29
الرحمن بسم ا الرحمن بسم ا الرحيم الرحيم
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | mohamed-zaki |
| View: | 50 times |
| Download: | 1 times |

الرحمن ا الرحمن بسم ا بسمالرحيمالرحيم
Pediatric Refraction Pediatric Refraction
when to prescribe ?when to prescribe ?
· Mohamed Zaki (M.Sc) · Tanta University
· Child eye is not a small adult eye
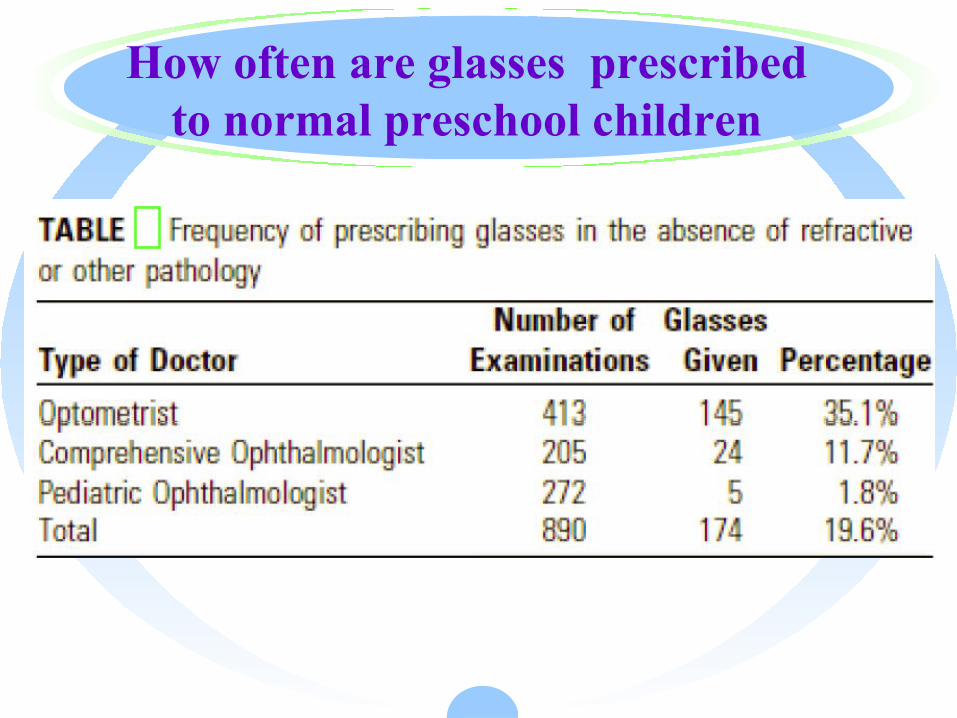
How often are glasses prescribed to normal preschool children
1. Interfere with normal emmetropisation
2. Expense of spectacles3. Inconvenience to parents 4. Lack of perceived benefit to child
5- Prismatic effect and ↓ field of vision
What is peculiar to children eyes?
