55
UPDATE ON JUPITER I AND II CLINICAL TRIALS WITH THE SORIN CARBOSTENT TRACROLIMUS ELUTING STENT GB Danzi, MD Ospedale Maggiore Policlinico University of Milan Milan - Italy
UPDATE ON JUPITER I AND II CLINICAL TRIALSWITH THE SORIN CARBOSTENT TRACROLIMUS
ELUTING STENT
GB Danzi, MDOspedale Maggiore Policlinico
University of MilanMilan - Italy
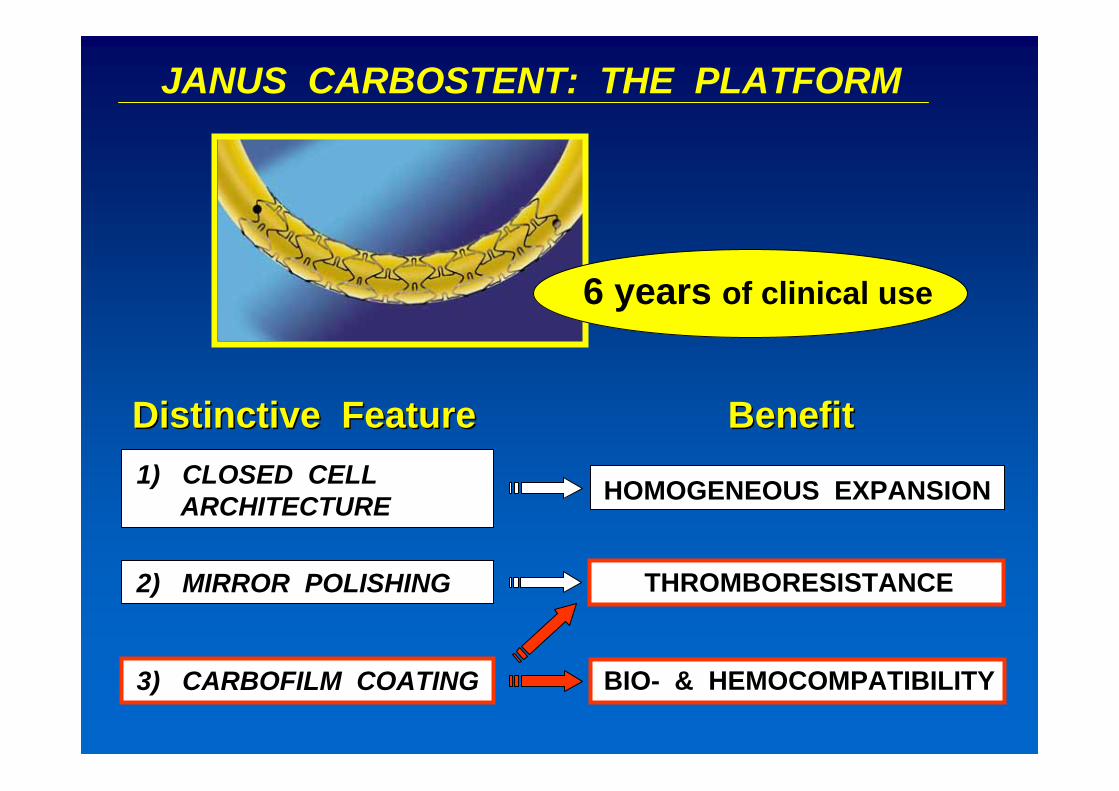
JANUS CARBOSTENT: THE PLATFORM
2) MIRROR POLISHING
1) CLOSED CELLARCHITECTURE
THROMBORESISTANCE
Distinctive FeatureDistinctive FeatureDistinctive Feature
6 years of clinical use
3) CARBOFILM COATING BIO- & HEMOCOMPATIBILITY
BenefitBenefitBenefit
HOMOGENEOUS EXPANSION

Stent crosssection
Reservoirs on theexternal surface
Strut crosssection
THE EXTERNAL SURFACE OF JANUS CARBOSTENT IS SUITABLY GROOVED TO PROVIDE DEEP RESERVOIRS FOR THE DRUG
AFTER THE RESERVOIRS ARE REALIZED THE WHOLE SURFACE OF THE STENT IS COATED WITH CARBOFILM™
IntegralCarbofilm™
coating
RESERVOIRS ON THE SURFACE TO LOAD THE DRUG

JANUS JANUS CarbostentCarbostent
Deep drug reservoirson the external surface
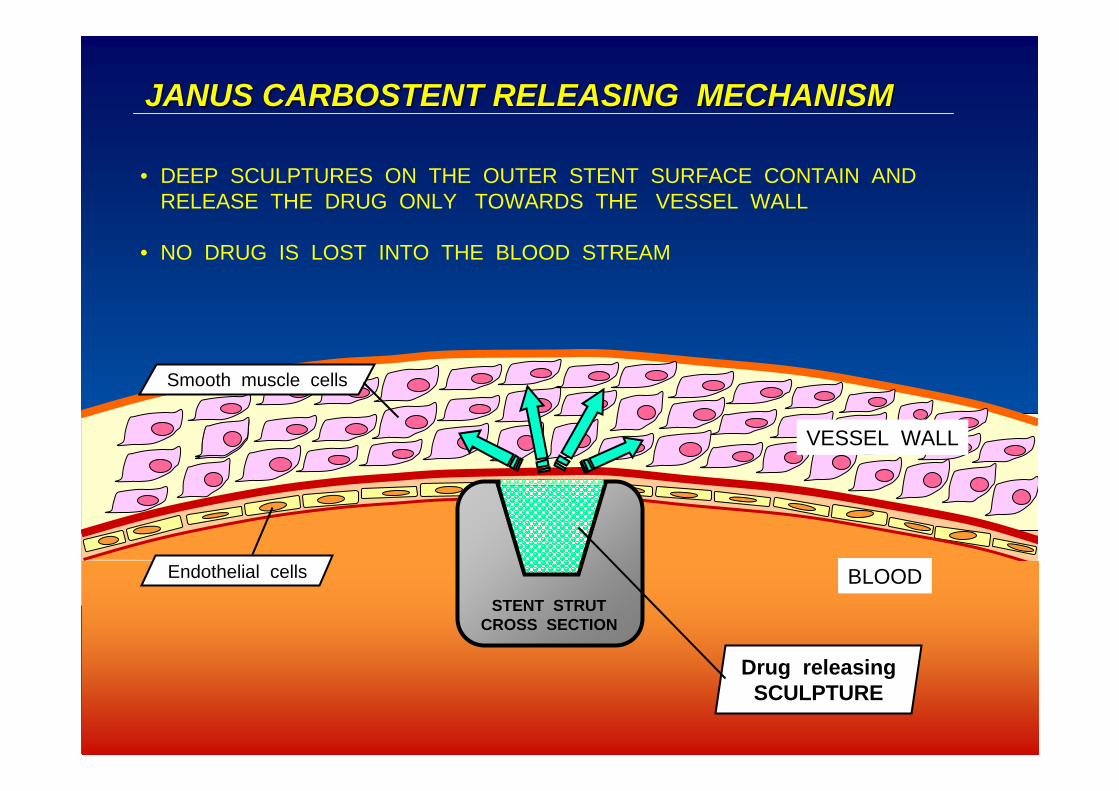
Endothelial cells
Smooth muscle cells
VESSEL WALL
BLOOD
JANUS CARBOSTENT RELEASING MECHANISMJANUS CARBOSTENT RELEASING MECHANISM
• DEEP SCULPTURES ON THE OUTER STENT SURFACE CONTAIN AND RELEASE THE DRUG ONLY TOWARDS THE VESSEL WALL
• NO DRUG IS LOST INTO THE BLOOD STREAM
STENT STRUTCROSS SECTION
Drug releasingSCULPTURE
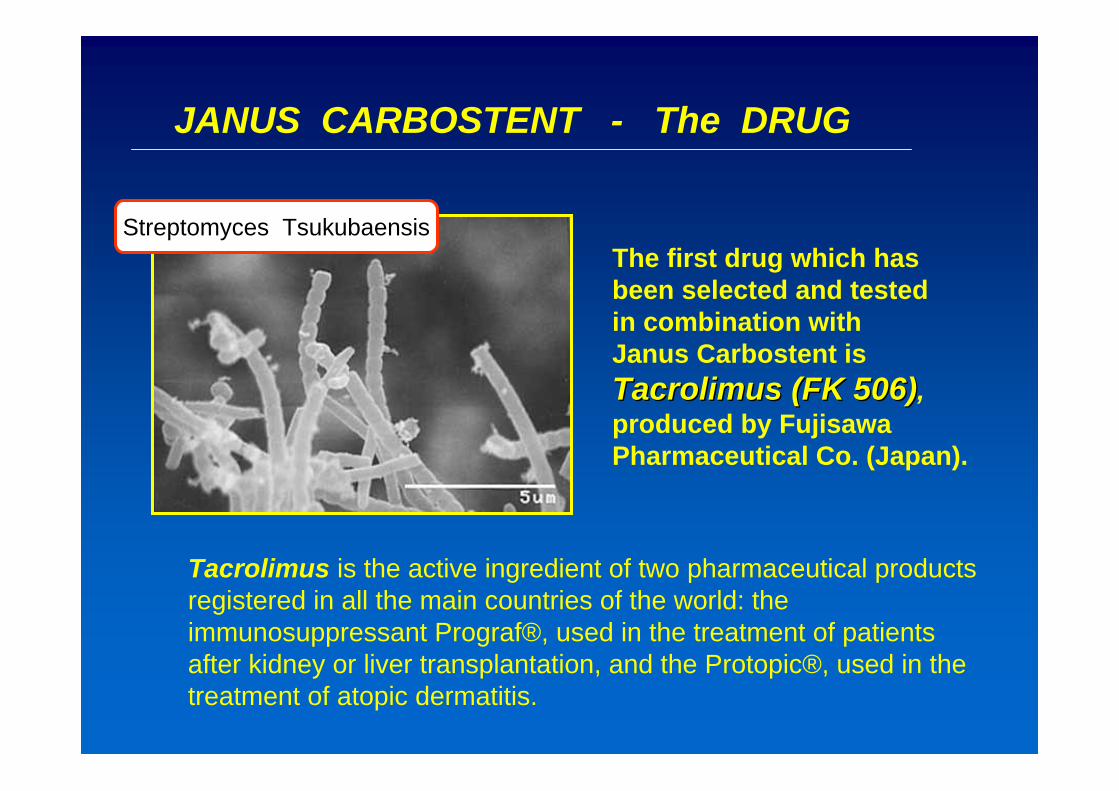
JANUS CARBOSTENT - The DRUG
Tacrolimus is the active ingredient of two pharmaceutical products registered in all the main countries of the world: the immunosuppressant Prograf®, used in the treatment of patients after kidney or liver transplantation, and the Protopic®, used in the treatment of atopic dermatitis.
The first drug which has been selected and tested in combination with Janus Carbostent is TacrolimusTacrolimus (FK 506)(FK 506),produced by Fujisawa Pharmaceutical Co. (Japan).
Streptomyces Tsukubaensis

