38
March 16, 2015 Government Programs Landscape and Overview Phyllis Feeney – Executive Director, Pricing & Reimbursement Bristol-Myers Squibb Company

March 16, 2015
Government Programs Landscape and Overview
Phyllis Feeney –Executive Director, Pricing & Reimbursement Bristol-Myers Squibb Company
Disclaimer
2
• The opinions expressed in this presentation are my own and do not necessarily represent those of Bristol-Myers Squibb.
• The presentation materials are offered only for informational and educational purposes. You should not act or rely on any information contained in this presentation without first seeking the legal advice of your attorney, if appropriate.

Agenda
• Introduction • Government Programs Landscape• Medicaid Reporting Overview• Medicare Reporting Overview• PHS / FSS / ADAP / TRICARE discount &
rebates Overview
3

Contract Performance Management
Market Access Strategy
Contracting Opportunity Evaluation
Quarterly Close, Projections, and
Budget
Other Discounting
Opportunities
Re-evaluate Contracting
Strategy
Launch Price and Contracting
Strategy
4
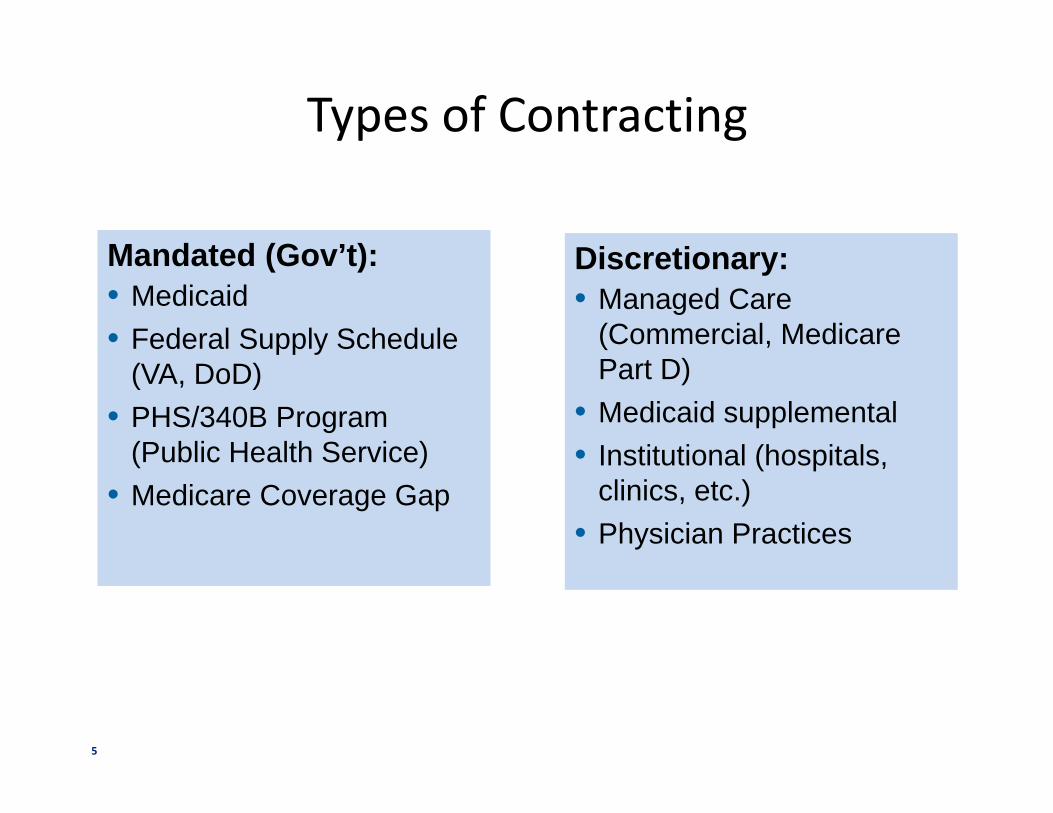
Types of Contracting
Mandated (Gov’t):• Medicaid• Federal Supply Schedule
(VA, DoD)• PHS/340B Program
(Public Health Service)• Medicare Coverage Gap
Mandated (Gov’t):• Medicaid• Federal Supply Schedule
(VA, DoD)• PHS/340B Program
