Gastrointestinal Drugs Advisory Committee Introductory Remarks NDA203214 Tofacitinib: treatment of adults with moderate to severely active ulcerative colitis Tara Altepeter, MD Clinical Team Leader Division of Gastroenterology and Inborn Errors Products Office of Drug Evaluation III Center for Drug Evaluation and Research, FDA
NDA203214Tofacitinib: treatment of adults with moderate to severely active ulcerative colitis
Tara Altepeter, MDClinical Team Leader
Division of Gastroenterology and Inborn Errors Products
Office of Drug Evaluation III
Center for Drug Evaluation and Research, FDA
2
Disease Overview• Ulcerative colitis (UC) is a chronic, inflammatory disease affecting the
colon• Currently there is no cure• More than 900,000 US adults are affected• Patients experience recurrent flares of abdominal pain and bloody
diarrhea, which may be associated with various extra-intestinal manifestations
• Available treatments are aimed at controlling symptoms, reducing complications, avoiding the need for surgery, and reducing the long term risk of colon cancer
– Treatment of adults with moderate to severely active UC who have had inadequate response, loss of response, or intolerance to: corticosteroids, azathioprine (AZA), 6-mercaptopurine (6-MP), or tumor necrosis factor (TNF) blocker therapy.
4
FDA Approved
Treatments
Year of Approval
ClassEfficacy Information
Clinical RemissionBoxed Warning
Infliximab
(Remicade®)2005
TNF blocker
Study 1: 32% -39% at Week 8
20% at Week 8, 30 and 54
Study 2: 28-34% at Week 8
Serious infections including tuberculosis (TB),malignancies, hepatitis B virus reactivation, hepatotoxicity, hypersensitivity, cytopenias, demyelinating disease, heart failure, lupus-like syndrome
Adalimumab
(Humira®)2011
TNF blocker
Study I: 18.5% at week 8
Study II: 16.5% at Week 8.
8.5% at both Weeks 8 and 52
Serious infections including TB, bacterial sepsis, invasive
fungal infections, and opportunistic infections,
malignancies, anaphylaxis or serious allergic reactions,
hepatitis B virus reactivation, demyelinating disease,
• Ulcerative Colitis – Application submitted on May 4, 2017
6
Drug Development Considerations in Inflammatory Bowel Disease
• Phase 2 – Adequate dose finding
– Exploration of time to response/remission
• Phase 3– Confirmation of efficacy and broader understanding of
safety
– Relevant subgroup analyses
7
Applicant’s Proposed DosingAdults with moderate to severely active UC who have had inadequate response, loss of response, or intolerance to: corticosteroids, azathioprine, 6-mercaptopurine, or TNF blocker therapy.
• Induction: – 10 mg twice daily for 8 weeks– For patients who do not achieve adequate therapeutic benefit (response) by Week 8, the induction dose
of 10 mg twice daily can be extended for an additional 8 weeks (16 weeks total). – Discontinue therapy in patients who do not achieve adequate therapeutic benefit by Week 16.
• Maintenance: – 5 mg twice daily– For those with an inadequate response, loss of response, or intolerance to TNF blocker therapy: 10 mg
twice daily
8
Questions to Committee (1):1) The Applicant has proposed an induction dosing regimen of 10 mg BID for a total for 16 Weeks in patients who have not achieved “adequate therapeutic benefit” by Week 8 based on exploratory analyses of trial data in patients who continued induction treatment when they had not achieved clinical response defined as a decrease from baseline in Mayo score of ≥3 points and ≥ 30%, with an accompanying decrease in the subscore of rectal bleeding of ≥ 1 point or absolute subscore for rectal bleeding of 0 or 1.
a) Discuss the adequacy of the efficacy data to support the use of the 10 mg BID dosing for extended induction therapy for a total of 16 weeks in patients who have not achieved “adequate therapeutic benefit” by Week 8.
b) Discuss the adequacy of the safety data to support the use of the 10 mg BID dosing for induction for a total of 16 weeks in patients who have not achieved “adequate therapeutic benefit” by Week 8.
c) Do you recommend the inclusion of this dosing regimen for this population in the product label?
d) If you recommend inclusion of this dosing regimen in the product label, discuss how inadequate therapeutic benefit that merits extension of induction treatment should be distinguished from inadequate therapeutic benefit that should prompt discontinuation of tofacitinib therapy.
