41
Created November 1, 2013 Edited November 20, 2013 UNIT RESOURCE MANUAL Produced by Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic
| Date post: | 15-Feb-2017 |
| Category: |
Documents |
| Upload: | ashley-pham |
| View: | 18 times |
| Download: | 0 times |

Created November 1, 2013 Edited November 20, 2013
UNIT RESOURCE MANUAL
Produced by
Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic

2 Created November 1, 2013 Edited November 20, 2013
TABLE OF CONTENTS
CONFIDENTIALITY PROTOCOL ...................................................................................................... 3 Privacy .................................................................................................................................................... 4
Storage of Records Procedures .............................................................................................................. 4
Release of Information ............................................................................................................................ 4
Patient Consent ....................................................................................................................................... 4
HOSPITAL FORMS ................................................................................................................................ 5 COMMUNITY AGENCY REFERRAL FORM ........................................................................................ 6
KARDEX FORM ................................................................................................................................... 10
DOCTORS ORDER SHEET ................................................................................................................. 12
ADMISSION FORM.............................................................................................................................. 13
PATIENT HISTORY FORM .................................................................................................................. 14
MULTI-DAY MEDICAL ADMINISTRATION FORM .......................................................................... 18
SINGLE DAY MEDICAL ADMINISTRATION RECORD .................................................................... 19
PRE-OPERATIVE FORM ..................................................................................................................... 20
RESPONSIBILITIES OF THE CLINICAL SECRETARY .............................................................. 22 RESPONSIBILITIES OF THE MEDICAL ADMINISTRATION ASSISTANTS THROUGHOUT THE
HOSPITAL ............................................................................................................................................ 23
POSTING INSTRUCTIONS ................................................................................................................. 24 CODES FOR EMERGENCIES ............................................................................................................. 25
DESCRIPTION OF THE CODES ........................................................................................................ 26
CARDIOPULMONARY EMERGENCIES ............................................................................................ 27
H1N1 PROTOCOL ............................................................................................................................... 27
TRAINING SESSION ............................................................................................................................ 28 OVERVIEW OF NUTRITION WORKSHOP ........................................................................................ 29
AGENDA ............................................................................................................................................... 30
EMAIL FOR REGISTRATION FOR THE EVENT ............................................................................... 31
REGISTRATION FORM AND FLYER ................................................................................................. 32
REMINDER EMAIL .............................................................................................................................. 33
APPENDIX .............................................................................................................................................. 34 Appendix 1 ............................................................................................................................................ 35
Appendix 2 ............................................................................................................................................ 36
Appendix 3 ............................................................................................................................................ 37
Appendix 4 ............................................................................................................................................ 38
Appendix 5 ............................................................................................................................................ 39
Appendix 6 ............................................................................................................................................ 40
Works Cited ............................................................................................................................................. 41
3 Created November 1, 2013 Edited November 20, 2013
CONFIDENTIALITY PROTOCOL
4 Created November 1, 2013 Edited November 20, 2013
Privacy
Privacy does not disappear in a hospital setting health cards must be kept private and confidential at all
times. The Health Card is for health care purposes only. Patients should show their health cards every
time they are at the clinic or hospital.
Any Medical Administrative Assistant that oversees the health records of patients must ensure that they
are kept secure, private and only are released with a written consent from the patient, because clients’
health records are extremely confidential and private. The records are considered to be owned by the
facility that the patients go to and the patient. The facility owns the hard copy of the records and the
patient’s own the information within them. The owners of the facilities must make sure to form their
policies and rules around the privacy of these records.
(Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D.
Thompson, Chapter 2, page 54-55, Chapter 10, Page 305, and Chapter 13 423-429)
Storage of Records Procedures
Records have to be kept for 10 years in a private, organized, and secure location. If a patient asks for his
or her files, they should be faxed and not emailed for security reasons. Access to records is limited to
only those that are caring for the patient by having a written consent by the patient. Records now should
keep a hard and electronic copy for redundancy. Hospitals should make sure to have a disaster recovery
plan implemented to recover records in case of disasters.
Release of Information
When handling personal information, administration assistants must be careful to whom they can release
information. Certain facilities may allow you to give basic information about a client to their families if
they request it; other facilities may not. In general, do not give out any information without permission
from the patient and/or doctor. If the assistants feel that the situation is out of their hands, they simply
need to pass the call on to the patient’s nurse. All of these rules apply to face-to-face conversations as
well.
(Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D.
Thompson, Chapter 14, Page 464)
Patient Consent
It is required that the hospital have written permission from the patient/client in regards to releasing of
any and all personal information to anyone that asks for their documents.