(Public Health Service)• Medicare Coverage Gap
Discretionary:• Managed Care
(Commercial, Medicare Part D)
• Medicaid supplemental• Institutional (hospitals,
clinics, etc.)• Physician Practices
Discretionary:• Managed Care
(Commercial, Medicare Part D)
• Medicaid supplemental• Institutional (hospitals,
clinics, etc.)• Physician Practices
5
Why do Manufacturers Contract?
– Decrease overall purchasing costs
– Remove cost barriers for payers, institutions and physicians
– Ensures patient access to products
– Gain formulary access
6
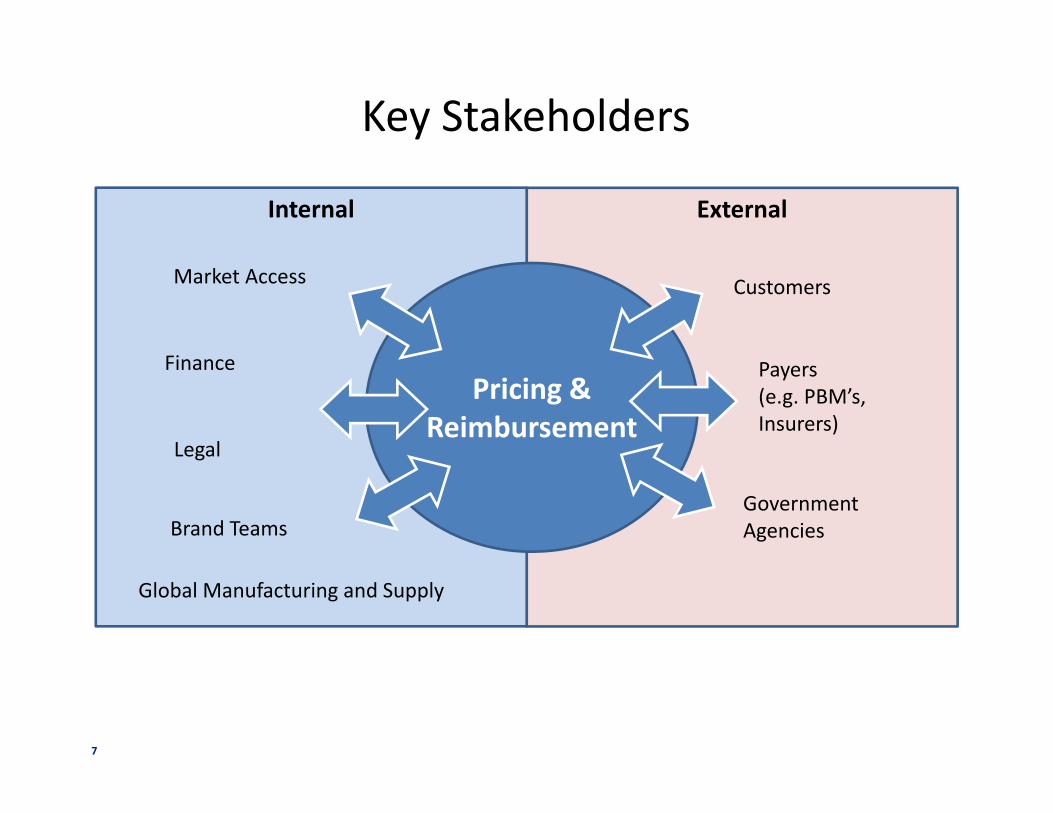
Key Stakeholders
ExternalInternal
Pricing & Reimbursement
Market Access
Finance
Brand Teams
Legal
Customers
Payers (e.g. PBM’s, Insurers)
Government Agencies
Global Manufacturing and Supply
7
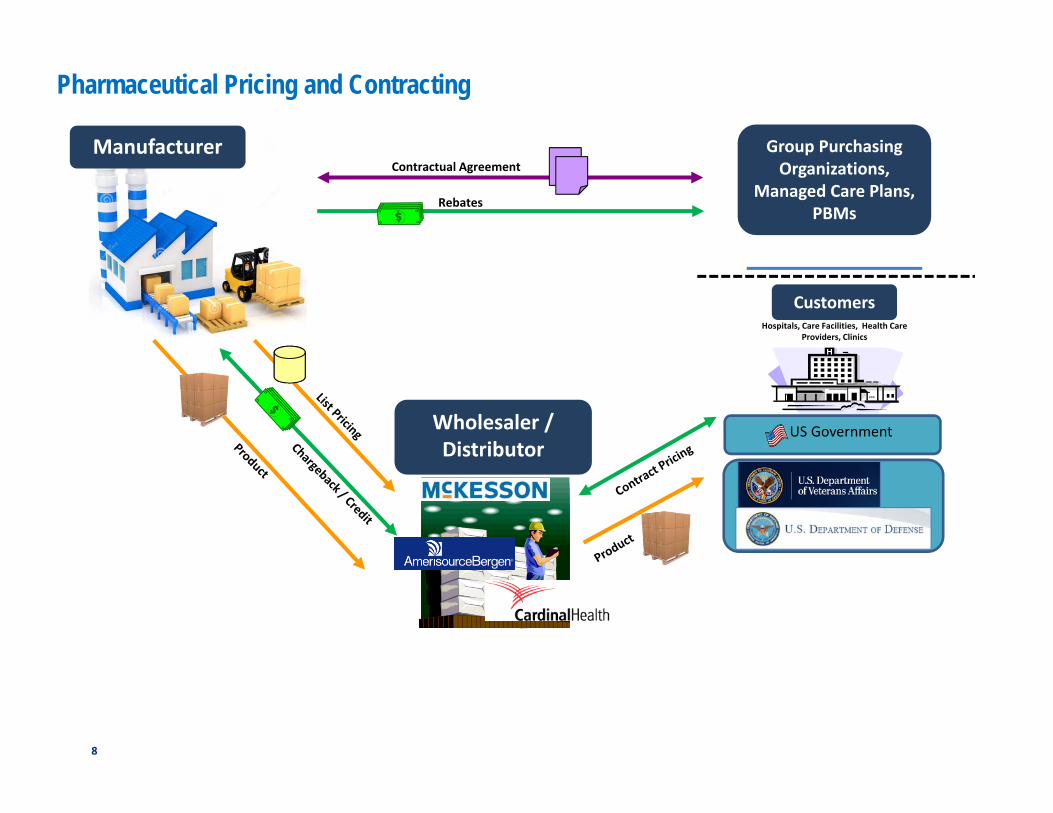
Pharmaceutical Pricing and Contracting
Contractual AgreementManufacturer
Wholesaler / Distributor
Group Purchasing Organizations,
Managed Care Plans, PBMs
US Government
Rebates
Hospitals, Care Facilities, Health Care Providers, Clinics
Customers
8
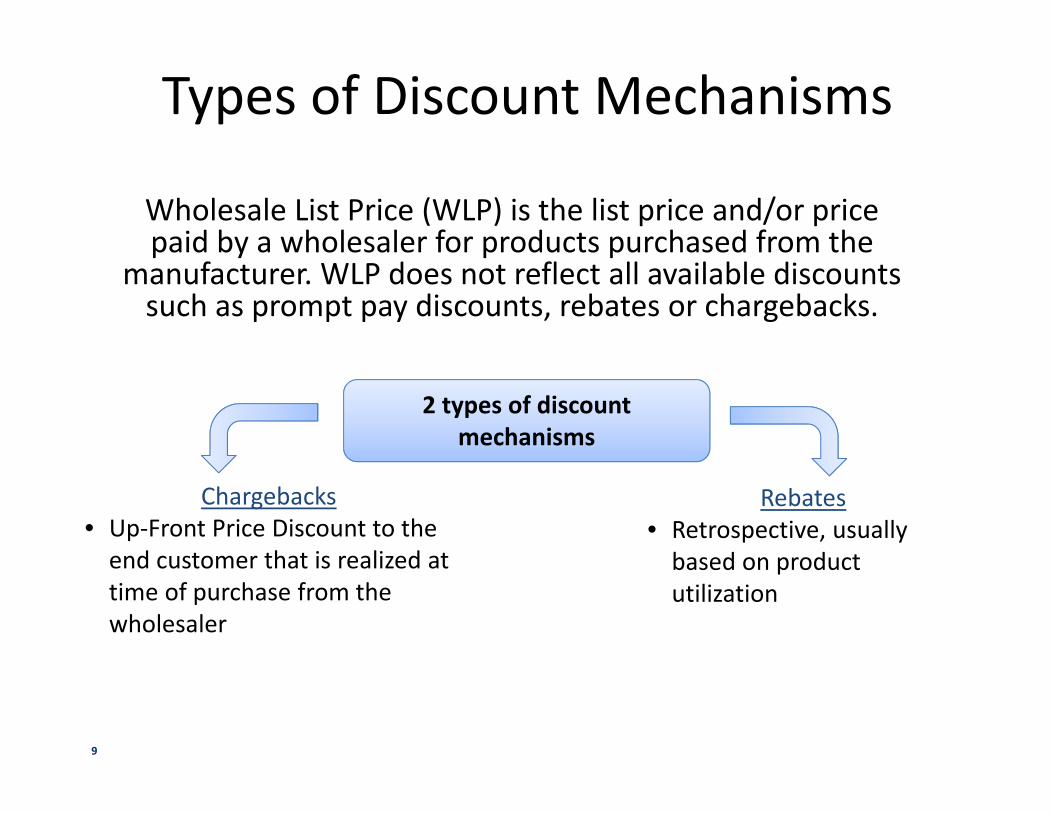
Types of Discount Mechanisms
Wholesale List Price (WLP) is the list price and/or price paid by a wholesaler for products purchased from the
manufacturer. WLP does not reflect all available discounts such as prompt pay discounts, rebates or chargebacks.
