50
GLOBAL VALUE DOSSIER FOR MINIMALLY INVASIVE SURGERY MIS GVD – Thoracic surgery 1 GLOBAL VALUE DOSSIER FOR MINIMALLY INVASIVE SURGERY (MIS) THORACIC SURGERY

GLOBAL VALUE DOSSIER FOR MINIMALLY INVASIVE SURGERY
MIS GVD – Thoracic surgery 1
GLOBAL VALUE DOSSIER FOR MINIMALLY INVASIVE SURGERY (MIS)
THORACIC SURGERY

MIS GVD – Thoracic surgery 2
Prepared by: Jayne Smith-Palmer and Helen Sharland
Ossian Health Economics and Communications, Bäumleingasse 20, 4051 Basel, Switzerland
Phone: +41 61 271 6214
E-mail: [email protected]
Version No. 3.0
Date: November 28, 2019

MIS GVD – Thoracic surgery 3
Contents
1. Video-assisted thoracic surgery (wedge, segmentectomy, lobectomy) ......................... 4
1.1. Overview of procedure .............................................................................................. 4
1.2. Clinical and economic outcomes with VATS versus open thoracic surgery for pulmonary resection .............................................................................................................. 9
1.1.1. Clinical and economic evidence tables ............................................................ 18
1.3. References ............................................................................................................... 46
List of Tables
Table 1-1 Summary of meta-analyses comparing video-assisted versus open thoracic surgery .............................................................................................................................. 19
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery .............................................................................................................................. 22
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery ................................................................................................. 38
List of Figures
Figure 1-1 Indications for VATS major pulmonary resection in Russia .............................. 5
Figure 1-2 Wedge resection (segmentectomy), lobectomy and pneumonectomy .......... 6
Figure 1-3 Sleeve lobectomy ............................................................................................... 7
Figure 1-4 Length of stay with VATS lobectomy versus open lobectomy ....................... 12
Figure 1-5 Estimated blood loss with VATS versus open lobectomy ............................... 13
Figure 1-6 Mean (or median) operating time for VATS versus open lobectomy .............. 14
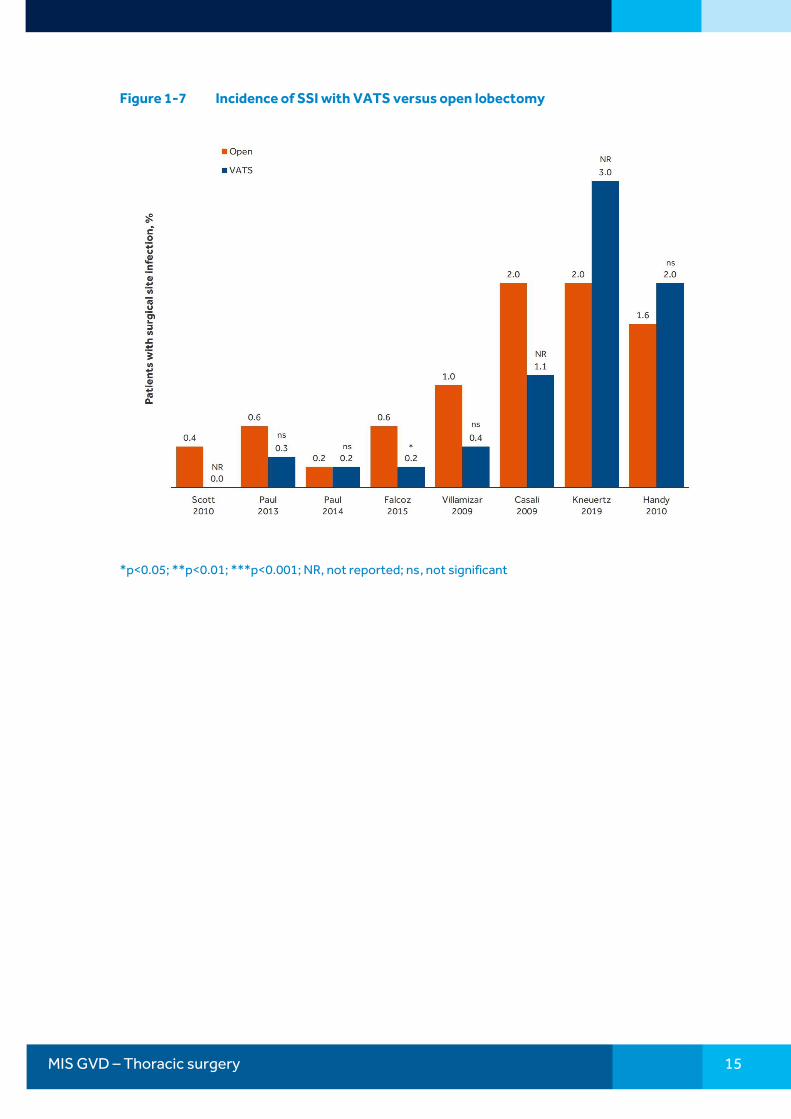
Figure 1-7 Incidence of SSI with VATS versus open lobectomy ....................................... 15
Figure 1-8 5 year survival rates in lung cancer patients undergoing VATS or open pulmonary resection ............................................................................................................... 16
Figure 1-9 Total hospital costs of VATS versus open pulmonary resection in studies conducted in Europe ............................................................................................................... 17
Figure 1-10 Total hospital costs of VATS versus open pulmonary resection in US-based studies .......................................................................................................................... 18

MIS GVD – Thoracic surgery 4
1. Video-assisted thoracic surgery (wedge, segmentectomy, lobectomy)
1.1. Overview of procedure
Video-assisted thoracic surgery (VATS) is used for both diagnostic and therapeutic procedures, with VATS procedures including wedge resections, segmentectomy, lobectomy, sleeve resections and pneumonectomy. VATS is becoming increasingly used for stage I and II non-small cell lung cancer (NSCLC) as well as in the treatment of spontaneous pneumothorax, biopsy and several benign conditions. The increased use of VATS in recent years has been partly attributed to improvements in optics and instrumentation and better anesthesia.1 VATS is preferred to open surgery, especially for some populations including those with pulmonary compromise, advanced age or impaired wound healing. Relative contraindications to VATS include tumor >6 cm in diameter. A key benefit of VATS over open surgery is reduced post-operative pain and reduced trauma to the chest wall as VATS, or thoracoscopic surgery, utilizes small incisions rather than the long incision required in traditional thoracotomy.
One of the most common indications for VATS procedures is NSCLC, which is one of the most commonly occurring cancers in the US and Europe, with >220,000 new cases of lung cancer in the US in 20152 and >380,000 cases in Europe in 2008.3 The use of VATS procedures in the US is continuing to increase at approximately 5% per year from an estimated 26,000 per year in 2005 to 43,000 per year in 2014.1 Additionally, the economic burden associated with lung resections is substantial; in the US alone, the cost of lung resections is an estimated USD 1.9 billion per year.4
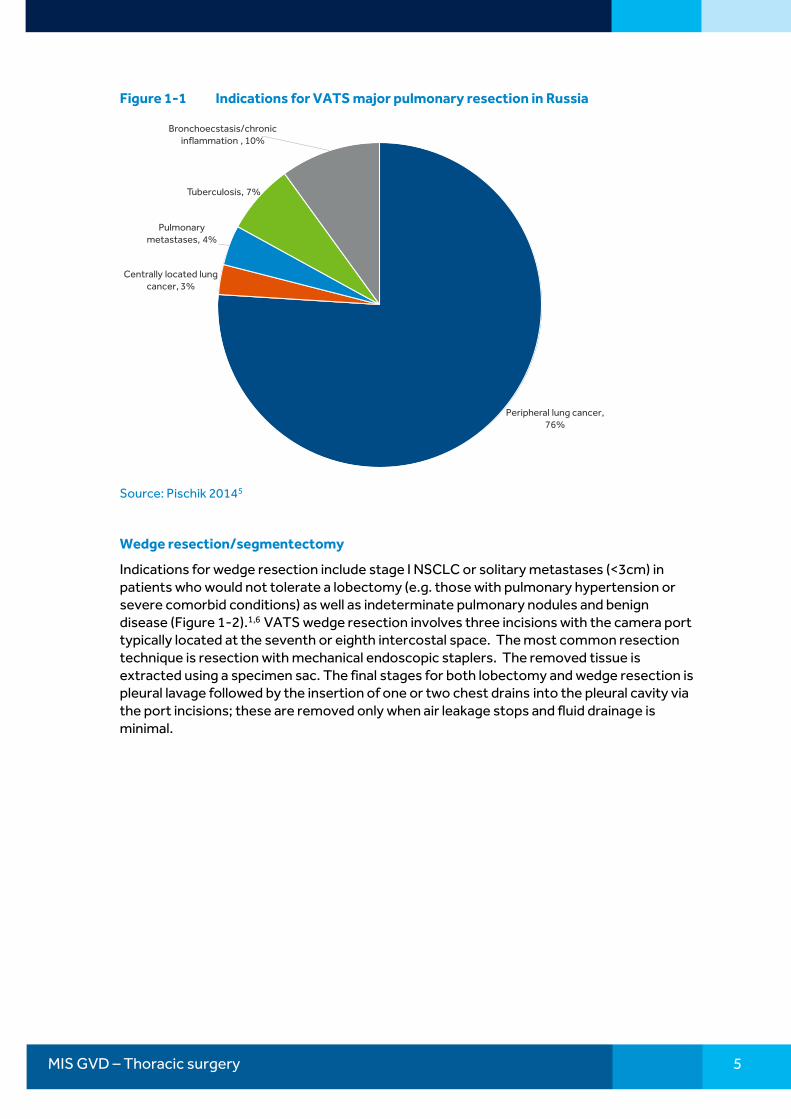
Typically, VATS procedures are performed with the patient in the lateral decubitus position with flexion of the operating table (to widen the intercostal spaces) and require general anesthesia with isolation of one lung and utilize three incisions including one utility incision (ranging from 4–10 cm in length, providing instrument access and through which the resected material is removed) and two for instrument access; however, some procedures can be performed using a single port. Lung cancer is the most common indication for major pulmonary resections with VATS (Figure 1-1); where the indication for VATS is lung cancer, hilar and mediastinal lymphadenectomy or node sampling are performed.
MIS GVD – Thoracic surgery 5
Figure 1-1 Indications for VATS major pulmonary resection in Russia
Peripheral lung cancer, 76%
Centrally located lung cancer, 3%
Pulmonary metastases, 4%
Tuberculosis, 7%
Bronchoecstasis/chronic inflammation , 10%
Source: Pischik 20145
Wedge resection/segmentectomy
Indications for wedge resection include stage I NSCLC or solitary metastases (<3cm) in patients who would not tolerate a lobectomy (e.g. those with pulmonary hypertension or severe comorbid conditions) as well as indeterminate pulmonary nodules and benign disease (Figure 1-2).1,6 VATS wedge resection involves three incisions with the camera port typically located at the seventh or eighth intercostal space. The most common resection technique is resection with mechanical endoscopic staplers. The removed tissue is extracted using a specimen sac. The final stages for both lobectomy and wedge resection is pleural lavage followed by the insertion of one or two chest drains into the pleural cavity via the port incisions; these are removed only when air leakage stops and fluid drainage is minimal.

MIS GVD – Thoracic surgery 6
Figure 1-2 Wedge resection (segmentectomy), lobectomy and pneumonectomy
Source: Colorado Cardiovascular Surgical Associates (available at: http://ccvsa.com/medical-surgical-procedures/thoracic-surgery)
Lobectomy
VATS lobectomy involves the removal of an entire lobe of the lung and is a relatively commonly performed procedure (Figure 1-2). Indications for lobectomy include stage I or II NSCLC in patients with sufficient pulmonary reserve to tolerate lobectomy as well as benign conditions such as granuloma, organized pneumonia, bronchiectasis, abscess and malformations.6 VATS lobectomy typically utilizes three incisions; the hilar structures are dissected first, after which the pulmonary vessels and bronchi within the hilum are then dissected, most commonly using endoscopic staplers.
Pneumonectomy
Pneumonectomy is a rarely performed procedure and a relatively low proportion of pneumonectomy procedures are performed using VATS and involves the removal of the entire lung, making it the most extensive pulmonary resection, pneumonectomy is generally avoided if other procedures can be performed instead of pneumonectomy (Figure 1-2). One of the most common indications for VATS pneumonectomy is bronchial tumors that cannot be resected using sleeve lobectomy. Three incisions are typically used and soft tissues retracted at the access incision, this is followed by hilar dissection then dissection of the pulmonary vessels, the lung is then then extracted from the thoracic cavity through the utility port using a specimen sac.7
Sleeve lobectomy
Sleeve lobectomy using VATS was first reported in 2002 but is not common and generally only performed by thoracic surgeons with considerable experience in VATS. Sleeve lobectomy is the most common bronchoplastic resection procedure, and involves circumferential airway resection and end-to-end anastomosis to join the remaining airways (Figure 1-3).8 The most common indications for sleeve lobectomy are benign or low grade malignant neoplasms or stenoses involving the main or lobar bronchi. Sleeve lobectomy is also indicated for patients who have compromised cardiopulmonary function (FEV1 <50%

