CLINICAL—LIVER Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection: A Systematic Review and Meta-analysis Yee Hui Yeo, 1 Hsiu J. Ho, 2 Hwai-I Yang, 3 Tai-Chung Tseng, 4 Tetsuya Hosaka, 5 Huy N. Trinh, 6 Min-Sun Kwak, 7 Young Min Park, 8 James Yan Yue Fung, 9 Maria Buti, 10,11 Manuel Rodríguez, 12 Sombat Treeprasertsuk, 13 Carmen Monica Preda, 14 Teerapat Ungtrakul, 15 Phunchai Charatcharoenwitthaya, 16 Xiangyong Li, 17 Jiayi Li, 18 Jian Zhang, 19,20 Michael Huan Le, 1 Bin Wei, 1 Biyao Zou, 1 An Le, 1 Donghak Jeong, 1 Nicholas Chien, 21 Leslie Kam, 21 Chiao-Chin Lee, 22 Mar Riveiro-Barciela, 10,11 Doina Istratescu, 14 Tassanee Sriprayoon, 16 Yutian Chong, 17 Tawesak Tanwandee, 16 Mariko Kobayashi, 23 Fumitaka Suzuki, 5 Man-Fung Yuen, 9 Hyo-Suk Lee, 7 Jia-Horng Kao, 4,24 Anna S. Lok, 25 Chun-Ying Wu, 2,26 and Mindie H. Nguyen 1 1 Division of Gastroenterology and Hepatology, Stanford University Medical Center, Palo Alto, California; 2 Division of Translational Research, Taipei Veterans General Hospital, Taipei City, Taiwan; 3 Genomics Research Center, Academia Sinica, Taipei, Taiwan; 4 Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan; 5 Department of Hepatology, Toranomon Hospital, Takatsu-ku, Kawasaki, Japan; 6 San Jose Gastroenterology, San Jose, California; 7 Department of Internal Medicine and Liver Research Institute, Seoul National University Hospital, Seoul, Republic of Korea; 8 Hepatology Center, Department of Internal Medicine and Biomedical Research Center, Bundang Jesaeng General Hospital, Seongnam-si, Gyeonggi-do, Republic of Korea; 9 Department of Medicine, The University of Hong Kong, Hong Kong, People’s Republic of China; 10 Liver Unit, Hospital Universitari Vall d’Hebron and Ciberehd del Instituto Carlos III, Barcelona, Spain; 11 Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd), Instituto de Salud Carlos III, Barcelona, Spain; 12 Liver Unit, Division of Gastroenterology and Hepatology, Hospital Universitario Central de Asturias, Oviedo, Asturias, Spain; 13 Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 14 Department of Gastroenterology, Clinic Fundeni Institute, Bucharest, Romania; 15 Faculty of Medicine and Public Health, HRH Princess Chulabhorn College of Medical Science, Chulabhorn Royal Academy, Thailand; 16 Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand; 17 Department of Infectious Diseases, The Third Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 18 Palo Alto Medical Foundation, Mountain View Division, Palo Alto, California; 19 Chinese Hospital, San Francisco, California; 20 School of Nursing, University of California, San Francisco, California; 21 Kaohsiung Medical University, Kaohsiung, Taiwan; 22 Department of Internal Medicine, Tri-Service General Hospital, Taipei, Taiwan; 23 Research Institute for Hepatology, Toranomon Hospital, Takatsu-ku, Kawasaki, Japan; 24 Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan; 25 Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan; and 26 College of Public Health, China Medical University, Taichung, Taiwan This article has an accompanying continuing medical education activity, also eligible for MOC credit, on page e18 (https://www. gastrojournal.org/cme/home). Learning Objective: Upon completion of this CME activity, successful learners will be able to explain the prevalence, predictors, and significance of hepatitis B surface antigen (HBsAg) seroclearance in adults with chronic hepatitis B virus (HBV) infection. Gastroenterology 2019;156:635–646 CLINICAL LIVER
Transcript
Gastroenterology 2019156635ndash646
CLINICALmdashLIVER
Factors Associated With Rates of HBsAg Seroclearance inAdults With Chronic HBV Infection A Systematic Reviewand Meta-analysis
Jia-Horng Kao424 Anna S Lok25 Chun-Ying Wu226 and Mindie H Nguyen1
1Division of Gastroenterology and Hepatology Stanford University Medical Center Palo Alto California 2Division of TranslationalResearch Taipei Veterans General Hospital Taipei City Taiwan 3Genomics Research Center Academia Sinica Taipei Taiwan4Division of Gastroenterology and Hepatology Department of Internal Medicine National Taiwan University Hospital TaipeiTaiwan 5Department of Hepatology Toranomon Hospital Takatsu-ku Kawasaki Japan 6San Jose Gastroenterology San JoseCalifornia 7Department of Internal Medicine and Liver Research Institute Seoul National University Hospital Seoul Republic ofKorea 8Hepatology Center Department of Internal Medicine and Biomedical Research Center Bundang Jesaeng GeneralHospital Seongnam-si Gyeonggi-do Republic of Korea 9Department of Medicine The University of Hong Kong Hong KongPeoplersquos Republic of China 10Liver Unit Hospital Universitari Vall drsquoHebron and Ciberehd del Instituto Carlos III Barcelona Spain11Centro de Investigacioacuten Biomeacutedica en Red de Enfermedades Hepaacuteticas y Digestivas (CIBERehd) Instituto de Salud Carlos IIIBarcelona Spain 12Liver Unit Division of Gastroenterology and Hepatology Hospital Universitario Central de Asturias OviedoAsturias Spain 13Department of Medicine Faculty of Medicine Chulalongkorn University Bangkok Thailand 14Department ofGastroenterology Clinic Fundeni Institute Bucharest Romania 15Faculty of Medicine and Public Health HRH PrincessChulabhorn College of Medical Science Chulabhorn Royal Academy Thailand 16Department of Medicine Faculty of MedicineSiriraj Hospital Mahidol University Bangkok Thailand 17Department of Infectious Diseases The Third Affiliated Hospital SunYat-sen University Guangzhou Peoplersquos Republic of China 18Palo Alto Medical Foundation Mountain View Division Palo AltoCalifornia 19Chinese Hospital San Francisco California 20School of Nursing University of California San Francisco California21Kaohsiung Medical University Kaohsiung Taiwan 22Department of Internal Medicine Tri-Service General Hospital TaipeiTaiwan 23Research Institute for Hepatology Toranomon Hospital Takatsu-ku Kawasaki Japan 24Graduate Institute of ClinicalMedicine College of Medicine National Taiwan University Taipei Taiwan 25Division of Gastroenterology and HepatologyUniversity of Michigan Ann Arbor Michigan and 26College of Public Health China Medical University Taichung Taiwan
This article has an accompanying continuing medical education activity also eligible for MOC credit on page e18 (httpswwwgastrojournalorgcmehome) Learning Objective Upon completion of this CME activity successful learners will be able to explainthe prevalence predictors and significance of hepatitis B surface antigen (HBsAg) seroclearance in adults with chronic hepatitis Bvirus (HBV) infection
WHAT YOU NEED TO KNOW
636 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
See editorial on page 548
BACKGROUND AND CONTEXT
Functional cure of HBV infection is defined based onHBsAg seroclearance but reported annual rates ofHBsAg seroclearance vary
NEW FINDINGS
In a meta-analysis of 42588 patients in 34 studies thepooled annual rate of HBsAg seroclearance was 102which increased to 1799 after 15 years Testingnegative for HBeAg and low level of HBV DNA orHBsAg level at baseline were associated with higherrates of HBsAg seroclearance
LIMITATIONS
This was a meta-analysis and there was a high level ofheterogeneity in pooled rates among studies
IMPACT
The findings identify annual rate and factors associatedwith HBsAg seroclearance indicate the need for life-longtreatment for most patients These factors might beconsidered in balancing treatment groups for clinicaltrials of agents designed to cure HBV infection
BACKGROUND amp AIMS Seroclearance of hepatitis B surfaceantigen (HBsAg) is a marker for clearance of chronic hepatitis Bvirus (HBV) infection but reported annual incidence rates ofHBsAg seroclearance vary We performed a systematic reviewand meta-analysis to provide more precise estimates of HBsAgseroclearance rates among subgroups and populationsMETHODS We searched PubMed Embase and the Cochranelibrary for cohort studies that reported HBsAg seroclearance inadults with chronic HBV infection with more than 1 year offollow-up and at least 1 repeat test for HBsAg Annual and 5-10- and 15-year cumulative incidence rates were pooled usinga random effects model RESULTS We analyzed 34 publishedstudies (with 42588 patients 303754 person-years of follow-up and 3194 HBsAg seroclearance events) including additionaland updated aggregated data from 19 studies The pooledannual rate of HBsAg seroclearance was 102 (95 CI 079ndash127) Cumulative incidence rates were 403 at 5 years (95CI 249ndash593) 816 at 10 years (95 CI 524ndash1172) and1799 at 15 years (95 CI 618ndash2324) There were no sig-nificant differences between the sexes A higher proportion ofpatients who tested negative for HBeAg at baseline had sero-clearance (133 95 CI 076ndash205) than those who testedpositive for HBeAg (040 95 CI 025ndash059) (P lt 01)Having HBsAg seroclearance was also associated with a lowerbaseline HBV DNA level (661 log10 IUmL 95 CI 594ndash727)vs not having HBsAg seroclearance (771 log10 IUmL 95 CI741ndash802) (P lt 01) and with a lower level of HBsAg atbaseline (274 log10 IUmL 95 CI 188ndash360) vs not havingHBsAg seroclearance (390 log10 IUmL 95 CI 373ndash406)(P lt 01) HBsAg seroclearance was not associated with HBVgenotype or treatment history Heterogeneity was substantialacross the studies (I2 frac14 9749) CONCLUSION In a systematicreview and meta-analysis we found a low rate of HBsAgseroclearance in untreated and treated patients (pooled annualrate approximately 1) Seroclearance occurred mainly inpatients with less active disease Patients with chronic HBVinfection should therefore be counseled on the need for lifelongtreatment and curative therapies are needed
Keywords Natural History Prognosis Disease ProgressionCHB
hronic hepatitis B (CHB) is a significant public health
Abbreviations used in this paper ALT alanine aminotransferase cccDNAcovalently closed circular DNA CHB chronic hepatitis B CI confidenceinterval HBeAg hepatitis B e antigen HBsAg hepatitis B surface antigenHBV hepatitis B virus HCC hepatocellular carcinoma NOS NewcastlendashOttawa quality assessment scale
Most current article
copy 2019 by the AGA Institute0016-5085$3600
httpsdoiorg101053jgastro201810027
Cproblem affecting approximately 257 million peopleglobally1 Patients who are chronically infected with hepatitisB virus (HBV) are at greater risk of developing cirrhosis andhepatocellular carcinoma (HCC) Because the development ofthese complications may take decades to present virologicmarkers such as hepatitis B e antigen (HBeAg) status serumHBV DNA alanine aminotransferase (ALT) levels and quan-titative hepatitis B surface antigen (HBsAg) are used todetermine the status of CHB and to predict prognosis
A sterilizing cure for CHB is not possible because of thepresence of integrated HBV DNA and the long half-life ofcovalently closed circular DNA (cccDNA) Therefore thetherapeutic goal for new treatments of CHB is to achieve
functional cure that is HBsAg seroclearance2 HBsAg sero-clearance signifies sustained immune control of HBV and isassociated with improved clinical outcomes with a lowerrisk of decompensated cirrhosis HCC and liver-relateddeath3ndash5 HBsAg seroclearance can occur spontaneouslybut the reported rates have been variable Prior cohortstudies showed that the annual HBsAg seroclearance ratecan range from a low of 012 to a high of 2386ndash8 and isaffected by a myriad of patient characteristics such as sexage cirrhosis HBeAg status HBV DNA level and serumHBsAg level69 In addition reported rates of HBsAg sero-clearance with currently available treatments are low2
Because HBsAg seroclearance is a rare event that isaffected by a variety of host and viral factors determining anaccurate incidence rate and the predictors for HBsAg sero-clearance has been difficult Therefore using a systematicreview and meta-analysis of multiple cohorts from differentgeographic regions we aimed to provide more precise esti-mates of HBsAg seroclearance rates among different sub-groups and populations that can then be usedwhen discussingtreatment decisions with patients In addition these estimatesmay assist with the development of new therapeutic agents
MethodsThis study was performed and presented according to the
Preferred Reporting Items for Systematic Reviews and
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 637
CLINICAL
LIVE
R
Meta-analyses (ie PRISMA) guidelines10 The protocol of thisstudy is available online at PROSPERO (CRD42017079843)
Search Strategy and Study SelectionElectronic searches were performed in PubMed Embase and
the Cochrane library from the inception of the database to July 52017 by using various combinations of the keywords HBVinfection HBsAg seroclearance and cohort studies (see supple-mentary data for search strategies) In addition we manuallysearched the bibliography of the included articles and relevantsystematic reviews for additional articles No language restric-tion was imposed All literature searches reviews and selectionswere independently performed by 2 authors Discrepancies wereresolved through consultation with a third author
Cohort studies that reported HBsAg seroclearance in adultpatients (gt18 years old) with CHB (HBsAg andor HBV DNApositive for more than 6 months) with more than 1-year follow-up and at least 1 repeat test for HBsAg were included Bothpopulation-based cohorts and hospital- or clinic-based cohortswere included There was no restriction on treatment history
Studies that were clinical trials cross-sectional studies caseseries and case reports were excluded Given the rarity ofHBsAg seroclearance events studies with less than 200 pa-tients were also excluded Finally to enhance the homogeneityof the included studies we excluded patients with human im-munodeficiency virus hepatitis D virus or hepatitis C virus co-infection and patients with prior HCC
Data ExtractionTwo authors independently extracted the following data
from each study using a standardized data extraction formfollow-up period (person-years) baseline characteristics ofpatients at entry (age sex raceethnicity history of HBVtreatment HBeAg HBV genotype ALT level platelet count HBVDNA and cirrhosis status) and outcomes (annual HBsAgseroclearance rate cumulative seroclearance rates subsequentliver transplantation HCC and death) For articles that did notreport the annual HBsAg seroclearance rate we estimated it byusing the following formula
number of patients with HBsAg seroclearancemean follow up duration frac12years total number of patients
We estimated person-years of follow-up by dividing thenumber of patients with seroclearance by the annual sero-clearance rate in articles that did not report person-years offollow-up Any discrepancies were resolved in consultationwith a third reviewer
Corresponding authors of eligible studies were contacted formissing data andor updated aggregated data for primaryoutcome and subgroup analyses if additional follow-up data of thepublished cohorts were available To avoid overlapped patientswe also contacted the authors to request the data of the entirecohort if there were multiple articles published from that cohort
Risk-of-Bias AssessmentWe used a risk-of-bias tool modified from the Newcastlendash
Ottawa quality assessment scale (NOS) to assess the qualityof individual reports11 The NOS is a scoring tool comprising8 items with 9 scores that assesses how well the investigators
selected their participants (score ranges from 0 to 4) howcomparable their results may be (score ranges from 0 to 2) andhow applicable the outcomes are (score ranges from 0 to 3)The higher the score the better the quality of the study and thelower the risk of bias We categorized the studies as goodquality if the total score was 7 or more fair if the score was 4ndash6 and poor if the score was lt4
OutcomesThe prespecified primary outcomes were the annual rate
and cumulative seroclearance rate of HBsAg seroclearance at 510 and 15 years HBsAg seroclearance was defined as havingnegative HBsAg test results in patients with previously positiveresults The secondary outcome was the distribution of annualHBsAg seroclearance in patients with different demographicand clinical characteristics (geographic regions HBV genotypesHBeAg status presence of cirrhosis treatment history andother clinical characteristics) For analysis by treatment historywe selected studies that included only untreated patients whoalso remained untreated throughout the study period for theuntreated group and we selected studies that included onlypatients who were treatment naiumlve and initiated therapy atstudy entry for the treated group
Statistical AnalysisAnnual HBsAg seroclearance rate and 5- 10- 15-year cu-
mulative incidence rates were pooled using the random effectsmodel of DerSimonian and Laird12 Because the values of theseestimates can be close to 0 we used the FreemanndashTukeytransformation to stabilize the variance and the Wilson scoremethod to generate 95 confidence intervals (CIs)13 Theresulting values were then back-transformed and are presentedas a percentage14 Heterogeneity across studies was assessedby I2 statistics and Cochranrsquos Q test15 The Eggerrsquos test was usedto evaluate small study bias quantitatively
We performed subgroup analyses to examine whether theannual HBsAg seroclearance rates were modified by the pre-planned variables including study locationregion (becauseethnicity data were difficult to discern) study settings (popula-tion based vs health care service based) mean age sex baselinecirrhosis HBeAg positivity and HBV genotype We calculated theannual seroclearance rates of the aforementioned subgroup an-alyses only in studies that provided us with original dataFurthermore we pooled the mean value of key clinical parame-ters (ALT platelet count HBV DNA and quantitative HBsAg level)to determine differences in baseline laboratory values betweenpatients with and without incident HBsAg seroclearance We alsoperformed a sensitivity analysis by excluding studies with a highrisk of bias and studies with sample sizes lt500
We set 05 as the threshold of statistical significance for theP value (2-tailed) All analyses were conducted using the metapackage of R software version 33216 Metarate was used tocompute the pooled estimate of both the annual and cumulativeHBsAg seroclearance rates and metamean was used to pool themean values of various baseline laboratory data
ResultsFrom the electronic and manual search 4833 records
were identified (Figure 1) After removing duplicates and
638 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
screening the titles and abstracts 180 potentially eligiblestudies were retrieved for full-text reviews After review atotal of 34 articles (42588 CHB patients) met our inclusionand exclusion criteria and were included in the meta-analysis We received updated aggregated data from 19 ofthe 34 studies717ndash34 including 3 studies from 1 center(Toranomon Hospital Tokyo Japan) but we contacted thestudy authors and confirmed that only nonduplicate pa-tients were included in our meta-analysis192031
Characteristics of Included StudiesTable 1 shows the characteristics of included studies and
of the participants CHB patients from 14 countries wereincluded with the majority from the Asia Pacific region (23studies) Four studies were population based and the restwere conducted with data derived from hospitals or healthcare centers The sample sizes of the included studiesranged from 217 to 6621 with the proportion of malesranging from 444 to 903 The mean age ranged from342 to 50 years Twenty-two out of 34 studies showed lowrisk of bias (Supplementary Table 1)
Overall Annual Seroclearance and CumulativeIncidence
Among the 42588 CHB patients 3194 patients experi-enced HBsAg seroclearance The annual seroclearance ratesranged from 015 to 302 with a pooled rate of 102
Figure 1 Preferred Reporting Items for Systematic Reviewsand Meta-analyses (PRISMA) flow chart of article selection
(95 CI 079ndash127) and high heterogeneity (I2 frac14 9749)(Figure 2) The pooled 5- 10- and 15-year cumulativeincidence rates were nonlinear at 403 (95 CI 246ndash597 I2 frac14 9957) 816 (95 CI 519ndash1179 I2 frac149976) and 1799 (95 CI 1083ndash2696 I2 frac14 9991)respectively (Figure 3 and Supplementary Table 2)
Annual Seroclearance Rate by BaselineDemographic and Clinical Characteristics
