18
Gestational Gestational Trophoblastic Trophoblastic Disease Disease Current management Current management
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | harvey-hawkins |
| View: | 235 times |
| Download: | 0 times |

Gestational Gestational Trophoblastic DiseaseTrophoblastic Disease
Current managementCurrent management

BackgroundBackgroundIncidence – Incidence – U.S. and Europe 1/1500U.S. and Europe 1/1500
South East Asia 1/150South East Asia 1/150 ((↓↓ Carotene, animal fat and Carotene, animal fat and Vit. A)Vit. A)
Can follow any gestational event – abortion, miscarriage, ectopic, normal Can follow any gestational event – abortion, miscarriage, ectopic, normal pregnancypregnancy
Curable in vast majority – chemotherapy 1956Curable in vast majority – chemotherapy 1956
Complete & partial moleComplete & partial moleInvasive moleInvasive molePlacental-site trophoblastic tumourPlacental-site trophoblastic tumourChoriocarcinoma ( always if follows term pregnancy 1/50,000 )Choriocarcinoma ( always if follows term pregnancy 1/50,000 )
Latter 3 Latter 3 usuallyusually derive from molar pregnancy derive from molar pregnancy

Complete MoleComplete MolePathology:Pathology: Generalized hydatidiform swelling and trophoblastic hyperplasiaGeneralized hydatidiform swelling and trophoblastic hyperplasia
fetal/embryonic tissue absentfetal/embryonic tissue absent
Karyotype:Karyotype: 90% 46XX haploid sperm fertilizes ovum and duplicates90% 46XX haploid sperm fertilizes ovum and duplicatesovum nucleus either absent or inactivatedovum nucleus either absent or inactivated
10% 46XY10% 46XY
Clinical:Clinical: Vaginal bleedingVaginal bleeding 95% 95% (prune juice, anaemia)(prune juice, anaemia)Enlarged uterusEnlarged uterus 50%50%Theca lutein cystsTheca lutein cysts 50% 50% (often >6cm.- may take 3 months)(often >6cm.- may take 3 months)HyperemesisHyperemesis 25%25%PETPET 25%25% (no reported case of eclampsia)(no reported case of eclampsia)HyperthyroidismHyperthyroidism 5% 5% (if free T4(if free T4↑ - B-blockade)↑ - B-blockade)Trophoblastic emboli 2%Trophoblastic emboli 2%
Diagnosis:Diagnosis: U/S usually very sensitive – generalized swelling (snow-storm )U/S usually very sensitive – generalized swelling (snow-storm )


