ACUTE CORONARY SYNDROMES . FRANCIS, ÜB, EDITOR MATTHEW T. ROE, MD Division of Cardiology, Duke Clinical Research Institute SHELLY K. SAPP, MS Senior blostatistician, Cleveland Clinic Cardiovascular Coordinating Center A. MICHAEL LINCOFF, MD Director, Experiental Interventional Laboratory Department of Cardiology, Cleveland Clinic Editor of Glycoprotein llblllla Inhibitors in Cardiovascular Diseases Glycoprotein Ilb/IIIa inhibitors in acute coronary syndromes ABSTRACT Glycoprotein (GP) Ilb/IIIa inhibitors are potent antiplatelet agents and represent an exciting breakthrough in the treatment of acute coronary syndromes. However, their safety and cost-effectiveness require further investigation, and more information on risk stratification is needed to clarify which patients benefit the most from empiric use of these agents. KEY POINTS In a combined analysis of trials of GP Ilb/IIIa inhibitors during percutaneous interventions or in non-ST-segment elevation acute coronary syndromes, the addition of these agents to standard therapy reduced the incidence of death or myocardial infarction by one fifth at 30 days. Abciximab and eptifibatide are both approved for use during percutaneous coronary interventions; eptifibatide and tirofiban are approved as empiric therapy in patients with non-ST-segment elevation acute coronary syndromes. During combination therapy with a GP Ilb/IIIa inhibitor and heparin, the risk of bleeding can be decreased by using lower doses of heparin, with no loss of efficacy. REATMENT STRATEGIES for acute coro- nary syndromes now focus on potent agents called glycoprotein (GP) Ilb/IIIa inhibitors, which block the final common pathway of platelet aggregation. This is a shift from previous strategies, which focused on fib- rinolytics, antithrombins, and aspirin, a rela- tively weak platelet inhibitor. • ROLE OF PLATELETS IN ACUTE CORONARY SYNDROMES Acute coronary syndromes—unstable angina, non-ST-segment elevation myocardial infarc- tion. (MI), and acute ST-segment elevation MI—all begin by a similar mechanism. First, an atherosclerotic plaque forms on a coronary artery wall. Then the plaque ruptures, expos- ing platelets to substances that activate them, such as collagen and von Willebrand factor. Activated platelets in tLim release substances such as thromboxane A 2 , serotonin, adenosine diphosphate (ADP), and thrombin, which activate more platelets. 1 Finally, activated platelets join together or "aggregate" to form a thrombus. 2 The size of the thrombus and the degree to which it disrupts coronary blood flow determine the clinical presentation of an acute coronary syndrome. 3 Platelets join to one another via their GP Ilb/IIIa receptors, found exclusively on platelets and megakaryocytes. Each platelet has up to 80,000 GP Ilb/IIIa receptors. When a platelet is activated, its GP Ilb/IIIa recep- tors undergo a conformational change and then bind circulating adhesive proteins, including fibrinogen. 4 After binding to fib- rinogen, GP llb/IIla receptors link adjacent platelets to propagate the developing throm- bus ( FIGURE 1). CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 67 • NUMBER 2 FEBRUARY 2000 131 on November 26, 2021. For personal use only. All other uses require permission. www.ccjm.org Downloaded from
Transcript
A C U T E C O R O N A R Y S Y N D R O M E S . F R A N C I S , Ü B , E D I T O R
MATTHEW T. ROE, M D Division of Cardiology, Duke Clinical Research Institute
SHELLY K. SAPP, MS Senior blostatistician, Cleveland Clinic Cardiovascular Coordinating Center
A. MICHAEL LINCOFF, M D Director, Experiental Interventional Laboratory Department of Cardiology, Cleveland Clinic Editor of Glycoprotein llblllla Inhibitors in Cardiovascular Diseases
Glycoprotein Ilb/IIIa inhibitors in acute coronary syndromes
A B S T R A C T Glycoprotein (GP) Ilb/IIIa inhibitors are potent antiplatelet agents and represent an exciting breakthrough in the treatment of acute coronary syndromes. However, their safety and cost-effectiveness require further investigation, and more information on risk stratification is needed to clarify which patients benefit the most from empiric use of these agents.
KEY P O I N T S In a combined analysis of trials of GP Ilb/IIIa inhibitors during percutaneous interventions or in non-ST-segment elevation acute coronary syndromes, the addition of these agents to standard therapy reduced the incidence of death or myocardial infarction by one fifth at 30 days.
Abciximab and eptifibatide are both approved for use during percutaneous coronary interventions; eptifibatide and tirofiban are approved as empiric therapy in patients with non-ST-segment elevation acute coronary syndromes.
During combination therapy with a GP Ilb/IIIa inhibitor and heparin, the risk of bleeding can be decreased by using lower doses of heparin, with no loss of efficacy.
REATMENT STRATEGIES for acute coro-nary syndromes now focus on potent
agents called glycoprotein (GP) Ilb/IIIa inhibitors, which block the final common pathway of platelet aggregation. This is a shift from previous strategies, which focused on fib-rinolytics, antithrombins, and aspirin, a rela-tively weak platelet inhibitor.
• ROLE OF PLATELETS IN ACUTE CORONARY SYNDROMES
Acute coronary syndromes—unstable angina, non-ST-segment elevation myocardial infarc-tion. (MI), and acute ST-segment elevation MI—all begin by a similar mechanism. First, an atherosclerotic plaque forms on a coronary artery wall. Then the plaque ruptures, expos-ing platelets to substances that activate them, such as collagen and von Willebrand factor. Activated platelets in tLim release substances such as thromboxane A2 , serotonin, adenosine diphosphate (ADP), and thrombin, which activate more platelets.1 Finally, activated platelets join together or "aggregate" to form a thrombus.2 T h e size of the thrombus and the degree to which it disrupts coronary blood flow determine the clinical presentation of an acute coronary syndrome.3
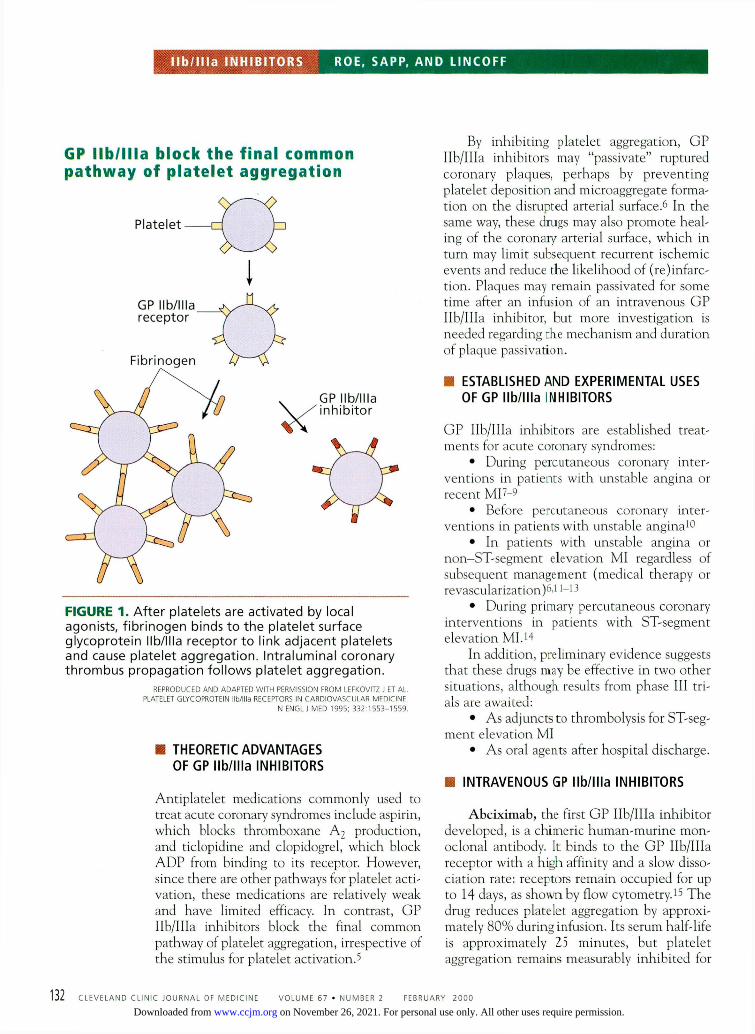
Platelets join to one another via their G P Ilb/IIIa receptors, found exclusively on platelets and megakaryocytes. Each platelet has up to 80,000 G P Ilb/IIIa receptors. W h e n a platelet is activated, its G P Ilb/IIIa recep-tors undergo a conformational change and t h e n bind c i rcula t ing adhesive proteins, including fibrinogen.4 Af ter binding to fib-rinogen, G P llb/IIla receptors link adjacent platelets to propagate the developing throm-b u s ( F I G U R E 1 ) .