5 Created November 1, 2013 Edited November 20, 2013
HOSPITAL FORMS

6 Created November 1, 2013 Edited November 20, 2013
COMMUNITY AGENCY REFERRAL FORM
Community Care Access Centre
Patient’s LAST Name: ___________________ Patient’s First name:______________________
Date:
Please complete the form thoroughly and PLEASE print clearly. Each referring agency or institution
should be decided on how the physician will be the most appropriate for the completed form.
Reason for Referral:
Application Checklist (include if available):
Care protocols attached
Communication to the individual’s family physician of referral for palliative care services
Copy of completed Do Not Resuscitate Confirmation Form
Diagnostic imaging (X-ray, Ultrasound, CT scan, MRI)
Recent chest x-ray
Infection control management
Recent consultation notes
Recent laboratory results
Pathology reports
Type of Service requested Urgency of response Pages require
Community Care Access Centre 1 to 2 Days
1 to 2 Weeks
Pages 1-5
Community Palliative Care Physician
Referral: Consultant care or Primary care
1 to 2 Days
1 to 2 Weeks
Pages 1-4
Victorian Order on Nurse 1 to 2 Days
1 to 2 Weeks
Future
Pages 1-5
Clinic (Specify):
1 to 2 Days
1 to 2 Weeks
Pages 1-5
Other (specify): 1 to 2 Days
1 to 2 Weeks
Future
Pages 1-5
Page 1
http://www.ccac-ont.ca/Upload/toronto/General/Palliative_CRF_Nov2010.pdf
7 Created November 1, 2013 Edited November 20, 2013
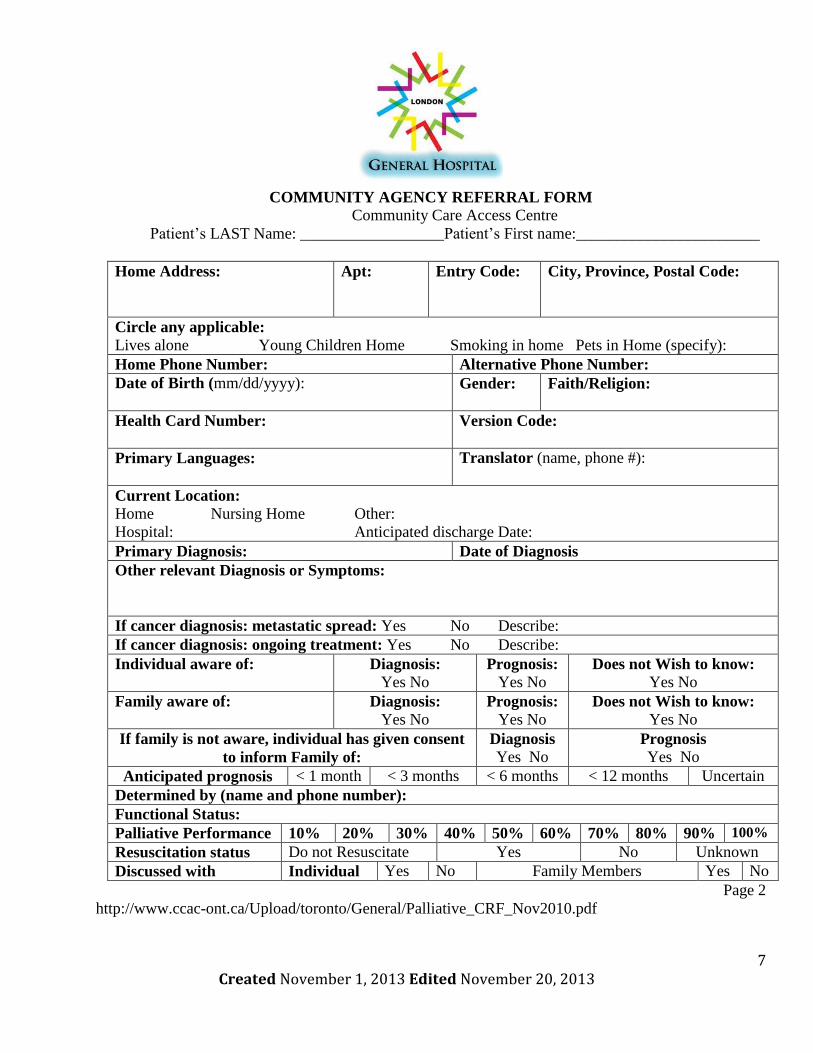
COMMUNITY AGENCY REFERRAL FORM
Community Care Access Centre
Patient’s LAST Name: __________________Patient’s First name:_______________________
Home Address:
Apt: Entry Code: City, Province, Postal Code:
Circle any applicable:
Lives alone Young Children Home Smoking in home Pets in Home (specify):
Home Phone Number: Alternative Phone Number:
Date of Birth (mm/dd/yyyy): Gender:
Faith/Religion:
Health Card Number:
Version Code:
Primary Languages:
Translator (name, phone #):
Current Location:
Home Nursing Home Other:
Hospital: Anticipated discharge Date:
Primary Diagnosis: Date of Diagnosis
Other relevant Diagnosis or Symptoms:
If cancer diagnosis: metastatic spread: Yes No Describe:
If cancer diagnosis: ongoing treatment: Yes No Describe:
Individual aware of: Diagnosis:
Yes No Prognosis:
Yes No Does not Wish to know:
Yes No
Family aware of: Diagnosis:
Yes No Prognosis:
Yes No Does not Wish to know:
Yes No
If family is not aware, individual has given consent
to inform Family of:
Diagnosis Yes No
Prognosis
Yes No
Anticipated prognosis < 1 month < 3 months < 6 months < 12 months Uncertain
Determined by (name and phone number):
Functional Status:
Palliative Performance 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Resuscitation status Do not Resuscitate Yes No Unknown
Discussed with Individual Yes No Family Members Yes No
Page 2
http://www.ccac-ont.ca/Upload/toronto/General/Palliative_CRF_Nov2010.pdf

8 Created November 1, 2013 Edited November 20, 2013
COMMUNITY AGENCY REFERRAL FORM
Community Care Access Centre
Patient’s LAST Name: ___________________Patient’s First name:_______________________
Family/Informal Caregiver:
Provide Power Of Attorney for Personal Care if known: _______________________________
Name Relationship Home Phone Business/Cell Phone
Please list all Providers and Services currently involved: (if Known)
Additional list attached
Name Phone Fax
Family Physician
CCAC
Community Nurse
Hospice
Other
Page 3
http://www.ccac-ont.ca/Upload/toronto/General/Palliative_CRF_Nov2010.pdf

9 Created November 1, 2013 Edited November 20, 2013
COMMUNITY AGENCY REFERRAL FORM
Community Care Access Centre
Patient’s LAST Name: __________________Patient’s First name:_______________________
Co-Morbidities:
Check Here if documentation is attached
Year Diagnosis Year Diagnosis
Infection Control:
MRSA/VRE (+)
C-DIFF (+)
Other (specify precaution):
Allergies
Yes, If yes, please specify:
No
Unknown
Pharmacy (name and phone number): ____________________________________________
Current medications: (Include complementary alternative & over-the-counter medications)
Medication list attached
Drug Dose Route Interval Drug Does Route Interval
Details of social situation, including any needs or concern of the family:
Page 4
http://www.ccac-ont.ca/Upload/toronto/General/Palliative_CRF_Nov2010.pdf

10 Created November 1, 2013 Edited November 20, 2013
KARDEX FORM
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D. Thompson, Chapter 16, pages 519-
520
Date Date
Routine: pre-op post-op other FP Glucose Times
Extra teaching Tubes / drains
Emotional support: routine extra (explain below): routine extra (explain below) Hemovac Remove (ed) on
Family conferece/teaching Abd Penrose Drain Shorten Out
Other Sump Pump
NG (Levine) Tube
NUTRITION Gomco Suction to low intermittent
NPO
Diet SAFETY MANAGEMENT
Feeding Tube side rails X1 X2
Intermittent Continuous Call bell
Solution: mealtimes HS Night rounds - special consideration
Other Restraints type
LEVELS FOR ACTIVIES OF DAILY LIVING Other
General Assistance Level: HYGIENE
Independent Assist X1 X2 Shower Bath
Toileting: Self Assist X1 X2 Mouth Care foot Care
Bath: Self Assist by nurse Other:
Diet Self Assist by nurse
CLINICAL PARAMETERS ELIMINATION - bowel
No vital signs Vital signs Temp only BID BR Commode bedpan only
Q shift bid tid other Ostomy Care Nurse Patient
Print v/s flow sheet q shift
Wight q am ac breakfast: qd q2d Other Enema Suppository
Glasgow Coma Scale Yes No
Print flow sheet q shift Other
Blood Glucose Monitoring Yes No ELIMINATION - Urinary
Intake / Output Yes No Catheter: Insert/Remove
Print 1 & 0 Flow sheet q shift Foley - #
Lab Values For Regular Monitoring 3-way
Blood sugar INR APTT Suprapubic
Other Condom cath
INTRAVENOUS MONITORING (circle solution) Irrigation:
2/3& 1/3 N/S; 5% D/W; 0.45NaC1/W; 0.45NaCI Strain all urine
Primary Line Other REST AND ACTIVITY
1 @ cc/hr Turn q2h Other
2/3 & 1/3; N/S; 5% D/W; 0.45NaC1/W; 0.45NaCI ROM Active Passive Assist
Other Skin Care decubitus ulcer
2 @ cc/hr Rx
Secondary Line with meds note times of med administration pressure mattress sheep skin
1 Other
2 ISOLATION Sate Started:
Tubind & site change q 72 hrs. Date Type
Reason
Dates Change Site: Location Date last hospitalized
PRN Adaptor-site Change Site: Location Location:
Flush-(minimum once/shift) VRE swab + - C Difficille + -
Times: VRSA swad + - MRSA + -
IV PRN adaptor d/c Date Infection control notified Date:
ROOM #
Page 1
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D. Thompson, Chapter 16, pages 519-520
PATIENT DATA PROFILE (Kardex) LONDON GENERAL HOSPITAL
TEACHING AND EMOTIONAL SUPPORT PROCEDURES / TRATMENTS / DIRECT CARE
MRP / hospitalist FAMILY DOCTOR NURSE PRACTITIONER
NAME HOSPITAL #
PROVISIONAL DIAGNOSIS SECONDAY DIAGNOSIS (other problems) DISCHARGE DIAGNOSIS