MIS GVD – Thoracic surgery 7
predicted1 and maximum voluntary ventilation <50% predicted value) to preserve lung parenchyma and avoid pneumonectomy.
Sleeve lobectomy may be performed for any lobe but the most common site for sleeve lobectomy is right upper lobe followed by the left upper lobe; left lobe sleeve resections are more technically challenging owing to the proximity of the aorta and left recurrent nerve.
The procedure begins with dividing hilar structures followed by identification and transection of the pulmonary vessels then bronchial resection and anastomosis. Possible complications following sleeve lobectomy include sputum retention, bronchovascular and bronchopulmonary fistula, and anastomotic failure.
Figure 1-3 Sleeve lobectomy
Source: Gonzalez-Rivas et al. 20149
Guidelines on VATS
2017 European Society of Medical Oncology clinical practice guidelines for the treatment of early and locally advanced non-small cell lung cancer (NSCLC)10
For the treatment of stage I and II NSCLC:
• Either open thoracotomy or VATS access can be carried out as appropriate to the expertise of the surgeon (Level III, Grade A)
• VATS should be the approach of choice for stage I tumors (Level V, Grade C)
2007 Recommendations from the Consensus Statement of the International Society of Minimally Invasive Cardiothoracic Surgery11
For patients with clinical stage I non-small cell lung cancer (NSCLC) undergoing lung lobectomy
1 FEV1; forced expiratory volume in 1 second
MIS GVD – Thoracic surgery 8
• VATS can be recommended to reduce overall postoperative complications (class IIa, level A evidence)
• VATS can be recommended to reduce pain and overall functionality over the short term (class IIa, level B evidence)
• VATS can be recommended to improve delivery of adjuvant chemotherapy delivery (class IIa, level B evidence)
• VATS can be recommended for lobectomy in clinical stage I and II NSCLC patients with no proven difference in stage-specific 5-year survival compared with open thoracotomy (class IIb, level B evidence)
2014 Recommendations from the Japanese Association for Chest Surgery
For patients with pneumothorax undergoing surgery12
• VATS is broadly indicated as surgery for pneumothorax
• VATS is judged to be less invasive, as it results in minimal post-operative pain, the periods of chest tube placement and hospitalization are short, and it shows a trend toward early realization of social integration
• There is no difference in terms of safety and complications between VATS and open thoracotomy
• As it is anticipated that VATS will result in a higher recurrence rate than open thoracotomy, it may be desirable to add a supplemental procedure during surgery
For patients with lung cancer13
• VATS lobectomy may be considered and applied for patients with clinical stage I NSCLC; however, well-established evidence is lacking (Recommendation grade: Level C1) VATS lobectomy by an experienced thoracic surgeon may be considered for patients with clinical stage I NSCLC
• VATS lobectomy is estimated to be less invasive
• VATS showed better or at least equivalent outcomes regarding intra- or postoperative complications compared with thoracotomy
• Long-term survival by VATS lobectomy is suggested to be at least equivalent, although there is lack of evidence
2013 Recommendations from the American College of Chest Physicians (ACCP) for the treatment of patients with stage I and II NSCLC14
Lobectomy: for patients with clinical stage I NSCLC, a minimally invasive approach such as VATS (thoracoscopy) is preferred over a thoracotomy for anatomic pulmonary resection and is suggested in experienced centers (Grade 2C)

MIS GVD – Thoracic surgery 9
1.2. Clinical and economic outcomes with VATS versus open thoracic surgery for pulmonary resection
Key findings
Clinical outcomes
• Length of stay: Studies showed that in patients undergoing lobectomy, VATS was consistently associated with a shorter LoS than open surgery (Figure 1-4), with this difference achieving statistical significance in several individual studies29,30,32,34,36,38,39,41,42,43,44,45,47,48,50,52,53,54,55,57,60 and meta-analyses24,25,27
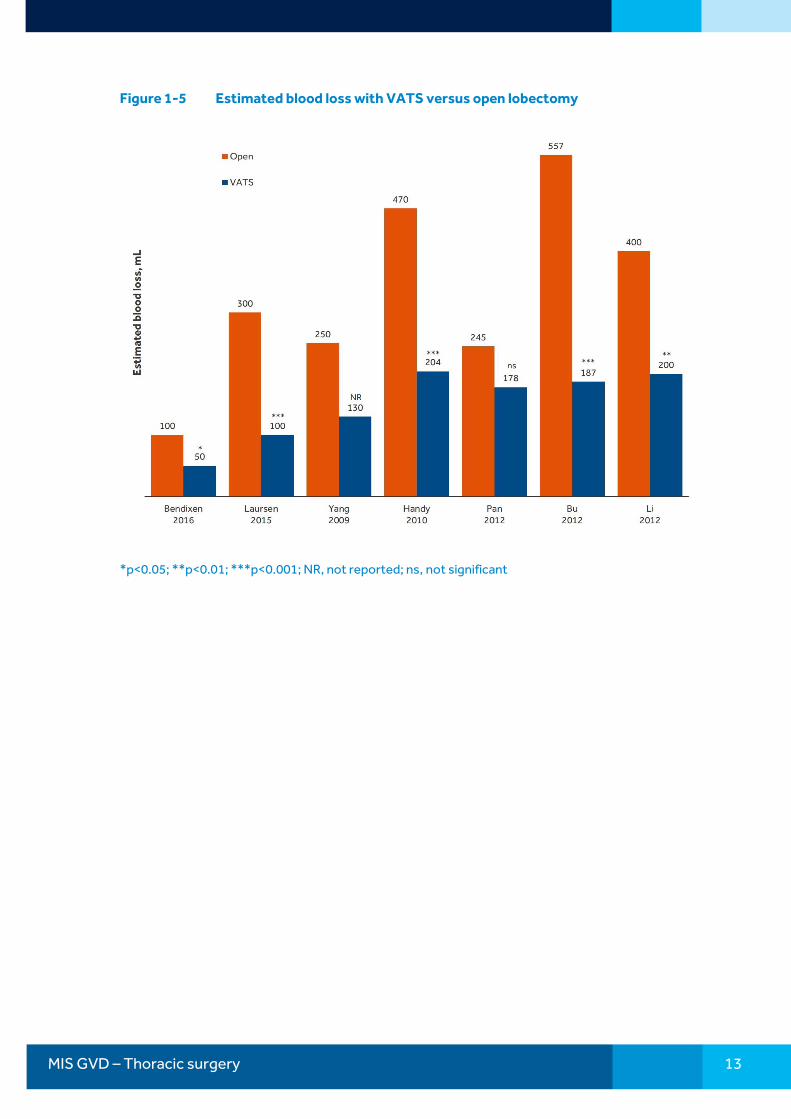
• Blood loss: Mean (or median) blood loss was consistently and significantly lower with VATS lobectomy compared with open lobectomy in individual studies30,44,54,58,59 (Figure 1-5) and meta-analyses25,27
• Blood transfusion: A lower proportion of patients undergoing VATS resection required blood transfusion compared with those undergoing open lung resection37,44,45,52,54 in the majority of studies the difference was significant37,44,45,54
• Operating time: VATS lobectomy was associated with significantly longer operating times than open lobectomy across several studies (Figure 1-6). 30,41,50,52,55,56,57 However, some studies showed operating times to be significantly shorted with VATS lobectomy compared with open lobectomy29,43,44,58,59
• SSI: In general, rates of SSI were similar for lobectomy performed as an open procedure or VATS;32,37,45,54 one study reported a significantly lower incidence of SSI with VATS versus open lobectomy40 (Figure 1-7)
• Overall survival: For patients undergoing lung resection for lung cancer, 5-year survival rates were similar for open and VATS resection (Figure 1-8).28,36,38,46,47 One study57 and three meta-analyses showed a significant survival benefit in favor of VATS24,25,26
• Chest tubes: Meta-analyses showed that the length of time chest tube drainage was required was significantly shorter with VATS than open lobectomy;25,27 findings among individual studies were inconsistent, three reported a significant difference in favor of VATS44,45,60 but six reported no significant difference30,54,55,57,58,59
• Post-operative pain: Post-operative pain scores were lower with VATS versus open lung resection24,30,48 The proportion of patients requiring pain medication was also significantly lower54, and pain medication was required for a significantly shorter length of time30
• Health care utilization: One US-based retrospective analysis showed that in the first 90 days post-discharge, patients who underwent VATS lobectomy had significantly fewer days of health care utilization and a significantly lower likelihood of utilizing inpatient services compared with patients who underwent open lobectomy (no significant difference was shown between VATS versus open wedge resection)42
MIS GVD – Thoracic surgery 10
Economic outcomes
• Total costs: Overall, in the majority of cost studies included in the analysis, total costs with VATS were lower than for corresponding open procedures, the one exception to this was studies conducted in China where inconsistency was noted
o United States: Total hospital costs in US-based studies were consistently lower with VATS lung resection than with open lung resection (Figure 1-9)34,38,41,42,43,56, 60,64 with this difference achieving statistical significance in several studies34,41,43,42,64 One US-based study showed that in the first 90 days post-discharge drug expenditure was significantly lower for patients who underwent VATS lobectomy versus open lobectomy (the difference between patients undergoing VATS versus open wedge resection was not significant)42
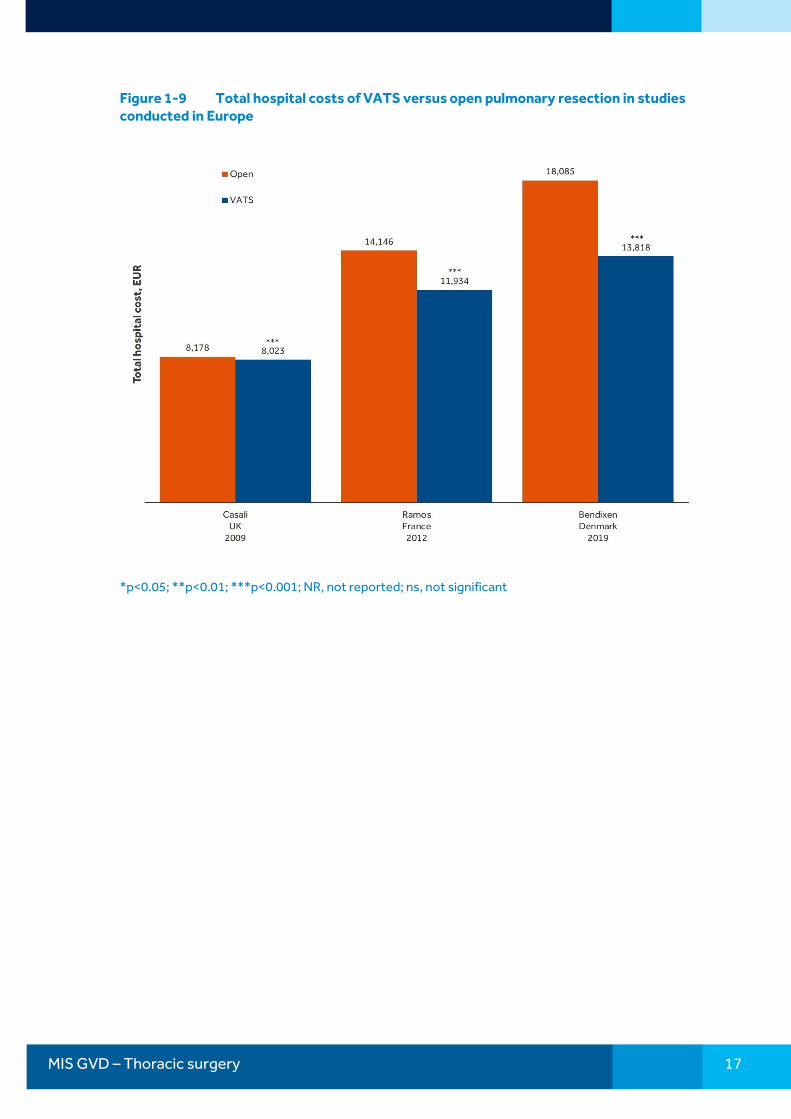
o Europe: In studies conducted in Europe (UK, France and Denmark) total hospital costs were significantly lower with VATS lung resection than with open lung resection (Figure 1-10)31,50,52
o China: Findings of cost studies from China were inconsistent, one study reported lower costs with VATS versus open surgery48 but a second study reported significantly higher total costs with VATS59
• Savings due to clinical benefits: Studies presenting a breakdown of total costs demonstrate that the lower post-operative ward stay costs, primarily due to a shorter LoS are a key driver of lower overall costs.50,52,61 The lower rate of post-operative complications with VATS is also likely to translate into economic benefits
Other findings
• Learning curve: Operating time for VATS procedures is influenced by surgeon experience and a learning curve is evidence with operating time decreasing as surgeon experience increases.15,16,17 Higher levels of surgeon experience is also associated with reduced costs16
• Barriers to use: A survey of surgeons showed that 92% of surgeons are willing to learn VATS lobectomy, but barriers included limited resources (50%), limited exposure/mentoring (45%) and limited clinical evidence (20%). When questioned about the advantages of VATS versus open thoracotomy, a high proportion of surgeons believed that VATS was associated with less post-operative pain (81%), shorter LoS (72%) and higher patient satisfaction (80%)18
• Economic impact of complications: Intra-operative and post-operative complications, which are more common with open surgery, are associated with higher overall costs. For example, in a study of VATS procedures intra-operative blood transfusion increased costs by >USD 15,000. Similarly, post-operative pneumonia and blood transfusion increased costs by more than USD 2,900 and USD 5,800, respectively19
• Re-admission: Re-admission within 30 days following lung cancer resection is associated with a 6-fold increase in 90-day post-operative mortality20
• Tissue trauma: Studies looking at inflammatory markers (e.g. tumor necrosis factor-ɑ, interleukin-6, interleukin-8, interleukin-10 and C-reactive protein [CRP]) have shown that VATS is associated with lower levels of interleukin-6 and CRP and a

MIS GVD – Thoracic surgery 11
quicker return of immune function compared with open lobectomy, although the significance of this remains unknown21
• Pulmonary function: In a Japanese study of n=204 patients (n=42 with dyspnea) undergoing major lung resections (mean age 64 years) post-operative pulmonary function (including FEV1 and FVC) shows significantly better improvement in patients undergoing VATS compared with those undergoing open thoracotomy22
• High risk patients: The benefits of VATS relative to open lobectomy in terms of reduced complications may be of particular importance in patients considered to be high risk, such as those with substantial pre-operative comorbidities21
• Quality of life: Compared with open lobectomy VATS lobectomy has been shown to be associated with a better profile in terms of quality of life and faster return to normal activities23,30,31
• Ambulation: Patients who underwent VATS lobectomy performed significantly better in the 6-minute walk test at 48 hours, and 7, 14 and 30 days post-discharge compared with patients who underwent lobectomy for NSCLC24
• Disease recurrence: In two meta-analyses, patients who underwent VATS lobectomy were shown to have lower overall disease recurrence compared with open lobectomy24,58 with one reporting significantly lower recurrence.24 Both local and distant recurrence was shown to be lower in VATS lobectomy patients than open lobectomy24 but only significantly lower for distant recurrence 24,26

MIS GVD – Thoracic surgery 12
Figure 1-4 Length of stay with VATS lobectomy versus open lobectomy
*p<0.05; **p<0.01; ***p<0.001; NR, not reported; ns, not significant
MIS GVD – Thoracic surgery 13
Figure 1-5 Estimated blood loss with VATS versus open lobectomy
*p<0.05; **p<0.01; ***p<0.001; NR, not reported; ns, not significant

MIS GVD – Thoracic surgery 14
Figure 1-6 Mean (or median) operating time for VATS versus open lobectomy
*p<0.05; **p<0.01; ***p<0.001; NR, not reported; ns, not significant
MIS GVD – Thoracic surgery 15
Figure 1-7 Incidence of SSI with VATS versus open lobectomy
*p<0.05; **p<0.01; ***p<0.001; NR, not reported; ns, not significant

MIS GVD – Thoracic surgery 16
Figure 1-8 5 year survival rates in lung cancer patients undergoing VATS or open pulmonary resection
*p<0.05; **p<0.01; ***p<0.001; NR, not reported; ns, not significant
MIS GVD – Thoracic surgery 17
Figure 1-9 Total hospital costs of VATS versus open pulmonary resection in studies conducted in Europe
*p<0.05; **p<0.01; ***p<0.001; NR, not reported; ns, not significant

MIS GVD – Thoracic surgery 18
Figure 1-10 Total hospital costs of VATS versus open pulmonary resection in US-based studies
*p<0.05; **p<0.01; ***p<0.001; NR, not reported; ns, not significant
1.1.1. Clinical and economic evidence tables
A summary of clinical evidence on VATS compared with open surgery from published meta-analyses and published studies is shown in Table 1-1 and Table 1-2, respectively. A summary of economic evidence from published cost studies is shown in Table 1-3.
In the following tables outcomes where p<0.05 are underlined.

