Global Fund Strategy for increased domestic financing Satellite Session: Where is the Money?? Challenges & opportunities in mobilizing Increased Domestic Financing Melbourne, 23 July 2014 Dr Christoph Benn Director, External Relations Division Global Fund
Transcript
Global Fund Strategy for increased domestic financing
Satellite Session: Where is the Money?? Challenges & opportunities in mobilizing Increased Domestic Financing
Melbourne, 23 July 2014
Dr Christoph Benn
Director, External Relations Division
Global Fund
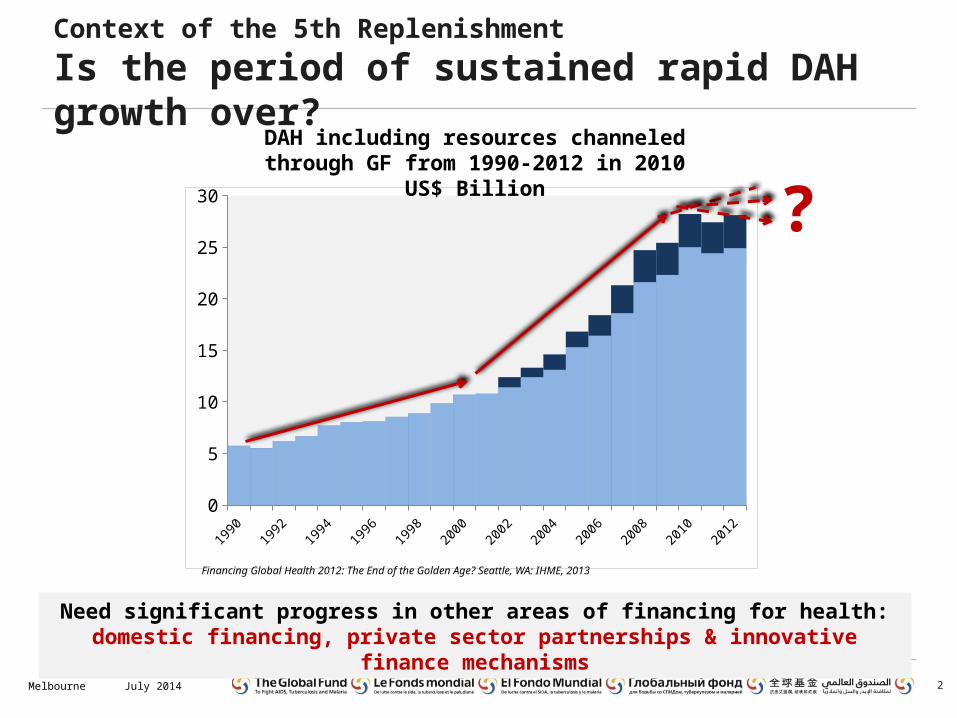
Context of the 5th Replenishment
Is the period of sustained rapid DAH growth over?
2
0
5
10
15
20
25
30
DAH including resources channeled through GF from 1990-2012 in 2010 US$ Billion
Financing Global Health 2012: The End of the Golden Age? Seattle, WA: IHME, 2013
July 2014Melbourne
?