11 Created November 1, 2013 Edited November 20, 2013
KARDEX FORM
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D.
Thompson, Chapter 16, pages 519-520
OXYGENATION LAB
Yes No
Mask N/P
Litres- DIAGNOSTIC TESTS
Blood nTransfusions ordered/given
1
2
SUCTIONING 3
Type
Frequency STAT blood Work & Tests
Dressing Change/Check
Location: Frequency: Swabs and Cultures
Simple
Complex:
Abdominal Assessment:
Clip/suture removal cast Physician (s)
Comments: Pastoral Care
Pain Management Home Care Liaison Nurse
CSM (cirdulation/sensation, movement) Social Worker
Other Physio
Discharge Planning Dietary
Destination OT
Transportation Transport # Other
Medications Level of Nursing Care:
Teaching Presciption #1 nurseX 1 hr
Ability to fill Ability to pay #1 nurseX1-4 hr
Follow -UP #2 nurseX 1 hr
Patient aware Private room ordered
Notification of Discharge Advance Directives
Patient Caregiver code No code
Family Doctor Consultants Details
Community supports organ donation Yes No
Home Care
Mental Health Equipment MESSAGES / Other Orders:
Oxygen Home IV antibiotics
Wait-Listed for Facility Date:
Facility 1
2
NAME ROOM # HOSPITAL NUMBER
Page 2
Date ROUTINE AND DAILY TESTS Done
PATIENT DATA PROFILE (Kardex) LONDON GENERAL HOSPITAL
No allergiesALLERGIES:
Constant care
home care support worker
POST OPERATIVE ASSESSMENTS/CARE
Physio/Nurse DB&C
Oximetry
Chest Assessment
Spirometer
Aerosol Rx
Trach cannulae care
CONSULTATIONS (reason/date seen/ to be seen)
Date PROCEDURES / DIRECT CARE ORDERS

12 Created November 1, 2013 Edited November 20, 2013
DOCTORS ORDER SHEET
Please Fax to Pharmacy & note date/time
AGE WT (Kg)
DATE TIME PHYSICIANS – PRINTED NAME SIGNATURE PLEASE CHECK IF
PATIENT
IS A NEW
ADMISSION
WT (Kg)
DATE TIME PHYSICIANS – PRINTED NAME SIGNATURE
WT (Kg)
DATE TIME PHYSICIANS – PRINTED NAME SIGNATURE
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D.
Thompson, Chapter 16, Page 533
13 Created November 1, 2013 Edited November 20, 2013
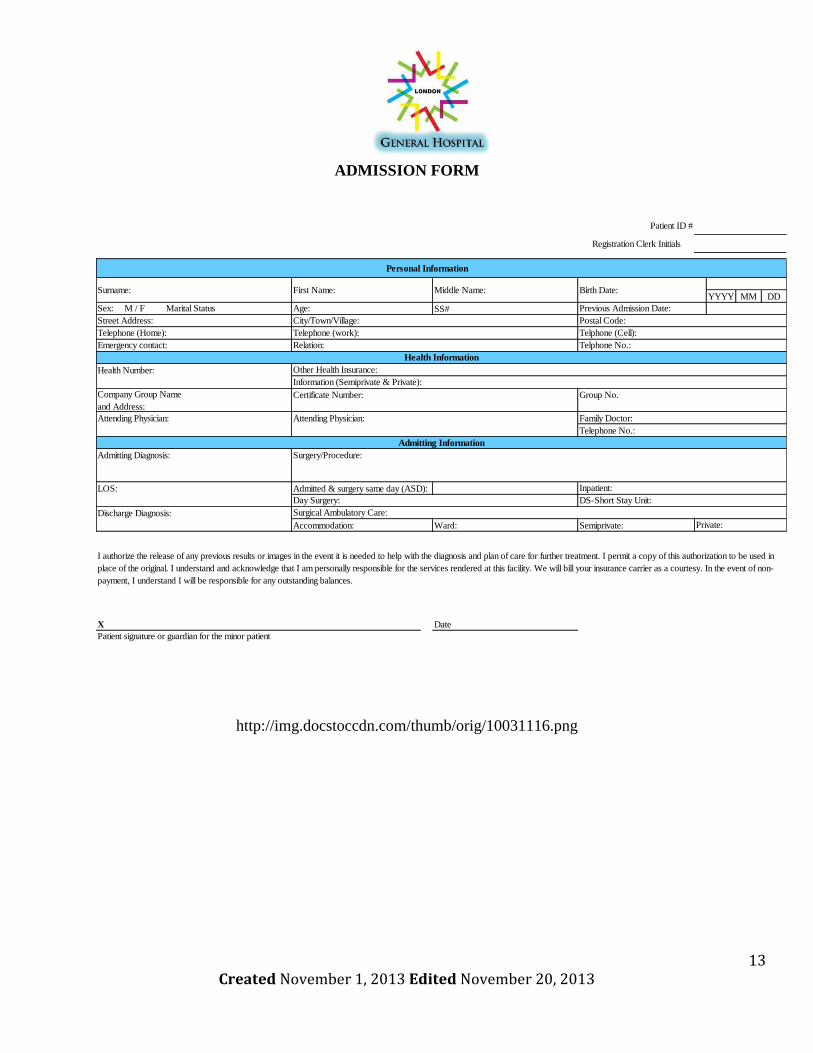
ADMISSION FORM
http://img.docstoccdn.com/thumb/orig/10031116.png
Patient ID #
Registration Clerk Initials
YYYY MM DD
SS#
Company Group Name
and Address:
Admitted & surgery same day (ASD):
Ward: Semiprivate:
X Date
Street Address: City/Town/Village: Postal Code:
Surname:
Personal Information
Previous Admission Date:
First Name: Middle Name:
Age:Sex: M / F Marital Status
Birth Date:
Telephone (Home):
Emergency contact:
Health Information
Telephone (work): Telphone (Cell):
Relation: Telphone No.:
Accommodation:
Attending Physician: Attending Physician:
Information (Semiprivate & Private):
Health Number:
Certificate Number: Group No.
Other Health Insurance:
I authorize the release of any previous results or images in the event it is needed to help with the diagnosis and plan of care for further treatment. I permit a copy of this authorization to be used in
place of the original. I understand and acknowledge that I am personally responsible for the services rendered at this facility. We will bill your insurance carrier as a courtesy. In the event of non-
payment, I understand I will be responsible for any outstanding balances.
Patient signature or guardian for the minor patient
DS-Short Stay Unit:
Family Doctor:
Admitting Information
Telephone No.:
Admitting Diagnosis: Surgery/Procedure:
Discharge Diagnosis:
LOS: Inpatient:
Day Surgery:
Surgical Ambulatory Care:
Private:

14 Created November 1, 2013 Edited November 20, 2013
PATIENT HISTORY FORM
http://superhouseplanswallpaper.blogspot.ca/2012/11/patient-history-form.html
Date
LAST name First Name M.I.
Birthdate
(mm/dd/yyyy) Age Sex F M
Drug Allergies No
Yes
Dosage
1
2
3
4
5
6
7
8
9
10
Page 1Physician initials _____
How long have you been
taking this medicine?
To:
Name of Drug
Please list any medications that you are now taking.
Current Medications
Include non-prescription medications & vitamins or supplements:
How did you hear about us?
Describe your syptoms:
Please list the names of other practitioners you have seen for this problem:
Psychiatric Hospitalizations (include where, when, & for what reason):
Have you ever had ECT?
Have you had psychotherapy?
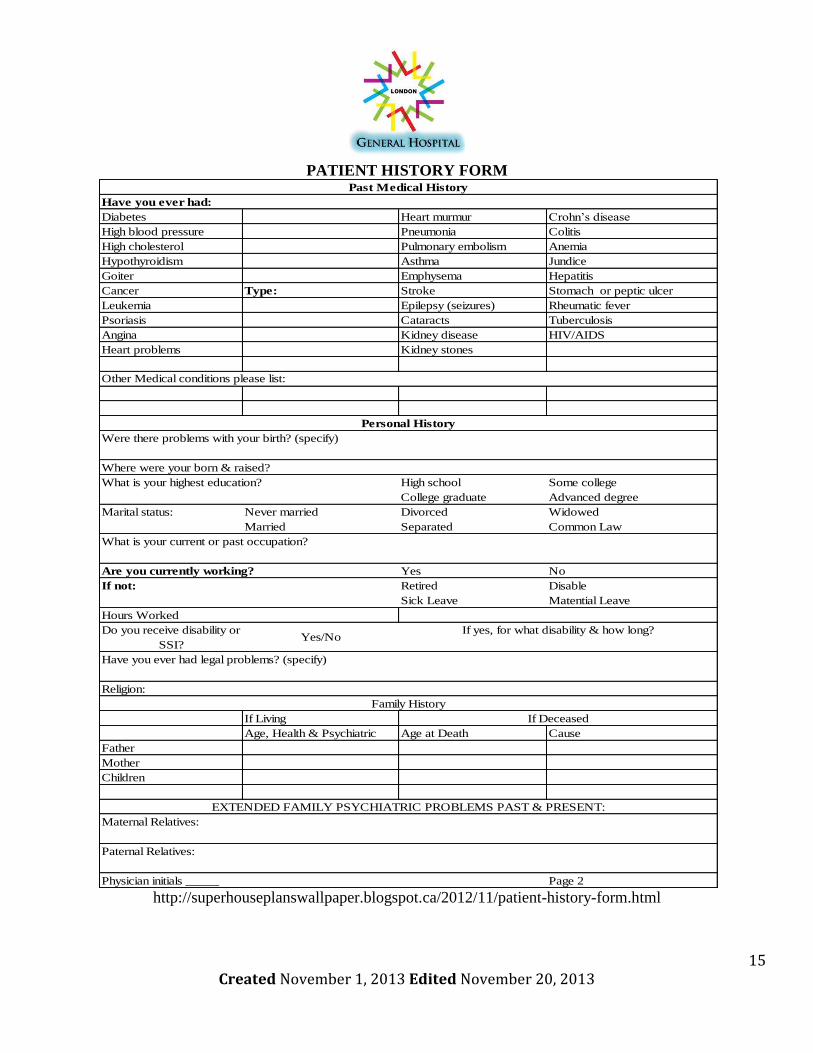
15 Created November 1, 2013 Edited November 20, 2013
PATIENT HISTORY FORM
http://superhouseplanswallpaper.blogspot.ca/2012/11/patient-history-form.html
Diabetes Heart murmur Crohn’s disease
High blood pressure Pneumonia Colitis
High cholesterol Pulmonary embolism Anemia
Hypothyroidism Asthma Jundice
Goiter Emphysema Hepatitis
Cancer Type: Stroke Stomach or peptic ulcer
Leukemia Epilepsy (seizures) Rheumatic fever
Psoriasis Cataracts Tuberculosis
Angina Kidney disease HIV/AIDS
Heart problems Kidney stones
High school Some college
College graduate Advanced degree
Marital status: Never married Divorced Widowed
Married Separated Common Law
Yes No
If not: Retired Disable
Sick Leave Matential Leave
Religion:
If Living
Age, Health & Psychiatric Age at Death Cause
Father
Mother
Children
Page 2
Do you receive disability or
SSI? Yes/No
If yes, for what disability & how long?
Family History
EXTENDED FAMILY PSYCHIATRIC PROBLEMS PAST & PRESENT:
If Deceased
Maternal Relatives:
Paternal Relatives:
Physician initials _____
What is your current or past occupation?
Were there problems with your birth? (specify)
Have you ever had legal problems? (specify)
Hours Worked
Are you currently working?
Personal History
Where were your born & raised?
What is your highest education?
Have you ever had:
Past Medical History
Other Medical conditions please list:
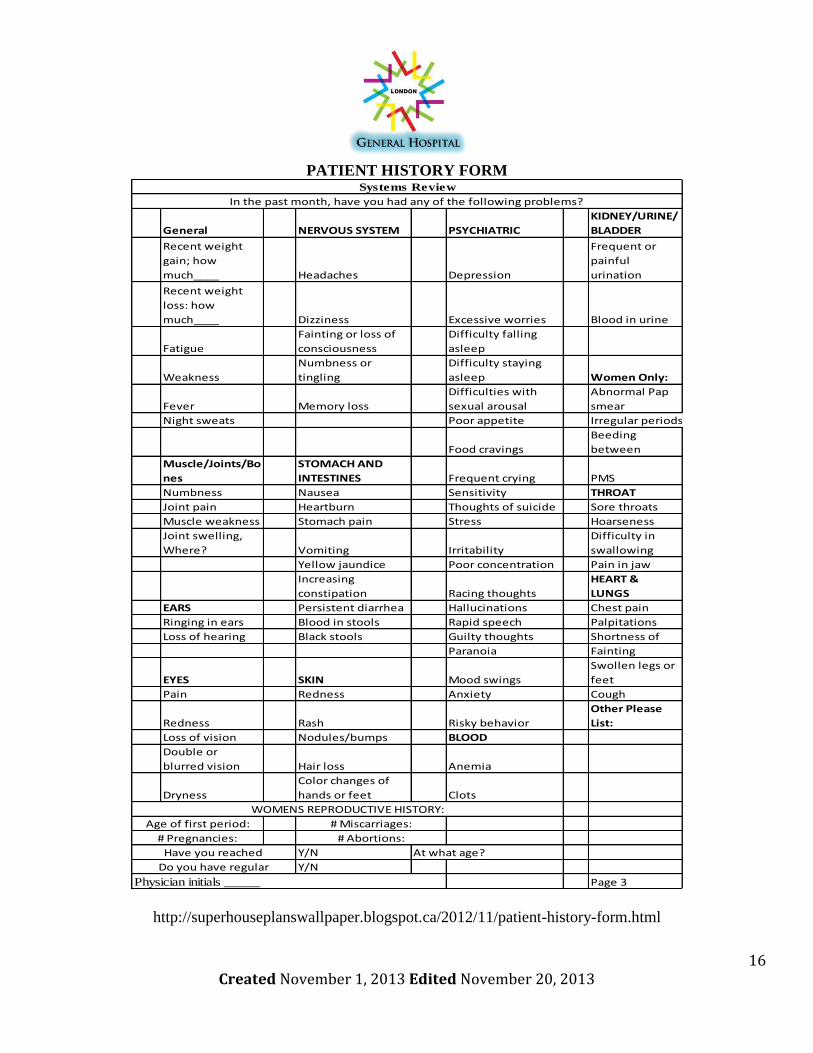
16 Created November 1, 2013 Edited November 20, 2013
PATIENT HISTORY FORM
http://superhouseplanswallpaper.blogspot.ca/2012/11/patient-history-form.html
General NERVOUS SYSTEM PSYCHIATRIC
KIDNEY/URINE/
BLADDER
