God, Sex, & Germs: Obsessive Compulsive Disorder in Children January 23, 2010 Penn State Cooperative Extension Early Childhood Education & Care Professionals Conference, State College, PA Marolyn Morford, PhD Center for Child and Adult Development State College, PA
Transcript
God, Sex, & Germs:Obsessive Compulsive
Disorder in Children
January 23, 2010Penn State Cooperative Extension
Early Childhood Education & Care Professionals Conference, State College, PA
Marolyn Morford, PhDCenter for Child and Adult Development
State College, PA
Clinical examples
How childhood OCD might first appear
Eczema (from handwashing) Skin lesions (skin picking) Bathroom problems (from fear of contamination) Ordering others, including adults Teacher complaints about not completing work,
time out of classroom, excessive erasing Child complains that s/he can’t stop doing
something Child asks the same or similar question over
(and over)
OCD is an Anxiety Disorder
Anxiety disorders are the most common mental health problems affecting both children and adults.
An estimated 19 million adult Americans and children suffer from anxiety disorders
Types of anxiety disorders found in children
Separation anxiety disorder Post traumatic stress disorder Phobias Panic disorder Social anxiety disorder Generalized anxiety disorder Obsessive-compulsive disorder
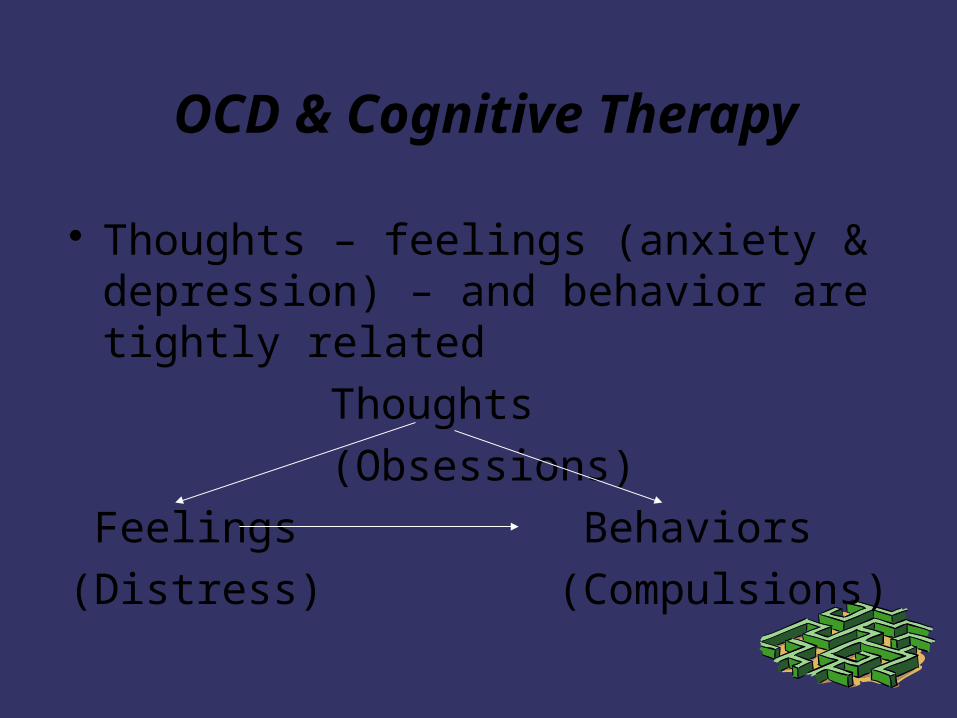
Thoughts that trigger high anxiety (fear, disgust, doubt, feeling something incomplete)
Obsessions: recurrent, persistent thoughts, impulses, images, considered intrusive, inappropriate, cause anxiety and distress; not simply excessive worries about real life problems; person tries to suppress them with some other thought or action, recognizes that they are a product of own mind
Obsessive-Compulsive Disorder, definition, cont.
Behaviors or mental actions (covert) done to get rid of 'bad thought', reduce the anxiety
Compulsions: repetitive behaviors (hand-washing, ordering, checking), mental acts (praying, counting, repeating words) that person is driven to perform in response to an obsession, or according to rules that must be applied; behaviors/acts are aimed at preventing or reducing distress or a dreaded event, but are not realistically connected
All repeating behavior is not OCD
Differs from normal temporary worries or needs for sameness that some children have (bedtime rituals, lining up toys)
To differentiate, identify Developmental stage of child The relationship between the thought and the
behavior The content of the thought or image (seems
‘bizarre’) The severity and breadth of impairment
Obsessive-Compulsive Disorder, definition, cont.