The pooled annual seroclearance rates for male (n frac1411142) and female (n frac14 6080) patients were 113 (95CI 078ndash155) and 087 (95 CI 049ndash136) respectivelybut the difference was not statistically significant (P frac14 43)(Figure 4) The mean age of the study cohort was 45 andthe pooled annual seroclearance rates were similar forstudies with a mean age less than 45 years (095 95 CI069ndash126) compared with studies with a mean age of 45years and older (112 95 CI 040ndash220) (SupplementaryFigure 1) Analyses by patients of specific age groups andraceethnicity were not performed because of lack of pri-mary data with most studies not reporting data by agegroups and many studies of mixed racesethnicities notreporting results stratified by raceethnicity
There were 9 studies that separately reported theannual seroclearance rate in patients who were HBeAgpositive (n frac14 3922) and those who were HBeAg negative(n frac14 15205) at baseline (Figure 4) Patients who wereHBeAg negative (133 95 CI 076ndash205) had almost a33 times higher HBsAg seroclearance rate than patientswho were HBeAg positive (040 95 CI 025ndash059)There were no significant differences in the annual sero-clearance rates between patients with cirrhosis (08495 CI 031ndash158 n frac14 970) and those without cirrhosis(104 95 CI 063ndash155 n frac14 13398) (P frac14 74)
Baseline Laboratory Parameters in PatientsWith HBsAg Seroclearance vs Those WithoutHBsAg Seroclearance
We investigated several baseline laboratory data that havebeen reported to have an association with HBsAg seroclear-ance (Figure 5) From 5 studies with quantitative HBsAg leveldata (1173 with incident HBsAg seroclearance 6246 without)the pooled mean quantitative HBsAg level was found to besignificantly lower among patients with HBsAg seroclearancecompared with those without seroclearance (274 log10 IUmL 95 CI 187ndash360 vs 390 log10 IUmL 95 CI 373ndash406 P lt 01) From 10 studies with HBV DNA data (1431with incident HBsAg seroclearance 16590 without) patientswith HBsAg seroclearance also showed a significantly lowerbaseline HBV DNA than those with no seroclearance (661log10 IUmL 95 CI 594ndash727 vs 771 log10 IUmL 95 CI741ndash802 P lt 01) In 16 studies with ALT data the pooledmean ALT levels among 1663 patients with and 14974without HBsAg seroclearance were not statistically different(64 UL 95 CI 27ndash150 vs 58 UL 95 CI 19ndash178 P frac1490) The pooled mean platelet count among 822 patients withand 9536 patients without HBsAg seroclearance in 10 studieswas also not statistically different (195 109L 95 CI
Table 1Characteristics of the Included Studies and Patients
Year and First Authora Region Settings Cohort TypePatients
n MaleMeanAge y
HBeAg(thorn)at Entry
Cirrhosisat Entry
IncidentHBsAg
Seroclearance
AnnualSeroclearance
Rate 5-yearCSR
10-yearCSR
15-yearCSR
2014 Kobayashi20 Asia Pacific Community Health care service 1130 705 405 81 273 200 163 9 18 262013 Hosaka19 Asia Pacific Community Health care service 791 627 43 442 169 38 070 24 8 182011 Suzuki31 Asia Pacific Community Health care service 615 464 35b 414 72 69 181 65 15 352016 Charatcharoenwi-
tthaya17Asia Pacific Mixed Health care service 233 172 416 135 22 7 229 mdash mdash mdash
2013 Treeprasertsuk25 Asia Pacific Academic Health care service 431 310 434 262 0 2 015 mdash mdash mdash
2015 Lauret22 Europe Academic Health care service 614 391 371 139 52 78 141 44 118 2172017 Riveiro-Barciela30 Europe Mixed Health care service 633 459 496 77 42 9 041 182 253 mdash
2016 Park28 Asia Pacific Academic Health care service 954 627 433 mdash mdash 75 105 365 903 25482014 Preda29 Europe Mixed Health care service 533 340 415 mdash 43 7 087 mdash mdash mdash
2015 Tseng33 Asia Pacific Academic Health care service 2686 1631 414 0 0 381 095 273 676 12392014 Fung18 Asia Pacific Academic Health care service 775 483 362 0 mdash 60 052 131 333 7192017 Ungtrakul34 Asia Pacific Academic Health care service 297 132 415 0 0 15 237 mdash mdash mdash
2016 Nguyen26 North America Mixed Health care service 3479 1987 443 1096 202 37 021 09 292 4252010 Liu7 Asia Pacific Community Population based 3302 1994 461 482 0 568 213 742 1732 36772011 Kwak21 Asia Pacific Academic Health care service 714 476 477 0 mdash 41 181 977 mdash mdash
2013 Luo24 Asia Pacific Academic Health care service 217 196 407 113 74 9 081 417 711 mdash
2015 Yapali44 North America Academic Health care service 234 122 35b 44 mdash 9 080 mdash mdash mdash
2002 Sanchez-Tapias8 Europe Academic Health care service 269 218 36 173 21 29 139 mdash mdash mdash
2015 Habersetzer45 Europe Academic Health care service 315 211 35b 69 mdash 29 158 mdash mdash mdash
2014 Farzi46 Middle East Community Health care service 399 231 356 0 0 48 122 mdash mdash mdash
2012 Arai47 Asia Pacific Academic Health care service 423 239 405 183 mdash 25 097 mdash mdash mdash
2005 Ahn48 Asia Pacific Academic Health care service 432 mdash mdash 0 mdash 49 046 mdash mdash mdash
2014 Ferreira49 South America Academic Health care service 548 336 377 mdash mdash 40 056 mdash mdash mdash
2016 Han50 Asia Pacific mdash Population based 634 485 486 0 0 117 302 mdash mdash mdash
2010 Simonetti36 North America Community Population based 1271 mdash 209b mdash mdash 158 065 mdash mdash mdash
2014 Kim9 Asia Pacific mdash Health care service 5409 3699 449 3601 2684 110 032 mdash mdash mdash
2016 Nagaoka51 Asia Pacific Academic Health care service 392 278 395b 285 111 50 091 mdash 54 982015 Orito27 Asia Pacific Academic Health care service 602 381 52b 295 110 13 030 mdash mdash mdash
2010 Tai32 Asia Pacific Mixed Health care service 6621 3761 342 1386 0 555 171 mdash mdash mdash
2016 Ari52 Middle East mdash Health care service 1427 767 371 48 mdash 84 104 mdash mdash mdash
2007 Nam53 Asia Pacific mdash Health care service 4061 2639 500 1584 893 47 036 mdash mdash mdash
2011 Lu54 Asia Pacific Academic Health care service 220 156 mdash 168 25 17 159 mdash mdash mdash
1998 Huo55 Asia Pacific Community Health care service 1355 1113 41 mdash mdash 58 157 mdash mdash mdash
2015 Lim23 Asia Pacific Community Population based 572 359 mdash 234 mdash 145 130 mdash mdash mdash
CSR cumulative seroclearance rateaTable 1 referencesbMedian age
February2019
HBsAgSeroclearance
inAdults
With
ChronicHBV
Infection639
CLINICAL LIVER
Figure 2 Pooled annualHBsAg seroclearance rateof chronic hepatitis B pa-tients Annual HBsAgseroclearance rates werecombined using a randomeffects model The size ofeach square representsthe weight of that studyThe vertical dotted linerepresents the pooledrate See Table 1 for fullcitation details for thestudies ASR annualseroclearance rate SPnumber of patients whohave achieved HBsAgseroclearance
Figure 3 Pooled 5- 10- and 15-year cumulative incidencerates of HBsAg seroclearance
640 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
183 109ndash208 109 vs 196 109L 95 CI 182 109ndash210 109 P frac14 95)
Region Scale and Setting of StudiesWe stratified the pooled HBsAg seroclearance rates by
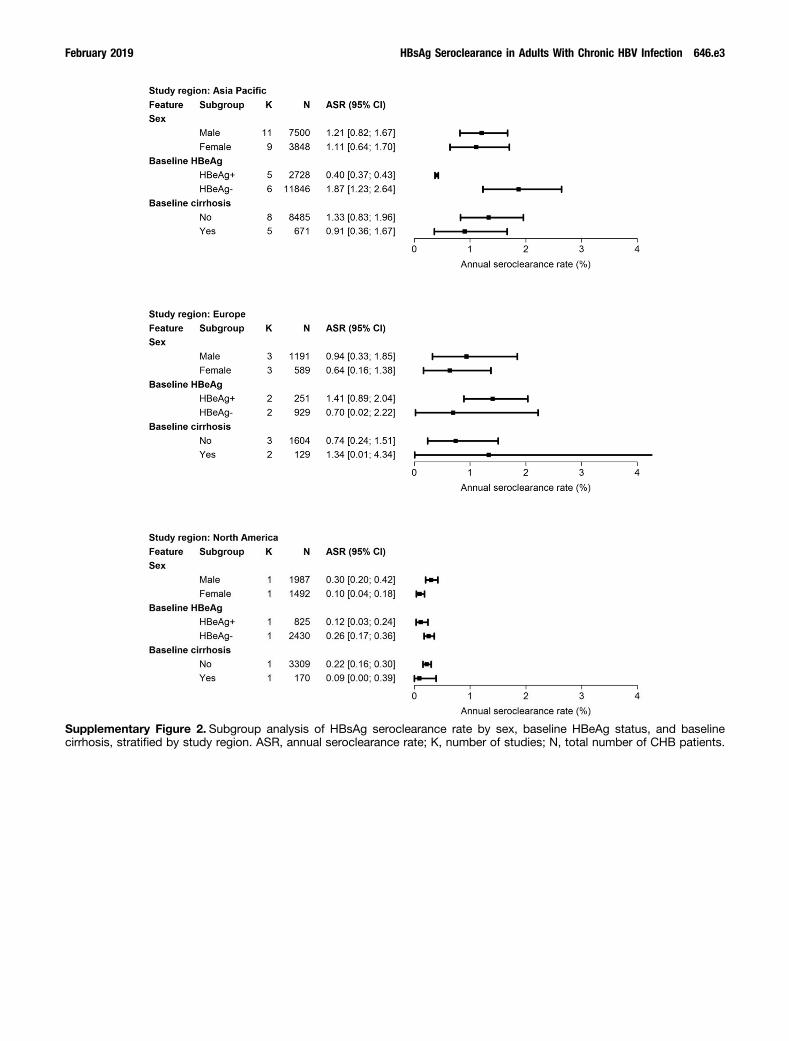
geographic region (Figure 6) and found that there was atrend toward differences in seroclearance rates (P frac14 06)with the Asia Pacific region (109 95 CI 081ndash142 23studies with 32866 patients) Europe (108 95 CI064ndash163 5 studies with 2364 patients) and the MiddleEast (105 95 CI 082ndash131 2 studies with 1826 pa-tients) having higher annual rates and North (050 95CI 015ndash104 3 studies with 4984 patients) and SouthAmerica (070 95 CI 050ndash094 1 study with 548 pa-tients) having lower rates However the difference acrossregions did not reach the conventional level of statisticalsignificance We performed additional subgroup analyses byregion and showed that HBsAg seroclearance rates inEurope (P frac14 977) and North America (P frac14 051) were notsignificantly different compared with that in the Asia Pacificregion when the results were stratified by subgroups
Figure 4 Subgroup anal-ysis of HBsAg seroclear-ance rate by sex baselineHBeAg status and base-line cirrhosis ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 641
CLINICAL
LIVE
R
(eg age HBeAg status cirrhosis HBV DNA study setting)(Supplementary Figures 2 and 3 and SupplementaryTable 3)
Regarding study settings and design the pooled HBsAgseroclearance rate was higher in population-based studies(168 95 CI 086ndash278) than health care servicendashbasedstudies (093 95 CI 072ndash117) but this difference wasnot statistically significant (P frac14 10) (Figure 6) Howeverheterogeneity was high (9874 for population-basedstudies 9670 for health care servicendashbased studies P lt01 for both) Similarly studies that collected data from acommunity-based health care servicendashbased population(134 95 CI 092ndash183) also had higher seroclearancerates than university-based studies (097 95 CI 078ndash118) although the difference again was not statisticallysignificant (P frac14 27)
HBsAg Seroclearance Rates in CHBPatients With Different HBV Genotypes andby Treatment History
There was no significant difference in HBsAg seroclear-ance across different genotypes among more than 10000patients with genotype data (331 patients with genotype A4685 with genotype B 5756 with genotype C 94 with ge-notype D and 231 with genotype F) (Supplementary
Figure 4) The annual seroclearance rates were 126(95 CI 029ndash285) 079 (95 CI 042ndash126) 102(95 CI 071ndash139) 105 (95 CI 043ndash193) and 059(95 CI 039ndash083) for genotypes A B C D and Frespectively Comparative analysis for the 2 largest groupsgenotypes B (n frac14 4685) and C (n frac14 5756) also found nosignificant difference between these 2 groups (P frac14 453) Inaddition there was no significant difference in HBsAgseroclearance between treated (n frac14 7565 082 95 CI034ndash150) and untreated (n frac14 20556 131 95 CI098ndash167) patients (P frac14 195) (Supplementary Figure 5)For the treated group we further subanalyzed HBsAgseroclearance rates by specific treatment regimen and founda higher rate in interferon-treated patients (1 study 3833person-years 180 95 CI 140ndash225) than in entecavir-treated patients (2 studies 1997 person-years 080 95CI 044ndash125) and lamivudine-treated patients (1 study5428 person-years 065 95 CI 045ndash089) There wereno data for patients treated by other nucleos(t)ideanalogues
Sensitivity AnalysisWe performed 5 sensitivity tests In the first we
excluded studies with a fair or high risk of bias (NOS scorelt 7) (Supplementary Figure 6A) The annual seroclearance
Figure 5 The baselinelaboratory data of CHBpatients categorized byachievement of HBsAgseroclearance Data werederived from articles thatprovided baseline resultsin patients who achievedand those who did notachieve HBsAg seroclear-ance during the follow-upperiod ASR annual sero-clearance rate K numberof studies N total numberof CHB patients qHBsAgquantitative hepatitis Bsurface antigen
Figure 6 Subgroup anal-ysis of HBsAg seroclear-ance rate by study regionscale of study and prac-tice settings ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
642 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
rate became higher (109 95 CI 082ndash141) but het-erogeneity remained high (I2 frac14 9770) In the secondsensitivity analysis we omitted 12 studies with smallersample size (n lt 500 patients) (Supplementary Figure 6B)Data from the remaining 22 larger studies showed anannual seroclearance rate of 100 (95 CI 073ndash132) butheterogeneity again remained high (I2 frac14 9830)
In the third sensitivity test to clarify whether thenonlinear increase of cumulative HBsAg seroclearance ratewas associated with the longer follow-up period in thepopulation-based cohort we performed a subgroup analysisand showed that the cumulative incident HBsAg seroclear-ance rates were indeed nonlinear in both population-basedand health care servicendashbased cohorts (SupplementaryFigure 7) In the fourth sensitivity test we subanalyzeddata for studies that confirmed HBsAg seroclearance byrepeated testing and excluded those that did not specifythis The pooled annual seroclearance rate remained similar(111 95 CI 085ndash139) (Supplementary Figure 8)Finally we excluded studies for which we imputed theannual HBsAg seroclearance rate and the pooled annualHBsAg seroclearance rate was 098 (95 CI 074ndash125)
Heterogeneity and Publication BiasThe heterogeneity of the HBsAg seroclearance rate was
severe as evidenced by the high I2 statistics in the pooledannual and 5- 10- and 15-year cumulative seroclearancerates (97 99 99 and 99 respectively)(Supplementary Table 2) Subgroup analysis also showedhigh heterogeneity However as presented by the Eggerrsquostest there was no publication bias in the pooled annualHBsAg seroclearance rates or any of the pooled cumulativeseroclearance rates (Supplementary Table 2)
DiscussionIn this meta-analysis of 34 studies which included
42588 CHB patients with 303754 person-years of follow-up we found that 3194 patients had an incident HBsAgseroclearance event resulting in a pooled HBsAg
seroclearance rate of 102 (95 CI 079ndash127) and con-firming that HBsAg is a rare event In addition by combiningthe published and updated aggregated data we determinedthe 5- 10- and 15-year cumulative seroclearance rates andfound that the rates of seroclearance increased 4-fold byyear 5 (403) further doubled by year 10 (816) anddoubled again by year 15 such that almost 18 of patientshad achieved seroclearance by year 15 after study entryOur finding is consistent with a prior report of a large-scaleprospective study by Chu et al6 in which the rate of HBsAgseroclearance increased in a nonlinear fashion from 81after the first 10 years to 249 after 20 years and to447 after 25 years of follow-up However the severeheterogeneity of our results requires that they be inter-preted with caution
Similar to other single-center studies we found thatpatients who were HBeAg negative at baseline had lowerbaseline HBV DNA levels and had lower quantitative HBsAgexperienced higher rates of HBsAg seroclearance793536
These characteristics are typical of the inactive carrierphase suggesting that these patients are better able tomount an immune response to the virus leading to virologicremission and over time spontaneous HBsAg seroclear-ance3337 Our analysis also confirmed findings of others thatlower baseline serum HBsAg levels predict HBsAg sero-clearance particularly if the HBsAg levels were lt100 IUmL33 Quantification of HBsAg has been adopted as animportant marker of immune control of CHB and has beensuggested to correlate with the covalently close circularDNA levels in the liver In addition a low HBsAg level isassociated with a lower risk of HCC and liver-related mor-tality among HBeAg-negative patients with low viremia38
Although the finding of an association between HBsAglevel and HBsAg seroclearance is a self-fulfilling prophecybecause the level has to decrease before it becomes unde-tectable this has implications for the design of clinical trialsaimed at HBV cure in that randomization must be stratifiedby baseline HBsAg levels
Furthermore we were able to provide pooled HBsAgseroclearance rates for CHB patients from different
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
WHAT YOU NEED TO KNOW
636 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
See editorial on page 548
BACKGROUND AND CONTEXT
Functional cure of HBV infection is defined based onHBsAg seroclearance but reported annual rates ofHBsAg seroclearance vary
NEW FINDINGS
In a meta-analysis of 42588 patients in 34 studies thepooled annual rate of HBsAg seroclearance was 102which increased to 1799 after 15 years Testingnegative for HBeAg and low level of HBV DNA orHBsAg level at baseline were associated with higherrates of HBsAg seroclearance
LIMITATIONS
This was a meta-analysis and there was a high level ofheterogeneity in pooled rates among studies
IMPACT
The findings identify annual rate and factors associatedwith HBsAg seroclearance indicate the need for life-longtreatment for most patients These factors might beconsidered in balancing treatment groups for clinicaltrials of agents designed to cure HBV infection
BACKGROUND amp AIMS Seroclearance of hepatitis B surfaceantigen (HBsAg) is a marker for clearance of chronic hepatitis Bvirus (HBV) infection but reported annual incidence rates ofHBsAg seroclearance vary We performed a systematic reviewand meta-analysis to provide more precise estimates of HBsAgseroclearance rates among subgroups and populationsMETHODS We searched PubMed Embase and the Cochranelibrary for cohort studies that reported HBsAg seroclearance inadults with chronic HBV infection with more than 1 year offollow-up and at least 1 repeat test for HBsAg Annual and 5-10- and 15-year cumulative incidence rates were pooled usinga random effects model RESULTS We analyzed 34 publishedstudies (with 42588 patients 303754 person-years of follow-up and 3194 HBsAg seroclearance events) including additionaland updated aggregated data from 19 studies The pooledannual rate of HBsAg seroclearance was 102 (95 CI 079ndash127) Cumulative incidence rates were 403 at 5 years (95CI 249ndash593) 816 at 10 years (95 CI 524ndash1172) and1799 at 15 years (95 CI 618ndash2324) There were no sig-nificant differences between the sexes A higher proportion ofpatients who tested negative for HBeAg at baseline had sero-clearance (133 95 CI 076ndash205) than those who testedpositive for HBeAg (040 95 CI 025ndash059) (P lt 01)Having HBsAg seroclearance was also associated with a lowerbaseline HBV DNA level (661 log10 IUmL 95 CI 594ndash727)vs not having HBsAg seroclearance (771 log10 IUmL 95 CI741ndash802) (P lt 01) and with a lower level of HBsAg atbaseline (274 log10 IUmL 95 CI 188ndash360) vs not havingHBsAg seroclearance (390 log10 IUmL 95 CI 373ndash406)(P lt 01) HBsAg seroclearance was not associated with HBVgenotype or treatment history Heterogeneity was substantialacross the studies (I2 frac14 9749) CONCLUSION In a systematicreview and meta-analysis we found a low rate of HBsAgseroclearance in untreated and treated patients (pooled annualrate approximately 1) Seroclearance occurred mainly inpatients with less active disease Patients with chronic HBVinfection should therefore be counseled on the need for lifelongtreatment and curative therapies are needed
Keywords Natural History Prognosis Disease ProgressionCHB
hronic hepatitis B (CHB) is a significant public health
Abbreviations used in this paper ALT alanine aminotransferase cccDNAcovalently closed circular DNA CHB chronic hepatitis B CI confidenceinterval HBeAg hepatitis B e antigen HBsAg hepatitis B surface antigenHBV hepatitis B virus HCC hepatocellular carcinoma NOS NewcastlendashOttawa quality assessment scale
Most current article
copy 2019 by the AGA Institute0016-5085$3600
httpsdoiorg101053jgastro201810027
Cproblem affecting approximately 257 million peopleglobally1 Patients who are chronically infected with hepatitisB virus (HBV) are at greater risk of developing cirrhosis andhepatocellular carcinoma (HCC) Because the development ofthese complications may take decades to present virologicmarkers such as hepatitis B e antigen (HBeAg) status serumHBV DNA alanine aminotransferase (ALT) levels and quan-titative hepatitis B surface antigen (HBsAg) are used todetermine the status of CHB and to predict prognosis
A sterilizing cure for CHB is not possible because of thepresence of integrated HBV DNA and the long half-life ofcovalently closed circular DNA (cccDNA) Therefore thetherapeutic goal for new treatments of CHB is to achieve
functional cure that is HBsAg seroclearance2 HBsAg sero-clearance signifies sustained immune control of HBV and isassociated with improved clinical outcomes with a lowerrisk of decompensated cirrhosis HCC and liver-relateddeath3ndash5 HBsAg seroclearance can occur spontaneouslybut the reported rates have been variable Prior cohortstudies showed that the annual HBsAg seroclearance ratecan range from a low of 012 to a high of 2386ndash8 and isaffected by a myriad of patient characteristics such as sexage cirrhosis HBeAg status HBV DNA level and serumHBsAg level69 In addition reported rates of HBsAg sero-clearance with currently available treatments are low2
Because HBsAg seroclearance is a rare event that isaffected by a variety of host and viral factors determining anaccurate incidence rate and the predictors for HBsAg sero-clearance has been difficult Therefore using a systematicreview and meta-analysis of multiple cohorts from differentgeographic regions we aimed to provide more precise esti-mates of HBsAg seroclearance rates among different sub-groups and populations that can then be usedwhen discussingtreatment decisions with patients In addition these estimatesmay assist with the development of new therapeutic agents
MethodsThis study was performed and presented according to the