Complete MoleComplete Mole

Complete Mole HistologyComplete Mole Histology

Partial MolePartial MoleTriploid karyotype – extra haploid set paternalTriploid karyotype – extra haploid set paternalSometimes fetus present – usually triploid Sometimes fetus present – usually triploid growth restricted / multiple anomaliesgrowth restricted / multiple anomalies
Pathology differs from complete:Pathology differs from complete: focal hydatidiform swellingfocal hydatidiform swellingvarying size of chorionic villivarying size of chorionic villimarked villous scallopingmarked villous scallopingfocal trophoblastic hyperplasiafocal trophoblastic hyperplasiaidentifiable embryonic or fetal tissuesidentifiable embryonic or fetal tissues
Clinical:Clinical: Usually as a regular incomplete or missed abortionUsually as a regular incomplete or missed abortionExcessive uterine enlargement / PET very rareExcessive uterine enlargement / PET very rareNo hyperemesis / hyperthyroidism / theca-lutein cystsNo hyperemesis / hyperthyroidism / theca-lutein cysts
Diagnosis: Diagnosis: U/S may detect focal cystic spaces of varying diameterU/S may detect focal cystic spaces of varying diameterDiagnosis on histology of curettingsDiagnosis on histology of curettings
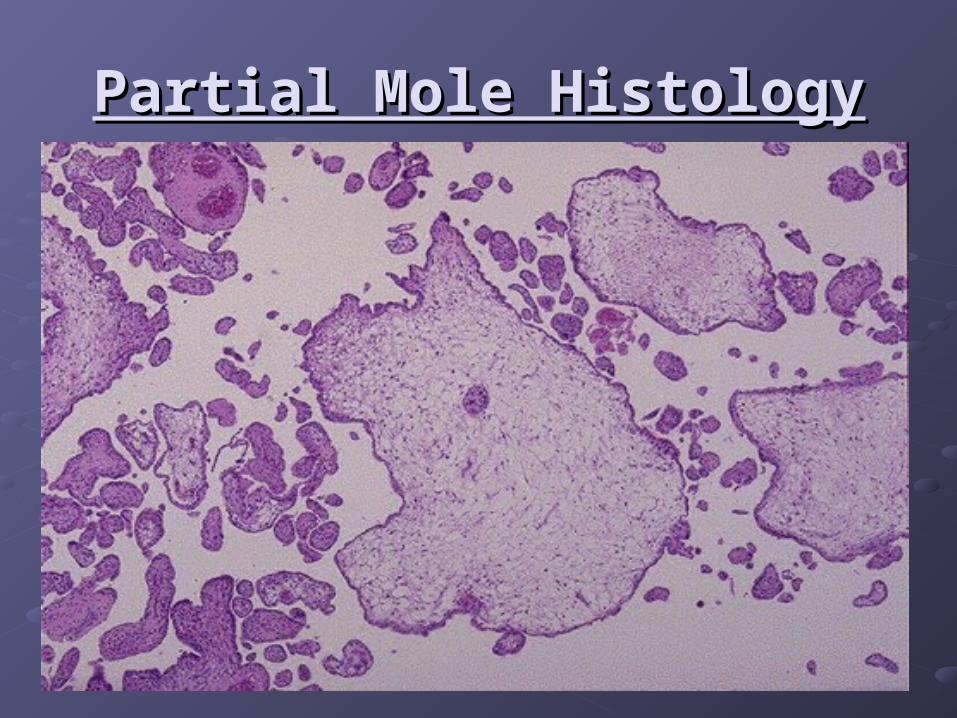
Partial Mole HistologyPartial Mole Histology
ManagementManagementPre-operative assessment – medical complications / CXRPre-operative assessment – medical complications / CXR
Evacuation -Evacuation - oxytocin infusion after curettageoxytocin infusion after curettageheavy bleeding should not deter from cervical dilatationheavy bleeding should not deter from cervical dilatationsuction curettage (fundal massage)suction curettage (fundal massage)uterus usually dramatically reduces in size / bleeding controlleduterus usually dramatically reduces in size / bleeding controlledcomplete with sharp curettagecomplete with sharp curettageHistological evaluation of all tissueHistological evaluation of all tissue
Natural history:Natural history: Complete - 15% local uterine invasionComplete - 15% local uterine invasion 4% metastatic disease4% metastatic disease
High risk - hCG > 100000High risk - hCG > 100000(40%)(40%) large uterus large uterus 30% local invasion30% local invasion
theca lutein cysts > 6cm. theca lutein cysts > 6cm. 9% metastases9% metastases
Partial mole - Partial mole - 4% local uterine persistence/no cases choriocarcinoma4% local uterine persistence/no cases choriocarcinomaMany centres have abandoned follow-upMany centres have abandoned follow-up

Follow upFollow upWeekly Weekly -hCG (syncytiotrophoblast) -hCG (syncytiotrophoblast) levelslevels until untilnormal for 3 consecutive weeksnormal for 3 consecutive weeksCan take 12-14 weeksCan take 12-14 weeks
Then monthly until normalThen monthly until normalfor 6 monthsfor 6 months
Contraception:Contraception: ImmediateImmediate
Oral / barrier / permanentOral / barrier / permanent
No IUCD until hCG normal (perforation)No IUCD until hCG normal (perforation)
No No persistent disease on OCP and persistent disease on OCP and regression time not influencedregression time not influenced