CLEVELAND CLINIC JOURNAL OF MEDICINE V O L U M E 67 • NUMBER 2 FEBRUARY 2 0 0 0 1 3 1
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
I l b / l l l a I N H I B I T O R S R O E , S A P P , A N D L I N C O F F
G P I l b / l l l a b l o c k t h e f i n a l c o m m o n p a t h w a y o f p l a t e l e t a g g r e g a t i o n
I
FIGURE 1. A f t e r p l a t e l e t s a re a c t i v a t e d by loca l agon i s t s , f i b r i n o g e n b i n d s t o t h e p l a t e l e t s u r f a c e g l y c o p r o t e i n I lb / l l la r e c e p t o r t o l i nk a d j a c e n t p l a t e l e t s a n d cause p l a t e l e t a g g r e g a t i o n . I n t r a l u m i n a l c o r o n a r y t h r o m b u s p r o p a g a t i o n f o l l o w s p l a t e l e t a g g r e g a t i o n .
R E P R O D U C E D A N D A D A P T E D W I T H PERMISSION F R O M LEFKOVITZ J ET A L . PLATELET GLYCOPROTEIN I lb / l l la RECEPTORS IN C A R D I O V A S C U I AR M F D I C I N F
N ENGL J M E D 1 9 9 5 ; 3 3 2 : 1 5 5 3 - 1 5 5 9 .
• THEORETIC ADVANTAGES OF GP I lb/ l l la INHIBITORS
Antiplatelet medications commonly used to treat acute coronary syndromes include aspirin, which blocks thromboxane A 2 production, and ticlopidine and C l o p i d o g r e l , which block A D P from binding to its receptor. However, since there are other pathways for platelet acti-vation, these medications are relatively weak and have limited efficacy. In contrast, GP Ilb/IIIa inhibitors block the final common pathway of platelet aggregation, irrespective of the stimulus for platelet activation.5
By inhibiting platelet aggregation, G P Ilb/IIIa inhibitors may "passivate" ruptured coronary plaques, perhaps by prevent ing platelet deposition and microaggregate forma-tion on the disrupted arterial surface.6 In the same way, these drugs may also promote heal-ing of the coronary arterial surface, which in turn may limit subsequent recurrent ischemic events and reduce the likelihood of (re)infarc-tion. Plaques may remain passivatcd for some time after an infusion of an intravenous G P Ilb/IIIa inhibitor, but more investigation is needed regarding che mechanism and duration of plaque passivation.
• ESTABLISHED AND EXPERIMENTAL USES OF GP I lb/ l l la INHIBITORS
G P Ilb/IIIa inhibitors are established treat-ments for acute coronary syndromes:
• During percutaneous coronary inter-ventions in patients with unstable angina or recent MI7-9
• Before percutaneous coronary inter-ventions in patients with unstable angina1 0
• In patients with unstable angina or non-ST-segment elevation MI regardless of subsequent management (medical therapy or revascularization)6.11—13
• During primary percutaneous coronary interventions in patients with ST-segment elevation MI.14
In addition, preliminary evidence suggests that these drugs may be effective in two other situations, although results from phase III tri-als are awaited:
• As adjuncts to thrombolysis for ST-seg-ment elevation Ml
• As oral agents after hospital discharge.
• INTRAVENOUS GP I lb/ l l la INHIBITORS
Abciximab, the first G P Ilb/IIIa inhibitor developed, is a chimeric human-murine mon-oclonal antibody. It binds to the G P Ilb/IIIa receptor with a high affinity and a slow disso-ciation rate: receptors remain occupied for up to 14 days, as shown by flow cytometry.15 T h e drug reduces platelet aggregation by approxi-mately 80% during infusion. Its serum half-life is approximately 25 minutes, but platelet aggregation remains measurably inhibited for
1 3 2 C L E V E L A N D C L I N I C J O U R N A L O F M E D I C I N E V O L U M E 6 7 • N U M B E R 2 F E B R U A R Y 2 0 0 0
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
I n t r a v e n o u s g l y c o p r o t e i n I l b / 1 I I a i n h i b i t o r s
GENERIC BRAND APPROVED DOSAGE NAME N A M E USES IN PERCUTANEOUS
CORONARY INTERVENTIONS IN ACUTE CORONARY SYNDROMES
Abcix imab ReoPro Before and during percutaneous coronary interventions
0.25 jag/kg bolus, then 0.125 |ag/kg/mmute infusion for 12 hours*
Not approved
Ept i f ibat ide Integrilin Percutaneous coronary interventions, acute coronary syndromes
135 ju.g/kg bolus, then 0.5 |ig/kg/minute infusion for 24 hours*
180 (ig/kg bolus, then 2.0 |ag/kg/minute infusion for up to 72 hours*
Tirof iban Aggrastat Acute coronary syndromes
Not approved 0.4 |jg/kg/mmute bolus for 30 minutes, 0.1 pg/kg/minute infusion for up to 72 hours§
Lamif iban None None Not approved Not approved
"The infusion can he started up to 24 hours before before percutaneous coronary interventions and continued at the same rate through the procedure fThis is the FDA-approved dosage for percutaneous coronary interventions, but pharmacodynamic data suggest that the higher dosage be used in both situations *No specific recommendations have been made for reducing the eptifibatide dose wi th renal insufficiency, but a reasonable adjustment would be to reduce the infusion rate by 50% § If the creatinine clearance is < 30 mL/min, the tirofiban infusion rate should be reduced by 50%
18 to 36 hours after the infusion is stopped as abciximab distributes from old to new platelets entering the circulation.16
Abciximab is approved for use before and during percutaneous coronary interventions ( T A B L E 1 ) .
Small-molecule GP Ilb/lIIa inhibitors. Eptifibatide (a synthetic peptide) and tirofiban and lamifiban (which are not peptides) are highly specific for binding to the G P Ilb/IIIa receptor, but rapidly dissociate from the recep-tor so that platelet inhibition persists for only 1 to 2 hours after stopping the infusion.17
Eptifibatide is approved for use during percutaneous coronary interventions and in non-ST-segment elevation acute coronary syndromes. Tirofiban is approved for use only in non-ST-segment elevation acute coronary syndromes.
• CLINICAL TRIALS OF GP Ilb/IIIa INHIBITORS
Topol1 8 performed a meta-analysis of nine large-scale clinical trials of G P Ilb/IIIa inhibitors in acute coronary syndromes and
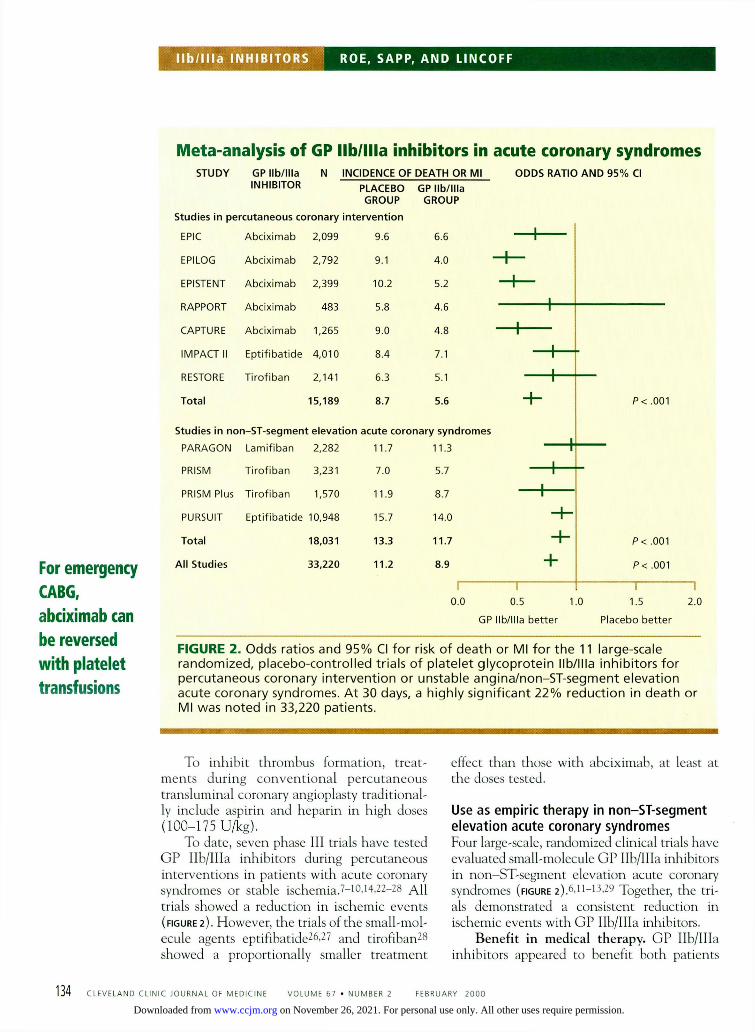
calculated that these agents reduced the 30-day incidence of death or MI by 19% when added to standard therapy. Not available at the time of Topol's analysis were the EPIS-T E N T 9 and RAPPORT 1 4 trials. W h e n the results of these trials were incorporated into the meta-analysis, the relative reduction in the risk of death or MI at 30 days was approx-imately 22% ( F I G U R E 2 ) .
