27
Harvard University Initiative for Global Health Global Health Challenges Social Analysis 76: Lecture 20
| Date post: | 02-Jan-2016 |
| Category: |
Documents |
| Upload: | zerlina-mcgowan |
| View: | 23 times |
| Download: | 1 times |

Harvard University Initiative for Global Health
Global Health ChallengesSocial Analysis 76: Lecture 20

Harvard University Initiative for Global Health
Attributable Disease Burden of 20 Risk Factors
0.0% 1.0% 2.0% 3.0% 4.0% 5.0% 6.0% 7.0% 8.0% 9.0% 10.0%
Underw eight
Unsafe sex
High blood pressure
Tobacco
Alcohol
Unsafe w ater, sanitation, and hygiene
High cholesterol
Indoor smoke from solid fuels
Iron deficiency
High BMI
Zinc deficiency
Low fruit and vegetable intake
Vitamin A deficiency
Physical inactivity
Occupational risk factors for injury
Lead exposure
Illicit drugs
Unsafe health care injections
Lack of contraception
Childhood sexual abuse
Attributable DALY (% of global DALY - Total 1.46 billion)
High-mortality developing
Lower-mortality developing
Developed

Harvard University Initiative for Global Health
Iron Deficiency Anaemia
Vitamin A Deficiency
Zinc Deficiency
Review of Diseases, Injuries and Risk Factors

Harvard University Initiative for Global Health
Odds Ratio Estimate.3 .5 .75 1 1.1
Combined
UK86
PNG99
Nigeria85
Nigeria82
Nigeria75
Nepal98
Malaysia65
Kenya63
India95
China96
Summary OR: 0.72
Perinatal mortality: OR’s for each 1 g/dL Hb increase
From Stoltzfus et al, 2005

Harvard University Initiative for Global Health
Harvard University Initiative for Global Health
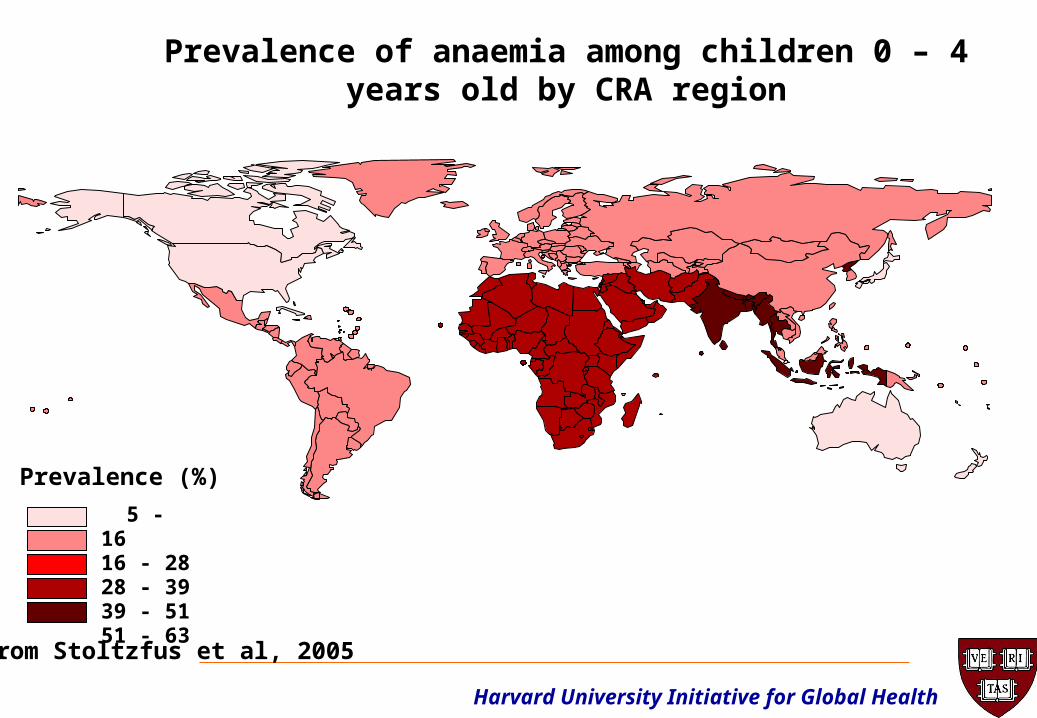
Prevalence of anaemia among children 0 – 4 years old by CRA region
5 - 1616 - 2828 - 3939 - 5151 - 63
Prevalence (%)
From Stoltzfus et al, 2005

