31
HEMATOLOGY & ONCOLOGY FOCUSED COMPANY September 22, 2016
| Date post: | 15-Apr-2017 |
| Category: |
Investor Relations |
| Upload: | galenabio |
| View: | 4,369 times |
| Download: | 0 times |

HEMATOLOGY &
ONCOLOGY FOCUSED
COMPANY
September 22, 2016

FORWARD LOOKING STATEMENT
This presentation contains forward-looking statements within the meaning of the
Private Securities Litigation Reform Act of 1995. Such statements include, but are
not limited to, statements about future expectations, plans and prospects for the
development and commercialization of the Company's product candidates,
including patient enrollment in our clinical trials, present or future licensing,
collaborative or financing arrangements, expected outcomes with regulatory
agencies, and projected market opportunities for product candidates are subject
to a number of risks, uncertainties and assumptions, including those identified
under “Risk Factors” in the Company’s most recently filed Annual Report on Form
10-K and Quarterly Report on Form 10-Q and in other filings the
Company periodically makes with the SEC. Actual results may differ materially
from those contemplated by these forward-looking statements. The
Company does not undertake to update any of these forward-looking statements
to reflect a change in its views or events or circumstances that occur after the
date of this presentation.
2

TARGETING AREAS OF UNMET MEDICAL NEED
Hematology
GALE-401
• Proprietary controlled release
version of anagrelide
• Targeting 3rd Line Essential
Thrombocythemia (ET)
• Phase 3 initiation expected in
Q2, 2017
Plan to develop under 505(b)2
pathway
Immunotherapy
NeuVax™ (nelipepimut-S)
• Development in key settings
Combination with trastuzumab in HER2 1+/2+
Combination with trastuzumab in HER2 3+
DCIS
Gastric
GALE-301/GALE-302
• Targeted development in gynecological cancers
3
Diversified pipeline with multiple mid-to late stage clinical trials
focused in hematology-oncology
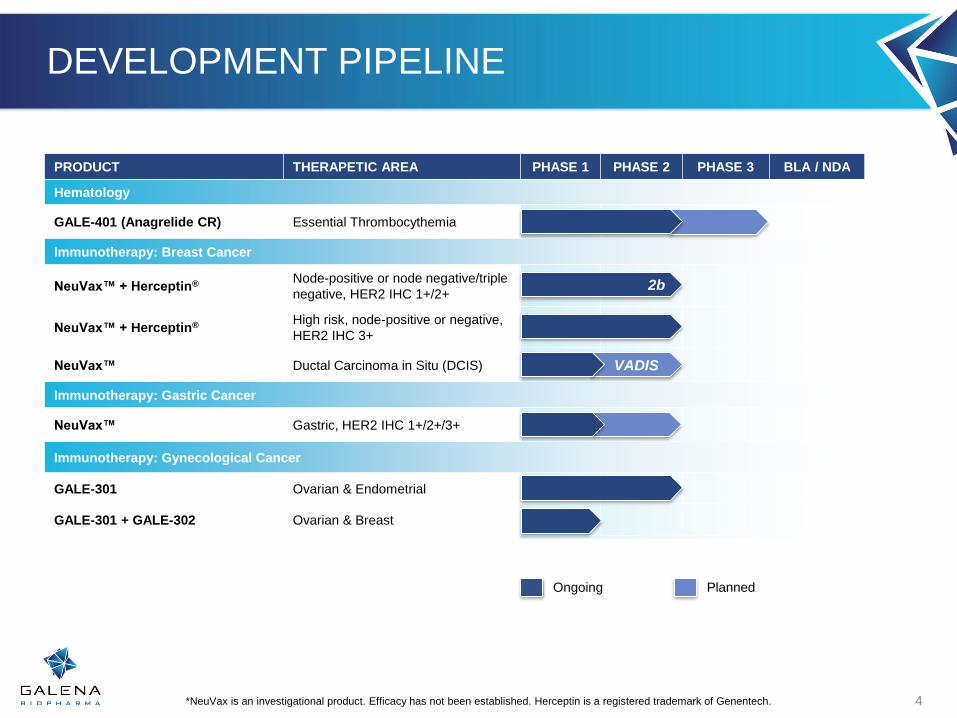
DEVELOPMENT PIPELINE
PRODUCT THERAPETIC AREA PHASE 1 PHASE 2 PHASE 3 BLA / NDA
Hematology
GALE-401 (Anagrelide CR) Essential Thrombocythemia
Immunotherapy: Breast Cancer
NeuVax™ + Herceptin® Node-positive or node negative/triple
negative, HER2 IHC 1+/2+
NeuVax™ + Herceptin® High risk, node-positive or negative,
HER2 IHC 3+
NeuVax™ Ductal Carcinoma in Situ (DCIS)
Immunotherapy: Gastric Cancer
NeuVax™ Gastric, HER2 IHC 1+/2+/3+
Immunotherapy: Gynecological Cancer
GALE-301 Ovarian & Endometrial
GALE-301 + GALE-302 Ovarian & Breast
*NeuVax is an investigational product. Efficacy has not been established. Herceptin is a registered trademark of Genentech.
Ongoing Planned
VADIS
4
2b