Preferred Reporting Items for Systematic Reviews and
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 637
CLINICAL
LIVE
R
Meta-analyses (ie PRISMA) guidelines10 The protocol of thisstudy is available online at PROSPERO (CRD42017079843)
Search Strategy and Study SelectionElectronic searches were performed in PubMed Embase and
the Cochrane library from the inception of the database to July 52017 by using various combinations of the keywords HBVinfection HBsAg seroclearance and cohort studies (see supple-mentary data for search strategies) In addition we manuallysearched the bibliography of the included articles and relevantsystematic reviews for additional articles No language restric-tion was imposed All literature searches reviews and selectionswere independently performed by 2 authors Discrepancies wereresolved through consultation with a third author
Cohort studies that reported HBsAg seroclearance in adultpatients (gt18 years old) with CHB (HBsAg andor HBV DNApositive for more than 6 months) with more than 1-year follow-up and at least 1 repeat test for HBsAg were included Bothpopulation-based cohorts and hospital- or clinic-based cohortswere included There was no restriction on treatment history
Studies that were clinical trials cross-sectional studies caseseries and case reports were excluded Given the rarity ofHBsAg seroclearance events studies with less than 200 pa-tients were also excluded Finally to enhance the homogeneityof the included studies we excluded patients with human im-munodeficiency virus hepatitis D virus or hepatitis C virus co-infection and patients with prior HCC
Data ExtractionTwo authors independently extracted the following data
from each study using a standardized data extraction formfollow-up period (person-years) baseline characteristics ofpatients at entry (age sex raceethnicity history of HBVtreatment HBeAg HBV genotype ALT level platelet count HBVDNA and cirrhosis status) and outcomes (annual HBsAgseroclearance rate cumulative seroclearance rates subsequentliver transplantation HCC and death) For articles that did notreport the annual HBsAg seroclearance rate we estimated it byusing the following formula
number of patients with HBsAg seroclearancemean follow up duration frac12years total number of patients
We estimated person-years of follow-up by dividing thenumber of patients with seroclearance by the annual sero-clearance rate in articles that did not report person-years offollow-up Any discrepancies were resolved in consultationwith a third reviewer
Corresponding authors of eligible studies were contacted formissing data andor updated aggregated data for primaryoutcome and subgroup analyses if additional follow-up data of thepublished cohorts were available To avoid overlapped patientswe also contacted the authors to request the data of the entirecohort if there were multiple articles published from that cohort
Risk-of-Bias AssessmentWe used a risk-of-bias tool modified from the Newcastlendash
Ottawa quality assessment scale (NOS) to assess the qualityof individual reports11 The NOS is a scoring tool comprising8 items with 9 scores that assesses how well the investigators
selected their participants (score ranges from 0 to 4) howcomparable their results may be (score ranges from 0 to 2) andhow applicable the outcomes are (score ranges from 0 to 3)The higher the score the better the quality of the study and thelower the risk of bias We categorized the studies as goodquality if the total score was 7 or more fair if the score was 4ndash6 and poor if the score was lt4
OutcomesThe prespecified primary outcomes were the annual rate
and cumulative seroclearance rate of HBsAg seroclearance at 510 and 15 years HBsAg seroclearance was defined as havingnegative HBsAg test results in patients with previously positiveresults The secondary outcome was the distribution of annualHBsAg seroclearance in patients with different demographicand clinical characteristics (geographic regions HBV genotypesHBeAg status presence of cirrhosis treatment history andother clinical characteristics) For analysis by treatment historywe selected studies that included only untreated patients whoalso remained untreated throughout the study period for theuntreated group and we selected studies that included onlypatients who were treatment naiumlve and initiated therapy atstudy entry for the treated group
Statistical AnalysisAnnual HBsAg seroclearance rate and 5- 10- 15-year cu-
mulative incidence rates were pooled using the random effectsmodel of DerSimonian and Laird12 Because the values of theseestimates can be close to 0 we used the FreemanndashTukeytransformation to stabilize the variance and the Wilson scoremethod to generate 95 confidence intervals (CIs)13 Theresulting values were then back-transformed and are presentedas a percentage14 Heterogeneity across studies was assessedby I2 statistics and Cochranrsquos Q test15 The Eggerrsquos test was usedto evaluate small study bias quantitatively
We performed subgroup analyses to examine whether theannual HBsAg seroclearance rates were modified by the pre-planned variables including study locationregion (becauseethnicity data were difficult to discern) study settings (popula-tion based vs health care service based) mean age sex baselinecirrhosis HBeAg positivity and HBV genotype We calculated theannual seroclearance rates of the aforementioned subgroup an-alyses only in studies that provided us with original dataFurthermore we pooled the mean value of key clinical parame-ters (ALT platelet count HBV DNA and quantitative HBsAg level)to determine differences in baseline laboratory values betweenpatients with and without incident HBsAg seroclearance We alsoperformed a sensitivity analysis by excluding studies with a highrisk of bias and studies with sample sizes lt500
We set 05 as the threshold of statistical significance for theP value (2-tailed) All analyses were conducted using the metapackage of R software version 33216 Metarate was used tocompute the pooled estimate of both the annual and cumulativeHBsAg seroclearance rates and metamean was used to pool themean values of various baseline laboratory data
ResultsFrom the electronic and manual search 4833 records
were identified (Figure 1) After removing duplicates and
638 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
screening the titles and abstracts 180 potentially eligiblestudies were retrieved for full-text reviews After review atotal of 34 articles (42588 CHB patients) met our inclusionand exclusion criteria and were included in the meta-analysis We received updated aggregated data from 19 ofthe 34 studies717ndash34 including 3 studies from 1 center(Toranomon Hospital Tokyo Japan) but we contacted thestudy authors and confirmed that only nonduplicate pa-tients were included in our meta-analysis192031
Characteristics of Included StudiesTable 1 shows the characteristics of included studies and
of the participants CHB patients from 14 countries wereincluded with the majority from the Asia Pacific region (23studies) Four studies were population based and the restwere conducted with data derived from hospitals or healthcare centers The sample sizes of the included studiesranged from 217 to 6621 with the proportion of malesranging from 444 to 903 The mean age ranged from342 to 50 years Twenty-two out of 34 studies showed lowrisk of bias (Supplementary Table 1)
Overall Annual Seroclearance and CumulativeIncidence
Among the 42588 CHB patients 3194 patients experi-enced HBsAg seroclearance The annual seroclearance ratesranged from 015 to 302 with a pooled rate of 102
Figure 1 Preferred Reporting Items for Systematic Reviewsand Meta-analyses (PRISMA) flow chart of article selection
(95 CI 079ndash127) and high heterogeneity (I2 frac14 9749)(Figure 2) The pooled 5- 10- and 15-year cumulativeincidence rates were nonlinear at 403 (95 CI 246ndash597 I2 frac14 9957) 816 (95 CI 519ndash1179 I2 frac149976) and 1799 (95 CI 1083ndash2696 I2 frac14 9991)respectively (Figure 3 and Supplementary Table 2)
Annual Seroclearance Rate by BaselineDemographic and Clinical Characteristics
The pooled annual seroclearance rates for male (n frac1411142) and female (n frac14 6080) patients were 113 (95CI 078ndash155) and 087 (95 CI 049ndash136) respectivelybut the difference was not statistically significant (P frac14 43)(Figure 4) The mean age of the study cohort was 45 andthe pooled annual seroclearance rates were similar forstudies with a mean age less than 45 years (095 95 CI069ndash126) compared with studies with a mean age of 45years and older (112 95 CI 040ndash220) (SupplementaryFigure 1) Analyses by patients of specific age groups andraceethnicity were not performed because of lack of pri-mary data with most studies not reporting data by agegroups and many studies of mixed racesethnicities notreporting results stratified by raceethnicity
There were 9 studies that separately reported theannual seroclearance rate in patients who were HBeAgpositive (n frac14 3922) and those who were HBeAg negative(n frac14 15205) at baseline (Figure 4) Patients who wereHBeAg negative (133 95 CI 076ndash205) had almost a33 times higher HBsAg seroclearance rate than patientswho were HBeAg positive (040 95 CI 025ndash059)There were no significant differences in the annual sero-clearance rates between patients with cirrhosis (08495 CI 031ndash158 n frac14 970) and those without cirrhosis(104 95 CI 063ndash155 n frac14 13398) (P frac14 74)
Baseline Laboratory Parameters in PatientsWith HBsAg Seroclearance vs Those WithoutHBsAg Seroclearance
We investigated several baseline laboratory data that havebeen reported to have an association with HBsAg seroclear-ance (Figure 5) From 5 studies with quantitative HBsAg leveldata (1173 with incident HBsAg seroclearance 6246 without)the pooled mean quantitative HBsAg level was found to besignificantly lower among patients with HBsAg seroclearancecompared with those without seroclearance (274 log10 IUmL 95 CI 187ndash360 vs 390 log10 IUmL 95 CI 373ndash406 P lt 01) From 10 studies with HBV DNA data (1431with incident HBsAg seroclearance 16590 without) patientswith HBsAg seroclearance also showed a significantly lowerbaseline HBV DNA than those with no seroclearance (661log10 IUmL 95 CI 594ndash727 vs 771 log10 IUmL 95 CI741ndash802 P lt 01) In 16 studies with ALT data the pooledmean ALT levels among 1663 patients with and 14974without HBsAg seroclearance were not statistically different(64 UL 95 CI 27ndash150 vs 58 UL 95 CI 19ndash178 P frac1490) The pooled mean platelet count among 822 patients withand 9536 patients without HBsAg seroclearance in 10 studieswas also not statistically different (195 109L 95 CI
Table 1Characteristics of the Included Studies and Patients
Year and First Authora Region Settings Cohort TypePatients
n MaleMeanAge y
HBeAg(thorn)at Entry
Cirrhosisat Entry
IncidentHBsAg
Seroclearance
AnnualSeroclearance
Rate 5-yearCSR
10-yearCSR
15-yearCSR
2014 Kobayashi20 Asia Pacific Community Health care service 1130 705 405 81 273 200 163 9 18 262013 Hosaka19 Asia Pacific Community Health care service 791 627 43 442 169 38 070 24 8 182011 Suzuki31 Asia Pacific Community Health care service 615 464 35b 414 72 69 181 65 15 352016 Charatcharoenwi-
tthaya17Asia Pacific Mixed Health care service 233 172 416 135 22 7 229 mdash mdash mdash
2013 Treeprasertsuk25 Asia Pacific Academic Health care service 431 310 434 262 0 2 015 mdash mdash mdash
2015 Lauret22 Europe Academic Health care service 614 391 371 139 52 78 141 44 118 2172017 Riveiro-Barciela30 Europe Mixed Health care service 633 459 496 77 42 9 041 182 253 mdash
2016 Park28 Asia Pacific Academic Health care service 954 627 433 mdash mdash 75 105 365 903 25482014 Preda29 Europe Mixed Health care service 533 340 415 mdash 43 7 087 mdash mdash mdash
2015 Tseng33 Asia Pacific Academic Health care service 2686 1631 414 0 0 381 095 273 676 12392014 Fung18 Asia Pacific Academic Health care service 775 483 362 0 mdash 60 052 131 333 7192017 Ungtrakul34 Asia Pacific Academic Health care service 297 132 415 0 0 15 237 mdash mdash mdash
2016 Nguyen26 North America Mixed Health care service 3479 1987 443 1096 202 37 021 09 292 4252010 Liu7 Asia Pacific Community Population based 3302 1994 461 482 0 568 213 742 1732 36772011 Kwak21 Asia Pacific Academic Health care service 714 476 477 0 mdash 41 181 977 mdash mdash
2013 Luo24 Asia Pacific Academic Health care service 217 196 407 113 74 9 081 417 711 mdash
2015 Yapali44 North America Academic Health care service 234 122 35b 44 mdash 9 080 mdash mdash mdash
2002 Sanchez-Tapias8 Europe Academic Health care service 269 218 36 173 21 29 139 mdash mdash mdash
2015 Habersetzer45 Europe Academic Health care service 315 211 35b 69 mdash 29 158 mdash mdash mdash
2014 Farzi46 Middle East Community Health care service 399 231 356 0 0 48 122 mdash mdash mdash
2012 Arai47 Asia Pacific Academic Health care service 423 239 405 183 mdash 25 097 mdash mdash mdash
2005 Ahn48 Asia Pacific Academic Health care service 432 mdash mdash 0 mdash 49 046 mdash mdash mdash
2014 Ferreira49 South America Academic Health care service 548 336 377 mdash mdash 40 056 mdash mdash mdash
2016 Han50 Asia Pacific mdash Population based 634 485 486 0 0 117 302 mdash mdash mdash
2010 Simonetti36 North America Community Population based 1271 mdash 209b mdash mdash 158 065 mdash mdash mdash
2014 Kim9 Asia Pacific mdash Health care service 5409 3699 449 3601 2684 110 032 mdash mdash mdash
2016 Nagaoka51 Asia Pacific Academic Health care service 392 278 395b 285 111 50 091 mdash 54 982015 Orito27 Asia Pacific Academic Health care service 602 381 52b 295 110 13 030 mdash mdash mdash
2010 Tai32 Asia Pacific Mixed Health care service 6621 3761 342 1386 0 555 171 mdash mdash mdash
2016 Ari52 Middle East mdash Health care service 1427 767 371 48 mdash 84 104 mdash mdash mdash
2007 Nam53 Asia Pacific mdash Health care service 4061 2639 500 1584 893 47 036 mdash mdash mdash
2011 Lu54 Asia Pacific Academic Health care service 220 156 mdash 168 25 17 159 mdash mdash mdash
1998 Huo55 Asia Pacific Community Health care service 1355 1113 41 mdash mdash 58 157 mdash mdash mdash
2015 Lim23 Asia Pacific Community Population based 572 359 mdash 234 mdash 145 130 mdash mdash mdash
CSR cumulative seroclearance rateaTable 1 referencesbMedian age
February2019
HBsAgSeroclearance
inAdults
With
ChronicHBV
Infection639
CLINICAL LIVER
Figure 2 Pooled annualHBsAg seroclearance rateof chronic hepatitis B pa-tients Annual HBsAgseroclearance rates werecombined using a randomeffects model The size ofeach square representsthe weight of that studyThe vertical dotted linerepresents the pooledrate See Table 1 for fullcitation details for thestudies ASR annualseroclearance rate SPnumber of patients whohave achieved HBsAgseroclearance
Figure 3 Pooled 5- 10- and 15-year cumulative incidencerates of HBsAg seroclearance
640 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
183 109ndash208 109 vs 196 109L 95 CI 182 109ndash210 109 P frac14 95)
Region Scale and Setting of StudiesWe stratified the pooled HBsAg seroclearance rates by
geographic region (Figure 6) and found that there was atrend toward differences in seroclearance rates (P frac14 06)with the Asia Pacific region (109 95 CI 081ndash142 23studies with 32866 patients) Europe (108 95 CI064ndash163 5 studies with 2364 patients) and the MiddleEast (105 95 CI 082ndash131 2 studies with 1826 pa-tients) having higher annual rates and North (050 95CI 015ndash104 3 studies with 4984 patients) and SouthAmerica (070 95 CI 050ndash094 1 study with 548 pa-tients) having lower rates However the difference acrossregions did not reach the conventional level of statisticalsignificance We performed additional subgroup analyses byregion and showed that HBsAg seroclearance rates inEurope (P frac14 977) and North America (P frac14 051) were notsignificantly different compared with that in the Asia Pacificregion when the results were stratified by subgroups
Figure 4 Subgroup anal-ysis of HBsAg seroclear-ance rate by sex baselineHBeAg status and base-line cirrhosis ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 641
CLINICAL
LIVE
R
(eg age HBeAg status cirrhosis HBV DNA study setting)(Supplementary Figures 2 and 3 and SupplementaryTable 3)
Regarding study settings and design the pooled HBsAgseroclearance rate was higher in population-based studies(168 95 CI 086ndash278) than health care servicendashbasedstudies (093 95 CI 072ndash117) but this difference wasnot statistically significant (P frac14 10) (Figure 6) Howeverheterogeneity was high (9874 for population-basedstudies 9670 for health care servicendashbased studies P lt01 for both) Similarly studies that collected data from acommunity-based health care servicendashbased population(134 95 CI 092ndash183) also had higher seroclearancerates than university-based studies (097 95 CI 078ndash118) although the difference again was not statisticallysignificant (P frac14 27)
HBsAg Seroclearance Rates in CHBPatients With Different HBV Genotypes andby Treatment History
There was no significant difference in HBsAg seroclear-ance across different genotypes among more than 10000patients with genotype data (331 patients with genotype A4685 with genotype B 5756 with genotype C 94 with ge-notype D and 231 with genotype F) (Supplementary
Figure 4) The annual seroclearance rates were 126(95 CI 029ndash285) 079 (95 CI 042ndash126) 102(95 CI 071ndash139) 105 (95 CI 043ndash193) and 059(95 CI 039ndash083) for genotypes A B C D and Frespectively Comparative analysis for the 2 largest groupsgenotypes B (n frac14 4685) and C (n frac14 5756) also found nosignificant difference between these 2 groups (P frac14 453) Inaddition there was no significant difference in HBsAgseroclearance between treated (n frac14 7565 082 95 CI034ndash150) and untreated (n frac14 20556 131 95 CI098ndash167) patients (P frac14 195) (Supplementary Figure 5)For the treated group we further subanalyzed HBsAgseroclearance rates by specific treatment regimen and founda higher rate in interferon-treated patients (1 study 3833person-years 180 95 CI 140ndash225) than in entecavir-treated patients (2 studies 1997 person-years 080 95CI 044ndash125) and lamivudine-treated patients (1 study5428 person-years 065 95 CI 045ndash089) There wereno data for patients treated by other nucleos(t)ideanalogues
Sensitivity AnalysisWe performed 5 sensitivity tests In the first we
excluded studies with a fair or high risk of bias (NOS scorelt 7) (Supplementary Figure 6A) The annual seroclearance
Figure 5 The baselinelaboratory data of CHBpatients categorized byachievement of HBsAgseroclearance Data werederived from articles thatprovided baseline resultsin patients who achievedand those who did notachieve HBsAg seroclear-ance during the follow-upperiod ASR annual sero-clearance rate K numberof studies N total numberof CHB patients qHBsAgquantitative hepatitis Bsurface antigen
Figure 6 Subgroup anal-ysis of HBsAg seroclear-ance rate by study regionscale of study and prac-tice settings ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
642 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
rate became higher (109 95 CI 082ndash141) but het-erogeneity remained high (I2 frac14 9770) In the secondsensitivity analysis we omitted 12 studies with smallersample size (n lt 500 patients) (Supplementary Figure 6B)Data from the remaining 22 larger studies showed anannual seroclearance rate of 100 (95 CI 073ndash132) butheterogeneity again remained high (I2 frac14 9830)
In the third sensitivity test to clarify whether thenonlinear increase of cumulative HBsAg seroclearance ratewas associated with the longer follow-up period in thepopulation-based cohort we performed a subgroup analysisand showed that the cumulative incident HBsAg seroclear-ance rates were indeed nonlinear in both population-basedand health care servicendashbased cohorts (SupplementaryFigure 7) In the fourth sensitivity test we subanalyzeddata for studies that confirmed HBsAg seroclearance byrepeated testing and excluded those that did not specifythis The pooled annual seroclearance rate remained similar(111 95 CI 085ndash139) (Supplementary Figure 8)Finally we excluded studies for which we imputed theannual HBsAg seroclearance rate and the pooled annualHBsAg seroclearance rate was 098 (95 CI 074ndash125)
Heterogeneity and Publication BiasThe heterogeneity of the HBsAg seroclearance rate was
