93
GERIATRIC SYNDROMES FARHAD ZARGARI, MD, PHD
| Date post: | 15-Jul-2015 |
| Category: |
Healthcare |
| Upload: | farhad-zargari |
| View: | 328 times |
| Download: | 1 times |

GERIATRIC
SYNDROMES
FARHAD ZARGARI, MD, PHD

GERIATRIC SYNDROMES

GERIATRIC SYNDROMES
1-Disability
2-Dementia and Delirium
3-Falls
4-Poly-pharmacy
5-Pressure Ulcers
6-Urinary Incontinence

DISABILITY

1-LONGER LIVES AND DISABILITY
Are we living healthier as well as longer lives, or are our
additional years spent in poor health? There is
considerable debate about this question among
researchers, and the answers have broad implications for
the growing number of older people around the world.
One way to examine the question is to look at changes
in rates of disability, one measure of health and function.

1-LONGER LIVES AND DISABILITY
Disability is part of the human condition. Almost everyone
will be temporarily or permanently impaired at some
point in life, and those who survive to old age will
experience increasing difficulties in functioning.

1-LONGER LIVES AND DISABILITY
Disability is the umbrella term for impairments, activity
limitations and participation restrictions, referring to the
negative aspects of the interaction between an
individual (with a health condition) and that individual’s
contextual factors (environmental and personal factors).

1-LONGER LIVES AND DISABILITY
Disability is “an evolving concept”, also “disability results
from the interaction between persons with impairments
and attitudinal and environmental barriers that hinder
their full and effective participation in society on an
equal basis with others”. Defining disability as an
interaction means that “disability” is not an attribute of
the person.

1-LONGER LIVES AND DISABILITY
Responses to disability have changed since the 1970s,
prompted largely by the self-organization of people with
disabilities, and by the growing tendency to see disability
as a human rights issue. Historically, people with
disabilities have largely been provided for through
solutions that segregate them, such as residential
institutions and special schools. Policy has now shifted
towards community and educational inclusion, and
medically- focused solutions have given way to more
interactive approaches recognizing that people are
disabled by environmental factors as well as by their
bodies.

1-LONGER LIVES AND DISABILITY
Disability encompasses the child born with a congenital
condition such as cerebral palsy or the young soldier
who loses his leg to a land-mine, or the middle-aged
woman with severe arthritis, or the older person with
dementia, among many others.

DISABILITY AND HUMAN RIGHTS
Disability is a human rights issue because:
People with disabilities experience inequalities – for example,
when they are denied equal access to health care,
employment, education, or political participation because of
their disability.
People with disabilities are subject to violations of dignity – for
example, when they are subjected to violence, abuse,
prejudice, or disrespect because of their disability.
Some people with disability are denied autonomy – for
example, when they are subjected to involuntary sterilization,
or when they are confined in institutions against their will, or
when they are regarded as legally incompetent because of
their disability.

DISABILITY AND DEVELOPMENT
Disability is a development issue, because of its
bidirectional link to poverty: disability may increase the
risk of poverty, and poverty may increase the risk of
disability. A growing body of empirical evidence from
across the world indicates that people with disabilities
and their families are more likely to experience
economic and social disadvantage than those without
disability.

1-LONGER LIVES AND DISABILITY
Some researchers think there will be a decrease in the
prevalence of disability as life expectancy increases,
termed a “compression of morbidity.” Others see an
“expansion of morbidity”—an increase in the prevalence
of disability as life expectancy increases. Yet others
argue that, as advances in medicine slow the
progression from chronic disease to disability, severe
disability will lessen, but milder chronic diseases will
increase.

1-LONGER LIVES AND DISABILITY
In the United States, between 1982 and 2001 severe
disability fell about 25 percent among those aged 65 or
older even as life expectancy increased. This very
positive trend suggests that we can affect not only how
long we live, but also how well we can function with
advancing age. Unfortunately, this trend may not
continue in part because of rising obesity among those
now entering older ages.