GALE-401
Anagrelide Controlled
Release (CR)
ANAGRELIDE
Anagrelide suppresses megakaryocytopoiesis by inhibiting PDE III-dependent and PDE III-independent mechanisms
No DNA damaging or cytotoxic effect
Immediate release version indicated for the treatment of patients with thrombocythemia, secondary to myeloproliferative disorders to reduce the elevated platelet count and the risk of thrombosis and to ameliorate associated symptoms including thrombo-hemorrhagic events
Approved to treat Myleoproliferative Neoplasms (MPNs) including Essential Thrombocythemia (ET)
6

ANAGRELIDE IMMEDIATE RELEASE (IR) AEs
Related Adverse Events (AEs)AGRYLINa
(n=942)%
Cardiac 42
Generalc 83
Gastrointestinal 92
Respiratory, thoracic and mediastinal 18
Skin and subcutaneous tissue 14
Musculoskeletal and connective tissue 6
Nervous system 65
Vascular <5
Hepatobiliary <5
Blood and Lymphatic <5
Number of AEs/patient 3.3
a Anagrelide IR ADR data from the product labelc General AEs referred to fatigue, peripheral edema, and malaise
Most common
reasons for
discontinuation
7Sources: Harrison et al N Engl J Med 2005;353:33-45; Mehta et al, (2014) Epidemiology of myeloproliferative neoplasms in the United
States, Leukemia & Lymphoma, 55:3, 595-600, DOI: 10.3109/10428194.2013.813500; Agrylin is a registered trademark of Shire.
Approximately 25% – 30%
of patients are intolerant
to Anagrelide IR
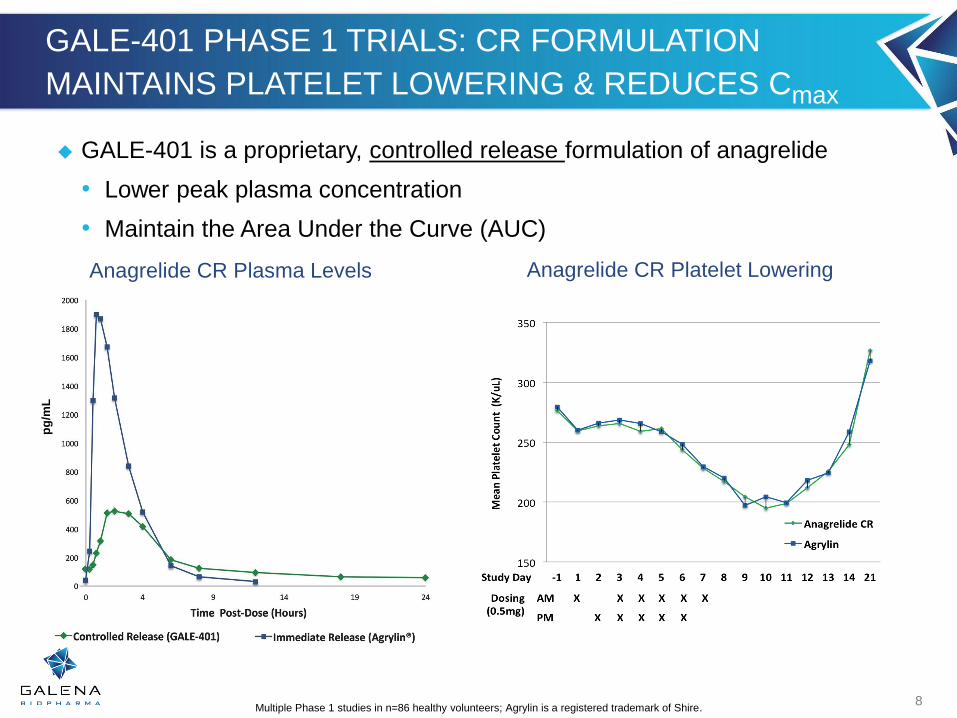
GALE-401 PHASE 1 TRIALS: CR FORMULATION
MAINTAINS PLATELET LOWERING & REDUCES Cmax
8Multiple Phase 1 studies in n=86 healthy volunteers; Agrylin is a registered trademark of Shire.
Anagrelide CR Plasma Levels
pg
/mL
Anagrelide CR Platelet Lowering
GALE-401 is a proprietary, controlled release formulation of anagrelide
• Lower peak plasma concentration
• Maintain the Area Under the Curve (AUC)