severe as evidenced by the high I2 statistics in the pooledannual and 5- 10- and 15-year cumulative seroclearancerates (97 99 99 and 99 respectively)(Supplementary Table 2) Subgroup analysis also showedhigh heterogeneity However as presented by the Eggerrsquostest there was no publication bias in the pooled annualHBsAg seroclearance rates or any of the pooled cumulativeseroclearance rates (Supplementary Table 2)
DiscussionIn this meta-analysis of 34 studies which included
42588 CHB patients with 303754 person-years of follow-up we found that 3194 patients had an incident HBsAgseroclearance event resulting in a pooled HBsAg
seroclearance rate of 102 (95 CI 079ndash127) and con-firming that HBsAg is a rare event In addition by combiningthe published and updated aggregated data we determinedthe 5- 10- and 15-year cumulative seroclearance rates andfound that the rates of seroclearance increased 4-fold byyear 5 (403) further doubled by year 10 (816) anddoubled again by year 15 such that almost 18 of patientshad achieved seroclearance by year 15 after study entryOur finding is consistent with a prior report of a large-scaleprospective study by Chu et al6 in which the rate of HBsAgseroclearance increased in a nonlinear fashion from 81after the first 10 years to 249 after 20 years and to447 after 25 years of follow-up However the severeheterogeneity of our results requires that they be inter-preted with caution
Similar to other single-center studies we found thatpatients who were HBeAg negative at baseline had lowerbaseline HBV DNA levels and had lower quantitative HBsAgexperienced higher rates of HBsAg seroclearance793536
These characteristics are typical of the inactive carrierphase suggesting that these patients are better able tomount an immune response to the virus leading to virologicremission and over time spontaneous HBsAg seroclear-ance3337 Our analysis also confirmed findings of others thatlower baseline serum HBsAg levels predict HBsAg sero-clearance particularly if the HBsAg levels were lt100 IUmL33 Quantification of HBsAg has been adopted as animportant marker of immune control of CHB and has beensuggested to correlate with the covalently close circularDNA levels in the liver In addition a low HBsAg level isassociated with a lower risk of HCC and liver-related mor-tality among HBeAg-negative patients with low viremia38
Although the finding of an association between HBsAglevel and HBsAg seroclearance is a self-fulfilling prophecybecause the level has to decrease before it becomes unde-tectable this has implications for the design of clinical trialsaimed at HBV cure in that randomization must be stratifiedby baseline HBsAg levels
Furthermore we were able to provide pooled HBsAgseroclearance rates for CHB patients from different
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 637
CLINICAL
LIVE
R
Meta-analyses (ie PRISMA) guidelines10 The protocol of thisstudy is available online at PROSPERO (CRD42017079843)
Search Strategy and Study SelectionElectronic searches were performed in PubMed Embase and
the Cochrane library from the inception of the database to July 52017 by using various combinations of the keywords HBVinfection HBsAg seroclearance and cohort studies (see supple-mentary data for search strategies) In addition we manuallysearched the bibliography of the included articles and relevantsystematic reviews for additional articles No language restric-tion was imposed All literature searches reviews and selectionswere independently performed by 2 authors Discrepancies wereresolved through consultation with a third author
Cohort studies that reported HBsAg seroclearance in adultpatients (gt18 years old) with CHB (HBsAg andor HBV DNApositive for more than 6 months) with more than 1-year follow-up and at least 1 repeat test for HBsAg were included Bothpopulation-based cohorts and hospital- or clinic-based cohortswere included There was no restriction on treatment history
Studies that were clinical trials cross-sectional studies caseseries and case reports were excluded Given the rarity ofHBsAg seroclearance events studies with less than 200 pa-tients were also excluded Finally to enhance the homogeneityof the included studies we excluded patients with human im-munodeficiency virus hepatitis D virus or hepatitis C virus co-infection and patients with prior HCC
Data ExtractionTwo authors independently extracted the following data
from each study using a standardized data extraction formfollow-up period (person-years) baseline characteristics ofpatients at entry (age sex raceethnicity history of HBVtreatment HBeAg HBV genotype ALT level platelet count HBVDNA and cirrhosis status) and outcomes (annual HBsAgseroclearance rate cumulative seroclearance rates subsequentliver transplantation HCC and death) For articles that did notreport the annual HBsAg seroclearance rate we estimated it byusing the following formula
number of patients with HBsAg seroclearancemean follow up duration frac12years total number of patients
We estimated person-years of follow-up by dividing thenumber of patients with seroclearance by the annual sero-clearance rate in articles that did not report person-years offollow-up Any discrepancies were resolved in consultationwith a third reviewer
Corresponding authors of eligible studies were contacted formissing data andor updated aggregated data for primaryoutcome and subgroup analyses if additional follow-up data of thepublished cohorts were available To avoid overlapped patientswe also contacted the authors to request the data of the entirecohort if there were multiple articles published from that cohort
Risk-of-Bias AssessmentWe used a risk-of-bias tool modified from the Newcastlendash
Ottawa quality assessment scale (NOS) to assess the qualityof individual reports11 The NOS is a scoring tool comprising8 items with 9 scores that assesses how well the investigators
selected their participants (score ranges from 0 to 4) howcomparable their results may be (score ranges from 0 to 2) andhow applicable the outcomes are (score ranges from 0 to 3)The higher the score the better the quality of the study and thelower the risk of bias We categorized the studies as goodquality if the total score was 7 or more fair if the score was 4ndash6 and poor if the score was lt4
OutcomesThe prespecified primary outcomes were the annual rate
and cumulative seroclearance rate of HBsAg seroclearance at 510 and 15 years HBsAg seroclearance was defined as havingnegative HBsAg test results in patients with previously positiveresults The secondary outcome was the distribution of annualHBsAg seroclearance in patients with different demographicand clinical characteristics (geographic regions HBV genotypesHBeAg status presence of cirrhosis treatment history andother clinical characteristics) For analysis by treatment historywe selected studies that included only untreated patients whoalso remained untreated throughout the study period for theuntreated group and we selected studies that included onlypatients who were treatment naiumlve and initiated therapy atstudy entry for the treated group
Statistical AnalysisAnnual HBsAg seroclearance rate and 5- 10- 15-year cu-
mulative incidence rates were pooled using the random effectsmodel of DerSimonian and Laird12 Because the values of theseestimates can be close to 0 we used the FreemanndashTukeytransformation to stabilize the variance and the Wilson scoremethod to generate 95 confidence intervals (CIs)13 Theresulting values were then back-transformed and are presentedas a percentage14 Heterogeneity across studies was assessedby I2 statistics and Cochranrsquos Q test15 The Eggerrsquos test was usedto evaluate small study bias quantitatively
We performed subgroup analyses to examine whether theannual HBsAg seroclearance rates were modified by the pre-planned variables including study locationregion (becauseethnicity data were difficult to discern) study settings (popula-tion based vs health care service based) mean age sex baselinecirrhosis HBeAg positivity and HBV genotype We calculated theannual seroclearance rates of the aforementioned subgroup an-alyses only in studies that provided us with original dataFurthermore we pooled the mean value of key clinical parame-ters (ALT platelet count HBV DNA and quantitative HBsAg level)to determine differences in baseline laboratory values betweenpatients with and without incident HBsAg seroclearance We alsoperformed a sensitivity analysis by excluding studies with a highrisk of bias and studies with sample sizes lt500
We set 05 as the threshold of statistical significance for theP value (2-tailed) All analyses were conducted using the metapackage of R software version 33216 Metarate was used tocompute the pooled estimate of both the annual and cumulativeHBsAg seroclearance rates and metamean was used to pool themean values of various baseline laboratory data
ResultsFrom the electronic and manual search 4833 records
were identified (Figure 1) After removing duplicates and
638 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
screening the titles and abstracts 180 potentially eligiblestudies were retrieved for full-text reviews After review atotal of 34 articles (42588 CHB patients) met our inclusionand exclusion criteria and were included in the meta-analysis We received updated aggregated data from 19 ofthe 34 studies717ndash34 including 3 studies from 1 center(Toranomon Hospital Tokyo Japan) but we contacted thestudy authors and confirmed that only nonduplicate pa-tients were included in our meta-analysis192031
Characteristics of Included StudiesTable 1 shows the characteristics of included studies and
of the participants CHB patients from 14 countries wereincluded with the majority from the Asia Pacific region (23studies) Four studies were population based and the restwere conducted with data derived from hospitals or healthcare centers The sample sizes of the included studiesranged from 217 to 6621 with the proportion of malesranging from 444 to 903 The mean age ranged from342 to 50 years Twenty-two out of 34 studies showed lowrisk of bias (Supplementary Table 1)
Overall Annual Seroclearance and CumulativeIncidence
Among the 42588 CHB patients 3194 patients experi-enced HBsAg seroclearance The annual seroclearance ratesranged from 015 to 302 with a pooled rate of 102
Figure 1 Preferred Reporting Items for Systematic Reviewsand Meta-analyses (PRISMA) flow chart of article selection
(95 CI 079ndash127) and high heterogeneity (I2 frac14 9749)(Figure 2) The pooled 5- 10- and 15-year cumulativeincidence rates were nonlinear at 403 (95 CI 246ndash597 I2 frac14 9957) 816 (95 CI 519ndash1179 I2 frac149976) and 1799 (95 CI 1083ndash2696 I2 frac14 9991)respectively (Figure 3 and Supplementary Table 2)
Annual Seroclearance Rate by BaselineDemographic and Clinical Characteristics
The pooled annual seroclearance rates for male (n frac1411142) and female (n frac14 6080) patients were 113 (95CI 078ndash155) and 087 (95 CI 049ndash136) respectivelybut the difference was not statistically significant (P frac14 43)(Figure 4) The mean age of the study cohort was 45 andthe pooled annual seroclearance rates were similar forstudies with a mean age less than 45 years (095 95 CI069ndash126) compared with studies with a mean age of 45years and older (112 95 CI 040ndash220) (SupplementaryFigure 1) Analyses by patients of specific age groups andraceethnicity were not performed because of lack of pri-mary data with most studies not reporting data by agegroups and many studies of mixed racesethnicities notreporting results stratified by raceethnicity
There were 9 studies that separately reported theannual seroclearance rate in patients who were HBeAgpositive (n frac14 3922) and those who were HBeAg negative(n frac14 15205) at baseline (Figure 4) Patients who wereHBeAg negative (133 95 CI 076ndash205) had almost a33 times higher HBsAg seroclearance rate than patientswho were HBeAg positive (040 95 CI 025ndash059)There were no significant differences in the annual sero-clearance rates between patients with cirrhosis (08495 CI 031ndash158 n frac14 970) and those without cirrhosis(104 95 CI 063ndash155 n frac14 13398) (P frac14 74)
Baseline Laboratory Parameters in PatientsWith HBsAg Seroclearance vs Those WithoutHBsAg Seroclearance
We investigated several baseline laboratory data that havebeen reported to have an association with HBsAg seroclear-ance (Figure 5) From 5 studies with quantitative HBsAg leveldata (1173 with incident HBsAg seroclearance 6246 without)the pooled mean quantitative HBsAg level was found to besignificantly lower among patients with HBsAg seroclearancecompared with those without seroclearance (274 log10 IUmL 95 CI 187ndash360 vs 390 log10 IUmL 95 CI 373ndash406 P lt 01) From 10 studies with HBV DNA data (1431with incident HBsAg seroclearance 16590 without) patientswith HBsAg seroclearance also showed a significantly lowerbaseline HBV DNA than those with no seroclearance (661log10 IUmL 95 CI 594ndash727 vs 771 log10 IUmL 95 CI741ndash802 P lt 01) In 16 studies with ALT data the pooledmean ALT levels among 1663 patients with and 14974without HBsAg seroclearance were not statistically different(64 UL 95 CI 27ndash150 vs 58 UL 95 CI 19ndash178 P frac1490) The pooled mean platelet count among 822 patients withand 9536 patients without HBsAg seroclearance in 10 studieswas also not statistically different (195 109L 95 CI
Table 1Characteristics of the Included Studies and Patients
Year and First Authora Region Settings Cohort TypePatients
n MaleMeanAge y
HBeAg(thorn)at Entry
Cirrhosisat Entry
IncidentHBsAg
Seroclearance
AnnualSeroclearance
Rate 5-yearCSR
10-yearCSR
15-yearCSR
2014 Kobayashi20 Asia Pacific Community Health care service 1130 705 405 81 273 200 163 9 18 262013 Hosaka19 Asia Pacific Community Health care service 791 627 43 442 169 38 070 24 8 182011 Suzuki31 Asia Pacific Community Health care service 615 464 35b 414 72 69 181 65 15 352016 Charatcharoenwi-
tthaya17Asia Pacific Mixed Health care service 233 172 416 135 22 7 229 mdash mdash mdash
2013 Treeprasertsuk25 Asia Pacific Academic Health care service 431 310 434 262 0 2 015 mdash mdash mdash
2015 Lauret22 Europe Academic Health care service 614 391 371 139 52 78 141 44 118 2172017 Riveiro-Barciela30 Europe Mixed Health care service 633 459 496 77 42 9 041 182 253 mdash
2016 Park28 Asia Pacific Academic Health care service 954 627 433 mdash mdash 75 105 365 903 25482014 Preda29 Europe Mixed Health care service 533 340 415 mdash 43 7 087 mdash mdash mdash
2015 Tseng33 Asia Pacific Academic Health care service 2686 1631 414 0 0 381 095 273 676 12392014 Fung18 Asia Pacific Academic Health care service 775 483 362 0 mdash 60 052 131 333 7192017 Ungtrakul34 Asia Pacific Academic Health care service 297 132 415 0 0 15 237 mdash mdash mdash
2016 Nguyen26 North America Mixed Health care service 3479 1987 443 1096 202 37 021 09 292 4252010 Liu7 Asia Pacific Community Population based 3302 1994 461 482 0 568 213 742 1732 36772011 Kwak21 Asia Pacific Academic Health care service 714 476 477 0 mdash 41 181 977 mdash mdash
2013 Luo24 Asia Pacific Academic Health care service 217 196 407 113 74 9 081 417 711 mdash
2015 Yapali44 North America Academic Health care service 234 122 35b 44 mdash 9 080 mdash mdash mdash
2002 Sanchez-Tapias8 Europe Academic Health care service 269 218 36 173 21 29 139 mdash mdash mdash
2015 Habersetzer45 Europe Academic Health care service 315 211 35b 69 mdash 29 158 mdash mdash mdash
2014 Farzi46 Middle East Community Health care service 399 231 356 0 0 48 122 mdash mdash mdash
2012 Arai47 Asia Pacific Academic Health care service 423 239 405 183 mdash 25 097 mdash mdash mdash
2005 Ahn48 Asia Pacific Academic Health care service 432 mdash mdash 0 mdash 49 046 mdash mdash mdash
2014 Ferreira49 South America Academic Health care service 548 336 377 mdash mdash 40 056 mdash mdash mdash
2016 Han50 Asia Pacific mdash Population based 634 485 486 0 0 117 302 mdash mdash mdash
2010 Simonetti36 North America Community Population based 1271 mdash 209b mdash mdash 158 065 mdash mdash mdash
2014 Kim9 Asia Pacific mdash Health care service 5409 3699 449 3601 2684 110 032 mdash mdash mdash
2016 Nagaoka51 Asia Pacific Academic Health care service 392 278 395b 285 111 50 091 mdash 54 982015 Orito27 Asia Pacific Academic Health care service 602 381 52b 295 110 13 030 mdash mdash mdash
2010 Tai32 Asia Pacific Mixed Health care service 6621 3761 342 1386 0 555 171 mdash mdash mdash
2016 Ari52 Middle East mdash Health care service 1427 767 371 48 mdash 84 104 mdash mdash mdash
2007 Nam53 Asia Pacific mdash Health care service 4061 2639 500 1584 893 47 036 mdash mdash mdash
2011 Lu54 Asia Pacific Academic Health care service 220 156 mdash 168 25 17 159 mdash mdash mdash
1998 Huo55 Asia Pacific Community Health care service 1355 1113 41 mdash mdash 58 157 mdash mdash mdash
2015 Lim23 Asia Pacific Community Population based 572 359 mdash 234 mdash 145 130 mdash mdash mdash
CSR cumulative seroclearance rateaTable 1 referencesbMedian age
February2019
HBsAgSeroclearance
inAdults
With
ChronicHBV
Infection639
CLINICAL LIVER
Figure 2 Pooled annualHBsAg seroclearance rateof chronic hepatitis B pa-tients Annual HBsAgseroclearance rates werecombined using a randomeffects model The size ofeach square representsthe weight of that studyThe vertical dotted linerepresents the pooledrate See Table 1 for fullcitation details for thestudies ASR annualseroclearance rate SPnumber of patients whohave achieved HBsAgseroclearance
Figure 3 Pooled 5- 10- and 15-year cumulative incidencerates of HBsAg seroclearance
640 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
183 109ndash208 109 vs 196 109L 95 CI 182 109ndash210 109 P frac14 95)
Region Scale and Setting of StudiesWe stratified the pooled HBsAg seroclearance rates by
geographic region (Figure 6) and found that there was atrend toward differences in seroclearance rates (P frac14 06)with the Asia Pacific region (109 95 CI 081ndash142 23studies with 32866 patients) Europe (108 95 CI064ndash163 5 studies with 2364 patients) and the MiddleEast (105 95 CI 082ndash131 2 studies with 1826 pa-tients) having higher annual rates and North (050 95CI 015ndash104 3 studies with 4984 patients) and SouthAmerica (070 95 CI 050ndash094 1 study with 548 pa-tients) having lower rates However the difference acrossregions did not reach the conventional level of statisticalsignificance We performed additional subgroup analyses byregion and showed that HBsAg seroclearance rates inEurope (P frac14 977) and North America (P frac14 051) were notsignificantly different compared with that in the Asia Pacificregion when the results were stratified by subgroups
Figure 4 Subgroup anal-ysis of HBsAg seroclear-ance rate by sex baselineHBeAg status and base-line cirrhosis ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 641
CLINICAL
LIVE
R
(eg age HBeAg status cirrhosis HBV DNA study setting)(Supplementary Figures 2 and 3 and SupplementaryTable 3)
Regarding study settings and design the pooled HBsAgseroclearance rate was higher in population-based studies(168 95 CI 086ndash278) than health care servicendashbasedstudies (093 95 CI 072ndash117) but this difference wasnot statistically significant (P frac14 10) (Figure 6) Howeverheterogeneity was high (9874 for population-basedstudies 9670 for health care servicendashbased studies P lt01 for both) Similarly studies that collected data from acommunity-based health care servicendashbased population(134 95 CI 092ndash183) also had higher seroclearancerates than university-based studies (097 95 CI 078ndash118) although the difference again was not statisticallysignificant (P frac14 27)
HBsAg Seroclearance Rates in CHBPatients With Different HBV Genotypes andby Treatment History
There was no significant difference in HBsAg seroclear-ance across different genotypes among more than 10000patients with genotype data (331 patients with genotype A4685 with genotype B 5756 with genotype C 94 with ge-notype D and 231 with genotype F) (Supplementary
Figure 4) The annual seroclearance rates were 126(95 CI 029ndash285) 079 (95 CI 042ndash126) 102(95 CI 071ndash139) 105 (95 CI 043ndash193) and 059(95 CI 039ndash083) for genotypes A B C D and Frespectively Comparative analysis for the 2 largest groupsgenotypes B (n frac14 4685) and C (n frac14 5756) also found nosignificant difference between these 2 groups (P frac14 453) Inaddition there was no significant difference in HBsAgseroclearance between treated (n frac14 7565 082 95 CI034ndash150) and untreated (n frac14 20556 131 95 CI098ndash167) patients (P frac14 195) (Supplementary Figure 5)For the treated group we further subanalyzed HBsAgseroclearance rates by specific treatment regimen and founda higher rate in interferon-treated patients (1 study 3833person-years 180 95 CI 140ndash225) than in entecavir-treated patients (2 studies 1997 person-years 080 95CI 044ndash125) and lamivudine-treated patients (1 study5428 person-years 065 95 CI 045ndash089) There wereno data for patients treated by other nucleos(t)ideanalogues