UPDATE
on
JUPITER I

Jupiter I:: StudyStudy DesignDesign
α phase
Clinical registry≥ 50 patients
Interim analysis
at 1 month
“Safety” evaluation
Clinical evaluation randomized 1:1
multicenterdouble blind
Investig. & Core-Lab
β phaseJANUS≥ 50 patients
TECNIC (control)≥ 50 patients
Clinical, angiographicand IVUS follow-up at
6 months
Clinical follow-up at 12 and 24
months
Follow-up at 1, 6, 12 and 24 months
•• 1 1 monthmonth: : ClinicalClinical
•• 6 6 monthsmonths: : ClinicalClinical, , angiographicangiographic and IVUSand IVUS
•• 12 12 monthsmonths: : ClinicalClinical
•• 24 24 monthsmonths: : ClinicalClinical
Jupiter I study - β phase

Jupiter I -- β: Study UpdateUpdate
32
102
3719 24
17
50
19
11010
19
52
110
271418
0
20
40
60
80
100
120
Monzin
o-Mila
no
Poliam
bulan
za-B
rescia
San Pietro
FBF-Rom
a
Osped
ale de
gli Infe
rmi-R
imini
Hespe
ria H
ospit
al-Mod
ena
Osped
ale Ferr
arotto-
Catania
TOTAL
# pa
tient
s Nb patientsGroup AGroup B
Enrolment completed on December 2004
32
102
3719 24
17
50
19
11010
19
52
110
271418
0
20
40
60
80
100
120
Monzin
o-Mila
no
Poliam
bulan
za-B
rescia
San Pietro
FBF-Rom
a
Osped
ale de
gli Infe
rmi-R
imini
Hespe
ria H
ospit
al-Mod
ena
Osped
ale Ferr
arotto-
Catania
TOTAL
# pa
tient
s
Nb patientsGroup AGroup B
Jupiter I study - β phase

GROUP A GROUP B P P valuevalueN° of enrolled pts (102) 50 52
N° of available pts (92) 46 49
Male 89.1% 79.6% .203Age (yrs) 64.6 ± 11.6 64.0 ± 10.4 .788
Clinical Status .436Asymptomatic 6.5% (3 pts) 8.2% (4 pts)Silent Ischemia 8.7% (4 pts) 8.2% (4 pts)Stable Angina 60.9% (28 pts) 42.8% (21 pts)Unstable Angina 15.2% (7 pts) 28.6% (14 pts)MI 8.7% (4 pts) 12.2% (6 pts)
Jupiter I - β: Base-Line Clinical CharacteristicsJupiter I study - β phase

Unstable angina
28,6
14,3
0 7,1
28,6
50,0
14,2
0
28,6 28,6
0
20
40
60
80
100
1B 2A 2B 2C 3B
GROUP AGROUP B
%
21,420,0
50,0 50,0
21,430,0
7,20
0
20
40
60
80
100
I II III IV
GROUP AGROUP B
Stable angina
%
p=.619
p=.478
Jupiter I - β: Base-Line Clinical Characteristics
Jupiter I study - β phase

GROUP A GROUP B P value
Risk factors 46 49
Smokers 37.0% (17 pts) 42.9% (21 pts) .557
Diabetes 17.4% (8 pts) 28.6% (14 pts) .197
ID Diabetes 4.3% (2 pts) 2.0% (1 pts) .520
NID Diabetes 13.0% (6 pts) 26.5% (13 pts) .101
Hypertension 69.6% (32 pts) 59.2% (29 pts) .291
Hypercholesterolemia 63.0% (29 pts) 79.6% (39 pts) .074
Family history of CAD 21.7% (10 pts) 22.4% (11 pts) .934
Jupiter I - β: Base-Line Clinical Characteristics
Jupiter I study - β phase

Jupiter I - β: Target lesion characteristics
GROUP A GROUP B P value N° of available lesions (103) 50 53
De Novo 100% 100%
Lesion morphology .942Concentric 46.0% (23/50 les) 45.3% (24/53 les)Eccentric 54.0% (27/50 les) 54.7% (29/53 les)
Calcification 10.0% (5/50 les) 9.4% (5/53 les) .923
Tortuosity 12.0% (6/50 les) 3.8% (2/53 les) .119
Bifurcation 0% 0%
Ostial Lesion 0% 0%
Total Chronic Occlusion 2.0% (1/50 les) 0% .301
Jupiter I study - β phase

2,05,9
38,033,3
50,045,1
10,015,7
0
20
40
60
80
100
A B1 B2 C
GROUP AGROUP B
Lesion Type
%
p=.598
Jupiter I - β: Target lesion characteristics
Jupiter I study - β phase

% 40,034,0
22,0 22,6
38,043,4
0,0
20,0
40,0
60,0
80,0
100,0
LAD LCX RCA
Group AGroup B
Target Vessels p=.801
Jupiter I - β: Target lesion characteristics
Jupiter I study - β phase

Jupiter I - β : Procedural angiographic data
15.1
3.11 0.843.22 0.76 2.79
73.2
3.27 2.91
7.7
76.0
15.1
3.11
8.7
0
20
40
60
80
100
Les.length
PRE (mm)
RVD PRE(mm)
RVDPOST(mm)
MLD PRE(mm)
MLDPOST(mm)
D.S. PRE(%)
D.S. POST(%)
Group AGroup B
Jupiter I study - β phase