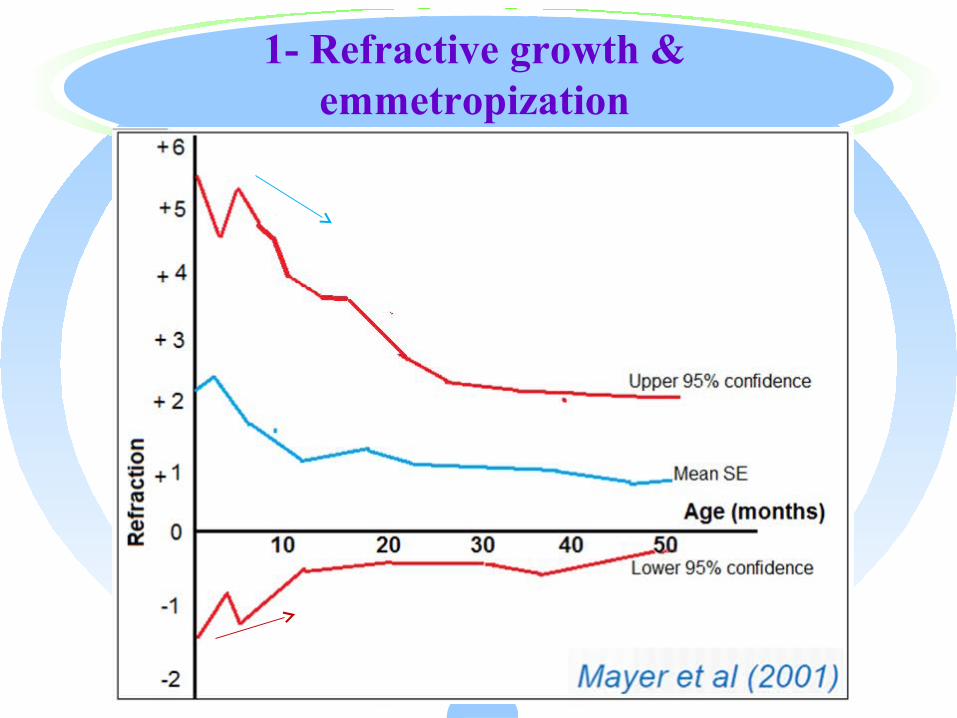
1- Refractive growth & emmetropization
Emmetropisation is both an active and a passive process i.e. error stimulate the
eye to correct it
requires normal visual experience
Atkinson et al (2007)
2-Risk of Amblyopia
Emmetropisation fails when refractive errors are outside normal range for age and the risk of amblyopia and
strabismus is increased
Glasses reduce the risk
· Atkinson et al (2007)
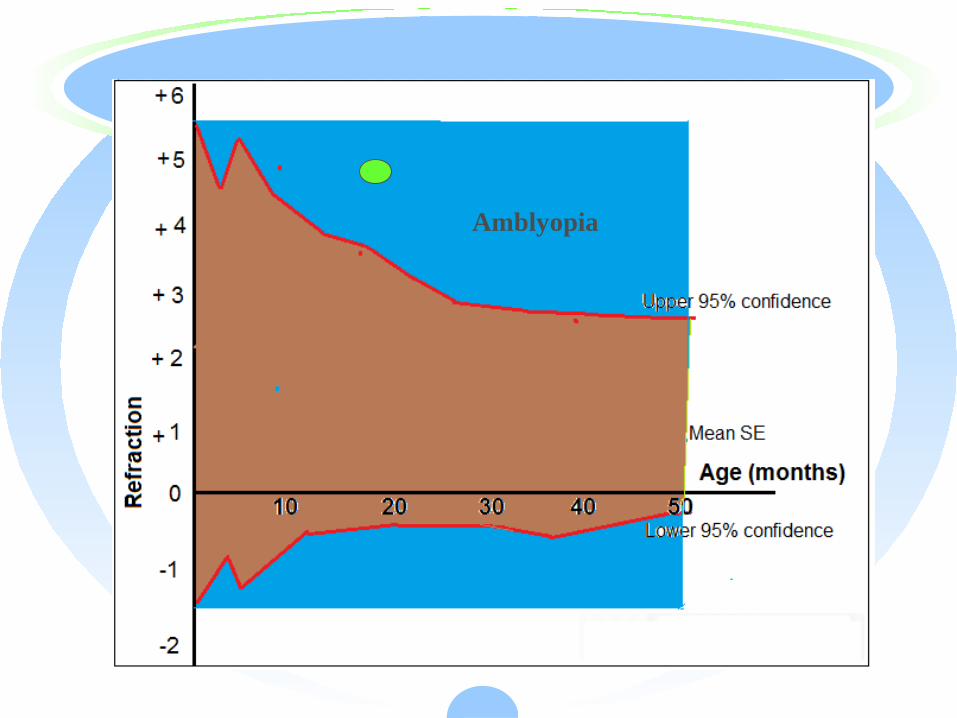
Amblyopia
3- Power of accommodation
· The mean accommodative amplitude is
14 diopters for 8 years old child.
Southall, 1937
General RulesSmall errors usually don’t need correction
(stimulus of emmetropization)Large errors shouldn’t be fully corrected
(but converted to small errors)No emmetropization after 3 years.