Need significant progress in other areas of financing for health: domestic financing, private sector partnerships & innovative finance mechanisms
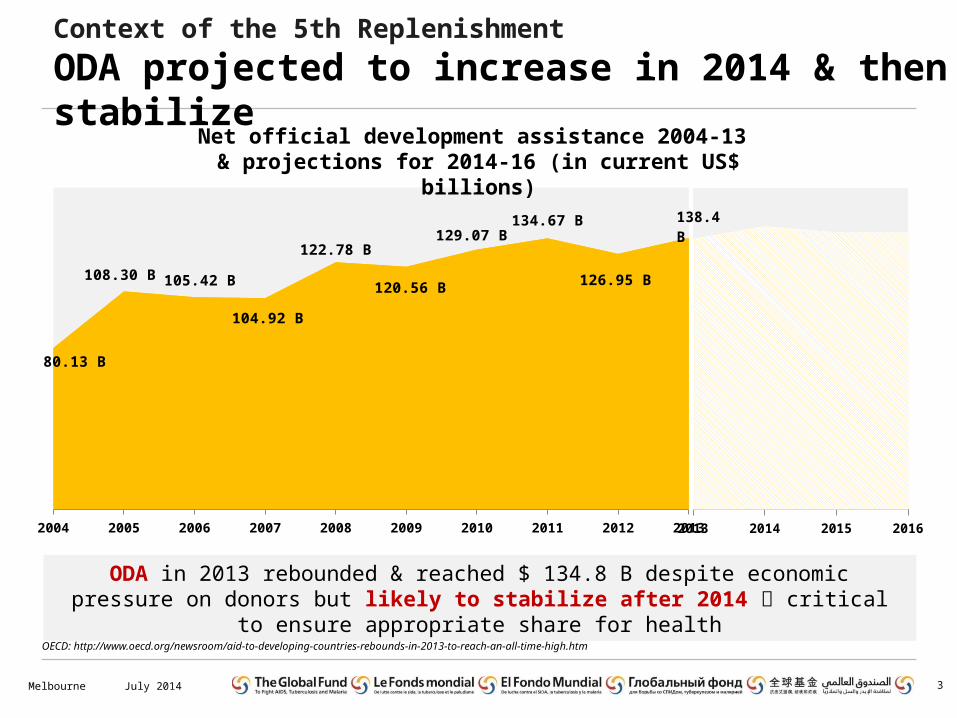
Context of the 5th Replenishment
ODA projected to increase in 2014 & then stabilize
3July 2014Melbourne
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
80.13 B
108.30 B 105.42 B
104.92 B
122.78 B
120.56 B
129.07 B134.67 B
126.95 B
2013 2014 2015 2016
138.4 B
Net official development assistance 2004-13 & projections for 2014-16 (in current US$ billions)
ODA in 2013 rebounded & reached $ 134.8 B despite economic pressure on donors but likely to stabilize after 2014 critical to ensure appropriate share for health
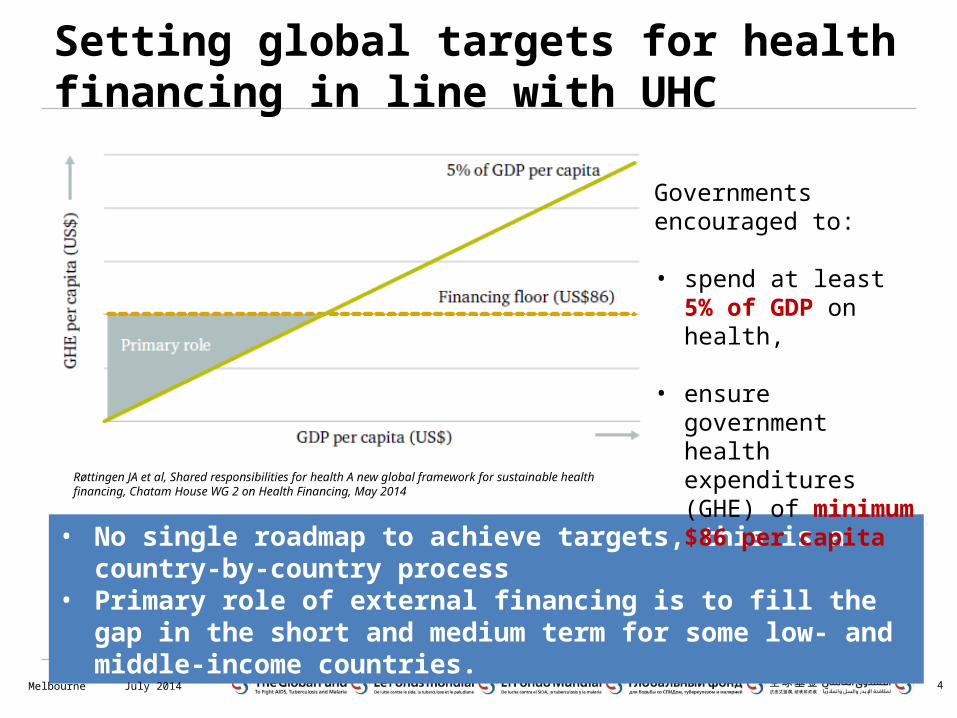
Setting global targets for health financing in line with UHC
4
• No single roadmap to achieve targets, this is a country-by-country process
• Primary role of external financing is to fill the gap in the short and medium term for some low- and middle-income countries.