2 types of discountmechanisms
Chargebacks • Up-Front Price Discount to the
end customer that is realized at time of purchase from the wholesaler
Rebates• Retrospective, usually
based on product utilization
9
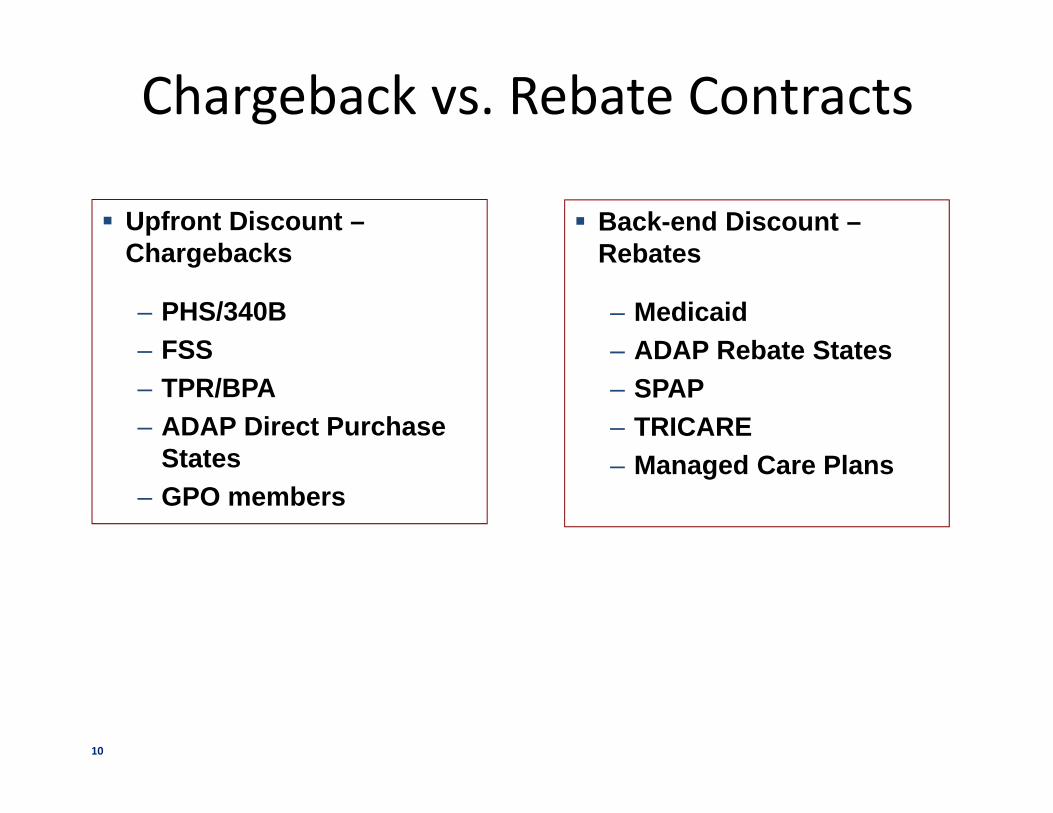
Chargeback vs. Rebate Contracts
Upfront Discount –Chargebacks
– PHS/340B– FSS– TPR/BPA– ADAP Direct Purchase
States– GPO members
Back-end Discount –Rebates
– Medicaid– ADAP Rebate States– SPAP– TRICARE– Managed Care Plans
10

Government Programs Landscape
11

Government Program Administration• The U.S. Department of Health and Human Services (HHS) administers
the Medicaid, Medicare and 340B/PHS programs.
• Within HHS:
– The Centers for Medicare and Medicaid Services (CMS) issues regulations and guidance concerning pricing calculations and requirements under the Medicaid and Medicare programs.
– The Health Resources and Services Administration (HRSA) issues regulations and guidance concerning the 340B/PHS program.
• The Department of Veterans Affairs (VA) issues regulations and guidance for the pricing of pharmaceutical products listed on the Federal Supply Schedule (FSS) and has responsibility for administering the FSS.
12
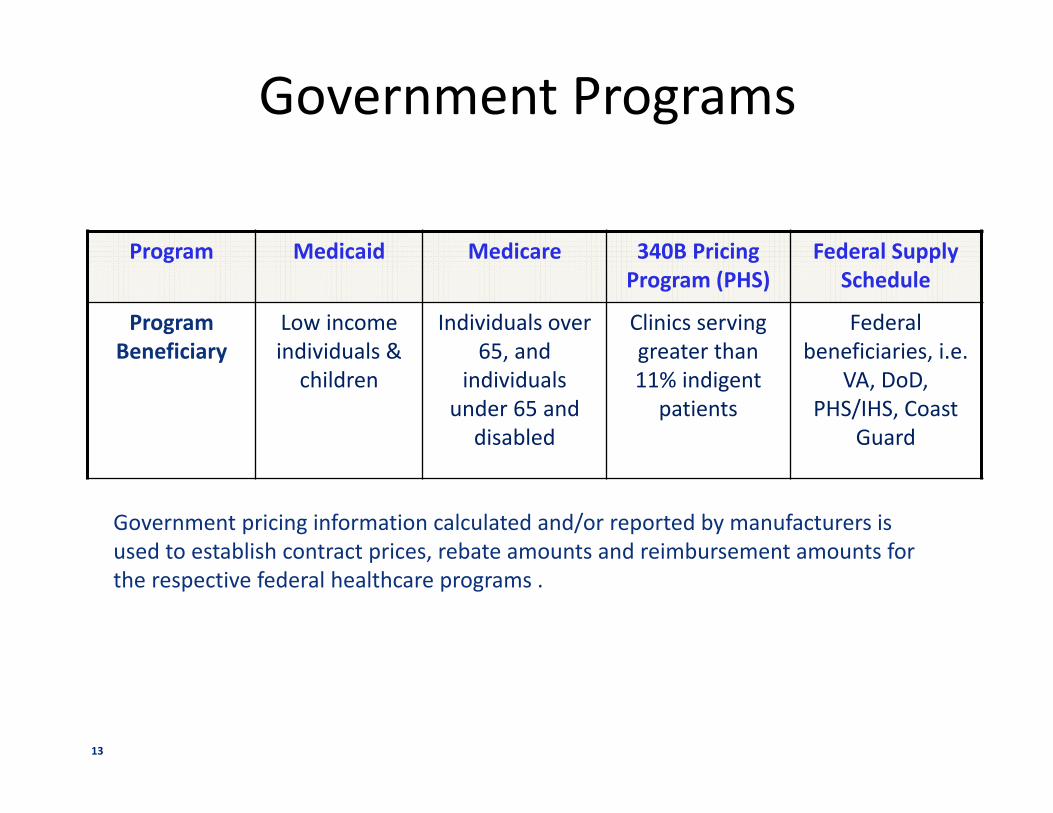
Government Programs
Program Medicaid Medicare 340B Pricing Program (PHS)
Federal Supply Schedule
Program Beneficiary
Low income individuals &
children
Individuals over 65, and
individuals under 65 and
disabled
Clinics serving greater than 11% indigent
patients
Federal beneficiaries, i.e.
VA, DoD, PHS/IHS, Coast
Guard
Government pricing information calculated and/or reported by manufacturers is used to establish contract prices, rebate amounts and reimbursement amounts for the respective federal healthcare programs .