Sensitivity AnalysisWe performed 5 sensitivity tests In the first we
excluded studies with a fair or high risk of bias (NOS scorelt 7) (Supplementary Figure 6A) The annual seroclearance
Figure 5 The baselinelaboratory data of CHBpatients categorized byachievement of HBsAgseroclearance Data werederived from articles thatprovided baseline resultsin patients who achievedand those who did notachieve HBsAg seroclear-ance during the follow-upperiod ASR annual sero-clearance rate K numberof studies N total numberof CHB patients qHBsAgquantitative hepatitis Bsurface antigen
Figure 6 Subgroup anal-ysis of HBsAg seroclear-ance rate by study regionscale of study and prac-tice settings ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
642 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
rate became higher (109 95 CI 082ndash141) but het-erogeneity remained high (I2 frac14 9770) In the secondsensitivity analysis we omitted 12 studies with smallersample size (n lt 500 patients) (Supplementary Figure 6B)Data from the remaining 22 larger studies showed anannual seroclearance rate of 100 (95 CI 073ndash132) butheterogeneity again remained high (I2 frac14 9830)
In the third sensitivity test to clarify whether thenonlinear increase of cumulative HBsAg seroclearance ratewas associated with the longer follow-up period in thepopulation-based cohort we performed a subgroup analysisand showed that the cumulative incident HBsAg seroclear-ance rates were indeed nonlinear in both population-basedand health care servicendashbased cohorts (SupplementaryFigure 7) In the fourth sensitivity test we subanalyzeddata for studies that confirmed HBsAg seroclearance byrepeated testing and excluded those that did not specifythis The pooled annual seroclearance rate remained similar(111 95 CI 085ndash139) (Supplementary Figure 8)Finally we excluded studies for which we imputed theannual HBsAg seroclearance rate and the pooled annualHBsAg seroclearance rate was 098 (95 CI 074ndash125)
Heterogeneity and Publication BiasThe heterogeneity of the HBsAg seroclearance rate was
severe as evidenced by the high I2 statistics in the pooledannual and 5- 10- and 15-year cumulative seroclearancerates (97 99 99 and 99 respectively)(Supplementary Table 2) Subgroup analysis also showedhigh heterogeneity However as presented by the Eggerrsquostest there was no publication bias in the pooled annualHBsAg seroclearance rates or any of the pooled cumulativeseroclearance rates (Supplementary Table 2)
DiscussionIn this meta-analysis of 34 studies which included
42588 CHB patients with 303754 person-years of follow-up we found that 3194 patients had an incident HBsAgseroclearance event resulting in a pooled HBsAg
seroclearance rate of 102 (95 CI 079ndash127) and con-firming that HBsAg is a rare event In addition by combiningthe published and updated aggregated data we determinedthe 5- 10- and 15-year cumulative seroclearance rates andfound that the rates of seroclearance increased 4-fold byyear 5 (403) further doubled by year 10 (816) anddoubled again by year 15 such that almost 18 of patientshad achieved seroclearance by year 15 after study entryOur finding is consistent with a prior report of a large-scaleprospective study by Chu et al6 in which the rate of HBsAgseroclearance increased in a nonlinear fashion from 81after the first 10 years to 249 after 20 years and to447 after 25 years of follow-up However the severeheterogeneity of our results requires that they be inter-preted with caution
Similar to other single-center studies we found thatpatients who were HBeAg negative at baseline had lowerbaseline HBV DNA levels and had lower quantitative HBsAgexperienced higher rates of HBsAg seroclearance793536
These characteristics are typical of the inactive carrierphase suggesting that these patients are better able tomount an immune response to the virus leading to virologicremission and over time spontaneous HBsAg seroclear-ance3337 Our analysis also confirmed findings of others thatlower baseline serum HBsAg levels predict HBsAg sero-clearance particularly if the HBsAg levels were lt100 IUmL33 Quantification of HBsAg has been adopted as animportant marker of immune control of CHB and has beensuggested to correlate with the covalently close circularDNA levels in the liver In addition a low HBsAg level isassociated with a lower risk of HCC and liver-related mor-tality among HBeAg-negative patients with low viremia38
Although the finding of an association between HBsAglevel and HBsAg seroclearance is a self-fulfilling prophecybecause the level has to decrease before it becomes unde-tectable this has implications for the design of clinical trialsaimed at HBV cure in that randomization must be stratifiedby baseline HBsAg levels
Furthermore we were able to provide pooled HBsAgseroclearance rates for CHB patients from different
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
638 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
screening the titles and abstracts 180 potentially eligiblestudies were retrieved for full-text reviews After review atotal of 34 articles (42588 CHB patients) met our inclusionand exclusion criteria and were included in the meta-analysis We received updated aggregated data from 19 ofthe 34 studies717ndash34 including 3 studies from 1 center(Toranomon Hospital Tokyo Japan) but we contacted thestudy authors and confirmed that only nonduplicate pa-tients were included in our meta-analysis192031
Characteristics of Included StudiesTable 1 shows the characteristics of included studies and
of the participants CHB patients from 14 countries wereincluded with the majority from the Asia Pacific region (23studies) Four studies were population based and the restwere conducted with data derived from hospitals or healthcare centers The sample sizes of the included studiesranged from 217 to 6621 with the proportion of malesranging from 444 to 903 The mean age ranged from342 to 50 years Twenty-two out of 34 studies showed lowrisk of bias (Supplementary Table 1)
Overall Annual Seroclearance and CumulativeIncidence
Among the 42588 CHB patients 3194 patients experi-enced HBsAg seroclearance The annual seroclearance ratesranged from 015 to 302 with a pooled rate of 102
Figure 1 Preferred Reporting Items for Systematic Reviewsand Meta-analyses (PRISMA) flow chart of article selection
(95 CI 079ndash127) and high heterogeneity (I2 frac14 9749)(Figure 2) The pooled 5- 10- and 15-year cumulativeincidence rates were nonlinear at 403 (95 CI 246ndash597 I2 frac14 9957) 816 (95 CI 519ndash1179 I2 frac149976) and 1799 (95 CI 1083ndash2696 I2 frac14 9991)respectively (Figure 3 and Supplementary Table 2)
Annual Seroclearance Rate by BaselineDemographic and Clinical Characteristics
The pooled annual seroclearance rates for male (n frac1411142) and female (n frac14 6080) patients were 113 (95CI 078ndash155) and 087 (95 CI 049ndash136) respectivelybut the difference was not statistically significant (P frac14 43)(Figure 4) The mean age of the study cohort was 45 andthe pooled annual seroclearance rates were similar forstudies with a mean age less than 45 years (095 95 CI069ndash126) compared with studies with a mean age of 45years and older (112 95 CI 040ndash220) (SupplementaryFigure 1) Analyses by patients of specific age groups andraceethnicity were not performed because of lack of pri-mary data with most studies not reporting data by agegroups and many studies of mixed racesethnicities notreporting results stratified by raceethnicity
There were 9 studies that separately reported theannual seroclearance rate in patients who were HBeAgpositive (n frac14 3922) and those who were HBeAg negative(n frac14 15205) at baseline (Figure 4) Patients who wereHBeAg negative (133 95 CI 076ndash205) had almost a33 times higher HBsAg seroclearance rate than patientswho were HBeAg positive (040 95 CI 025ndash059)There were no significant differences in the annual sero-clearance rates between patients with cirrhosis (08495 CI 031ndash158 n frac14 970) and those without cirrhosis(104 95 CI 063ndash155 n frac14 13398) (P frac14 74)
Baseline Laboratory Parameters in PatientsWith HBsAg Seroclearance vs Those WithoutHBsAg Seroclearance
We investigated several baseline laboratory data that havebeen reported to have an association with HBsAg seroclear-ance (Figure 5) From 5 studies with quantitative HBsAg leveldata (1173 with incident HBsAg seroclearance 6246 without)the pooled mean quantitative HBsAg level was found to besignificantly lower among patients with HBsAg seroclearancecompared with those without seroclearance (274 log10 IUmL 95 CI 187ndash360 vs 390 log10 IUmL 95 CI 373ndash406 P lt 01) From 10 studies with HBV DNA data (1431with incident HBsAg seroclearance 16590 without) patientswith HBsAg seroclearance also showed a significantly lowerbaseline HBV DNA than those with no seroclearance (661log10 IUmL 95 CI 594ndash727 vs 771 log10 IUmL 95 CI741ndash802 P lt 01) In 16 studies with ALT data the pooledmean ALT levels among 1663 patients with and 14974without HBsAg seroclearance were not statistically different(64 UL 95 CI 27ndash150 vs 58 UL 95 CI 19ndash178 P frac1490) The pooled mean platelet count among 822 patients withand 9536 patients without HBsAg seroclearance in 10 studieswas also not statistically different (195 109L 95 CI
Table 1Characteristics of the Included Studies and Patients
Year and First Authora Region Settings Cohort TypePatients
n MaleMeanAge y
HBeAg(thorn)at Entry
Cirrhosisat Entry
IncidentHBsAg
Seroclearance
AnnualSeroclearance
Rate 5-yearCSR
10-yearCSR
15-yearCSR
2014 Kobayashi20 Asia Pacific Community Health care service 1130 705 405 81 273 200 163 9 18 262013 Hosaka19 Asia Pacific Community Health care service 791 627 43 442 169 38 070 24 8 182011 Suzuki31 Asia Pacific Community Health care service 615 464 35b 414 72 69 181 65 15 352016 Charatcharoenwi-
tthaya17Asia Pacific Mixed Health care service 233 172 416 135 22 7 229 mdash mdash mdash
2013 Treeprasertsuk25 Asia Pacific Academic Health care service 431 310 434 262 0 2 015 mdash mdash mdash
2015 Lauret22 Europe Academic Health care service 614 391 371 139 52 78 141 44 118 2172017 Riveiro-Barciela30 Europe Mixed Health care service 633 459 496 77 42 9 041 182 253 mdash
2016 Park28 Asia Pacific Academic Health care service 954 627 433 mdash mdash 75 105 365 903 25482014 Preda29 Europe Mixed Health care service 533 340 415 mdash 43 7 087 mdash mdash mdash
2015 Tseng33 Asia Pacific Academic Health care service 2686 1631 414 0 0 381 095 273 676 12392014 Fung18 Asia Pacific Academic Health care service 775 483 362 0 mdash 60 052 131 333 7192017 Ungtrakul34 Asia Pacific Academic Health care service 297 132 415 0 0 15 237 mdash mdash mdash
2016 Nguyen26 North America Mixed Health care service 3479 1987 443 1096 202 37 021 09 292 4252010 Liu7 Asia Pacific Community Population based 3302 1994 461 482 0 568 213 742 1732 36772011 Kwak21 Asia Pacific Academic Health care service 714 476 477 0 mdash 41 181 977 mdash mdash
2013 Luo24 Asia Pacific Academic Health care service 217 196 407 113 74 9 081 417 711 mdash
2015 Yapali44 North America Academic Health care service 234 122 35b 44 mdash 9 080 mdash mdash mdash
2002 Sanchez-Tapias8 Europe Academic Health care service 269 218 36 173 21 29 139 mdash mdash mdash
2015 Habersetzer45 Europe Academic Health care service 315 211 35b 69 mdash 29 158 mdash mdash mdash
2014 Farzi46 Middle East Community Health care service 399 231 356 0 0 48 122 mdash mdash mdash
2012 Arai47 Asia Pacific Academic Health care service 423 239 405 183 mdash 25 097 mdash mdash mdash
2005 Ahn48 Asia Pacific Academic Health care service 432 mdash mdash 0 mdash 49 046 mdash mdash mdash
2014 Ferreira49 South America Academic Health care service 548 336 377 mdash mdash 40 056 mdash mdash mdash
2016 Han50 Asia Pacific mdash Population based 634 485 486 0 0 117 302 mdash mdash mdash
2010 Simonetti36 North America Community Population based 1271 mdash 209b mdash mdash 158 065 mdash mdash mdash
2014 Kim9 Asia Pacific mdash Health care service 5409 3699 449 3601 2684 110 032 mdash mdash mdash
2016 Nagaoka51 Asia Pacific Academic Health care service 392 278 395b 285 111 50 091 mdash 54 982015 Orito27 Asia Pacific Academic Health care service 602 381 52b 295 110 13 030 mdash mdash mdash
2010 Tai32 Asia Pacific Mixed Health care service 6621 3761 342 1386 0 555 171 mdash mdash mdash
2016 Ari52 Middle East mdash Health care service 1427 767 371 48 mdash 84 104 mdash mdash mdash
2007 Nam53 Asia Pacific mdash Health care service 4061 2639 500 1584 893 47 036 mdash mdash mdash
2011 Lu54 Asia Pacific Academic Health care service 220 156 mdash 168 25 17 159 mdash mdash mdash
1998 Huo55 Asia Pacific Community Health care service 1355 1113 41 mdash mdash 58 157 mdash mdash mdash
2015 Lim23 Asia Pacific Community Population based 572 359 mdash 234 mdash 145 130 mdash mdash mdash
CSR cumulative seroclearance rateaTable 1 referencesbMedian age
February2019
HBsAgSeroclearance
inAdults
With
ChronicHBV
Infection639
CLINICAL LIVER
Figure 2 Pooled annualHBsAg seroclearance rateof chronic hepatitis B pa-tients Annual HBsAgseroclearance rates werecombined using a randomeffects model The size ofeach square representsthe weight of that studyThe vertical dotted linerepresents the pooledrate See Table 1 for fullcitation details for thestudies ASR annualseroclearance rate SPnumber of patients whohave achieved HBsAgseroclearance
Figure 3 Pooled 5- 10- and 15-year cumulative incidencerates of HBsAg seroclearance
640 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
183 109ndash208 109 vs 196 109L 95 CI 182 109ndash210 109 P frac14 95)
Region Scale and Setting of StudiesWe stratified the pooled HBsAg seroclearance rates by
geographic region (Figure 6) and found that there was atrend toward differences in seroclearance rates (P frac14 06)with the Asia Pacific region (109 95 CI 081ndash142 23studies with 32866 patients) Europe (108 95 CI064ndash163 5 studies with 2364 patients) and the MiddleEast (105 95 CI 082ndash131 2 studies with 1826 pa-tients) having higher annual rates and North (050 95CI 015ndash104 3 studies with 4984 patients) and SouthAmerica (070 95 CI 050ndash094 1 study with 548 pa-tients) having lower rates However the difference acrossregions did not reach the conventional level of statisticalsignificance We performed additional subgroup analyses byregion and showed that HBsAg seroclearance rates inEurope (P frac14 977) and North America (P frac14 051) were notsignificantly different compared with that in the Asia Pacificregion when the results were stratified by subgroups
Figure 4 Subgroup anal-ysis of HBsAg seroclear-ance rate by sex baselineHBeAg status and base-line cirrhosis ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 641
CLINICAL
LIVE
R
(eg age HBeAg status cirrhosis HBV DNA study setting)(Supplementary Figures 2 and 3 and SupplementaryTable 3)
Regarding study settings and design the pooled HBsAgseroclearance rate was higher in population-based studies(168 95 CI 086ndash278) than health care servicendashbasedstudies (093 95 CI 072ndash117) but this difference wasnot statistically significant (P frac14 10) (Figure 6) Howeverheterogeneity was high (9874 for population-basedstudies 9670 for health care servicendashbased studies P lt01 for both) Similarly studies that collected data from acommunity-based health care servicendashbased population(134 95 CI 092ndash183) also had higher seroclearancerates than university-based studies (097 95 CI 078ndash118) although the difference again was not statisticallysignificant (P frac14 27)
HBsAg Seroclearance Rates in CHBPatients With Different HBV Genotypes andby Treatment History
There was no significant difference in HBsAg seroclear-ance across different genotypes among more than 10000patients with genotype data (331 patients with genotype A4685 with genotype B 5756 with genotype C 94 with ge-notype D and 231 with genotype F) (Supplementary
Figure 4) The annual seroclearance rates were 126(95 CI 029ndash285) 079 (95 CI 042ndash126) 102(95 CI 071ndash139) 105 (95 CI 043ndash193) and 059(95 CI 039ndash083) for genotypes A B C D and Frespectively Comparative analysis for the 2 largest groupsgenotypes B (n frac14 4685) and C (n frac14 5756) also found nosignificant difference between these 2 groups (P frac14 453) Inaddition there was no significant difference in HBsAgseroclearance between treated (n frac14 7565 082 95 CI034ndash150) and untreated (n frac14 20556 131 95 CI098ndash167) patients (P frac14 195) (Supplementary Figure 5)For the treated group we further subanalyzed HBsAgseroclearance rates by specific treatment regimen and founda higher rate in interferon-treated patients (1 study 3833person-years 180 95 CI 140ndash225) than in entecavir-treated patients (2 studies 1997 person-years 080 95CI 044ndash125) and lamivudine-treated patients (1 study5428 person-years 065 95 CI 045ndash089) There wereno data for patients treated by other nucleos(t)ideanalogues
Sensitivity AnalysisWe performed 5 sensitivity tests In the first we
excluded studies with a fair or high risk of bias (NOS scorelt 7) (Supplementary Figure 6A) The annual seroclearance
Figure 5 The baselinelaboratory data of CHBpatients categorized byachievement of HBsAgseroclearance Data werederived from articles thatprovided baseline resultsin patients who achievedand those who did notachieve HBsAg seroclear-ance during the follow-upperiod ASR annual sero-clearance rate K numberof studies N total numberof CHB patients qHBsAgquantitative hepatitis Bsurface antigen
Figure 6 Subgroup anal-ysis of HBsAg seroclear-ance rate by study regionscale of study and prac-tice settings ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
642 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
rate became higher (109 95 CI 082ndash141) but het-erogeneity remained high (I2 frac14 9770) In the secondsensitivity analysis we omitted 12 studies with smallersample size (n lt 500 patients) (Supplementary Figure 6B)Data from the remaining 22 larger studies showed anannual seroclearance rate of 100 (95 CI 073ndash132) butheterogeneity again remained high (I2 frac14 9830)
In the third sensitivity test to clarify whether thenonlinear increase of cumulative HBsAg seroclearance ratewas associated with the longer follow-up period in thepopulation-based cohort we performed a subgroup analysisand showed that the cumulative incident HBsAg seroclear-ance rates were indeed nonlinear in both population-basedand health care servicendashbased cohorts (SupplementaryFigure 7) In the fourth sensitivity test we subanalyzeddata for studies that confirmed HBsAg seroclearance byrepeated testing and excluded those that did not specifythis The pooled annual seroclearance rate remained similar(111 95 CI 085ndash139) (Supplementary Figure 8)Finally we excluded studies for which we imputed theannual HBsAg seroclearance rate and the pooled annualHBsAg seroclearance rate was 098 (95 CI 074ndash125)
Heterogeneity and Publication BiasThe heterogeneity of the HBsAg seroclearance rate was
severe as evidenced by the high I2 statistics in the pooledannual and 5- 10- and 15-year cumulative seroclearancerates (97 99 99 and 99 respectively)(Supplementary Table 2) Subgroup analysis also showedhigh heterogeneity However as presented by the Eggerrsquostest there was no publication bias in the pooled annualHBsAg seroclearance rates or any of the pooled cumulativeseroclearance rates (Supplementary Table 2)
DiscussionIn this meta-analysis of 34 studies which included
42588 CHB patients with 303754 person-years of follow-up we found that 3194 patients had an incident HBsAgseroclearance event resulting in a pooled HBsAg
seroclearance rate of 102 (95 CI 079ndash127) and con-firming that HBsAg is a rare event In addition by combiningthe published and updated aggregated data we determinedthe 5- 10- and 15-year cumulative seroclearance rates andfound that the rates of seroclearance increased 4-fold byyear 5 (403) further doubled by year 10 (816) anddoubled again by year 15 such that almost 18 of patientshad achieved seroclearance by year 15 after study entryOur finding is consistent with a prior report of a large-scaleprospective study by Chu et al6 in which the rate of HBsAgseroclearance increased in a nonlinear fashion from 81after the first 10 years to 249 after 20 years and to447 after 25 years of follow-up However the severeheterogeneity of our results requires that they be inter-preted with caution