19
Table 1-1 Summary of meta-analyses comparing video-assisted versus open thoracic surgery
Authors Details Procedures Outcome OR (95% CI) P value
Ng et al. 201924 115 studies Multiport VATS versus open lobectomy for NSCLC
Post-operative LoS Complications Cardiopulmonary Atrial fibrillation Prolonged air leak Pneumonia Wound infections 30 day mortality 90 day mortality Forced expiration volume, % Day 7 Day 30 Day 90 Pain using visual analog scale Day 1 Day 7 Day 14 Day 30 Day 90 European Quality of Life 5 Dimensions scale 2 weeks 4 weeks 8 weeks 12 weeks 26 weeks Global quality of life at 1 year 6 minute walk 48 hours Day 7, % change from baseline Day 14, % change from baseline
Mean difference –1.90 (–2.25, –1.54) 0.64 (0.59, 0.71) 0.60 (0.48, 0.75) 0.62 (0.45, 0.84) 0.78 (0.67, 0.90) 0.74 (0.66, 0.83) 0.50 (0.36, 0.68) 0.77 (0.62, 0.95) 0.78 (0.56 1.07) Mean difference 3.04 (1.01, 5.08) Mean difference 2.02 (–3.54, 7.58) Mean difference 2.36 (–3.42, 8.14) Mean difference –0.68 (–1.01, –0.35) Mean difference –1.01 (–1.46, –0.56) Mean difference –0.37 (–0.66, –0.08) Mean difference –0.84 (–1.41, –0.26) Mean difference –1.31 (–1.80, –0.82) Mean difference 3.80 (–0.90, 8.50) Mean difference 4.60 (–0.07, 9.27) Mean difference 11.70 (7.05, 16.35) Mean difference 3.10 (–0.91, 7.11) Mean difference 3.60 (–1.07, 8.27) Standardized mean difference 0.42 (0.20, 0.64) Mean difference 55.53 (34.49, 76.57) Mean difference 11.60 (11.54, 11.66) Mean difference 4.20 (4.16, 4.24)
<0.001 <0.001 <0.001 0.002 0.001 <0.001 <0.001 0.02 0.12 0.003 0.48 0.42 <0.001 <0.001 0.01 0.004 <0.001 0.11 0.05 <0.001 0.13 0.13 <0.001 <0.001 <0.001 <0.001

20
Table 1-1 Summary of meta-analyses comparing video-assisted versus open thoracic surgery
Authors Details Procedures Outcome OR (95% CI) P value
Day 30, meters Post-discharge Survival at 5 years Disease-free survival at 5 years Overall disease recurrence Local recurrence Distant recurrence
Mean difference 63.10 (38.31, 87.89) 1.35 (1.17, 1.56) 1.15 (0.94, 1.40) 0.73 (0.61, 0.87) 0.77 (0.58, 1.03) 0.67 (0.52, 0.85)
<0.001 <0.001 0.18 <0.001 0.08 0.001
Chen et al. 201325 20 studies, n=3,457 patients
VATS versus open lobectomy for stage I non-small cell lung cancer
Peri-operative Operating time, mins Blood loss, mL Post-operative Drainage time, days LoS, days Complication incidence Post-discharge 5 year survival
−14.68 (−4.68, 34.03) −62.49 (−79.32, −45.66) −0.39 (−0.69, −0.09) −1.74 (−2.20, −1.20) 0.61 (0.49, 0.76) 1.82 (1.43, 2.31)
0.14 <0.00001 0.01 <0.00001 <0.0001 <0.00001
Yan et al. 200926 21 studies (2 RCTs and 19 non RCTs), n=2,641 patients
VATS versus open lobectomy for early stage NSCLC
Post-operative Mortality Pneumonia Post-discharge Systemic recurrence 5-year mortality
0.49 (0.06, 3.76) 0.34 (0.10, 1.16) 0.57 (0.34, 0.96) 0.66 (0.45, 0.97)
0.49 0.09 0.03 0.04
Cheng et al. 200727 Level A meta-analysis; 3 RCTs, n=205 patients Level B meta-analysis 33 non-RCT studies, n=3,384 patients
VATS versus open (thoracotomy) lobectomy for non-small cell lung cancer
Operating time, mins RCT non-RCT Blood loss, mL RCT non-RCT Chest tube drainage, days RCT
16.17 (2.46, 29.89)a 7.62 (−24.44, 39.69)a 17.20 (2.62, 31.79)a −79.1 (−106.9, −52.4)a NA −79.1 (−106.9, −52.4)a −0.96 (−1.59, −0.34)a −1.90 (−4.05, 0.25)a
0.02 0.64 0.02 <0.00001 NA <0.00001 0.002 0.08

21
Table 1-1 Summary of meta-analyses comparing video-assisted versus open thoracic surgery
Authors Details Procedures Outcome OR (95% CI) P value
non-RCT LoS, days RCT non-RCT Any complication RCT non-RCT Pneumonia RCT non-RCT Prolonged air leak (>7 days) RCT non-RCT In-hospital mortality (non-RCT)
−0.92 (−1.56, −0.28)a −2.60 (−1.47, −0.72)a 0.10 (−1.63, 1.83)a −2.99 (−5.07, −0.91)a 0.48 (0.32, 0.70) 0.30 (0.11, 0.81) 0.52 (0.34, 0.80) 0.56 (0.26, 1.21) 0.10 (0.01, 2.17) 0.68 (0.30, 1.53) 1.67 (0.92, 3.03) 0.38 (0.09, 1.60) 2.44 (1.21, 4.90) 0.79 (0.38, 1.64)
0.005 0.007 0.91 0.005 0.0002 0.02 0.003 0.14 0.14 0.35 0.09 0.19 0.01 0.53
Odds ratios below 1.00 favor VATS; odds ratios above 1.00 favor open Weighted mean difference, negative values favor VATS
22
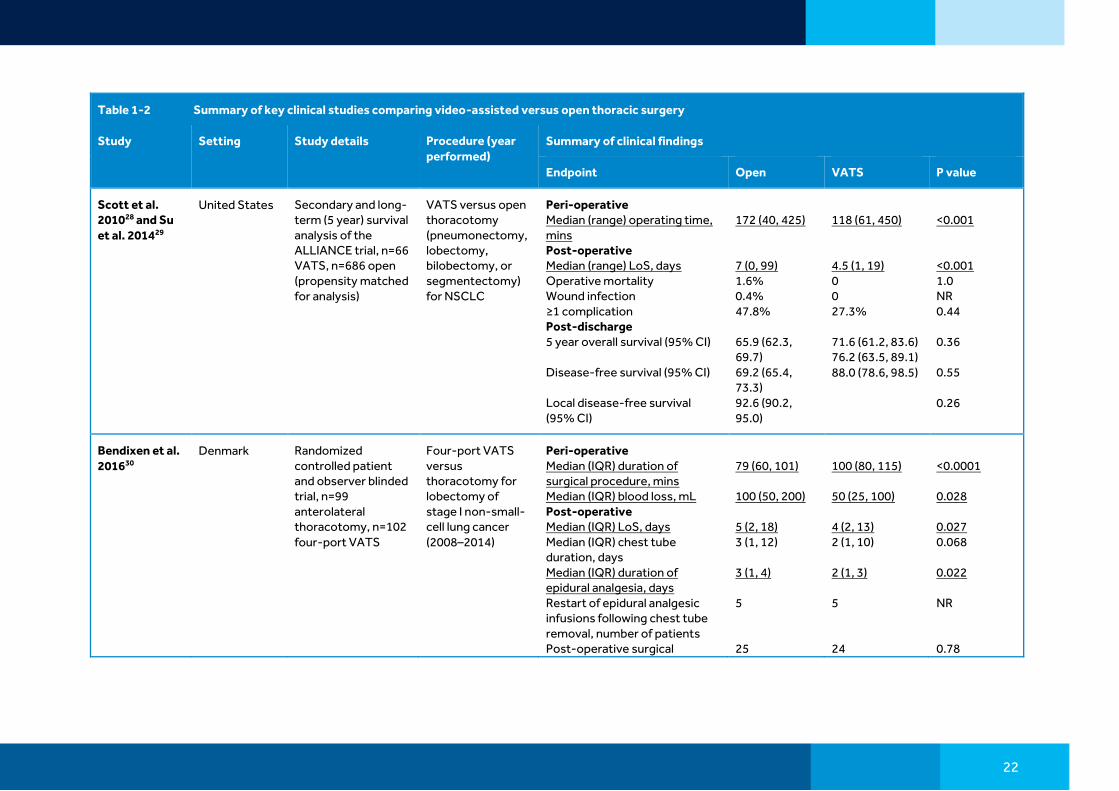
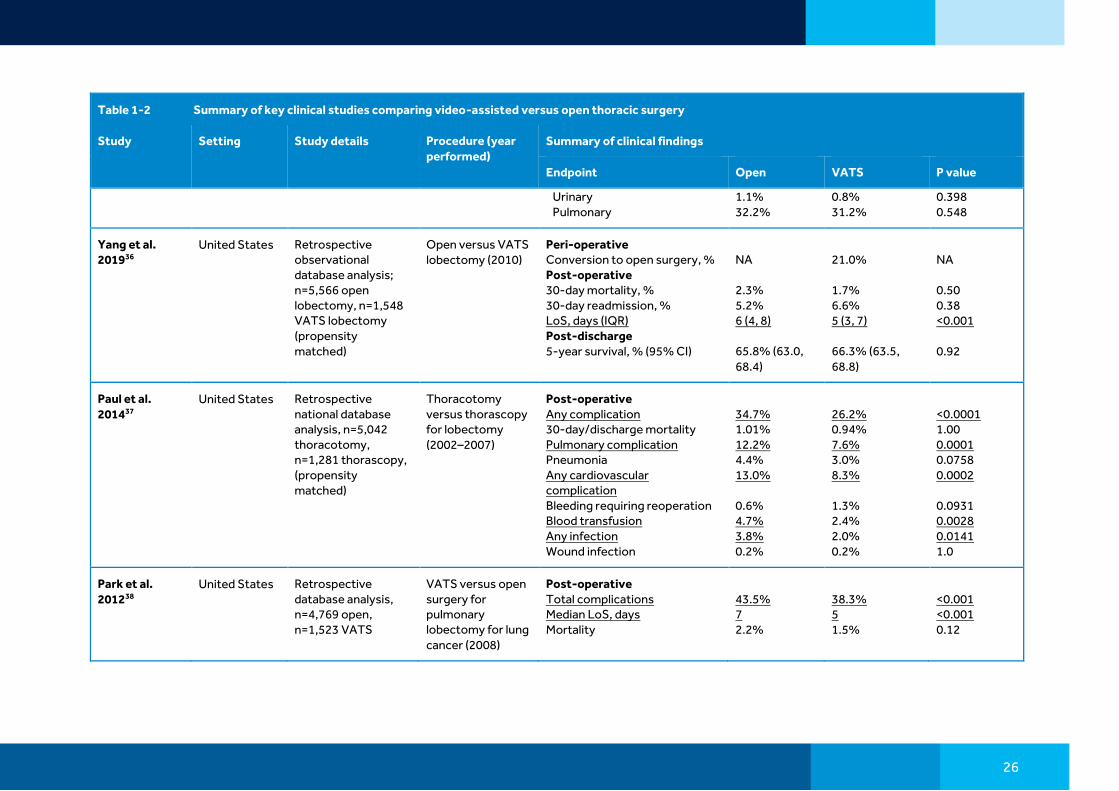
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
Scott et al. 201028 and Su et al. 201429
United States Secondary and long-term (5 year) survival analysis of the ALLIANCE trial, n=66 VATS, n=686 open (propensity matched for analysis)
VATS versus open thoracotomy (pneumonectomy, lobectomy, bilobectomy, or segmentectomy) for NSCLC
Peri-operative Median (range) operating time, mins Post-operative Median (range) LoS, days Operative mortality Wound infection ≥1 complication Post-discharge 5 year overall survival (95% CI) Disease-free survival (95% CI) Local disease-free survival (95% CI)
172 (40, 425) 7 (0, 99) 1.6% 0.4% 47.8% 65.9 (62.3, 69.7) 69.2 (65.4, 73.3) 92.6 (90.2, 95.0)
118 (61, 450) 4.5 (1, 19) 0 0 27.3% 71.6 (61.2, 83.6) 76.2 (63.5, 89.1) 88.0 (78.6, 98.5)
<0.001 <0.001 1.0 NR 0.44 0.36 0.55 0.26
Bendixen et al. 201630
Denmark Randomized controlled patient and observer blinded trial, n=99 anterolateral thoracotomy, n=102 four-port VATS
Four-port VATS versus thoracotomy for lobectomy of stage I non-small-cell lung cancer (2008–2014)
Peri-operative Median (IQR) duration of surgical procedure, mins Median (IQR) blood loss, mL Post-operative Median (IQR) LoS, days Median (IQR) chest tube duration, days Median (IQR) duration of epidural analgesia, days Restart of epidural analgesic infusions following chest tube removal, number of patients Post-operative surgical
79 (60, 101) 100 (50, 200) 5 (2, 18) 3 (1, 12) 3 (1, 4) 5 25
100 (80, 115) 50 (25, 100) 4 (2, 13) 2 (1, 10) 2 (1, 3) 5 24
<0.0001 0.028 0.027 0.068 0.022 NR 0.78
23
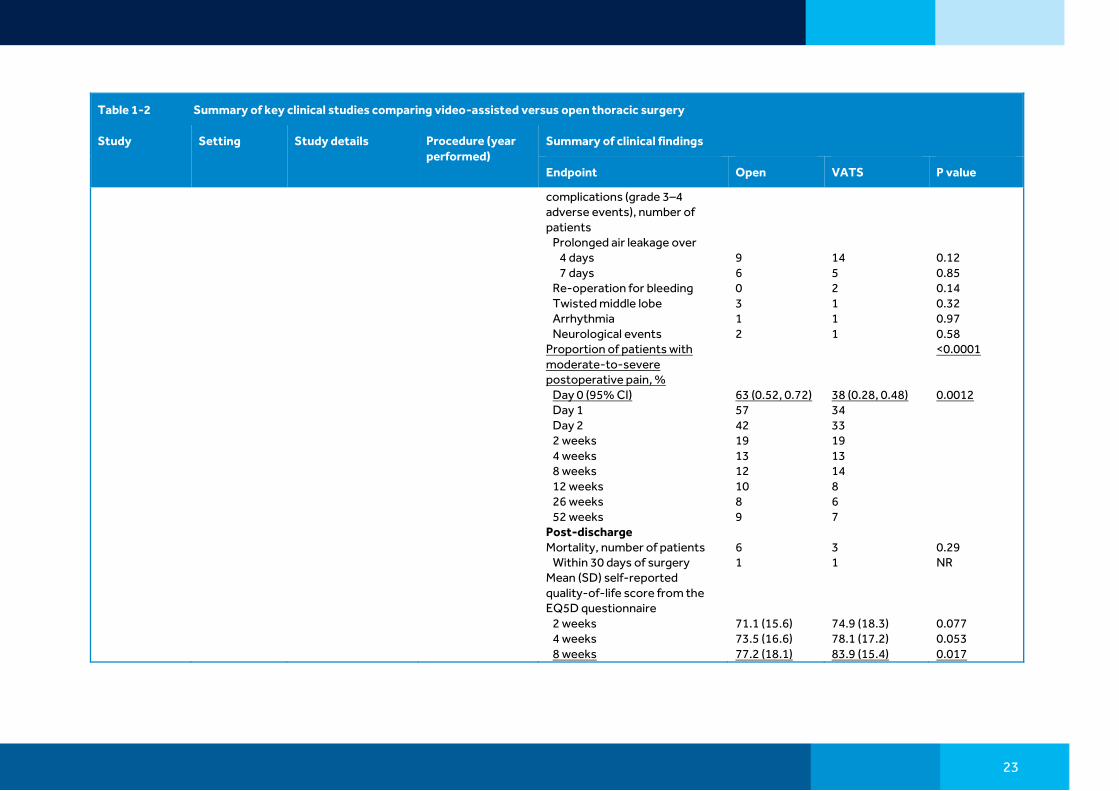
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
complications (grade 3–4 adverse events), number of patients Prolonged air leakage over 4 days 7 days Re-operation for bleeding Twisted middle lobe Arrhythmia Neurological events Proportion of patients with moderate-to-severe postoperative pain, % Day 0 (95% CI) Day 1 Day 2 2 weeks 4 weeks 8 weeks 12 weeks 26 weeks 52 weeks Post-discharge Mortality, number of patients Within 30 days of surgery Mean (SD) self-reported quality-of-life score from the EQ5D questionnaire 2 weeks 4 weeks 8 weeks
9 6 0 3 1 2 63 (0.52, 0.72) 57 42 19 13 12 10 8 9 6 1 71.1 (15.6) 73.5 (16.6) 77.2 (18.1)
14 5 2 1 1 1 38 (0.28, 0.48) 34 33 19 13 14 8 6 7 3 1 74.9 (18.3) 78.1 (17.2) 83.9 (15.4)
0.12 0.85 0.14 0.32 0.97 0.58 <0.0001 0.0012 0.29 NR 0.077 0.053 0.017

