12
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | calvin-mccormick |
| View: | 214 times |
| Download: | 0 times |




GASTRIC LYMPHOMAS
Aswad H. Al.Obeidy
FICMS, FICMS GE&Hep
Kirkuk General Hospital

GASTRIC LYMPHOMAS The stomach is the most common site of GI lymphoma in
developed countries B cell Marginal zone B cell lymphoma of MALT type Diffuse large B cell lymphoma Uncommon types Malignant transformation of B cells from the marginal zone
of MALT leads to extranodal marginal zone B cell lymphoma of MALT type
lymphoma of MALT type represents approximately 40% of gastric lymphomas
The median age at diagnosis is approximately 60 years, with a wide age range.
The male-to-female ratio is equal.

Etiology and Pathogenesis Several lines of evidence support the key role of H. pylori in the
development of gastric MALT lymphoma Infection by H. pylori is present in approximately 90% of cases of
gastric MALT lymphoma examined histologically and in 98% of cases studied by serology
The epidemiologic studies cited earlier have shown a close correlation between the prevalence of H. pylori infection and gastric lymphoma in a given population
In vitro studies have shown that gastric MALT lymphoma tissue contains T cells that are specifically reactive to H. pylori.
regression of gastric MALT lymphoma in response to eradication of H. pylori.
Approximately 30% of gastric MALT lymphomas have a t(11;18) (q21;q21) translocation

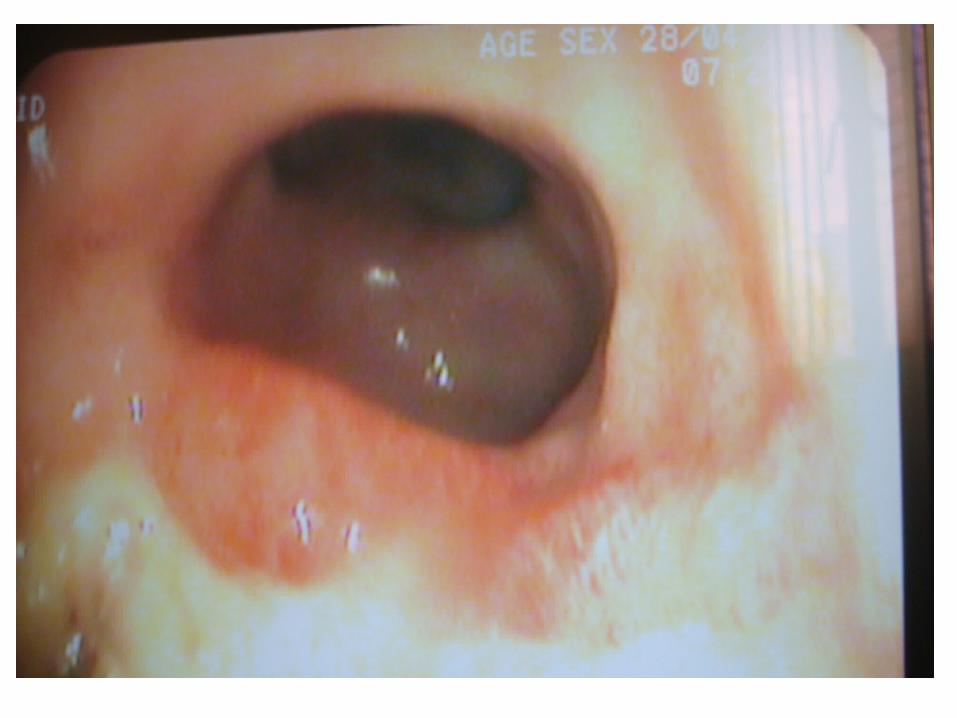
Gross Appearance Location and Histology
Low-grade gastric MALT lymphomas are most commonly located in the antrum (41%)
may be multifocal in 33% of cases Lesions may appear as ulcers in 47% of cases, erosions in 23%, or simply as erythema in 30%. The key histologic feature of low-grade MALT lymphoma is
the presence of lymphoepithelial lesions

Symptoms, Signs, and Laboratory
Tests The most common symptoms at presentation are epigastric
or abdominal pain (53%) dyspepsia (32%) Nausea or evidence of gastric bleeding is unusual B symptoms (fever, night sweats, weight loss) are distinctly
unusual Serum levels of LDH and β2-microglobulin are usually
normal.

Diagnosis and Staging Studies
Patients are evaluated by EGD H. pylori infection should be established by histology, breath test,
or serology upper airway examination CT scans of the abdomen and pelvis CT scan of the chest or chest radiograph bone marrow aspiration and biopsy measurement of serum LDH Gastric endoscopic ultrasound should be performed to assess the
thickness of stomach wall involvement Screening for translocations t(11;18), t(1;14), and t(14;18) is not
routinely performed

Treatment eradicating H. pylori have become the mainstay of therapy for low-
grade gastric MALT lymphoma reserving more toxic therapies such as radiation, chemotherapy,
or surgery for more advanced disease or early-stage disease that does not respond adequately to antibiotics.
Follow-up endoscopy with multiple biopsies should be done 6 to 8 weeks after completion of treatment to document clearance of infection and to assess disease regression
then followed with endoscopy approximately every 6 months for 2 years and then yearly
Surgical resection cures greater than 80% of patients with stage IIE disease
Single-agent oral chemotherapy using cyclophosph. or chlorambucil has activity, with a 75% complete remission rate and a 5-year survival rate of 75%
Rituximab also appears to have significant activity Localized low-dose radiotherapy is associated with a 5-year
disease-free survival of approximately 80% and 5-year overall survival of 90%
DIFFUSE LARGE B CELL LYMPHOMA OF THE STOMACH Approximately 45% to 50% of gastric lymphomas WHO classification agreed to use the term extranodal marginal
zone B cell lymphoma of MALT type for “low-grade” lesions, and the term diffuse large B cell lymphoma for “high-grade” lesions
The optimal management of diffuse large B cell lymphoma of the stomach is controversial
localized disease was approached with surgery alone or surgery followed by radiation and/or chemotherapy for patients with poor prognostic features
70% of patients with stage I disease are disease free 5 years after surgery.[On the other hand, surgery carries a 5% to 10% risk of mortality and is associated with significant morbidity
Radiation therapy has significant activity in gastric large B cell lymphoma
Chemotherapy has significant activity in more advanced-stage gastric large B cell lymphoma
CHOP[†] × 3-4 cycles + XRT[‡] + rituximab

