1-LONGER LIVES AND DISABILITY
The analysis of the Global Burden of Disease estimates
that 15.3% of the world population (some 978 million
people of the estimated 6.4 billion in 2004 had
“moderate or severe disability”, while 2.9% or about 185
million experienced “severe dis- ability”. Among those
aged 0–14 years, the figures were 5.1% and 0.7%, or 93
million and 13 million children, respectively. Among those
15 years and older, the figures were 19.4% and 3.8%, or
892 million and 175 million, respectively.

1-LONGER LIVES AND DISABILITY
Based on 2010 population estimates – 6.9 billion with 5.04
billion 15 years and over and 1.86 billion under 15 years –
and 2004 disability prevalence estimates (World Health
Survey and Global Burden of Disease) there were around
785 (15.6%) to 975 (19.4%) million persons 15 years and
older living with disability. Of these, around 110 (2.2%) to
190 (3.8%) million experienced significant difficulties in
functioning. Including children, over a billion people (or
about 15% of the world’s population) were estimated to
be living with disability.

1-LONGER LIVES AND DISABILITY
Fig. 2.1. Global disability prevalence estimates from
different sources:
This figure compares the
population-weighted average
prevalence of disability for
high-income, middle- income,
and low-income countries
from multiple sources. The solid
grey bars show the average
prevalence based on
available data, the range lines
indicate the 10th and 90th
percentiles for available
country prevalence within
each income group. The data
used for this figure are not age
standardized and cannot be
directly compared with Table
2.1 and Table 2.3. WHS = World
Health Survey; GBD = the
Global Burden of Disease, 2004

1-LONGER LIVES AND DISABILITY
Age-specific disability prevalence, derived from multi-
domain functioning levels in 59 countries, by country
income level and sex:

1-LONGER LIVES AND DISABILITY
Age-specific disability prevalence, derived from multi-
domain functioning levels in 59 countries, by country
income level and sex:

1-LONGER LIVES AND DISABILITY
1-LONGER LIVES AND DISABILITY
American adults reported worse health than did
European adults as indicated by the presence of chronic
diseases and by measures of disability. At all levels of
wealth, Americans were less healthy than their European
counterparts. Analyses of the same data sources also
showed that cognitive functioning declined further
between ages 55 and 65 in countries where workers left
the labor force at early ages, suggesting that
engagement in work might help preserve cognitive
functioning.

1-LONGER LIVES AND DISABILITY
Prevalence of
Chronic Disease and
Disability among Men
and Women Aged
50-74 Years in the
United States,
England, and Europe:
2004
Source: Adapted from Avendano
M, Glymour MM, Banks J,
Mackenbach JP. Health
disadvantage in US adults aged 50
to 74 years
REHABILITATION
Rehabilitation as “a set of measures that assist individuals
who experience, or are likely to experience, disability to
achieve and maintain optimal functioning in interaction
with their environments”. A distinction is sometimes made
between habilitation, which aims to help those who
acquire disabilities con- genitally or early in life to
develop maximal functioning; and rehabilitation, where
those who have experienced a loss in function are
assisted to regain maximal functioning.

DEMENTIA
2-THE BURDEN OF DEMENTIA
Physicians often define dementia based on the criteria
given in the Diagnostic and Statistical Manual of Mental
Disorders (DSM). In 2013 the American Psychiatric
Association released the fifth edition of the DSM (DSM-5),
which incorporates dementia into the diagnostic
categories of major and mild neurocognitive disorders.