13

Government Program Pricing Calculation
• Federal healthcare programs entail many complex price-related calculations.
• Manufacturers are required to calculate prices in accordance with applicable Federal Pricing Statutes, regulations and guidance.
• Examples of the calculations used within the major healthcare programs include:
● AMP (Average Manufacturer Price)
● BP (Best Price)
● ASP (Averages Sales Price)
● 340B/PHS Ceiling Price
● NFAMP (Non-Federal Average Manufacturer Price)
● FCP (Federal Ceiling Price)
14
Typical Government Contracts
• Medicaid Master Agreement • State Medicaid Supplemental Rebate Agreement• SPAP - State Pharmaceutical Assistance Program• ADAP – AIDS Drug Assistance Program• FSS – Federal Supply Schedule
o TPR (Temporary Price Reduction)o BPA (Blanket Purchase Agreement). Sub-ceiling price agreement
with Department of Defenseo TRICARE
• PHS/340B – Public Health Services
15
Government PricingMedicaid Reporting Overview
Government Pricing
16
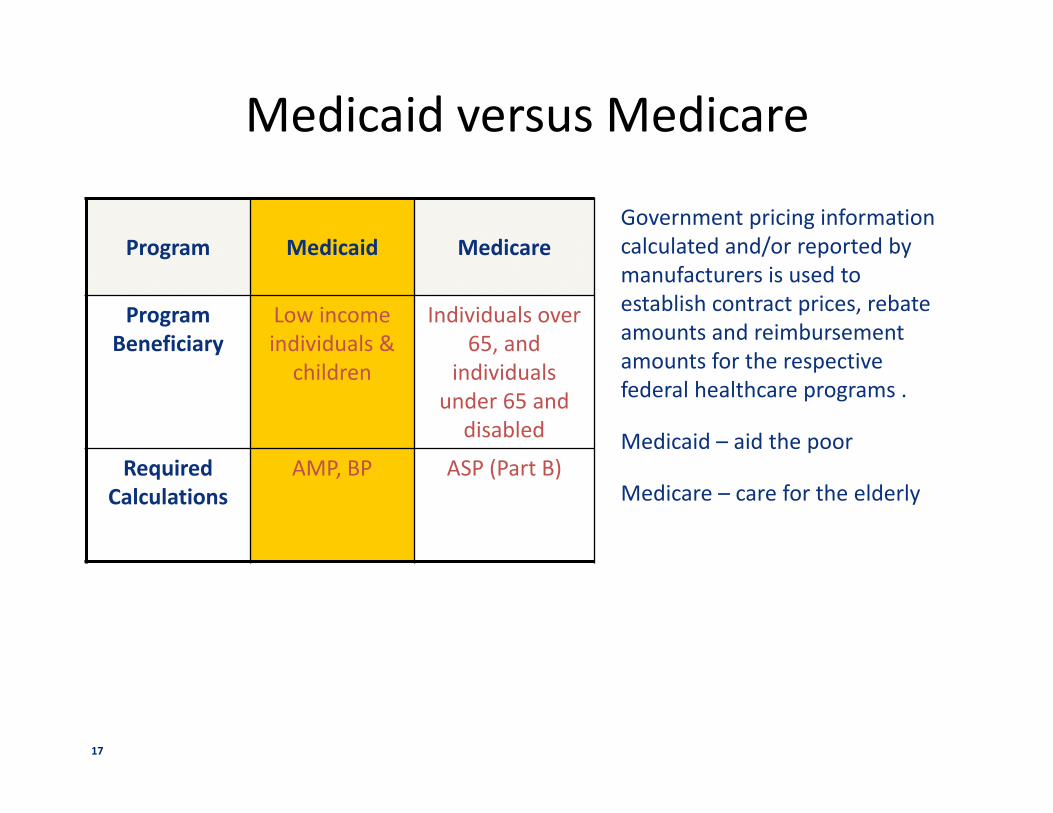
Medicaid versus Medicare
Government pricing information calculated and/or reported by manufacturers is used to establish contract prices, rebate amounts and reimbursement amounts for the respective federal healthcare programs .
Medicaid – aid the poor
Medicare – care for the elderly
Program Medicaid Medicare
Program Beneficiary
Low income individuals &
children
Individuals over 65, and
individuals under 65 and
disabled
Required Calculations
AMP, BP ASP (Part B)
17
Medicaid Overview• Manufacturer enters into a Medicaid Rebate Agreement with the Secretary of
Health and Human Services (HHS) that requires drug manufacturers to pay rebates on Medicaid retail drug utilization
• For a branded drug:
Minimum rebate is 23.1% of AMP, plus an additional amount based on price increases greater than the Consumer Price Index (CPI)
Potential incremental Best Price rebate, that is calculated based on the lowest price provided to commercial purchasers within the United States
• Reporting Requirements
Monthly and Quarterly Average Manufacturer Price (AMP)*
Quarterly Best Price (BP)*
Pay rebates to the states within 38 days to avoid interest
Various state specific requirements
*These pricing submissions require certification to CMS.
18
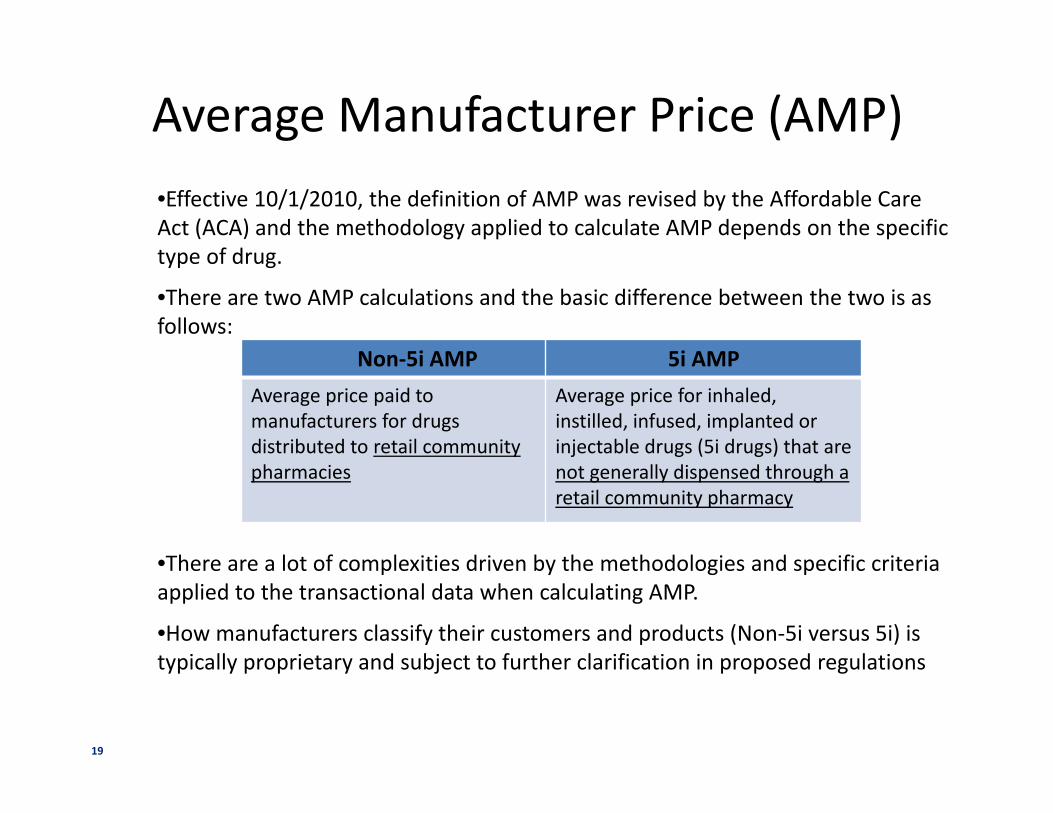
Average Manufacturer Price (AMP)•Effective 10/1/2010, the definition of AMP was revised by the Affordable Care Act (ACA) and the methodology applied to calculate AMP depends on the specific type of drug.