Harvard University Initiative for Global Health
Global DALYs From Iron Deficiency
56%
10%
34% Perinatal Causes
Maternal Causes
Iron DeficiencyAnemia

Harvard University Initiative for Global Health
DALYs from Perinatal Conditions, Maternal Conditions and Iron Deficiency Anaemia, Attributable to Iron
Deficiency, by Subregion (000s)
AFR-D
AFR-E
AMR-B
EUR-A
SEAR-D
WPR-A
WPR-B
EMR-D
EUR-BEUR-C
SEAR-B
EMR-BAMR-D
AMR-A

Harvard University Initiative for Global Health
Effect of Iron/Folic Acid (IFA) Supplementation on Adverse Events in
Children 1-48 Months Old
• Nepal (19,299 child-years IFA, 9,799 placebo) – no effect on deaths1
• Zanzibar (16,950 child-years IFA, 8,574 placebo) – 12% increase in all hospitalizations/deaths, 16% in malaria, 33% in pneumonia2
1Tielsch et al, submitted2Sazawal et al, submitted
Harvard University Initiative for Global Health
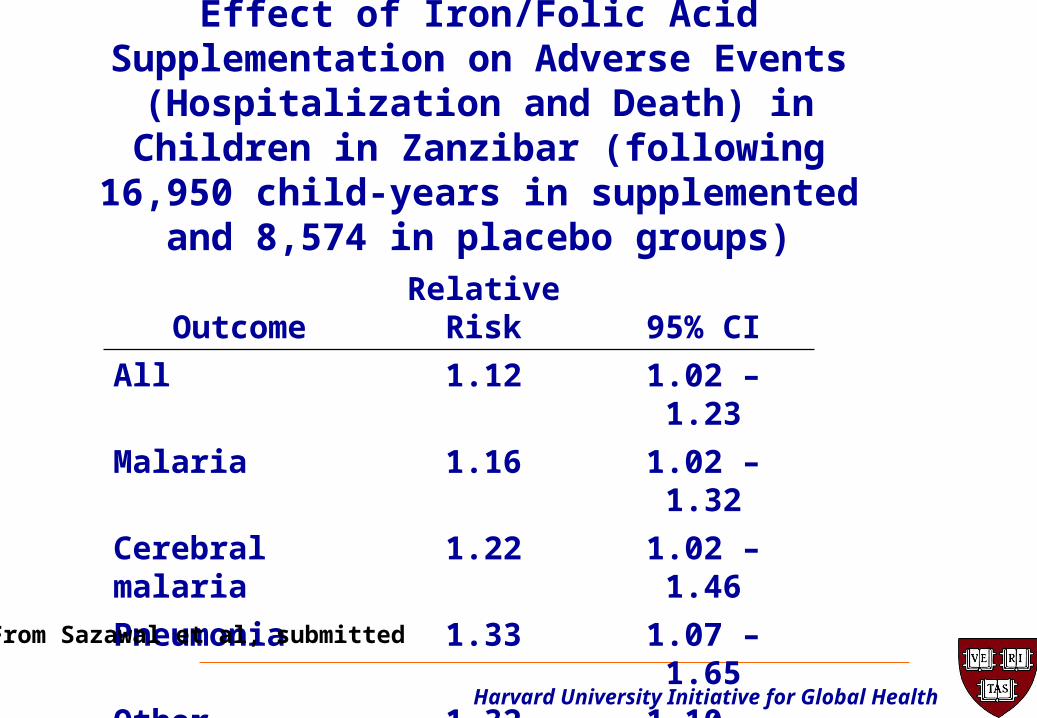
Effect of Iron/Folic Acid Supplementation on Adverse Events (Hospitalization and Death)
in Children in Zanzibar (following 16,950 child-years in supplemented and 8,574 in
placebo groups)
OutcomeRelative
Risk 95% CI
All 1.12 1.02 – 1.23
Malaria 1.16 1.02 – 1.32
Cerebral malaria 1.22 1.02 – 1.46
Pneumonia 1.33 1.07 – 1.65
Other infections 1.32 1.10 – 1.59
From Sazawal et al, submitted