Recent weight
gain; how
much____ Headaches Depression
Frequent or
painful
urination
Recent weight
loss: how
much____ Dizziness Excessive worries Blood in urine
Fatigue
Fainting or loss of
consciousness
Difficulty falling
asleep
Weakness
Numbness or
tingling
Difficulty staying
asleep Women Only:
Fever Memory loss
Difficulties with
sexual arousal
Abnormal Pap
smear
Night sweats Poor appetite Irregular periods
Food cravings
Beeding
between
Muscle/Joints/Bo
nes
STOMACH AND
INTESTINES Frequent crying PMS
Numbness Nausea Sensitivity THROAT
Joint pain Heartburn Thoughts of suicide Sore throats
Muscle weakness Stomach pain Stress Hoarseness
Joint swelling,
Where? Vomiting Irritability
Difficulty in
swallowing
Yellow jaundice Poor concentration Pain in jaw
Increasing
constipation Racing thoughts
HEART &
LUNGS
EARS Persistent diarrhea Hallucinations Chest pain
Ringing in ears Blood in stools Rapid speech Palpitations
Loss of hearing Black stools Guilty thoughts Shortness of
Paranoia Fainting
EYES SKIN Mood swings
Swollen legs or
feet
Pain Redness Anxiety Cough
Redness Rash Risky behavior
Other Please
List:
Loss of vision Nodules/bumps BLOOD
Double or
blurred vision Hair loss Anemia
Dryness
Color changes of
hands or feet Clots
Y/N At what age?
Y/N
Page 3
Have you reached
Do you have regular
Systems Review
In the past month, have you had any of the following problems?
Physician initials _____
WOMENS REPRODUCTIVE HISTORY:
Age of first period:
# Pregnancies:
# Miscarriages:
# Abortions:
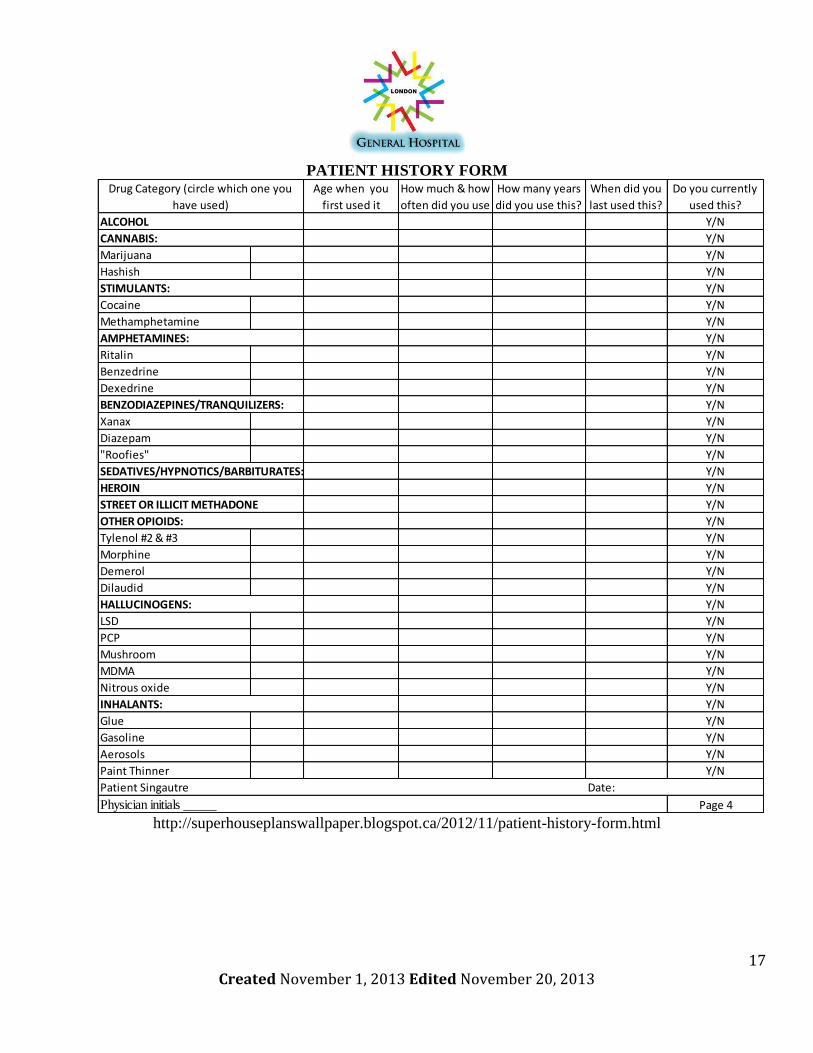
17 Created November 1, 2013 Edited November 20, 2013
PATIENT HISTORY FORM
http://superhouseplanswallpaper.blogspot.ca/2012/11/patient-history-form.html
Y/N
Y/N
Marijuana Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Page 4Physician initials _____
Patient Singautre Date:
Morphine
Demerol
Dilaudid
LSD
PCP
Mushroom
MDMA
Glue
Gasoline
Aerosols
Paint Thinner
HEROIN
STREET OR ILLICIT METHADONE
OTHER OPIOIDS:
HALLUCINOGENS:
INHALANTS:
Nitrous oxide
Tylenol #2 & #3
Xanax
Diazepam
"Roofies"
SEDATIVES/HYPNOTICS/BARBITURATES:
Dexedrine
BENZODIAZEPINES/TRANQUILIZERS:
AMPHETAMINES:
STIMULANTS:
CANNABIS:
ALCOHOL
Methamphetamine
Ritalin
Benzedrine
How many years
did you use this?
When did you
last used this?
Do you currently
used this?
Drug Category (circle which one you
have used)
Cocaine
Age when you
first used it
How much & how
often did you use
Hashish