GALE-401 DEMONSTRATES IMPROVED AE PROFILES
IN KEY CATEGORIES
Related Adverse Events (AEs)GALE-401a
(N=18)n (%)
AGRYLINb
(n=942)%
Cardiac 6 (33) 42
Generalc 5 (27.8) 83
Gastrointestinal 9 (50) 92
Respiratory, thoracic and mediastinal 2 (11) 18
Skin and subcutaneous tissue 2 (11) 14
Musculoskeletal and connective tissue 1 (6) 6
Nervous system 9 (50) 65
Vascular 3 (16) <5
Hepatobiliary 2 (11) <5
Blood and Lymphatic 1 (6) <5
Number of AEs/patient 2.3 3.3
A Anagrelide CR Related AE data from the Phase 2 study; Source: Table 4, 2/12/2016b Anagrelide IR ADR data from the product labelc General AEs referred to fatigue, peripheral edema, and malaise
9

GALE-401 PHASE 2 STUDY SUPPORTS TARGETING IR INTOLERANT POPULATION
0
50
100
150
200
250
6001 2002 9001
On IR On GALE-401
Mean 7days 106 days
Median 7days 75 days
Max 7days 196 days
Min 7days 47 days
Three patients that discontinued IR were
on GALE-401 for average of 106 daysTwo IR intolerant patients were on
GALE-401 for 660 days and 450 days
0
200
400
600
800
1000
1200
1400
1600
2001 6005
On GALE-401
On IR
10
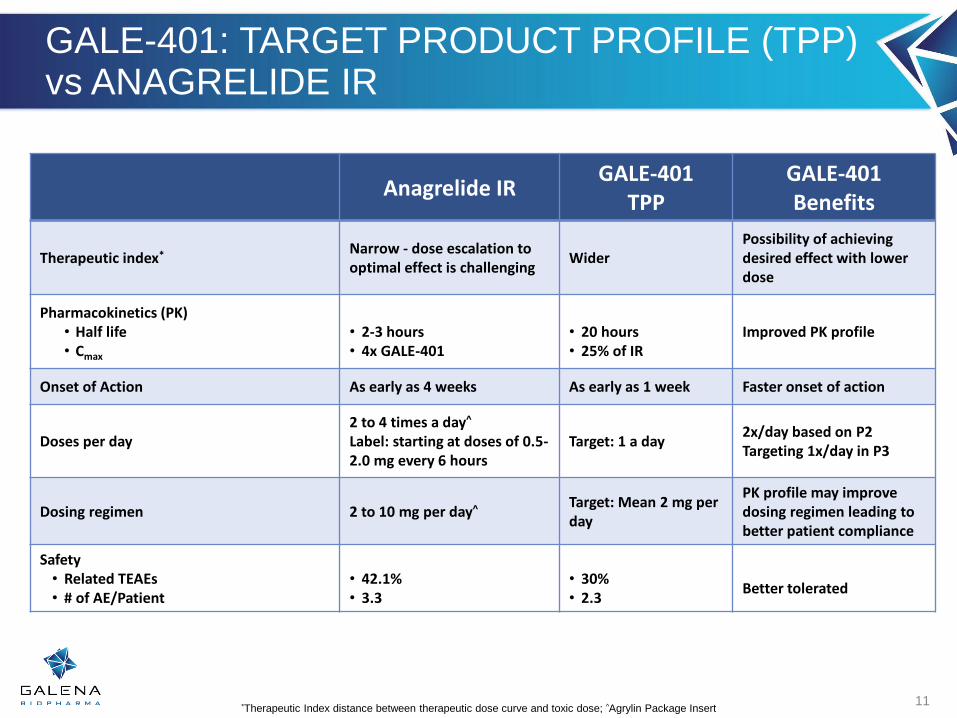
GALE-401: TARGET PRODUCT PROFILE (TPP) vs ANAGRELIDE IR
11
Anagrelide IRGALE-401
TPPGALE-401Benefits
Therapeutic index* Narrow - dose escalation to optimal effect is challenging
WiderPossibility of achieving desired effect with lower dose
Pharmacokinetics (PK) • Half life• Cmax
• 2-3 hours• 4x GALE-401
• 20 hours• 25% of IR
Improved PK profile
Onset of Action As early as 4 weeks As early as 1 week Faster onset of action
Doses per day2 to 4 times a day^
Label: starting at doses of 0.5-2.0 mg every 6 hours
Target: 1 a day2x/day based on P2Targeting 1x/day in P3
Dosing regimen 2 to 10 mg per day^ Target: Mean 2 mg per day
PK profile may improvedosing regimen leading to better patient compliance
Safety• Related TEAEs• # of AE/Patient
• 42.1%• 3.3
• 30%• 2.3
Better tolerated
*Therapeutic Index distance between therapeutic dose curve and toxic dose; ^Agrylin Package Insert
ESSENTIAL THROMBOCYTHEMIA (ET)
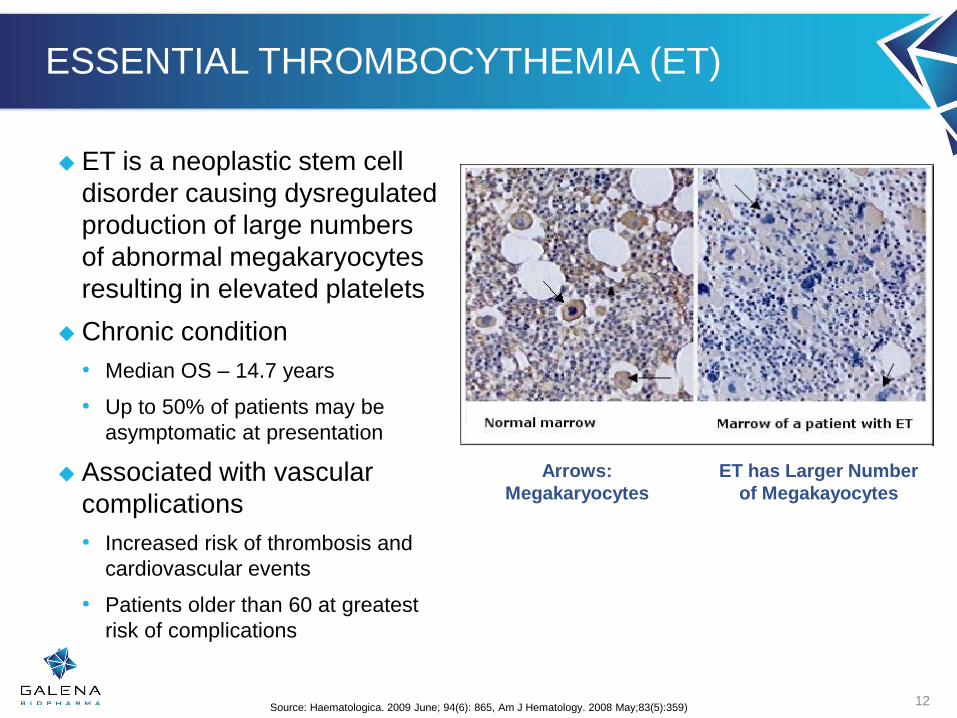
ET is a neoplastic stem cell
disorder causing dysregulated
production of large numbers
of abnormal megakaryocytes
resulting in elevated platelets
Chronic condition