Person recognizes that obsessions and compulsions are not reasonable (does not apply to children)
Obsessions/compulsions cause distress, are time consuming (>1 hour/day), or significantly interfere with normal routine, job, school, social activities, relationships
“Functional impairment”
Time lost to obsessions and compulsions Cause distress (for children or perhaps only
to family) Avoidance of situations likely to prompt
obsessions Diminished concentration Withdrawal from social contact, interfere with
school, social activities, or important relationships
Criteria of insight is waived for children
Contamination Compulsions: Washers/cleaners
Situations that cause distress: anything that might be contaminated (toilets, garbage, bodily fluids, school desk seat, shoes, paper on a floor, a doorknob, markers, public salt/pepper shakers)
Thoughts/Images: ”NO!” “I am contaminated/dirty”, “I haven’t gotten it all off”, “I/someone else will become contaminated (or die) if I am not clean”, “I can’t stand this, I’ll go crazy”
Checkers
Situations that cause distress: making a mistake (writing the wrong word or number, writing something incriminating), leaving home, eating food (without checking it), putting homework in backpack, identifying correct assignment
Thoughts/Images: “Did I do the right assignment? “Did I accidentally leave water running?” “Did I take the right book?” “Did I put the right name on the paper?” “Is there glass in this food? Did I put it there?” “Do I have my phone?”
Repeaters
Situations that cause distress: Not doing something the ‘right’ number of times, leaving/entering a room, doing things the ‘wrong’ way
Thoughts/Images: “My father will have an accident/parents will die”, “I am a bad person” “I must do this the right way”, “The teacher wants it a certain way” (and not able to identify clearly)
Orderers
Situations that cause distress: Objects not placed in exact order/sequence (pillows, clothing, pencils, collections), asymmetry
Thoughts/Images: “Things are out of place” “Things are touching each other the wrong way” “This is not right” “I will go crazy if this is not fixed”
Hoarders
Situations that cause distress: throwing things away, change to one’s collection, removal of a part of something, leaving something somewhere
Thoughts/Images: “What if I need this and I don’t have it, what will I do then?” “What if I can’t find it?” “I will go crazy if I cannot keep this” “I have to have this”
Pure Obsessionals (Worriers, Thinking Ritualizers)
Situations that cause distress: Any situation in which harm could come to someone, a situation in which the child could make a ‘bad’ mistake or decision, any other place or event that, for the child, produces distressing thoughts
Thoughts/Images: Self-criticism and criticism from others, “I’ve made mistake/I did that all wrong” “Something terrible will happen” “Something I do/don’t do will harm someone” “The world is dangerous” “I will never get better” “I had sex with my cousin when I was 5” “What if I’m gay?” “I’m going to kiss her/she’s going to touch me”
Childhood OCD
Prevalence is estimated at 1-3% of population, or 1-3 in 100 children and adolescents 6-8 in an avg elementary school; ~40 in a high
school Ratio of males to females higher in preteens
then equalizes Early identification and intervention may
prevent behavioral restrictions and impairments that affect later development
Childhood OCD, cont.
Boys more likely To have prepubertal onset To have a family member with OCD or
Tourette’s syndrome To show tic-like symptoms
Girls more likely To have onset during adolescence To have more phobic symptoms
Childhood OCD, cont.