18 Created November 1, 2013 Edited November 20, 2013
MULTI-DAY MEDICAL ADMINISTRATION FORM
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D.
Thompson, Chapter 15, pages 488
Start/
RecordedStop Date
Patinent's Name:
MR #:
DOB:
Physican:
Schedule Medical Admission Record
Medication
dose, route, frequencyHour Due

19 Created November 1, 2013 Edited November 20, 2013
SINGLE DAY MEDICAL ADMINISTRATION RECORD
SCHEDULED MEDICATION ADMINISTRATION RECORD
From To LAST NAME, First Name
ALLERGIES: Address, City, Province
Diagnosis MR # Doctor
Hour 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6
Initial
Initial
Initial
Initial
Initial
Initial
Room # Bed # MAR Checked by Page 1
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D.
Thompson, Chapter 15, pages 487

20 Created November 1, 2013 Edited November 20, 2013
PRE-OPERATIVE FORM
Page 1
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D.
Thompson, Chapter 15, pages 490-491
Language Spoken: English Other: Nickname/Preferred Name .
Surgery:
Allergies:
alert confused agitated unconscious relaxed apprehensive
Other:
Yes No
Lab Work
NOT
APPLICABLE ON ON CHART
CALL TO
OR
1 CBC ………………………………………………………………..
2 Urinalysis ……………………………………………………..
3 Electrolytes ………………………………………………...
4 HCG ………………………………………………………………
5 Gr & Reserve Serum …………………………………….
6 C & T# units ………………………………………….
7 Glucose/BUN/Creatnine …………………………….
8 FBS @ …………………………………………………….
9 Addressograph ……………………………………………
10 Other .
Other Documentation
NOT
APPLICABLE ON ON CHART
CALL TO
OR
1 Consent ………………………………………………………..
2 History / Physical ………………………………………...
3 Medical Consult …………………………………………..
4 Surgical Consult …………………………………………...
5 Anaesthetic Consult …………………………………...
6 Chest X-Ray / Other ……………………………
7 Pre-op Prep (Type )………………………..
8 Pre-anaesthetic Questionnaire .
9 Addressograph ……………………………………………….
10 Face Sheet ……………………………………………………
11 Arm Band on Patient …………………………………….
12 Other .
Surgery Date: Time: .
Mental Status: (Circle as appropriate)
PRELIMINRY PRE-OP PREPARATION
Any change in health history since pre-admit/ admission assessment?

21 Created November 1, 2013 Edited November 20, 2013
PRE-OPERATIVE FORM
Page 2
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D. Thompson, Chapter 15, pages 490-491
IMMEDIATE PRE-OP
PREPARATION NOT APPLICABLE PRESENT REMOVED
Contact Lenses/Glasses Type
Heating Aid Locked up
Prosthesis (Type) Home
Valuables Caps
Nail Polish Loose
Make Up Dentrues Top Bottom
Medic Alert Tag
Dental work
PRESENT REMOVED
Given
Held
Not Order
Order Sheet
MAR
Anaesthetic Record
NPO No Yes @
Voided No Yes @
Catheterized No Yes @
I.V. Therapy No Yes
Blood Infusing No Yes
Oxygen No Yes
To OR Via Surgilift @ hrs. Initials
Stretcher @ hrs. Initials
Crib @ hrs. Initials
Walking @ hrs. Initials
Carried by Paretns @ hrs. Initials
Bed @ hrs. Initials
Initials
Initials
Signed Off:
Pre-op Medication
Received in OR @
Doctor Please See/ Call @ .
Recovery room: Lab Work top Be Done SPECIFY: .
Type cc/hr
@ cc/hr
@ l itres/min or %

22 Created November 1, 2013 Edited November 20, 2013
RESPONSIBILITIES OF THE CLINICAL SECRETARY

23 Created November 1, 2013 Edited November 20, 2013
RESPONSIBILITIES OF THE MEDICAL ADMINISTRATION ASSISTANTS THROUGHOUT
THE HOSPITAL
Daily:
Prepare patient documents and files
Manage phone calls, meetings and appointments
Maintain office environment
Handle patient and other hospital staff questions
Transfer files and phone calls from department to department
Deal with billing, i.e. OHIP and insurance
Back up medical files
Deal with hospital staff and doctors
Weekly: Please also see Daily.
Deal with drug reps
Order office supplies
Possibly assist doctors with medical research
Calculate hours for payroll
Back up medical files
Monthly: Please also see Daily and Weekly.
Print medical reports, audits
Back up medical files
24 Created November 1, 2013 Edited November 20, 2013
POSTING INSTRUCTIONS

25 Created November 1, 2013 Edited November 20, 2013
CODES FOR EMERGENCIES
http://www.stjoes.ca/default.asp?action=article&ID=1185
Name of Code IncidentCode Red Fire
Code Blue Cardiac Arrest
Code Green Internal Evacuation
Code Yellow Missing Patient
Code Black Bomb Threat
Code White Violent situation
Code Brown Chemical Spill
Code Orange External Disaster
Code Purple Hostage/Abduction
Code Grey Loss of essential services