2-THE BURDEN OF DEMENTIA
To meet DSM-5 criteria for major neurocognitive disorder,
an individual must have evidence of significant cognitive
decline (for example, decline in memory, language or
learning), and the cognitive decline must interfere with
independence in everyday activities (for example,
assistance may be needed with complex activities such
as paying bills or managing medications). To meet DSM-5
criteria for mild neurocognitive disorder, an individual
must have evidence of modest cognitive decline, but
the decline does not interfere with everyday activities
(individuals can still perform complex activities such as
paying bills or managing medications, but the activities
require greater effort).
2-THE BURDEN OF DEMENTIA
Dementia is a syndrome due to disease of the brain –
usually of a chronic or progressive nature – in which there
is disturbance of multiple higher cortical functions,
including memory, thinking, orientation, comprehension,
calculation, learning capacity, language, and
judgment. Consciousness is not clouded. The
impairments of cognitive function are commonly
accompanied, and occasionally preceded, by
deterioration in emotional control, social behavior, or
motivation. This syndrome occurs in a large number of
conditions primarily or secondarily affecting the brain.

2-THE BURDEN OF DEMENTIA
The cause of most dementia is unknown, but the final
stages of this disease usually means a loss of memory,
reasoning, speech, and other cognitive functions. The risk
of dementia increases sharply with age and, unless new
strategies for prevention and management are
developed, this syndrome is expected to place growing
demands on health and long term care providers as
population ages.

2-THE BURDEN OF DEMENTIA
The disease is not easy to diagnose, especially in its early
stages. The memory problems, misunderstandings, and
behavior common in the early and intermediate stages
are often attributed to normal effects of aging,
accepted as personality traits, or simply ignored.

2-THE BURDEN OF DEMENTIA
Many cases remain undiagnosed even in the
intermediate, more serious stages. A cross-national
assessment conducted by the Organization for
Economic Cooperation and Development (OECD)
estimated that dementia affected about 10 million
people in OECD member countries around 2000, just
under 7 percent of people aged 65 or older.

2-THE BURDEN OF DEMENTIA

2-THE BURDEN OF DEMENTIA

2-THE BURDEN OF DEMENTIA

2-THE BURDEN OF DEMENTIA

2-THE BURDEN OF DEMENTIA

2-THE BURDEN OF DEMENTIA
Types of Dementia
Alzheimer’s disease
Vascular dementia=Post-stroke dementia
Dementia with Lewy bodies (DLB)
Frontotemporal lobar degeneration (FTLD)
Mixed dementia
Parkinson’s disease (PD) dementia
CreutzfeldtJakob disease
Normal pressure hydrocephalus

2-THE BURDEN OF DEMENTIA
The total number of people with dementia worldwide in
2010 is estimated at 35.6 million and is projected to
nearly double every 20 years, to 65.7 million in 2030 and
115.4 million in 2050. The total number of new cases of
dementia each year worldwide is nearly 7.7 million,
implying one new case every four seconds.

2-THE BURDEN OF DEMENTIA
The total estimated worldwide costs of dementia were
US$ 604 billion in 2010. In high-income countries, informal
care (45%) and formal social care (40%) account for the
majority of costs, while the proportionate contribution of
direct medical costs (15%) is much lower. In low-income
and lower-middle-income countries direct social care
costs are small, and informal care costs (i.e. unpaid care
provided by the family) predominate.

2-THE BURDEN OF DEMENTIA
Alzheimer’s disease(AD) is the most common form of
dementia and accounted for between two-fifth and four
fifth of all dementia cases cited in the OECD report. More
recent analyses have estimated the worldwide number
of people living with AD/dementia at between 27 million
and 36 million. The prevalence of AD and other
dementias is very low at younger ages, then nearly
doubles with every five years of age after age 65.

2-THE BURDEN OF DEMENTIA
In the OECD review, for example, dementia affected
fewer than 3 percent of those aged 65 to 69, but almost
30 percent of those aged 85 to 89. More than one-half of
women aged 90 or older had dementia in France and
Germany, as did about 40 percent in the United States,
and just under 30 percent in Spain.