Use during percutaneous coronary intervent ions Percutaneous coronary interventions injure the vessel wall, damage the intima, and expose the subendothel ium. As a result, platelets become activated and a thrombus can form. Intracoronary thrombus formation can cause abrupt vessel closure, which can lead to death or MI after percutaneous inter-ventions.1 9 In addition, many patients with acute coronary syndromes who undergo per-cutaneous interventions have a pre-existing intracoronary thrombus, which is a predictor of abrupt closure and o ther complica-tions.20.21
Abciximab is longer-acting than tirofiban or eptifibatide
CLEVELAND CLINIC JOURNAL OF MEDICINE V O L U M E 6 7 • NUMBER 2 FEBRUARY 2 0 0 0 1 3 3
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
I l b / l l l a I N H I B I T O R S R O E , S A P P , A N D L I N C O F F
For emergency CABG, abciximab can be reversed with platelet transfusions
Meta-analysis of GP Ilb/llla inhibitors in acute coronary syndromes S T U D Y G P I l b / l l l a
I N H I B I T O R N I N C I D E N C E O F D E A T H O R M l
P L A C E B O G P I l b / l l l a G R O U P G R O U P
O D D S R A T I O A N D 9 5 % CI
S t u d i e s in p e r c u t a n e o u s c o r o n a r y i n t e r v e n t i o n
EPIC A b c i x i m a b 2 , 0 9 9 9 . 6 6 . 6
E P I L O G A b c i x i m a b 2 , 7 9 2 9 . 1 4 . 0
E P I S T E N T A b c i x i m a b 2 , 3 9 9 1 0 . 2 5 . 2
R A P P O R T A b c i x i m a b 4 8 3 5 . 8 4 . 6
C A P T U R E A b c i x i m a b 1 , 2 6 5 9 . 0 4 . 8
I M P A C T II E p t i f i b a t i d e 4 , 0 1 0 8 . 4 7 . 1
R E S T O R E T i r o f i b a n 2 , 1 4 1 6 . 3 5 .1
T o t a l 1 5 , 1 8 9 8 . 7 5 . 6
S t u d i e s in n o n - S T - s e g m e n t e l e v a t i o n a c u t e c o r o n a r y s y n d r o m e s
P A R A G O N L a m i f i b a n 2 , 2 8 2 1 1 . 7 1 1 . 3 h
P R I S M T i r o f i b a n 3 , 2 3 1 7 . 0 5 . 7 — h -
P R I S M P l u s T i r o f i b a n 1 , 5 7 0 1 1 . 9 8 . 7 — I
P U R S U I T E p t i f i b a t i d e 1 0 , 9 4 8 1 5 . 7 1 4 . 0 H -
T o t a l 1 8 , 0 3 1 1 3 . 3 1 1 . 7 - h P < . 0 0 1
A l l S t u d i e s 3 3 , 2 2 0 1 1 . 2 8 . 9 + P < . 0 0 1
P< . 0 0 1
I 1
0 . 0 0 . 5 1 .0
G P I l b / l l l a b e t t e r
1.5 2.0
P l a c e b o b e t t e r
F I G U R E 2 . O d d s r a t i o s a n d 9 5 % CI f o r r isk o f d e a t h o r M l f o r t h e 11 la rge -sca le r a n d o m i z e d , p l a c e b o - c o n t r o l l e d t r i a l s o f p l a t e l e t g l y c o p r o t e i n I lb / l l l a i n h i b i t o r s f o r p e r c u t a n e o u s c o r o n a r y i n t e r v e n t i o n o r u n s t a b l e a n g i n a / n o n - S T - s e g m e n t e l e v a t i o n a c u t e c o r o n a r y s y n d r o m e s . A t 30 days, a h i g h l y s i g n i f i c a n t 2 2 % r e d u c t i o n in d e a t h o r M l w a s n o t e d in 33 ,220 p a t i e n t s .
To inhibit thrombus formation, treat-ments during convent iona l percutaneous transluminal coronary angioplasty traditional-ly include aspirin and heparin in high doses (100-175 U/kg).
To date, seven phase III trials have tested G P Ilb/IIIa inhibitors during percutaneous interventions in patients with acute coronary syndromes or stable ischemia.7-10,14,22-28 All trials showed a reduction in ischemic events (FIGURE 2 ) . However, the trials of the small-mol-ecule agents eptifibatide26-27 and tirofiban28
showed a proportionally smaller t reatment
effect than those with abciximab, at least at the doses tested.
Use as empir ic the rapy in non-ST-segment e leva t ion acute coronary syndromes Four large-scale, randomized clinical trials have evaluated small-molecule G P Ilb/IIIa inhibitors in non-ST-segment elevation acute coronary syndromes (FIGURE 2):6,11-13,;29 Together, the tri-als demonstrated a consistent reduction in ischemic events with G P Ilb/IIIa inhibitors.
Benefit in medical therapy. GP Ilb/IIIa inhibitors appeared to benefit both patients
1 3 4 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 67 • NUMBER 2 FEBRUARY 2000
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
• P r o t h r o m b o t i c e f fec ts o f f i b r ino ly t i c t h e r a p y A c o r o n a r y t h r o m b u s is c o m p o s e d o f a p l a t e l e t c o r e w i t h a f i b r i n - t h r o m b i n a d m i x t u r e . F i b r i n o l y t i c d r u g s e x p o s e f r e e t h r o m b i n a n d t h u s p r o m o t e p l a t e l e t a g g r e g a t i o n . P la te l e t s c a n also be r e s i s t a n t t o f i b r i n o l y t i c t h e r a p y s ince t h e y sec re te l a r g e q u a n t i t i e s o f PAI-1 ( p l a s m i n o g e n a c t i v a t o r i n h i b i t o r - 1 ) , w h i c h is a p o t e n t a n t a g o n i s t t o f i b r i n o l y s i s .