•There are two AMP calculations and the basic difference between the two is as follows:
•There are a lot of complexities driven by the methodologies and specific criteria applied to the transactional data when calculating AMP.
•How manufacturers classify their customers and products (Non-5i versus 5i) is typically proprietary and subject to further clarification in proposed regulations
Non-5i AMP 5i AMPAverage price paid tomanufacturers for drugs distributed to retail community pharmacies
Average price for inhaled, instilled, infused, implanted or injectable drugs (5i drugs) that are not generally dispensed through a retail community pharmacy
19
Best Price (BP)• The Best or lowest price achieved by non-excluded commercial
purchasers
• Unlike “average” price calculations, the best price is set by an individual transaction
• Drug manufacturers must provide the Medicaid program with the lowest price they offer the rest of the drug marketplace
• There are only a few types of customers and transactions excluded from Best Price (i.e. FSS, PHS, Inpatient DSH, etc.)
• When evaluating commercial contracting offers, manufacturers need to understand the Best Price implications of the offer
• Best Price is reported to CMS on a quarterly basis and needs to be “trued up” within 3 years of the initial submission
20
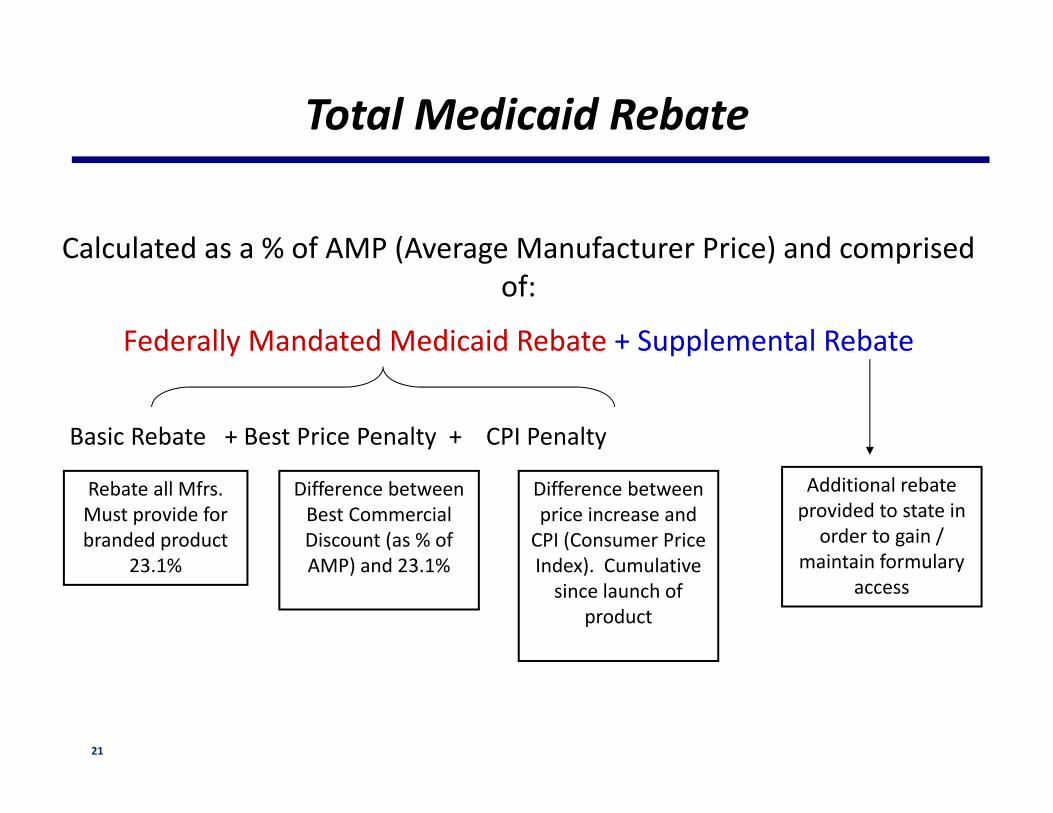
Calculated as a % of AMP (Average Manufacturer Price) and comprised of:
Federally Mandated Medicaid Rebate + Supplemental Rebate
Total Medicaid Rebate
Basic Rebate + Best Price Penalty + CPI Penalty
Rebate all Mfrs. Must provide for branded product
23.1%
Difference between Best Commercial Discount (as % of AMP) and 23.1%
Additional rebate provided to state in
order to gain / maintain formulary
access
Difference between price increase and
CPI (Consumer Price Index). Cumulative
since launch of product
21

Medicaid Mandated Rebate Calculation
• AMP (Average Manufacturer Price) is calculated each month and quarter and submitted to CMS. BP (Best Price) is calculated each quarter and submitted to CMS
• AMP and BP is calculated at NDC 9 level (i.e. 2mg, 5mg…etc)
• AMP and BP can change from quarter to quarter due to price increase action and commercial contacting activities
• CMS calculates mandated Medicaid URA (Unit Rebate Amount) quarterly and sends it to states. States generate quarterly Medicaid invoices based on the units reimbursed to pharmacies (not Rx units filled within the quarter) and URA to claim mandated rebate $
22
What drives quarterly changes in the Federal Unit Rebate Amount (URA)?
•AMP Fluctuations - AMP is calculated each quarter and submitted to CMS.
•Best Price (BP) Penalty Fluctuations – As commercial contracted discounts exceed the 23.1% threshold, this will ultimately affect the discounts available to the Medicaid segment. If a product does not have a commercial discount in excess of 23.1%, the BP penalty component of the Mandated Medicaid Rebate will be 0%
• CPI Penalty Fluctuations – Most significant in quarter of price increase, levels off during remaining 3 quarters. If CPI increases during a contract period, will reduce penalty (and mandated rebate).
