Glossectomy as an adjunct to correct an open-bite malocclusion with shortened maxillary central incisor roots Orlando Motohiro Tanaka, a Odilon Guariza-Filho, b Jo~ ao Luiz Carlini, c Dauro Douglas Oliveira, d Matheus Mello Pithon, e and Elisa Souza Camargo f Curitiba, Parana, Belo Horizonte, Minas Gerais, and Jequie, Bahia, Brazil, and St Louis, Mo A young man, 19 years of age, with the chief complaint of an anterior open bite, came for orthodontic treatment with a skeletal Class I relationship, anterior open bite, shortened maxillary incisor roots, and relative macroglossia. The malocclusion was treated by extracting the maxillary first premolars and using a fixed edgewise appliance. A partial glossectomy was performed before the orthognathic surgery with a 3-piece segmental LeFort I mandibular setback, and advancement was achieved with a reduction genioplasty. A functional and esthetic occlusion with an improved facial profile was established, and the apex of the maxillary left central incisor became slightly rounded after prolonged and significant tooth movement. Four years after treatment, there was occlusal stability of the results, and no further root shortening was observed. (Am J Orthod Dentofacial Orthop 2013;144:130-40) I t is well accepted that tongue size and position affect skeletal and dental components. 1 Macroglossia, or enlarged tongue, is thought to be an etiologic factor in open bite, bimaxillary protrusion, and dental arch spacing, and it might cause instability after orthodontic treatment. A partial glossectomy to reduce tongue size can be useful in treating these problems. 1 Understand- ing the signs and symptoms of macroglossia will help to identify patients who could benefit from a reduction glossectomy to improve function, esthetics, and treatment stability. 2 True macroglossia occurs when the tongue size is truly abnormal, caused by either congenital or acquired factors, or when histologic abnormalities correlate with the clinical findings of tongue enlargement. 2 Vascular malformations, muscular enlargement, and tumors are the most common forms of true macroglossia. 3 Pseudomacroglossia, or relative macroglossia, is a condition in which the tongue can be normal in size but appears large relative to its anatomic interrelationships 2 and includes cases of apparent tongue enlargement in which the histology does not provide a pathologic explanation. 3 There is no practical method of measuring tongue size, and it is sometimes difficult to evaluate the degree to which macroglossia is implicated in a malocclusion. 4 Therefore, a clinical understanding of the signs and symptoms of macroglossia are important when planning orthodontic treatment and in predicting posttreatment stability. Tongue size should be judged by clinical appearance based on a discrepancy between the size of the tongue and that of the oral cavity. 5 Macroglossia can also cause diastemas in the mandib- ular arch. 6 This article describes the treatment of a patient with an anterior open bite and shortened maxillary central a Professor, graduate Dentistry Program in Orthodontics, School of Health and Bio- sciences, Pontifical Catholic University of Parana, Curitiba, Parana, Brazil; postdoc- toral fellow, Center for Advanced Dental Education, Saint Louis University, St Louis, Mo. b Senior professor, graduate Dentistry Program in Orthodontics, Pontifical Catholic University of Parana, Curitiba, Parana, Brazil. c Adjunct professor and staff of Service of Oral and Maxillofacial Surgery of the Cleft Palate Center of Parana, Federal University of Parana, Curitiba, Parana, Brazil. d Program director, Department of Orthodontics, Pontifical Catholic University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil. e Professor, Department of Orthodontics, Southwest Bahia State University, Jequi e, Bahia, Brazil. f Associate professor, graduate Dentistry Program in Orthodontics, Pontifical Cath- olic University of Parana, Curitiba, Parana, Brazil. All authors have completed and submitted the ICMJE Form for Disclosure of Po- tential Conflicts of Interest and none were reported. Reprint requests to: Orlando Motohiro Tanaka, Graduate Dentistry Program, Orthodontics, PUCPR, Bolsista da CAPES, Proc. No BEX 1632/11-6, R. Imaculada Conceic ¸ ~ ao, 1155, CEP 80215-901, Curitiba, Parana, Brazil; e-mail, [email protected]. Submitted, July 2012; revised and accepted, August 2012. 0889-5406/$36.00 Copyright Ó 2013 by the American Association of Orthodontists. http://dx.doi.org/10.1016/j.ajodo.2012.08.029 130 CASE REPORT