PAI-1 ( p l a s m i n o g e n a c t i v a t o r - i n h i b i t o r ) , r e l e a s e d by p l a t e l e t s , b l o c k s f i b r i n o l y t i c d r u g s
FIBRINOLYTIC D R U G • (eg, t -PA) f r e e s t h r o m b i n f r o m c l o t
T H R O M B I N p r o m o t e s p r o d u c t i o n o f m o r e t h r o m b i n
PLATELETS, a c t i v a t e d b y f r e e t h r o m b i n , a c t i v a t e m o r e p l a t e l e t s a n d c o n t i n u e t o a g g r e g a t e
FIGURE 3 managed medically and those who underwent percutaneous interventions, although none of the trials randomly assigned patients to these management strategies. For example, patients receiving tirofiban who underwent medical management in the PRISM-PLUS trial had a reduction in the 30-day incidence of death or nonfatal MI of 2.3%; (those who underwent percutaneous interventions had a reduction of
4.3%).1 2 Similarly, in the P U R S U I T trial, the effect of eptifibatide was greater in patients who underwent percutaneous interventions while receiving the study drug infusion, but a sizable proportion of the t reatment effect occurred before the procedure was performed, demonstrating a preprocedural stabilization effect in these patients.15 W h e n patients who did no t undergo percutaneous or surgical
C L E V E L A N D CLINIC J O U R N A L OF M E D I C I N E V O L U M E 6 7 • N U M B E R 2 FEBRUARY 2 0 0 0 1 3 5
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
I l b / l l l a I N H I B I T O R S R O E , S A P P , A N D L I N C O F F
T A B L E 2
D o s e - r a n g i n g t r i a l s o f G P I l b / l l l a i n h i b i t o r s i n a c u t e S T - s e g m e n t m y o c a r d i a l i n f a r c t i o n
TRIAL NO. OF GP IIB/IIIA FIBRINOLYTIC PATIENTS INHIBITOR AGENT
Trials of full-dose fibrinolytics plus partial-dose GP Ilb/llla inhibitors TAMI-832 70 Abciximab t-PA IMPACT-AMI33 132 Eptifibatide t-PA Ronner et al34 181 Eptifibatide Streptokinase PARADIGM35 3 45 Lamifiban Streptokinase / t-PA
Trials of reduced-dose fibrinolytics plus full-dose GP Ilb/llla inhibitors TIMI-143 6 888 Abciximab Streptokinase / t-PA SPEED37 193 Abciximab r-PA
Monitor the platelet count for 24 hours after starting a GP Ilb/llla inhibitor
revascularization in PURSUIT were separate-ly analyzed, a significant reduction in 30-day death or nonfatal MI was still demonstrated in the eptifibatide group.30
Use in acute ST-segment e levat ion M l Fibrinolytic therapy is a well-established method of reperfusion for acute ST-segment elevation MI and reduces mortality by 25% to 30% compared with placebo. However, even ideal fibrinolytic regimens restore complete perfusion (TIMI grade 3 flow) in only approx-imately half of patients, and half of patients who initially achieve r e p e r f L i s i o n subsequently experience reocclusion or intermittent patency of the infarct vessel. Thus, fibrinolytic therapy alone establishes and maintains reperfusion in only approximately one fourth of patients with acute ST-segment elevation MI.31
Why does fibrinolysis so often fail? Fibrinolytic agents break down fibrin in a coronary thrombus, but also increase throm-bin generation by exposing underlying clot-bound thrombin. Since thrombin is a potent platelet activator, fibrinolytic therapy can paradoxically make a ruptured plaque more prothrombotic. In addition, platelets are rich in PAI-1 (plasminogen activator inhibitor-1), so the expanding platelet thrombus may resist fibrinolysis by inhibiting tissue plasminogen activator (t-PA) with PAI-1 ( F I G U R E S ) . 1 8
With these limitations of fibrinolytic ther-apy in mind, investigators hope that the com-bination of G P Ilb/IIIa inhibitors plus fibri-
nolytic agents will produce better results. So far, four dose-ranging trials32^35 evaluated combina t ion therapy with G P Ilb/IIIa inhibitors and full doses of fibrinolytic agents for acute ST-segment e levat ion MI. Subsequently, two trials56*3? used partial doses of fibrinolytics with G P Ilb/IIIa inhibitors (TABLE 2 ) .
The collective results suggest that adding a GP Ilb/IIIa inhibitor increases the percentage of patients who achieve patency of the infarct-related artery. This combined approach appears safe and did not substantially increase the rate of bleeding complications except when strep-tokinase was used with full doses of G P Ilb/IIIa inhibitors.34-36 Intracranial hemorrhage rates did not appear to increase, although trials to date included too few patients to assess this infrequent complication. Also, the ideal dose of heparin to use with combination reperfusion therapy has not yet been established. T h e ongoing G U S T O IV trial will determine if combination theiapy with reteplase and abcix-imab will improve clinical outcomes in a large-scale, definitive study.
• SAFETY ISSUES
T h e safety profile of intravenous G P Ilb/IIIa inhibitors evaluated in phase III clinical trials has generally been favorable.
Periprocedural bleeding. W h e n abcix-imab was first used with standard, high-dose heparin during percutaneous coronary inter-
136 CLEVELAND CLINIC JOURNAL OF MEDICINE V O L U M E 67 • NUMBER 2 FEBRUARY 2 0 0 0
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
ventions, bleeding complications increased, mostly at the puncture site.38 W h e n the hepar in dose used with abciximab was decreased and weight-adjusted, bleeding com-plications decreased without a loss in effica-cy.8 Minor bleeding complicat ions were increased when the small-molecule G P lib/Ilia inhibitors were used with weight-adjusted heparin, and major bleeding requir-ing transfusion occurred in 0.7% to 1.5% of patients.6-11"13 Intracranial hemorrhage has rarely been seen with G P Ilb/IIIa inhibitors, alone or in combination with heparin.3 9 '4 0
Bleeding during surgery. In theory, patients who receive abciximab may be at increased risk of bleeding during any subse-quent emergency coronary artery bypass graft-ing (CABG) . However, patients in the EPI-LOG and EPI STENT trials who underwent emergency CABG after receiving abciximab did not have a higher incidence of bleeding complicat ions than did placebo-treated pat ients .4 1 If a pat ient needs emergency C A B G , abciximab can be reversed with platelet transfusions. Increased bleeding dur-ing emergency CABG is not an issue with ept i f ibat ide or t irofiban, since their antiplatelet effect rapidly decreases after they are stopped.
Thrombocytopenia occurs in 0.5% to 1.0% of patients treated with intravenous G P Ilb/IIIa inhibitors. T h e mechanism has not been clearly delineated.42 Severe thrombocy-topenia (platelet count < 20 x 109/L) has occurred within 24 hours of receiving abcix-imab.43 '44 In the EPIC and C A P T U R E trials, severe thrombocytopenia occurred in 0.3% of patients.1 0-4 3 Thrombocytopenia resolved with platelet transfusions and stopping antiplatelet therapy and heparin, and no major complications were reported. Thus, platelet counts should be closely monitored for 24 hours after starting a G P Ilb/IIIa inhibitor. If bleeding and severe thrombocy-topenia occur, platelet transfusions should be given and the GP Ilb/IIIa inhibitor, heparin, and aspirin should be stopped.
Efficacy and safety of repeated use. Whethe r G P Ilb/IIIa inhibitors remain safe and effective with repeated use is important, since many patients who undergo percuta-neous interventions or fibrinolytic therapy
ultimately require fur ther interventions. Approximately 6% of patients develop anti-bodies to abciximab after the first dose.7
Recent data from the Abciximab Readministration Registry46 showed no cases of allergic, hypersensitivity, or anaphylactic reactions among 329 patients who received abciximab a second time. In addition, the clinical efficacy and level of platelet inhibi-tion was similar the second time. There was, however, a moderate increase in thrombocy-topenia. No antibodies have been detected after use of the synthetic agents eptifibatide or tirofiban.
• COST-EFFECTIVENESS
T h e high cost of G P Ilb/IIIa inhibitors (abcix-imab costs $1,407 per dose) has limited their widespread use, but given their substantial benefit, they may be cost-effective.
A formal economic analysis of the EPIC trial47 concluded that abciximab paid for itself during percutaneous coronary interven-tions by reducing ischemic events that neces-sitated readmission to the hospital and urgent revascularization procedures. Other analy-ses48 '49 concluded that abciximab is approxi-mately as cost-effective as other widely used therapies. In addition, trials performed after the EPIC trial showed markedly fewer bleed-ing events, making the cost-benefit ratio of G P Ilb/IIIa inhibi tors more favorable. Economic analyses from the PURSUIT and PRISM-PLUS trials are expected soon and will help to determine the cost-effectiveness of empiric use of Ilb/IIIa inhibitors for acute coronary syndromes.
• UNRESOLVED ISSUES
Several issues require further research. Which GP Ilb/IIIa inhibitor should be
used in a given situation? The answer is not clear, since these agents have not been direct-ly compared in clinical trials. Overwhelming data support the efficacy of abciximab during percutaneous coronary interventions over the short and long term. Abciximab appears more potent than the closes of eptifibatide or tirofiban that have been used during percuta-neous interventions.
Though costly, GP Ilb/IIIa inhibitors may be cost-effective
C L E V E L A N D CLINIC J O U R N A L OF M E D I C I N E V O L U M E 67 • N U M B E R 2 FEBRUARY 2 0 0 0 60
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
I l b / l l l a I N H I B I T O R S R O E , S A P P , A N D L I N C O F F
Inability to titrate low-molecular-weight heparins is a barrier to use with GP Ilb/llla inhibitors
O n the other hand, there are no apparent differences between eptifibatide and tirofiban when used for empiric treatment of unstable angina, although more patients were enrolled in trials of eptifibatide (ie, the PURSUIT trial) than in trials of tirofiban.
What if a patient starts out receiving epti-fibatide or tirofiban as empiric treatment and then undergoes angioplasty? One may be tempted to change to abciximab, which seems to be more beneficial during angioplasty than the other agents. We cannot recommend this, however, since eptifibatide and tirofiban also are beneficial during percutaneous coronary interventions, and we have no data on whether changing to abciximab is safe or effective.
What is the proper eptifibatide dosage in percutaneous coronary interventions? As shown in TABLE 1 , the Food and Drug Administration recommends a lower dose of eptifibatide during percutaneous coronary interventions than in acute non—ST-segment elevation coronary syndromes, because the lower dose was used in the 1MPACT-I1 trial. However, we suspect that the higher dose should be used in bot h situations: a 180 (Xg/kg bolus followed by a 2.0 |ig/kg/min infusion. Clinical trials are underway to examine this issue.