Frequently unidentified or untreated, called “the hidden epidemic” (Jenike, 1989) Child secretiveness and lack of insight Community lack of familiarity with diagnosis Clinician lack of familiarity or unwillingness to
use proven treatments Lack of access to treatment resources Behaviors & thoughts are often ‘ego syntonic’
Childhood OCD characteristics
Obsessions and/or compulsions Obsessions are distressing, intrusive, often
more to family than to the child Content can be very unusual and frightening to
both the child and the adult who hears about it, therefore often misdiagnosed or overlooked
Insight about the problem can range from very good to poor or absent
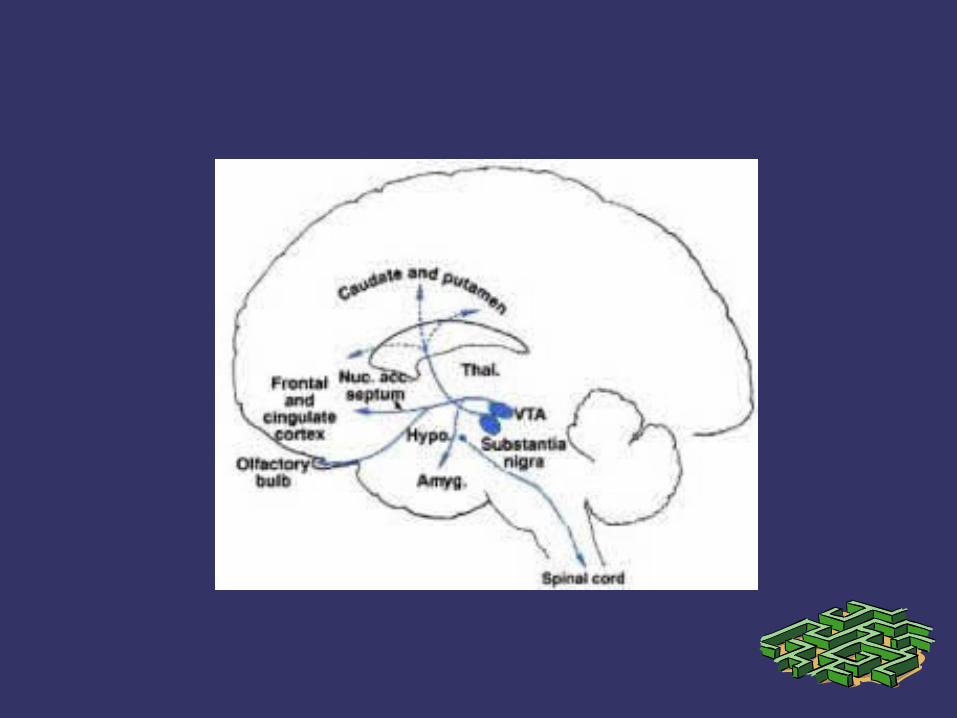
Neuroimaging studies implicate abnormal basal ganglia*/frontostriatal pathways, that show response to treatment; amygdala implicated
*caudate nucleus, putamen, substantia nigra, globus pallidus – organize muscle driven motor movements of body
Nature of many of the compulsions (licking, picking, washing, evening up), joined with trichotillomania (hair pulling) led to hypothesis of OCD as “grooming behavior gone awry”
Family genetic studies show OCD and TS may represent alternate expressions of same gene
PANDAS: Pediatric Autoimmune Neuropsychiatric
Disorders Associated with Strep Sudden or dramatic OCD symptom and/or tic
Sydenham’s chorea (neurological variant of rheumatic fever) – symptoms are tic-like writhing in extremities
Not characteristic of most childhood OCD
Developmental Course
Symptoms can change over time Can have more than one symptom at a time Approximately 50% of adult OCD sufferers
experienced childhood onset Complete remission rate in 10-50% of children
by late adolescence (varies by study) Unknown : the course or exact experience of
OCD in childhood
6 most common obsessions in childhood OCD
Concern with dirt, germs, or toxins Concern that something terrible will
happen such as fire, illness, death, murder Symmetry order, or exactness Scrupulosity (religious obsessions) Sexual themes Concern about bodily waste, secretions
6 most common compulsions in childhood OCD
Excessive or ritualized handwashing, showering, toothbrushing, other grooming
Repeating by going in & out of door or up & down from chair, erasing, rereading
Checking doors, locks, stove, homework Rituals to remove contact w/contaminants
(eating, sitting, touching) Ritual touching or pattern of tapping Reassurance seeking (repetitive
questioning)
Some observations from my office
Distress of involved parent Of 95 children (under 18) with an anxiety
disorder of some type seen over 3.5 years, 23 (24%) were diagnosed with OCD
Of those 23, 18 (78%) were first seen before 13 years of age in my office.
11 (61%) of these 18 were male
What I see regarding young children’s obsessions or rituals :
Ordering/Need for order of sequence of events of day/Need to order others’ behavior
Self contamination worries and avoidances: eating, sitting, touching
Repeating behaviors: mostly verbal repetition, typically questions
Confessing behaviors have to do with offending God, sexual thoughts, or thoughts of having harmed someone
Sexual thoughts described by children 10 and up; sexual-like behaviors in two 8 y.o. females
Preoccupation w/danger & doubt
Other problems
Eating behaviors or conditions for eating Tactile hypersensitivities: avoidance of
restrictions on body Most have indications of hyperarousal
(anxiety) Most have tantrums Most have sleep onset or maintenance
problems
Family involvement & symptoms
History of parental compensation ‘Frog in the pot’
Parent distress
Examples: buying & preparing ‘safe’ foods, buying acceptable socks, allowing more time in bathroom (for rituals), responding to questions, ritual demands, requests for reassurance
How can I tell it's OCD?