9
Questions to Committee (2):2) For adult patients with moderately to severely active UC with an inadequate response, loss of response, or intolerance to TNF blocker therapy:
a) Discuss the adequacy of the efficacy data to support the use of the 10 mg BID dosing as continuous maintenance treatment.
b) Discuss the adequacy of the safety data to support the use of the 10 mg BID dosing as continuous maintenance treatment.
c) Do you recommend inclusion of this dosing regimen for this population in the product label?
d) Do you recommend that the Applicant conduct a post-marketing efficacy trial in this population comparing a 10 mg BID continuous dosing regimen vs a regimen of 10 mg induction and 5mg BID as maintenance?
10
Questions to Committee (3):3) For discussion (non-voting):
– Discuss if additional post-marketing evaluation of safety is warranted, and the mechanism(s) you recommend (e.g., registry, observational study, etc.) for such evaluation.
4) For discussion (non-voting):
a) Are there unique characteristics of the pediatric UC population that should be taken into account when planning the tofacitinib pediatric development program? In particular, consider the ontogeny of the immune system and the described mechanism of action of tofacitinib.
b) Given the safety concerns (malignancy and serious infections) described with long term use of 10mg BID and the severity of UC in the pediatric population, please recommend the maximum dose that should be targeted for evaluation for long term treatment in pediatric UC.
c) Discuss whether you recommend limiting enrollment in the pediatric trials (and subsequent pediatric indications) to patients who have failed other biologic therapies.
FDA Gastrointestinal Drugs Advisory Committee (GIDAC)
Introduction of FDA Speakers and Presentations
NDA 203214
Tofacitinib for the Treatment of Adult Patients with Moderately to Severely Active Ulcerative Colitis (UC)
Lesley S. Hanes, MD MSc
Division of Gastroenterology and Inborn Errors Products
• Dose Selection Rationale for Phase 3 Induction Studies
• Exposure–Response Analysis for Efficacy in Maintenance Trial
www.fda.gov
19
Phase 2 Dose-Ranging Trial for Induction
www.fda.gov
Ran
do
miz
atio
n 10 mg BID
3 mg BID
Placebo BID
0.5 mg BID
15 mg BID
Weeks 0 2-1-3 4 128-2
Efficacy Follow-Up
Safety
End
of
Tre
atm
en
t
Screening
Week -1 to -3
Study 1063
20
Dose-Response for Induction in Phase 2 Trial
www.fda.gov
Treatment DosePlacebo
(N=40)
0.5 mg
(N= 27)
3 mg
(N=31)
10 mg
(N=30)
15 mg
(N=45)
Clinical Response
(Primary Endpoint)47.5% 29.6% 51.6% 63.6% 80%
Clinical Remission
(Secondary Endpoint)12.2% 7.4% 35.5% 50% 42.2%
• Clinical Response: a decrease from baseline in Mayo score of > 3 points and > 30%, with an
accompanying decrease in the subscore for rectal bleeding of > 1 point or an absolute subscore for rectal
bleeding of 0 or 1
• Clinical Remission: a total Mayo score < 2 points, with no individual subscore exceeding 1 point
Study 1063
21
Exposure-Response for Induction of Clinical Remission at Week 8 in Phase 2 Trial
www.fda.gov
Pro
bab
ility
to
Ach
ieve
Clin
ical
Re
mis
sio
n
Study 1063
22
Dose Selection for Phase 3 Trials
• The dose-response and exposure-response relationship in phase 2 trial supported the selection of 10 mg BID dose for induction of remission in phase 3 trials.