2-THE BURDEN OF DEMENTIA
The projected costs of caring for the growing numbers of
people with dementia are daunting. The 2010 World
Alzheimer Disease Report estimates that the total
worldwide cost of dementia exceeded US$600 billion in
2010, including informal care provided by family and
others, social care provided by community care
professionals, and direct costs of medical care. Family
members often play a key caregiving role, especially in
the initial stages of what is typically a slow decline. Ten
years ago, U.S. researchers estimated that the annual
cost of informal caregiving for dementia in the United
States was US$18 billion.
2-THE BURDEN OF DEMENTIA
The complexity of the disease and the wide variety of
living arrangements can be difficult for people and
families dealing with dementia, and countries must cope
with the mounting financial and social impact. The
challenge is even greater in the less developed world,
where an estimated two-thirds or more of dementia
sufferers live but where few coping resources are
available.
2-THE BURDEN OF DEMENTIA
Projections by World Alzheimer Disease Report suggest
that 115 million people worldwide will be living with
AD/dementia in 2050, with a markedly increasing
proportion of this total in less developed countries.
2-THE BURDEN OF DEMENTIA
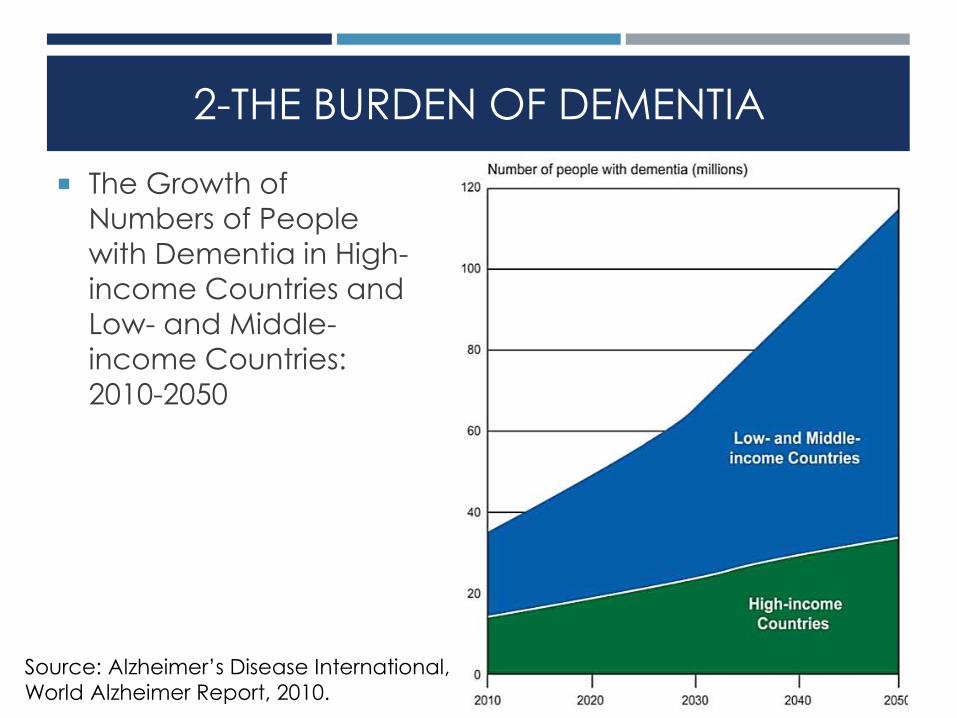
The Growth of
Numbers of People
with Dementia in High-
income Countries and
Low- and Middle-
income Countries:
2010-2050
Source: Alzheimer’s Disease International,
World Alzheimer Report, 2010.

GERIATRIC FALLS

HELP! I’VE FALLEN AND I CAN’T GET UP!

3-GERIATRIC FALLS
Falls are the leading cause of external injuries.
Most common in children less than 5 years old and adults 65
and older.
Trauma is the 5th cause of death in those >65 years
Falls are responsible for 70% of accidental deaths in
people over 75 years old.
1/4 of the elderly people who fracture their hips die
within 6 months of the injury.
35%-40% of people 65+ fall each year. Those who
fall are 2-3 times more likely to fall again.
10%-20% of falls cause serious injuries.