24
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
12 weeks 26 weeks 52 weeks
82.2 (14.7) 81.3 (17.5) 80.6 (19.3)
85.3 (14.3) 84.9 (16.2) 86.7 (14.2)
0.14 0.18 0.012
Bendixen et al. 201931
Denmark Retrospective analysis of randomized controlled patient and observer blinded trial, n=99 anterolateral thoracotomy, n=102 four-port VATS
Four-port VATS versus thoracotomy for lobectomy of stage I non-small-cell lung cancer (2008–2014)
Post-discharge Mean (SD) number of Combined outpatient visits Standard outpatient visits Blood test visits Rehabilitation treatments Other outpatient visits Specialist consultations General practitioner consultations Out-of-hours General practitioner visits Hospital readmissions Mean (SD) admission time for readmissions, days Mean (SD) QALYs gained over 52 weeks of follow-up
0.7 (0.31) 1.7 (1.4) 0.03 (0.22) 0.74 (2.6) 0.82 (0.4) 4.1 (6.6) 39.6 (23) 2. (5.3) 2.71 (2.1) 10.31 (16.8) 0.830 (0.13)
0.44 (0.61) 2.06 (1.9) 0.05 (0.26) 1.2 (5.0) 0.78 (0.32) 3.96 (4.96) 40.98 (26.3) 2.2 (4.5) 2.60 (2.2) 8.46 (13.4) 0.851 (0.16)
ns ns ns ns ns ns ns ns ns ns 0.048
Paul et al. 201332
United States Retrospective database analysis (Nationwide Inpatient Sample), n=10,554 thorascopy; n=57,796 thoracotomy,
Thorascopy versus thoracotomy for lobectomy (2007–2008)
Peri-operative Puncture/laceration Bleeding Post-operative Mortality Median (range) LoS, days Any complication
1.1% 1.5% 2.3% 7 (5, 9) 50.4%
0.9% 1.7% 1.6% 5 (3, 8) 46.5%
0.422 0.474 0.062 <0.001 0.003

25
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
patients were propensity matched
Pneumonia Wound infection
8.2% 0.6%
7.3% 0.3%
0.170 0.053
Kent et al. 201433
United States Retrospective national database analysis, n=20,238 open; n=12,427 VATS, n=430 robotic (not presented), propensity matched analysis
Open versus VATS versus robotic lobectomy or segmentectomy (2008–2010)
Post-operative Mortality Mean LoS, days Routine discharge Prolonged LoS Any complication Bleeding complication
2.0% 8.2 59.5% 9.6% 54.1% 1.9%
1.1% 6.3 64.5% 6.9% 45.3% 1.3%
NR NR NR NR NR NR
Farjah et al. 201434
United States Retrospective cohort study using the MarketScan database, n=6,893 thoracotomy, n=3,069 VATS
VATS versus open lobectomy for lung cancer (2007−2011)
Post-operative Median LoS, days Prolonged LoS 90-day re-admission
6 7.2% 12%
4 3.0% 10%
<0.001 <0.001 0.026
Gopaldas et al. 201035
United States Retrospective national database analysis; n=12,860 thoracotomy; n=759 VATS
VATS versus open lobectomy (2004–2006)
Post-operative LoS, days Mortality Total complications Wound Infection Cardiovascular Intraoperative Systemic Gastrointestinal
9.3 (0.1) 3.1% 43.1% 0.8% 0.6% 3.4% 2.8% 1.0% 1.2%
9.2 (0.4) 3.4% 44.1% 1.3% 0.5% 3.9% 4.1% 1.2% 1.1%
0.696 0.676 0.592 0.151 0.726 0.431 0.033 0.563 0.792
26
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
Urinary Pulmonary
1.1% 32.2%
0.8% 31.2%
0.398 0.548
Yang et al. 201936
United States Retrospective observational database analysis; n=5,566 open lobectomy, n=1,548 VATS lobectomy (propensity matched)
Open versus VATS lobectomy (2010)
Peri-operative Conversion to open surgery, % Post-operative 30-day mortality, % 30-day readmission, % LoS, days (IQR) Post-discharge 5-year survival, % (95% CI)
NA 2.3% 5.2% 6 (4, 8) 65.8% (63.0, 68.4)
21.0% 1.7% 6.6% 5 (3, 7) 66.3% (63.5, 68.8)
NA 0.50 0.38 <0.001 0.92
Paul et al. 201437
United States Retrospective national database analysis, n=5,042 thoracotomy, n=1,281 thorascopy, (propensity matched)
Thoracotomy versus thorascopy for lobectomy (2002–2007)
Post-operative Any complication 30-day/discharge mortality Pulmonary complication Pneumonia Any cardiovascular complication Bleeding requiring reoperation Blood transfusion Any infection Wound infection
34.7% 1.01% 12.2% 4.4% 13.0% 0.6% 4.7% 3.8% 0.2%
26.2% 0.94% 7.6% 3.0% 8.3% 1.3% 2.4% 2.0% 0.2%
<0.0001 1.00 0.0001 0.0758 0.0002 0.0931 0.0028 0.0141 1.0
Park et al. 201238
United States Retrospective database analysis, n=4,769 open, n=1,523 VATS
VATS versus open surgery for pulmonary lobectomy for lung cancer (2008)
Post-operative Total complications Median LoS, days Mortality
43.5% 7 2.2%
38.3% 5 1.5%
<0.001 <0.001 0.12

27
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
Paul et al. 201439
United States Retrospective national database analysis, n=4,715 thoracotomy, n=1,293 thorascopy, propensity matched analysis
Thoracotomy versus thorascopic lobectomy for lung cancer (2007–2009)
Post-operative Mean (SD) LoS, days Median (IQR) LoS, days In-hospital mortality
8.7 (6.6) 7 (5, 10) 43 (3.6)
6.6 (6) 5 (3, 8) 25 (2.1)
<0.0001 <0.001 0.0290
Falcoz et al. 201540
Multinational (Europe)
Retrospective analysis of the ESTS database, n=2,721 open; n=2,721 VATS propensity matched patients
VATS versus open lobectomy for lung cancer (2007–2013)
Post-operative Mean (SD) LoS Any complication Major cardiopulmonary complication Air leak duration <5 days Pneumonia Reoperation for bleeding Wound infection Death
9.8 (6.9) 31.7% 19.6% 9.2% 6.2% 1.5% 0.6% 1.9%
7.8 (5.8) 29.1% 15.9% 10.1% 6.0% 1.5% 0.2% 1.0%
NR 0.0357 0.0094 0.2363 0.7739 1 0.0218 0.0201
Swanson et al. 201241
United States Retrospective database analysis, n=2,907 open, n=1,054 VATS
Open versus VATS lobectomy (2007–2008)
Peri-operative Mean (SD) operation time, hours Post-operative Mean (SD) LoS, days
3.75 (0.47) 7.83 (2.05)
4.09 (0.52) 6.15 (1.61)
0.000 0.000
Watson and Qiu 201442
United States Retrospective database analysis, n=669 open lobectomy, n=270 VATS lobectomy,
Open versus VATS lobectomy and wedge resection (2010)
Lobectomy Post-operative Mean (95% CI) LoS difference (Open-VATS), days Post-discharge
1.79 (1.36, 2.22)
<0.0001

28
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
n=340 open wedge resection, n=1332 VATS wedge resection
Health care utilization in 90 days Office visits Hospital outpatient visits Estimated days of health care utilization ER visits, odds ratio Inpatient services, odds ratio Health care utilization in 365 days Office visits Hospital outpatient visits Estimated days of health care utilization ER visits, odds ratio Inpatient services, odds ratio Wedge resection Post-operative Mean (95% CI) LoS difference (Open-VATS), days Post-discharge Health care utilization in 90 days Office visits Hospital outpatient visits Estimated days of health care utilization ER visits, odds ratio Inpatient services, odds ratio Health care utilization in 365 days Office visits Hospital outpatient visits
6.83 4.43 10.31 1.15 1.86 21.72 12.30 28.43 1.28 1.22 1.49 (1.21, 1.78) 5.59 3.81 9.48 1.13 0.90 18.36 12.32
6.30 3.58 8.07 20.65 10.89 24.97 5.87 4.48 9.85 18.50 13.11
0.27 0.02 0.0002 0.54 0.008 0.39 0.14 0.03 0.16 0.25 <0.0001 0.46 0.04 0.55 0.51 0.53 0.89 0.48