23
Would 5 mg BID Dose be as Efficacious as 10 mg BID Dose for Induction of Remission?
www.fda.gov
24
Predicted Induction of Remission Rate at Week 8 for 5 mg BID
www.fda.gov
Probability (%)(95% CI)
Placebo 5 mg BID(Cavg=16.8 ng/mL)
10 mg BID(Cavg=33.6 ng/mL)
Observed Remission
6.5(3.6-10.6)
19.0(16.4-21.8)
Model-Predicted Remission
6.4(3.2-9.7)
12.8(9.2-16.4)
19.1(16.3-21.9)
• Remission: a total Mayo score < 2 points, with no individual subscore exceeding 1 point and a rectal
bleeding subscore of 0
Exposure-Response Analysis using Pooled Phase 3 Data
25
Outline
• Exposure Comparison Among Disease Populations
• Dose Selection Rationale for Phase 3 Induction Studies
• Exposure–Response Analysis for Efficacy in Maintenance Trial
www.fda.gov
26
Model-Predicted Remission Rate at Week 52 by Baseline Remitter Status following Induction Treatment
www.fda.gov
Study 1096
27
Model-Predicted Remission Rate at Weeks 24 and 52by Prior TNF blocker Responder Status
www.fda.gov
Study 1096
28
Summary• UC patients have similar systemic exposure to patients with plaque
psoriasis and psoriatic arthritis and about 20% lower exposure than rheumatoid arthritis patients at both 5 mg BID and 10 mg BID doses.
• The dose/exposure dependent increase in clinical remission rate supported the selection of 10 mg BID dose for induction treatment in phase 3 trials.
• In maintenance treatment, the 10 mg BID dose showed numerically higher remission rate at week 52 than the 5 mg BID dose regardless of baseline remitter status or prior TNF blocker responder status.
www.fda.gov
NDA 203214Tofacitinib (Xeljanz)
Analyses of Efficacy Data for Proposed Dosing Regimens
Sara Jimenez, PhDOffice of Biostatistics, CDER
March 8, 2018
31
Outline• Overview of studies in the New Drug Application (NDA)
• Dosing regimens for ulcerative colitis (UC)
• Evidence regarding the applicant’s additional dosing regimens for two subgroups
o Induction non-responders
o TNF blocker failures
32
Overview of Studies
www.fda.gov
33
Overview of Study Designs
Source: PMAR-EQDD-A392i-sNDA-514 Figure 1
34
Studies 1094, 1095 Primary and (Key) Secondary Efficacy Endpoints at Week 8
Source: Study 1094 CSR Table 16, Study 1095 CSR Table 16, reviewer’s analysis
35
Study 1096 Primary and (Key) Secondary Efficacy Endpoints at Week 52
Endpoint
Placebo
N=198
n (%)
[95% CI]
Tofacitinib 5
mg BID
N=198
n (%)
[95% CI]
Difference from Placebo
Tofacitinib 10
mg BID
N=197
n (%)
[95% CI]
Difference from
Placebo
Difference
(95% CI) P-value
Difference
(95% CI) P-value
Primary
(remission)
22 (11.1)
[6.7, 15.5]
68 (34.3)
[27.7, 41.0]
23.2
(15.3, 31.2) <0.0001
80 (40.6)
[33.8, 47.5]
29.5
(21.4, 37.6) <0.0001
(Key)
Secondary
(“mucosal
healing”)
26 (13.1)
[8.4, 17.8]
74 (37.4)
[30.6, 44.5]
24.2
(16.0,32.5) <0.0001
90 (45.7)
[38.7, 52.6]
32.6
(24.2, 41.0) <0.0001
(Key)
Secondary
(sustained
steroid-free
remission)
3 (5.1)
[0.0, 10.7]
(n=59)
23 (35.4)
[23.8, 47.0]
(n=65) 30.3
(17.4,43.2) <0.0001
26 (47.3)
[34.1, 60.5]
(n=55)
42.2
(27.9, 56.5) <0.0001
Source: Study 1096 CSR: Table 21, Table 24, Table 27; reviewer’s analysis; based on full analysis set (FAS)
