877 This study was supported by a grant from the Wellcome Trust. We thank the other members of the Uganda Buruli Group for their help and encouragement, and also Dr P. N. Williams, Dr Y. Y. Lee, Dr H. Coleridge, and Mr F. Onono; Dr P. D. Fowler of Geigy (U.K.) who supplied drugs and placebo; and the Chief Medical Officer, Ministry of Health, Uganda, for permission to publish. M. C. P. was on second- ment from the U.K. Medical .Research Council’s Statistical Research Unit, London. Requests for reprints should be addressed to W. D. L. R., Leicester City Health Department, Midland House, 52-54 Charles Street, Leicester LEI 1FN. REFERENCES 1. Revill, W. D. L., Morrow, R. H., Parson, W., Kiryabwire, J. W. M. in Medicine in a Tropical Environment (edited by A. G. Shaper, J. W. Kibukamusoke, and M. S. R. Hutt); p. 19. London, 1972. 2. Uganda Buruli Group. Trans. R. Soc. trop. Med. Hyg. 1971, 65, 763. 3. Barker, D. J. P. ibid. 1972, 67, 43. 4. Revill, W. D. L. Unpublished. 5. Revill, W. D. L. in Health and Disease in Africa (edited by G. C. Gould); p. 289. Nairobi, 1971. 6. Lunn, H. F., Rees, R. J. W. Lancet, 1964, i. 247. 7. MacCallum, P., Tolhurst, J. C., Buckle, G., Sissons, H. A. J. Path. Bact. 1948, 60, 93. 8. Uganda Buruli Group. Br. med. J. 1970, ii, 390. 9. Revill, W. D. L. Unpublished. 10. Stanford, J. L., Phillips, I. J. med. Microbiol. 1972, 5, 39. GENU VALGUM AND OSTEOPOROSIS IN AN AREA OF ENDEMIC FLUOROSIS K. A. V. R. KRISHNAMACHARI KAMALA KRISHNASWAMY National Institute of Nutrition, Indian Council of Medical Research, Hyderabad 500007, India Summary Twenty-four male patients with genu- valgum deformity drawn from an area of endemic fluorosis in Andhra Pradesh, India, were investigated clinically, radiologically, and biochemi- cally. All had evidence of spinal osteosclerosis along with extensive osteoporotic changes in the bones of the extremities. Levels of serum calcium, phosphorus, and alkaline-phosphatase activity were normal. It is concluded that deficiency of several nutrients may modify and aggravate the toxic effects of chronic fluoride intoxication. Hormones may play a part in the causation of the syndrome. Introduction ENDEMIC fluorosis is a well-defined clinical entity characterised by dental and skeletal changes. Endemic fluorosis due to the presence of high concentrations of fluoride in drinking-water has been reported from several parts of India 1-5 Bone changes characterised by osteosclerosis, ligamental calcification, and calcification of membranes and tendinous insertions had been reported among adults 3,! and children 6 living in areas of endemic fluorosis. Crippling deformities of skeleton due to fluoride toxicity such as kyphosis, stiffness of the spine, reduced mobility of bony cage, and bony exostoses have been reported from different parts of the world. We describe here a syndrome of genu aigum and extensive osteoporotic changes of the bones of the lower extremities associated with skeletal fluorosis. Patients and Methods The patients lived in an area of the State of Andhra Pradesh known to be endemic for fluorosis.3 Two hundred and twenty cases of the syndrome were observed in six villages situated miles apart. Twenty-four male patients aged between 8 and 40 years from three of the villages took part in detailed investigations. All of them were investigated clinically and radiologically. X-rays of the spine, knee-joints, and the left hand were taken along with an aluminium wedge as a standard, for the purpose of densitometric studies. X-rays of the skull, pelvis, fore- arm, upper arm, legs, and ribs were done in some patients. Serum calcium, inorganic-phosphorus, and alkaline- phosphatase activities were determined in eighteen patients. Serum-calcium was measured by Clark and Collip’s modification of the Kramer-Tisdall method.s Alkaline phosphatase was measured by the method of Bodansky as modified by Shinovara et al.l° Fiske and Subbarow’s method was used to estimate phosphorus.l1 The fluoride content of drinking-water samples obtained from the villages was estimated by the method described by Wadhwani.12 Results Clinical Features The typical clinical features are shown in fig. 1. Most patients were between the ages of 10 and 30 years. All had dental changes. Genu valgum, which became prominent while walking, was a striking feature. There was internal rotation and adduction of the hip. As a result, the gait was slow, laborious, and awkward. In severe cases there was flexion deformity of the knees. Almost all the patients had enlarged femoral condyles. In some of them the patella was externally rotated. In less severe cases, the deformity was masked in the supine position with full extension of the knee-joints, but reappeared on standing or on walking. In severe cases, the deformity prevented the patients from assuming Fig. 1-Four patients with severe genu valgum.