• Median OS – 14.7 years
• Up to 50% of patients may be
asymptomatic at presentation
Associated with vascular
complications
• Increased risk of thrombosis and
cardiovascular events
• Patients older than 60 at greatest
risk of complications
12
Arrows:
Megakaryocytes
ET has Larger Number
of Megakayocytes
Source: Haematologica. 2009 June; 94(6): 865, Am J Hematology. 2008 May;83(5):359)
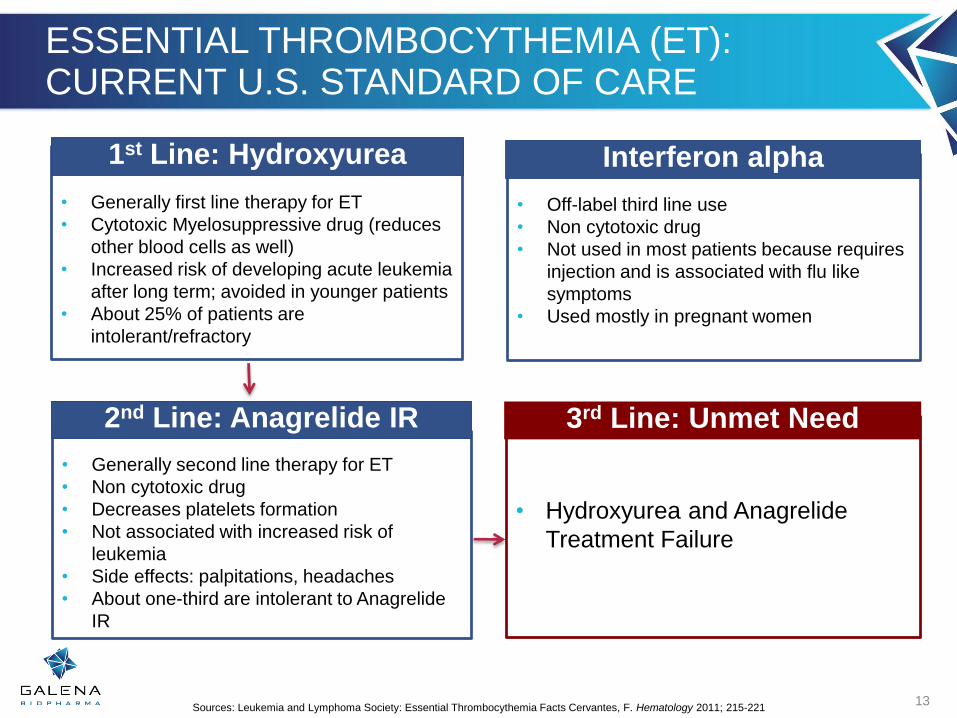
ESSENTIAL THROMBOCYTHEMIA (ET):CURRENT U.S. STANDARD OF CARE
13
• Generally first line therapy for ET
• Cytotoxic Myelosuppressive drug (reduces
other blood cells as well)
• Increased risk of developing acute leukemia
after long term; avoided in younger patients
• About 25% of patients are
intolerant/refractory
• Off-label third line use
• Non cytotoxic drug
• Not used in most patients because requires
injection and is associated with flu like
symptoms
• Used mostly in pregnant women
• Generally second line therapy for ET
• Non cytotoxic drug
• Decreases platelets formation
• Not associated with increased risk of
leukemia
• Side effects: palpitations, headaches
• About one-third are intolerant to Anagrelide
IR
• Hydroxyurea and Anagrelide
Treatment Failure
Sources: Leukemia and Lymphoma Society: Essential Thrombocythemia Facts Cervantes, F. Hematology 2011; 215-221
1st Line: Hydroxyurea
2nd Line: Anagrelide IR
Interferon alpha
3rd Line: Unmet Need
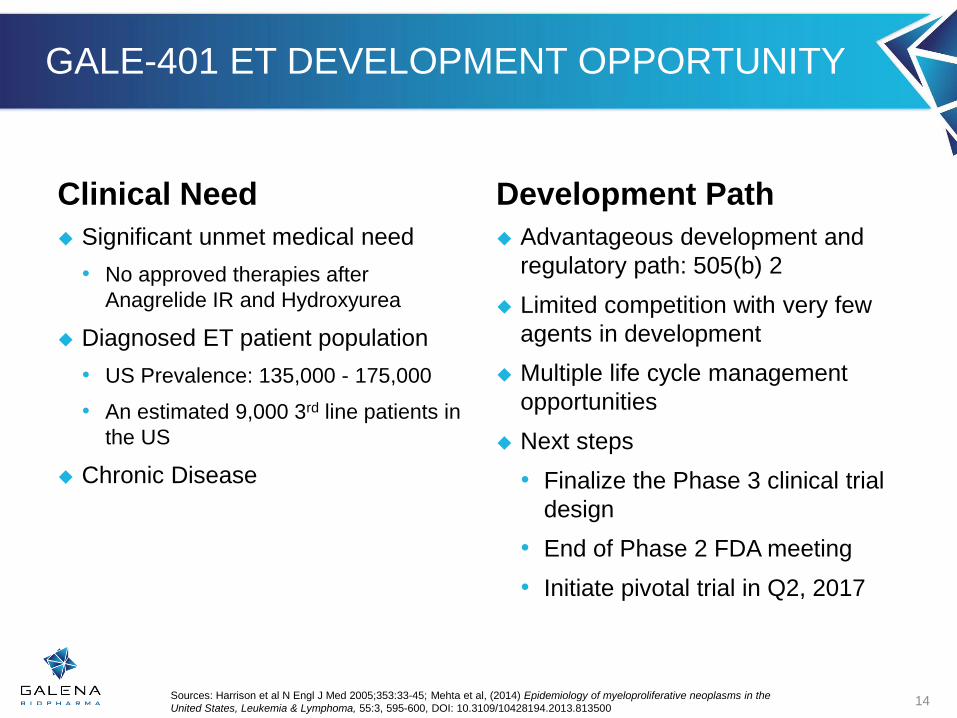
GALE-401 ET DEVELOPMENT OPPORTUNITY
Clinical Need
Significant unmet medical need
• No approved therapies after
Anagrelide IR and Hydroxyurea
Diagnosed ET patient population
• US Prevalence: 135,000 - 175,000
• An estimated 9,000 3rd line patients in
the US
Chronic Disease
Development Path
Advantageous development and
regulatory path: 505(b) 2
Limited competition with very few
agents in development
Multiple life cycle management
opportunities
Next steps
• Finalize the Phase 3 clinical trial
design
• End of Phase 2 FDA meeting
• Initiate pivotal trial in Q2, 2017
14Sources: Harrison et al N Engl J Med 2005;353:33-45; Mehta et al, (2014) Epidemiology of myeloproliferative neoplasms in the
United States, Leukemia & Lymphoma, 55:3, 595-600, DOI: 10.3109/10428194.2013.813500