Transcript
CASE REPORT
Glossectomy as an adjunct to correct anopen-bite malocclusion with shortenedmaxillary central incisor roots
A young man, 19 years of age, with the chief complaint of an anterior open bite, came for orthodontictreatment with a skeletal Class I relationship, anterior open bite, shortened maxillary incisor roots, and relativemacroglossia. The malocclusion was treated by extracting the maxillary first premolars and using a fixededgewise appliance. A partial glossectomy was performed before the orthognathic surgery with a 3-piecesegmental LeFort I mandibular setback, and advancement was achieved with a reduction genioplasty.A functional and esthetic occlusion with an improved facial profile was established, and the apex of themaxillary left central incisor became slightly rounded after prolonged and significant tooth movement.Four years after treatment, there was occlusal stability of the results, and no further root shortening wasobserved. (Am J Orthod Dentofacial Orthop 2013;144:130-40)
It is well accepted that tongue size and position affectskeletal and dental components.1 Macroglossia, orenlarged tongue, is thought to be an etiologic factor
in open bite, bimaxillary protrusion, and dental archspacing, and it might cause instability after orthodontictreatment. A partial glossectomy to reduce tongue sizecan be useful in treating these problems.1 Understand-ing the signs and symptoms of macroglossia will help
ssor, graduate Dentistry Program in Orthodontics, School of Health and Bio-es, Pontifical Catholic University of Paran�a, Curitiba, Paran�a, Brazil; postdoc-fellow, Center for Advanced Dental Education, Saint Louis University,is, Mo.r professor, graduate Dentistry Program in Orthodontics, Pontifical Catholicrsity of Paran�a, Curitiba, Paran�a, Brazil.nct professor and staff of Service of Oral andMaxillofacial Surgery of the CleftCenter of Paran�a, Federal University of Paran�a, Curitiba, Paran�a, Brazil.ram director, Department of Orthodontics, Pontifical Catholic University ofGerais, Belo Horizonte, Minas Gerais, Brazil.ssor, Department of Orthodontics, Southwest Bahia State University, Jequi�e,, Brazil.iate professor, graduate Dentistry Program in Orthodontics, Pontifical Cath-niversity of Paran�a, Curitiba, Paran�a, Brazil.thors have completed and submitted the ICMJE Form for Disclosure of Po-l Conflicts of Interest and none were reported.t requests to: Orlando Motohiro Tanaka, Graduate Dentistry Program,dontics, PUCPR, Bolsista da CAPES, Proc. No BEX 1632/11-6, R.lada Conceic~ao, 1155, CEP 80215-901, Curitiba, Paran�a, Brazil; e-mail,[email protected], July 2012; revised and accepted, August 2012.5406/$36.00ight � 2013 by the American Association of Orthodontists./dx.doi.org/10.1016/j.ajodo.2012.08.029
to identify patients who could benefit from a reductionglossectomy to improve function, esthetics, andtreatment stability.2
True macroglossia occurs when the tongue size istruly abnormal, caused by either congenital or acquiredfactors, or when histologic abnormalities correlate withthe clinical findings of tongue enlargement.2 Vascularmalformations, muscular enlargement, and tumorsare the most common forms of true macroglossia.3
Pseudomacroglossia, or relative macroglossia, isa condition in which the tongue can be normal in size butappears large relative to its anatomic interrelationships2
and includes cases of apparent tongue enlargementin which the histology does not provide a pathologicexplanation.3
There is no practical method of measuring tonguesize, and it is sometimes difficult to evaluate the degreeto which macroglossia is implicated in a malocclusion.4
Therefore, a clinical understanding of the signsand symptoms of macroglossia are important whenplanning orthodontic treatment and in predictingposttreatment stability. Tongue size should be judgedby clinical appearance based on a discrepancy betweenthe size of the tongue and that of the oral cavity.5
Macroglossia can also cause diastemas in the mandib-ular arch.6
This article describes the treatment of a patient withan anterior open bite and shortened maxillary central
Fig 1. Pretreatment facial and intraoral photographs: Angle Class I malocclusion with anterior openbite, maxillary midline deviation, and posturing of the tongue between the anterior teeth.