Transcript
877
This study was supported by a grant from the WellcomeTrust. We thank the other members of the Uganda BuruliGroup for their help and encouragement, and also Dr P. N.Williams, Dr Y. Y. Lee, Dr H. Coleridge, and Mr F. Onono;Dr P. D. Fowler of Geigy (U.K.) who supplied drugs andplacebo; and the Chief Medical Officer, Ministry of Health,Uganda, for permission to publish. M. C. P. was on second-ment from the U.K. Medical .Research Council’s StatisticalResearch Unit, London.
Requests for reprints should be addressed to W. D. L. R.,Leicester City Health Department, Midland House, 52-54Charles Street, Leicester LEI 1FN.
REFERENCES
1. Revill, W. D. L., Morrow, R. H., Parson, W., Kiryabwire, J. W. M.in Medicine in a Tropical Environment (edited by A. G. Shaper,J. W. Kibukamusoke, and M. S. R. Hutt); p. 19. London, 1972.
3. Barker, D. J. P. ibid. 1972, 67, 43.4. Revill, W. D. L. Unpublished.5. Revill, W. D. L. in Health and Disease in Africa (edited by G. C.
Gould); p. 289. Nairobi, 1971.6. Lunn, H. F., Rees, R. J. W. Lancet, 1964, i. 247.7. MacCallum, P., Tolhurst, J. C., Buckle, G., Sissons, H. A.
J. Path. Bact. 1948, 60, 93.8. Uganda Buruli Group. Br. med. J. 1970, ii, 390.9. Revill, W. D. L. Unpublished.
10. Stanford, J. L., Phillips, I. J. med. Microbiol. 1972, 5, 39.
GENU VALGUM AND OSTEOPOROSIS IN
AN AREA OF ENDEMIC FLUOROSIS
K. A. V. R. KRISHNAMACHARI
KAMALA KRISHNASWAMY
National Institute of Nutrition, Indian Council of MedicalResearch, Hyderabad 500007, India
Summary Twenty-four male patients with genu-valgum deformity drawn from an area
of endemic fluorosis in Andhra Pradesh, India, wereinvestigated clinically, radiologically, and biochemi-cally. All had evidence of spinal osteosclerosis alongwith extensive osteoporotic changes in the bones ofthe extremities. Levels of serum calcium, phosphorus,and alkaline-phosphatase activity were normal. Itis concluded that deficiency of several nutrients maymodify and aggravate the toxic effects of chronicfluoride intoxication. Hormones may play a partin the causation of the syndrome.
Introduction
ENDEMIC fluorosis is a well-defined clinical entitycharacterised by dental and skeletal changes.Endemic fluorosis due to the presence of highconcentrations of fluoride in drinking-water hasbeen reported from several parts of India 1-5 Bone
changes characterised by osteosclerosis, ligamentalcalcification, and calcification of membranes andtendinous insertions had been reported amongadults 3,! and children 6 living in areas of endemicfluorosis. Crippling deformities of skeleton due tofluoride toxicity such as kyphosis, stiffness of the
spine, reduced mobility of bony cage, and bonyexostoses have been reported from different partsof the world. We describe here a syndrome of genuaigum and extensive osteoporotic changes of the
bones of the lower extremities associated withskeletal fluorosis.