GTN Follow-upGTN Follow-up

WHO Prognostic ScoringWHO Prognostic Scoring
Original assessment and scoring system 1984 changed in 2000Original assessment and scoring system 1984 changed in 2000
Metastatic disease occurs in 4% patients with molar pregnancyMetastatic disease occurs in 4% patients with molar pregnancy
Plateau:Plateau: 4 values over 3 weeks4 values over 3 weeks
Rise:Rise: 10% for 3 values over 2 weeks 10% for 3 values over 2 weeks
Clinical examination – especially pelvis, vagina and vulvaClinical examination – especially pelvis, vagina and vulva
U/S to exclude pregnancyU/S to exclude pregnancy
Brain – MRI superior to CT scanBrain – MRI superior to CT scan
Chest – CXR adequate for counting metastases / CT scan also acceptableChest – CXR adequate for counting metastases / CT scan also acceptable
Abdomen – CT scanAbdomen – CT scan
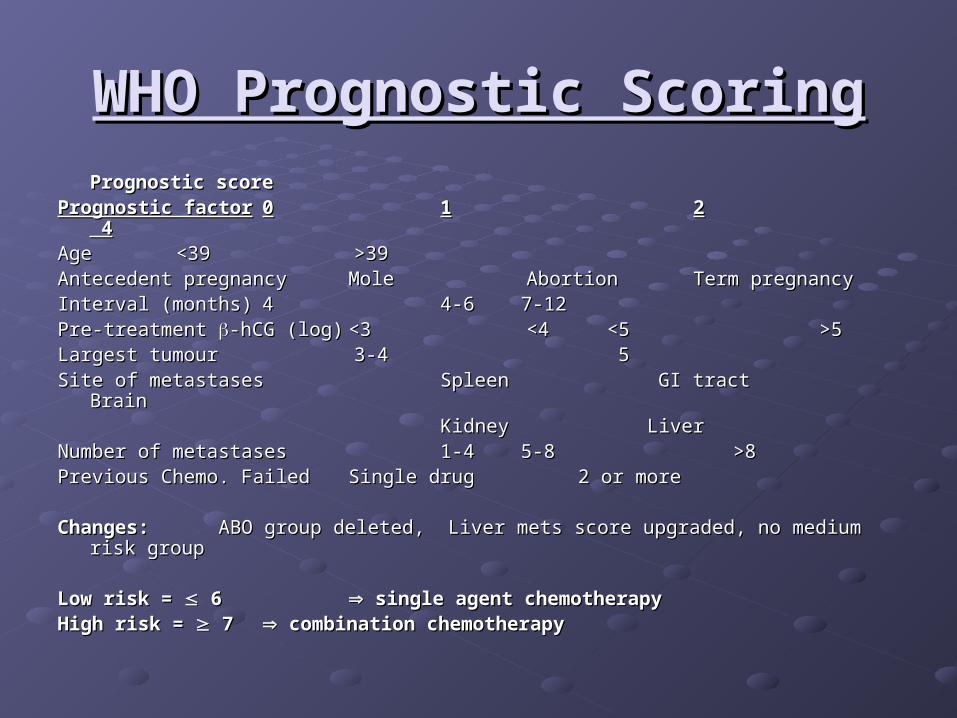
WHO Prognostic ScoringWHO Prognostic ScoringPrognostic scorePrognostic score
Prognostic factorPrognostic factor 00 11 22 4 4AgeAge <39<39 >39 >39Antecedent pregnancyAntecedent pregnancy MoleMole Abortion Abortion Term pregnancyTerm pregnancyInterval (months)Interval (months) 44 4-6 4-6 7-127-12Pre-treatment Pre-treatment -hCG (log)-hCG (log) <3<3 <4 <4 <5<5 >5 >5Largest tumourLargest tumour 3-4 3-4 5 5Site of metastasesSite of metastases Spleen GI tract Spleen GI tract Brain Brain
KidneyKidney Liver LiverNumber of metastasesNumber of metastases 1-4 1-4 5-85-8 >8 >8Previous Chemo. FailedPrevious Chemo. Failed Single drug 2 or moreSingle drug 2 or more
Changes: Changes: ABO group deleted, Liver mets score upgraded, no medium risk groupABO group deleted, Liver mets score upgraded, no medium risk group