Similar to other single-center studies we found thatpatients who were HBeAg negative at baseline had lowerbaseline HBV DNA levels and had lower quantitative HBsAgexperienced higher rates of HBsAg seroclearance793536
These characteristics are typical of the inactive carrierphase suggesting that these patients are better able tomount an immune response to the virus leading to virologicremission and over time spontaneous HBsAg seroclear-ance3337 Our analysis also confirmed findings of others thatlower baseline serum HBsAg levels predict HBsAg sero-clearance particularly if the HBsAg levels were lt100 IUmL33 Quantification of HBsAg has been adopted as animportant marker of immune control of CHB and has beensuggested to correlate with the covalently close circularDNA levels in the liver In addition a low HBsAg level isassociated with a lower risk of HCC and liver-related mor-tality among HBeAg-negative patients with low viremia38
Although the finding of an association between HBsAglevel and HBsAg seroclearance is a self-fulfilling prophecybecause the level has to decrease before it becomes unde-tectable this has implications for the design of clinical trialsaimed at HBV cure in that randomization must be stratifiedby baseline HBsAg levels
Furthermore we were able to provide pooled HBsAgseroclearance rates for CHB patients from different
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Table 1Characteristics of the Included Studies and Patients
Year and First Authora Region Settings Cohort TypePatients
n MaleMeanAge y
HBeAg(thorn)at Entry
Cirrhosisat Entry
IncidentHBsAg
Seroclearance
AnnualSeroclearance
Rate 5-yearCSR
10-yearCSR
15-yearCSR
2014 Kobayashi20 Asia Pacific Community Health care service 1130 705 405 81 273 200 163 9 18 262013 Hosaka19 Asia Pacific Community Health care service 791 627 43 442 169 38 070 24 8 182011 Suzuki31 Asia Pacific Community Health care service 615 464 35b 414 72 69 181 65 15 352016 Charatcharoenwi-
tthaya17Asia Pacific Mixed Health care service 233 172 416 135 22 7 229 mdash mdash mdash
2013 Treeprasertsuk25 Asia Pacific Academic Health care service 431 310 434 262 0 2 015 mdash mdash mdash
2015 Lauret22 Europe Academic Health care service 614 391 371 139 52 78 141 44 118 2172017 Riveiro-Barciela30 Europe Mixed Health care service 633 459 496 77 42 9 041 182 253 mdash
2016 Park28 Asia Pacific Academic Health care service 954 627 433 mdash mdash 75 105 365 903 25482014 Preda29 Europe Mixed Health care service 533 340 415 mdash 43 7 087 mdash mdash mdash
2015 Tseng33 Asia Pacific Academic Health care service 2686 1631 414 0 0 381 095 273 676 12392014 Fung18 Asia Pacific Academic Health care service 775 483 362 0 mdash 60 052 131 333 7192017 Ungtrakul34 Asia Pacific Academic Health care service 297 132 415 0 0 15 237 mdash mdash mdash
2016 Nguyen26 North America Mixed Health care service 3479 1987 443 1096 202 37 021 09 292 4252010 Liu7 Asia Pacific Community Population based 3302 1994 461 482 0 568 213 742 1732 36772011 Kwak21 Asia Pacific Academic Health care service 714 476 477 0 mdash 41 181 977 mdash mdash
2013 Luo24 Asia Pacific Academic Health care service 217 196 407 113 74 9 081 417 711 mdash
2015 Yapali44 North America Academic Health care service 234 122 35b 44 mdash 9 080 mdash mdash mdash
2002 Sanchez-Tapias8 Europe Academic Health care service 269 218 36 173 21 29 139 mdash mdash mdash
2015 Habersetzer45 Europe Academic Health care service 315 211 35b 69 mdash 29 158 mdash mdash mdash
2014 Farzi46 Middle East Community Health care service 399 231 356 0 0 48 122 mdash mdash mdash
2012 Arai47 Asia Pacific Academic Health care service 423 239 405 183 mdash 25 097 mdash mdash mdash
2005 Ahn48 Asia Pacific Academic Health care service 432 mdash mdash 0 mdash 49 046 mdash mdash mdash
2014 Ferreira49 South America Academic Health care service 548 336 377 mdash mdash 40 056 mdash mdash mdash
2016 Han50 Asia Pacific mdash Population based 634 485 486 0 0 117 302 mdash mdash mdash
2010 Simonetti36 North America Community Population based 1271 mdash 209b mdash mdash 158 065 mdash mdash mdash
2014 Kim9 Asia Pacific mdash Health care service 5409 3699 449 3601 2684 110 032 mdash mdash mdash
2016 Nagaoka51 Asia Pacific Academic Health care service 392 278 395b 285 111 50 091 mdash 54 982015 Orito27 Asia Pacific Academic Health care service 602 381 52b 295 110 13 030 mdash mdash mdash
2010 Tai32 Asia Pacific Mixed Health care service 6621 3761 342 1386 0 555 171 mdash mdash mdash
2016 Ari52 Middle East mdash Health care service 1427 767 371 48 mdash 84 104 mdash mdash mdash
2007 Nam53 Asia Pacific mdash Health care service 4061 2639 500 1584 893 47 036 mdash mdash mdash
2011 Lu54 Asia Pacific Academic Health care service 220 156 mdash 168 25 17 159 mdash mdash mdash
1998 Huo55 Asia Pacific Community Health care service 1355 1113 41 mdash mdash 58 157 mdash mdash mdash
2015 Lim23 Asia Pacific Community Population based 572 359 mdash 234 mdash 145 130 mdash mdash mdash
CSR cumulative seroclearance rateaTable 1 referencesbMedian age
February2019
HBsAgSeroclearance
inAdults
With
ChronicHBV
Infection639
CLINICAL LIVER
Figure 2 Pooled annualHBsAg seroclearance rateof chronic hepatitis B pa-tients Annual HBsAgseroclearance rates werecombined using a randomeffects model The size ofeach square representsthe weight of that studyThe vertical dotted linerepresents the pooledrate See Table 1 for fullcitation details for thestudies ASR annualseroclearance rate SPnumber of patients whohave achieved HBsAgseroclearance
Figure 3 Pooled 5- 10- and 15-year cumulative incidencerates of HBsAg seroclearance
640 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
183 109ndash208 109 vs 196 109L 95 CI 182 109ndash210 109 P frac14 95)
Region Scale and Setting of StudiesWe stratified the pooled HBsAg seroclearance rates by
geographic region (Figure 6) and found that there was atrend toward differences in seroclearance rates (P frac14 06)with the Asia Pacific region (109 95 CI 081ndash142 23studies with 32866 patients) Europe (108 95 CI064ndash163 5 studies with 2364 patients) and the MiddleEast (105 95 CI 082ndash131 2 studies with 1826 pa-tients) having higher annual rates and North (050 95CI 015ndash104 3 studies with 4984 patients) and SouthAmerica (070 95 CI 050ndash094 1 study with 548 pa-tients) having lower rates However the difference acrossregions did not reach the conventional level of statisticalsignificance We performed additional subgroup analyses byregion and showed that HBsAg seroclearance rates inEurope (P frac14 977) and North America (P frac14 051) were notsignificantly different compared with that in the Asia Pacificregion when the results were stratified by subgroups
Figure 4 Subgroup anal-ysis of HBsAg seroclear-ance rate by sex baselineHBeAg status and base-line cirrhosis ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 641
CLINICAL
LIVE
R
(eg age HBeAg status cirrhosis HBV DNA study setting)(Supplementary Figures 2 and 3 and SupplementaryTable 3)
Regarding study settings and design the pooled HBsAgseroclearance rate was higher in population-based studies(168 95 CI 086ndash278) than health care servicendashbasedstudies (093 95 CI 072ndash117) but this difference wasnot statistically significant (P frac14 10) (Figure 6) Howeverheterogeneity was high (9874 for population-basedstudies 9670 for health care servicendashbased studies P lt01 for both) Similarly studies that collected data from acommunity-based health care servicendashbased population(134 95 CI 092ndash183) also had higher seroclearancerates than university-based studies (097 95 CI 078ndash118) although the difference again was not statisticallysignificant (P frac14 27)
HBsAg Seroclearance Rates in CHBPatients With Different HBV Genotypes andby Treatment History
There was no significant difference in HBsAg seroclear-ance across different genotypes among more than 10000patients with genotype data (331 patients with genotype A4685 with genotype B 5756 with genotype C 94 with ge-notype D and 231 with genotype F) (Supplementary
Figure 4) The annual seroclearance rates were 126(95 CI 029ndash285) 079 (95 CI 042ndash126) 102(95 CI 071ndash139) 105 (95 CI 043ndash193) and 059(95 CI 039ndash083) for genotypes A B C D and Frespectively Comparative analysis for the 2 largest groupsgenotypes B (n frac14 4685) and C (n frac14 5756) also found nosignificant difference between these 2 groups (P frac14 453) Inaddition there was no significant difference in HBsAgseroclearance between treated (n frac14 7565 082 95 CI034ndash150) and untreated (n frac14 20556 131 95 CI098ndash167) patients (P frac14 195) (Supplementary Figure 5)For the treated group we further subanalyzed HBsAgseroclearance rates by specific treatment regimen and founda higher rate in interferon-treated patients (1 study 3833person-years 180 95 CI 140ndash225) than in entecavir-treated patients (2 studies 1997 person-years 080 95CI 044ndash125) and lamivudine-treated patients (1 study5428 person-years 065 95 CI 045ndash089) There wereno data for patients treated by other nucleos(t)ideanalogues
Sensitivity AnalysisWe performed 5 sensitivity tests In the first we
excluded studies with a fair or high risk of bias (NOS scorelt 7) (Supplementary Figure 6A) The annual seroclearance
Figure 5 The baselinelaboratory data of CHBpatients categorized byachievement of HBsAgseroclearance Data werederived from articles thatprovided baseline resultsin patients who achievedand those who did notachieve HBsAg seroclear-ance during the follow-upperiod ASR annual sero-clearance rate K numberof studies N total numberof CHB patients qHBsAgquantitative hepatitis Bsurface antigen
Figure 6 Subgroup anal-ysis of HBsAg seroclear-ance rate by study regionscale of study and prac-tice settings ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
642 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
rate became higher (109 95 CI 082ndash141) but het-erogeneity remained high (I2 frac14 9770) In the secondsensitivity analysis we omitted 12 studies with smallersample size (n lt 500 patients) (Supplementary Figure 6B)Data from the remaining 22 larger studies showed anannual seroclearance rate of 100 (95 CI 073ndash132) butheterogeneity again remained high (I2 frac14 9830)
In the third sensitivity test to clarify whether thenonlinear increase of cumulative HBsAg seroclearance ratewas associated with the longer follow-up period in thepopulation-based cohort we performed a subgroup analysisand showed that the cumulative incident HBsAg seroclear-ance rates were indeed nonlinear in both population-basedand health care servicendashbased cohorts (SupplementaryFigure 7) In the fourth sensitivity test we subanalyzeddata for studies that confirmed HBsAg seroclearance byrepeated testing and excluded those that did not specifythis The pooled annual seroclearance rate remained similar(111 95 CI 085ndash139) (Supplementary Figure 8)Finally we excluded studies for which we imputed theannual HBsAg seroclearance rate and the pooled annualHBsAg seroclearance rate was 098 (95 CI 074ndash125)
Heterogeneity and Publication BiasThe heterogeneity of the HBsAg seroclearance rate was
severe as evidenced by the high I2 statistics in the pooledannual and 5- 10- and 15-year cumulative seroclearancerates (97 99 99 and 99 respectively)(Supplementary Table 2) Subgroup analysis also showedhigh heterogeneity However as presented by the Eggerrsquostest there was no publication bias in the pooled annualHBsAg seroclearance rates or any of the pooled cumulativeseroclearance rates (Supplementary Table 2)
DiscussionIn this meta-analysis of 34 studies which included
42588 CHB patients with 303754 person-years of follow-up we found that 3194 patients had an incident HBsAgseroclearance event resulting in a pooled HBsAg
seroclearance rate of 102 (95 CI 079ndash127) and con-firming that HBsAg is a rare event In addition by combiningthe published and updated aggregated data we determinedthe 5- 10- and 15-year cumulative seroclearance rates andfound that the rates of seroclearance increased 4-fold byyear 5 (403) further doubled by year 10 (816) anddoubled again by year 15 such that almost 18 of patientshad achieved seroclearance by year 15 after study entryOur finding is consistent with a prior report of a large-scaleprospective study by Chu et al6 in which the rate of HBsAgseroclearance increased in a nonlinear fashion from 81after the first 10 years to 249 after 20 years and to447 after 25 years of follow-up However the severeheterogeneity of our results requires that they be inter-preted with caution
Similar to other single-center studies we found thatpatients who were HBeAg negative at baseline had lowerbaseline HBV DNA levels and had lower quantitative HBsAgexperienced higher rates of HBsAg seroclearance793536
These characteristics are typical of the inactive carrierphase suggesting that these patients are better able tomount an immune response to the virus leading to virologicremission and over time spontaneous HBsAg seroclear-ance3337 Our analysis also confirmed findings of others thatlower baseline serum HBsAg levels predict HBsAg sero-clearance particularly if the HBsAg levels were lt100 IUmL33 Quantification of HBsAg has been adopted as animportant marker of immune control of CHB and has beensuggested to correlate with the covalently close circularDNA levels in the liver In addition a low HBsAg level isassociated with a lower risk of HCC and liver-related mor-tality among HBeAg-negative patients with low viremia38
Although the finding of an association between HBsAglevel and HBsAg seroclearance is a self-fulfilling prophecybecause the level has to decrease before it becomes unde-tectable this has implications for the design of clinical trialsaimed at HBV cure in that randomization must be stratifiedby baseline HBsAg levels
Furthermore we were able to provide pooled HBsAgseroclearance rates for CHB patients from different
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Figure 2 Pooled annualHBsAg seroclearance rateof chronic hepatitis B pa-tients Annual HBsAgseroclearance rates werecombined using a randomeffects model The size ofeach square representsthe weight of that studyThe vertical dotted linerepresents the pooledrate See Table 1 for fullcitation details for thestudies ASR annualseroclearance rate SPnumber of patients whohave achieved HBsAgseroclearance
Figure 3 Pooled 5- 10- and 15-year cumulative incidencerates of HBsAg seroclearance
640 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
183 109ndash208 109 vs 196 109L 95 CI 182 109ndash210 109 P frac14 95)
Region Scale and Setting of StudiesWe stratified the pooled HBsAg seroclearance rates by
geographic region (Figure 6) and found that there was atrend toward differences in seroclearance rates (P frac14 06)with the Asia Pacific region (109 95 CI 081ndash142 23studies with 32866 patients) Europe (108 95 CI064ndash163 5 studies with 2364 patients) and the MiddleEast (105 95 CI 082ndash131 2 studies with 1826 pa-tients) having higher annual rates and North (050 95CI 015ndash104 3 studies with 4984 patients) and SouthAmerica (070 95 CI 050ndash094 1 study with 548 pa-tients) having lower rates However the difference acrossregions did not reach the conventional level of statisticalsignificance We performed additional subgroup analyses byregion and showed that HBsAg seroclearance rates inEurope (P frac14 977) and North America (P frac14 051) were notsignificantly different compared with that in the Asia Pacificregion when the results were stratified by subgroups
Figure 4 Subgroup anal-ysis of HBsAg seroclear-ance rate by sex baselineHBeAg status and base-line cirrhosis ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 641
CLINICAL
LIVE
R
(eg age HBeAg status cirrhosis HBV DNA study setting)(Supplementary Figures 2 and 3 and SupplementaryTable 3)
Regarding study settings and design the pooled HBsAgseroclearance rate was higher in population-based studies(168 95 CI 086ndash278) than health care servicendashbasedstudies (093 95 CI 072ndash117) but this difference wasnot statistically significant (P frac14 10) (Figure 6) Howeverheterogeneity was high (9874 for population-basedstudies 9670 for health care servicendashbased studies P lt01 for both) Similarly studies that collected data from acommunity-based health care servicendashbased population(134 95 CI 092ndash183) also had higher seroclearancerates than university-based studies (097 95 CI 078ndash118) although the difference again was not statisticallysignificant (P frac14 27)
HBsAg Seroclearance Rates in CHBPatients With Different HBV Genotypes andby Treatment History
There was no significant difference in HBsAg seroclear-ance across different genotypes among more than 10000patients with genotype data (331 patients with genotype A4685 with genotype B 5756 with genotype C 94 with ge-notype D and 231 with genotype F) (Supplementary
Figure 4) The annual seroclearance rates were 126(95 CI 029ndash285) 079 (95 CI 042ndash126) 102(95 CI 071ndash139) 105 (95 CI 043ndash193) and 059(95 CI 039ndash083) for genotypes A B C D and Frespectively Comparative analysis for the 2 largest groupsgenotypes B (n frac14 4685) and C (n frac14 5756) also found nosignificant difference between these 2 groups (P frac14 453) Inaddition there was no significant difference in HBsAgseroclearance between treated (n frac14 7565 082 95 CI034ndash150) and untreated (n frac14 20556 131 95 CI098ndash167) patients (P frac14 195) (Supplementary Figure 5)For the treated group we further subanalyzed HBsAgseroclearance rates by specific treatment regimen and founda higher rate in interferon-treated patients (1 study 3833person-years 180 95 CI 140ndash225) than in entecavir-treated patients (2 studies 1997 person-years 080 95CI 044ndash125) and lamivudine-treated patients (1 study5428 person-years 065 95 CI 045ndash089) There wereno data for patients treated by other nucleos(t)ideanalogues
Sensitivity AnalysisWe performed 5 sensitivity tests In the first we
excluded studies with a fair or high risk of bias (NOS scorelt 7) (Supplementary Figure 6A) The annual seroclearance
Figure 5 The baselinelaboratory data of CHBpatients categorized byachievement of HBsAgseroclearance Data werederived from articles thatprovided baseline resultsin patients who achievedand those who did notachieve HBsAg seroclear-ance during the follow-upperiod ASR annual sero-clearance rate K numberof studies N total numberof CHB patients qHBsAgquantitative hepatitis Bsurface antigen
Figure 6 Subgroup anal-ysis of HBsAg seroclear-ance rate by study regionscale of study and prac-tice settings ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
642 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
rate became higher (109 95 CI 082ndash141) but het-erogeneity remained high (I2 frac14 9770) In the secondsensitivity analysis we omitted 12 studies with smallersample size (n lt 500 patients) (Supplementary Figure 6B)Data from the remaining 22 larger studies showed anannual seroclearance rate of 100 (95 CI 073ndash132) butheterogeneity again remained high (I2 frac14 9830)
In the third sensitivity test to clarify whether thenonlinear increase of cumulative HBsAg seroclearance ratewas associated with the longer follow-up period in thepopulation-based cohort we performed a subgroup analysisand showed that the cumulative incident HBsAg seroclear-ance rates were indeed nonlinear in both population-basedand health care servicendashbased cohorts (SupplementaryFigure 7) In the fourth sensitivity test we subanalyzeddata for studies that confirmed HBsAg seroclearance byrepeated testing and excluded those that did not specifythis The pooled annual seroclearance rate remained similar(111 95 CI 085ndash139) (Supplementary Figure 8)Finally we excluded studies for which we imputed theannual HBsAg seroclearance rate and the pooled annualHBsAg seroclearance rate was 098 (95 CI 074ndash125)
Heterogeneity and Publication BiasThe heterogeneity of the HBsAg seroclearance rate was
severe as evidenced by the high I2 statistics in the pooledannual and 5- 10- and 15-year cumulative seroclearancerates (97 99 99 and 99 respectively)(Supplementary Table 2) Subgroup analysis also showedhigh heterogeneity However as presented by the Eggerrsquostest there was no publication bias in the pooled annualHBsAg seroclearance rates or any of the pooled cumulativeseroclearance rates (Supplementary Table 2)