GROUP A GROUP B P value Stenting procedure 50 53 .923
Direct stenting 10.0% (5/50 les) 9.4% (5/53 les)
Predilation 90.0% (45/50 les) 90.6% (48/53 les)
N° stent / lesion 1.08 1.00
Max. stent depl. pressure (atm) 15.29 ± 2.86 15.36 ± 2.59 .893
Postdilation 52.0% (26/50 les) 50.9% (27/53 les) .915
Dissection 0% 0%
Procedural success 100% 100%
TIMI flow 3 100% 100%
Residual stenosis <20% 100% 100%
Jupiter I - β : Procedural dataJupiter I study - β phase
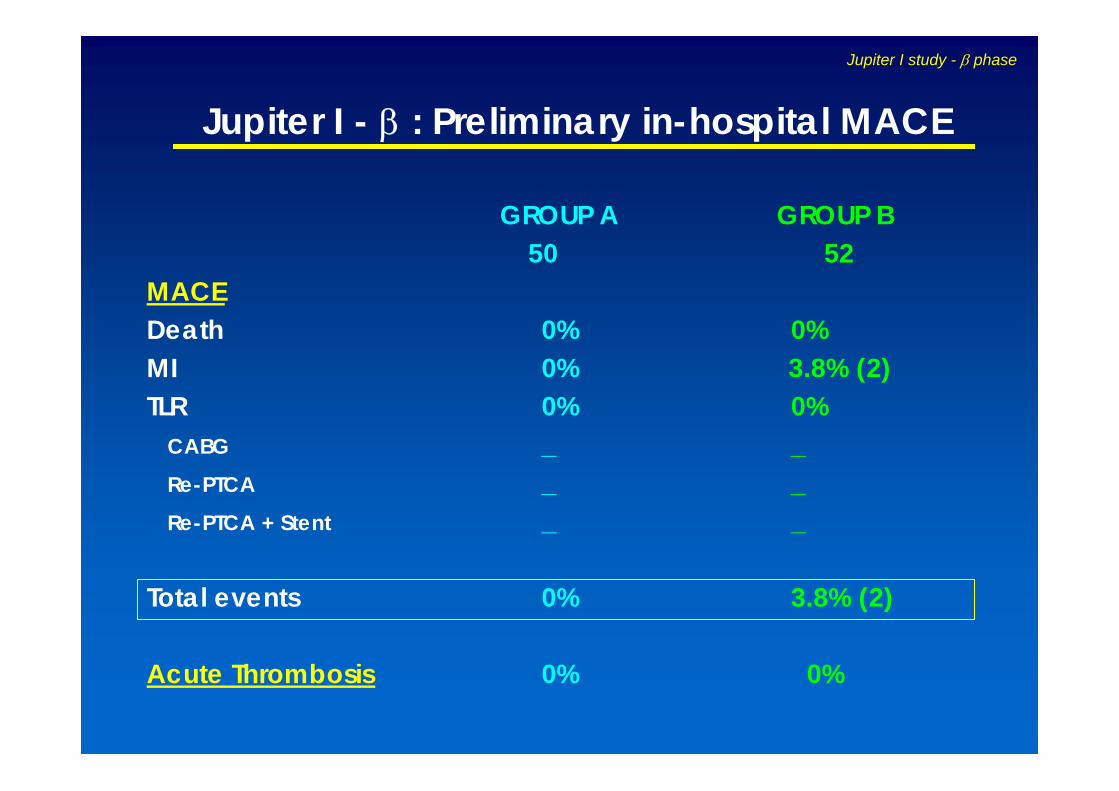
GROUP A GROUP B50 52
MACEDeath 0% 0%MI 0% 3.8% (2)TLR 0% 0%
CABG _ _Re-PTCA _ _Re-PTCA + Stent _ _
Total events 0% 3.8% (2)
Acute Thrombosis 0% 0%
Jupiter I - β : Preliminary in-hospital MACE
Jupiter I study - β phase
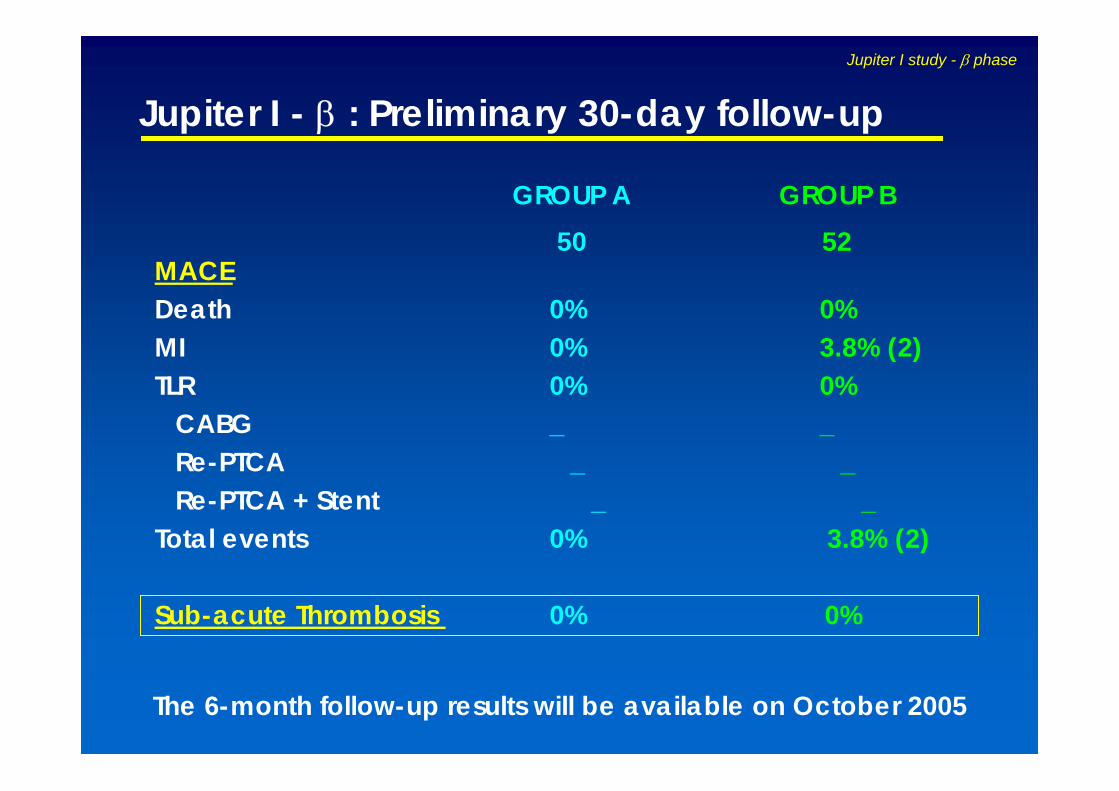
Jupiter I - β : Preliminary 30-day follow-up
GROUP A GROUP B50 52
MACEDeath 0% 0%MI 0% 3.8% (2)TLR 0% 0%
CABG _ _Re-PTCA _ _Re-PTCA + Stent _ _
Total events 0% 3.8% (2)
Sub-acute Thrombosis 0% 0%
Jupiter I study - β phase
The 6-month follow-up results will be available on October 2005

