23
UW MEDICINE │ 2015 Legislative Staff Tour GME FUNDING: 2015 LEGISLATIVE STAFF TOUR AMITY NEUMEISTER, MBA, RYT ASSISTANT DEAN, GRADUATE MEDICAL EDUCATION AUGUST 11, 2015
UW MEDICINE │ 2015 Legislative Staff Tour
GME FUNDING:2015 LEGISLATIVE STAFF TOUR
AMITY NEUMEISTER, MBA, RYTASSISTANT DEAN, GRADUATE MEDICAL EDUCATION
AUGUST 11, 2015
• The UW GME Enterprise• How is GME funded nationally?
• CMS, HRSA, VA, THC• Detail on Medicare payments• UW Medicine GME funding
AGENDA
2
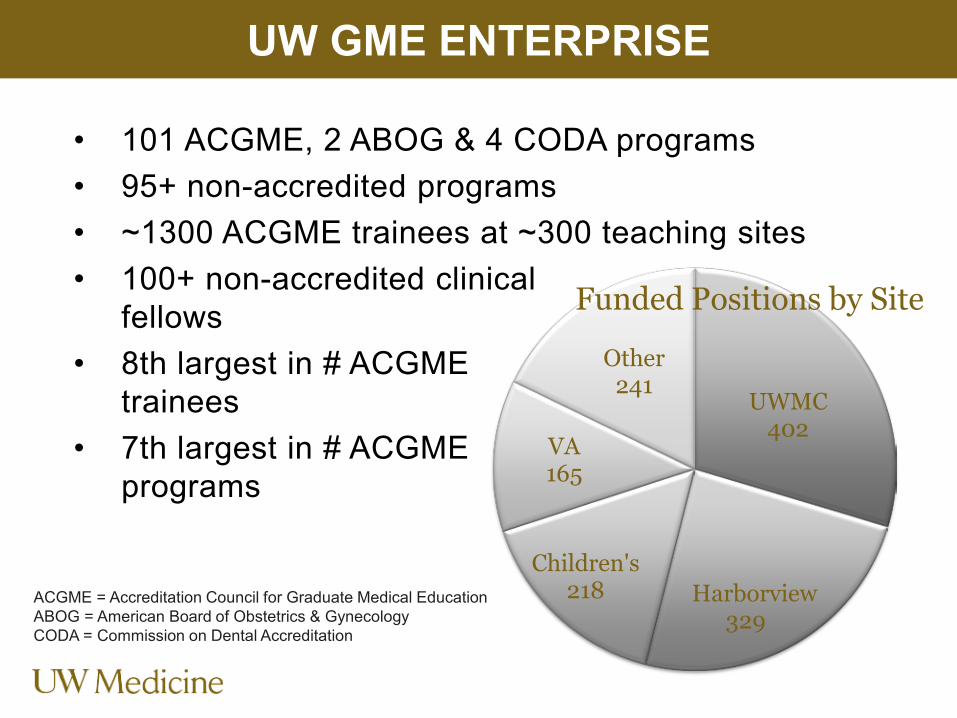
• 101 ACGME, 2 ABOG & 4 CODA programs• 95+ non-accredited programs• ~1300 ACGME trainees at ~300 teaching sites• 100+ non-accredited clinical
fellows• 8th largest in # ACGME
trainees• 7th largest in # ACGME
programs
UW GME ENTERPRISE
UWMC402
Harborvie329
Children's218
VA165
Other241
w
Funded Positions by Site
ACGME = Accreditation Council for Graduate Medical EducationABOG = American Board of Obstetrics & GynecologyCODA = Commission on Dental Accreditation