Low risk = Low risk = 6 6 single agent chemotherapy single agent chemotherapyHigh risk = High risk = 7 7 combination chemotherapy combination chemotherapy
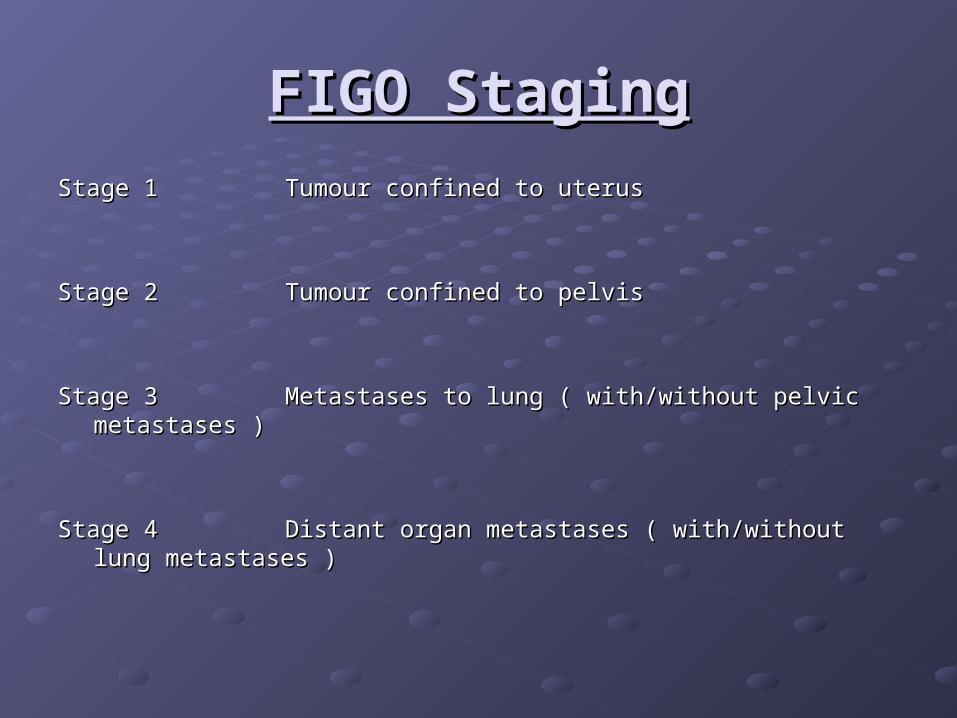
FIGO StagingFIGO Staging
Stage 1Stage 1 Tumour confined to uterusTumour confined to uterus
Stage 2Stage 2 Tumour confined to pelvisTumour confined to pelvis
Stage 3Stage 3 Metastases to lung ( with/without pelvic metastases )Metastases to lung ( with/without pelvic metastases )
Stage 4Stage 4 Distant organ metastases ( with/without lung metastases )Distant organ metastases ( with/without lung metastases )
ChemotherapyChemotherapyLow-riskLow-risk If non-metastatic - always curable ( Hysterectomy if chemo fails) If non-metastatic - always curable ( Hysterectomy if chemo fails)
Methotrexate:Methotrexate:Many regimesMany regimesI.M. Methotrexate 1mg/Kg days 1,3,5,7I.M. Methotrexate 1mg/Kg days 1,3,5,7I.M./ P.O. Folinic acid 0.1mg/Kg days 2,4,6,8I.M./ P.O. Folinic acid 0.1mg/Kg days 2,4,6,8
I.M. Methotrexate 40mg/mI.M. Methotrexate 40mg/m²² weekly weekly
Actinomycin D:Actinomycin D: I.V. push 1.25mg/mI.V. push 1.25mg/m² every 14 days² every 14 days
Follow-up:Follow-up: -hCG, FBC, LFTs and U/Es, creatinine prior to each cycle-hCG, FBC, LFTs and U/Es, creatinine prior to each cycleContinue treatment cycle for 1-3 weeks after normal Continue treatment cycle for 1-3 weeks after normal -hCG-hCGCheck Check -hCG monthly for 12 months, then 2 monthly for 12 months-hCG monthly for 12 months, then 2 monthly for 12 monthsContraception for 12 monthsContraception for 12 months
Complete remission in 85-90% Complete remission in 85-90% 80% require only one course80% require only one course
Toxicity:Toxicity: Thrombocytopenia 2%, neutropenia 6% and hepatotoxicity 14%Thrombocytopenia 2%, neutropenia 6% and hepatotoxicity 14%