NEUVAX™ (nelipepimut-S)
Targeting HER2
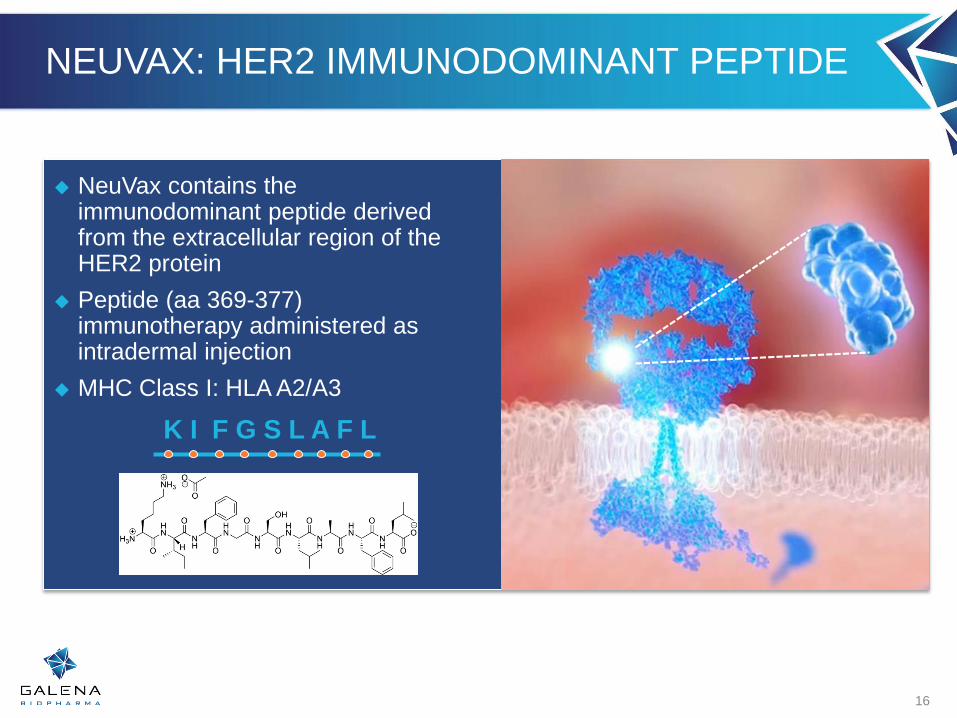
NEUVAX: HER2 IMMUNODOMINANT PEPTIDE
NeuVax contains the immunodominant peptide derived from the extracellular region of the HER2 protein
Peptide (aa 369-377) immunotherapy administered as intradermal injection
MHC Class I: HLA A2/A3
16
K I F G S L A F L