JUPITER II preliminary
clinical data
Jupiter II study

Clinical evaluation randomized 1:1
16 centers in Europedouble blind
(Investigator & Core-Lab)
JANUS150 + 10% drop-out = 165 pts
TECNIC150 + 10% drop-out = 165 pts
Follow-up• 1 month: Clinical
• 6 months: Clinical, Angiographic
• 12 months: Clinical
• 24 months: Clinical
Jupiter II: Study Design with high dose: 2.3µg/mm2
Jupiter II study
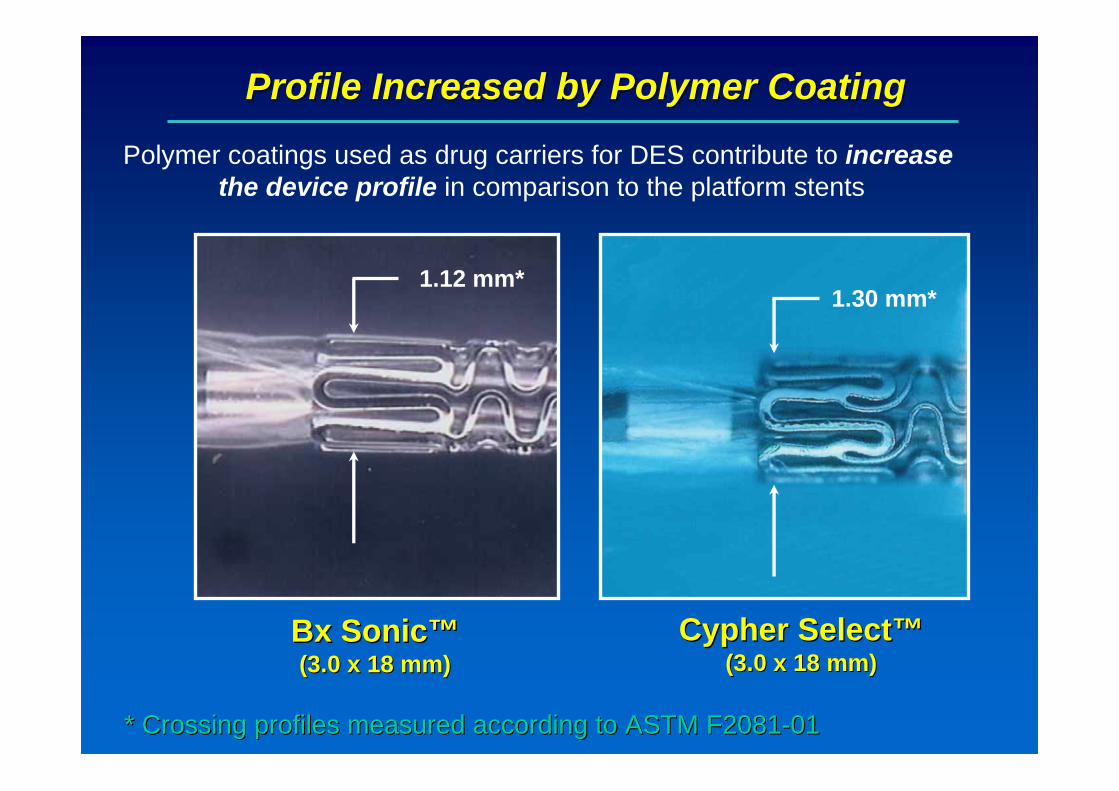
Profile Increased by Polymer CoatingProfile Increased by Polymer Coating
Polymer coatings used as drug carriers for DES contribute to increase the device profile in comparison to the platform stents
1.12 mm*1.30 mm*
* * CrossingCrossing profilesprofiles measuredmeasured accordingaccording toto ASTM F2081ASTM F2081--0101
BxBx SonicSonic™™(3.0 x 18 mm)(3.0 x 18 mm)
CypherCypher SelectSelect™™(3.0 x 18 mm)(3.0 x 18 mm)
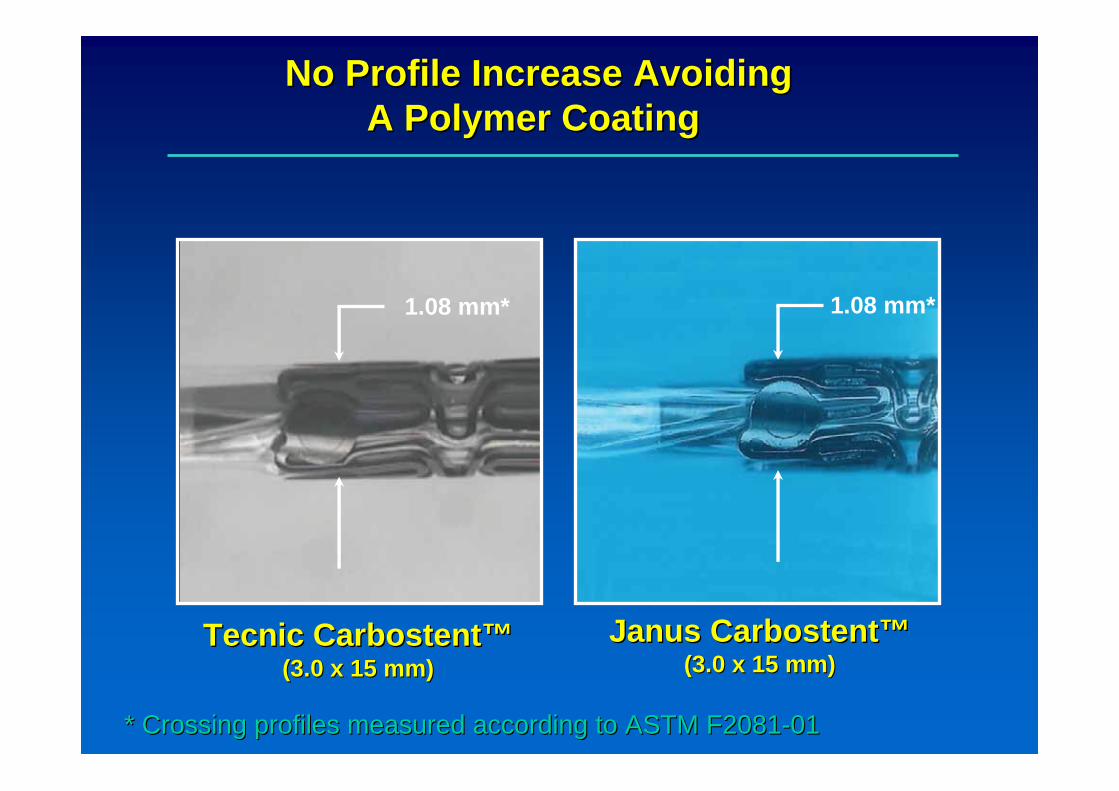
No Profile Increase AvoidingNo Profile Increase AvoidingA Polymer Coating A Polymer Coating
1.08 mm* 1.08 mm*
* * CrossingCrossing profilesprofiles measuredmeasured accordingaccording toto ASTM F2081ASTM F2081--0101
TecnicTecnic CarbostentCarbostent™™(3.0 x 15 mm)(3.0 x 15 mm)
JanusJanus CarbostentCarbostent™™(3.0 x 15 mm)(3.0 x 15 mm)
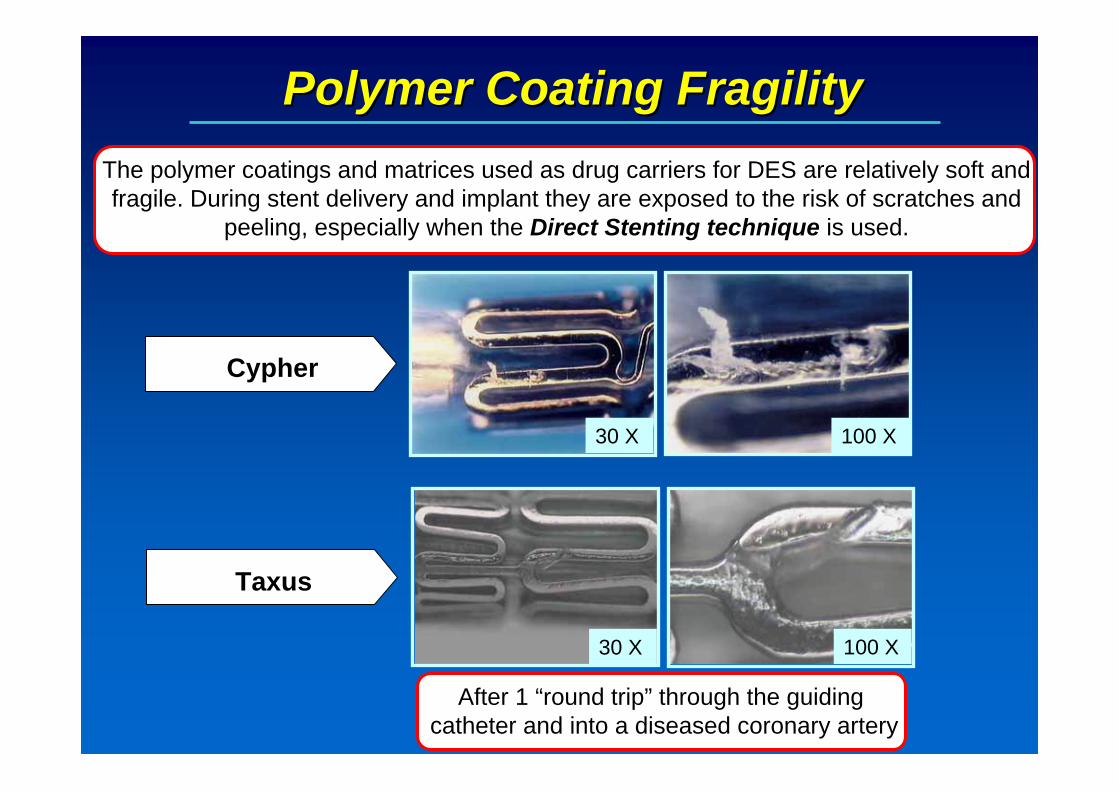
Polymer Coating FragilityPolymer Coating FragilityThe polymer coatings and matrices used as drug carriers for DES are relatively soft and fragile. During stent delivery and implant they are exposed to the risk of scratches and
peeling, especially when the Direct Stenting technique is used.is used.
100 X30 X
30 X 100 X
TaxusTaxus
CypherCypher
After 1 After 1 ““round tripround trip”” through the through the guiding guiding cathetercatheter and and intointo a a diseaseddiseased coronarycoronary arteryartery
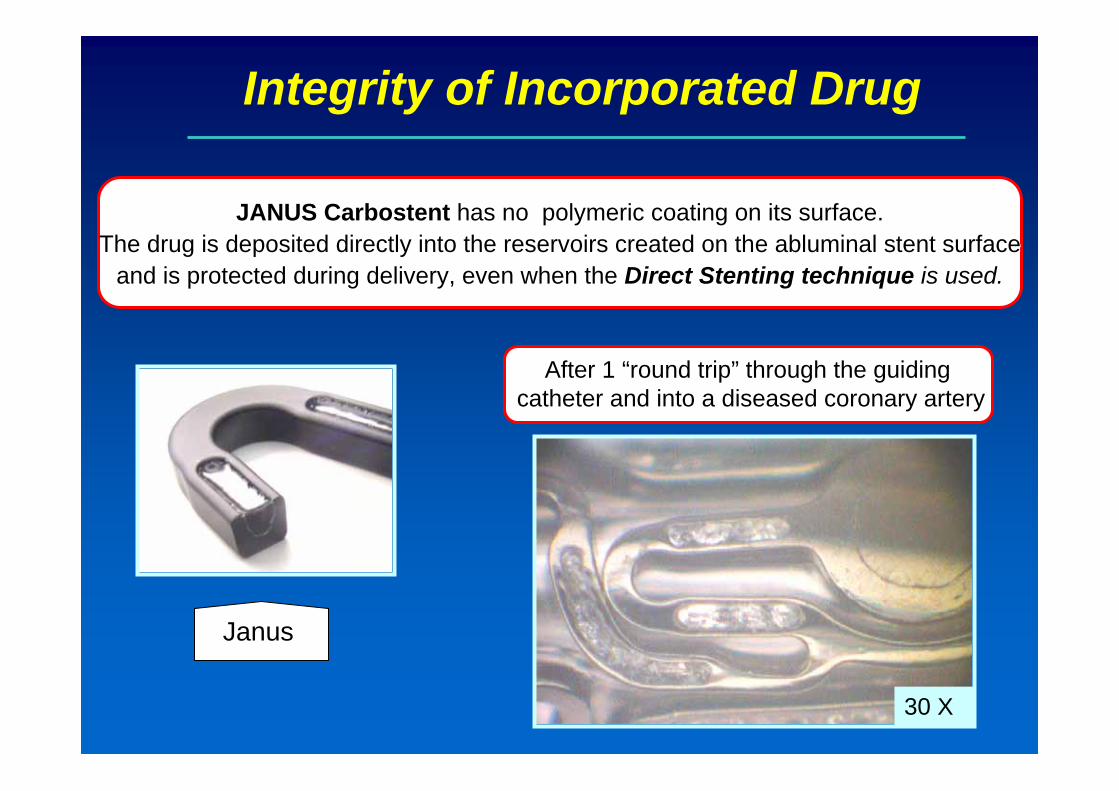
Integrity of Incorporated Drug
JANUS JANUS CarbostentCarbostent has no polymeric coating on its surface.has no polymeric coating on its surface.The drug is deposited directly into the reservoirs created on thThe drug is deposited directly into the reservoirs created on the e abluminalabluminal stent surface stent surface
and is protected during delivery, even when the and is protected during delivery, even when the Direct Stenting technique Direct Stenting technique is used.is used.
Janus
30 X
After 1 After 1 ““round tripround trip”” through the through the guiding guiding cathetercatheter and and intointo a a diseaseddiseased coronarycoronary arteryartery

Jupiter II: Participating centers
Prof. Macaya - MadridSPAIN (1)
Dr. Cremonesi – CotignolaITALY (1)Prof. Di Mario, Prof. Ilsey - LondonU.K. (2)
Prof.Neumann, Prof. Bestehorn – Bad Krozingen
Dr. Hoffmann - BerlinDr. Hempel - Dresden
GERMANY (3)
Dr. Morice (PI) – MassyProf. Carrié - Toulouse
FRANCE (2)
Dr. De Bruyne, Dr. Wijns - AalstDr. Verheye – Antwerp
Dr. Dubois - Leuven
BELGIUM (3)
Prof. Amann - ZurichSWITZERLAND (1)Prof. Pachinger - InnsbruckAUSTRIA (1)
Dr. Aengevaeren-NijmegenProf. Serruys - Rotterdam
Dr. De Winter - Amsterdam
THE NETHERLANDS (3)
INVESTIGATORCOUNTRY
Jupiter II study

