, 67(1), 209-225.
Centers for Disease Control and Prevention (CDC). (2011). Fetal alcohol spectrum disorders. Retrieved from http://www.cdc.gov/ncbddd/fasd/treatments.html
Douzgou, S., Breen, C., Crow, Y. J., Chandler, K., Metcalfe, K., Jones, E., ... & Clayton-Smith, J. (2012). Diagnosing fetal alcohol syndrome: new insights from newer genetic technologies. Archives of disease in childhood, 97(9), 812-817.
Fetal alcohol syndrome.(n.d.) Retrieved March 23, 2013 from the Wiki : http://en.wikipedia.org/wiki/Fetal_alcohol_syndrome
Floyd, R. L., Jack, B. W., Cefalo, R., Atrash, H., Mahoney, J., Herron, A., ... & Sokol, R. J. (2008). The clinical content of preconception care: alcohol, tobacco, and illicit drug exposures. American journal of obstetrics and gynecology, 199(6), S333-S339.
Gomella, T. L, Cunningham, M. D. & Eyal, F. G. (2013). Infant of a substance-abusing mother. Neonatology: Management, procedures, on-call problems, diseases and drugs (7th Ed., pp. 715-724). New York: McGraw Hill Education.
Jacobson, S. W., Jacobson, J. L., Stanton, M. E., Meintjes, E. M., & Molteno, C. D. (2011). Biobehavioral markers of adverse effect in fetal alcohol spectrum disorders. Neuropsychology review, 21(2), 148-166.
Martin, R. J., Fanaroff, A. A., & Walsh, M. C. (2011). Pharmacology. Fanaroff and Martin's neonatal-perinatal medicine: diseases of the fetus and infant (9th ed., pp. 708-757). Philadelphia: Saunders/Elsevier.
May, P. A., & Gossage, J. P. (2011). Maternal risk factors for fetal alcohol spectrum disorders: Not as simple as it might seem. Alcohol Research & Health, 34(1), 15.
Medina, A. E. (2011). Fetal alcohol spectrum disorders and abnormal neuronal plasticity. The Neuroscientist, 17(3), 274-287.
National Organization on Fetal Alcohol Syndrome (NOFAS). (n.d..). Fetal alcohol spectrum disorders. Retrieved from http://www.nofas.org
Paoletti, A. M., Atzeni, I., Orrù, M., Pilloni, M., Loddo, A., Zirone, M., ... & Melis, G. B. (2013). Alcohol and pregnancy. Journal of Pediatric and Neonatal Individualized Medicine (JPNIM), 2(2), e020215.
Popova, S., Stade, B., Bekmuradov, D., Lange, S., & Rehm, J. (2011). What do we know about the economic impact of fetal alcohol spectrum disorder? A systematic literature review. Alcohol and Alcoholism, 46(4), 490-497.
Riley, E. P., Infante, M. A., & Warren, K. R. (2011). Fetal alcohol spectrum disorders: an overview. Neuropsychology review, 21(2), 73-80.
Sadler, T. W., & Langman, J. (2012). Langman's medical embryology (12th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Schaefer, G. B., & Deere, D. (2011). Recognition, diagnosis and treatment of fetal alcohol syndrome. The Journal of the Arkansas Medical Society, 108(2), 38-40.
Vaux, K. K. (2012). Fetal Alcohol Syndrome . Medscape. Retrieved from http://emedicine .medscape.com/article/974016-overview
Warren, K. R., Hewitt, B. G., & Thomas, J. D. (2011). Fetal alcohol spectrum disorders: research challenges and opportunities. Alcohol research & health: the journal of the National Institute on Alcohol Abuse and Alcoholism, 34(1), 4.