What is the proper dosage of heparin to use with GP Ilb/IIIa inhibitors? No clear rec-ommendations have emerged despite the mul-tiple clinical trials completed.
Can low-molecular-weight heparin be used with G P I lb ' I I Ia inhibitors? Al th
i l l H T h enoxaparin reduced ischemic events when compared with unfractionated heparin in the ESSENCE trial, it has not been tested in com-bination with G P Ilb/IIIa inhibitors.50
A problem with low-molecular-weight heparins is that we cannot monitor their anti-coagulant effect closely with tests such as the activated clotting time assay.51 Given the known risk of hemorrhage when excessive doses of unfractionated heparin are used with G P Ilb/IIIa agents during coronary interven-tion, the inability to titrate the dosage of low-molecular-weight heparins poses a barrier to using them with G P Ilb/IIIa inhibitors.
Other issues. Ongoing trials are address-ing specific questions regarding the optimal
dose and duration of G P Ilb/IIIa inhibitor therapy (PARAGON-B and SYMPHONY, respectively), the safety and efficacy of combi-nation reperfusion therapy with fibrinolytics and G P Ilb/IIIa inhibitors (GUSTO-IV) , and the ideal balance between antiplatelet therapy and percutaneous revascularization for non-ST-segment elevation acute coronary syndromes (TACTICS-TIMI 18).
• ORAL GP Ilb/llla INHIBITORS
After initially being treated with fibrinolytics and antithrombins, patients with acute MI and unstable angina can remain in a prothrombot-ic state for several months.52 In addition, the underlying ruptured plaque may take weeks to months to heal.55 Further, many of the trials of intravenous G P Ilb/IIIa inhibitors showed a large benefit early on but a smaller benefit at 30 days. With these observations in mind, investigators hope to extend the benefits of G P Ilb/IIIa blockade by giving oral agents.54
Sibrafiban in varying doses was compared with aspirin in 329 patients with acute coro-nary syndromes in the TIMI-12 trial.55
Sibrafiban produced a rapid and sustained inhibi t ion of platelet aggregation at the expense of a moderate increase in "nuisance" bleeding at the highest dose studied. However, a sizable percentage of patients had to stop tak-ing the drug because of such "nuisance" bleed-ing (eg, epistaxis, gum bleeding), suggesting that intense inhibition of platelet aggregation may not be tolerated in the long term. Adverse ischemic events were rare in both the aspirin and sibrafiban groups. Sibrafiban was com-pared with aspirin for the treatment of acute coronary syndromes in the phase III SYM-PHONY trial among 9,000 patients, but no consistent benefit was demonstrated.5 6
Xemilofiban was tested in 549 patients after elective percutaneous coronary interven-tion in the ORBIT trial; sustained platelet inhi-bition was seen after 1 month of therapy.57 The agent was also tested in the large-scale EXCITE trial in patients undergoing coronary interven-tion, but no treatment benefit was seen.58
Orofiban was tested in patients with acute coronary syndromes in the S O A R trial; sus-tained platelet inhibition for 12 weeks was demonstrated.59 The agent was also tested in
61 CLEVELAND CLINIC JOURNAL OF MEDICINE V O L U M E 67 • NUMBER 2 FEBRUARY 2 0 0 0
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
the large-scale O P U S TIM1 16 trial, which was prematurely halted because of unfavorable results. Excess mortality was demonstrated in the orofiban arms, but a mechanistic explana-tion for this finding has not been elucidated.58
Other oral G P Ilb/IIIa inhibitors being evaluated include lotrifiban, lefradifiban, and roxifiban.
Therefore , multiple questions remain regarding oral G P Ilb/IIIa inhibitors: Are these agents safe? Is there synergistic benefit with concomitant aspirin therapy? Will oral G P Ilb/IIIa inhibitors cause unacceptable rates of bleeding or thrombocytopenia?60 '61
Also unknown are the optimal dosage and the necessary duration of treatment.
• RECOMMENDATIONS
Consider t rea tment with a G P Ilb/IIIa inhibitor in:
• All patients undergoing percutaneous revascularization (al though pat ients with unstable angina or an evolving or recent acute MI may derive more benefit).
• Patients with non-ST-segment eleva-tion acute coronary syndromes who have high-risk characteristics, regardless of the intended management strategy. High-risk characteristics include dynamic ST-segment electrocardiographic changes, positive car-diac markers, postinfarction angina, pro-longed chest pain refractory to other medica-tions, hemodynamic instability, and previous revascularization procedures. In addit ion, patients with elevated troponin levels appear to derive more benefit from G P Ilb/IIIa inhibitors.62
Aspirin and heparin should be given with eptifibatide or tirofiban for empiric treatment of unstable angina unless specific contraindi-cations exist. "
• REFERENCES 1. L e f k o v i t s J, T o p o ! EJ. T h e c l i n i ca l r o l e o f p l a t e l e t g l y c o p r o t e i n I lb / I I Ia
r e c e p t o r i n h i b i t o r s i n i s c h e m i c h e a r t d isease . C leve C l i n J M e d 1996 ; 6 3 : 1 8 1 - 1 8 9 .
2. Falk E, S h a h PK, F u s t e r V. C o r o n a r y p l a q u e d i s r u p t i o n . C i r c u l a t i o n 1995 ; 9 2 : 6 5 7 - 6 7 1 .
3. F u s t e r V, B a d i m o n L, B a d i m o n JJ, C h e s e b o r o JH. T h e p a t h o g e n e s i s o f c o r o n a r y a r t e r y d i sease a n d t h e a c u t e c o r o n a r y s y n d r o m e s . N E n g l J M e d 1992 ; 3 2 6 : 2 4 2 - 2 5 0 .
4. C o l l e r BS. B l o c k a d e o f p l a t e l e t g l y c o p r o t e i n I lb / I I Ia r e c e p t o r as a n a n t i -t h r o m b o t i c s t r a t e g y . C i r c u l a t i o n 1995 ; 9 2 : 2 3 7 3 - 2 3 8 0 .
5. T c h e n g JE, El l is SG, G e o r g e BS, e t a l . P h a r m a c o d y n a m i c s o f c h i m e r i c g l y c o p r o t e i n I lb / I I Ia I n t e g r i n a n t i p l a t e l e t a n t i b o d y Fab 7E3 i n h i g h - r i s k c o r o n a r y a n g i o p l a s t y . C i r c u l a t i o n 1994; 9 0 : 1 7 5 7 - 1 7 6 4 .
6. T h e P A R A G O N I n v e s t i g a t o r s . I n t e r n a t i o n a l , r a n d o m i z e d , c o n t r o l l e d t r i a l o f l a m i f i b a n (a p l a t e l e t g l y c o p r o t e i n I lb / I I Ia i n h i b i t o r ) , h e p a r i n , o r b o t h in u n s t a b l e a n g i n a . C i r c u l a t i o n 1998; 9 7 : 2 3 8 6 - 2 3 9 5 .
7. T h e EPIC I n v e s t i g a t o r s . Use o f a m o n o c l o n a l a n t i b o d y d i r e c t e d a g a i n s t t h e p l a t e l e t g l y c o p r o t e i n I lb / I I Ia r e c e p t o r i n h i g h - r i s k c o r o n a r y a n g i o -p las ty . N E n g l J M e d 1994 ; 3 3 0 : 9 5 6 - 9 6 1 .
8. T h e EPILOG I n v e s t i g a t o r s . P l a t e l e t g l y c o p r o t e i n I lb/ I I Ia r e c e p t o r b l o c k -a d e a n d l o w - d o s e h e p a r i n d u r i n g p e r c u t a n e o u s c o r o n a r y r e v a s c u l a r -i z a t i o n . N E n g l J M e d 1997 ; 3 3 6 : 1 6 8 9 - 1 6 9 6 .
9. T h e EPISTENT I n v e s t i g a t o r s . R a n d o m i s e d p l a c e b o - c o n t r o l l e d a n d b a l -l o o n - a n g i o p l a s t y - c o n t r o l l e d t r i a l t o assess s a f e t y o f c o r o n a r y s t e n t i n g w i t h use o f p l a t e l e t g l y c o p r o t e i n - l l b / l l l a b l o c k a d e . L a n c e t 1998 ; 3 5 2 : 8 7 - 3 9 2 .