Never begin an evaluation looking for one category or diagnosis, use general assessment diagnostic tools
Clinical interview Instruments
Clinical Interview
Distress of parent “I’m walking on eggshells” “I don’t have a life
anymore” “I can’t stand my child much of the time” “S/he’s always trying to control me” “S/he tantrums about everything” “I haven’t slept solidly for years” “S/he just won’t stop”
Child concerns “My parents are always mad at me” “I can’t
stop” “I don’t have any control over this” Listen, ask child & parents to describe minutely
each of their experience (‘mapping OCD’)
Diagnostic Procedure
*NIMH/Children’s Yale Brown OCS Therapeutic nature of this interview
➲ Preventing the response (ritual): Wait longer Walk away, go somewhere else Limit where, when, and how long you do it Change the ritual (invite the worry thought in) Do the opposite of what you're being told to do Do something else you like to do Make it funny, ridiculous
Cognitive Behavioral Therapy
➲ Talking back to OCD➲ Name it, separate it from the rest of you➲ Label it (“bossy”)➲ Call it out: “That's my OCD!”➲ Practice having the thought on purpose,
to get away from the fear from “thought-action fusion”
Behavioral Therapy
Trigger the child's obsessions and fears, encourage them NOT to do the compulsion
Exposure and Ritual Prevention (E/RP)– “…blah, blah, blah..do the thing you’re afraid
of…” [or, NOT do it]– “…blah, blah, blah..the more you do it the
easier it gets.”
Gwen Franklin, Age 6
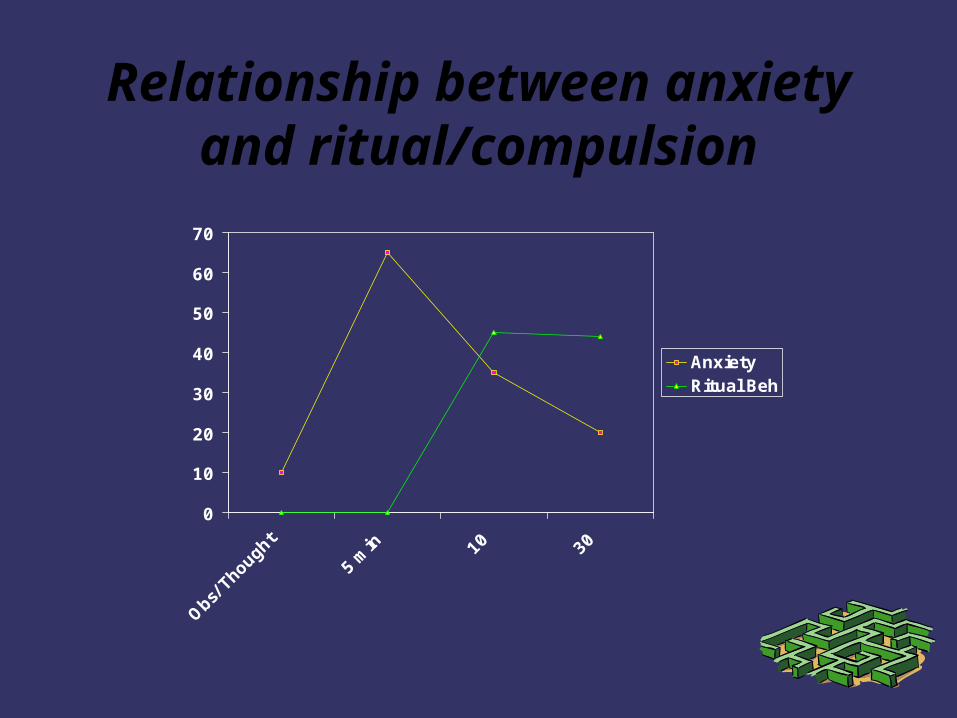
Conceptualization behind E/RP
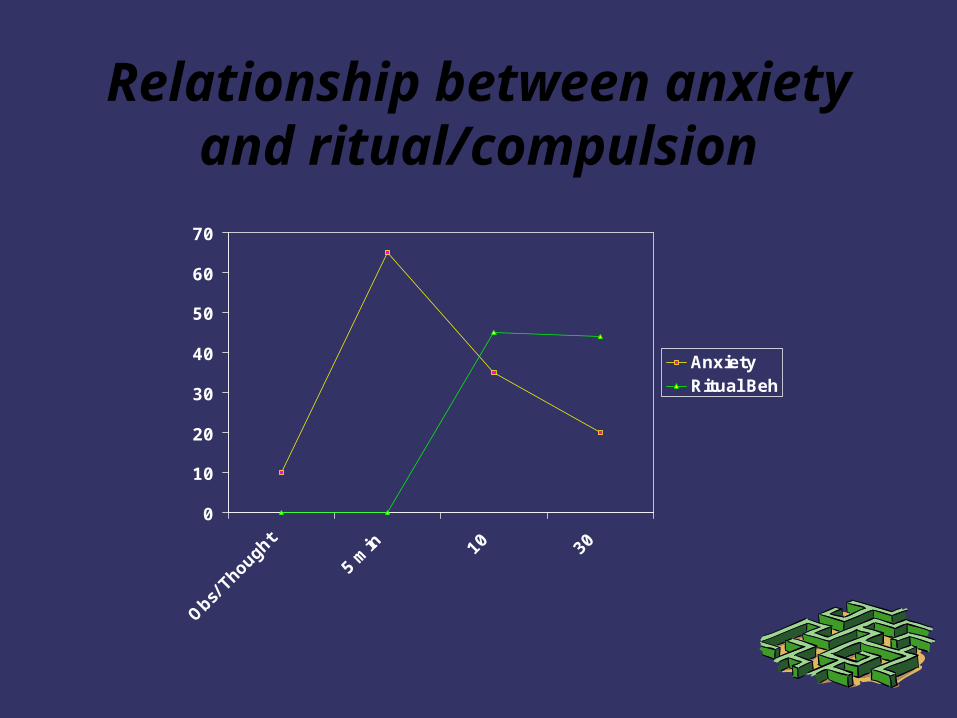
An association has been made between the ritual and the obsession. The conclusion is that the ritual will take away the anxiety associated with the obsession and prevent the catastrophe that is often assumed will happen. In the absence of contradictory experience, this link is reinforced and strengthened every time the pairing occurs.
Relationship between anxiety and ritual/compulsion
0
10
20
30
40
50
60
70
Obs/ T
houg
ht
5 min 10 30
AnxietyRitual Beh
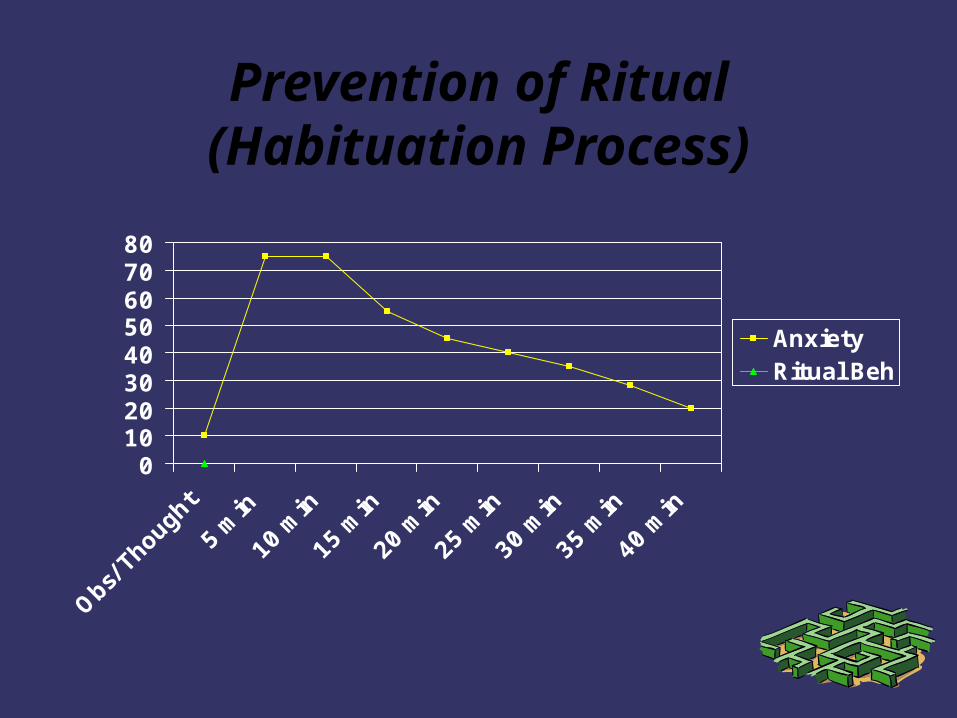
Prevention of Ritual(Habituation Process)
01020304050607080
Obs/ T
houg
ht
5 min
10 m
in
15 m
in
20 m
in
25 m
in
30 m
in
35 m
in
40 m
in
AnxietyRitual Beh
Anxiety Hierarchies and SUDS List stressful situations Develop awareness of triggers *Self-monitoring of thoughts/behaviors Competing responses: what else can you
do besides the compulsion?