ELICITS A STRONG CD8+ T-CELL RESPONSE
NeuVax binds to antigen presenting cells (APCs)
NeuVax stimulates APCs to activate CD8+ cytotoxic T lymphocytes (CTLs)
CTLs rapidly replicate to seek out and destroy HER2 expressing tumor cells and micro-metastases
Booster series maintains long term immunologic response
Demonstrated inter- and intra-antigenic epitope spreading
17Sources: Peoples GE, et al (2005) JCO, 23(300, 7536-7545; Mittendorf EA, et al (2006) Surgery, 139(3): 407-418. Peoples, et al, ASCO 2012 Poster Presentation
0.4
1.8
0.7
0.5
0.0
0.5
1.0
1.5
2.0
2.5
% N
eu
Va
xsp
ecific
CD
8+
T c
ells
NeuVax Specific CD-8 CTLs: Pre-, Post, Mean and Long-Term (6 months)
Pre Max Mean Long-Term

T-Cell
CD28
OX40
GITR
CD122
CD27
CD360
HVEM
CD137
CTLA-4
PD-1
TIM-3
BTLA
VISTA
LAG-3
Activating Receptors Inhibitory Receptors
OUR VACCINES STIMULATE T-CELL
PROLIFERATION AND EXPANSION
18
T
cells
Checkpoint
inhibitors
Indirect Immune
Modulators
Co-
stimulators
Immune
Inhibitory
Enzymes
T
cells
T
cells
T
cells
T
cells
T
cells
T
cells
T
cells
T
cells
T
cells
Trastuzuma
b
IMMUNO-ONCOLOGY: COMBINATION STRATEGY
19
“There is growing evidence that a
multimodality approach targeting
different aspects of the immune
system may yield the greatest
clinical benefit.”