3-GERIATRIC FALLS
Falls are the leading cause of external injuries.
Most common in children less than 5 years old and adults 65
and older.
Trauma is the 5th cause of death in those >65 years.
Falls are responsible for 70% of accidental deaths in
people over 75 years old.
1/4 of the elderly people who fracture their hips die
within 6 months of the injury.

3-GERIATRIC FALLS
Up to 20-30% of falls in older adults result in an injury
requiring medical care
Most fractures in Medicare population are due to falls
Falls in older adults are the leading cause of traumatic
brain injury
Men have a higher rate of fatal falls (due to TBI)
Women are more likely to have non-fatal falls

3-GERIATRIC FALLS
Age GroupFirst Leading
of Trauma Death
Second Leading
Cause of
Death
35 – 64Motor Vehicle
36.8%
Falls
29.6%
65+Falls
43.3%
Motor Vehicle
10.2%
3-GERIATRIC FALLS
Consequences of Geriatric Falls
Death
Injury
Fractures 10-15%
Hip 1-2%
Long Lie
Fear of Falling
Reduced Activity/Independence (25%)

3-GERIATRIC FALLS-HIP FRACTURE
In 1996 more than 250,000 older Americans had fractured hips.
90% are associated with falls
Excess of $10 billion
Leading fall-related injury that results in hospitalization –which are often prolonged and costly.
What Happens After the Hip Fracture?
One in four people that have a hip fracture that lived independently before the fracture had to live in a nursing home for a year afterward, according to the CDC.
Some never recover their balance and strength.
This can lead to depression and dementia and a downhill spiral.
Unfortunately 1/4 of the elderly people who fracture their hips die within 6 months of the injury.

3-GERIATRIC FALLS-BRAIN INJURY
Also a common injury following a fall
Many elderly on “blood thinners”
Symptoms may be subtle and not apparent at the time
of injury.

RISK FACTORS FOR FALLS
Increased age
Living alone
Previous falls
Use of a cane or walker
Acute illness
Reduced vision
Glare intolerance
Altered depth perception
Decreased night vision
Decline in peripheral vision

RISK FACTORS FOR FALLS
CVA that results in hemiparesis, sensory and/or
motor function deficits.
Decreased range of motion and flexibility in lower
legs and spine.
Weakness
Decreased step length (short shuffling steps)
Alzheimer’s or dementia
Arthritis
Parkinson’s disease
Foot problems
Toenail length, callouses, bunions, deformities

RISK FACTORS FOR FALLS
Difficulty rising from a chair
Neurologic changes
Slowed reaction times
Diminished sensory awareness for light touch, vibration,
and temperature
Decline in proprioception
Decreased hearing
Impaired speech discrimination
Excessive cerumen accumulation
Loss of high frequency tones
Risky behaviors

RISK FACTORS FOR FALLS
Medications
Some antidepressants
Sedatives
Some antihypertensive and cardiac medications
Hypoglycemic drugs
Alcohol

3-GERIATRIC FALLS
American Geriatrics Society: Most Common Intrinsic Fall
Risk Factors
Muscle weakness: 4.4
History of falls: 3.0
Gait or balance deficit: 2.9
Use of assistive device: 2.6
Visual deficit: 2.5
Arthritis: 2.4
Depression: 2.2
Cognitive impairment: 1.8
Age over 80 years: 1.7
Data from AGS Panel on Falls Prevention. Guideline for the prevention of falls in older
persons. J Am Geriatr Soc 2001;49(5):664–72.

4-POLY-PHARMACY
POLYPHARMACY-DEFINITION
Polypharmacy means “many drugs.”
In practice, polypharmacy refers to the use of more
medication than is clinically indicated or warranted.
Polypharmacy can result in a gradual accumulation of
side effects and/or adverse drug reactions, which
negatively effects elders’ health and well-being.