DiscussionIn this meta-analysis of 34 studies which included
42588 CHB patients with 303754 person-years of follow-up we found that 3194 patients had an incident HBsAgseroclearance event resulting in a pooled HBsAg
seroclearance rate of 102 (95 CI 079ndash127) and con-firming that HBsAg is a rare event In addition by combiningthe published and updated aggregated data we determinedthe 5- 10- and 15-year cumulative seroclearance rates andfound that the rates of seroclearance increased 4-fold byyear 5 (403) further doubled by year 10 (816) anddoubled again by year 15 such that almost 18 of patientshad achieved seroclearance by year 15 after study entryOur finding is consistent with a prior report of a large-scaleprospective study by Chu et al6 in which the rate of HBsAgseroclearance increased in a nonlinear fashion from 81after the first 10 years to 249 after 20 years and to447 after 25 years of follow-up However the severeheterogeneity of our results requires that they be inter-preted with caution
Similar to other single-center studies we found thatpatients who were HBeAg negative at baseline had lowerbaseline HBV DNA levels and had lower quantitative HBsAgexperienced higher rates of HBsAg seroclearance793536
These characteristics are typical of the inactive carrierphase suggesting that these patients are better able tomount an immune response to the virus leading to virologicremission and over time spontaneous HBsAg seroclear-ance3337 Our analysis also confirmed findings of others thatlower baseline serum HBsAg levels predict HBsAg sero-clearance particularly if the HBsAg levels were lt100 IUmL33 Quantification of HBsAg has been adopted as animportant marker of immune control of CHB and has beensuggested to correlate with the covalently close circularDNA levels in the liver In addition a low HBsAg level isassociated with a lower risk of HCC and liver-related mor-tality among HBeAg-negative patients with low viremia38
Although the finding of an association between HBsAglevel and HBsAg seroclearance is a self-fulfilling prophecybecause the level has to decrease before it becomes unde-tectable this has implications for the design of clinical trialsaimed at HBV cure in that randomization must be stratifiedby baseline HBsAg levels
Furthermore we were able to provide pooled HBsAgseroclearance rates for CHB patients from different
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Figure 4 Subgroup anal-ysis of HBsAg seroclear-ance rate by sex baselineHBeAg status and base-line cirrhosis ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 641
CLINICAL
LIVE
R
(eg age HBeAg status cirrhosis HBV DNA study setting)(Supplementary Figures 2 and 3 and SupplementaryTable 3)
Regarding study settings and design the pooled HBsAgseroclearance rate was higher in population-based studies(168 95 CI 086ndash278) than health care servicendashbasedstudies (093 95 CI 072ndash117) but this difference wasnot statistically significant (P frac14 10) (Figure 6) Howeverheterogeneity was high (9874 for population-basedstudies 9670 for health care servicendashbased studies P lt01 for both) Similarly studies that collected data from acommunity-based health care servicendashbased population(134 95 CI 092ndash183) also had higher seroclearancerates than university-based studies (097 95 CI 078ndash118) although the difference again was not statisticallysignificant (P frac14 27)
HBsAg Seroclearance Rates in CHBPatients With Different HBV Genotypes andby Treatment History
There was no significant difference in HBsAg seroclear-ance across different genotypes among more than 10000patients with genotype data (331 patients with genotype A4685 with genotype B 5756 with genotype C 94 with ge-notype D and 231 with genotype F) (Supplementary
Figure 4) The annual seroclearance rates were 126(95 CI 029ndash285) 079 (95 CI 042ndash126) 102(95 CI 071ndash139) 105 (95 CI 043ndash193) and 059(95 CI 039ndash083) for genotypes A B C D and Frespectively Comparative analysis for the 2 largest groupsgenotypes B (n frac14 4685) and C (n frac14 5756) also found nosignificant difference between these 2 groups (P frac14 453) Inaddition there was no significant difference in HBsAgseroclearance between treated (n frac14 7565 082 95 CI034ndash150) and untreated (n frac14 20556 131 95 CI098ndash167) patients (P frac14 195) (Supplementary Figure 5)For the treated group we further subanalyzed HBsAgseroclearance rates by specific treatment regimen and founda higher rate in interferon-treated patients (1 study 3833person-years 180 95 CI 140ndash225) than in entecavir-treated patients (2 studies 1997 person-years 080 95CI 044ndash125) and lamivudine-treated patients (1 study5428 person-years 065 95 CI 045ndash089) There wereno data for patients treated by other nucleos(t)ideanalogues
Sensitivity AnalysisWe performed 5 sensitivity tests In the first we
excluded studies with a fair or high risk of bias (NOS scorelt 7) (Supplementary Figure 6A) The annual seroclearance
Figure 5 The baselinelaboratory data of CHBpatients categorized byachievement of HBsAgseroclearance Data werederived from articles thatprovided baseline resultsin patients who achievedand those who did notachieve HBsAg seroclear-ance during the follow-upperiod ASR annual sero-clearance rate K numberof studies N total numberof CHB patients qHBsAgquantitative hepatitis Bsurface antigen
Figure 6 Subgroup anal-ysis of HBsAg seroclear-ance rate by study regionscale of study and prac-tice settings ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
642 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
rate became higher (109 95 CI 082ndash141) but het-erogeneity remained high (I2 frac14 9770) In the secondsensitivity analysis we omitted 12 studies with smallersample size (n lt 500 patients) (Supplementary Figure 6B)Data from the remaining 22 larger studies showed anannual seroclearance rate of 100 (95 CI 073ndash132) butheterogeneity again remained high (I2 frac14 9830)
In the third sensitivity test to clarify whether thenonlinear increase of cumulative HBsAg seroclearance ratewas associated with the longer follow-up period in thepopulation-based cohort we performed a subgroup analysisand showed that the cumulative incident HBsAg seroclear-ance rates were indeed nonlinear in both population-basedand health care servicendashbased cohorts (SupplementaryFigure 7) In the fourth sensitivity test we subanalyzeddata for studies that confirmed HBsAg seroclearance byrepeated testing and excluded those that did not specifythis The pooled annual seroclearance rate remained similar(111 95 CI 085ndash139) (Supplementary Figure 8)Finally we excluded studies for which we imputed theannual HBsAg seroclearance rate and the pooled annualHBsAg seroclearance rate was 098 (95 CI 074ndash125)
Heterogeneity and Publication BiasThe heterogeneity of the HBsAg seroclearance rate was
severe as evidenced by the high I2 statistics in the pooledannual and 5- 10- and 15-year cumulative seroclearancerates (97 99 99 and 99 respectively)(Supplementary Table 2) Subgroup analysis also showedhigh heterogeneity However as presented by the Eggerrsquostest there was no publication bias in the pooled annualHBsAg seroclearance rates or any of the pooled cumulativeseroclearance rates (Supplementary Table 2)
DiscussionIn this meta-analysis of 34 studies which included
42588 CHB patients with 303754 person-years of follow-up we found that 3194 patients had an incident HBsAgseroclearance event resulting in a pooled HBsAg
seroclearance rate of 102 (95 CI 079ndash127) and con-firming that HBsAg is a rare event In addition by combiningthe published and updated aggregated data we determinedthe 5- 10- and 15-year cumulative seroclearance rates andfound that the rates of seroclearance increased 4-fold byyear 5 (403) further doubled by year 10 (816) anddoubled again by year 15 such that almost 18 of patientshad achieved seroclearance by year 15 after study entryOur finding is consistent with a prior report of a large-scaleprospective study by Chu et al6 in which the rate of HBsAgseroclearance increased in a nonlinear fashion from 81after the first 10 years to 249 after 20 years and to447 after 25 years of follow-up However the severeheterogeneity of our results requires that they be inter-preted with caution
Similar to other single-center studies we found thatpatients who were HBeAg negative at baseline had lowerbaseline HBV DNA levels and had lower quantitative HBsAgexperienced higher rates of HBsAg seroclearance793536
These characteristics are typical of the inactive carrierphase suggesting that these patients are better able tomount an immune response to the virus leading to virologicremission and over time spontaneous HBsAg seroclear-ance3337 Our analysis also confirmed findings of others thatlower baseline serum HBsAg levels predict HBsAg sero-clearance particularly if the HBsAg levels were lt100 IUmL33 Quantification of HBsAg has been adopted as animportant marker of immune control of CHB and has beensuggested to correlate with the covalently close circularDNA levels in the liver In addition a low HBsAg level isassociated with a lower risk of HCC and liver-related mor-tality among HBeAg-negative patients with low viremia38
Although the finding of an association between HBsAglevel and HBsAg seroclearance is a self-fulfilling prophecybecause the level has to decrease before it becomes unde-tectable this has implications for the design of clinical trialsaimed at HBV cure in that randomization must be stratifiedby baseline HBsAg levels
Furthermore we were able to provide pooled HBsAgseroclearance rates for CHB patients from different
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Figure 6 Subgroup anal-ysis of HBsAg seroclear-ance rate by study regionscale of study and prac-tice settings ASR annualseroclearance rate Knumber of studies N totalnumber of CHB patients
642 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
rate became higher (109 95 CI 082ndash141) but het-erogeneity remained high (I2 frac14 9770) In the secondsensitivity analysis we omitted 12 studies with smallersample size (n lt 500 patients) (Supplementary Figure 6B)Data from the remaining 22 larger studies showed anannual seroclearance rate of 100 (95 CI 073ndash132) butheterogeneity again remained high (I2 frac14 9830)
In the third sensitivity test to clarify whether thenonlinear increase of cumulative HBsAg seroclearance ratewas associated with the longer follow-up period in thepopulation-based cohort we performed a subgroup analysisand showed that the cumulative incident HBsAg seroclear-ance rates were indeed nonlinear in both population-basedand health care servicendashbased cohorts (SupplementaryFigure 7) In the fourth sensitivity test we subanalyzeddata for studies that confirmed HBsAg seroclearance byrepeated testing and excluded those that did not specifythis The pooled annual seroclearance rate remained similar(111 95 CI 085ndash139) (Supplementary Figure 8)Finally we excluded studies for which we imputed theannual HBsAg seroclearance rate and the pooled annualHBsAg seroclearance rate was 098 (95 CI 074ndash125)
Heterogeneity and Publication BiasThe heterogeneity of the HBsAg seroclearance rate was
severe as evidenced by the high I2 statistics in the pooledannual and 5- 10- and 15-year cumulative seroclearancerates (97 99 99 and 99 respectively)(Supplementary Table 2) Subgroup analysis also showedhigh heterogeneity However as presented by the Eggerrsquostest there was no publication bias in the pooled annualHBsAg seroclearance rates or any of the pooled cumulativeseroclearance rates (Supplementary Table 2)
DiscussionIn this meta-analysis of 34 studies which included
42588 CHB patients with 303754 person-years of follow-up we found that 3194 patients had an incident HBsAgseroclearance event resulting in a pooled HBsAg
seroclearance rate of 102 (95 CI 079ndash127) and con-firming that HBsAg is a rare event In addition by combiningthe published and updated aggregated data we determinedthe 5- 10- and 15-year cumulative seroclearance rates andfound that the rates of seroclearance increased 4-fold byyear 5 (403) further doubled by year 10 (816) anddoubled again by year 15 such that almost 18 of patientshad achieved seroclearance by year 15 after study entryOur finding is consistent with a prior report of a large-scaleprospective study by Chu et al6 in which the rate of HBsAgseroclearance increased in a nonlinear fashion from 81after the first 10 years to 249 after 20 years and to447 after 25 years of follow-up However the severeheterogeneity of our results requires that they be inter-preted with caution
Similar to other single-center studies we found thatpatients who were HBeAg negative at baseline had lowerbaseline HBV DNA levels and had lower quantitative HBsAgexperienced higher rates of HBsAg seroclearance793536
These characteristics are typical of the inactive carrierphase suggesting that these patients are better able tomount an immune response to the virus leading to virologicremission and over time spontaneous HBsAg seroclear-ance3337 Our analysis also confirmed findings of others thatlower baseline serum HBsAg levels predict HBsAg sero-clearance particularly if the HBsAg levels were lt100 IUmL33 Quantification of HBsAg has been adopted as animportant marker of immune control of CHB and has beensuggested to correlate with the covalently close circularDNA levels in the liver In addition a low HBsAg level isassociated with a lower risk of HCC and liver-related mor-tality among HBeAg-negative patients with low viremia38
Although the finding of an association between HBsAglevel and HBsAg seroclearance is a self-fulfilling prophecybecause the level has to decrease before it becomes unde-tectable this has implications for the design of clinical trialsaimed at HBV cure in that randomization must be stratifiedby baseline HBsAg levels
Furthermore we were able to provide pooled HBsAgseroclearance rates for CHB patients from different
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 643
CLINICAL
LIVE
R
geographic regions providing more specific information forthose making treatment decisions We found that the HBsAgseroclearance rates were higher in the Asian Pacific andEuropean cohorts than in American cohorts We surmisethat these differences may be due to several factorsincluding the small number of studies outside of Asia lack ofadjustment for patient demographic and clinical character-istics and the mixed raceethnicity of the American andEuropean cohorts CHB cohorts in the West and specificallyNorth America comprise patients from diverse raceseth-nicities According to data from the Hepatitis B ResearchNetwork approximately 82 of CHB patients in NorthAmerica are immigrants from highly endemic and diversegeographic areas39 Most cohorts from North America werealso recruited from health care centers with relatively shortfollow-up times which may have contributed to the lowerHBsAg seroclearance rate observed for this region whereasdata from the Asia Pacific region were derived from bothhealth care centers and the community they includedlonger follow-up periods and a higher proportion of studyparticipants had less active disease
Population-based cohorts had a nonsignificant trend(P frac14 10) toward higher pooled HBsAg seroclearance ratesthan studies derived from health care centers As alluded towe believe that these findings are related to the types ofpatients seen in different settings For example the RiskEvaluation of Viral Load Elevation and Associated LiverDiseaseCancer-Hepatitis B Virus (REVEAL-HBV) cohortwas recruited from the community and had a higher pro-portion of patients with negative HBeAg low HBV DNA andolder age7 whereas participants in health care servicendashbased studies may have more active or advanced liverdisease
Regarding the association between HBV genotypes andHBsAg seroclearance we found no statistically significantdifferences in HBsAg seroclearance rates among thedifferent genotypes Numerically genotype A appeared tohave the highest HBsAg seroclearance rate and genotype Fhad the lowest but the number of studies and patients withgenotypes A D and F were small Further analysiscomparing genotype B (n frac14 4685) and C (n frac14 5756) pa-tients also found no significant difference in HBsAg sero-clearance rate These results will be helpful to cliniciansbecause results of previous studies were conflicting withseveral studies suggesting no association between HBsAgseroclearance and HBV genotype but another suggestingthat patients with genotype B had a higher rate of HBsAgseroclearance than those with genotype C and yet anothersuggesting that genotype C was associated with a higherlifetime chance of HBsAg loss than genotype B33363740
With regard to antiviral therapy a recent meta-analysisreported the HBsAg seroclearance rate to be as high as9 in patients who received combination pegylated inter-feron plus nucleos(t)ide therapy41 However the reviewincluded many studies with small sample sizes (1824included studies had a sample size of lt200 patients) Wealso compared the pooled seroclearance rates betweentreated and untreated cohorts We were able to include7565 treated (treatment-naiumlve and initiated therapy at
study entry) and 20556 never-treated patients to examinethe effect of treatment on HBsAg seroclearance rates Wedid not find a statistically significant difference in HBsAgseroclearance rates between treated and untreated patientsDespite our attempts to include studies of only untreatedpatients and studies of only treated patients who wereinitially treatment naiumlve there was still severe heterogene-ity in both the treated and untreated groups In addition themajority of treated patients included in the analysisreceived lamivudine or entecavir with no data for tenofovirIn another subanalysis which was limited by the smallnumber of studies we showed that interferon-treated pa-tients had a significantly higher HBsAg seroclearance ratethan nucleoside analogue-treated patients and this isconsistent with the results from prior clinical trials4243 Alarger cohort study or individual patient data meta-analysiswith appropriate adjustment for confounders is needed todetermine the long-term effect of treatment on HBsAgseroclearance
The strength of our study is that to our knowledge it isthe most comprehensive systematic review and meta-analysis of annual and cumulative real-world HBsAg sero-clearance rate to date We included articles published from1998 through 2017 from 14 countries By pooling the datafrom the existing literature we were able to enhance thestatistical power in estimating this rare event Moreoverupdated aggregated data from the authors of 19 includedstudies allowed us to meta-analyze data with updatedfollow-up periods and to perform detailed subgroup ana-lyses with larger sample sizes We excluded data fromrandomized controlled trials so our estimates provideincidence rates in more generalized patient populations
Our study also has limitations that warrant attentionFirst there were no articles from Africa and only 1 articlefrom South America which limits generalization of ourfindings to these geographic regions Second because of thenature of the meta-analysis of aggregated data variablessuch as age and their potential effects on study outcomescould not be studied because reported data representedonly the average results of the included cohorts For thesame reason we were not able to adjust for HBeAg statusbaseline quantitative HBsAg and HBV DNA levels Thirdonly slightly more than half of the included studies met thecriteria for low risk of bias but we performed a sensitivityanalysis of only studies with a low risk of bias and found asimilar pooled estimate as the main result Fourthpopulation-based and health care servicendashbased cohortsmay differ such that community cohort participants aremore likely to be HBeAg negative and have lower level ofdisease activity factors associated with higher rates ofHBsAg seroclearance Our subgroup analysis showed thatthe HBsAg seroclearance rate was higher in population-based community cohorts than health care center cohortsalthough the differences were not statistically differentFifth some cohorts included both treated and untreatedpatients To clarify the impact of treatment we performedsensitivity analysis comparing studies that included onlypreviously treatment-naiumlve patients who initiated treatmentat entry to the study vs studies that included only patients