23
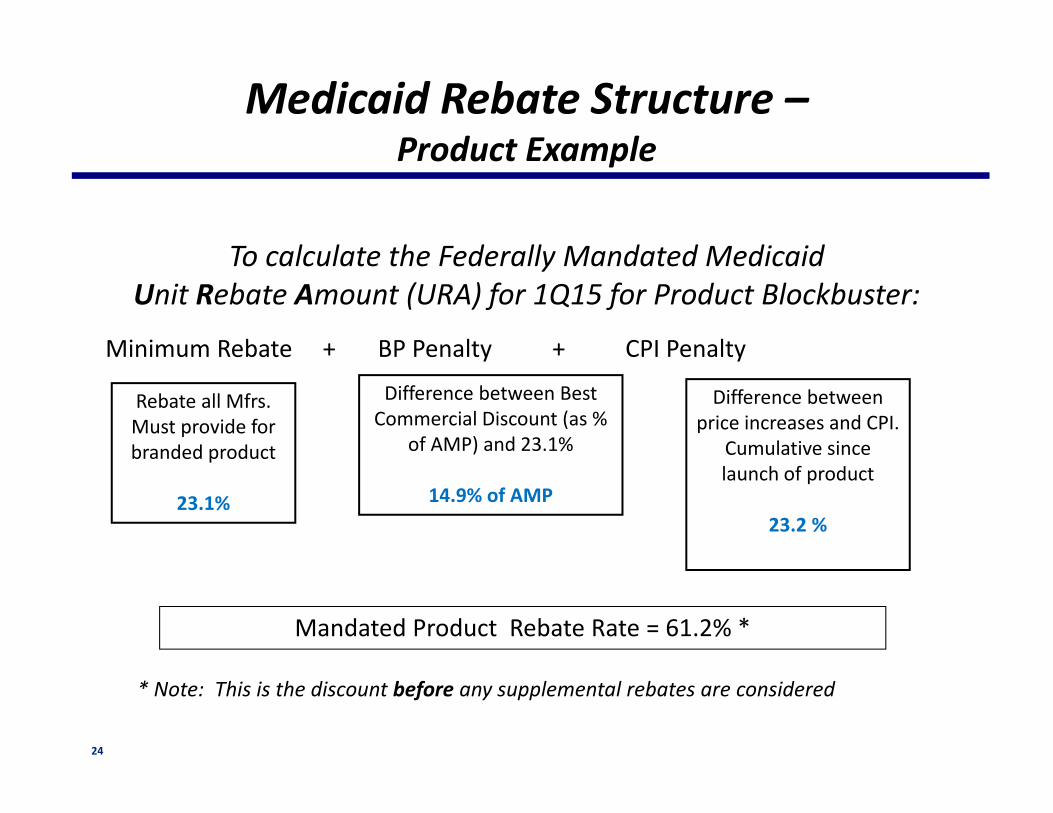
To calculate the Federally Mandated Medicaid Unit Rebate Amount (URA) for 1Q15 for Product Blockbuster:
Medicaid Rebate Structure –Product Example
Mandated Product Rebate Rate = 61.2% *
* Note: This is the discount before any supplemental rebates are considered
Minimum Rebate + BP Penalty + CPI Penalty
Rebate all Mfrs. Must provide for branded product
23.1%
Difference between Best Commercial Discount (as %
of AMP) and 23.1%
14.9% of AMP
Difference between price increases and CPI.
Cumulative since launch of product
23.2 %
24
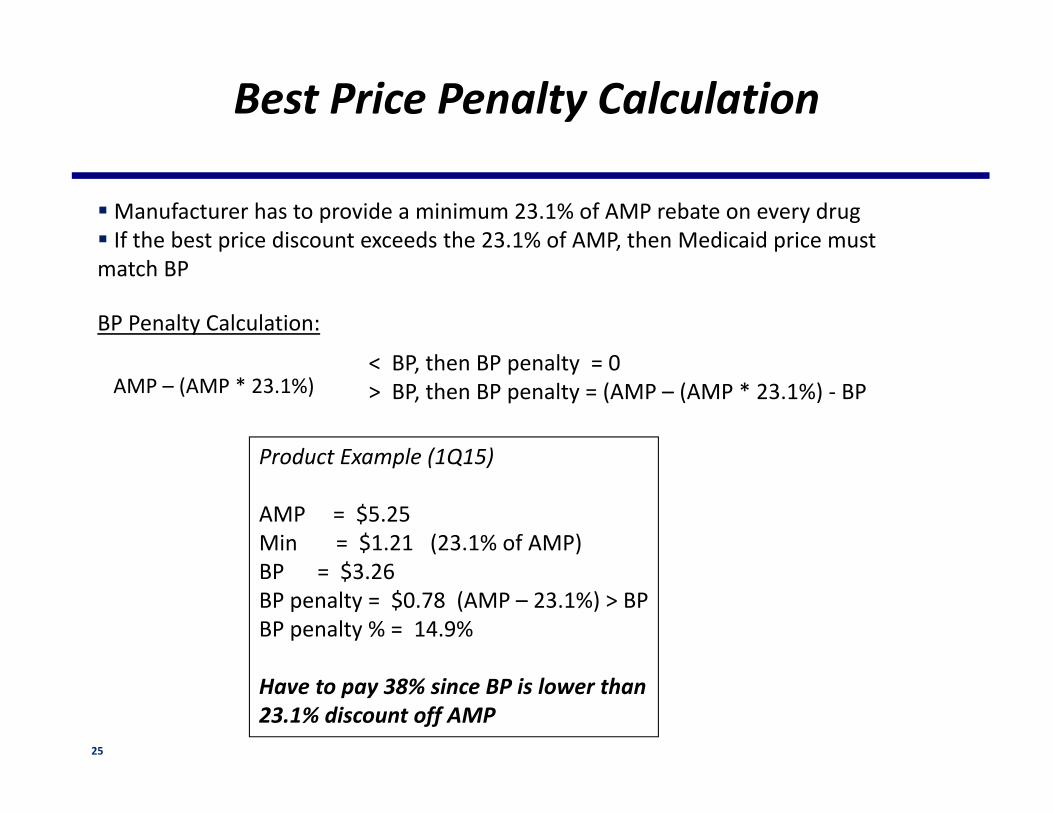
Manufacturer has to provide a minimum 23.1% of AMP rebate on every drug If the best price discount exceeds the 23.1% of AMP, then Medicaid price must match BP
Best Price Penalty Calculation
BP Penalty Calculation:
AMP – (AMP * 23.1%)< BP, then BP penalty = 0> BP, then BP penalty = (AMP – (AMP * 23.1%) - BP
Product Example (1Q15)
AMP = $5.25Min = $1.21 (23.1% of AMP)BP = $3.26BP penalty = $0.78 (AMP – 23.1%) > BPBP penalty % = 14.9%
Have to pay 38% since BP is lower than 23.1% discount off AMP
25

Government PricingMedicare Reporting Overview
26

Medicaid versus Medicare
Government pricing information calculated and/or reported by BMS is used to establish contract prices, rebate amounts and reimbursement amounts for the respective federal healthcare programs .
Medicaid – aid the poor
Medicare – care for the elderly
Program Medicaid Medicare
Program Beneficiary
Low income individuals &
children
Individuals over 65, and
individuals under 65 and disabled
Required Calculations
AMP, BP ASP (Part B)
27
Medicare Overview
• Beginning January 1, 2005, CMS began using the reported ASP prices to set reimbursement for Part B administered drugs and biologics not paid on a cost or prospective payment basis• The ASP pricing is used to set reimbursement for physician administered drugs/biologics versus AMP/BP where the pricing determines rebates paid to the government• Reimbursement to providers is currently set by CMS at ASP plus 4.3%. There is a two quarter lag between the submission of ASP and its use in reimbursing providers.