Tanaka et al 131
incisor roots associated with relative macroglossia; hewas treated with a partial glossectomy beforeorthognathic surgery. The long-term results are shown4 years after appliance removal.
DIAGNOSIS AND ETIOLOGY
The patient was a 19-year-old man who came fororthodontic treatment with the chief complaint of aninability to bite on his front teeth. He had a long lowerfacial height, lack of lip seal, and slight facial asymme-try with the left side more rounded than the right. Hehad an Angle Class I malocclusion, anterior open bite,and occlusal contact only in the premolar and molarareas, with the maxillary midline shifted to the right.He had chronic posturing of the tongue between theanterior teeth (Figs 1 and 2). The panoramic andperiapical radiographs showed shortened roots ofboth maxillary central incisors (Fig 3). The lateralcephalometric radiograph showed marked verticaldiscrepancy between the 2 jaws (FMA, 34�), skeletal
American Journal of Orthodontics and Dentofacial Orthoped
Class I (ANB, 1�), proclined maxillary incisors(1.NA, 35�), and good mandibular incisor positioning(1.NB, 25�) (Fig 4, Table).
TREATMENT OBJECTIVES AND PLAN
The treatment goals were to (1) correct the openbite, (2) reduce the dental protrusion, (3) improve lipfunction, (4) reduce the size of the tongue for greaterstability and appropriate function, (5) achieve better fa-cial balance, and (6) maintain the root length.
The treatment consisted of extraction of themaxillary first premolars; alignment, leveling, andstraightening the maxillary incisors; and surgery withmaxillary posterior impaction by LeFort I osteotomy,mandibular setback, and reduction genioplasty. Inthe mandible, interproximal enamel reduction wasperformed. Before the orthodontic treatment, thepatient and his parents were informed of the risk offurther root shortening and possible loss of toothstability.
ics July 2013 � Vol 144 � Issue 1
Fig 2. Pretreatment dental casts.
Fig 3. Pretreatment panoramic and periapical radiographs.
132 Tanaka et al
TREATMENT ALTERNATIVES
Because of the severity of this patient's malocclu-sion, a combination of orthodontic treatment andsurgery was proposed as a favorable treatment optionto achieve realistic treatment objectives, as suggestedby Kokich.7 The second suggested option was toattempt to treat without surgery with molar intrusionusing titanium screw anchorage to level and achievenormal overjet and overbite.8 When both optionswere discussed, the patient was explicitly told that itwould be necessary to reduce the tongue size thatwas associated with the open bite, and that would beimportant for posttreatment stability. After discussing
July 2013 � Vol 144 � Issue 1 American
the treatment options, the patient and his parentschose the partial glossectomy before surgery, with thepotential risks and complications associated with theprocedure.
TREATMENT PROGRESS
The maxillary premolar extraction spaces were closedusing a fixed standard (0.0223 0.028-in) edgewise ap-pliance, but the anterior open bite began to worsen.Therefore, we decided to reopen andmaintain the spacesbetween the canines and the second premolars tofacilitate a 3-piece maxillary LeFort I osteotomy withoutdamaging the roots (Fig 5).
Journal of Orthodontics and Dentofacial Orthopedics
Fig 4. Pretreatment cephalometric radiograph and tracing.
Table. Cephalometric measurements
Measurement Pretreatment PosttreatmentRetention(4 y 2 mo)
Surgical-orthodontic correction of this patient'scondition was undertaken in 2 stages. The initialstage involved bonding and banding of both archeswith edgewise orthodontic appliances. After themaxillary and mandibular arches were partiallyleveled and aligned, a partial glossectomy wasperformed to reduce the tongue size (Fig 6). Theroot morphology of the maxillary incisors wassatisfactory.