Jupiter II: Enrolment
154 10 16
0 3 2 116 10 5
3515 5 9 18 20 21
0 3 0 1 1 10 9 3 2
309
34 39 42
0 6 2 5 8 3
332
19 2114 9
30
166
14
166
24251919 2
65
0
40
80
120
160
200
240
280
320
Bad K
rozing
enAals
tInn
sbruc
kMas
syNijm
egen
Madrid
Tou
louse
Zurich
Lond
on B.
Lond
on H
.Coti
gnola
Rotterd
amAntw
erpLe
uven
Amsterda
mBerl
inDres
den
TOTAL
Group AGroup B TOTAL
Jupiter II study
Enrolment Completed as for Dec. 2004

Jupiter II: Primary Endpoint
Assessment of in-stent and peri-stent “Late Lumen Loss (LLL)” at 6 month follow-up by Quantitative Coronary Angiography (QCA)
In-stent: measurement within the stented areaPeri-stent: measurement within the stented segment and within 5 mm proximal and distal to the stent edges
Peri-stent5 mm 5 mm
in stent
Jupiter II study
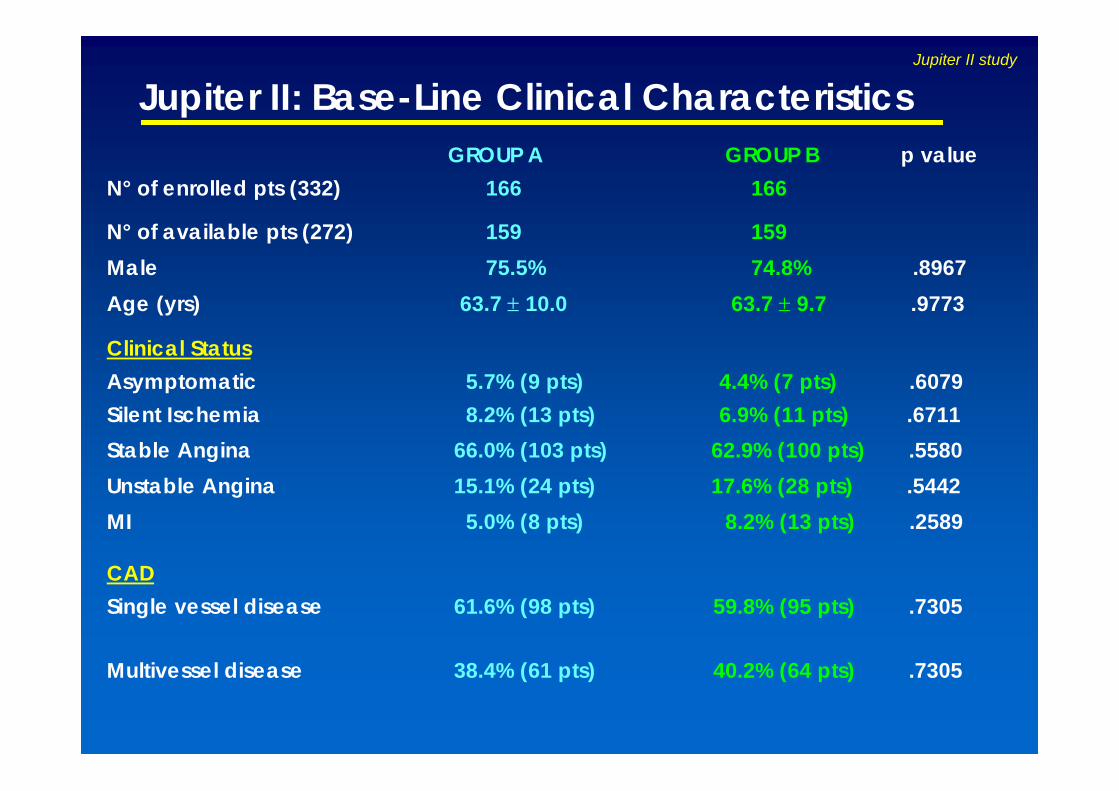
GROUP A GROUP B p valueN° of enrolled pts (332) 166 166
N° of available pts (272) 159 159Male 75.5% 74.8% .8967Age (yrs) 63.7 ± 10.0 63.7 ± 9.7 .9773
Clinical StatusAsymptomatic 5.7% (9 pts) 4.4% (7 pts) .6079Silent Ischemia 8.2% (13 pts) 6.9% (11 pts) .6711Stable Angina 66.0% (103 pts) 62.9% (100 pts) .5580Unstable Angina 15.1% (24 pts) 17.6% (28 pts) .5442MI 5.0% (8 pts) 8.2% (13 pts) .2589
CADSingle vessel disease 61.6% (98 pts) 59.8% (95 pts) .7305
Multivessel disease 38.4% (61 pts) 40.2% (64 pts) .7305
Jupiter II: Base-Line Clinical CharacteristicsJupiter II study

GROUP A GROUP B p value
Risk factors 159 159
Smokers 38.4% (61 pts) 44.0% (70 pts) .3052
Diabetes 19.5% (31 pts) 17.6% (28 pts) .6652ID Diabetes 6.3% (10 pts) 2.5% (4 pts) .1698NID Diabetes 13.2% (21 pts) 15.1% (24 pts) .6293
Hypertension 62.9% (100 pts) 57.2% (91 pts) .3028
Hypercholesterolemia 69.2% (110 pts) 67.3% (107 pts) .7178
Family history of CAD 7.7% (44 pts) 28.9% (46 pts) .8034
Other Pathology 6.9% (11 pts) 9.4% (15 pts) .4130
Jupiter II: Base-Line Clinical CharacteristicsJupiter II study

GROUP A GROUP B p value
N° of lesions (365) 182 183De Novo 98.9% (178/180 les) 99.5% (181/182 les) .6219
Concentric 53.4% (87/163 les) 47.7% (83/174 les) .2979
Eccentric 46.6% (76/163 les) 52.3% (91/174 les) .2979
Calcification 17.2% (31/180 les) 21.4% (39/182 les) .3110
Tortuosity 6.7% (12/180 les) 13.1% (24/183 les) .0399
Bifurcation 0% 2.7% (5/183 les) .0608
Ostial Lesion 0.6% (1/180 les) 1.1% (2/183 les) 1.000
Total Chronic Occlusion 0% 1.1% (2/183 les) .4987
Jupiter II: Target lesions CharacteristicsJupiter II study

19,3 17,8
54,7
47,9
23,629,5
2,5 4,9
0
20
40
60
80
100
A B1 B2 C
GROUP AGROUP B
Lesion Type
%
Jupiter II: Target lesions Characteristics
p=0.3854
Jupiter II study