•Reporting Requirements
Quarterly Average Sales Price (ASP)
It cannot be restated for late arriving or “lagged” data
28
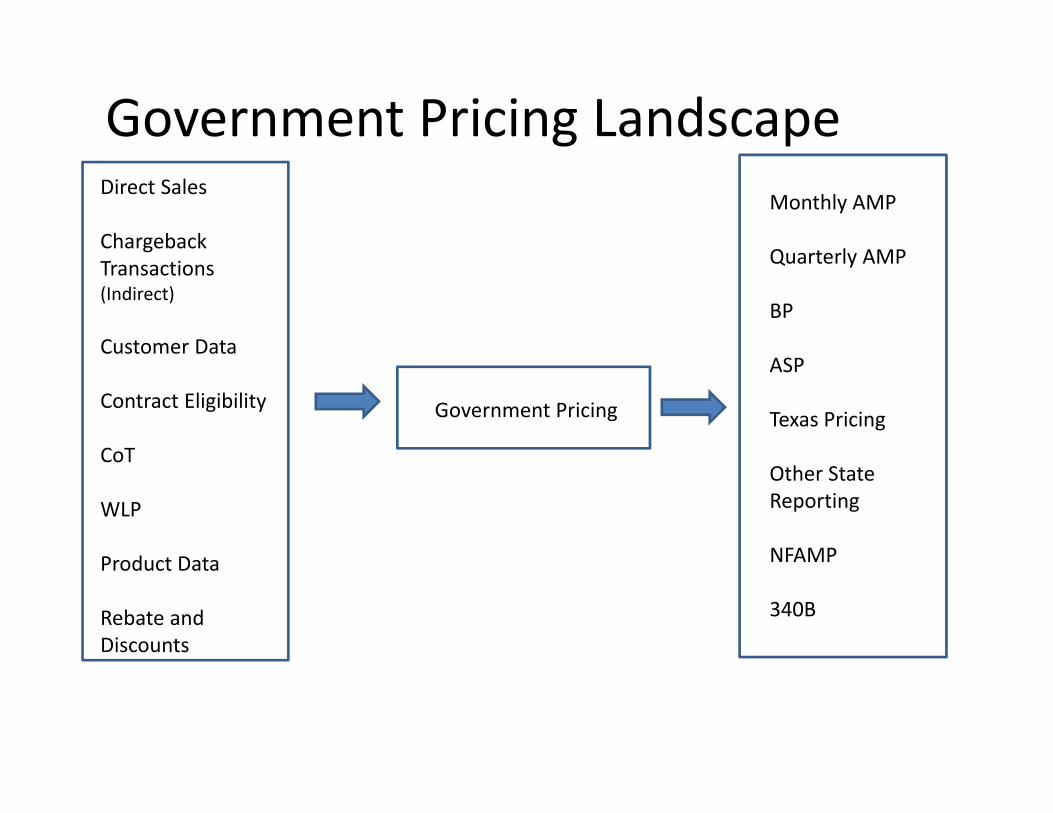
Government Pricing
Direct Sales
Chargeback Transactions (Indirect)
Customer Data
Contract Eligibility
CoT
WLP
Product Data
Rebate and Discounts
Monthly AMP
Quarterly AMP
BP
ASP
Texas Pricing
Other State Reporting
NFAMP
340B
Government Pricing Landscape

PHS / FSS / ADAP / TRICARE Discount & Rebates OverviewPrime Vendor Accounts
30

FSS (Federal Supply Schedule) Program
The Veteran’s Health Care Act of 1992 (VHCA ‘92):– Mandated discounted prices on pharmaceuticals to the “Big Four” federal agencies: The VA,
Department of Defense (DoD), Public Health Service/Indian Health Service (IHS), and Coast Guard.
– Other Government Agencies (OGA) purchase at a “negotiated” price that serves as the FSS contract price.
The mandated price is called the Federal Ceiling Price (FCP). – Manufacturer calculates and reports quarterly and annual Non-Federal Average Manufacturer
price (NFAMP)– 24% mandated discount off NFAMP– CPI penalty is calculated based on 3Q NFAMP change from last year and not cumulative
change from product launch period
The FCP is effective for a calendar year (or portion thereof for a newly marketed product).
– 3Q14 and Annual 2014 NFAMP is due to VA on 11/15/2014.– 2015 FCP is calculated & awarded by VA in December 2014.
31
PHS (Public Health Services) Program Overview
The 340B program is a drug purchasing program originally designed to give discounted pricing on outpatient drugs to providers of “at risk” populations
– The program is administered by HRSA and the Office of Pharmacy Affairs (OPA)
Entities that participate in the program are referred to as Covered Entities– Although only 2,000 of the 11,000 Covered Entities in the program are hospitals, over 80% of the
purchased drugs in the 340B program are through hospitals
The 340B price is a statutory price equal to AMP minus URA from 2 quarters ago (e.g. 4Q14 AMP – URA sets 2Q15 PHS price)
Manufacturers issue credit to wholesalers on 340B drugs purchased through the covered entity’s 340B account
– Wholesaler credit = WLP – 340B price
Covered Entities are allowed to contract with pharmacies to dispense 340B drugs – these arrangements are referred to as Contract Pharmacies
32
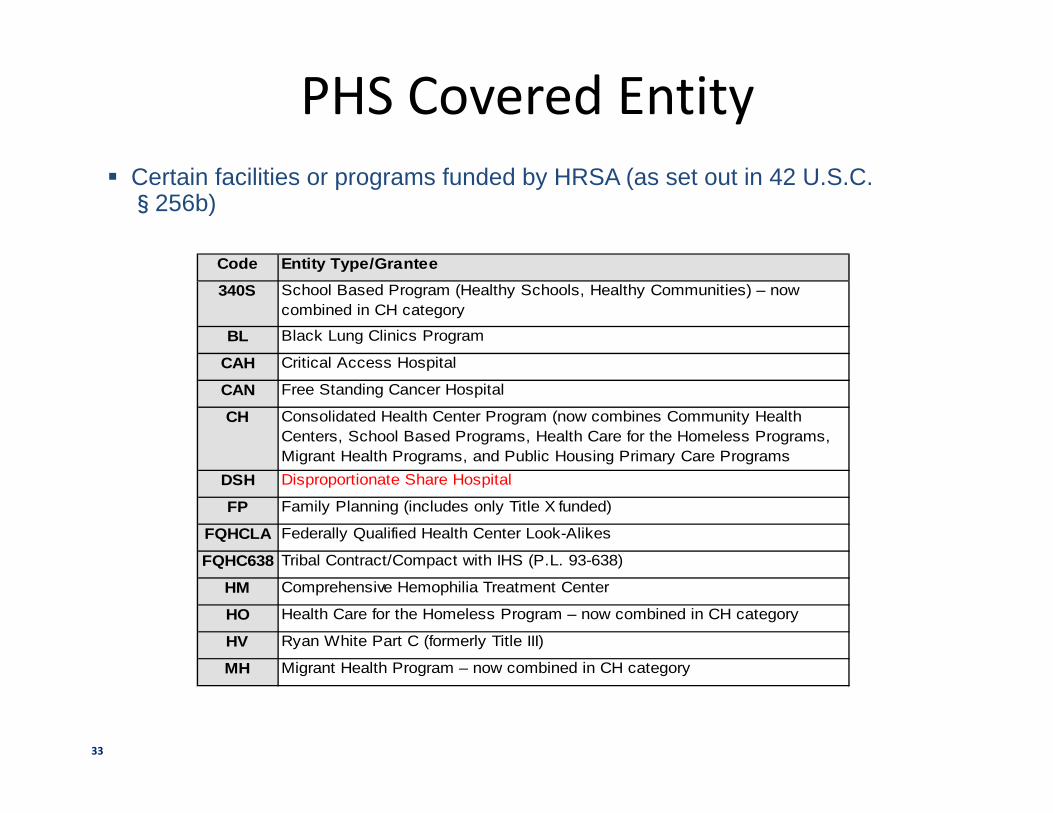
PHS Covered Entity Certain facilities or programs funded by HRSA (as set out in 42 U.S.C. §256b)
Code Entity Type/Grantee
340S School Based Program (Healthy Schools, Healthy Communities) – now combined in CH category
BL Black Lung Clinics Program
CAH Critical Access Hospital
CAN Free Standing Cancer Hospital