The effects of the tofacitinib 5mg BID and 10mg BID doses were not statistically different for primary and (key) secondary endpoints at a nominal alpha level of 0.05
• For patients who do not achieve adequate therapeutic benefit by week 8 (induction non-responders), the induction dose of 10 mg BID can be extended for an additional 8 weeks (16 weeks total), followed by 5 mg BID for maintenance
• Discontinue therapy in patients who do not achieve adequate therapeutic benefit by week 16
• For patients with moderately to severely active UC with an inadequate response, loss of response, or intolerance to TNF blocker therapy, 10 mg BID for maintenance may be considered in order to maintain therapeutic benefit
o Refractory patients are defined as those with a history of prior TNF blocker failure
www.fda.gov
41
Induction Non-responders• Remission results for
o Locally read endoscopies
o Centrally read endoscopies
• Focus on patients with 16 weeks (active treatment during induction) of tofacitinib 10mg BID
42
Exploratory Analyses for Induction Non-responders
• Patients in Study 1094/1095 who did not achieve clinical response by week 8, and who were then treated with an additional 8 weeks of tofacitinib 10mg BID in the open-label extension Study 1139
• Patients in this group may have received o 8 weeks (placebo during induction) of tofacitinib 10mg
BID, or o 16 weeks (active treatment during induction) of tofacitinib
10mg BID
www.fda.gov
43
Study 1139 Overall Remission Rates were Similar to Placebo Remission Rates in Comparable UC Clinical TrialsInduction Non-responders Remission (Full Mayo Score)
*Includes only patients who received tofacitinib 10mg BID in Study 1094/1095 and failed to demonstrate clinical response at week 8 (patients who received ongoing 10mg BID therapy through 24 months)**Includes only patients who received tofacitinib 10mg BID in Study 1094/1095 and failed to demonstrate clinical response at week 8; N/A=not applicableSource: Reviewer’s table, created from Study 1139 CSR Table 27, Table 229a.27.1, Table 229a.27.2
Of note, estimates of placebo remission rates in controlled clinical trials for UC in the literature vary, but are in the range of 5–12% for induction and 8.5-17% at week 52
44
Patients with Prior TNF Blocker Failure
www.fda.gov
45
Remission at Week 8
(%)
Study
Prior TNF Blocker
Failure
Placebo
N=122 (Study 1094)
N=112 (Study 1095)
Tofacitinib 10 mg BID
N=476 (Study 1094)
N=429 (Study 1095)
Difference from
Placebo (95% CI)
N n (%) N n (%)
Study 1094
Yes 64 1 (1.6) 243 27 (11.1) 9.5 (4.6, 14.5)
No 58 9 (15.5) 233 61 (26.2) 10.7 (-0.2, 21.6)
Study 1095
Yes 60 0 (0.0) 222 26 (11.7) 11.7 (7.5, 15.9)
No 52 4 (7.7) 207 45 (21.7) 14.0 (4.9, 23.2)
Patients in the Prior TNF Blocker Failure Subgroup in Studies 1094, 1095 had Smaller Remission Rates at Week 8
Source: Study 1094 CSR Table 17, Study 1095 CSR Table 17
46
5mg BID and 10mg BID Doses in Study 1096 did not Differ Statistically at Week 52, Regardless of Prior TNF Failure
Pattern(s) of recovery from low ALC levels are not well described in the UC patient population
78
Infection Risks in the Tofacitinib UC Program
79
All Infections (Serious and Non-Serious)