(i.e. do full correction)Hypermetropia shouldn’t be fully corrected
(except …)
If you prescribe .. follow up refraction after 3 months.
Cycloplegic refraction is routine.
A child with VA ( 6/6 ) and dry autorefraction (+0.00) may need glasses.
0.5% to 1.0% Cyclopentolate1 drop tid x 3 days
When to prescribe ?
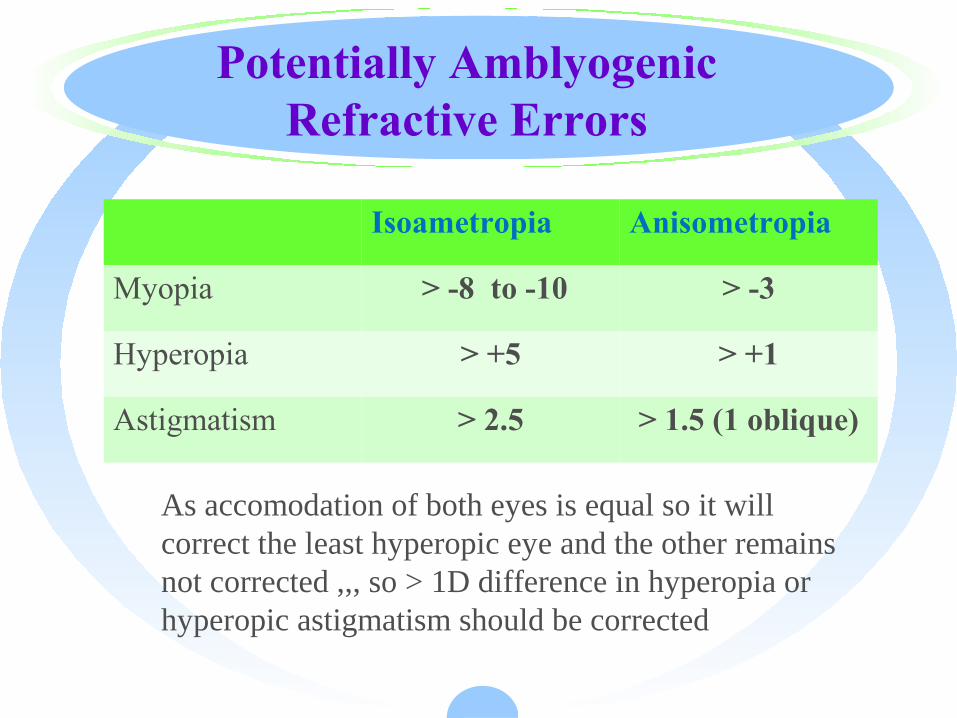
Potentially Amblyogenic Refractive Errors
Isoametropia Anisometropia
Myopia > -8 to -10 > -3
Hyperopia > +5 > +1
Astigmatism > 2.5 > 1.5 (1 oblique)
As accomodation of both eyes is equal so it will correct the least hyperopic eye and the other remains not corrected ,,, so > 1D difference in hyperopia or hyperopic astigmatism should be corrected
Normal
· Myopia , Astig, Aniso < 0.75D
· Hyperopia < 2 D

Many guidelines …
Glasses prescription in children is a decision not just refraction
· Age ,
· History : child and family.
· Examination : ocular alignment , binocular vision.
History· School performance· Medical history (e.g., CP or Down syndrome)· Family history (hyperopia, aniso, strab, ambly)· Previous SRx & compliance
Symptoms/Signs· Tearing / redness Asthenopia
Blinking· Blurred vision Difficulty with reading/near
work
Myopia
< 3 years old:
partial correction of large error (>-3 to -4 D )
(subtract 1-2D)
>3-4 years old : full correction
Functional concern :
Vision / presence of XT
Astigmatism
< 3 years old:
partial correction of large error (>2)
(subtract 1-2 D or 50%)
>3-4 years : Full correction
Oblique axis (>1D) and Stable with repeated measures
Hyperopia why to treat ?