CORRELATION BETWEEN HER2 & MHC-1
There is an inverse correlation between HER2 and MHC class I
HER2 overexpression is associated with decreased expression of components of the antigen processing/ presentation pathway
Hypothesis: Trastuzumab treatment will
enhance response to vaccination by making tumor
cells more visible to T-cells/immune system
20

COMBINATION IMMUNOTHERAPY ENHANCES ANTIGEN PRESENTATION
Trastuzumab
HER2/neu
Breast
tumor cell
HER2/neu –derived peptide
presented on MHC-I
HER2/neu-
derived
peptide
Trastuzumab/HER2 complexes are internalized
and processed by proteasomes into short
peptides which are then presented on
MHC class I molecules.
Source: Mittendorf EA, et al (2006). Ann Surg Oncol;13:1085-98.
20.0
25.0
30.0
35.0
40.0
45.0
50.0
55.0
60.0
Ave
rage
% C
yto
toxi
city
51
Cr
0 ug 10 ug 50 ug
* p=0.015
22
Trastuzumab
PBMC from HER2/neu peptide, E75,
vaccinated patients efficiently recognize
and lyse trastuzumab-treated HER2/neu-
expressing tumor cell lines

Interim
Analysis
at 1 Year
DFS
Standard of Care: Standard Herceptin
dosing every 3 weeks for 1 year
6 doses of NeuVax given every 3 weeks
starting with third dose of Herceptin
+ 1 booster
dose every
6 months
thereafter
+ Dosing to disease
progression;
36 mo follow up
Primary
Endpoint
DFS at
24 mos.
300 adjuvant breast cancer patients, randomized 1:1
Single blind (subject)
Node positive or high risk node negative
HLA A2/A3+
HLA A24/A26+
HER2 IHC 1+/2+
Stratified by nodal status and HER2 status
Study Population
NEUVAX+TRASTUZUMAB: HER2 1+/2+ PHASE 2 STUDY
GM-CSF
+ GM-CSF
22

NEUVAX: CURRENT CLINICAL TRIALS
Phase Treatment HER2 Status
Indication Trial StatusProtocol Defined
# of PatientsCollaborations
2bCombination
with trastuzumab
1+, 2+
BREAST Node Positive or High Risk Node Negative
HLA A2+, A3+, A24+, A26+
EnrollingU.S. only
33 centers300
2Combination
with trastuzumab
3+ high risk
BREASTNode PositiveHLA A2+, A3+
EnrollingU.S. only
28 centers100
2Single agentVADIS Study
1+, 2+,3+
BREASTDuctal Carcinoma in
Situ (DCIS)HLA A2+
SuspendedU.S. only4 centers
48
2 Single agent1+,
2+,3+GASTRIC
HLA A2+, A3+Planned
India Only50
23

Targeting Folate Binding
Protein
GALE-301 &
GALE-302

GALE-301 & GALE-302
25Source: U.S. Ovarian Cancer http://seer.cancer.gov/statfacts/html/ovary.html
Targeted cancer immunotherapy
Folate Binding Protein (FBP) is over-expressed (20-80 fold) in >90% of ovarian and endometrial cancers
FBP has very limited tissue distribution and expression in non-malignant tissue making it an ideal immunotherapy target
Current treatments are generic
• Carboplatin and paclitaxel
• High recurrence rate
Most patients relapse with poor prognosis

GALE-301: OPTIMAL DOSE GROUP SHOWS PRELIMINARY EFFICACY
Source: Peoples, et. al, Poster Presentation, American Society of Clinical Oncology 201626
Phase 1/2a trial ongoing
Phase 1: Determined optimal dose and demonstrated safety and potent immune response
Phase 2a Preliminary data:
• At 16 months median follow-up:
Overall recurrence rate was 44.8% in the VG versus 54.5% in the CG (p=0.58),
Recurrence rate of 23.5% in patients who received booster inoculations.
• Two year DFS estimate in 1000 mcg dose group is 73.5% vaccine vs. 38.1% control (p=.03)
• GALE-301 plus GM-CSF is well tolerated and elicits a strong in vivo immune response with primarily Grade 1 and Grade 2 toxicities
Estimated 24 months Disease Free Survival by
Dosing Cohort