10. T h e CAPTURE I n v e s t i g a t o r s . R a n d o m i s e d p l a c e b o - c o n t r o l l e d t r i a l o f a b c i x i m a b b e f o r e a n d d u r i n g c o r o n a r y i n t e r v e n t i o n in r e f r a c t o r y u n s t a b l e a n g i n a : t h e CAPTURE s t u d y . L a n c e t 1997 ; 3 4 9 : 1 4 2 9 - 1 4 3 5 .
11. T h e PRISM I n v e s t i g a t o r s . A c o m p a r i s o n o f a s p i r i n p l u s t i r o f i b a n w i t h a s p i r i n p l u s h e p a r i n f o r u n s t a b l e a n g i n a . N E n g l J M e d 1998; 3 3 8 : 1 4 9 8 - 1 5 0 5 .
12. T h e PRISM-PLUS I n v e s t i g a t o r s . I n h i b i t i o n o f t h e p l a t e l e t g l y c o p r o t e i n I lb / I I Ia r e c e p t o r w i t h t i r o f i b a n in u n s t a b l e a n g i n a a n d n o n - Q - w a v e m y o c a r d i a l i n f a r c t i o n . N E n g l J M e d 1998 ; 3 3 8 : 1 4 8 8 - 1 4 9 7 .
13. T h e PURSUIT I n v e s t i g a t o r s . I n h i b i t i o n o f p l a t e l e t g l y c o p r o t e i n I lb / I I Ia w i t h e p t i f i b a t i d e i n p a t i e n t s w i t h a c u t e c o r o n a r y s y n d r o m e s . N E n g l J M e d 1998 ; 3 3 9 : 4 3 6 - 4 4 3 .
14. B r e n e r SJ, Ba r r LA, B u r c h e n a l JEB, e t a l . R a n d o m i z e d , p l a c e b o - c o n -t r o l l e d t r i a l o f p l a t e l e t g l y c o p r o t e i n I lb / I I Ia b l o c k a d e w i t h p r i m a r y a n g i o p l a s t y f o r a c u t e m y o c a r d i a l i n f a r c t i o n . C i r c u l a t i o n 1 9 9 8 ; 9 8 : 7 3 4 - 7 4 1 .
15. C o l l e r BS, A n d e r s o n K, W e i s m a n HF. N e w a n t i p l a t e l e t a g e n t s : p l a t e l e t GPI Ib / l l la a n t a g o n i s t s . T h r o m b H a e m o s t 1995 ; 7 4 : 3 0 2 - 3 0 8 .
16. K l e i m a n NS, R a i z n e r AE , J o r d a n R, e t a l . D i f f e r e n t i a l i n h i b i t i o n o f p l a t e l e t a g g r e g a t i o n i n d u c e d b y a d e n o s i n e d i p h o s p h a t e o r a t h r o m -b i n r e c e p t o r - a c t i v a t i n g p e p t i d e in p a t i e n t s t r e a t e d w i t h b o l u s c h i m e r i c 7E3 Fab: i m p l i c a t i o n s f o r i n h i b i t i o n o f t h e i n t e r n a l p o o l o f G P I lb/ I I Ia r e c e p t o r s . J A m Col l C a r d i o l 1995; 2 6 : 1 6 6 5 - 1 6 7 1 .
17. C o l l e r BS, A n d e r s o n K M , W e i s m a n HF. T h e a n t i - G P l l b - l l l a a g e n t s : f u n -d a m e n t a l a n d c l i n i ca l aspec ts . H a e m o s t a s i s 1996 ; 2 6 : 2 8 5 - 2 9 3 .
18. T o p o l EJ. T o w a r d a n e w f r o n t i e r in m y o c a r d i a l r e p e r f u s i o n t h e r a p y : e m e r g i n g p l a t e l e t p r e e m i n e n c e . C i r c u l a t i o n 1998 ; 9 7 : 2 1 1 - 2 1 8 .
19. L i n c o f f A M , P o p m a JJ, El l is SG, H a c k e r JA , T o p o l EJ. A b r u p t vesse l c l o -s u r e c o m p l i c a t i n g c o r o n a r y a n g i o p l a s t y : c l i n i ca l , a n g i o g r a p h i c , a n d t h e r a p e u t i c p r o f i l e . J A m C o l l C a r d i o l 1992; 1 9 : 9 2 6 - 9 3 5 .
20 . El l is SG, R o u b i n GS, K i n g SB III. A n g i o g r a p h i c a n d c l i n i c a l p r e d i c t o r s o f a c u t e c l o s u r e a f t e r n a t i v e vessel c o r o n a r y a n g i o p l a s t y . C i r c u l a t i o n 1988; 7 7 : 3 7 2 - 3 7 9 .
2 1 . F e y t e r PJ, R u y g r o k PN. C o r o n a r y i n t e r v e n t i o n : r isk s t r a t i f i c a t i o n a n d m a n a g e m e n t o f a b r u p t c o r o n a r y o c c l u s i o n . Eur H e a r t J 1 9 9 5 ; 1 6 : 9 7 - 1 0 3 .
22 . L i n c o f f A M , C a l i f f R M , A n d e r s o n K M , e t a l . E v i d e n c e f o r p r e v e n t i o n o f d e a t h a n d m y o c a r d i a l i n f a r c t i o n w i t h p l a t e l e t m e m b r a n e g l y c o p r o t e i n I lb / I I Ia r e c e p t o r b l o c k a d e b y a b c i x i m a b (c7E3 Fab) a m o n g p a t i e n t s w i t h u n s t a b l e a n g i n a u n d e r g o i n g p e r c u t a n e o u s c o r o n a r y r e v a s c u l a r i z a t i o n . EPIC I n v e s t i g a t o r s . E v a l u a t i o n o f 7E3 i n P r e v e n t i n g I schemic C o m p l i c a t i o n s . J A m Co l l C a r d i o l 1997 ; 3 0 : 1 4 9 - 1 5 6 .
23 . L e f k o v i t s J, I v a n h o e RJ, C a l i f f R M , e t a l . E f fec t s o f p l a t e l e t g l y c o p r o -t e i n I lb/ I I Ia r e c e p t o r b l o c k a d e b y a c h i m e r i c m o n o c l o n a l a n t i b o d y ( a b c i x i m a b ) o n a c u t e a n d s i x - m o n t h o u t c o m e s a f t e r p e r c u t a n e o u s t r a n s l u m i n a l c o r o n a r y a n g i o p l a s t y f o r a c u t e m y o c a r d i a l I n f a r c t i o n . EPIC i n v e s t i g a t o r s . A m J C a r d i o l 1996; 7 7 : 1 0 4 5 - 1 0 5 1 .
24. T o p o l EJ, F e r g u s o n JJ, W e i s m a n HF, e t a l . L o n g - t e r m p r o t e c t i o n f r o m m y o c a r d i a l i s chemic e v e n t s i n a r a n d o m i z e d t r i a l o f b r i e f I n t e g r i n b e t a 3 b l o c k a d e w i t h p e r c u t a n e o u s c o r o n a r y i n t e r v e n t i o n . EPIC I n v e s t i g a t o r G r o u p . E v a l u a t i o n o f P l a t e l e t I lb / I I Ia I n h i b i t i o n f o r P r e v e n t i o n o f I schemic C o m p l i c a t i o n . J A M A 1997 ; 2 7 8 : 4 7 9 ^ 4 8 4 .