26 Created November 1, 2013 Edited November 20, 2013
DESCRIPTION OF THE CODES
http://www.stjoes.ca/default.asp?action=article&ID=1185
Code DescriptionIn case of a fire:
Call 911
Activate the fire alarm closest to you
Get patients and staff members to a safe
location
Close all doors to confine the fire and
smoke
If safe to do so, use a fire extinguisher to
tame the fire
In case of cardiac event:
Page for the nearest doctor or nurse
Start CPR right away
In Case of Evacuation:
Call 911
Evacuate all patients, employees and
volunteers to a safe location
Use stairs and not elevators
File out of the building as claimly and
quickly as possible
Code Red
Code Blue
Code Green
Code DescriptionIn case of a missing person and
location is unknown:
Call security
Be aware of all patients in the unit
Make sure to be informed about patients
leaving the unit
In case of a bomb threat:
CALL POLICE
Staff should NOT handle any packages
that are suspicious looking
Stay calm
Try and get as much information if it is a
caller giving a bomb treat
In case of Violent or threaten
behaviour:
Call security
Page a code white in the location the
Keep staff and patient safe and aware of
the situation
Code White
Code Yellow
Code Black
Code DescriptionIn Case of Chemical Spill:
Follow procedures and polices set by the
Containment and Chemical Team
Respond to the situation quickly, safely,
effective and efficiently
In case of an External Disaster:
Follow protocol issued by the
Emergency Prepared Team
Be flexible with any disasters that may
occur
In case of a Hostage Crisis:
CALL POLICE
Stay calm and co-operate with the
perpetrators
Observe and gather as much information
In case of loss or interruption of vital and
critical services
E.X. hydro, ventilation
Code Purple
Code Grey
Code Brown
Code Orange

27 Created November 1, 2013 Edited November 20, 2013
CARDIOPULMONARY EMERGENCIES
When there is a cardiopulmonary emergency anywhere in the hospital, follow the directions below to
save lives and to prevent any loss of life or injuries due to the situation.
CARDIOPULMONARY EMERGENCY DIRECTIONS:
1. Page a Code Blue to the location of the emergency so that any available nearby doctors
and nurses can assist with the emergency.
2. Assess what type of cardiopulmonary emergency it is.
3. Perform the relevant lifesaving procedure(s).
4. Notify the proper departments and ensure proper communication protocol is followed.
5. Complete mandatory training for all staff in First Aid, CPR & AED.
H1N1 PROTOCOL
As a big hospital, it is very critical that the administration assistants don’t spread disease around to the
rest of the population. Below are directions to take appropriate measures to prevent exposure from any
viruses spreading to other patients and staff.
H1N1 PROTOCOL DIRECTIONS:
1. Reduce likely sources of infection by putting off surgeries and visits for patients that may
be infected with H1N1, deny visits to patients from outside family that may be infected as
well. Staffs that are ill should stay at home and not go to work.
2. Make workplace preventative from ergonomics by installing partitions to reduce airborne
transmission from/to each other; have ventilation inside the facility to use for airborne
treatments. Make sure in the labs that they use hazmat suits; have proper ventilation in
ambulances, and make sure hands free soap and water dispensers are placed in
abundance.
3. Make sure all staff has a flu shot or the most up to date vaccine against H1N1. Any
patients that may have H1N1 should be isolated. Make sure proper hygiene/cough
etiquette is followed. Make sure to use precautions for patients and staff if there is any
indication they may be infected at hospital entrances. Make sure to clean frequently
touched surfaces.
4. Make sure to use appropriate Personal Protective Equipment.
http://www.cdc.gov/h1n1flu/guidelines_infection_control.htm

28 Created November 1, 2013 Edited November 20, 2013
TRAINING SESSION

29 Created November 1, 2013 Edited November 20, 2013
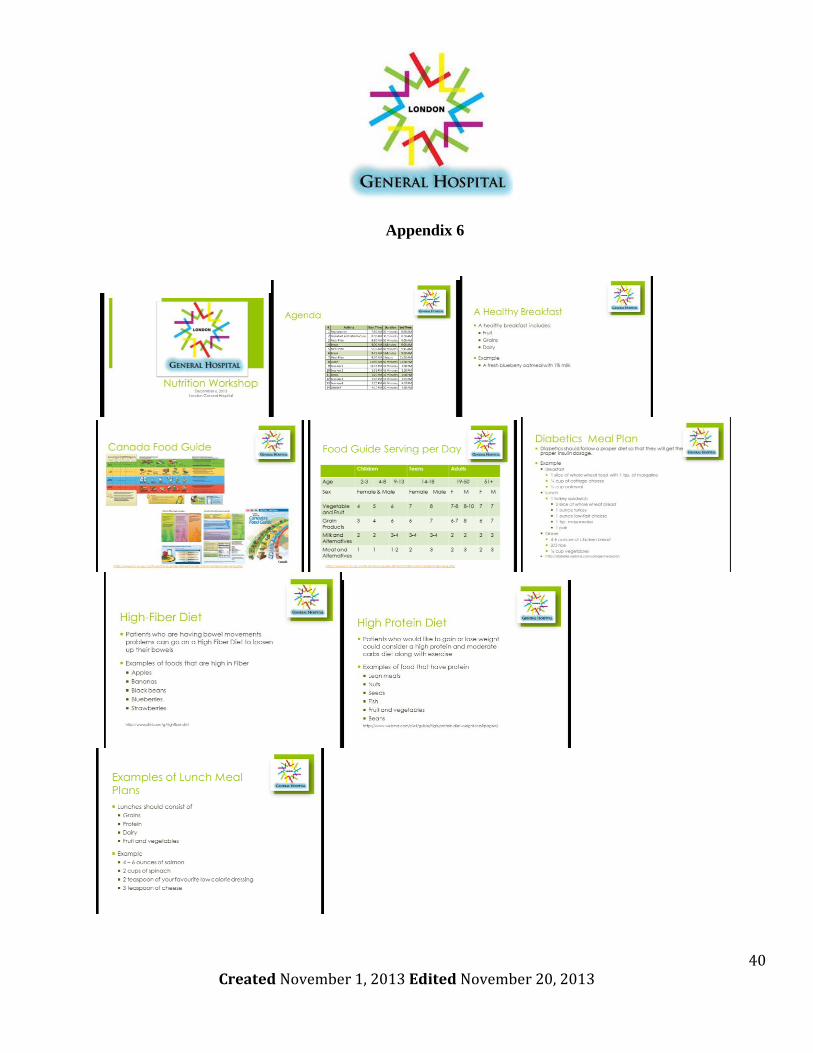
OVERVIEW OF NUTRITION WORKSHOP
This workshop will be about nutrition that people can do for themselves and to patients. The presenters
will give examples of different nutritional needs for everyone from expectant mothers to people who
have diabetes.
Participants will learn that one patient’s diet will be different from another patient, so they will have to
make sure that all allergies and food restrictions are placed in the patients’ files, so they are given the
proper meals if they are staying for a long time period at the hospital.
The workshop will be held on the first Friday, of December, every year, from 8 am to 4:30 pm.
Breakfast and lunch are provided, and they are also for training purposes. This year, the workshop is on
December 6th
.
There will be only 100 spots available, so please register as soon as you can. The workshop[ will start in
a conference room at the Best Western Lamplighter Inn on 591 Wellingtons Rd, and as the day goes on,
the participants will go to the room they are assigned to.
The equipment that will be required for this training will be as follows (was follow):
Computer or laptop to play the PowerPoint
Projector
Various tubes for the hands on sessions
o Levine/N-G tube
o G-tubes
o J-tubes
o PEG tube
Human mannequin to practice the insertions of the tubes
For full schedule of the workshop, please see attached schedule of the event. Below is a summary of
what the event will be about:
Discuss what each meal needs to have each day
Discuss meal plans for various of people
o Women who are pregnant or who just gave birth
o People who have diet restrictions due to diabetes and allergies
o People who want to gain or lose weight
o People who are having bowel movements, acute stomach problems
Hands on activities for insertions of feeding tubes for patients who need help feeding another
way
Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D. Thompson, Chapter 18, pages 577 to 589