29
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
Estimated days of health care utilization ER visits, odds ratio Inpatient services, odds ratio
28.03 1 0.83
29.54
0.42 0.98 0.22
Howington et al. 201243
United States Retrospective database analysis; n=999 open; n=1,052 VATS
VATS versus open thoracotomy for wedge resection in lung cancer (2007–2008)
Peri-operative Mean (SD) operating time, hours Mean (SD) LoS, days
3:16 (0:43) 6.34 (2.31)
2:82 (0:38) 4.44 (1.62)
0.000 0.000
Laursen et al. 201544
Denmark Retrospective database analysis of prospectively collected data, n=785 VATS and n=594 thoracotomy
VATS versus open (thoracotomy) lobectomy for lung cancer (2005–2011)
Peri-operative Median (range) blood loss, mL Median (range) operating time, mins Median (range) pleural cavity drainage, days Post-operative Median (range) LoS, days Conversion Re-do operation Minor complication Major complication Pneumonia Transfusion ICU Infection without specification
300 (0–11 000) 155 (55–405) 4.00 (1–100) 7.00 (2–61) NA 5.2% 48.5% 35.7% 10.6% 23.2% 4.0% 8.4%
100 (0–3500) 125 (42-360) 3.00 (0–101) 5.00 (1–65) 4.5% 4.2% 36.3% 20.0% 7.5% 7.0% 1.5% 2.7%
<0.001 <0.001 <0.001 <0.001 NA 0.375 <0.001 <0.001 0.045 <0.001 0.004 <0.001
Villamizar et al. 200945
United States Retrospective database of prospectively
Thorascopy versus thoracotomy for
Post-operative Median (IQR) LoS, days Median (IQR) chest tube
5 (4, 7) 4 (3, 6)
4 (3, 6) 3 (2, 4)
0.0001 0.0001
30
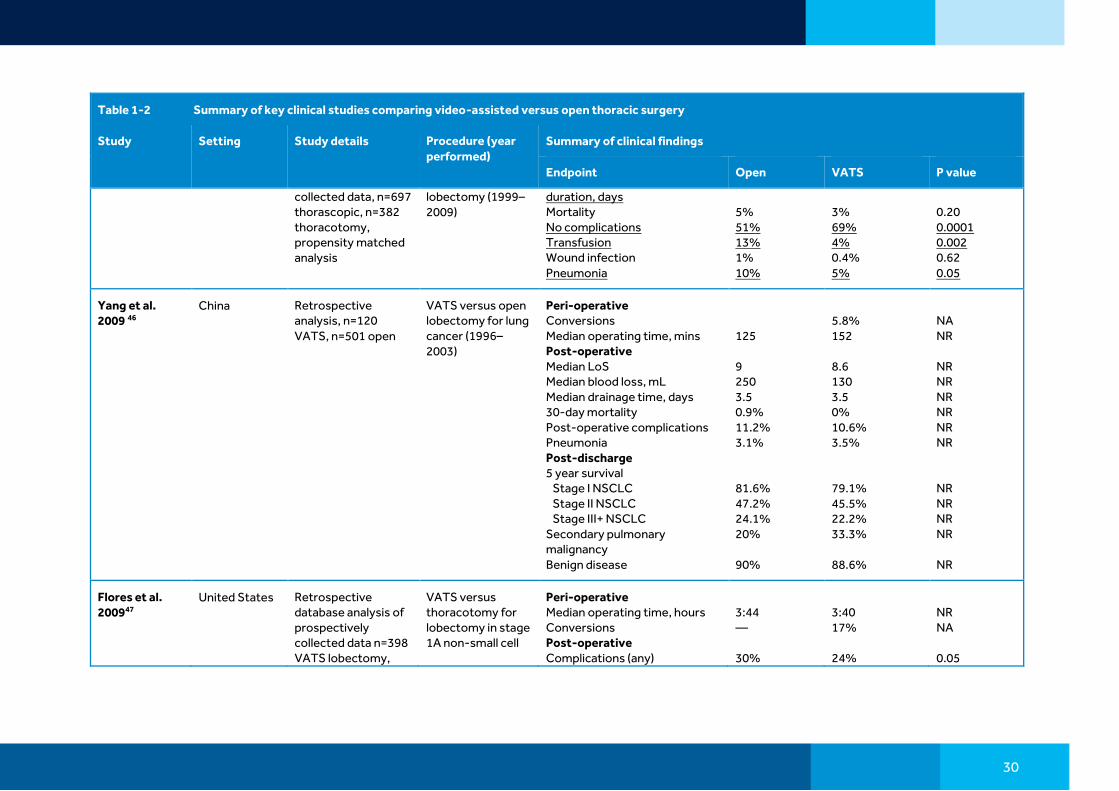
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
collected data, n=697 thorascopic, n=382 thoracotomy, propensity matched analysis
lobectomy (1999–2009)
duration, days Mortality No complications Transfusion Wound infection Pneumonia
5% 51% 13% 1% 10%
3% 69% 4% 0.4% 5%
0.20 0.0001 0.002 0.62 0.05
Yang et al. 2009 46
China Retrospective analysis, n=120 VATS, n=501 open
VATS versus open lobectomy for lung cancer (1996–2003)
Peri-operative Conversions Median operating time, mins Post-operative Median LoS Median blood loss, mL Median drainage time, days 30-day mortality Post-operative complications Pneumonia Post-discharge 5 year survival Stage I NSCLC Stage II NSCLC Stage III+ NSCLC Secondary pulmonary malignancy Benign disease
125 9 250 3.5 0.9% 11.2% 3.1% 81.6% 47.2% 24.1% 20% 90%
5.8% 152 8.6 130 3.5 0% 10.6% 3.5% 79.1% 45.5% 22.2% 33.3% 88.6%
NA NR NR NR NR NR NR NR NR NR NR NR NR
Flores et al. 200947
United States Retrospective database analysis of prospectively collected data n=398 VATS lobectomy,
VATS versus thoracotomy for lobectomy in stage 1A non-small cell
Peri-operative Median operating time, hours Conversions Post-operative Complications (any)
3:44 ― 30%
3:40 17% 24%
NR NA 0.05

31
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
n=343 thoracotomy, patients were propensity matched
lung cancer (2002–2007)
LoS, days 5-year survival
7 75%
5 79%
<0.0001 0.08
Chen et al. 201448
China Retrospective chart review, n=310 thoracotomy, n=76 VATS
VATS versus thoracotomy for pulmonary aspergilloma (lobectomy ± segmentectomy, bilobectomy, wedge resection, pneumonectomy) (2005–2012)
Peri-operative Median operating time, mins Blood loss, mL Post-operative Median LoS, days Post-operative pain Day 0 Day 1 Day 2 Day 3 Day 7 Day 14 Day 30
151 (85) 128 (73) 14 (12.5) 4.2 5.35 4.76 4.25 4.18 4.0 3.6
138 (76) 118 (80) 10 (6.5) 2.6 3.03 2.8 2.7 2.4 0.95 0.78
0.063 0.06 0.016 NR NR NR NR NR NR NR
Rodgers-Fischl et al. 201749
United States Retrospective chart review, n=48 thoracotomy, n=61 VATS
Open thoracotomy versus VATS lobectomy (2013–2014)
Peri-operative Mean time spent in operating theater, mins Conversions, % Post-operative Post-operative LoS, days ICU LoS, days Arrhythmia, % Pneumothorax, % Infection, % Ventilation, % Infusion, % Pneumonia, %
170.6 ― 5.7 2.1 22.9 56.2 8.3 12.5 12.5 8.3
196.3 15 5.5 2.4 39.3 31.1 11.4 11.4 4.1 4.1
0.06 NA 0.765 0.522 0.106 0.015 0.826 0.870 0.144 0.468

32
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
Returned to OR, % Deep venous thrombosis/pulmonary embolism, %
6.3 2.1
8.2 3.2
0.987 0.705
Casali et al. 200950
United Kingdom
Retrospective single center analysis, n=93 VATS lobectomy, n=253 thoracotomy
Video-assisted thorascopic lobectomy versus open (thoracotomy) lobectomy for early stage lung cancer (2004–2006)
Peri-operative Mean (SD) time in theatre, mins Air leak Surgical emphysema Post-operative Mean (SD) HDU length of stay, days Mean (SD) ward length of stay, days Mean (SD) post-operative hospital stay, days Wound infection Pneumonia/chest infection
140 (42) 8.7% 0.4% 2.21 (0.07) 4.66 (0.17) 6.87 (0.19) 2.0% 15.0%
163 (34) 12.9% 4.3% 1.48 (0.2) 4.06 (0.3) 5.54 (0.37) 1.1% 11.8%
0.00001 NR NR 0.0001 0.0001 0.001 NR NR
Kneuertz et al. 201951
United States Retrospective single center analysis, n=161 VATS lobectomy, n=240 open thoracotomy
Robotic-assisted (not presented) versus video-assisted thoracoscopic surgery versus open lobectomy (2012–2017)
Peri-operative Median (IQR) LoS, days Mean (95% CI) operating room time, mins Any complication, % Major complication, % Pulmonary complication, % Air leak Atelectasis Pleural effusion requiring drainage Pneumonia
5.4 (4.0, 7.6) 278.9 (265.1, 292.8) 55 15 31 9 16 2 8
3.8 (2.8, 7.0) 305.8 (288.7, 323.0) 45 12 31 9 6 3 2
NR NR NR NR NR NR NR NR NR

33
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
ARDS Respiratory failure Pneumothorax Cardiovascular complications, % Atrial fibrillation Infectious complications, % Surgical-site infection Gastrointestinal complications, % Ileus Post-operative Post-operative transfusion, % Return to operating room, % Discharge with chest tube, % ICU stay, % Mean (95% CI) days spent in ICU Mortality (30 days), %
1 8 2 15 10 9 2 4 2 10 4 7 11 6.8 (4.3, 10.8) 2
0 9 1 13 7 10 3 2 1 14 1 9 9 5.0 (3.9, 6.5) 5
NR NR NR NR NR NR NR NR NR NR NR NR NR NR NR
Ramos et al. 201252
France Retrospective single center analysis, n=98 thorascopy, n=189 thoracotomy
Thorascopic versus open lobectomy for stage I non-small cell lung cancer (2007-2009)
Peri-operative Median (IQR) operating time, mins Post-operative Median LoS, days Pneumonia Air leak Transfusion Reoperation
142.0 (40.0) 8.0 9.5% 11.6% 4.2% 2.1%
219.0 (56.5) 7.0 4.1% 6.1% 1.1% 1.0%
<0.001 <0.001 0.100 0.139 0.174 0.665

34
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
Ilonen et al. 201153
Finland Retrospective observational study, n=116 VATS, n=116 thoracotomy, patients were propensity matched for analysis
VATS versus open thoracotomy in stage I NSCLC patients undergoing lobectomy, bilobectomy or segmentectomy (2000–2010)
Post-operative Mean (SD) LoS, days In hospital mortality Complications
10.8 (7.4) 3.4% 26.7%
2.9 (1.7) 2.6% 15.5%
0.001 1 0.026
Handy et al. 201054
United States Retrospective analysis of prospectively collected data, n=49 VATS, n=192 open
VATS versus open lobectomy for non-small cell lung cancer (1998–2007)
Peri-operative Operation time, mins Estimated blood loss, mL Blood transfusion Post-operative In hospital mortality LoS, days Post-op ventilation >48h Pneumonia Reintubation Wound infection Pulmonary embolism Chest tube >5 days Readmission to ICU Post-discharge (6 months) 6-month mortality Readmission to hospital
144 470 24% 2.6% 6.6 4.7% 7.9% 9.4% 1.6% 1.0% 15% 8.9% 8.3% 20% −0.27 29% 36%
152 204 4.2% 4.1% 5.2 2.0% 4.1% 4.1% 2.0% 0.0% 14% 6.1% 4.1% 3.6% −0.49 21% 7.1%
0.29 0.00 0.00 0.58 0.03 0.40 0.36 0.22 0.82 0.47 0.94 0.53 0.31 0.03 0.17 0.43 0.00
35
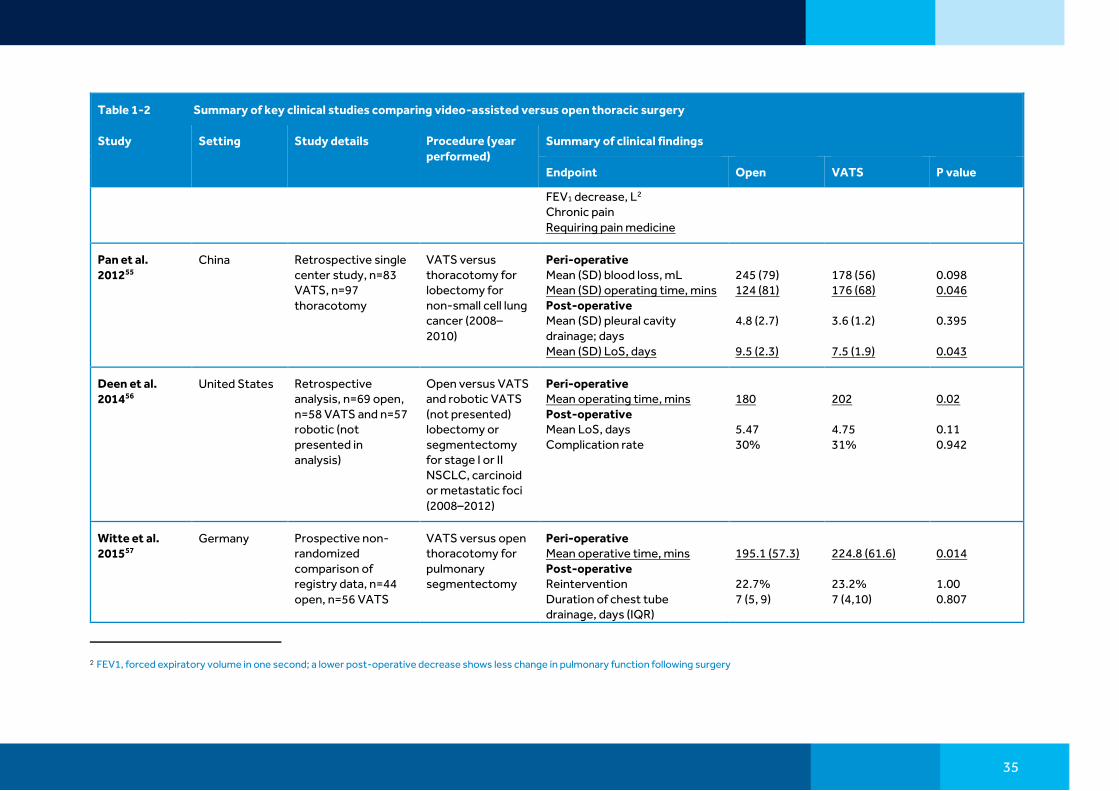
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
FEV1 decrease, L2 Chronic pain Requiring pain medicine
Pan et al. 201255
China Retrospective single center study, n=83 VATS, n=97 thoracotomy
VATS versus thoracotomy for lobectomy for non-small cell lung cancer (2008–2010)
Peri-operative Mean (SD) blood loss, mL Mean (SD) operating time, mins Post-operative Mean (SD) pleural cavity drainage; days Mean (SD) LoS, days
245 (79) 124 (81) 4.8 (2.7) 9.5 (2.3)
178 (56) 176 (68) 3.6 (1.2) 7.5 (1.9)
0.098 0.046 0.395 0.043
Deen et al. 201456
United States Retrospective analysis, n=69 open, n=58 VATS and n=57 robotic (not presented in analysis)
Open versus VATS and robotic VATS (not presented) lobectomy or segmentectomy for stage I or II NSCLC, carcinoid or metastatic foci (2008–2012)
Peri-operative Mean operating time, mins Post-operative Mean LoS, days Complication rate
180 5.47 30%
202 4.75 31%
0.02 0.11 0.942
Witte et al. 201557
Germany Prospective non-randomized comparison of registry data, n=44 open, n=56 VATS
VATS versus open thoracotomy for pulmonary segmentectomy
Peri-operative Mean operative time, mins Post-operative Reintervention Duration of chest tube drainage, days (IQR)
195.1 (57.3) 22.7% 7 (5, 9)
224.8 (61.6) 23.2% 7 (4,10)
0.014 1.00 0.807
2 FEV1, forced expiratory volume in one second; a lower post-operative decrease shows less change in pulmonary function following surgery