POLYPHARMACY-DEFINITION
Polypharmacy is the use of four or more medications by
a patient, generally adults aged over 65 years.
Polypharmacy (ie, the use of multiple medications
and/or the administration of more medications than are
clinically indicated, representing unnecessary drug use) is
common among the elderly, affecting about 40% of
older adults living in their own homes.

POLYPHARMACY-DEFINITION
Although polypharmacy can be appropriate, it is more
often inappropriate. Concerns about polypharmacy
include increased adverse drug reactions, drug
interactions, prescribing cascade, and higher costs.
Polypharmacy is often associated with a decreased
quality of life, decreased mobility and cognition.

POLYPHARMACY-DEFINITION
Patients at greatest risk for negative polypharmacy
consequences include the elderly, psychiatric patients,
patients taking five or more drugs concurrently, those
with multiple physicians and pharmacies, recently
hospitalized patients, individuals with concurrent
comorbidities, low educational level, and those with
impaired vision or dexterity.

POLYPHARMACY-DEFINITION
The literature review found that polypharmacy continues
to increase and is a known risk factor for important
morbidity and mortality.

POLYPHARMACY-DEFINITION
Older adults comprise 12% of the U.S. population, but use
35% of the prescription medications and 50 percent of
the over-the-counter medications.
The average medication usage for persons over 65 is:
2 to 6 prescription drugs, plus …
1 to 3.4 over-the-counter medicines.
In 2011, 58 percent of adults 65 years or older reported
taking 5 or more medications and 18% reported taking
10 or more (Slone Epidemiology Center).
The average American senior spends $870 annually for
pharmaceuticals.

POLYPHARMACY-CAUSES
1-Age:
Community elders- 90% > 1med; 40% > 5meds; 12% > 10meds.
Highest number of drugs per person in greater than 80 year
olds

POLYPHARMACY-CAUSES
2-Chronic Diseases:
Increased prevalence of somatic complaints and chronic
disease

POLYPHARMACY-CAUSES
3-Drug Regimen Changes:
New meds, different doses…
Changes from generic to brand- nomenclature, color and/or
shape

POLYPHARMACY-CAUSES
4-Providers – Patients Relationship:
The more the providers and physician visits, the more the
number of medications patients take.
2/3 of all physician visits end with a prescription.
Expectations to receive medication is growing from the patient
side.
Shortage in communicating with PCP about medications
changes.
Self-treatment

POLYPHARMACY-COMPLICATIONS
Polypharmacy leads to:
More adverse drug reactions.
Decreased adherence to drug regimens.
Higher rates of disease symptomatology.
(Unnecessary) drug expenses.
All of the above contribute to client distress and poorer
quality of life, which are of great concerns.

POLYPHARMACY-COMPLICATIONS
Polypharmacy leads to:
More adverse drug reactions (ADR).
Decreased adherence to drug regimens.
Higher rates of disease symptomatology.
(Unnecessary) drug expenses.
All of the above contribute to client distress and poorer
quality of life, which are of great concerns.

ADVERSE DRUG REACTIONS
Side effects: considered minor enough to allow
continuation of therapy.
Adverse Drug Reactions (ADRs): May necessitate
discontinuation of drug and require treatment of adverse
event.

ADVERSE DRUG REACTIONS
An adverse drug reaction (ADR) is defined as the unwanted, negative consequences associated with the use of a medications or medications.
Over 100,000 deaths a year are attributed to adverse drug reactions, making ADRs the fourth leading cause of death in the U.S. (Lazarou, Pomeranz, & Corey, 2009).
Other examples of ADRs include:
Peptic ulcers
Anemia
Deceased white blood cell production (which increases infection risk)
Liver damage
Kidney damage
Confusion/drowsiness (which can lead to falls and subsequent injuries)

ADVERSE DRUG REACTIONS
About 3 to 7% of all hospital admissions in the United
States are for treatment of adverse drug reactions.
Elderly 7 times more likely to have unwanted side effect
and 2-3 times more likely to have ADRs
Adverse drug reactions occur during 10 to 20% of
hospital admissions, and about 10 to 20% of these
reactions are severe.
The most consistent risk factor for an adverse drug
reactions is:
The number of drugs being taken.
Multiple medications is the factor most strongly
correlated with increased risk of ADRs. Exponential
increase in ADRs with addition of more drugs to a
regimen (2 drugs-15%, 5 drugs-50-60% ).