%37,9
30,128,0 27,9
34,1
41,5
0 0,50
20
40
60
80
100
LAD LCX RCA LM
Group AGroup B
Target Vessels
Jupiter II: Target lesions Characteristics
p=0.3018
Jupiter II study
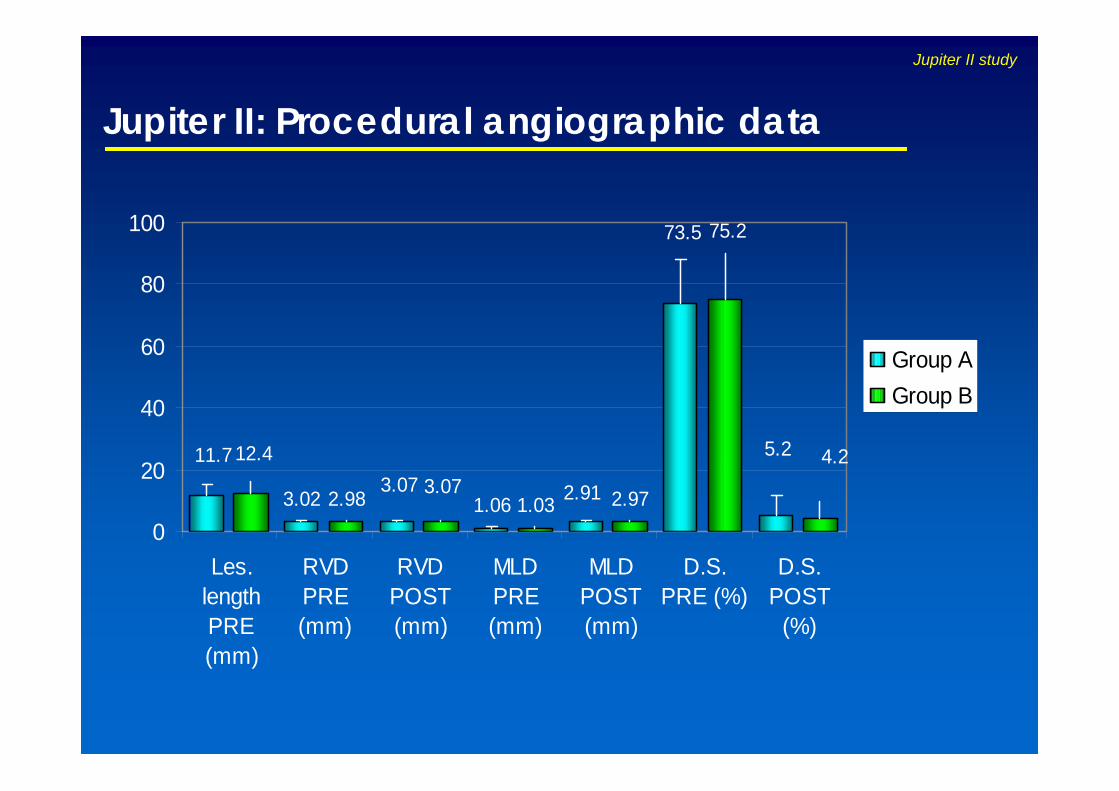
Jupiter II: Procedural angiographic data
3.02 1.062.98 1.03 2.97
11.7
73.5
3.07 2.91
5.2
75.2
12.43.07
4.2
0
20
40
60
80
100
Les.lengthPRE(mm)
RVDPRE(mm)
RVDPOST(mm)
MLDPRE(mm)
MLDPOST(mm)
D.S.PRE (%)
D.S.POST
(%)
Group AGroup B
Jupiter II study
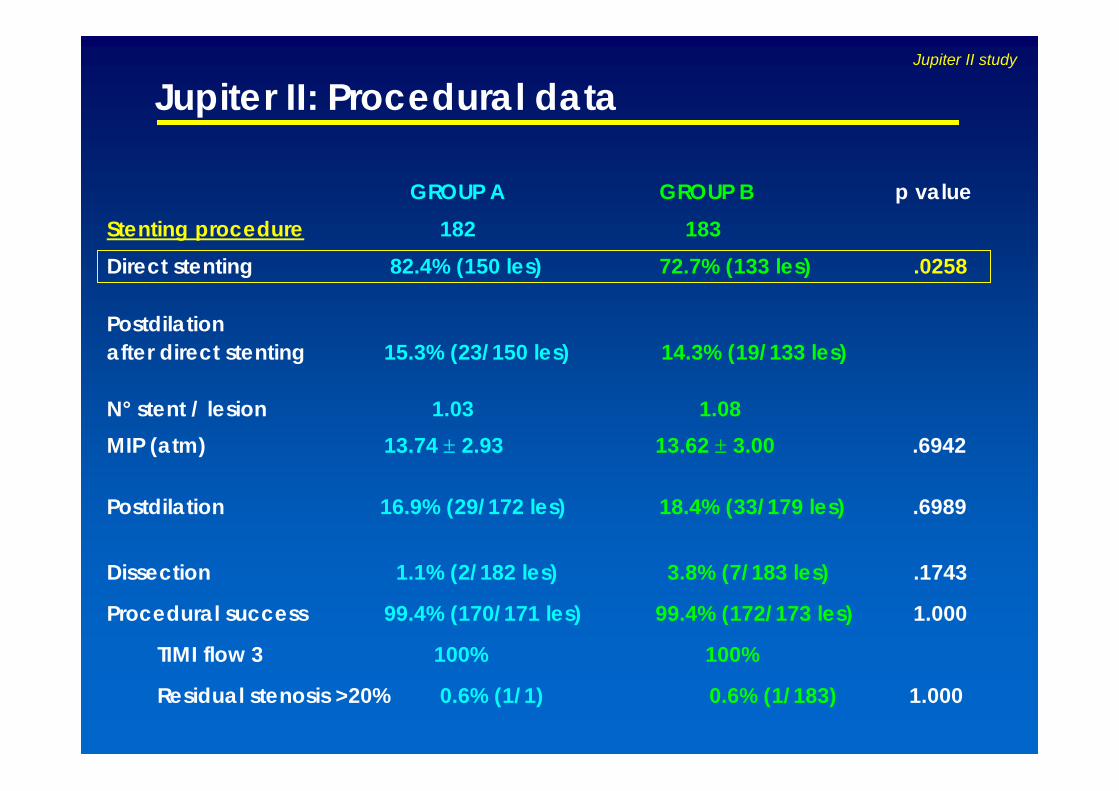
GROUP A GROUP B p valueStenting procedure 182 183Direct stenting 82.4% (150 les) 72.7% (133 les) .0258
Postdilation after direct stenting 15.3% (23/150 les) 14.3% (19/133 les)
N° stent / lesion 1.03 1.08MIP (atm) 13.74 ± 2.93 13.62 ± 3.00 .6942
Postdilation 16.9% (29/172 les) 18.4% (33/179 les) .6989
Dissection 1.1% (2/182 les) 3.8% (7/183 les) .1743
Procedural success 99.4% (170/171 les) 99.4% (172/173 les) 1.000
TIMI flow 3 100% 100%
Residual stenosis >20% 0.6% (1/1) 0.6% (1/183) 1.000
Jupiter II: Procedural dataJupiter II study
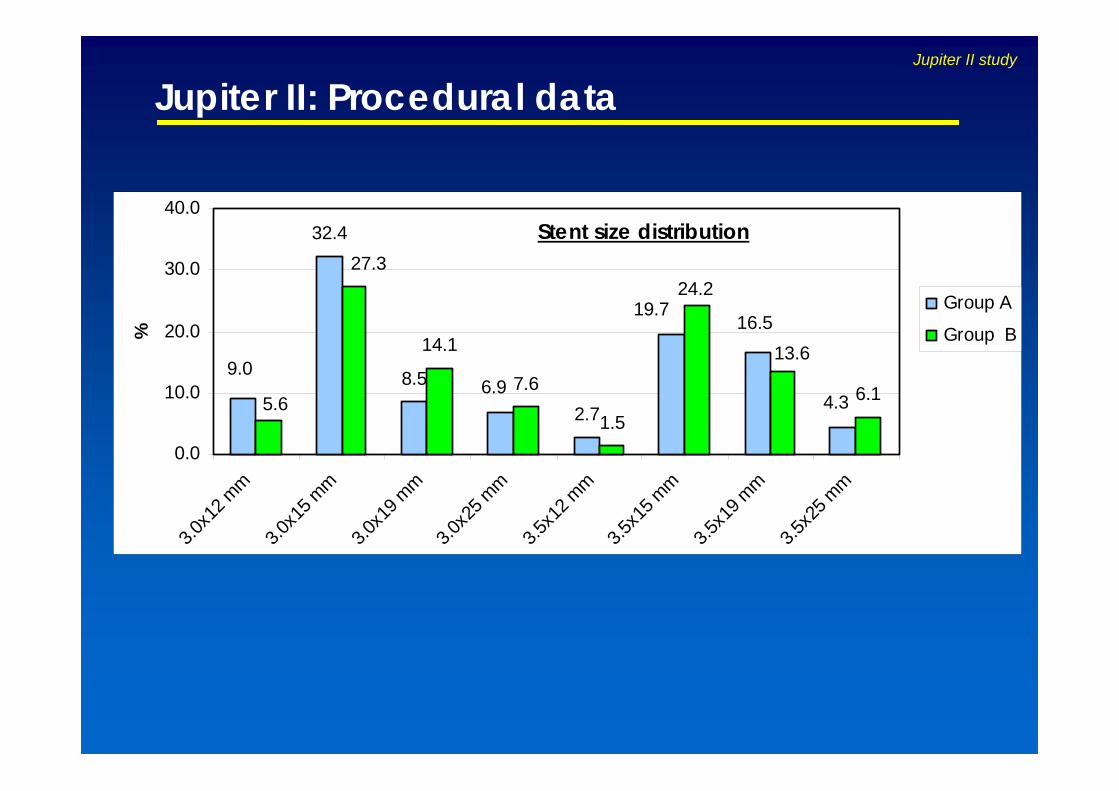
32.4
8.5
2.7
14.1
7.6
1.56.1
9.06.9
4.3
16.519.7
27.3
5.6
13.6
24.2
0.0
10.0
20.0
30.0
40.0
3.0x1
2 mm
3.0x1
5 mm
3.0x1
9 mm
3.0x2
5 mm
3.5x1
2 mm
3.5x1
5 mm
3.5x1
9 mm
3.5x2
5 mm
%
Group A
Group B
Stent size distribution
Jupiter II: Procedural dataJupiter II study

GROUP A GROUP B* p value159 159
MACEDeath 0% 0%MI 0.63%(1) 0.63% (1) 1.0000TLR 1.26% (2) 0% .3260
CABG 0% 0%
Re-PTCA 0.63% (1) 0%
Re-PTCA + Stent 0.63% (1) 0%
Total events 1.89% (3) 0.63% (1) .3812
Acute Thrombosis 0% 0%
Jupiter II: Preliminary in-hospital MACE
* 1 protocol deviation censored
Jupiter II study

Jupiter II: Preliminary 30-day follow-up*GROUP A GROUP B p value
Clinical status 159 159
MACEDeath 0% 0%MI 0.8% 0% .3772TLR 0% 0%
CABG 0% 0%
Re-PTCA 0% 0%
Re-PTCA + Stent 0% 0%
Total events 0.8%(1) 0% .3772
Sub-acute Thrombosis 1.6% (2) 0% .3246
* Clinical events not yet adjudicated by Critical Event Committee
Jupiter II study
The 6-month follow-up results will be available on October 2005
Conclusion: Clinical Studies
• Initial clinical outcomes are showing a positive performance in term of MACE, incidence of acute and subacute thrombosis in bothgroups;
• The preliminary Jupiter II 30-day results demonstrate low rate of clinical events in both groups confirming at short term that the two stents in evaluation have a comparable clinical safety (MACE and Thrombosis);
• Janus is the latest innovative DES platform, designed for resolving major limitations of current DES with polymer coatings.
Jupiter II study

DIABETes and drug Eluting Stent
The DIABETES III Trial
DIABETES III

Diabetes IIISTUDY DESIGN:
Multicenter:
• Madrid: Hospital Clinico San Carlos, Prof. Macaya, Dr. Sabaté (PIs)
• Barcelona: Hospital de Bellvitge, Dr. Cequier
• Murcia: Hospital Virgen de Arrixaca, Dr. Valdes
Spanish Prospective Trial (80 pts will be enrolled)
START OF THE STUDY: December 2004
AIM OF THE STUDY: To evaluate the efficacy of Janus Carbostent on the
inhibition of neointimal proliferation, assessed by QCA at 9 month follow-up, in
diabetic patients. The obtained results will be compared to an historical cohort
treated with bare metal stent (DIABETES I trial)
DIABETES III