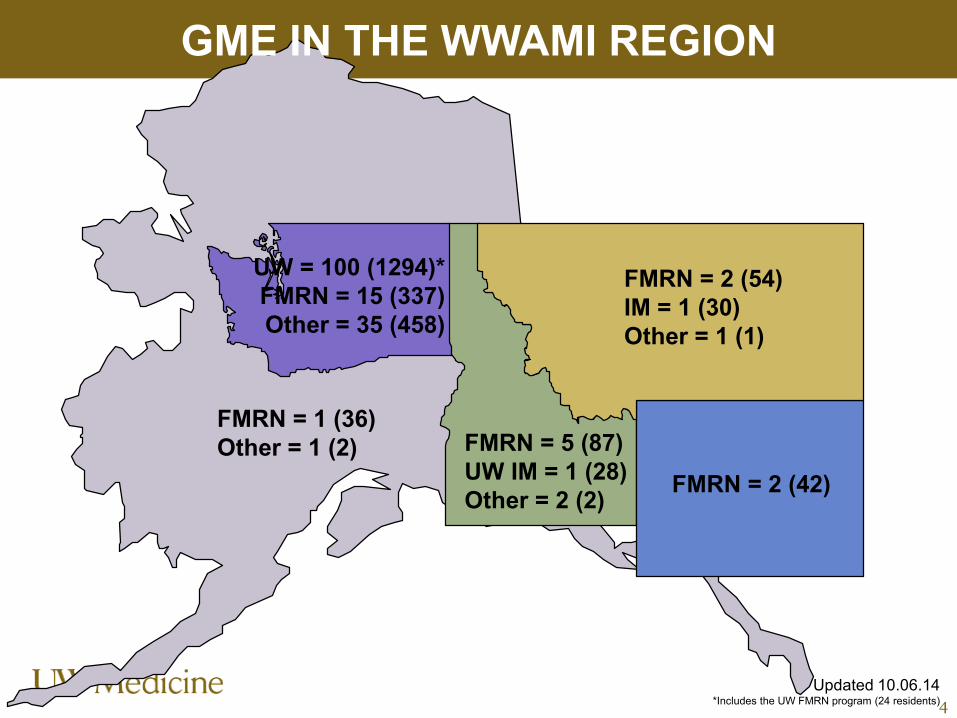
GME IN THE WWAMI REGION
4
FMRN = 1 (36)Other = 1 (2)
UW = 100 (1294)*FMRN = 15 (337)Other = 35 (458)
FMRN = 2 (54)IM = 1 (30)Other = 1 (1)
FMRN = 2 (42)FMRN = 5 (87)UW IM = 1 (28)Other = 2 (2)
Updated 10.06.14*Includes the UW FMRN program (24 residents)
Average cost to train a resident=
$152,000+ per year
5Source: AAMC’s What Does Medicare Have to Do With Graduate Medical Education?
How is GME funded nationally?
6

GME FUNDING SOURCES
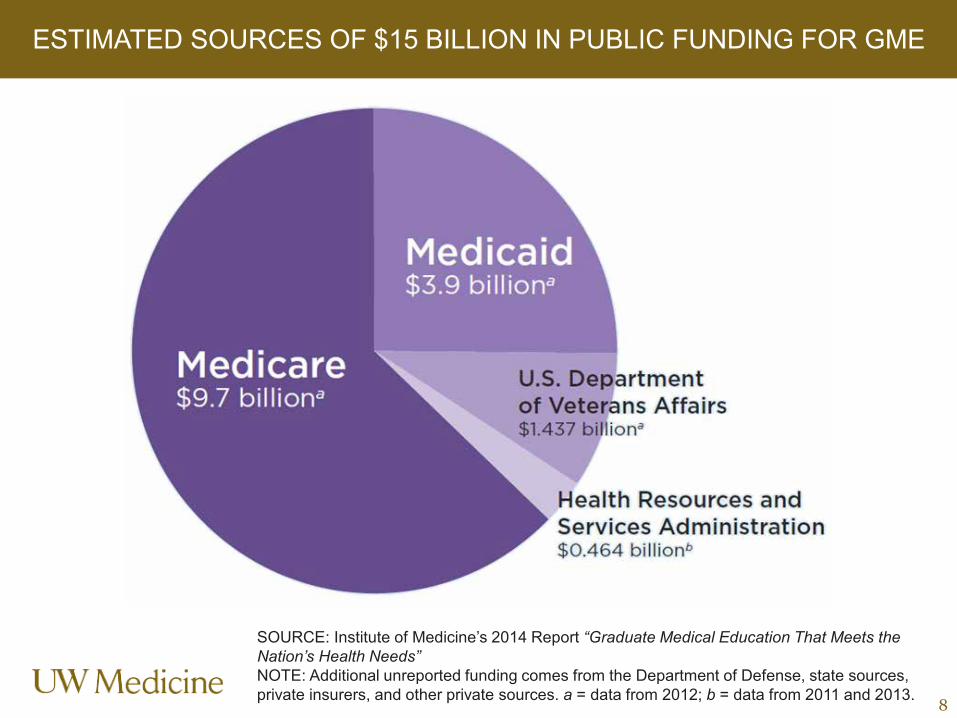
ESTIMATED SOURCES OF $15 BILLION IN PUBLIC FUNDING FOR GME
8
SOURCE: Institute of Medicine’s 2014 Report “Graduate Medical Education That Meets the Nation’s Health Needs” NOTE: Additional unreported funding comes from the Department of Defense, state sources, private insurers, and other private sources. a = data from 2012; b = data from 2011 and 2013.