CLEVELAND CLINIC JOURNAL OF MEDICINE V O L U M E 67 • NUMBER 2 FEBRUARY 2 0 0 0 62
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
I l b / l l l a I N H I B I T O R S R O E , S A P P , A N D L I N C O F F
R o e MT, B h a t t DL, B o o t h J. I n c r e m e n t a l b e n e f i t o f s t e n t i n g w i t h a b c i x -i m a b i r r e s p e c t i v e o f c l i n i c a l p r e s e n t a t i o n ( a b s t r a c t ] . C i r c u l a t i o n 1998 ; 98:1-572. T h e IMPACT- I I I n v e s t i g a t o r s . R a n d o m i s e d p l a c e b o - c o n t r o l l e d t r i a l o f e f f e c t o f e p t i f i b a t i d e o n c o m p l i c a t i o n s o f p e r c u t a n e o u s c o r o n a r y i n t e r v e n t i o n : IMPACT- I I . L a n c e t 1997 ; 3 4 9 : 1 4 2 2 - 1 4 2 8 . P h i l l i p s DR, T e n g W , A r f s t e n A , e t a l . E f f e c t o f c a l c i u m o n GP l l b - l l l a i n t e r a c t i o n s w i t h I n t e g r i l i n : e n h a n c e d GP l l b - l l l a b i n d i n g a n d i n h i b i -t i o n o f p l a t e l e t a g g r e g a t i o n by r e d u c t i o n s in t h e c o n c e n t r a t i o n o f i o n -i z e d c a l c i u m i n p l a s m a a n t i c o a g u l a t e d w i t h c i t r a t e . C i r c u l a t i o n 1997 ; 9 8 : 1 4 8 8 - 1 4 9 4 . T h e RESTORE I n v e s t i g a t o r s . E f fec t s o f P l a t e l e t G l y c o p r o t e i n I l b / l l l a b l o c k a d e w i t h t i r o f i b a n o n a d v e r s e c a r d i a c e v e n t s i n p a t i e n t s w i t h u n s t a b l e a n g i n a o r a c u t e m y o c a r d i a l i n f a r c t i o n u n d e r g o i n g c o r o n a r y a n g i o p l a s t y . C i r c u l a t i o n 1997 ; 9 6 : 1 4 4 5 - 1 4 5 3 . M o l i t e r n o DJ, H a r r i n g t o n RA , N e w b y KL , e t a l . La te d i v e r g i n g e v e n t c u r v e s f o r s u r v i v a l f o l l o w i n g I lb / l l l a a n t a g o n i s m in p a t i e n t s w i t h u n s t a -b l e a n g i n a : P A R A G O N s t u d y 1 - y e a r f o l l o w - u p [ a b s t r a c t ] , J A m C o l l C a r d i o l 1998; 3 1 : 2 0 8 A . R o e MT, M a r s o SP, S a p p SK, P e t e r s o n JG. E m p i r i c use o f I lb / l l l a b l o c k -a d e i n a c u t e c o r o n a r y s y n d r o m e s : e a r l y a n d d u r a b l e r e d u c t i o n i n i s c h e m i c e v e n t s w i t h e p t i f i b a t i d e i n p a t i e n t s w h o d i d n o t u n d e r g o c o r o n a r y r e v a s c u l a r i z a t i o n [ a b s t r a c t ] . C i r c u l a t i o n 1998 ; 98:1-505. M o l i t e r n o DJ, T o p o l EJ. C o n j u n c t i v e use o f p l a t e l e t g l y c o p r o t e i n I l b / l l l a a n t a g o n i s t s a n d t h r o m b o l y t i c t h e r a p y f o r a c u t e m y o c a r d i a l i n f a r c t i o n . T h r o m b H a e m o s t 1997; 7 8 : 2 1 4 - 2 1 9 . K l e i m a n NS, O h m a n E M , C a l i f f R M , e t a l . P r o f o u n d i n h i b i t i o n o f p l a t e l e t a g g r e g a t i o n w i t h m o n o c l o n a l a n t i b o d y 7E3 F a b a f t e r t h r o m -b o l y t i c t h e r a p y : Resu l ts o f t h e T h r o m b o l y s i s a n d A n g i o p l a s t y i n M y o c a r d i a l I n f a r c t i o n ( T A M I ) 8 P i l o t S tudy . J A m C o l l C a r d i o l 1993; 2 2 : 3 8 1 - 3 8 9 . O h m a n E M , K l e i m a n NS, G a c i o c h G, e t a l . C o m b i n e d a c c e l e r a t e d t i s -s u e - p l a s m i n o g e n a c t i v a t o r a n d p l a t e l e t g l y c o p r o t e i n I l b / l l l a i n t e g r i n r e c e p t o r b l o c k a d e w i t h I n t e g r i l i n i n a c u t e m y o c a r d i a l i n f a r c t i o n . Resu l ts o f a r a n d o m i z e d , p l a c e b o - c o n t r o l l e d , d o s e - r a n g i n g t r i a l . I M P A C T - A M I I n v e s t i g a t o r s . C i r c u l a t i o n 1997; 9 5 : 8 4 6 - 8 5 4 . R o n n e r E, v a n K e s t e r e n H A M , Z i j e n P, e t a l . C o m b i n e d t h e r a p y w i t h s t r e p t o k i n a s e a n d i n t e g r e l i n [ a b s t r a c t ] . J A m Co l l C a r d i o l 1998 ; 3 1 : 1 9 1 A . T h e P A R A D I G M I n v e s t i g a t o r s . C o m b i n i n g t h r o m b o l y s i s w i t h t h e p l a t e l e t g l y c o p r o t e i n I l b / l l l a i n h i b i t o r l a m i f i b a n : resu l t s o f t h e p l a t e l e t a g g r e g a t i o n r e c e p t o r a n t a g o n i s t d o s e i n v e s t i g a t i o n a n d r e p e r f u s i o n g a i n i n m y o c a r d i a l i n f a r c t i o n ( P A R A D I G M ) . J A m Co l l C a r d i o l 1998 ; 3 2 : 2 0 0 3 - 2 0 1 0 . A n t m a n E M , G i u g l i a n o RP, G i b s o n C M , e t a l . A b c i x i m a b f a c i l i t a t e s t h e r a t e a n d e x t e n t o f t h r o m b o l y s i s . Resu l ts o f T I M I 14 t r i a l . C i r c u l a t i o n 1 9 9 9 ; 9 9 : 2 7 2 0 - 2 7 3 2 . O h m a n E M , L i n c o f f A M , B o d e C, e t a l . E n h a n c e d e a r l y r e p e r f u s i o n a t 6 0 m i n u t e s w i t h l o w - d o s e r e t e p l a s e c o m b i n e d w i t h f u l l - d o s e a b c i x i m a b i n a c u t e m y o c a r d i a l i n f a r c t i o n : p r e l i m i n a r y resu l t s f r o m t h e G U S T O - 4 p i l o t (SPEED) d o s e - r a n g i n g t r i a l [ abs t rac t ] . C i r c u l a t i o n 1998; 98:1-504. A g u i r r e FV, T o p o l EJ, F e r g u s o n JJ, e t a l . B l e e d i n g c o m p l i c a t i o n s w i t h t h e c h i m e r i c a n t i b o d y t o p l a t e l e t g l y c o p r o t e i n I lb / l l l a i n t e g r i n in p a t i e n t s u n d e r g o i n g p e r c u t a n e o u s c o r o n a r y i n t e r v e n t i o n . C i r c u l a t i o n 1995 ; 9 1 : 2 8 8 2 - 2 8 9 0 . M a h a f f e y K W , H a r r i n g t o n RA, G r a f f a g n i n o C, e t a l . C o m p a r i s o n o f s t r o k e r a t e s i n p a t i e n t s w i t h a c u t e c o r o n a r y s y n d r o m e s a n d p a t i e n t s w i t h a c u t e m y o c a r d i a l i n f a r c t i o n [ a b s t r a c t ] . J A m C o l l C a r d i o l 1998 ; 3 1 : 4 0 6 A . D e c k e r s J, C a l i f f R M , T o p o l EJ, L i n c o f f A M , T c h e n g JE, S i m o o n s M L . Use o f a b c i x i m a b ( R e o p r o ) is n o t assoc ia ted w i t h a n i n c r e a s e in t h e r isk o f s t r o k e : o v e r v i e w o f t h r e e r a n d o m i z e d t r i a l s [ a b s t r a c t ] . J A m Col l C a r d i o l 1997 ; 2 9 : 2 4 1 A . B o o t h J, P a t e l VB , B a l o g C, e t a l . Is b l e e d i n g r isk i n c r e a s e d in p a t i e n t s u n d e r g o i n g u r g e n t c o r o n a r y bypass s u r g e r y f o l l o w i n g a b c i x i m a b ? [ a b s t r a c t ] C i r c u l a t i o n 1 9 9 8 ; 98:1-845. G i u g l i a n o RP, H y a t t RRJ. T h r o m b o c y t o p e n i a w i t h GP I l b / l l l a i n h i b i t o r s : a m e t a ana l ys i s [ a b s t r a c t ] . J A m C o l l C a r d i o l 1998 ; 3 1 : 1 8 5 A . K e r e i a k e s DJ, Essel l JH, A b b o t t s m i t h CW, B r o d e r i c k T M , R u n y o n JP. A b c i x i m a b - a s s o c i a t e d p r o f o u n d t h r o m b o c y t o p e n i a : t h e r a p y w i t h
i m m u n o g l o b u l i n a n d p l a t e l e t t r a n s f u s i o n . A m J C a r d i o l 1996 ; 7 8 : 1 1 6 1 - 1 1 6 3 .
44 . B e r k o w i t z SD, H a r r i n g t o n RA, R u n d M M , T c h e n g JE. A c u t e p r o f o u n d t h r o m b o c y t o p e n i a a f t e r c7E3 Fab ( a b c i x i m a b ) t h e r a p y . C i r c u l a t i o n 1997 ; 9 5 : 8 0 9 - 8 1 3 .