PRIMARY ENDPOINT:
• Late Lumen Loss (in-stent + edges) by QCA at 9 month f-up
SECONDARY ENDPOINTS:
• In-stent + edges neointimal hyperplasia area by IVUS at 9 month f-up
• Binary restenosis rate, MLD and mean luminal diameter at 9-month f-up
• MACE at 1, 9, 12 and 24 month f-up
• Occurrence of complications attributable to DES: late stent thrombosis,
edge effect, late stent malapposition, coronary aneurysm
Diabetes IIIDIABETES III

Diabetes III
Enrolment started in December 2004
12 16
64
36
0
40
80
Madrid Barcelona Murcia Total
DIABETES III
eJANUS
eJANUS

eJanus
STUDY DESIGN:European, Multicenter (100-200), Prospective Registry Based on electronic CRFs
START OF THE STUDY: November 2004
AIM OF THE STUDY:Assessment of clinical performances of Janus Carbostent in the treatment of de novo or restenotic lesions in “real world” population
STUDY POPULATION:All “real world” patients (2500 pts) with stable/unstable angina, documented ischemia or AMI who are scheduled to undergo coronaryangioplasty of de novo or restenotic lesion(s) in native coronary arteries
eJANUS

eJanusPRIMARY ENDPOINTS:
• Incidence of MACE within discharge, 30 days, 6, 12 & 24 months
• Thrombosis rate within discharge, 30 days, 6, 12 & 24 months (acute, sub-acute
& late thrombosis)
• Clinical performances of Janus Carbostent, during implant procedure
SECONDARY ENDPOINT:
• Clinically driven TLR at 6 months
eJANUS
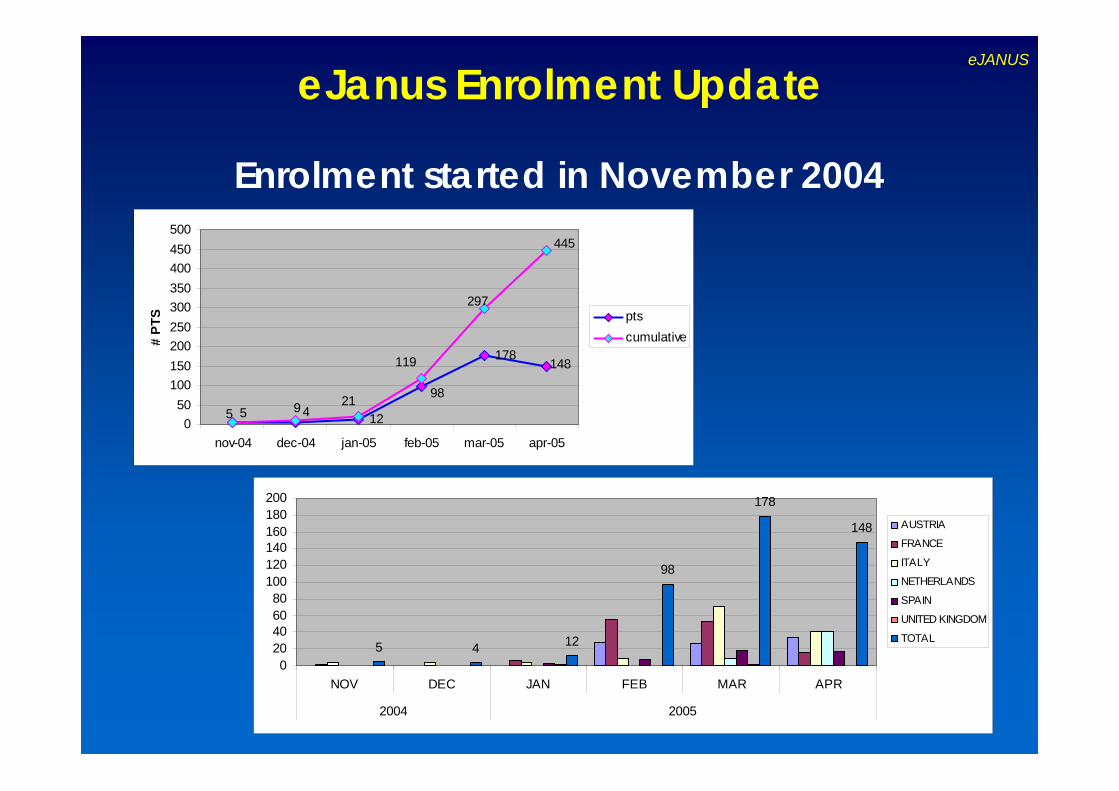
eJanus Enrolment UpdateeJANUS
Enrolment started in November 2004
12
178
498
5
148119
2195
297
445
050
100150200250300350400450500
nov-04 dec-04 jan-05 feb-05 mar-05 apr-05
# PT
S ptscumulative
5 4 12
98
178
148
020406080
100120140160180200
NOV DEC JAN FEB MAR APR
2004 2005
AUSTRIA
FRANCE
ITALY
NETHERLANDS
SPAIN
UNITED KINGDOM
TOTAL
SORIN JANUS CARBOSTENT
FUTURE DEVELOPMENTS
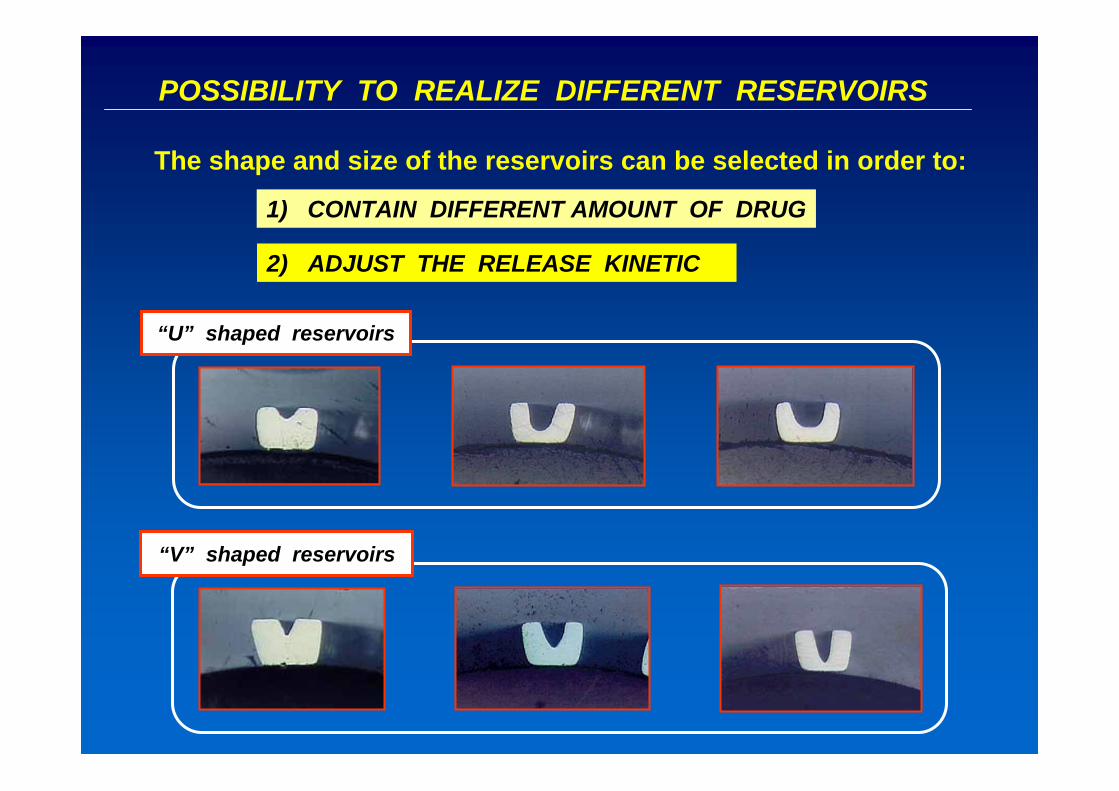
POSSIBILITY TO REALIZE DIFFERENT RESERVOIRS
“V” shaped reservoirs
“U” shaped reservoirs
The shape and size of the reservoirs can be selected in order to:
1) CONTAIN DIFFERENT AMOUNT OF DRUG
2) ADJUST THE RELEASE KINETIC