36
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
for lung carcinoma (2002–2012)
LoS, days (IQR) Post-discharge 5-year outcomes Overall survival Recurrence-free survival
12 (9, 16) 69.9% 48.6%
9 (7.75, 14) 86% 58.5%
0.034 0.047 0.480
Bu et al. 201258 China Retrospective single center study, n=46 VATS and n=87 thoracotomy included in study
VATS versus thoracotomy for lobectomy for non-small cell lung cancer with tumors >5 cm (2001–2011)
Peri-operative Mean (SD) operating time, mins Mean (SD) blood loss, mL Post-operative Complications Mean (SD) duration of drainage, days Mean (SD) LoS, days Post-discharge Recurrence 3-year survival
256.7 (67.5) 556.9 (187.2) 19.5% 7.5 (6.5) 12.7 (6.8) 3.8% 64.0%
186.5 (62.8) 218.5 (174.6) 8.7% 8.0 (3.5) 11.3 (5.9) 2.4% 69.6%
<0.001 <0.001 0.103 0.508 0.241 0.670 NR
Li et al. 201259 China Retrospective analysis, n=47 thoracotomy, n=29 VATS
Thoracotomy versus VATS lobectomy for NSCLC (2000–2009)
Peri-operative Operating time, mins Blood loss, mL Post-operative Chest drain, days LoS, days
235.0 (214.7–248.6) 400 (126.3–473.1) 7.5 (6.6–8.7) 11.0 (10.6–12.8)
195.0 (150.5–257.0) 200.0 (126.9–473.1) 8.0 (6.7–10.3) 11.0 (9.8–14.5)
0.003 0.002 0.308 0.498
Leshnower et al. 201060
United States Retrospective single center analysis, n=26 thoracotomy (open);
Video-assisted versus open
Peri-operative Mean (SD) operating room time, mins
140 (38)
145 (55)
0.70

37
Table 1-2 Summary of key clinical studies comparing video-assisted versus open thoracic surgery
Study Setting Study details Procedure (year performed)
Summary of clinical findings
Endpoint Open VATS P value
n=15 VATS (thorascopic)
segmentectomy (2002–2009)
Post-operative Mean (SD) chest tube duration, days Mean (SD) LoS, days Mortality Discharge to home
5.2 (3.0) 8.3 (6.1) 8% 85%
2.8 (1.3) 3.5 (1.4) 0 100%
0.001 0.01 0.27 0.63
CID, cumulative incidence of death; CTCAE, common terminology criteria for adverse events; ESTS, European Society of Thoracic Surgeons; EQ5D, European Quality of Life 5 Dimensions; FEV1, forced expiratory volume in 1 second; ICU, intensive care unit; IQR, inter-quartile range; LoS, length of stay: QALY, quality-adjusted life year; VATS, video-assisted thoracic surgery

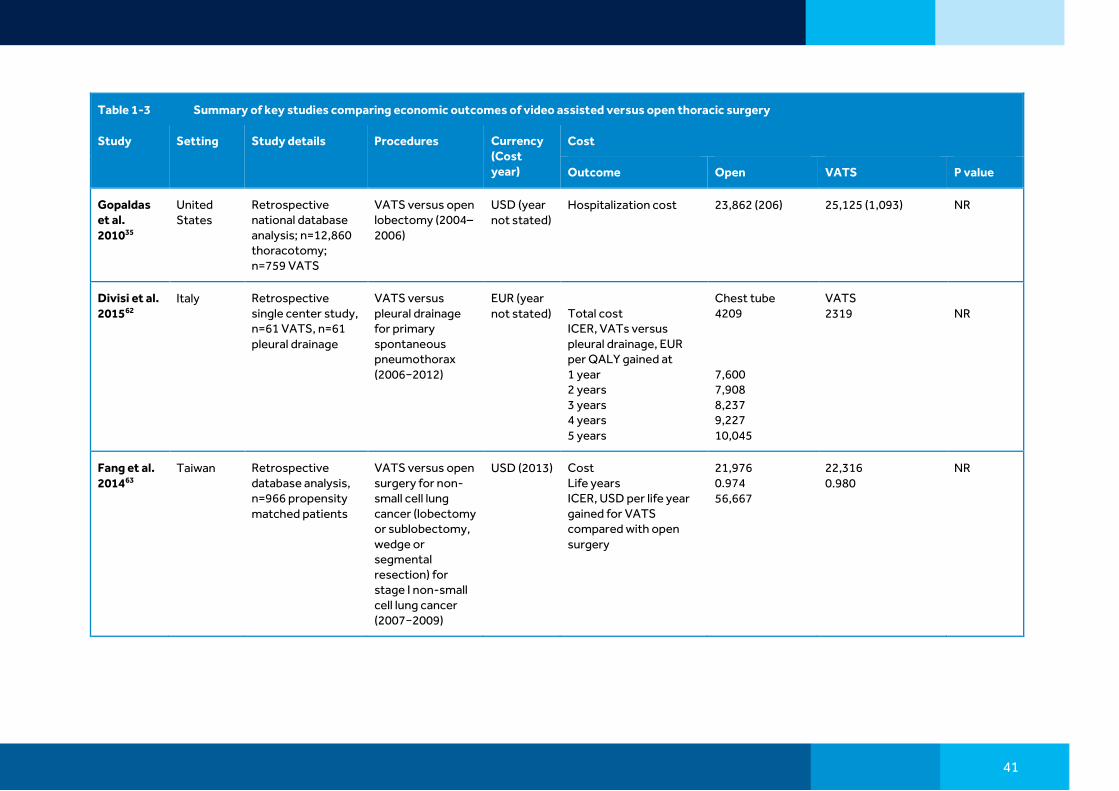
38
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery
Study Setting Study details Procedures Currency (Cost year)
Cost
Outcome Open VATS P value
Ng et al. 201924
Global Meta-analysis of 115 studies
Multiport VATS vs versus open lobectomy for NSCLC
EUR and USD (year not stated)
Mean difference (VATS−Open) in total cost, EUR Mean difference (VATS−Open) in total cost, USD
−155 (−271, −38) −1,951 (−3,171, −731
0.009 0.002
Bendixen et al. 201931
Denmark Retrospective analysis of randomized controlled patient and observer blinded trial, n=99 anterolateral thoracotomy, n=102 four-port VATS
Four-port VATS versus thoracotomy for lobectomy of stage I non-small-cell lung cancer (2008–2014)
DKK and EUR (2018)
General practitioner services and private practicing medical specialists’ services, DKK Prescription medicine, DKK Outpatient clinic, DKK Readmissions, DKR Surgical admission, DKK Total cost, DKK Total cost, EUR
6,757 (4,410) 784 (759) 61,575 (63,209) 51,734 (86,456) 14,095 (15,429) 134,945 (120,963) 18,085
7,544 (5,776) 847 (1,767) 51,415 (51,035) 29,247 (60,548) 14,058 (6,979) 103,108 (90,792) 13,818
0.03 0.52 0.012 <0.001 0.96 <0.001 <0.001
Casali et al. 200950
United Kingdom
Retrospective single center analysis, n=93 VATS lobectomy, n=253 thoracotomy
Video-assisted thorascopic lobectomy versus open (thoracotomy) lobectomy for early stage lung cancer (2004–2006)
EUR (year not stated)
Theater cost HDU stay cost Ward stay cost Total cost
1,280 (54) 2,571 (80) 4,325 (154) 8,178 (167)
2,533 (230) 1,713 (236) 3,776 (281) 8,023 (565)
0.00001 0.00001 0.00001 0.00002

39
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery
Study Setting Study details Procedures Currency (Cost year)
Cost
Outcome Open VATS P value
Kneuertz et al. 201951
United States
Retrospective single center analysis, n=161 VATS lobectomy, n=240 open thoracotomy
Robotic-assisted (not presented) versus video-assisted thoracoscopic surgery versus open lobectomy (2012–2017)
USD (year not stated)
Mean (95% CI) total direct costs Mean (95% CI) total indirect costs Mean (95% CI) operating room costs Mean (95% CI) total charges % of total direct cost, mean (SD) Preoperation Operating room/ ambulatory surgery unit/ postoperative care unit Anesthesia ICU Ward/nursing Pharmacy/blood bank/central supply Laboratory/path Imaging/tests/ interventional radiology Consulting services Physical therapy/ occupational therapy/ speech language
18,075 (16,920, 17308) 16,993 (15,941, 18,115) 8,698 (8,178, 9,218) 120,811 (113,464, 128,634) 2.7 (1.4) 42.2 (12.3) 3.9 (1.2) 1.5 (8.9) 22.7 (9.6) 8.5 (4.5) 9.6 (8.7) 4.3 (1.3) 0.1 (0.2) 4.4 (2.4)
17,260 (15,983, 18,639) 16,415 (15,191, 17,137) 9,491 (8,937, 10,046) 124,026 (115,459, 133,229) 3.1 (2.1) 47.5 (9.6) 4.2 (1.0) 0.0 (0.0) 19.5 (8.6) 7.3 (3.3) 11.7 (7.0) 3.3 (1.2) 0.6 (1.7) 2.7 (2.5)
0.64 0.78 0.10 0.85 NR NR NR NR NR NR NR NR NR NR

40
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery
Study Setting Study details Procedures Currency (Cost year)
Cost
Outcome Open VATS P value
pathology/ respiratory therapy
Leshnower et al. 201060
United States
Retrospective single center analysis, n=26 thoracotomy (open); n=15 VATS (thorascopic)
Video-assisted versus open segmentectomy (2002–2009)
USD (year not stated)
Total cost 46,798 45,101 0.56
Cho et al. 201161
Korea Prospective single center study, n=86 VATS, n=97 open
Video-assisted thoracic surgery (VATS) versus open lobectomy for non-small cell lung cancer (2007–2009)
USD (year not stated)
All patients Total hospital cost Ward stay cost Anesthesia cost Surgical material cost Surgical fee Benefit-service cost Non-benefit-service cost Patients without complications Total hospital cost Ward stay cost Anesthesia cost Surgical material cost Surgical fee Benefit-service cost Non-benefit-service cost
5,593 429 474 1,365 911 4,119 1,144 4,769 327 478 1,306 900 3,639 1,130
5,391 268 435 1,742 910 3,882 1,305 4,684 234 455 1,853 911 3,362 1,322
0.098 0.000 0.193 0.000 0.884 0.139 0.674 0.891 0.000 0.322 0.000 0.796 0.861 0.476
41
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery
Study Setting Study details Procedures Currency (Cost year)
Cost
Outcome Open VATS P value
Gopaldas et al. 201035
United States
Retrospective national database analysis; n=12,860 thoracotomy; n=759 VATS
VATS versus open lobectomy (2004–2006)
USD (year not stated)
Hospitalization cost 23,862 (206) 25,125 (1,093) NR
Divisi et al. 201562
Italy Retrospective single center study, n=61 VATS, n=61 pleural drainage
VATS versus pleural drainage for primary spontaneous pneumothorax (2006−2012)
EUR (year not stated)
Total cost ICER, VATs versus pleural drainage, EUR per QALY gained at 1 year 2 years 3 years 4 years 5 years
Chest tube 4209 7,600 7,908 8,237 9,227 10,045
VATS 2319
NR
Fang et al. 201463
Taiwan Retrospective database analysis, n=966 propensity matched patients
VATS versus open surgery for non-small cell lung cancer (lobectomy or sublobectomy, wedge or segmental resection) for stage I non-small cell lung cancer (2007−2009)
USD (2013) Cost Life years ICER, USD per life year gained for VATS compared with open surgery
21,976 0.974 56,667
22,316 0.980
NR