American Journal of Orthodontics and Dentofacial Orthoped
The surgical techniques available for tonguereduction are well known, and the results are acceptablefrom both functional and esthetic standpoints.5,9,10
Surgical reduction of tongue size and volume wasperformed 13 months before the orthognathic surgeryusing the keyhole-shaped technique (Fig 6).10,11 Aftersurgery, the patient was treated with antibiotics andanti-inflammatory medication and advised to consumeonly liquids for the first 3 days and a soft diet until thetenth day after surgery. There were no postoperativecomplications such as excessive swelling, infection,bleeding, or difficulties in phonation except for the2 weeks after surgery. Within 4 weeks after the surgery,the patient was able to speak, but with some limitations.
Coordination of the orthodontic arches was com-pleted during the orthognathic surgery; the dentofacialcorrection consisted of a LeFort I, 3-segment maxillaryosteotomy with a 5-mm impaction in the molar areaand a 4-mm advancement. Buccal root torque wasused to reposition the incisors by less than 4 mm, anda 4-mm transverse expansion was achieved. The promi-nence of the upper lip decreased, and lip competencewas achieved. Furthermore, plication of the base of thenose was performed to reduce the enlargement of thenasal base. A V-Y closure of the upper lip was performedto enhance the exposure of the upper lip vermilion.
The mandible was simultaneously repositionedwith bilateral sagittal ramus osteotomies to achieve
ics July 2013 � Vol 144 � Issue 1
Fig 5. Progress records: reopening of the space between the canines and the second premolars.
Fig 6. Glossectomy: a keyhole-shaped technique was used to decrease the width and length of thetongue. The 2 sides were sutured together in a straight line.
134 Tanaka et al
maxillomandibular harmony and a Class I canineocclusion, and to compensate for the autorotationaladvancement of the mandible.
A 6-mm advancement genioplasty increased the chinprominence, and a 5-mm reduction decreased the loweranterior facial height. The postoperative radiographshowed a significant modification of the occlusal planein the anterior portion of the arch (Fig 7). The occlusionwas markedly improved after surgery because of thecorrected open bite.
TREATMENT RESULTS
Postsurgical orthodontic treatment achieved thefinal alignment and intercuspation of the teeth. AClass I canine relationship with a satisfactory overbiteand overjet was accomplished with maxillary andmandibular osteotomies, genioplasty, and orthodontictreatment. The treatment time was 47 months. From
July 2013 � Vol 144 � Issue 1 American
a functional and esthetic perspective, the final resultswere good. The left premolar would ideally be seatedinto the embrasure of both mandibular premolars, butthe patient asked for the appliance to be removed(Fig 8). The deviation from the original treatment planresulted in a somewhat longer treatment time. Theapex of the maxillary left central incisor root wasresorbed slightly (Fig 9).
At the end of treatment, the reduction of the openbite resulted in decreased anterior face height(FMA, 28�; y-axis, 63�), reduced dental protrusion(1.NA, 23�), uprighting of the mandibular incisor(1.NB, 17�), improved facial balance (z-angle, 80�)(Fig 10, Table), and a decreased size of the tongue.The patient had no complaints or functional impair-ments after the procedure.