ADVERSE DRUG REACTIONS
1
10
100
0 2 4 6 8 10 12 14 16 18 20
number of drugs taken
per
cen
t of
pat
ien
ts w
ith
AD
R

ADVERSE DRUG REACTIONS
Other risk factors for ADRs include:
Having six or more chronic diseases.
Taking twelve or more doses of medication (of any type) per
day.
Taking nine or more medications total.
Having had a prior adverse drug reaction.
Being older than 85 years (this is important because persons 85
and older are the fastest growing segment of the population).
Having decreased kidney function.

ADVERSE DRUG REACTIONS
Drugs most frequently associated with adverse reactions
in the elderly:
Psychotropic drugs, especially benzodiazepines (valium,
ativan)
Anti-hypertensive agents (blood pressure medications)
Diuretics
Digoxin (a heart medication)
NSAIDS (Non-steroidal anti-inflammatory drugs, i.e. aspirin,
Aleve, celebrex)
Corticosteroids (i.e. prednisone - often used to treat arthritis)
Warfarin (coumadin - a blood thinner for treating blood clots)
Theophylline (theo-dur - for treating COPD, asthma)

PHARMACOKINETICS AND AGING
Pharmacokinetics means “What the body does to the
drug.”
It refers to the following functions by which the body
processes medications:
Absorption
Distribution
Metabolism
Excretion
Normal changes in these processes that occur with
aging increase the risk of adverse medication reactions
among older adults.

PHARMACOKINETICS AND AGING
Absorption
Age-related changes in the gastrointestinal tract and skin seem
to have little impact on medication usage.
So fortunately, there is not much to worry about here, however,
this is not the case for other components of medication
metabolism…

PHARMACOKINETICS AND AGING
Distribution
Important age-related changes:
Decrease in lean body mass and total body water.
Increased percentage body fat.
Increase in volume of distribution for fat-dissolving drugs, such
as sedatives (I.e. valium, dalmane, librium) that penetrate the
central nervous system.
This means older adults need most lower dosages of such
medications to achieve a therapeutic effect; they are at risk
for toxicity at doses considered normal for younger persons.
Protein-binding changes with aging are of modest significance
for most drugs, especially at steady-state (when the amount of
drug going in is the same as the amount of drug going out).

PHARMACOKINETICS AND AGING
Metabolism
Many medications are processed by the liver.
Although liver function is relatively unchanged with age, there
is some overall decline in metabolic capacity.
Plus, many of the chronic conditions common among older
adults do negatively impact liver function.
Decreased liver mass and hepatic blood flow lead to:
High variability with no good estimation algorithms for doctors
to determine appropriate medication dosages for older adults.
Minimal clinical manifestations of actual underlying problems,
so it is difficult for doctors to determine when someone may be
having problems.

PHARMACOKINETICS AND AGING
Renal Excretion
Medications are eliminated from the body via the kidneys and
urinary system.
Age-related decreases in renal blood flow and kidney function
(specifically, glomerular filtration rate) impact older adults’
ability to eliminate medications.
In addition, decreased lean body mass leads to decreased
creatinine production (a measure of kidney function, with high
levels being a cause for concern), thus, for older adults serum
creatinine may appear normal even when significant renal
impairment exists!