80
Serious Infection Risks
Dose-dependent risk for serious infections seen in UC program
3% of patients in the UC Program developed serious infections
PD 10 mg vs. PD 5 mg group: Incidence Rate Ratio (IRR) of 1.4
Estimated, increase in risk of 40%
• PD 10 mg: Incidence Rate of 2.01 per 100 PYs• PD 5 mg : Incidence Rate of 1.41 per 100 PYs
81
Opportunistic Infections (OI) Risks
2% (n=22) Opportunistic Infections in phase 3 program
• 18 were Herpes Zoster (HZ) - related opportunistic infections
• Six disseminated HZ cases:
one case of meningoencephalitis
two ophthalmic infections
three multi-dermatomal infection
• Non-HZ opportunistic infections occurred in four (4) patients
82
Herpes Zoster (HZ) Infections
83
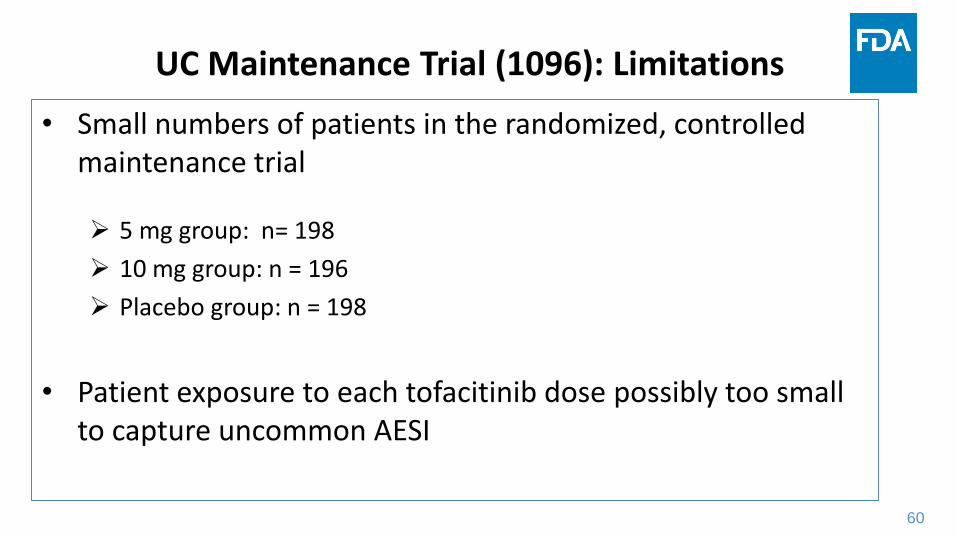
Maintenance Trial (1096):
Herpes Zoster (HZ) Infections
Patients withPrior TNF Failure
Dose GroupTofacitinib
10 mgn (%)
Tofacitinib5 mgn (%)
Placebon (%)
Patients, N 92 83 89
Herpes Zoster, n 9 (9.8%) 2 (2.4%) 0
OpportunisticHerpes Zoster, n
3 (3.3%) 1 (1.2%) 0
84
Discussion
• History of Tofacitinib Dosage
• 8-Week Induction and 16-Week Extended Induction Treatment
• Limitations to Safety Analyses
• Adverse Events of Special Interest (AESIs):
Higher safety risks observed with 10 mg dose treatment
• Summary and Benefit-Risk Considerations
85
Safety Analysis Limitations and Challenges
Multiple limitations and challenges in the safety analyses:
1. The majority of patients in PD 10 mg dose safety analyses group
as compared to the PD 5 mg dose group
2. Overall, the severity of disease was greater in those treated with
the higher versus lower dose
3. High rates of discontinuation in both dose groups
86
Benefit and Risk Assessment
Benefit: Both the 5 mg and 10 mg dose of tofacitinib are efficacious for long-term UC treatment
Risk: Evident and potentially, dose-dependent safety risks exist with the use of the higher 10 mg dose in comparison to the lower 5 mg dose
FDA Gastrointestinal Drugs Advisory Committee (GIDAC)
Tofacitinib UC Program Focused Safety Evaluation
NDA 203214
Remarks about Results from Truven MarketScan®
Joel L. Weissfeld, MD MPH
Office of Surveillance and Epidemiology (OSE)
Center for Drug Evaluation and Research
March 8, 2018
89
Truven MarketScan®
• Truven captures data submitted to U.S. health insurance companies or Medicaid.
• The Applicant used diagnosis, procedure, and drug codes in Truven.
www.fda.gov
90
Malignancy except NMSC
In 4420 patients with a drug or procedures code for a TNF-alpha blocker, the Applicant used an undisclosed code set to observe 31 malignancy events over 4895 patient-years, i.e., 0.6 per 100 patient-years.
www.fda.gov
91
Estimates of Background Risk
• Malignancy occurs in patients with moderate-to-severe UC.
• Background risks in moderate-to-severe UC might explain the number of patients observed with malignancy in the tofacitinib UC safety population.
www.fda.gov
92
Consideration of the Differences
• Real World vs. Clinical Research.
• Other challenges to interpretation,
– Inadequate controls for confounding.
– Markedly different methods for defining, ascertain-ing, and validating malignancy outcomes.