At the 4 years 2 month follow-up, we observeda slight change in the positioning of the right maxillary
Journal of Orthodontics and Dentofacial Orthopedics
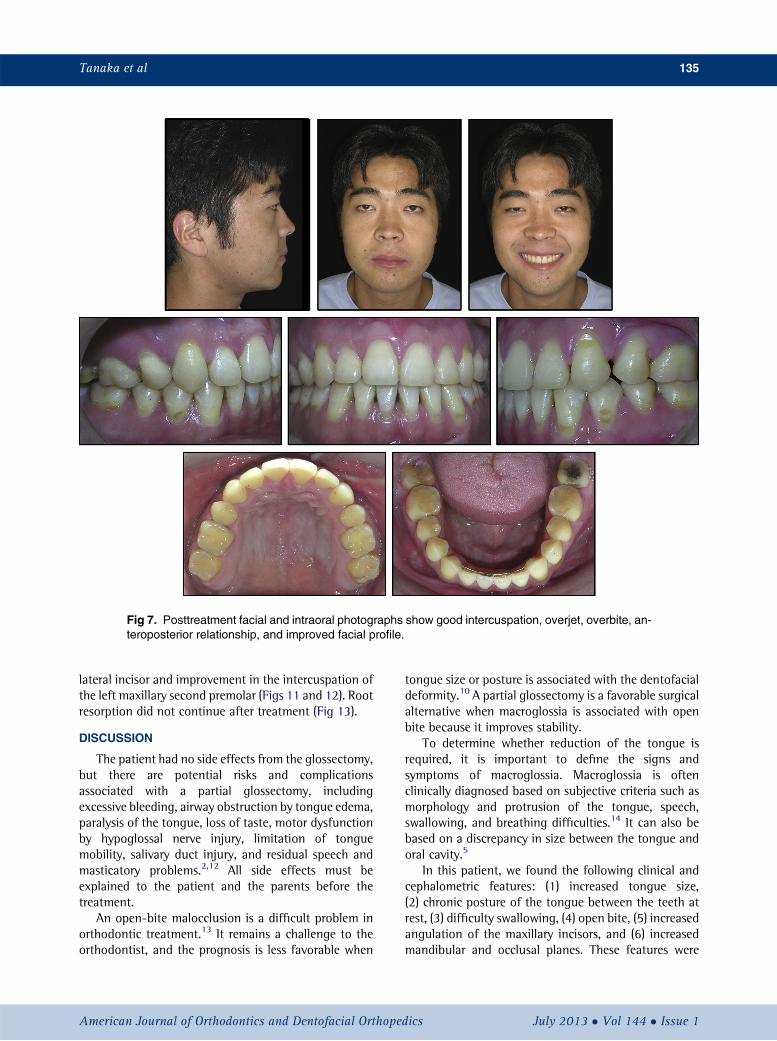
Fig 7. Posttreatment facial and intraoral photographs show good intercuspation, overjet, overbite, an-teroposterior relationship, and improved facial profile.
Tanaka et al 135
lateral incisor and improvement in the intercuspation ofthe left maxillary second premolar (Figs 11 and 12). Rootresorption did not continue after treatment (Fig 13).
DISCUSSION
The patient had no side effects from the glossectomy,but there are potential risks and complicationsassociated with a partial glossectomy, includingexcessive bleeding, airway obstruction by tongue edema,paralysis of the tongue, loss of taste, motor dysfunctionby hypoglossal nerve injury, limitation of tonguemobility, salivary duct injury, and residual speech andmasticatory problems.2,12 All side effects must beexplained to the patient and the parents before thetreatment.
An open-bite malocclusion is a difficult problem inorthodontic treatment.13 It remains a challenge to theorthodontist, and the prognosis is less favorable when
American Journal of Orthodontics and Dentofacial Orthoped
tongue size or posture is associated with the dentofacialdeformity.10 A partial glossectomy is a favorable surgicalalternative when macroglossia is associated with openbite because it improves stability.
To determine whether reduction of the tongue isrequired, it is important to define the signs andsymptoms of macroglossia. Macroglossia is oftenclinically diagnosed based on subjective criteria such asmorphology and protrusion of the tongue, speech,swallowing, and breathing difficulties.14 It can also bebased on a discrepancy in size between the tongue andoral cavity.5
In this patient, we found the following clinical andcephalometric features: (1) increased tongue size,(2) chronic posture of the tongue between the teeth atrest, (3) difficulty swallowing, (4) open bite, (5) increasedangulation of the maxillary incisors, and (6) increasedmandibular and occlusal planes. These features were
ics July 2013 � Vol 144 � Issue 1
Fig 8. Posttreatment dental casts.
Fig 9. Posttreatment radiographs: maxillary and mandibular osteotomies and genioplasty.
136 Tanaka et al
described by Wolford and Cottrell,2 among others,and might help the clinician identify the presence orabsence of macroglossia. However, not all of thesefeatures are always present, and their existence is notnecessarily a pathognomonic factor for the diagnosisof macroglossia.