Harvard University Initiative for Global Health
Iron Deficiency Anaemia
Vitamin A Deficiency
Zinc Deficiency
Review of Diseases, Injuries and Risk Factors

Harvard University Initiative for Global Health
Effects of Vitamin A on Infectious Disease Morbidity
• Possible effect on diarrhea severity, but not all morbidity
• No effect on pneumonia morbidity
• Effect on measles complications

Harvard University Initiative for Global Health
Prevalence of vitamin A deficiency among children 0-4 years old by CRA regions
From West et al., 2002
0 - 1010 - 1919 - 2929 - 3838 - 48
Prevalence (%)

Harvard University Initiative for Global Health
Major Trials of Vitamin A to Prevent Mortality
Over 165,000 children participated in these 8 trials

Harvard University Initiative for Global Health
Vitamin A Implementation
• Widespread implementation of Vitamin A supplementation often linked to immunization programs.
• Is coverage sustainable outside of immunization campaigns?

Harvard University Initiative for Global Health
Iron Deficiency Anaemia
Vitamin A Deficiency
Zinc Deficiency
Review of Diseases, Injuries and Risk Factors

Harvard University Initiative for Global Health

Harvard University Initiative for Global Health
Global Zinc Deficiency
0 – 14.9 % Deficient 15 – 24.9 % Deficient > 25 % Deficient
From Brown et al, 2004
Harvard University Initiative for Global Health
Preventive Effect of Zinc Supplementation on Diarrheal Prevalence in Continuous
Supplementation Trials B.Faso
IndiaMexico
PNGPeru
VietnamEthopia
GuatemalaJamaica
Pooled
0 0.25 0.5 0.75 1 1.25 1.5 1.75 2
Odds Ratio and 95% CI

Harvard University Initiative for Global Health
Preventive Effect of Zinc Supplementation on Pneumonia Incidence in Continuous
Supplementation Trials
3
India(S)
Peru
Vietnam
Jamaica
India(B)
Pooled
0 0.5 1 1.5 2 2.5
Relative Risk and 95% CI
Harvard University Initiative for Global Health
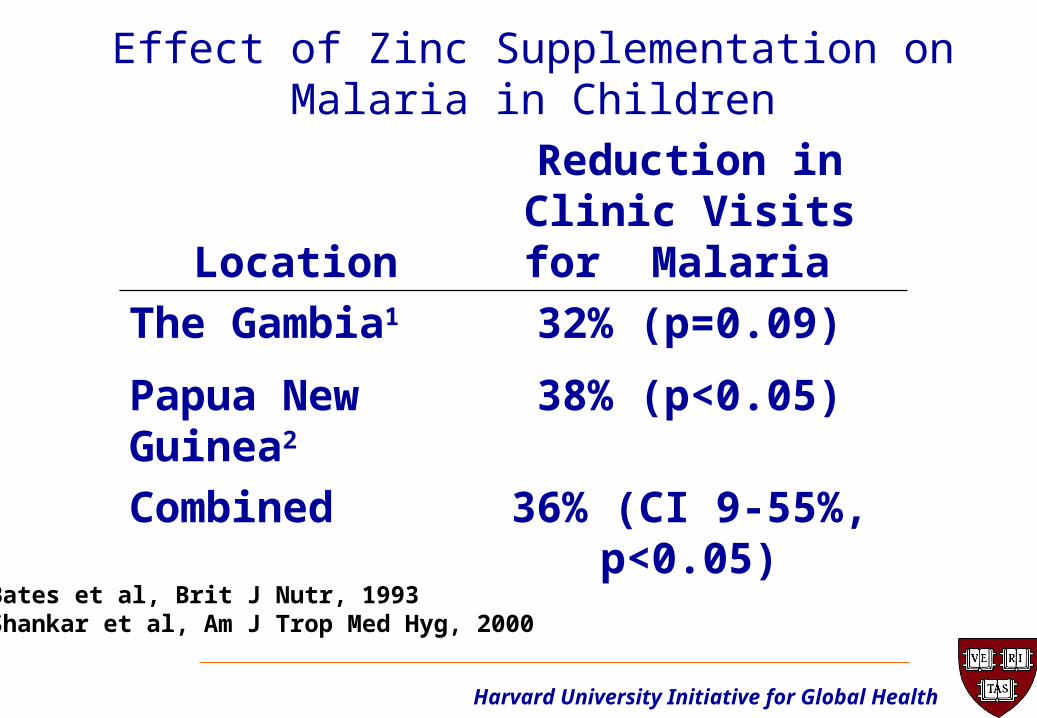
Effect of Zinc Supplementation on Malaria in Children
LocationReduction in Clinic Visits for Malaria
The Gambia1 32% (p=0.09)
Papua New Guinea2
38% (p<0.05)
Combined 36% (CI 9-55%, p<0.05)
1Bates et al, Brit J Nutr, 19932Shankar et al, Am J Trop Med Hyg, 2000
Harvard University Initiative for Global Health
Trial in Bangladesh Evaluating the Preventive Effect of
Weekly Zinc Supplementation
• 1-23 mo. old children, weekly zinc (70 mg)
• 6% less diarrhea, 17% less pneumonia, 49% less severe pneumonia and 42% less otitis media,
• 85% less mortality
From Brooks et al, Lancet 2005