– Statistical uncertainty.
www.fda.gov
Tofacitinib Development Program:Pediatric Ulcerative Colitis
Melanie E. Bhatnagar, MD
Medical Officer
Division of Pediatric and Maternal Health
Center for Drug Evaluation and Research
March 8, 2018
95
Outline
• Pediatric Drug Legislation
• JAK Inhibitors for Pediatric Use
• Applicant’s Proposed Pediatric UC Study Plan
• FDA’s Current Thinking on Pediatric UC
www.fda.gov
96
Outline
• Pediatric Drug Legislation
• JAK Inhibitors for Pediatric Use
• Applicant’s Proposed Pediatric UC Study Plan
• FDA’s Current Thinking on Pediatric UC
www.fda.gov
97
Pediatric Research Equity Act (PREA)
• Gives FDA authority to require pediatric dosing, safety, and efficacy data for the same indication(s) being sought in adults
• Applies to drug or biological products for which applicants are proposing a new active ingredient, new indication, new dosage form, new dosing regimen, or new route of administration
• Requires an initial Pediatric Study Plan (iPSP)
www.fda.gov
98
PREA + Janus Kinase (JAK) Inhibitors• JAK inhibitors approved by FDA for use in adults:
J O’Shea, et al, 2013, JAKs and STATs in Immunity, Immunodeficiency, and Cancer, NEJM 368:2 161-170
101
Ontogeny of the Immune System
Adapted from S Ygberg, et al, 2012, The developing immune system – from fetus to toddler, Acta Paediatrica, 101: 120-127
102
Outline
• Pediatric Drug Legislation
• JAK Inhibitors for Pediatric Use
• Applicant’s Proposed Pediatric UC Study Plan
• FDA’s Current Thinking on Pediatric UC
www.fda.gov
103
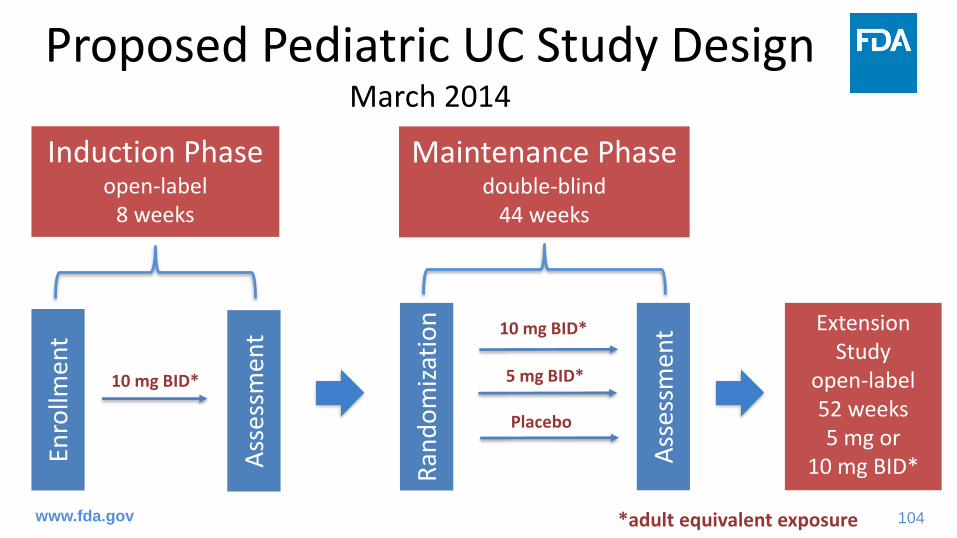
Proposed Pediatric UC Study Plan• Initial Pediatric Study Plan (March 18, 2014 )
– Single study of the safety and effectiveness of tofacitinib in pediatric patients 4 years to less than 18 years of age with moderate to severe UC who have had an inadequate response to prior therapies
• Pediatric Study Protocol (January 19, 2018)– Revised maintenance dosing regimen based on weight
stratification at randomization– Extended lower age limit for study enrollment from 4 years
to 2 years
www.fda.gov
104
Proposed Pediatric UC Study DesignMarch 2014
Enro
llmen
t
Induction Phaseopen-label
8 weeks
10 mg BID*
Maintenance Phasedouble-blind
44 weeks
Extension Study
open-label52 weeks5 mg or
10 mg BID*Ass
essm
ent
Ran
do
miz
atio
n
Ass
essm
ent 10 mg BID*
5 mg BID*
Placebo
*adult equivalent exposurewww.fda.gov
105
Proposed Pediatric UC Study DesignJanuary 2018
Enro
llmen
t
Induction Phaseopen-label
8 weeks
10 mg BID*
Maintenance Phasedouble-blind
44 weeks
Extension Study
open-label52 weeks5 mg or
10 mg BID*Ass
essm
ent
Ran
do
miz
atio
n
Ass
essm
ent
10 mg BID*
5 mg BID*
Placebo
Placebo
5 mg BID*
≥ 3
0 k
g<
30
kg
*adult equivalent exposurewww.fda.gov
106
Proposed Pediatric UC Study Plan
• Initial pediatric study plan (March 2014)– Plan to request that FDA waive the PREA requirement
to study patients less than 4 years of age based on theoretical safety concerns
• Extensive and severe disease in pediatric patients with UC may increase susceptibility to bacterial translocation across intestinal mucosa
• Severe sequelae of bacteremia if taking an immunomodulator– Immature immune systems – Immune suppression related to their disease