• Single largest funder of GME nationally• Goal: To pay for Medicare’s share of GME
costs, based on portion of hospital expenses related to Medicare patients
• Covers: Direct & Indirect expenses through Medicare Cost Report
• Sites: Adult teaching hospitals and limited non-hospital sites
MEDICARE FUNDING
6
• Medicaid payments in Alaska, Idaho Montana & Washington made under Fee-For-Service program
• Methodology varies by state (less than 5% of funding in WA)
MEDICAID FUNDING
10
• Goal: To enhance the quality of care provided to Veterans
• Covers: Direct & Indirect costs through Disbursement Agreement & VERA payments
• Sites: 124 VA hospitals, CBOCs, IOCs, limited community-based outpatient clinics
VETERANS AFFAIRS (VA) FUNDING
11
CBOCs: Community-based Outpatient Clinics, IOCs = Independent Outpatient Clinics,Direct: (resident stipends & fringe benefits), Indirect: (attending contributions, VA Program Administration, higher complexity care), VERA = Veterans Equitable Resource Allocation
• Goals: Enhance research capabilities & care for vulnerable and underserved children
• Covers: CHGME payments for Direct & Indirect GME expenses through annual initial & reconciliation application process
• Sites: 54 Children’s hospitals
HRSA FUNDING
12
HRSA: Health Resources and Services Administration, CHGME: Children’s Hospitals GME, Direct expenses = stipends for residents, salaries, salaries for faculty, overhead, Indirect expenses = reduced productivity and clinical inefficiencies
• $230 million, 5-year ACA initiative to increase primary care residents in community-based settings
• Goals: Increase access to the geographically isolated, economically or medically vulnerable
• Covers: Direct and indirect medical education expenses
• Sites: FQHCs & FQHC Look-Alikes, community mental health centers, rural health clinics, IHS or Tribal clinics, and Title X clinics (family planning clinics)
TEACHING HEALTH CENTER (THC) FUNDING
13
ACA = Affordable Care Act, FQHC = federally qualified health centers, IHS = Indian Health Service
Detail on Medicare payments
14
Hospital-specific, base-period per resident amount (PRA) to cover direct costs incurred by teaching hospitals:• Salaries and fringe benefits of residents• Salaries and fringe benefits of supervising