42
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery
Study Setting Study details Procedures Currency (Cost year)
Cost
Outcome Open VATS P value
Farjah et al. 201434
United States
Retrospective cohort study using the MarketScan database, n=6,893 thoracotomy, n=3,069 VATS
VATS versus open lobectomy for lung cancer (2007−2011)
USD (year not stated)
Mean total 90 day costs Mean Index hospitalization costs Mean 90-day readmission costs Mean 90-day outpatient health care use costs Mean 90-day outpatient pharmacy costs
46,470 37,673 36,845 3,828 713
42,076 35,307 35,550 3,530 672
0.001 0.002 0.772 0.043 0.170
Watson and Qiu 201442
United States
Retrospective database analysis, n=669 open lobectomy, n=270 VATS lobectomy, n=340 open wedge resection, n=1332 VATS wedge resection
Open versus VATS lobectomy and wedge resection (2010)
USD (2010) Lobectomy Mean (95% CI) net payment difference (Open-VATS), Hospital Physician Health care utilization in 90 days Health care expenditure Drug expenditure, Health care utilization in 365 days Health care expenditure Drug expenditure Wedge resection Mean (95% CI) net payment difference (Open-VATS),
3497 433 16,806 746 41,928 2,786
13,546 555 41,106 2,368
0.009 0.01 0.06 0.02 0.85 0.22
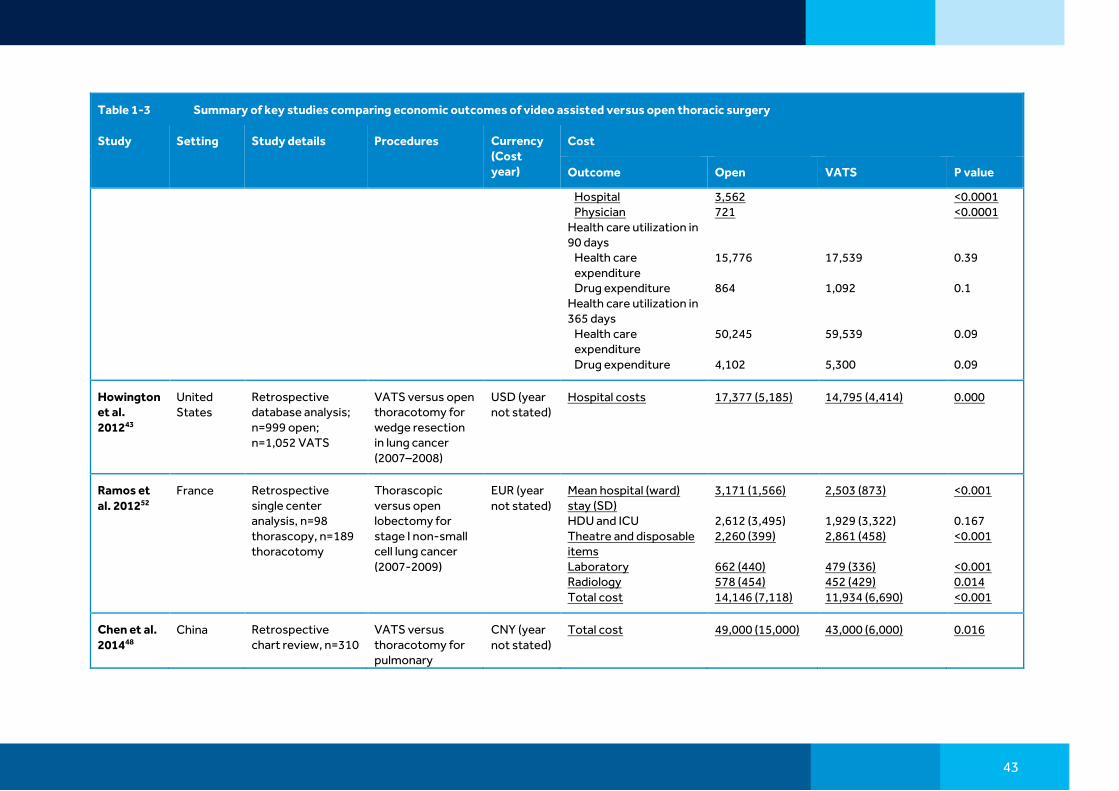
43
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery
Study Setting Study details Procedures Currency (Cost year)
Cost
Outcome Open VATS P value
Hospital Physician Health care utilization in 90 days Health care expenditure Drug expenditure Health care utilization in 365 days Health care expenditure Drug expenditure
3,562 721 15,776 864 50,245 4,102
17,539 1,092 59,539 5,300
<0.0001 <0.0001 0.39 0.1 0.09 0.09
Howington et al. 201243
United States
Retrospective database analysis; n=999 open; n=1,052 VATS
VATS versus open thoracotomy for wedge resection in lung cancer (2007–2008)
USD (year not stated)
Hospital costs 17,377 (5,185) 14,795 (4,414) 0.000
Ramos et al. 201252
France Retrospective single center analysis, n=98 thorascopy, n=189 thoracotomy
Thorascopic versus open lobectomy for stage I non-small cell lung cancer (2007-2009)
EUR (year not stated)
Mean hospital (ward) stay (SD) HDU and ICU Theatre and disposable items Laboratory Radiology Total cost
3,171 (1,566) 2,612 (3,495) 2,260 (399) 662 (440) 578 (454) 14,146 (7,118)
2,503 (873) 1,929 (3,322) 2,861 (458) 479 (336) 452 (429) 11,934 (6,690)
<0.001 0.167 <0.001 <0.001 0.014 <0.001
Chen et al. 201448
China Retrospective chart review, n=310
VATS versus thoracotomy for pulmonary
CNY (year not stated)
Total cost 49,000 (15,000) 43,000 (6,000) 0.016

44
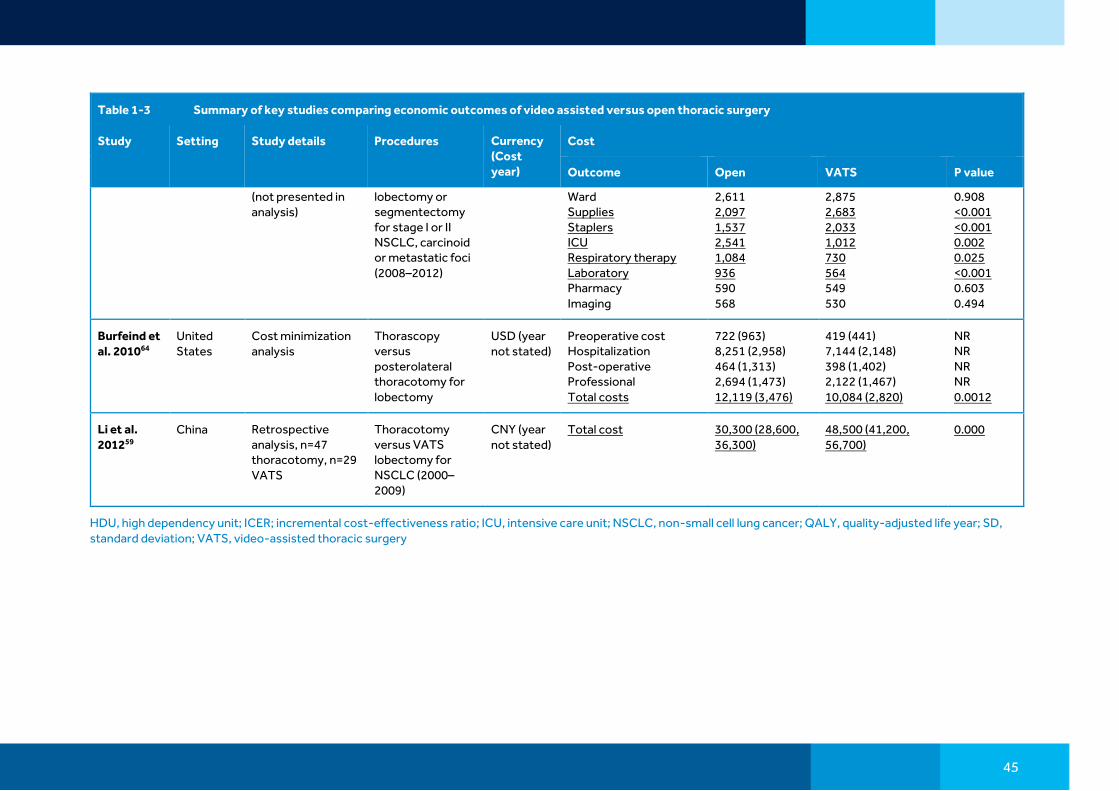
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery
Study Setting Study details Procedures Currency (Cost year)
Cost
Outcome Open VATS P value
thoracotomy, n=76 VATS
aspergilloma (lobectomy ± segmentectomy, bilobectomy, wedge resection, pneumonectomy) (2005–2012)
Rodgers-Fischl et al. 201749
United States
Retrospective chart review, n=48 thoracotomy, n=61 VATS
Open thoracotomy versus VATS lobectomy (2013–2014)
USD (2013–2014)
Cost per procedure 14,004 15,588 0.506
Park et al. 201238
United States
Retrospective database analysis, n=4,769 open, n=1,523 VATS
VATS versus open surgery for pulmonary lobectomy for lung cancer (2008)
USD (year not stated)
Median total cost 20,348 19,656 0.16
Swanson et al. 201241
United States
Retrospective database analysis, n=2,907 open, n=1,054 VATS
Open versus VATS lobectomy performed by a thoracic surgeon (2007–2008)
USD (year not stated)
Adjusted hospital costs (SD)
21,016 (5,645) 20,316 (5,457) 0.027
Deen et al. 201456
United States
Retrospective analysis, n=69 open, n=58 VATS and n=57 robotic
Open versus VATS and robotic VATS (not presented)
USD (year not stated)
Overall cost (cost plus capital depreciation) Procedure cost Operating room
15,036 15,036 4,301
13,829 13,663 4,520
0.227 0.169 0.248
45
Table 1-3 Summary of key studies comparing economic outcomes of video assisted versus open thoracic surgery
Study Setting Study details Procedures Currency (Cost year)
Cost
Outcome Open VATS P value
(not presented in analysis)
lobectomy or segmentectomy for stage I or II NSCLC, carcinoid or metastatic foci (2008–2012)
Ward Supplies Staplers ICU Respiratory therapy Laboratory Pharmacy Imaging
2,611 2,097 1,537 2,541 1,084 936 590 568
2,875 2,683 2,033 1,012 730 564 549 530
0.908 <0.001 <0.001 0.002 0.025 <0.001 0.603 0.494
Burfeind et al. 201064
United States
Cost minimization analysis
Thorascopy versus posterolateral thoracotomy for lobectomy
USD (year not stated)
Preoperative cost Hospitalization Post-operative Professional Total costs
722 (963) 8,251 (2,958) 464 (1,313) 2,694 (1,473) 12,119 (3,476)
419 (441) 7,144 (2,148) 398 (1,402) 2,122 (1,467) 10,084 (2,820)
NR NR NR NR 0.0012
Li et al. 201259
China Retrospective analysis, n=47 thoracotomy, n=29 VATS
Thoracotomy versus VATS lobectomy for NSCLC (2000–2009)
CNY (year not stated)
Total cost 30,300 (28,600, 36,300)
48,500 (41,200, 56,700)
0.000
HDU, high dependency unit; ICER; incremental cost-effectiveness ratio; ICU, intensive care unit; NSCLC, non-small cell lung cancer; QALY, quality-adjusted life year; SD, standard deviation; VATS, video-assisted thoracic surgery

1.3. References
1 Mohiuddin K, Swanson SJ. Maximizing the benefit of minimally invasive surgery. J Surg Oncol. 2013 Oct;108(5):315-9 (PMID: 24037974)
2 Cancer.org What are the key statistics about lung cancer? Available at: http://www.cancer.org/cancer/lungcancer-non-smallcell/detailedguide/non-small-cell-lung-cancer-key-statistics [Last accessed August 26, 2015]
3 European Respiratory Society White Book lung cancer. Available at: http://www.erswhitebook.org/chapters/lung-cancer/ [Last accessed August 26, 2015]
4 Wakeam E, Hyder JA, Lipsitz SR, Darling GE, Finlayson SR. Outcomes and Costs for Major Lung Resection in the United States: Which Patients Benefit Most From High-Volume Referral? Ann Thorac Surg. 2015 Sep;100(3):939-46 (PMID: 26116480)
5 Pischik VG. Technical difficulties and extending the indications for VATS lobectomy. J Thorac Dis. 2014 Oct;6(Suppl 6):S623-30 (PMID: 25379200)
6 Solaini L, Prusciano F, Bagioni P, di Francesco F, Solaini L, Poddie DB. Video-assisted thoracic surgery (VATS) of the lung: analysis of intraoperative and postoperative complications over 15 years and review of the literature. Surg Endosc. 2008 Feb;22(2):298-310 (PMID: 17943372)
7 Nwogu CE, Glinianski M, Demmy TL. Minimally invasive pneumonectomy. Ann Thorac Surg. 2006 Jul;82(1):e3-4 (PMID: 16798175)
8 Predina JD, Kunkala M, Aliperti LA, Singhal AK, Singhal S. Sleeve lobectomy: current indications and future directions. Ann Thorac Cardiovasc Surg. 2010 Oct;16(5):310-8 (PMID: 21030916)
9 Gonzalez-Rivas D, Fieira E, Delgado M, de la Torre M, Mendez L, Fernandez R. Uniportal video-assisted thoracoscopic sleeve lobectomy and other complex resections. J Thorac Dis. 2014 Oct;6(Suppl 6):S674-81 (PMID: 25379210)
10 Postmus PE, Kerr KM, Oudkerk M, Senan S, Waller DA, Vansteenkiste J, Escriu C, Peters S; ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017 Jul 1;28(suppl_4):iv1-iv21 (PMID: 28881918)
11 Downey RJ, Cheng D, Kernstine K, Stanbridge R, Shennib H, Wolf R, Ohtsuka T, Schmid R, Waller D, Fernando H, Yim A, Martin J. Video-Assisted Thoracic Surgery for Lung Cancer Resection: A Consensus Statement of the International Society of Minimally Invasive Cardiothoracic Surgery (ISMICS) 2007. Innovations (Phila). 2007 Nov;2(6):293-302 (PMID: 22437197)
12 Goto T, Kadota Y, Mori T, Yamashita S, Horio H, Nagayasu T, Iwasaki A. Video-assisted thoracic surgery for pneumothorax: republication of a systematic review and a proposal by the guideline committee of the Japanese association for chest surgery 2014. Gen Thorac Cardiovasc Surg. 2015 Jan;63(1):8-13 (PMID: 25182971)
13 Yamashita S, Goto T, Mori T, Horio H, Kadota Y, Nagayasu T, Iwasaki A. Video-assisted thoracic surgery for lung cancer: republication of a systematic review and a proposal by the guidelines committee of the Japanese Association for Chest Surgery 2014. Gen Thorac Cardiovasc Surg. 2014 Dec;62(12):701-5 (PMID: 25182970)
14 Howington JA, Blum MG, Chang AC, Balekian AA, Murthy SC. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American