Patients and Methods
The patients lived in an area of the State of AndhraPradesh known to be endemic for fluorosis.3 Two hundredand twenty cases of the syndrome were observed in six
villages situated miles apart. Twenty-four male patientsaged between 8 and 40 years from three of the villagestook part in detailed investigations. All of them were
investigated clinically and radiologically. X-rays of thespine, knee-joints, and the left hand were taken along withan aluminium wedge as a standard, for the purpose ofdensitometric studies. X-rays of the skull, pelvis, fore-
arm, upper arm, legs, and ribs were done in some patients.Serum calcium, inorganic-phosphorus, and alkaline-
phosphatase activities were determined in eighteenpatients. Serum-calcium was measured by Clark and
Collip’s modification of the Kramer-Tisdall method.sAlkaline phosphatase was measured by the method ofBodansky as modified by Shinovara et al.l° Fiske andSubbarow’s method was used to estimate phosphorus.l1The fluoride content of drinking-water samples obtainedfrom the villages was estimated by the method describedby Wadhwani.12
Results
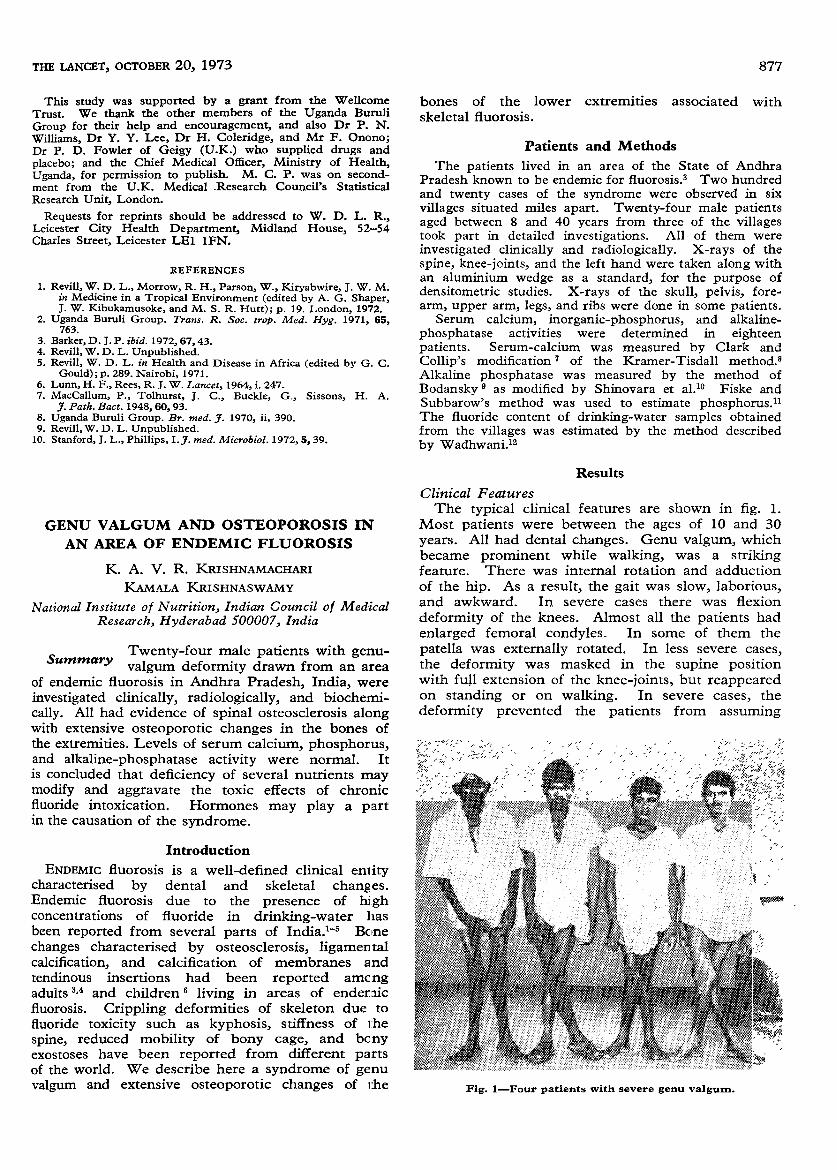
Clinical FeaturesThe typical clinical features are shown in fig. 1.
Most patients were between the ages of 10 and 30years. All had dental changes. Genu valgum, whichbecame prominent while walking, was a strikingfeature. There was internal rotation and adductionof the hip. As a result, the gait was slow, laborious,and awkward. In severe cases there was flexion
deformity of the knees. Almost all the patients hadenlarged femoral condyles. In some of them the
patella was externally rotated. In less severe cases,the deformity was masked in the supine positionwith full extension of the knee-joints, but reappearedon standing or on walking. In severe cases, the
deformity prevented the patients from assuming
Fig. 1-Four patients with severe genu valgum.