Governments encouraged to:
• spend at least 5% of GDP on health,
• ensure government health expenditures (GHE) of minimum $86 per capita
Røttingen JA et al, Shared responsibilities for health A new global framework for sustainable health financing, Chatam House WG 2 on Health Financing, May 2014
July 2014Melbourne
Key challenges & opportunities
• Value for Money: As the resource landscape is changing, focus is now more on improving health program efficiency and effectiveness which calls for both “more money for health and more health for money”
• Domestic Advocacy: a large part of any increase in public funding for health will need to come from governments, therefore need to develop a convincing business and advocacy case for increased / sustainable public commitment to programs
• Sustainability: Domestic public spending should continue as economic growth continues, however it will not be sufficient to address all the health needs. Therefore, still a need for external resources in the short to medium term as well as to explore PS partnerships & other innovative mechanisms.
5July 2014Melbourne
GF domestic financing strategy
6July 2014Melbourne 6
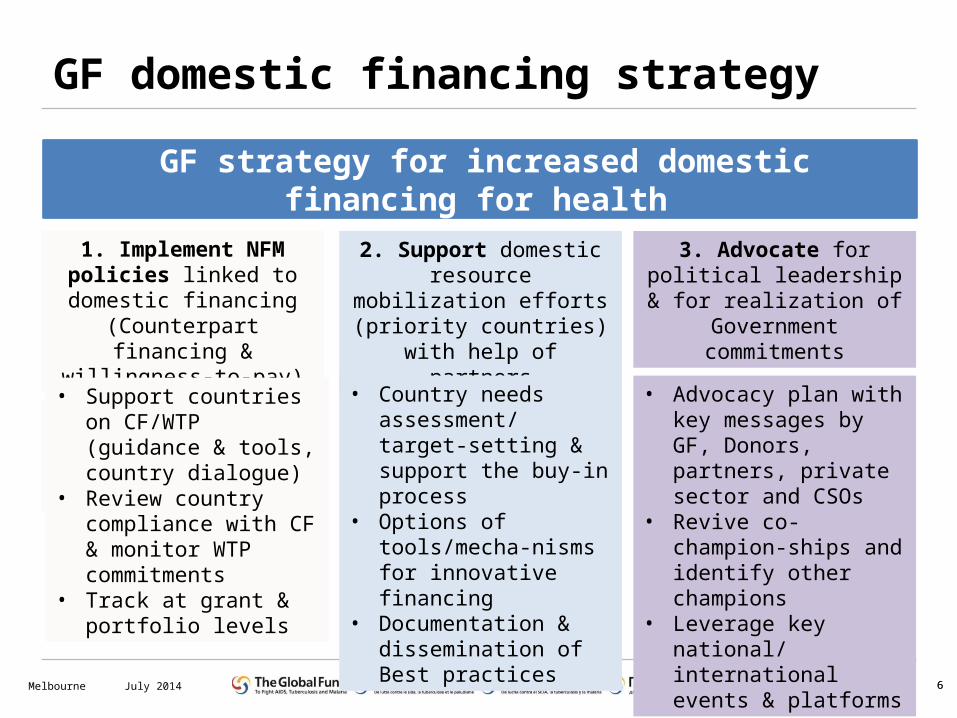
GF strategy for increased domestic financing for health
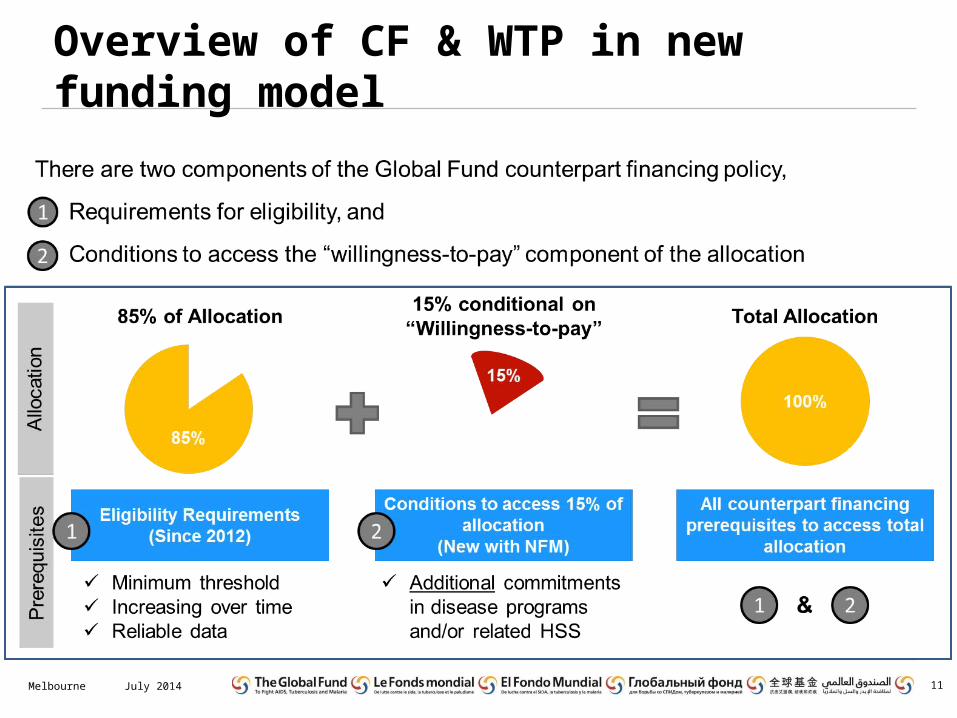
• Increasing government contribution to disease programs and health sector
• Reliable disease and health expenditure data
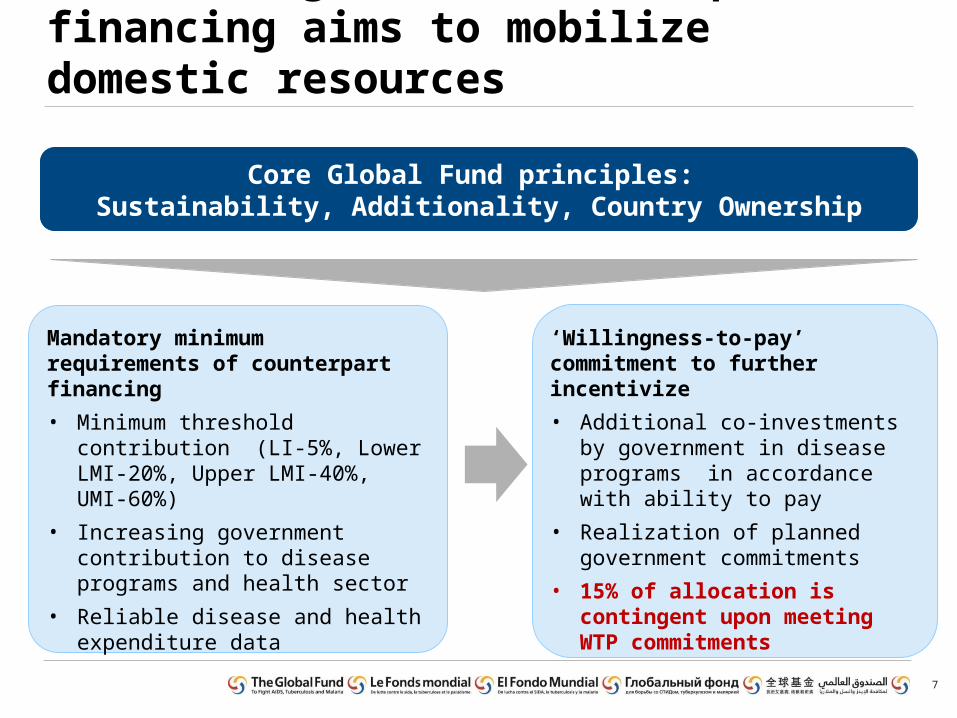
‘Willingness-to-pay’ commitment to further incentivize
• Additional co-investments by government in disease programs in accordance with ability to pay
• Realization of planned government commitments
• 15% of allocation is contingent upon meeting WTP commitments
Core Global Fund principles: Sustainability, Additionality, Country Ownership
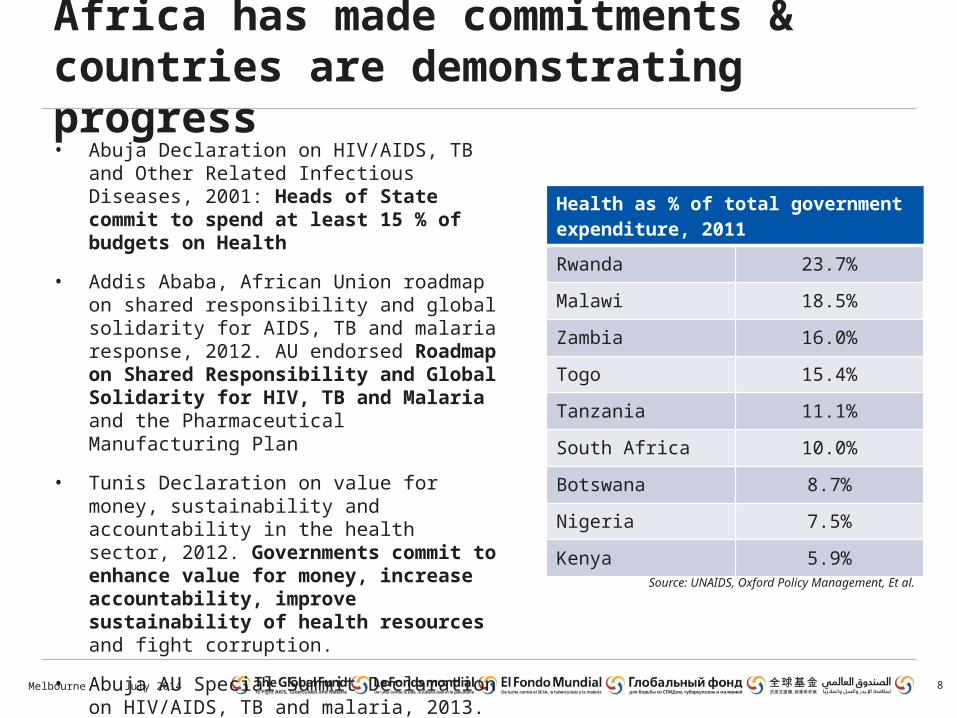
Africa has made commitments & countries are demonstrating progress• Abuja Declaration on HIV/AIDS, TB and Other
Related Infectious Diseases, 2001: Heads of State commit to spend at least 15 % of budgets on Health
• Addis Ababa, African Union roadmap on shared responsibility and global solidarity for AIDS, TB and malaria response, 2012. AU endorsed Roadmap on Shared Responsibility and Global Solidarity for HIV, TB and Malaria and the Pharmaceutical Manufacturing Plan