CORPORATE
OVERVIEW
27

LEADERSHIP TEAM
28
Mark W. Schwartz, Ph.D.
President & CEO
Apthera, Bayhill Therapeutics, Calyx
Therapeutics, Trega Biosciences, Incyte
Genomics, DuPont Diagnostics
Bijan Nejadnik, M.D.
Executive VP, Chief Medical Officer
Jazz Pharmaceuticals, Johnson & Johnson,
Stanford, Johns Hopkins, UC Davis
Remy Bernarda,
SVP, Investor Relations & Corporate
Communications
IR Sense, Hana Biosciences, Knight Equity
Markets, Bear Stearns, Goldman Sachs
John Burns, CPA
VP, Finance & Corporate Controller
Pixelworks, Moss Adams
Tom Knapp, Esq.
Interim General Counsel
Sucampo, Exemplar Law Partners,
NorthWestern Energy, Paul Hastings, The
Boeing Company
Joe Lasaga
VP, Business Development & Alliance
Management
Nektar Therapeutics, Rigel
Pharmaceuticals
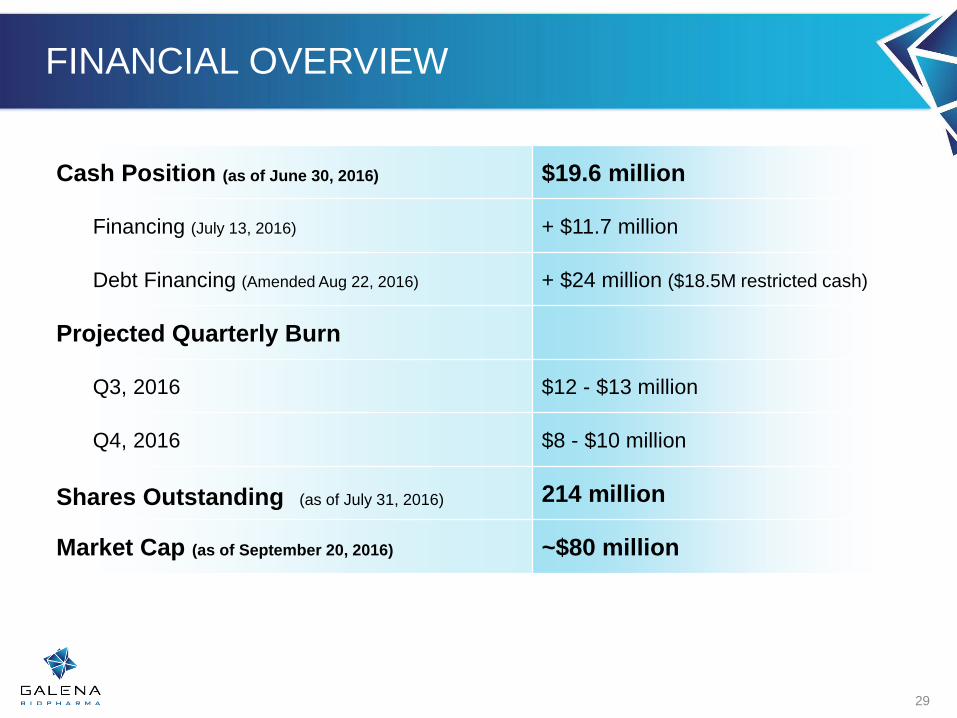
FINANCIAL OVERVIEW
Cash Position (as of June 30, 2016) $19.6 million
Financing (July 13, 2016) + $11.7 million
Debt Financing (Amended Aug 22, 2016) + $24 million ($18.5M restricted cash)
Projected Quarterly Burn
Q3, 2016 $12 - $13 million
Q4, 2016 $8 - $10 million
Shares Outstanding (as of July 31, 2016) 214 million
Market Cap (as of September 20, 2016) ~$80 million
29

MILESTONES
30
PROGRAM MILESTONEPROJECTEDDATE 2016
PROJECTEDDATE 2017
GALE-401 (anagrelide CR)
Present combined P1 & P2 safety data ✓
Confirmation of 505(b)2 pathway 2H
Phase 3 Initiation Q2
Phase 3 Dose Verification Q4
NeuVax™
(nelipepimut-S)
Fast Track Designation ✓
Initiate DCIS trial Q4
Combo H&N 1+/2+ Interim safety data Q4
Combo H&N Enrollment Complete Year-end
Combo H&N Interim Efficacy Q4
GALE-301GALE-302
Present 301/302 booster data ✓
Present GALE-301 Phase 2a primary analysis ✓
Orphan Drug Designation ✓
Present GALE-301 Biomarker & Dosing Data Q4

THANK YOU
NASDAQ: GALE

