After assessing the real need for tongue reductionsurgery, the surgery can be performed before, after, orduring the orthognathic surgery.2 Because the maxillaand mandible would be fixed with plates and screws, itwas considered safer to perform the partial glossectomy
July 2013 � Vol 144 � Issue 1 American
during the osteotomies. However, the glossectomy wasperformed 13 months before the orthognathic surgeryto prevent significant edema and respiratory problemsthat can occur when both procedures are done at thesame time.10
The keyhole-shaped technique was used for thepartial glossectomy. This excision offers a flexible modelto strengthen and shorten the tongue as needed.15-17
The glossectomy caused no complications, such asextensive edema, infection, or bleeding. The patientexperienced difficulty in speaking for 14 days after
Journal of Orthodontics and Dentofacial Orthopedics
Fig 10. Cephalometric radiograph and superimposition show a decreased lower facial third; the apexof the maxillary left central incisor became slightly rounded.
Tanaka et al 137
surgery. After 4 weeks, the function of the tongue wasrestored, but with limited movement.
The keyhole-shaped technique is the mostcommon type of partial glossectomy because itresults in a decrease in the total volume of the tongue(length, thickness) and is performed under generalanesthesia. The technique requires control of bleedingduring the surgery to prevent bruising and severeswelling. Hospitalization time is 1 day. The discom-fort is associated with difficulty in speech andswallowing, requiring a soft diet for 1 week. A changein taste sensation occurs in the first month becausethere is a change in the filiform papillae, and speechtherapy is recommended to restore the ability tospeak.
Austermann and Machtens18 considered tongueposture more important than size. The patient had anabnormal resting posture that affected the alignmentand leveling stage of opening of the anterior bite,possibly contributing to increasing the curve of Speeand opening of the bite. This finding might be relevantin diagnosing tongue interposition and interference,and it affects the surgical procedure. For example,a 3-piece segmental LeFort I surgical procedure mightbe preferable to a 1-piece LeFort I procedure.
Although there are few indications for surgicallyreducing tongue size when true macroglossia is notpresent, the procedure might be desirable in patients
American Journal of Orthodontics and Dentofacial Orthoped
with relative macroglossia who have been treatedclinically without success10 because open bites treatedwith LeFort I osteotomies exhibit a significant posttreat-ment relapse.19
Patients with anterior open bites can have dimin-ished root lengths, high incidences of root bluntingand periapical resorption, and root resorption beforeorthodontic treatment; they are therefore at risk ofexperiencing loss of root structure.20 In this patient,there was a potential risk for significant shortening ofthe maxillary central incisor roots. However, there wasno further shortening after prolonged and significanttooth movement, and even patients with severelyresorbed roots have experienced successful long-termoutcomes.14,21
At 4 years 2 months posttreatment, a good occlu-sion was maintained, and the partial glossectomymight be an important component of treatment fora patient with a malocclusion caused by an enlargedtongue because it contributes to the stability of theocclusion,1 and the incidence of relapse is less whenreduction of tongue size is combined with orthodontictreatment.4 This patient with an open-bite malocclu-sion was treated with extraction of both maxillary firstpremolars, a partial glossectomy, a 3-piece segmentalLeFort I osteotomy, a mandibular setback, andadvancement and reduction genioplasty, with goodocclusal stability.
ics July 2013 � Vol 144 � Issue 1
Fig 11. Posttreatment facial and intraoral photographs at 4 years 2 months show occlusal stability andmaintenance of overjet, overbite, and anteroposterior relationship.
138 Tanaka et al
CONCLUSIONS
An open-bite malocclusion with shortened maxillarycentral incisors and relative macroglossia was treatedby extraction of the maxillary first premolars. A partialglossectomy was performed before the orthognathicsurgery with a 3-piece segmental LeFort I osteotomy,mandibular setback, and advancement genioplasty. Afunctional and esthetic occlusion and improved facialprofile were established, and no further root shorteningwas observed after prolonged and significant toothmovement. Stability of the occlusion was observed at4 years 2 months posttreatment.
REFERENCES
1. Kawakami S, Yokozeki M, Takahashi T, Horiuchi S, Moriyama K.Siblings with spaced arches treated with and without partial
July 2013 � Vol 144 � Issue 1 American
glossectomy. Am J Orthod Dentofacial Orthop 2005;127:364-73.