• Tunis Declaration on value for money, sustainability and accountability in the health sector, 2012. Governments commit to enhance value for money, increase accountability, improve sustainability of health resources and fight corruption.
• Abuja AU Special Summit Declaration on HIV/AIDS, TB and malaria, 2013. Calls for countries to honor the 2001 Abuja Declaration and other health commitments.
8
Health as % of total government expenditure, 2011
Rwanda 23.7%
Malawi 18.5%
Zambia 16.0%
Togo 15.4%
Tanzania 11.1%
South Africa 10.0%
Botswana 8.7%
Nigeria 7.5%
Kenya 5.9%
Source: UNAIDS, Oxford Policy Management, Et al.
July 2014Melbourne
In sum, the Global Fund is working with countries and partners to:
• Leverage GF resources to encourage increased Government commitment to disease programs & related health systems strengthening
• Improve data quality and accessibility for both domestic and international health funding
• Identify and address rigid budgeting practices, allocative inefficiencies that are obstacles to the reallocation of revenues towards health
• Nurture political leadership --► ongoing work on multi-dimensional advocacy and messaging to ensure health is given top priority at national and international levels
9July 2014Melbourne
Conclusions
• Health expenditures should keep pace with economic growth
• There is no single blueprint for increasing domestic funding for health
• Lessons learned and best practices should
THANK YOU10July 2014Melbourne
Overview of CF & WTP in new funding model
11July 2014Melbourne
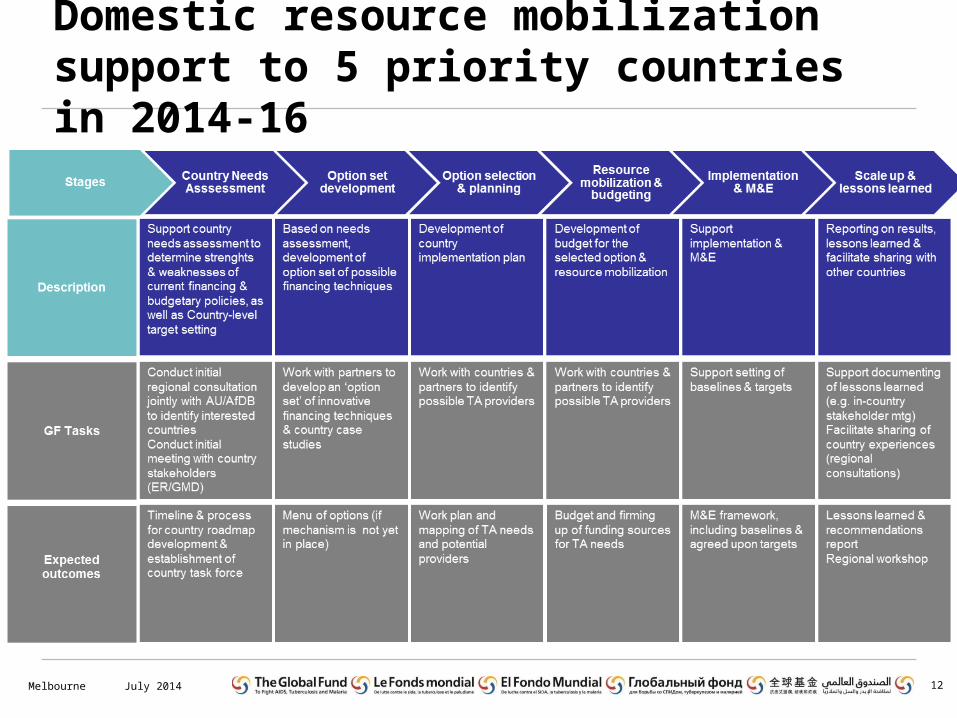
Domestic resource mobilization support to 5 priority countries in 2014-16
12July 2014Melbourne
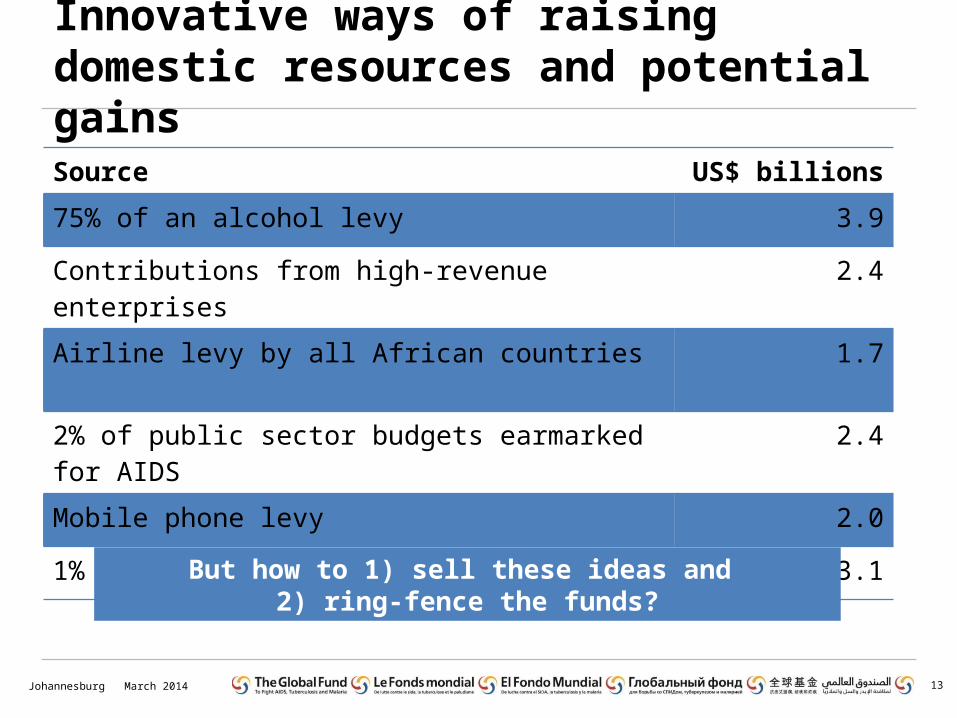
Innovative ways of raising domestic resources and potential gains
March 2014Johannesburg 13
Source US$ billions
75% of an alcohol levy 3.9
Contributions from high-revenue enterprises 2.4
Airline levy by all African countries 1.7
2% of public sector budgets earmarked for AIDS 2.4
Mobile phone levy 2.0
1% income tax levy earmarked for AIDS 3.1
But how to 1) sell these ideas and 2) ring-fence the funds?