878
Fig. 2-Spinal X-ray showing osteosclerosis.
postures and performing movements of their choice,thereby crippling them. All patients were physicallyhandicapped and psychologically upset.The earliest evidence of the syndrome was seen
around the early school-age period, and by thefifteenth year the syndrome was fully manifest, witha male to female ratio of 15/1.
Radiological Features
Anteroposterior views of the cervicothoracic andlumbodorsal spine showed the presence of osteo-
sclerosis in all but two patients. The spinal ligamentswere calcified and typical " bamboo spine " was seenin most cases (fig. 2). Radiological evidence ofinterosseous membrane calcification was seen in allcases. Sclerosis of humerus, scapulx, ribs, radiusand ulna, and pelvic bones, together with calcificationof muscular attachments, were seen in all. The most
striking radiological feature, however, was severe
osteoporosis of the lower end of the femur and upperends of tibia and fibula and rarefaction of the meta-
carpal bones. In some patients, rarefaction of pelvicbones, femoral neck, and lower ends of radius andulna was also observed.
The metacarpals were rarefied with coarse
(? cystic) trabecular markings. Subcortical loss of
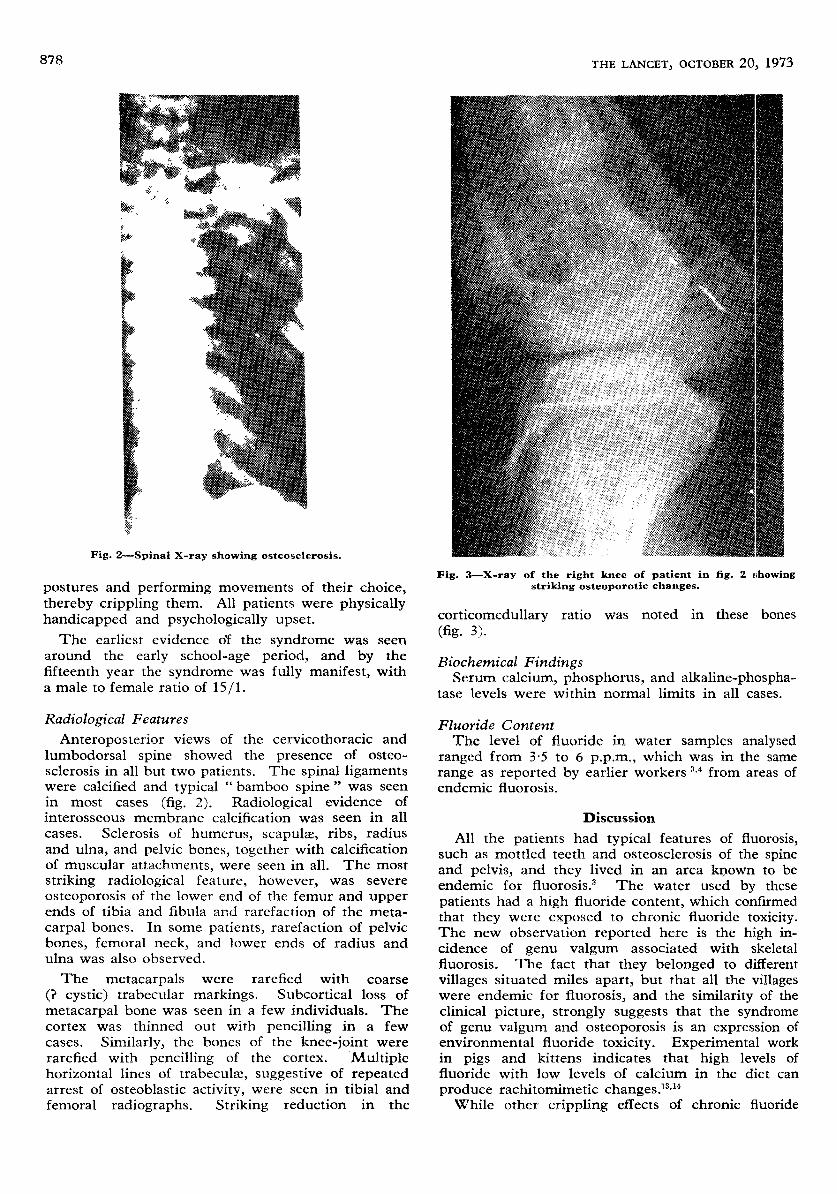
metacarpal bone was seen in a few individuals. Thecortex was thinned out with pencilling in a fewcases. Similarly, the bones of the knee-joint wererarefied with pencilling of the cortex. Multiplehorizontal lines of trabeculx, suggestive of repeatedarrest of osteoblastic activity, were seen in tibial andfemoral radiographs. Striking reduction in the
Fig. 3-X-ray of the right knee of patient in fig. 2 showingstriking osteoporotic changes.