College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013 May;143(5 Suppl):e278S-313S (PMID: 23649443)
15 Lee HS, Nam B-H, Zo J. Learning curvies for video-assisted thoracic surgery lobectomy in non-small cell lung cancer. Abstract presented at the 89th meeting of the American Association for Thoracic Surgery. 9-13 May 2009, Boston, MA, USA. Available at: http://www.aats.org/annualmeeting/abstracts/2009/15.cgi [Last accessed September 29, 2015]
16 David G, Gunnarsson CL, Moore M, Howington J, Miller DL, Maddaus MA, McKenna RJ Jr, Meyers BF, Swanson SJ. Surgeons' volume-outcome relationship for lobectomies and wedge resections for cancer using video-assisted thoracoscopic techniques. Minim Invasive Surg. 2012;2012:760292 (PMID: 23213500)
17 Zhao H, Bu L, Yang F, Li J, Li Y, Wang J. Video-assisted thoracoscopic surgery lobectomy for lung cancer: the learning curve. World J Surg. 2010 Oct;34(10):2368-72 (PMID: 20567972)
18 Cao C, Tian DH, Wolak K, Oparka J, He J, Dunning J, Walker WS, Yan TD. Cross-sectional survey on lobectomy approach (X-SOLA). Chest. 2014 Aug;146(2):292-8 (PMID: 24504007)
19 Medbery RL, Perez SD, Force SD, Gillespie TW, Pickens A, Miller DL, Fernandez FG. Video-assisted thoracic surgery lobectomy cost variability: implications for a bundled payment era. Ann Thorac Surg. 2014 May;97(5):1686-92 (PMID: 24792254)
20 Hu Y, McMurry TL, Isbell JM, Stukenborg GJ, Kozower BD. Readmission after lung cancer resection is associated with a 6-fold increase in 90-day postoperative mortality. J Thorac Cardiovasc Surg. 2014 Nov;148(5):2261-2267 (PMID: 24823283)
21 Grogan EL, Jones DR. VATS lobectomy is better than open thoracotomy: what is the evidence for short-term outcomes? Thorac Surg Clin. 2008 Aug;18(3):249-58 (PMID: 18831499)
22 Kaseda S, Aoki T, Hangai N, Shimizu K. Better pulmonary function and prognosis with video-assisted thoracic surgery than with thoracotomy. Ann Thorac Surg. 2000 Nov;70(5):1644-6 (PMID: 11093502)
23 Sugiura H, Morikawa T, Kaji M, Sasamura Y, Kondo S, Katoh H. Long-term benefits for the quality of life after video-assisted thoracoscopic lobectomy in patients with lung cancer. Surg Laparosc Endosc Percutan Tech. 1999 Dec;9(6):403-8 (PMID: 10872623)
24 Ng CSH, MacDonald JK, Gilbert S, Khan AZ, Kim YT, Louie BE, Blair Marshall M, Santos RS, Scarci M, Shargal Y, Fernando HC. Optimal approach to lobectomy for non-small cell lung cancer: systemic review and meta-analysis. Innovations (Phila). 2019 APR, 14(2):90-116 (PMID:31039680)
25 Chen FF, Zhang D, Wang YL, Xiong B. Video-assisted thoracoscopic surgery lobectomy versus open lobectomy in patients with clinical stage non-small cell lung cancer: a meta-analysis. Eur J Surg Oncol. 2013 Sep;39(9):957-63 (PMID: 23845704)
26 Yan TD, Black D, Bannon PG, McCaughan BC. Systematic review and meta-analysis of randomized and nonrandomized trials on safety and efficacy of video-assisted thoracic surgery lobectomy for early-stage non-small-cell lung cancer. J Clin Oncol. 2009 May 20;27(15):2553-62 (PMID: 19289625)
27 Cheng D, Downey RJ, Kernstine K, Stanbridge R, Shennib H, Wolf R, Ohtsuka T, Schmid R, Waller D, Fernando H, Yim A, Martin J. Video-assisted thoracic surgery in lung cancer resection: a meta-analysis and systematic review of controlled trials. Innovations (Phila). 2007 Nov;2(6):261-92 (PMID: 22437196)

28 Scott WJ, Allen MS, Darling G, Meyers B, Decker PA, Putnam JB, McKenna RW, Landrenau RJ, Jones DR, Inculet RI, Malthaner RA. Video-assisted thoracic surgery versus open lobectomy for lung cancer: a secondary analysis of data from the American College of Surgeons Oncology Group Z0030 randomized clinical trial. J Thorac Cardiovasc Surg. 2010 Apr;139(4):976-81 (PMID: 20172539)
29 Su S, Scott WJ, Allen MS, Darling GE, Decker PA, McKenna RJ, Meyers BF. Patterns of survival and recurrence after surgical treatment of early stage non-small cell lung carcinoma in the ACOSOG Z0030 (ALLIANCE) trial. J Thorac Cardiovasc Surg. 2014 Feb;147(2):747-52 (PMID: 24290575)
30 Bendixen M, Jørgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. 2016 Jun;17(6):836-44 (PMID: 27160473)
31 Bendixen M, Kronborg C, Jørgensen OD, Andersen C, Licht PB. Cost-utility analysis of minimally invasive surgery for lung cancer: a randomized controlled trial. Eur J Cardiothorac Surg. 2019 Oct;56(4):754-61 (PMID: 30838382)
32 Paul S, Sedrakyan A, Chiu YL, Nasar A, Port JL, Lee PC, Stiles BM, Altorki NK. Outcomes after lobectomy using thoracoscopy vs thoracotomy: a comparative effectiveness analysis utilizing the Nationwide Inpatient Sample database. Eur J Cardiothorac Surg. 2013 Apr;43(4):813-7 (PMID: 22826474)
33 Kent M, Wang T, Whyte R, Curran T, Flores R, Gangadharan S. Open, video-assisted thoracic surgery, and robotic lobectomy: review of a national database. Ann Thorac Surg. 2014 Jan;97(1):236-42 (PMID: 24090577)
34 Farjah F, Backhus LM, Varghese TK, Mulligan MS, Cheng AM, Alfonso-Cristancho R, Flum DR, Wood DE. Ninety-day costs of video-assisted thoracic surgery versus open lobectomy for lung cancer. Ann Thorac Surg. 2014 Jul;98(1):191-6 (PMID: 24820393)
35 Gopaldas RR, Bakaeen FG, Dao TK, Walsh GL, Swisher SG, Chu D. Video-assisted thoracoscopic versus open thoracotomy lobectomy in a cohort of 13,619 patients. Ann Thorac Surg. 2010 May;89(5):1563-70 (PMID: 20417778)
36 Yang CJ, Kuman A, Klapper JA, Hartwig MG, Tong BC, Harpole DH Jr, Berry MF, D’Amico TA. A national analysis of long-term survival following thorascopic versus open lobectomy for stage I non-small-cell lung cancer. Ann Surg. 2019 Jan;269(1):163-71 (PMID: 28799982)
37 Paul S, Altorki NK, Sheng S, Lee PC, Harpole DH, Onaitis MW, Stiles BM, Port JL, D'Amico TA. Thoracoscopic lobectomy is associated with lower morbidity than open lobectomy: a propensity-matched analysis from the STS database. J Thorac Cardiovasc Surg. 2010 Feb;139(2):366-78 (PMID: 20106398)
38 Park HS, Detterbeck FC, Boffa DJ, Kim AW. Impact of hospital volume of thoracoscopic lobectomy on primary lung cancer outcomes. Ann Thorac Surg. 2012 Feb;93(2):372-9 (PMID: 21945225)
39 Paul S, Isaacs AJ, Treasure T, Altorki NK, Sedrakyan A. Long term survival with thoracoscopic versus open lobectomy: propensity matched comparative analysis using SEER-Medicare database. BMJ. 2014 Oct 2;349:g5575 (PMID: 25277994)
40 Falcoz PE, Puyraveau M, Thomas PA, Decaluwe H, Hürtgen M, Petersen RH, Hansen H, Brunelli A; ESTS Database Committee and ESTS Minimally Invasive Interest Group. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: a propensity-matched analysis of outcome from the European Society of Thoracic

Surgeon database. Eur J Cardiothorac Surg. 2015 Apr 26. pii: ezv154. [Epub ahead of print] (PMID: 25913824)
41 Swanson SJ, Meyers BF, Gunnarsson CL, Moore M, Howington JA, Maddaus MA, McKenna RJ, Miller DL. Video-assisted thoracoscopic lobectomy is less costly and morbid than open lobectomy: a retrospective multiinstitutional database analysis. Ann Thorac Surg. 2012 Apr;93(4):1027-32 (PMID: 22130269)
42 Watson TJ, Qui J. The impact of thoracoscopic surgery on payment and health care utilization after lung resection. Ann Thorac Surg. 2016 Apr;101(4):1271-9 (PMID:26872730)
43 Howington JA, Gunnarsson CL, Maddaus MA, McKenna RJ, Meyers BF, Miller D, Moore M, Rizzo JA, Swanson S. In-hospital clinical and economic consequences of pulmonary wedge resections for cancer using video-assisted thoracoscopic techniques vs traditional open resections: a retrospective database analysis. Chest. 2012 Feb;141(2):429-35 (PMID: 21778260)
44 Laursen LØ, Petersen RH, Hansen HJ, Jensen TK, Ravn J, Konge L. Video-assisted thoracoscopic surgery lobectomy for lung cancer is associated with a lower 30-day morbidity compared with lobectomy by thoracotomy. Eur J Cardiothorac Surg. 2015 Jun 18. pii: ezv205. [Epub ahead of print] (PMID: 26088592)
45 Villamizar NR, Darrabie MD, Burfeind WR, Petersen RP, Onaitis MW, Toloza E, Harpole DH, D'Amico TA. Thoracoscopic lobectomy is associated with lower morbidity compared with thoracotomy. J Thorac Cardiovasc Surg. 2009 Aug;138(2):419-25 (PMID: 19619789)
46 Yang X, Wang S, Qu J. Video-assisted thoracic surgery (VATS) compares favorably with thoracotomy for the treatment of lung cancer: a five-year outcome comparison. World J Surg. 2009 Sep;33(9):1857-61 (PMID: 19626361)
47 Flores RM, Park BJ, Dycoco J, Aronova A, Hirth Y, Rizk NP, Bains M, Downey RJ, Rusch VW. Lobectomy by video-assisted thoracic surgery (VATS) versus thoracotomy for lung cancer. J Thorac Cardiovasc Surg. 2009 Jul;138(1):11-8 (PMID: 19577048)
48 Chen QK, Chen C, Chen XF, Jiang GN. Video-assisted thoracic surgery for pulmonary aspergilloma: a safe and effective procedure. Ann Thorac Surg. 2014 Jan;97(1):218-23 (PMID: 24094518)
49 Rodgers-Fischl PM, Martin JT, Saha SP. Video-Assisted Thoracoscopic versus Open Lobectomy: Costs and Outcomes. South Med J. 2017 Mar;110(3):229-33 (PMID: 28257551)
50 Casali G, Walker WS. Video-assisted thoracic surgery lobectomy: can we afford it? Eur J Cardiothorac Surg. 2009 Mar;35(3):423-8 (PMID: 19136272)
51 Kneuertz PJ, Singer E, D'Souza DM, Abdel-Rasoul M, Moffatt-Bruce SD, Merritt RE. Hospital cost and clinical effectiveness of robotic-assisted versus video-assisted thoracoscopic and open lobectomy: A propensity score-weighted comparison. J Thorac Cardiovasc Surg. 2019 May;157(5):2018-2026.e2. (PMID:30819575)
52 Ramos R, Masuet C, Gossot D. Lobectomy for early-stage lung carcinoma: a cost analysis of full thoracoscopy versus posterolateral thoracotomy. Surg Endosc. 2012 Feb;26(2):431-7 (PMID: 21898011)
53 Ilonen IK, Räsänen JV, Knuuttila A, Salo JA, Sihvo EI. Anatomic thoracoscopic lung resection for non-small cell lung cancer in stage I is associated with less morbidity and shorter hospitalization than thoracotomy. Acta Oncol. 2011 Oct;50(7):1126-32 (PMID: 21314296)

54 Handy JR Jr, Asaph JW, Douville EC, Ott GY, Grunkemeier GL, Wu Y. Does video-assisted thoracoscopic lobectomy for lung cancer provide improved functional outcomes compared with open lobectomy? Eur J Cardiothorac Surg. 2010 Feb;37(2):451-5 (PMID: 19747837)
55 Pan TW, Wu B, Xu ZF, Zhao XW, Zhong L. Video-assisted thoracic surgery versus thoracotomy for non-small-cell lung cancer. Asian Pac J Cancer Prev. 2012;13(2):447-50 (PMID: 22524804)
56 Deen SA, Wilson JL, Wilshire CL, Vallières E, Farivar AS, Aye RW, Ely RE, Louie BE. Defining the cost of care for lobectomy and segmentectomy: a comparison of open, video-assisted thoracoscopic, and robotic approaches. Ann Thorac Surg. 2014 Mar;97(3):1000-7 (PMID: 24480259)
57 Witte B, Stenz C, Vahl CF, Huertgen M. Comparative intention-to-treat analysis of the video-assisted thoracoscopic surgery approach to pulmonary segmentectomy for lung carcinoma‡. Interact Cardiovasc Thorac Surg. 2015 Jun 10. pii: ivv143. [Epub ahead of print] (PMID: 26063694)
58 Bu L, Li Y, Yang F, Zhao H, Jiang GC, Li JF, Liu J, Wang J. Completely video-assisted thoracoscopic lobectomy versus open lobectomy for non-small cell lung cancer greater than 5 cm: a retrospective study. Chin Med J (Engl). 2012 Feb;125(3):434-9 (PMID: 22490398)
59 Li Y, Wang J. Comparison of clinical outcomes for patients with clinical N0 and pathologic N2 non-small cell lung cancer after thoracoscopic lobectomy and open lobectomy: a retrospective analysis of 76 patients. J Surg Oncol. 2012 Sep 15;106(4):431-5 (PMID: 22442010)
60 Leshnower BG, Miller DL, Fernandez FG, Pickens A, Force SD. Video-assisted thoracoscopic surgery segmentectomy: a safe and effective procedure. Ann Thorac Surg. 2010 May;89(5):1571-6 (PMID: 20417779)
61 Cho S, Do YW, Lee EB. Comparison of costs for video-assisted thoracic surgery lobectomy and open lobectomy for non-small cell lung cancer. Surg Endosc. 2011 Apr;25(4):1054-61 (PMID: 20835729)
62 Divisi D, Di Leonardo G, Crisci R. Video-assisted thoracic surgery versus pleural drainage in the management of the first episode of primary spontaneous pneumothorax. Am J Surg. 2015 Jul;210(1):68-73 (PMID: 25769881)
63 Fang HY, Hsiao FY, Huang HC, Lin YS, Chen CY, Shieh SH, Chen PR, Chen CK, Chien CR. Cost and effectiveness of video-assisted thoracoscopic surgery for clinical stage I non-small cell lung cancer: a population-based analysis. J Thorac Dis. 2014 Dec;6(12):1690-6 (PMID: 25589961)
64 Burfeind WR Jr, Jaik NP, Villamizar N, Toloza EM, Harpole DH Jr, D'Amico TA. A cost-minimisation analysis of lobectomy: thoracoscopic versus posterolateral thoracotomy. Eur J Cardiothorac Surg. 2010 Apr;37(4):827-32 (PMID: 19939695)
©2020 Medtronic. All rights reserved. Medtronic, Medtronic logo and Further, Together are trademarks of Medtronic. All other brands are trademarks of a Medtronic company. 3/2020 US160336(2)

