Identify Subjective Units of Distress How to do this with children – develop a
vocabulary Arrange stressful events/situations by
hierarchy level: difficult with young children, consult with parents
Relaxation training
Imaginal (pretend) exposure/Response delay
In vivo (real) exposure/Response delay Overpracticing/Changing the response Competing responses: what else can you
do?
CBT & the family
Help child to “talk back” to OCD Positive self statements “There’s my OCD
again; I’m not going to let it ruin this day” “I will control my OCD, it won’t control me” “If I can’t remember it, it didn’t happen”
Accepting the obsession: Reducing the desire to avoid or run away from the obsession – Practicing this with the child
Paradoxical effect: The more you fight it, the more frequent and intense it can become
CBT & the family
Helping child to consider that other behaviors can reduce distress – teach flexibility
Help child to examine thoughts: “What is the probability that I had sex with my dog and no one saw me?” “Has anyone else ever touched that door handle without getting sick?” “How will my worry keep my parents safe?” “What can I do if my mother never comes home?”
CBT & the family and other important adults
***Unhook from the rituals and compulsions (gently refuse to participate) Address parents’ catastrophic thoughts Reframe their lack of response as helpful
Encourage cheerleading – lots of positive acknowledgement for achievements
Rewards for related behaviors
CBT & the family & others
Instruct parents to talk to the child with the confidence that they know child can triumph over their OCD (but acknowledge the challenge)
Model this for parents Keep an eye out for activities that allow
happiness (“flow”) and permit little time for rumination or rituals
What makes them happy? Make sure more of that can happen.
Conclusions
OCD is frequently missed or misdiagnosed in young children: Don’t ask & I won’t tell and the Fear Factor
OCD is a chronic vulnerability that can be managed (consider a diabetes model)
Anxiety is the primary dysfunction We are poorly informed about the nature and
course of OCD in children Special problems with diagnosing & treating
OCD in very young children
Unanswered questions:OCD thought content & developmental course
Is the thought content appreciably different from adult thought content?
What exactly is the variation of representation of thought content? Can the presence of unusual thought content, say, an 8 year old with disturbing sexual thoughts, be significant for an OCD diagnosis?
Is there a gender difference in content or preferred compulsion?
How long is a period of ‘remission’, is it related to age? To type of obsession or compulsion?
References
Christophersen, E.R. & Mortweet, S. (2002). Treatments that Work with Children: Empirically Supported Strategies of Managing Childhood Problems. Wash. D.C.: APA.
Foa, E. & Wilson, R. (2001). Stop Obsessing! How to overcome your obsessions & compulsions. NY: Bantam.
Franklin, M. et al. (2003). Treatment of obsessive-compulsive disorder. In Reinecke et al. Cognitive Therapy with Children & Adolescents. NY: Guilford.
March, J. & Mulle, K. (1998). OCD in Children & Adolescents: A cognitive-behavioral treatment manual. NY: Guilford.
Morris, T. & March, J. (2004). Anxiety Disorders in Children & Adolescents, 2nd Ed. NY: Guilford Press.
Swinson, R. P. et al. (1998). Obsessive Compulsive Disorder: Theory, Research, and Treatment. NY: Guilford Press.
Anxiety Disorders Association of America
ADAA www.adaa.org Obsessive Compulsive Foundation
www.ocfoundation.org www.bpchildresearch.org (search for CY-BOCS) www.effectivechildtherapy.com