www.fda.gov
107
Outline
• Pediatric Drug Legislation
• JAK Inhibitors for Pediatric Use
• Applicant’s Proposed Pediatric UC Study Plan
• FDA’s Current Thinking on Pediatric UC
www.fda.gov
108
FDA’s Current Thinking on Pediatric UC
• Pathogenesis of UC is similar to adults, though pediatric patients tend to present with more severe disease– Higher rates of extensive colonic involvement and increased likelihood for colectomy
• Assessment of safety and effectiveness required for pediatric UC patients ≥ 2 years of age
• One adequate, well-controlled pediatric UC study is generally acceptable if the expected response to the drug is similar between adults and pediatric patients
www.fda.gov
109
FDA’s Current Thinking on Pediatric UC
• Important need for therapies for pediatric UC
www.fda.gov *proposed
110
Summary
• Information on use of JAK inhibitors in the pediatric population is limited
• Pediatric UC tends to be more severe compared to adults• The applicant proposes studying pediatric UC patients 2
years of age and older at dosages targeting adult exposures up to 10 mg twice daily
• The apparent dose-dependent safety findings in adults, including malignancies and serious infections, raise concerns regarding the appropriate population and dosage to target in the pediatric UC study
www.fda.gov
FDA Backup Slides
113
Safety of Extended Induction: Select Safety Events Occurring From Week 8 to Week 16 of Treatment
n (%)
Patients who received 10 mg
induction in Trials1094/1095, followed
by 10 mg in Trial1096a
N = 167
Patients who received 10 mg induction in Trials 1094/1095
followed by 5 mg in Trial 1096a
N = 170
Patients who received 10 mg induction in Trials 1094/1095
Discontinuation for reason other than insufficient clinical response
2 (1.20) 2 (1.18) 2 (1.2) 13 (4.41)
a. Data only for the first 8 weeks of Study A3921096 participationb. Data only for the first 8 weeks of Study A3921139 participation (i.e., in the Induction non-responder subgroup)c. The number of subjects with SAEs was based on the safety database. For patients in the Induction non-responder subgroup who received 10 mg induction, the number of subjects with SAE is 12 based on the safety database instead of 11 derived from the clinical database as shown in Table 16 of the Pfizer Briefing document.
Source: Applicant’s Inquiry Response Submission and Table 3.4, received 3/1/18
114
Study 1096 Overall Remission Rates at Week 52 for Patients with Primary or Secondary Non-response to TNF Blockers
responder 34 4 (11.8) 36 9 (25.0) 13.2 (-4.6, 31.0) 41 17 (41.5) 29.7 (11.1, 48.3)*TNFi failure was further analyzed by primary non-response, defined as categories 2 or 4, and secondary non-response, defined as categories 3 or 5. Prior failure or intolerance to TNFi agents, as assessed by the investigator, included the following reasons: (1) adverse event (AE), (2) lack of efficacy with failure to achieve a response, (3) lack of efficacy with failure to maintain a response, (4) lack of efficacy with failure to achieve a response and AE, and (5) lack of efficacy with failure to maintain a response and AESource: Summary of Clinical Efficacy Table 77