corticomedullary ratio was noted in these bones
(fig. 3).
Biochemical FindingsSerum calcium, phosphorus, and alkaline-phospha-
tase levels were within normal limits in all cases.
Fluoride ContentThe level of fluoride in water samples analysed
ranged from 3,5 to 6 p.p.m., which was in the samerange as reported by earlier workers U from areas ofendemic fluorosis.
Discussion
All the patients had typical features of fluorosis,such as mottled teeth and osteosclerosis of the spineand pelvis, and they lived in an area known to beendemic for fluorosis.3 The water used by these
patients had a high fluoride content, which confirmedthat they were exposed to chronic fluoride toxicity.The new observation reported here is the high in-cidence of genu valgum associated with skeletalfluorosis. The fact that they belonged to different
villages situated miles apart, but that all the villageswere endemic for fluorosis, and the similarity of theclinical picture, strongly suggests that the syndromeof genu valgum and osteoporosis is an expression cfenvironmental fluoride toxicity. Experimental workin pigs and kittens indicates that high levels offluoride with low levels of calcium in the diet can
produce rachitomimetic changes.13,14While other crippling effects of chronic fluoride
879
toxicity such as kyphosis, rigid thoracic cage, and
compression of spinal cord have been reported to
affect people over 30 years of age,’," genu valgumwith osteoporosis was observed mostly among
adolescents, and, in a few cases, even among childrenless than 10 years of age.Hitherto, osteosclerosis had been described as the
characteristic and diagnostic radiological feature ofskeletal fluorosis. Radiological evidence of extensiveosteoporosis seen in several bones of the extremitiesin our patients therefore needs elucidation. The
radiodensity of bones of people from a poor socio-economic community is lower than that of bones ofpeople who are nutritionally better off. A dietarysurvey in this endemic fluorotic area indicates thatthe calcium intake was very low.3 Since the staplein the area is sorghum, which is relatively high inphytate content, the net calcium absorption may beexpected to be even lower. In skeletal fluorosis,the spinal column is the site of election. Spinalosteosclerosis resulting from chronic fluoride in-toxication may be expected to divert calciumpreferentially to the spinal column at the expenseof limb bones. In the presence of low dietary calciumintake such diversion may well result in osteoporosisof the limb bones. Sclerosis was observed in the
spine even among children under 10 years of agewith this syndrome. Why and how spinal sclerosisoccurs even with inadequate calcium intake needsfurther work.Predilection of this syndrome for males was another
interesting feature. This fact and the pre-adolescentnature of onset of the syndrome suggest that hor-mones may be involved in its pathogenesis. Thatmalnutrition modifies the clinical profile of fluorosisin developing countries had been suggested by thehigh rate of crippling deformities among poorindividuals residing in fluorotic areas.3,16 Theoccurrence of this syndrome among the poorer seg-ments of the populations is suggestive of detrimentalrole of undernutrition on fluoride-induced toxicity.The role of hormones, especially parathormone andcalcitonin, in the pathogenesis of this disorder also
requires consideration.
We thank Dr C. Gopalan and Dr S. G. Srikantia, NationalInstitute of Nutrition, Hyderabad, for their encouragement.Requests for reprints should be addressed to K. A. V. R. K.