PHARMACODYNAMICS AND AGING
Pharmacodynamics is the opposite of pharmacokinetics;
it refers to “What the drug does to the body.”
Generally, lower drug doses are required to achieve the
same effect with advancing age.
This is because:
Receptor numbers, affinity, or post-receptor cellular effects
may change with age.
Changes in homeostatic mechanisms can increase or
decrease drug sensitivity.

PHARMACODYNAMICS AND AGING
Panels of experts in pharmacology and geriatrics have
compiled lists of medications to avoid prescribing for
patients 65 years of age or older.
The most commonly used list is the Beers criteria, which
include 48 "potentially inappropriate medications" (PIMs)
for which there are more effective or safer alternatives
for older patients (Fick, et al, 2003).

PHARMACODYNAMICS AND AGING
However in spite of the Beers criteria:
Numerous studies in the last 15 years have found that PIMs
continue to be used in 12% to 40% of older patients in
community and nursing home settings (Raebel, Charles,
Dugan, & et al, 2007).
Administrative data from nearly 400 hospitals across the United
States reveals that nearly half of all older patients hospitalized
for 7 common conditions were prescribed at least 1 PIM
(Rothberg et al, 2008).

PHARMACODYNAMICS AND AGING
Such irrational polypharmacy can arise from several
factors:
The prescriber hesitates to discontinue medications the patient
has been taking a long time.
The prescriber may add more drugs to the patient's regimen
without removing any.
The prescriber orders medication to alleviate adverse reactions
to other medications.
he patient may be influenced by anecdotal reports touting the
benefits of certain medications.

MEDICATION NON-ADHERENCE
Sometimes being on multiple medications contributes to
patients not taking those medications as the physician
intended.
Not taking medications as prescribed.
Correlates more strongly with number of meds, rather
than age.
It is important to recognize that medication non-
adherence is a two-way street!
Physician factors play a role.
Patient factors play a role.
MEDICATION NON-ADHERENCE
Example contributing factors:
Patients
Underreporting symptoms
Use of multiple providers
Use of others’ medications
Physicians
Limited time for discussion, diagnostics
Limited knowledge of geriatric pharmacology
The power of inertia
MEDICATION NON-ADHERENCE
Additional contributing factors:
Large number of medications
Cost and other social barriers
Complexity of medication regimen or frequently changing medication schedule
Adverse reactions (ADRs)
Confusion about brand name/trade name
Difficult-to-open containers
Rectal, vaginal, subcutaneous modes of administration
Lack of insight into illness
Limited patient understanding of medication’s purpose
Cognitive impairment/psych issues
Illiteracy, language/cultural issues
Misunderstanding verbal instructions
Lack of follow up

MEDICATION NON-ADHERENCE
Like polypharmacy itself, the strongest predictor of
medication non-adherence is the number of
medications.
Non-adherence rates are estimated at 25-50 percent of
older adults.
Non-adherence is intentional about 75% of the time.
33-69% of drug-related admissions result from non-
adherence (for all patients)
Patients discharged with 4 or more meds- over 50% error
rate
Changes in medication regimen made by patients to:
Increase convenience
Reduce adverse effects

SOLUTIONS TO POLYPHARMACY
Review medication
Anticipate Adverse Drug Events ( ADEs)
Avoid errors- prescribe carefully
Give verbal and written instructions
Simplify
Understand obstacles (cost, memory loss…)
Enlist family/nursing/PCP
Make sure there is good follow up

ALWAYS REMEMBER
“Prescribing cascade”- a drug added to treat
(mistakenly) the ADR of another drug.
Clinical Pearl- “Any symptom in an elderly person should
be evaluated as a potential ADR until proven otherwise”.
Many geriatric syndromes can occur as a consequence
of medications: delirium, falls and fractures,
incontinence.

ALWAYS REMEMBER
Polypharmacy is a reality of prescribing when patients
have multiple comorbidities.
We must all anticipate and guard against the potential
complications of polypharmacy.
Optimal prescribing is key!

