45 . B e r k o w i t z SD, H a r r i n g t o n RA , R u n d M M , T c h e n g JE. A c u t e p r o f o u n d t h r o m b o c y t o p e n i a a f t e r c7E3 ( a b c i x i m a b ) t h e r a p y [ l e t t e r ] . C i r c u l a t i o n 1997 ; 9 6 : 3 8 1 0 .
46 . T c h e n g JE, K e r e i a k e s DJ, B r a d e n G A , e t a l . S a f e t y o f a b c i x i m a b r e t r e a t -m e n t — f i n a l c l i n i ca l r e p o r t o f t h e r e o p r o r e a d m i n i s t r a t i o n r e g i s t r y (R3) [ a b s t r a c t ] . C i r c u l a t i o n 1998 ; 98:1-17.
4 7 . M a r k DB, T a l l e y JD, T o p o l EJ, e t a l . E c o n o m i c assessmen t o f p l a t e l e t g l y c o p r o t e i n I l b / l l l a i n h i b i t i o n f o r p r e v e n t i o n o f i s c h e m i c c o m p l i c a t i o n s o f h i g h - r i s k c o r o n a r y a n g i o p l a s t y . EPIC I n v e s t i g a t o r s . C i r c u l a t i o n 1 9 9 6 ; 9 4 : 6 2 9 - 6 3 5 .
48 . G o k l a n e y A K , M u r p h y JD, H i l l e g a s s Jr. W B . A b c i x i m a b t h e r a p y i n p e r -c u t a n e o u s i n t e r v e n t i o n : e c o n o m i c issues i n t h e U n i t e d Sta tes . A m H e a r t J 1998 ; 135 :S90 -S97 .
49 . v a n H o u t BA , B o w m a n L, Z e l i n g e r DJ, S i m o o n s M L . Costs a n d e f f e c t s i n t h e r a p y f o r a c u t e c o r o n a r y s y n d r o m e s : t h e case o f a b c i x i m a b i n h i g h - r i s k p a t i e n t s u n d e r g o i n g p e r c u t a n e o u s t r a n s l u m i n a l c o r o n a r y a n g i o p l a s t y in t h e EPIC s t u d y . A m H e a r t J 1998 ; 1 3 5 : S 9 8 - S 1 0 6 .
50. C o h e n M , D e m e r s C, G u r f i n k e l EP, e t a l . A c o m p a r i s o n o f l o w - m o l e c u -lar w e i g h t h e p a r i n w i t h u n f r a c t i o n a t e d h e p a r i n f o r u n s t a b l e c o r o n a r y a r t e r y d isease . E f f i cacy a n d S a f e t y o f S u b c u t a n e o u s E n o x a p a r i n i n N o n - Q - W a v e C o r o n a r y E v e n t s S t u d y G r o u p . N e w E n g l J M e d 1997 ; 3 3 7 : 4 4 7 - 4 5 2 .
51. T h e T I M I 1 1 A I n v e s t i g a t o r s . D o s e - r a n g i n g t r i a l o f e n o x a p a r i n f o r u n s t a b l e a n g i n a : r e s u l t s o f T I M I 1 1 A . J A m C o l l C a r d i o l 1 9 9 7 ; 2 9 : 1 4 7 4 - 1 4 8 2 .
52. M e r l i n i PA, B a u e r K A , O l t r o n a L, e t a l . P e r s i s t e n t a c t i v a t i o n o f t h e c o a g u l a t i o n s y s t e m i n u n s t a b l e a n g i n a a n d m y o c a r d i a l i n f a r c t i o n . C i r c u l a t i o n 1994; 9 0 : 6 1 - 6 8 .
53. V a n Be l l e E, L a b l a n c h e J M , B a u t e r s C, R e n a u d N, M c F a d d e n EP, B e r t r a n d M E . C o r o n a r y a n g i o s c o p i c f i n d i n g s i n t h e i n f a r c t - r e l a t e d ves-sel w i t h i n 1 m o n t h o f a c u t e m y o c a r d i a l i n f a r c t i o n : n a t u r a l h i s t o r y a n d t h e e f f e c t o f t h r o m b o l y s i s . C i r c u l a t i o n 1998; 9 7 : 2 6 - 3 3 .
54. S m a l l i n g RW, A n d e r s o n HV. P a t h o p h y s i o l o g i c a l i n s i g h t i n t o t h e poss i -b l e o p t i m a l t h e r a p i e s f o r a c u t e m y o c a r d i a l i n f a r c t i o n a n d u n s t a b l e a n g i n a . C i r c u l a t i o n 1998; 9 7 : 1 0 - 1 1 .
55. C a n n o n CP, M c C a b e CH, B o r z a k S, e t a l . R a n d o m i z e d t r i a l o f a n o r a l p l a t e l e t g l y c o p r o t e i n I l b / l l l a a n t a g o n i s t , s i b r a f i b a n , in p a t i e n t s a f t e r a n a c u t e c o r o n a r y s y n d r o m e : r esu l t s o f t h e T I M I 12 t r i a l . C i r c u l a t i o n 1998 ; 9 7 : 3 4 0 - 3 4 9 .
56. T h e S Y M P H O N Y I n v e s t i g a t o r s A r a n d o m i z e d c o m p a r i s o n o f s i b r a f i b a n , a n o r a l p l a t e l e t g l y c o p r o t e i n I l b / l l l a r e c e p t o r a n t a g o n i s t , w i t h a s p i r i n f o r a c u t e c o r o n a r y s y n d r o m e s . L a n c e t . In press.
57. K e r e i a k e s DJ, K l e i m a n NS, F e r g u s o n JJ, e t a l . P h a r m a c o d y n a m i c e f f i c a -cy, c i i n i ca i sa fe t y , a n d o u t c o m e s a f t e r p r o l o n g e d p i a t e i e t g l y c o p r o t e i n I lb / l l l a r e c e p t o r b l o c k a d e w i t h o r a l x e m i l o f i b a n . C i r c u l a t i o n 1 9 9 8 ; 9 8 : 1 2 6 8 - 1 2 7 8 .
58. M o r r i s DC. Resu l ts f r o m l a t e - b r e a k i n g c l i n i c a l t r i a l s sess ions a t ACCIS ' 9 9 a n d A C C '99 . J A m Co l l C a r d i o l 1999 ; 3 4 : 1 - 8 .
59. D e e d w a n i a PC, F e r g u s o n JJ, K e r e i a k e s DJ, e t a l . S u s t a i n e d p l a t e l e t GP I l b / l l l a b l o c k a d e w i t h o r a l o r b o f i b a n : i n t e r i m s a f e t y a n d t o l e r a b i l i t y resu l t s o f t h e S O A R s t u d y [ a b s t r a c t ] . J A m Co l l C a r d i o l 1998 ; 3 1 : 9 4 A .
60. B r a u n w a l d E, M a s e r i A , A r m s t r o n g PW, e t a l . R a t i o n a l e a n d c l i n i c a l e v i d e n c e f o r t h e use o f GP I l b / l l l a i n h i b i t o r s i n a c u t e c o r o n a r y syn-d r o m e s . A m H e a r t J 1998 ; 135 :S56 -S66 .
61. V o r c h h e i m e r D A , F u s t e r V. O r a l p l a t e l e t g l y c o p r o t e i n I l b / l l l a r e c e p t o r a n t a g o n i s t s : t h e p r e s e n t c h a l l e n g e is sa fe t y . C i r c u l a t i o n 1 9 9 8 ; 9 7 : 3 1 2 - 3 1 4 .
62. H a m m CW, H e e s c h e n C, G o l d m a n n BU, B a r n a t h a n E, S i m o o n s M L . V a l u e o f t r o p o n i n s i n p r e d i c t i n g t h e r a p e u t i c e f f i c a c y o f a b c i x i m a b i n p a t i e n t s w i t h u n s t a b l e a n g i n a [ a b s t r a c t ] . J A m Co l l C a r d i o l 1998 ; 3 1 : 1 8 5 A .
ADDRESS: A. Michael Lincoff, MD, Department of Cardiology, Desk F25, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail [email protected].
63 CLEVELAND CLINIC JOURNAL OF MEDICINE V O L U M E 67 • NUMBER 2 FEBRUARY 2 0 0 0
on November 26, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

























![ILB brochure [PDF - 18 MB]](https://static.documents.pub/doc/80x56/5870a9331a28ab962d8b5b19/ilb-brochure-pdf-18-mb.jpg)