faculty• Institutional overhead costs (e.g., programs’
budgets, program director/administrator time)• GME Office staff
MEDICARE DME (DGME) FUNDING
DME/DGME = Direct (Graduate) Medical Education
An additional payment based on the “IME adjustment factor”• Additional costs associated with the teaching of
residents (e.g., clinical inefficiencies)• Severity of illness (patients require specialized
services and treatment programs)• Formula based on the resident-to-bed ratio
(different formula for rehab & psych units)
MEDICARE IME FUNDING
c x [(1 + r).405 - 1]
IME = Indirect Medical Education
Approved programs• ACGME, AOA, CODA, CPME and ABMS• Others that lead to board certificationLocation• Hospital-based • Non-hospital-based if hospital pays 100% of the costsResidency level & type• Initial Residency Period (IRP) = 1.0 FTE DME & IME• After IRP = 0.5 FTE DME/1.0 FTE IME • Gero, child neuro & prev med = 1.0 FTE for IRP + 2 yrs
“ALLOWABLE” GME EXPENSES
ACGME: Accreditation Council for Graduate Medical Education, AOA: American Osteopathic Association), CODA: Commission on Dental Accreditation, CPME: Council on Podiatric Medical Education
“ALLOWABLE” GME EXPENSES
Activity type• Patient care• Didactics • Non-patient specific research (DME only)• Patient specific research (difficult to track)
Resident cap• 1997 Balanced Budget Act• Dental and podiatry programs exempt• Adjustments allowed (e.g., affiliated groups, closed
hospitals, redistribution)
UW Medicine GME funding
19
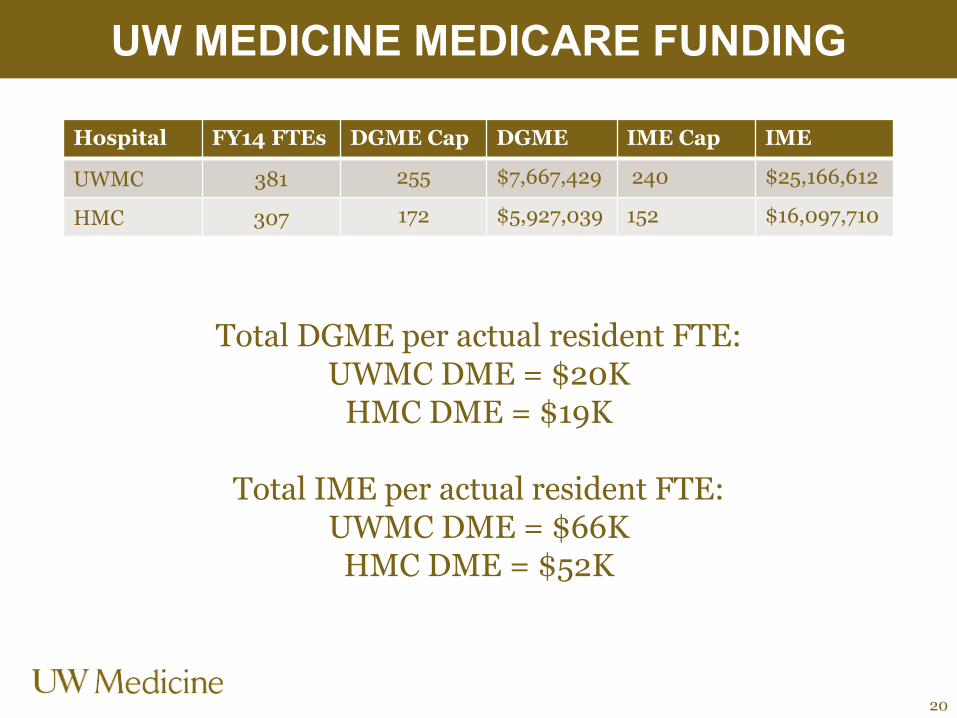
Hospital FY14 FTEs DGME Cap DGME IME Cap IME
UWMC 381 255 $7,667,429 240 $25,166,612
HMC 307 172 $5,927,039 152 $16,097,710
UW MEDICINE MEDICARE FUNDING
20
Total DGME per actual resident FTE:UWMC DME = $20K
HMC DME = $19K
Total IME per actual resident FTE:UWMC DME = $66KHMC DME = $52K
Average cost to train a resident=
$152,000+ per year
21Source: AAMC’s What Does Medicare Have to Do With Graduate Medical Education?
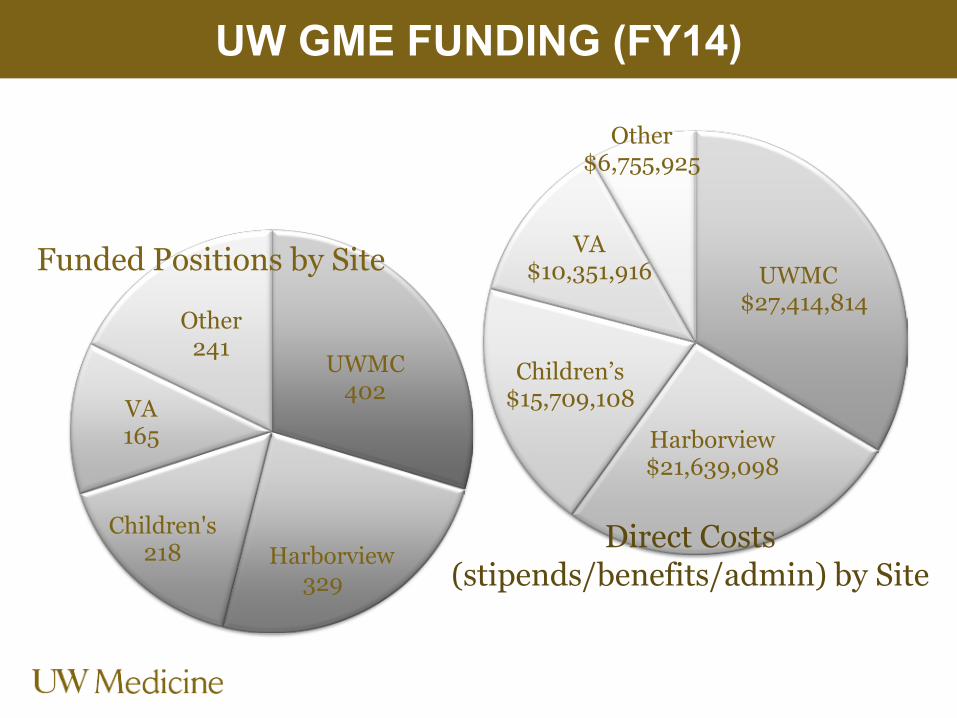
UWMC$27,414,814
Harborview$21,639,098
Children’s$15,709,108
VA$10,351,916
Other$6,755,925
UW GME FUNDING (FY14)
UWMC402
Harborvie329
Children's218
VA165
Other241
w
Funded Positions by Site
Direct Costs (stipends/benefits/admin) by Site
Questions?
23

