Harvard University Initiative for Global Health
Efficacy Trials of Zinc Supplementation on Child Mortality
• Zanzibar and Nepal
• Children 1-35 mo. old (>60,000 child-years)
• Randomized, controlled trials
• Daily 10 mg zinc (5 mg if <12 mo old)
• All children receive vitamin A
• Trial to be completed in Zanzibar in September 2005 and Nepal in January 2006

Harvard University Initiative for Global Health
Iron Deficiency Anaemia
Vitamin A Deficiency
Zinc Deficiency
Review of Diseases, Injuries and Risk Factors

Harvard University Initiative for Global Health
Leading Causes of the Global Burden of Disease 2002
1. Perinatal conditions 6.5
2. Lower respiratory infections 6.1
3. HIV/AIDS 5.7
4. Depression 4.5
5. Diarrhoeal diseases 4.2
6. Ischaemic heart disease 3.9
7. Cerebrovascular disease 3.3
8. Malaria 3.1
9. Road traffic accidents 2.6
10. Tuberculosis 2.3
DALYs%
Source: World Health Report, 2004Source: World Health Report, 2004

Harvard University Initiative for Global Health
Attributable Disease Burden of 20 Risk Factors
0.0% 1.0% 2.0% 3.0% 4.0% 5.0% 6.0% 7.0% 8.0% 9.0% 10.0%
Underw eight
Unsafe sex
High blood pressure
Tobacco
Alcohol
Unsafe w ater, sanitation, and hygiene
High cholesterol
Indoor smoke from solid fuels
Iron deficiency
High BMI
Zinc deficiency
Low fruit and vegetable intake
Vitamin A deficiency
Physical inactivity
Occupational risk factors for injury
Lead exposure
Illicit drugs
Unsafe health care injections
Lack of contraception
Childhood sexual abuse
Attributable DALY (% of global DALY - Total 1.46 billion)
High-mortality developing
Lower-mortality developing
Developed

Harvard University Initiative for Global Health
What diseases, injuries or risk factors are What diseases, injuries or risk factors are missing from these lists?missing from these lists?
What is Missing?



![Lecture 13 - Security and Ethical Challenges[1]](https://static.documents.pub/doc/80x56/547aca8db37959652b8b4b13/lecture-13-security-and-ethical-challenges1.jpg)