REFERENCES
1. Shortt, H. E., Pandit, C. G., Raghavachari, T. N. S. Indian med.Gaz. 1937, 72, 396.
2. Daver, M. B. ibid. 1945, 80, 332.3. Siddiqui, A. H. Br. med. J. 1955, ii, 1408.4. Singh, A., Jolly, S. S. Q. Jl Med. 1961, 30, 353.5 Teotia, S. P. S., Kunwar, K. B., Teotia, M. Fluoride, 1969, 2, 144.6. Teotia, M., Teotia, S. P. S., Kunwar, K. B. Archs Dis. Childh.
1971, 46, 686.7. Clark, E. P., Collip, J. B. J. biol. Chem. 1925, 63, 461.8. Kramer, B., Tisdall, F. F. ibid. 1921, 47, 475.9. Bodansky, A. ibid. 1932, 99, 197.
10. Shinovara, G. Y., Jones, L. M., Reinhart, H. L. ibid. 1942, 142, 921.11. Fiske, C. H., Subbarow, Y. ibid. 1925, 66, 375.12. Wadhwani, T. K. J. Indian Inst. Sci. 1952, 34, 135.13. Bellanger, L. F., Visekh, W. J., Lotz, W. E., Comar, C. L. Am. J.
Path. 1958, 34, 23.14 Burkhart, J. M., Jowsey, J. J. Lab. clin. Med. 1968, 72, 943.
Singh, A., Jolly, S. S., Bansal, B. C., Mathur, O. C. Medicine,Baltimore, 1963, 42, 229.
16. Singh, A., Jolly, S. S., Devi, P., Bansal, B. C., Singh, S. S. IndianJ. med. Res. 1962, 50, 387.
RE-EVALUATION OF NITROBLUE-
TETRAZOLIUM TEST
A. W. SEGAL SHEILA F. TRUSTEY
A. J. LEVI
Divisions of Clinical Investigation and Hospital Infection,Northwick Park Hospital and Clinical Research
Centre, Harrow HA1 3UJ, Middlesex
Summary The nitroblue tetrazolium (N.B.T.) test
has been widely recognised as a usefulmethod of distinguishing between pyogenic bacterialinfection and other disease processes. This test, doneby two different methods, has been re-evaluated on223 individuals including healthy controls and patientswith a wide spectrum of disease. There was a wide
overlap in the results obtained from controls, patientswith pyogenic infection, and patients with other dis-eases; and the test had no diagnostic relevance. TheN.B.T. result in patients with pyogenic infection wasfound to correlate with the severity of the illness.There was poor agreement between the resultsobtained from the two methods used for the test.
Significant observer error was found in interpretationof the results and this was related to observer experi-ence. The test has not upheld its early promise asa simple accurate method of distinguishing bacterialinfection from other disease processes.
Introduction
THE nitroblue tetrazolium (N.B.T.) test was devel-
oped in 1968 by Park et al.1 as a non-specific in-vitrodiagnostic test for bacterial infection. Heparinisedblood is incubated with a dilute solution of N.B.T.,and the percentage of neutrophils containing depositsof dark-blue formazan, the reduced product of N.B.T.,within their cytoplasm is counted. In patients withbacterial or fungal infections the percentage of neutro-phils containing formazan, called N.B.T.-positive cells,was greater than 10 % ; in healthy controls and patientswith non-pyogenic diseases the percentage of N.B.T.-positive cells was less than 10%. These findings havebeen confirmed in children 2e and adults,4·5 and thelist of diseases resulting in a positive test has beenexpanded to include malaria and helminthic andMycoplasma infections.8 Occasional false-negativeresults have been recorded, and these have beenattributed to an inability of the neutrophils to respondto the stimulus of infection. To distinguish true andfalse-negative results an in-vitro stimulation test,using Escherichia coli endotoxin, was developed 9 to
indicate the ability of neutrophils to respond to
stimulation.One of the technical difficulties of the test, as
described by Park, is the tendency of neutrophils toclump around particles, since shown to be precipi-tated fibrinogen and heparin.1o This makes identifica-tion and counting difficult. Clumping can be reducedby the use of ethylenediamine tetra-acetic acid
(E.D.T.A.) instead of heparin as anticoagulant, but thisreduces the sensitivity of the test; Gordon et al.11showed that the addition of the sucrose polymer’ Ficoll’ to the incubation mixture prevented thisloss of sensitivity and clumping of the cells.