Different shape reservoirs
0102030405060708090
0 2 4 6 8 10 12 14 16 18 20 22 24
Time (h)
% d
rug
rele
ased
V shaped reservoirU shaped reservoir
EFFECT OF THE RESERVOIR SHAPE ON RELEASE KINETIC
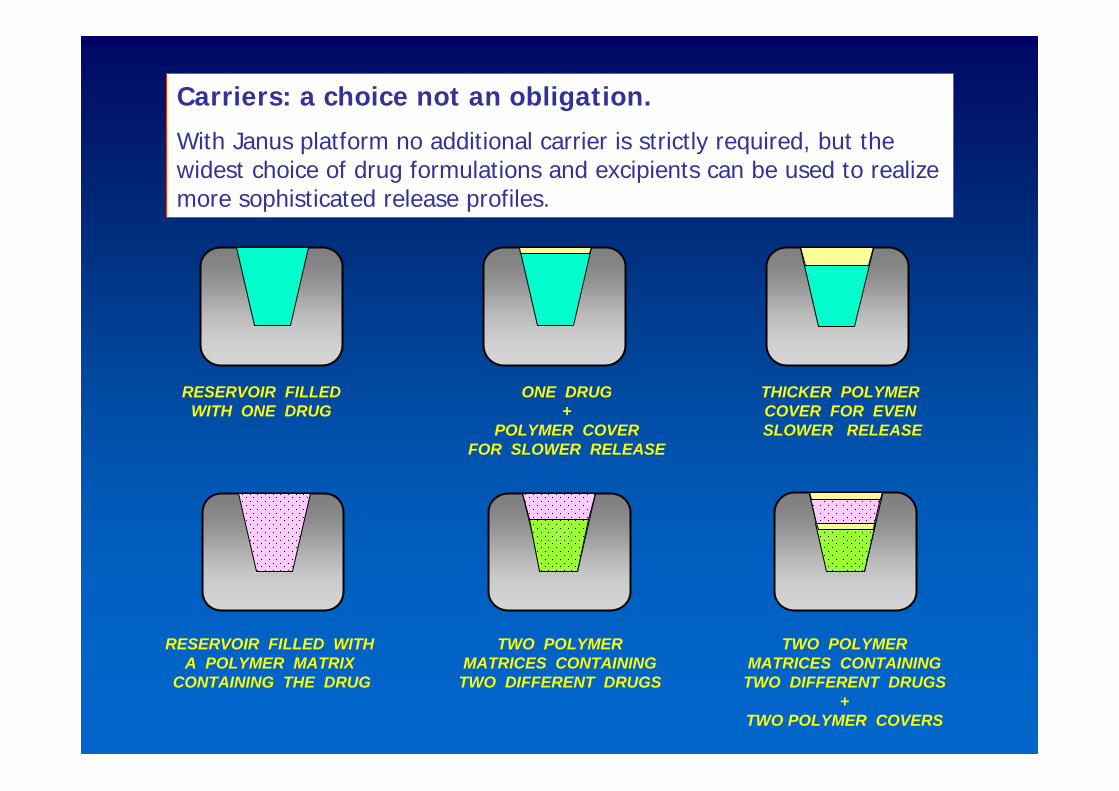
RESERVOIR FILLEDWITH ONE DRUG
ONE DRUG +
POLYMER COVER FOR SLOWER RELEASE
THICKER POLYMERCOVER FOR EVENSLOWER RELEASE
RESERVOIR FILLED WITH A POLYMER MATRIX
CONTAINING THE DRUG
TWO POLYMERMATRICES CONTAINING
TWO DIFFERENT DRUGS
TWO POLYMERMATRICES CONTAINING
TWO DIFFERENT DRUGS+
TWO POLYMER COVERS
Carriers: a choice not an obligation.
With Janus platform no additional carrier is strictly required, but the widest choice of drug formulations and excipients can be used to realizemore sophisticated release profiles.

SEM images of Sorin proprietarycarriers under evaluation
Porous matrix with top coat Porous matrix Tubular matrix
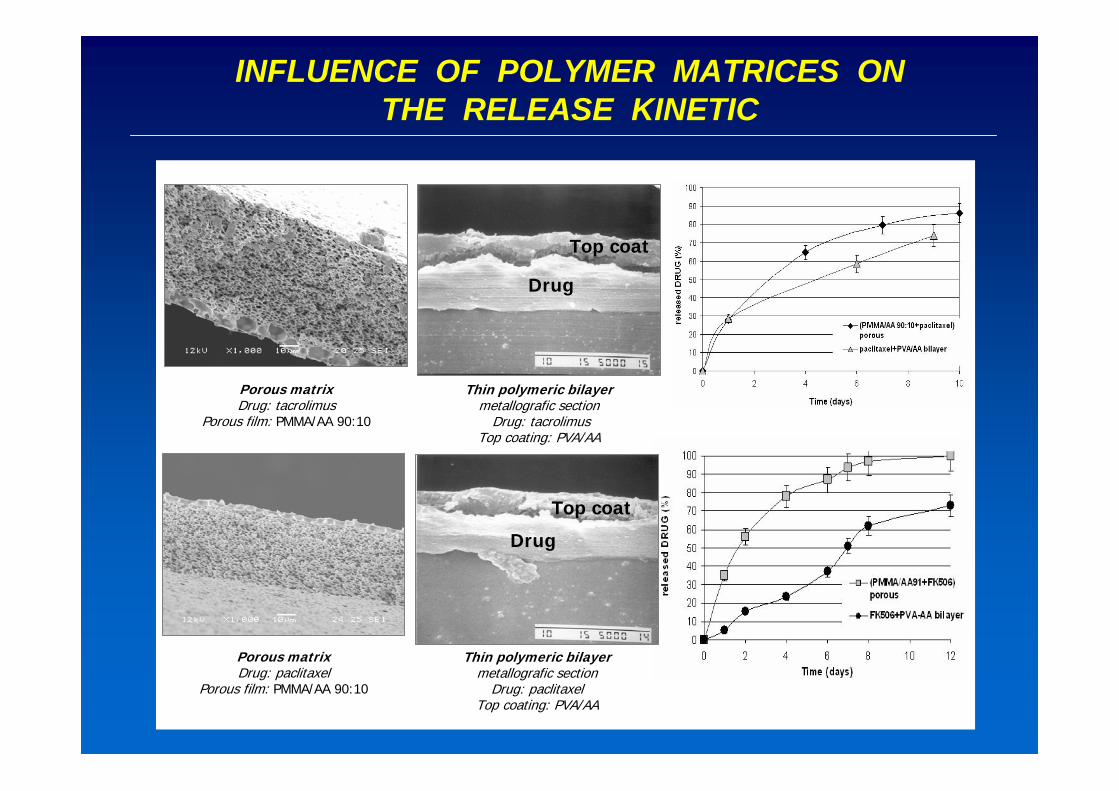
Thin polymeric bilayermetallografic section
Drug: tacrolimusTop coating: PVA/AA
Porous matrixDrug: paclitaxel
Porous film: PMMA/AA 90:10
Porous matrixDrug: tacrolimus
Porous film: PMMA/AA 90:10
Thin polymeric bilayermetallografic section
Drug: paclitaxelTop coating: PVA/AA
Drug
Top coat
Drug
Top coat
INFLUENCE OF POLYMER MATRICES ON THE RELEASE KINETIC
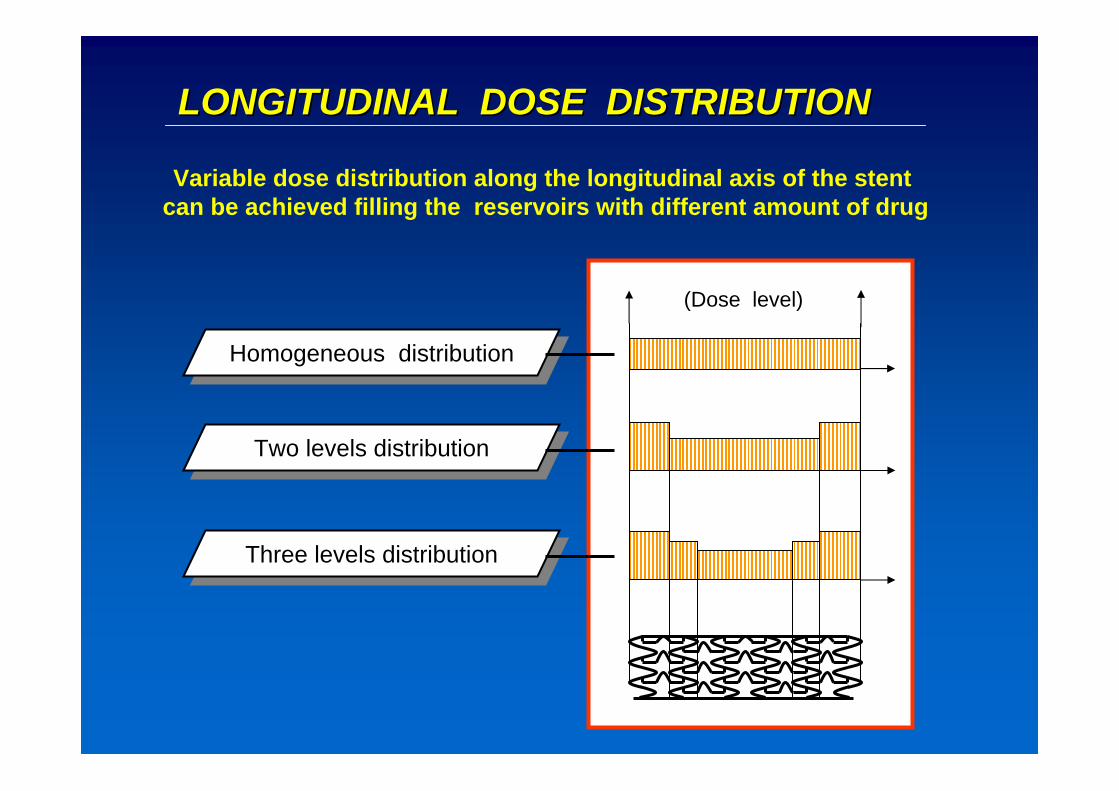
LONGITUDINAL DOSE DISTRIBUTIONLONGITUDINAL DOSE DISTRIBUTION
Variable dose distribution along the longitudinal axis of the stentcan be achieved filling the reservoirs with different amount of drug
Homogeneous distributionHomogeneous distribution
Two levels distributionTwo levels distribution
Three levels distributionThree levels distribution
(Dose level)

LONGITUDINAL DRUG / DOSE DISTRIBUTIONLONGITUDINAL DRUG / DOSE DISTRIBUTION
Suitable amount of different drugs can be loaded selectively alongthe longitudinal axis of the stent to provide synergic therapeutic effects
Homogeneous distributionof two different drugs
Homogeneous distributionof two different drugs
Two different drugs intwo different areas
Two different drugs intwo different areas
Three levels distributionThree levels distribution
(Dose level)

