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
644 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
who never received treatment We found that the rates ofHBsAg seroclearance were similar but we acknowledge thatthe baseline characteristics of treated and untreated pa-tients are likely to be different and that a true impact oftreatment might have been missed Sixth because of lack ofindividual level data we did not evaluate HBsAg sero-clearance rates in patients who were HBeAg positive atbaseline some of whom may have undergone HBeAg sero-conversion during follow-up Finally the pooled annual andcumulative seroclearance rates should be interpreted withcaution because they showed high heterogeneity despiteour attempt to mitigate it with subgroup and sensitivityanalyses
In conclusion in this systematic review and meta-analysis we determined that the incident rate of HBsAgseroclearance was a rare event such that by year 15 afterstudy entry less than 20 of patients had cleared HBsAgPatients who tested negative for HBeAg had a low level ofHBV DNA and had low quantitative HBsAg levels at baselinewere more likely to achieve HBsAg seroclearance HBV ge-notype and the use of currently available oral antiviraltherapy did not seem to have a substantial impact on HBsAgseroclearance although additional studies are needed tofurther examine these factors Our data have implications inthe design of clinical trials aimed at HBsAg seroclearanceproviding information on background event rate and factorsto stratify for to ensure balance between treatment groupsand assisting the clinician in discussing the need for lifelongtherapy for most of their patients
Supplementary MaterialNote To access the supplementary material accompanyingthis article visit the online version of Gastroenterology atwwwgastrojournalorg and at httpsdoiorg101053jgastro201810027
References
1 World Health Organization Global Hepatitis Report
2017 Geneva Switzerland World Health Organization2017
2 Lok AS Zoulim F Dusheiko G et al Hepatitis B curefrom discovery to regulatory approval Hepatology 2017661296ndash1313
3 Chen YC Sheen IS Chu CM et al Prognosis followingspontaneous HBsAg seroclearance in chronic hepatitis Bpatients with or without concurrent infection Gastroen-terology 20021231084ndash1089
4 Chung HT Lai CL Lok AS Pathogenic role of hepatitis Bvirus in hepatitis B surface antigen-negative decom-pensated cirrhosis Hepatology 19952225ndash29
5 Yuen MFWong DK Fung J et al HBsAg seroclearancein chronic hepatitis B in Asian patients replicative leveland risk of hepatocellular carcinoma Gastroenterology20081351192ndash1199
6 Chu CM Liaw YF HBsAg seroclearance in asymptom-atic carriers of high endemic areas appreciably highrates during a long-term follow-up Hepatology 2007451187ndash1192
7 Liu J Yang HI Lee MH et al Incidence and de-terminants of spontaneous hepatitis B surface antigenseroclearance a community-based follow-up studyGastroenterology 2010139474ndash482
8 Sanchez-Tapias JM Costa J Mas A et al Influence ofhepatitis B virus genotype on the long-term outcome ofchronic hepatitis B in western patients Gastroenterology20021231848ndash1856
9 Kim GA Lim YS An J et al HBsAg seroclearance afternucleoside analogue therapy in patients with chronichepatitis B clinical outcomes and durability Gut 2014631325ndash1332
10 Moher D Shamseer L Clarke M et al Preferred report-ing items for systematic review and meta-analysis pro-tocols (PRISMA-P) 2015 statement Syst Rev 201541
11 Wells G Shea BJ OrsquoConnell D et al The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses 2018 Availablefrom httpwwwohricaprogramsclinical_epidemiologyoxfordasp Accessed February 2 2018
12 DerSimonian R Laird N Meta-analysis in clinical trialsControl Clin Trials 19867177ndash188
13 Tukey JW Freeman MF Transformations related to theangular and the square root Ann Appl Stat 195021607ndash611
14 Miller JJ The inverse of the FreemanndashTukey doublearcsine transformation Am Stat 197832138
15 Higgins JP Thompson SG Deeks JJ et al Measuringinconsistency in meta-analyses BMJ 2003327557ndash560
16 Schwarzer G General package for meta-analysis 201817 Charatcharoenwitthaya P Sukeepaisarnjaroen W
Piratvisuth T et al Treatment outcomes and validation ofthe stopping rule for response to peginterferon in chronichepatitis B a Thai nationwide cohort studyJ Gastroenterol Hepatol 2016311874ndash1881
18 Fung J Wong DK Seto WK et al Hepatitis Bsurface antigen seroclearance Relationship to hepatitisB e-antigen seroclearance and hepatitis B e-antigen-negative hepatitis Am J Gastroenterol 20141091764ndash1770
19 Hosaka T Suzuki F Kobayashi M et al Clearance ofhepatitis B surface antigen during long-term nucleot(s)ide analog treatment in chronic hepatitis B results from anine-year longitudinal study J Gastroenterol 201348930ndash941
20 Kobayashi M Hosaka T Suzuki F et al Seroclearancerate of hepatitis B surface antigen in 2112 patients withchronic hepatitis in Japan during long-term follow-upJ Gastroenterol 201449538ndash546
21 Kwak MS Cho EJ Jang ES et al Predictors of HBsAgseroclearance in HBeAg-negative chronic hepatitis Bpatients Digestion 201184(Suppl 1)23ndash28
22 Lauret E Gonzalez-Dieguez ML Rodriguez M et alLong-term outcome in Caucasian patients with chronichepatitis B virus infection after HBsAg seroclearanceLiver Int 201535140ndash147
23 Lim TH Gane E Moyes C et al Serological and clinicaloutcomes of horizontally transmitted chronic hepatitis Binfection in New Zealand Maori results from a 28-yearfollow-up study Gut 201564966ndash972
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 645
CLINICAL
LIVE
R
24 Luo J Li X Wu Y et al Efficacy of entecavir treatment forup to 5 years in nucleos(t)ide-naive chronic hepatitis Bpatients in real life Int J Med Sci 201310427ndash433
25 Treeprasertsuk S Tanwandee T Piratvisuth T et alNatural history outcome and sustainability of treatmentresponse in chronic viral hepatitis B Thai multicenterstudy Asian Biomed 20137599ndash607
26 Nguyen LH Hoang J Nguyen NH et al Ethnic differ-ences in incidence of hepatitis B surface antigen sero-clearance in a real-life multicenter clinical cohort of 4737patients with chronic hepatitis B infection AlimentPharmacol Ther 201644390ndash399
27 Orito E Hasebe C Kurosaki M et al Risk of hepato-cellular carcinoma in cirrhotic hepatitis B virus patientsduring nucleosidenucleotide analog therapy HepatolRes 201545872ndash879
28 Park YM Lee SG Clinical features of HBsAg seroclear-ance in hepatitis B virus carriers in South Korea aretrospective longitudinal study World J Gastroenterol2016229836ndash9843
29 Preda CM Baicus C Negreanu L et al Effectiveness ofentecavir treatment and predictive factors for virologicresponse Rev Esp Enferm Dig 2014106305ndash311
30 Riveiro-Barciela M Tabernero D Calleja JL et al Effec-tiveness and safety of entecavir or tenofovir in a Spanishcohort of chronic hepatitis B patients validation of thePage-B score to predict hepatocellular carcinoma DigDis Sci 201762784ndash793
31 Suzuki F Arase Y Suzuki Y et al Long-term efficacy ofinterferon therapy in patients with chronic hepatitis Bvirus infection in Japan J Gastroenterol 201247814ndash822
32 Tai DI Tsay PK Chen WT et al Relative roles of HBsAgseroclearance and mortality in the decline of HBsAgprevalence with increasing age Am J Gastroenterol20101051102ndash1109
33 Tseng TC Liu CJ Chen CL et al Higher lifetime chanceof spontaneous surface antigen loss in hepatitis B car-riers with genotype C infection Aliment Pharmacol Ther201541949ndash960
34 Ungtrakul T Sriprayoon T Kusuman P et al Role ofquantitative hepatitis B surface antigen in predictinginactive carriers and HBsAg seroclearance in HBeAg-negative chronic hepatitis B patients Medicine(Baltimore) 201796e6554
35 Chan HL Wong GL Tse CH et al Viral determinants ofhepatitis B surface antigen seroclearance in hepatitis B eantigen-negative chronic hepatitis B patients J Infect Dis2011204408ndash414
36 Simonetti J Bulkow L McMahon BJ et al Clearance ofhepatitis B surface antigen and risk of hepatocellularcarcinoma in a cohort chronically infected with hepatitisB virus Hepatology 2010511531ndash1537
37 Liu J Lee MH Batrla-Utermann R et al A predictivescoring system for the seroclearance of HBsAg inHBeAg-seronegative chronic hepatitis B patients withgenotype B or C infection J Hepatol 201358853ndash860
38 Tseng TC Liu CJ Chen CL et al Risk stratificationof hepatocellular carcinoma in hepatitis B virus
e antigen-negative carriers by combining viral bio-markers J Infect Dis 2013208584ndash593
39 Ghany MG Perrillo R Li R et al Characteristics of adultsin the hepatitis B research network in North Americareflect their country of origin and hepatitis B virus ge-notype Clin Gastroenterol Hepatol 201513183ndash192
40 Yuen MF Wong DK Sablon E et al HBsAg seroclear-ance in chronic hepatitis B in the Chinese virologicalhistological and clinical aspects Hepatology 2004391694ndash1701
41 Qiu K Liu B Li SY et al Systematic review with meta-analysis combination treatment of regimens based onpegylated interferon for chronic hepatitis B focusing onhepatitis B surface antigen clearance Aliment PharmacolTher 2018471340ndash1348
42 Lau GK Piratvisuth T Luo KX et al Peginterferon Alfa-2a lamivudine and the combination for HBeAg-positive chronic hepatitis B N Engl J Med 20053522682ndash2695
43 Marcellin P Lau GK Bonino F et al Peginterferon alfa-2a alone lamivudine alone and the two in combinationin patients with HBeAg-negative chronic hepatitis BN Engl J Med 20043511206ndash1217
44 Yapali S Talaat N Fontana RJ et al Outcomes of pa-tients with chronic hepatitis B who do not meet criteriafor antiviral treatment at presentation Clin GastroenterolHepatol 201513193ndash201 httpsdoiorg101016jcgh201407019
45 Habersetzer F Moenne-Loccoz R Meyer N et alLoss of hepatitis B surface antigen in a real-life clinicalcohort of patients with chronic hepatitis B virus infec-tion Liver Int 201535130ndash139 httpsdoiorg101111liv12661
46 Farzi H Ebrahimi Daryani N et al Prognostic valuesof fluctuations in serum levels of alanine transaminasein inactive carrier state of HBV infection Hepat Mon201414(5)e17537 httpsdoiorg105812hepatmon17537
47 Arai M Togo S Kanda T et al Quantification of hepatitisB surface antigen can help predict spontaneous hepatitisB surface antigen seroclearance Eur J GastroenterolHepatol 201224414ndash418 httpsdoiorg101097MEG0b013e328350594d
48 Ahn SH Park YN Park JY et al Long-term clinical andhistological outcomes in patients with spontaneoushepatitis B surface antigen seroclearance J Hepatol200542188ndash194 httpsdoiorg101016jjhep200410026
49 Ferreira SC Chacha SG Souza FF et al Factors asso-ciated with spontaneous HBsAg clearance in chronichepatitis B patients followed at a university hospital AnnHepatol 201413762ndash770
50 Han ZG Qie ZH Qiao WZ HBsAg spontaneous sero-clearance in a cohort of HBeAg-seronegative patientswith chronic hepatitis B virus infection J Med Virol 20168879ndash85 httpsdoiorg101002jmv24311
51 Nagaoka S Abiru S Komori A et al Hepatic flarespromote rapid decline of serum hepatitis B surface an-tigen (HBsAg) in patients with HBsAg seroclearance a
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
646 Yeo et al Gastroenterology Vol 156 No 3
CLINICALLIVER
long-term follow-up study Hepatol Res 201646(3)E89ndashE99 httpsdoiorg101111hepr12533
52 Ari A Calik S Tosun S et al A persistently low HBV DNAlevel is a predictor of spontaneous HBsAg clearance inpatients with chronic hepatitis B Turk J Med Sci 20164648ndash52 httpsdoiorg103906sag-1411-156
53 Nam SW Jung JJ Bae SH et al Clinical outcomes ofdelayedclearanceof serumHBsAG inpatientswith chronicHBV infection Korean J Intern Med 20072273ndash76
54 Lu ZH Chen W Ju ZC et al Pathological features andprognosis in chronic hepatitis B virus carriers J Int MedRes 20113971ndash77 httpsdoiorg101177147323001103900109
55 Huo TI Wu JC Lee PC et al Sero-clearance of hepatitisB surface antigen in chronic carriers does not necessarilyimply a good prognosis Hepatology 199828231ndash236httpsdoiorg101002hep510280130
Author names in bold designate shared co-first authorship
Received July 18 2018 Accepted October 9 2018
Reprints requestsAddress requests for reprints to Mindie H Nguyen MD MAS Division ofGastroenterology and Hepatology Stanford University Medical Center 750Welch Road Suite 210 Palo Alto California 94304 e-mailmindiehnstanfordedu or Chun-Ying Wu MD PhD MPH LLM LLBDivision of Translational Research Taipei Veterans General Hospital No201 Section 2 Shipai Road Beitou District Taipei City Taiwan e-mailcywu22vghtpegovtw
AcknowledgmentsAuthor contributions YHY ASL CYW and MHN study design YHY MHLBW BZ AL DJ NC LK CCL systematic literature search and dataextraction HIY TCT HNT MSK YMP JYYF MB MR ST CMP TU PC
XL JL JZ TH MRB DP FS MK TS YC TT MFY HSL JHK MHNacquisition and contribution of original data YHY HJH CYW and MHNstatistical analyses YHY and MHN drafting of the manuscript ASL criticalrevision of the manuscript MHN study conception and study supervision allauthors data interpretation and critical review of the manuscript forimportant intellectual content
Conflicts of interestThe authors disclose the following Tai-Chung Tseng received researchsupport from the Ministry of Science and Technology Executive YuanTaiwan (MOST 105-2314-B-303-008) and National Taiwan UniversityHospital Taipei Taiwan (NTUH 106-003626) and received speaking feesfrom AbbVie Bristol-Myers Squibb and Gilead Sciences Huy N Trinhreceived research support from Gilead served on a consultancyadvisoryboard for Gilead received speaking fees from Gilead and holds stock inGilead James Yan Yue Fung received research support from NovartisMaria Buti received research support from Gilead served on consultancyadvisory boards for Gilead AbbVie and Merck Sharp amp Dohme andreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeManuel Rodriacuteguez served on a consultancyadvisory board for Gileadreceived speaking fees from Gilead AbbVie and Merck Sharp amp DohmeCarmen Monica Preda received research support from Roche Bristol-MyersSquibb and Merck Sharp amp Dohme and received speaking fees fromBristol-Myers Squibb Teerapat Ungtrakul received research support fromAstraZeneca and received speaking fees from AstraZeneca Mar Riveiro-Barciela received research support from Gilead and received speaking feesfrom Gilead and Merck Sharp amp Dohme Fumitaka Suzuki received speakingfees from Bristol-Myers Squibb Tawesak Tanwandee received researchsupport from Roche Merck and Contravir Man-Fung Yuen receivedresearch support andor served on consultancyadvisory boards for AbbVieArrowhead Pharmaceuticals Biocartis Bristol-Myers Squibb FujirebioGilead Sciences GlaxoSmithKline LF Asia Limited Merck Sharp amp DohmeNovartis Pharmaceuticals Roche and Sysmex Corporation Jia-Horng Kaoserved on consultancyadvisory boards for AbbVie Bristol-Myers SquibbGilead Sciences and Merck Sharp amp Dohme and received speaking feesfrom AbbVie Ascletis Bristol-Myers Squibb Gilead Sciences and MerckSharp amp Dohme Anna S Lok received research support from Bristol-MyersSquibb and Gilead and served on consultancyadvisory boards for RocheSpring Banks Viravaxx and Resverlogix Mindie H Nguyen receivedresearch support from Pfizer Gilead Sciences Janssen National CancerInstitute and BK Kee Foundation and served on consultingadvisoryboards for Anylam Janssen Intercept Spring Banks Bayer GileadDynavax Eisai Exact Sciences and Novartis The remaining authorsdisclose no conflicts
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Supplementary Methods
PubMed(hepatitis B chronic [MeSH] OR HBV [Tiab] OR hepatitis
B [Tiab] OR cirrhosis [MeSH] OR cirrhosis [Tiab] OR hepa-tocellular carcinoma [MeSH] OR liver neoplasms[MeSH]OR liver cancer [Tiab] OR liver transplantation [MeSH] ORhepatic transplantation [Tiab] NOT metastasis [Tiab]) AND(hepatitis B surface antigens [MeSH] OR hepatitis B surfaceantigen [Tiab] OR HBsAg [Tiab] OR HBs antigen [Tiab]) AND(seroclearance [Tiab] OR seroconversion [Tiab] OR loss[Tiab]) NOT (comment [publication type] OR editorial[publication type] OR review [publication type])
Embase
1 Hepatitis B2 Hepatitis B virus3 Hepatitis B virus X protein4 exp Hepatitis B antibody5 (hepatitis adj2 B)tiab6 (HBV or CHB or hep B or hepB)tiab7 Or1-68 liver cell carcinoma9 liver carcinoma10 liver cancer11 (hepatoma or hepatocarcinoma or hcc)tiab12 ((hepatocellular or liver or hepatic or hepato) adj2 (cancer or
carcinoma or neoplasm))tiab13 Or8-1214 exp liver cirrhosis15 fibrosis and liver16 (((liver or hepat) adj5 fibro) or cirrho)tiab17 Or14-1618 exp liver transplantation19 ((liver or hepatic) adj3 (transplan or graft))mp20 18 OR 1921 (Metastasis)tiab22 7 OR 13 OR 17 OR 20 NOT 2123 (Hepatitis B Surface Antigens)tiab24 (hbs Antigens)tiab25 (hbsag)tiab26 23 OR 24 OR 2527 seroclearance28 loss29 seroconversion30 27 OR 28 OR 2931 22 AND 26 AND 2932 (ANIMALSDE OR NONHUMANSDE) NOT (HUMANSDE OR
HUMAN-DE)33 31 NOT 3234 (systematic review)tiab35 (meta-analysis)tiab36 34 OR 3537 33 NOT 36
Cochrane Library(hepatitis brdquo OR ldquoHBVrdquo OR ldquohep Brdquo) AND (ldquohepatitis B
surface antigenrdquo OR ldquohbsagrdquo) AND (seroclear OR loss)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e1
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Supplementary Figure 1 Subgroup analysis of HBsAg seroclearance rate by mean age See Table 1 for full study detailsASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
646e2 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Supplementary Figure 2 Subgroup analysis of HBsAg seroclearance rate by sex baseline HBeAg status and baselinecirrhosis stratified by study region ASR annual seroclearance rate K number of studies N total number of CHB patients
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e3
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Supplementary Figure 3 The baseline laboratory data CHB patients categorized by achievement of HBsAg seroclearancestratified by study region K number of studies N total number of CHB patients qHBsAg quantitative hepatitis B surfaceantigen
646e4 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Supplementary Figure 4 Subgroup Analysis of HBsAg Seroclearance Rate by Genotype ASR annual seroclearance rate Knumber of studies N total number of CHB patients
Supplementary Figure 5 Subgroup analysis of HBsAg seroclearance rate by treatment history ASR annual seroclearancerate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e5
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Supplementary Figure 6 (A) Sensitivity analysis by excluding articles with high risk of bias (NOS lt 7) (B) Sensitivity analysisby excluding articles with sample size lt500 patients ASR annual seroclearance rate SCl total number of patients withincident HBsAg seroclearance
Supplementary Figure 7 Subgroup analysis of cumulative HBsAg seroclearance rate by scale of study CIR denotescumulative incidence rate of HBsAg seroclearance
646e6 Yeo et al Gastroenterology Vol 156 No 3
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients
Community Asia pacific 6 7765 092 (048ndash149) 097Non-Asia Pacific 2 1670 150 (111ndash195)
University Asia pacific 11 7541 114 (077ndash158) 301Non-Asia Pacific 5 1980 090 (068ndash115)
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e9
Factors Associated With Rates of HBsAg Seroclearance in Adults With Chronic HBV Infection A Systematic Review and Meta-ana
Methods
What You Need to Know
Outline placeholder
Search Strategy and Study Selection
Data Extraction
Risk-of-Bias Assessment
Outcomes
Statistical Analysis
Results
Characteristics of Included Studies
Overall Annual Seroclearance and Cumulative Incidence
Annual Seroclearance Rate by Baseline Demographic and Clinical Characteristics
Baseline Laboratory Parameters in Patients With HBsAg Seroclearance vs Those Without HBsAg Seroclearance
Region Scale and Setting of Studies
HBsAg Seroclearance Rates in CHB Patients With Different HBV Genotypes and by Treatment History
Sensitivity Analysis
Heterogeneity and Publication Bias
Discussion
Supplementary Material
References
Acknowledgments
Supplementary Methods
PubMed
Embase
Cochrane Library
Supplementary Figure 8 Sensitivity analysis by excluding articles without repeat testing to confirm HBsAg seroclearanceASR annual seroclearance rate SP total number of patients with incident HBsAg seroclearance
February 2019 HBsAg Seroclearance in Adults With Chronic HBV Infection 646e7
Supplementary Table 2The Annual HBsAg Seroclearance Rate and 5- 10- and 15-Year Cumulative Seroclearance Rate inChronic Hepatitis B Patients