2. Wolford LM, Cottrell DA. Diagnosis of macroglossia andindications for reduction glossectomy. Am J Orthod DentofacialOrthop 1996;110:170-7.
3. Vogel JE, Mulliken JB, Kaban LB. Macroglossia: a review of thecondition and a new classification. Plast Reconstr Surg 1986;78:715-23.
4. Schwenzer N, Voy ED, Niemczyk HM. Effect of tongue reductionon the orthodontic and surgical treatment of dysgnathia.J Maxillofac Surg 1977;5:15-20.
5. Ingervall B, Schmoker R. Effect of surgical reduction of the tongueon oral stereognosis, oral motor ability, and the rest position of thetongue and mandible. Am J Orthod Dentofacial Orthop 1990;97:58-65.
6. Vitral RWF, Tanaka OM, Fraga MR, Rosa EAR. Acromegaly in anorthodontic patient. Am J Orthod Dentofacial Orthop 2006;130:388-90.
Journal of Orthodontics and Dentofacial Orthopedics
Fig 13. Follow-up radiograph and cephalometric superimposition show no further root shortening.
Fig 12. Follow-up dental casts at 4 years 2 months.
Tanaka et al 139
8. Kuroda S, Sugawara Y, TamamuraN, Takano-YamamotoT.Anterioropen bite with temporomandibular disorder treated with titaniumscrew anchorage: evaluation of morphological and functionalimprovement. Am J Orthod Dentofacial Orthop 2007;131:550-60.
9. Allison ML, Miller CW, Troiano MF, Wallace WR. Partial glossec-tomy for macroglossia. J Am Dent Assoc 1971;82:852-7.
American Journal of Orthodontics and Dentofacial Orthoped
10. Medeiros PJ, Camargo ES, Vitral R, Rocha R. Orthodontic-sur-gical approach in a case of severe open-bite associated withfunctional macroglossia. Am J Orthod Dentofacial Orthop2000;118:347-51.
11. Bell WH, Proffit W, White RP. Surgical correction of dentofacialdeformities. Philadelphia: W. B. SaundeRS; 1980.
ics July 2013 � Vol 144 � Issue 1
140 Tanaka et al
12. Winstock D, Warnakulasuriya S. Partial glossectomy for macro-glossia in an elderly acromegalic. A case report. Int J Oral Maxillo-fac Surg 1986;15:629-31.
13. Ribeiro GL, Regis S Jr, da Cunha Tde M, Sabatoski MA, Guariza-Filho O, Tanaka OM. Multiloop edgewise archwire in the treatmentof a patient with an anterior open bite and a long face. Am JOrthod Dentofacial Orthop 2010;138:89-95.
14. Tanaka OM, Knop LHA, Shintcovsk RL, Hirata TM. Treatment ofa patient with severely shortened maxillary central incisor roots.J Clin Orthod 2008;42:729-31.
15. Kacker A, Honrado C, Martin D, Ward R. Tongue reduction inBeckwith-Wiedemann syndrome. Int J Pediatr Otorhinolaryngol2000;53:1-7.
16. Morgan WE, Friedman EM, Duncan NO, Sulek M. Surgicalmanagement of macroglossia in children. Arch Otolaryngol HeadNeck Surg 1996;122:326-9.
July 2013 � Vol 144 � Issue 1 American
17. Wang J, Goodger NM, Pogrel MA. The role of tongue reduction.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:269-73.
18. Austermann KH, Machtens E. The influence of tongue asymme-tries on the development of jaws and the position of teeth.Int J Oral Surg 1974;3:261-5.
19. Denison TF, Kokich VG, Shapiro PA. Stability of maxillary surgeryin openbite versus nonopenbite malocclusions. Angle Orthod1989;59:5-10.
20. Harris EF, Butler ML. Patterns of incisor root resorption be-fore and after orthodontic correction in cases with anterioropen bites. Am J Orthod Dentofacial Orthop 1992;101:112-9.
21. Kokich VG. Orthodontic and nonorthodontic root resorption:their impact on clinical dental practice. J Dent Educ 2008;72:895-902.
Journal of Orthodontics and Dentofacial Orthopedics