High Risk GTNHigh Risk GTNInvasive mole:Invasive mole: invades myometrium / diagnosed at hysterectomy / can metastasizeinvades myometrium / diagnosed at hysterectomy / can metastasize
mets may be choriocarcinomamets may be choriocarcinoma
Placental site trophoblastic tumour: Placental site trophoblastic tumour: Locally invasive composed of cytotrophopblastLocally invasive composed of cytotrophopblast small if any rise in hCG (<3000)small if any rise in hCG (<3000)
vaginal bleeding usually after amenorrhoeavaginal bleeding usually after amenorrhoea Large polypoid tumour / insensitive to Large polypoid tumour / insensitive to
chemotherapychemotherapy Curettage sometimes successful / Curettage sometimes successful / HysterectomyHysterectomy
Choriocarcinoma:Choriocarcinoma: Accounts for majority of metastatic diseaseAccounts for majority of metastatic diseaseEarly vascular invasion and widespread disseminationEarly vascular invasion and widespread disseminationFragile vessels Fragile vessels haemorrhagic complications haemorrhagic complications80% have lung mets – any respiratory symptom80% have lung mets – any respiratory symptom30% have vaginal mets – highly vascular (avoid biopsy)30% have vaginal mets – highly vascular (avoid biopsy)10% have liver mets – usually only with extensive tumour elsewhere10% have liver mets – usually only with extensive tumour elsewhere10% have brain mets – never isolated ( lung / vagina)10% have brain mets – never isolated ( lung / vagina)
Treatment:Treatment: EMA-CO chemotherapy +/- surgical resection / radiotherapyEMA-CO chemotherapy +/- surgical resection / radiotherapyPrognosis:Prognosis: 75% complete response rate75% complete response rate Salvage chemo – BEP varying successSalvage chemo – BEP varying success
Pregnancy After GTNPregnancy After GTN
No evidence of increased congenital anomalies after one year contraceptionNo evidence of increased congenital anomalies after one year contraception
Recent Japanese data – Recent Japanese data – Women who concieved during follow-up period < 1 Women who concieved during follow-up period < 1 yearyear
No adverse effect on anomalies nor preterm No adverse effect on anomalies nor preterm deliverydelivery
Risk of further molar pregnancy:Risk of further molar pregnancy: 0.5-2.5% if one previous molar0.5-2.5% if one previous molar
33% if two previous molar33% if two previous molar
3 molar pregnancies – poor live birth rate3 molar pregnancies – poor live birth rate
Risk of molar pregnancy increases with number of previous spontaneous abortionsRisk of molar pregnancy increases with number of previous spontaneous abortions
Previous term pregnancies reduce risk of GTN Previous term pregnancies reduce risk of GTN

ConclusionsConclusions
GTN is rareGTN is rare
Ultrasound diagnosis becoming more commonUltrasound diagnosis becoming more common
Senior staff should perform ERPC ( suction and sharp curettage)Senior staff should perform ERPC ( suction and sharp curettage)
Follow-up – clinical and serum Follow-up – clinical and serum -hCG measurements in specialized clinics-hCG measurements in specialized clinics
Chemotherapy curative in vast majority low risk patientsChemotherapy curative in vast majority low risk patients

