CH Consolidated Health Center Program (now combines Community Health Centers, School Based Programs, Health Care for the Homeless Programs, Migrant Health Programs, and Public Housing Primary Care Programs
DSH Disproportionate Share Hospital
FP Family Planning (includes only Title X funded)
FQHCLA Federally Qualified Health Center Look-Alikes
FQHC638 Tribal Contract/Compact with IHS (P.L. 93-638)
HM Comprehensive Hemophilia Treatment Center
HO Health Care for the Homeless Program – now combined in CH category
HV Ryan White Part C (formerly Title III)
MH Migrant Health Program – now combined in CH category
33
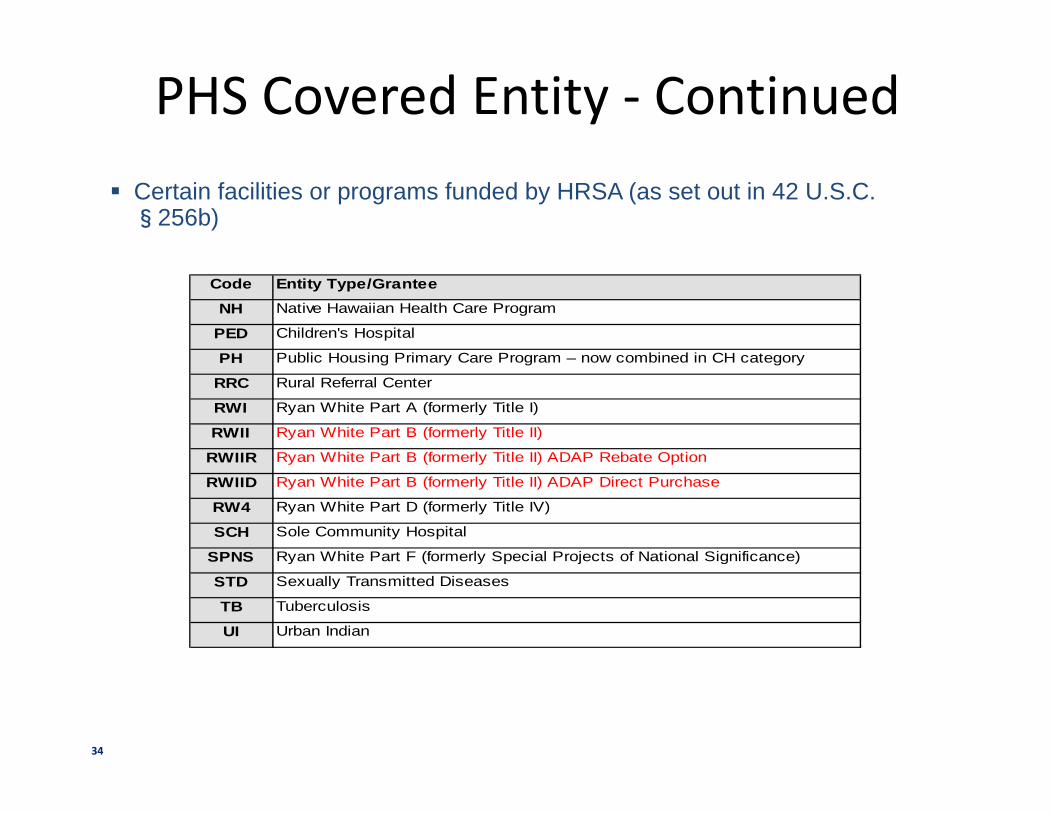
PHS Covered Entity - Continued Certain facilities or programs funded by HRSA (as set out in 42 U.S.C. §256b)
Code Entity Type/Grantee
NH Native Hawaiian Health Care Program
PED Children's Hospital
PH Public Housing Primary Care Program – now combined in CH category
RRC Rural Referral Center
RWI Ryan White Part A (formerly Title I)
RWII Ryan White Part B (formerly Title II)
RWIIR Ryan White Part B (formerly Title II) ADAP Rebate Option
RWIID Ryan White Part B (formerly Title II) ADAP Direct Purchase
RW4 Ryan White Part D (formerly Title IV)
SCH Sole Community Hospital
SPNS Ryan White Part F (formerly Special Projects of National Significance)
STD Sexually Transmitted Diseases
TB Tuberculosis
UI Urban Indian
34
PHS Orphan Drug Rule & Pricing
Orphan Drug Rule
– Effective 10/1/2013, certain expanded PHS entities (Free-standing Cancer Hospitals, Rural Referral Centers, Sole Community Hospitals, and Critical Access Hospitals ) can purchase outpatient orphan drugs at 340B price if the drug is used for non-orphan indications.
– Entity can opt-out of this program if they cannot maintain auditable records to demonstrate compliance.
35

PHS – Public Health Services Discount
PHS price = Mandated Medicaid price from 2 quarters ago
Example: Product ABC 1Q15 price = 3Q14 AMP $22 – URA $16 = $6 per tablet. PHS price per package is $180 (bottle of 30 tablets)
36

ADAP (AIDS Drug Assistance Program) & TRICARE Program Overview
ADAP provides FDA-approved HIV-related Rx drugs to low-income people with HIV/AIDS who have limited or no prescription drug coverage
– Funded jointly by Federal and State government– State ADAP can be Rebate structure or Direct Purchase structure through Prime Vendor. – ADAP is 340B covered entity and qualifies for 340B price
TRICARE customers are active military’s families. Rx filled at network pharmacies are eligible for rebate.
– Rebate = Annual NFAMP - FCP– Fixed rebate per unit for the entire calendar year except newly launched product– Invoice quarterly to claim rebate
37
Phyllis Feeney Executive Director, Pricing & Reimbursement Bristol-Myers Squibb [email protected]
Contact Info
38

