correcting hyperopia improves cognitive and visuo-perceptual abilities
(Rosner & Rosner 1987, Williams et al 2005,)
Atkinson prospective study
• Treated vs. untreated hyperopes
• If hyperopia > + 3.50
– 13x risk of strabismus or amblyopia
– Treatment decreases to 4 X
Hyperopia
< 3 years old: partial correction of large error (>+3.5 – 4.5 D)
(Subtract 1-2 D)
3-4 years : partial correction of large error (>+2.5)
School children : Vision / Any child with any hyperopia have learning or
other difficulties
Functional concern :/ presence of ET/ family history of squint / / children with
special needs /
Anisometropia
· > 1.00 D with hyperopia
· ≥2.00D of with myopia
·
Aphakia or Pseudophakia
· Overcorrect by 2 to 3.00D because child’s world is near.
· After 2 to 3 years, distance correction with bifocal is better option
· Aphakia correction not > +13
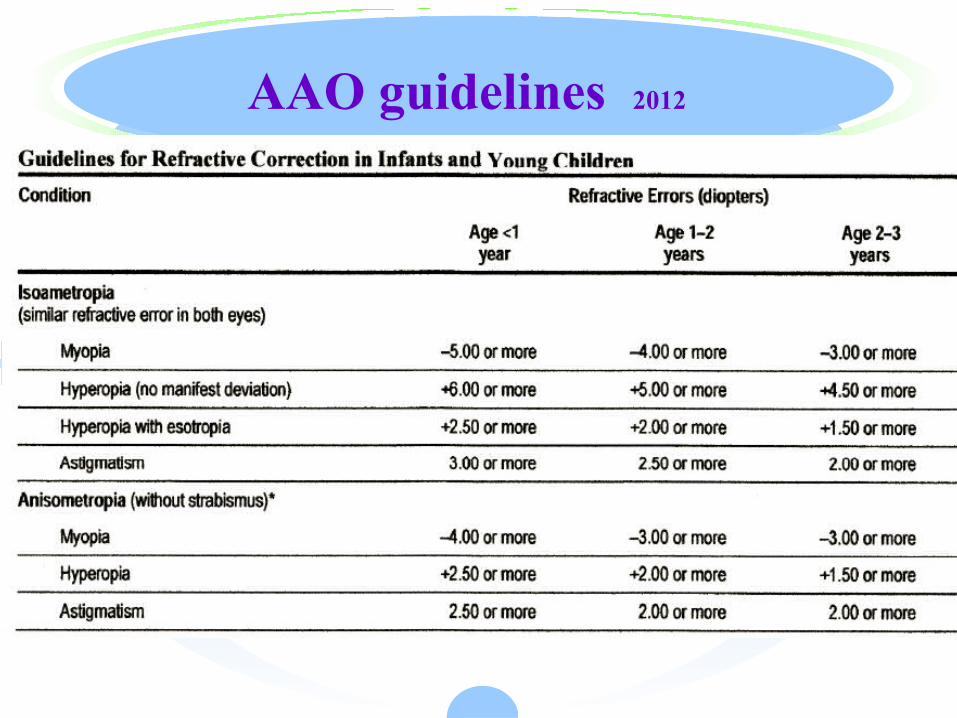
AAO guidelines 2012
LASIK in children
· at least 4 D difference between the two eyes, but most of the time it is at least 6 D in the patients I treat. The second group includes patients with neurobehavioral disorders with severe anisometropia who just won't wear glasses despite the need,
· craniofacial abnormalities that make spectacle or contact lens wear impractical (e.g., Goldenhar's with microtia and/or limbal dermoids) and those with severe neck weakness (e.g., some children with cerebral palsy) whose spectacles fall down their nose.
· LASEK or PRK e MMC is best use , not LASIK
· Age < 7 ys
· Intolerant to glasses and CL Poor compliance can be defined as wearing glasses for 25% or less of waking time (only one out of every four waking hours, a permissive
· boundary)
· The prevalence of any amblyopia (defined as two or more optotype lines difference between the eyes) in preschool children who have greater than 1 D of anisometropia is 66%.

