30 Created November 1, 2013 Edited November 20, 2013
AGENDA
The day will be divided into various sessions. Below is the outline for the day:
8:30 a.m. to 9 a.m. is the Breakfast session and introduction to the training
9 to 10 a.m., participants will learn how each age group is different from one another through
genetics, activities and their gender.
10:05 to 11:30 a.m., participants will learn about the different restricted diets that some of their
patients may needs after their diagnosis.
11:30am to 12: 30 pm lunch workshop and break
12:30 pm -4 pm, participants will be divided into 4 groups. This will be the hands-on portion of the
workshop. Participants will have a choice of which activity they will like to start with and will have
a chance to do each session. Each session should be about 45 minutes long and there will be a 10 to
15 minute break between session 2 and session 3.
Nasogastric tube insertion
Jejunstomy tube insertion
Gastrostomy tube insertion
Percutaneous endoscopic gastrostomy tube insertion
4: 00 pm to 4:30 will be a debrief with everyone discussing what can be changed, what they learned
from today, if they would like to come back next year and if they would recommend it to anyone
else. Administrative and Clinical Procedures for the Canadian Health Professional, 3rd Edition, Valerie D. Thompson, Chapter 18, pages 577 to 589
# Activity Start Time Duration End Time
1 Registration 8:30 AM 30 minutes 9:00 AM
2 Breakfast and Introduction 9:00 AM 30 minutes 9:30 AM
3 Meal Plan 9:30 AM 30 Minutes 10:00 AM
4 Break 10:00 AM 5 Minutes 10:05 AM
5 Meal Plan 10:05 AM 40 Minutes 10:45 AM
6 Break 10:45 AM 5 Minutes 10:50 AM
7 Meal Plan 10:50 AM 2 hours 11:30 AM
8 Lunch 11:30 AM 50 Minutes 12:30 PM
9 Session 1 12:30 PM 45 Minutes 1:25 PM
10 Session 2 1:30 PM 45 Minutes 2:15 PM
11 Break 2:15 PM 10 minutes 2:25 PM
12 Session 3 2:25 PM 45 Minutes 3:05 PM
13 Session 4 3:10 PM 45 Minutes 3:55 PM
14 Debrief 4:00 PM 30 minutes 4:30 PM
Agenda

31 Created November 1, 2013 Edited November 20, 2013
EMAIL FOR REGISTRATION FOR THE EVENT
To: Hospital Staff
From: Board Members
CC: CEO, President
Re: Annual Nutrition Workshop
Good Day,
As many of you may know, the Hospital holds an Annual Nutrition Workshop every year for all staff
members at the hospital, including doctors and nurses. This workshop is to help staff members become
aware of the variety of meal plans that patient and even staff can be on. The more aware staff members
are with these plans, the more patients will become healthier and longer living.
When: December 6, 2013
Time: 8:30 am to 4:30 pm
Where: Best Western Lamplighter Inn on Wellington Street
Registration Deadline: November 30, 2013
Fee: $50
Payment to: London General Hospital
Each participant that is involved will get breakfast, lunch and a certificate for participating in the event.
Attached is an agenda of the event and a registration form. Please fill out the registration form and
return it with the fee by November 30, 2013. If you have any questions or would like more information
about the event, feel free to contact us at 519-685-9987 or at nutrition @lgh.on.ca.
Thank you and we hope to see you at the event.
Sincerely,
Ashley Pham
Nutrition Office Assistant

32 Created November 1, 2013 Edited November 20, 2013
REGISTRATION FORM AND FLYER
Date of Event December 06 2013 Time 8 am to 4:30 pm
Registration Last
Name
Registration
First Name
Profession Title
Address City & Province Postal Code
Phone Number Cell Phone #
Work Phone # E-mail
1st Choice 2nd Choice 3rd Choice 4th Choice
Nasogastric tube
insertion
Jejunstomy tube
insertion
Gastrostomy
tube insertion
Percutaneous
endoscopic
gastrostomy tube
insertion
Registration Form for Nutrition Workshop
Choices for session, Please Rate from 1 to 4 for each topic. 1 = 1st choice, 4 = last choice

33 Created November 1, 2013 Edited November 20, 2013
REMINDER EMAIL
To: Hospital Staff
From: Board Members
Re: Reminder for Annual Nutrition Workshop
Good Day,
This is a reminder this upcoming Friday December 6th
, 2013 is the Annual Nutrition Workshop. If you
were unable to register for the event this year, we are glad to say that we are offering it again on
December 5, 2014.
Again, the upcoming Nutrition Workshop is on December 6th
, 2013. Please come at 8:30 am for
registration and Breakfast starts right at 8 am.
Feel free to contact us if there is any concern, or questions. See you bright and early!
Sincerely,
Ashley Pham
Nutrition Office Assistant

34 Created November 1, 2013 Edited November 20, 2013
APPENDIX

35 Created November 1, 2013 Edited November 20, 2013
Appendix 1
Minutes of Meeting
Location: Fanshawe College, F3009
Date: November 1, 2013
Time: 1:30 pm to 3:00 pm
Purpose: To discuss contract, meetings, and divide work
Recorder: Ashley Pham
Attendees:
Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic
CC:
Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic
Discussion
Topic 1
Action Items Who When
Contract Ashley Pham
Ting Ting Nie
Qiaohong Li
Ana Escobar
Chris Carantonis
Teo Kesic
November 1, 2013
Topic 2
Action Items Who When
Divide Work Ashley Pham
Ting Ting Nie
Qiaohong Li
Ana Escobar
Chris Carantonis
Teo Kesic
November 1, 2013
Next Meeting
Date: November 6, 2013
Time: 11 am – 12 pm
Location: Fanshawe College
Room Number: TBA
36 Created November 1, 2013 Edited November 20, 2013
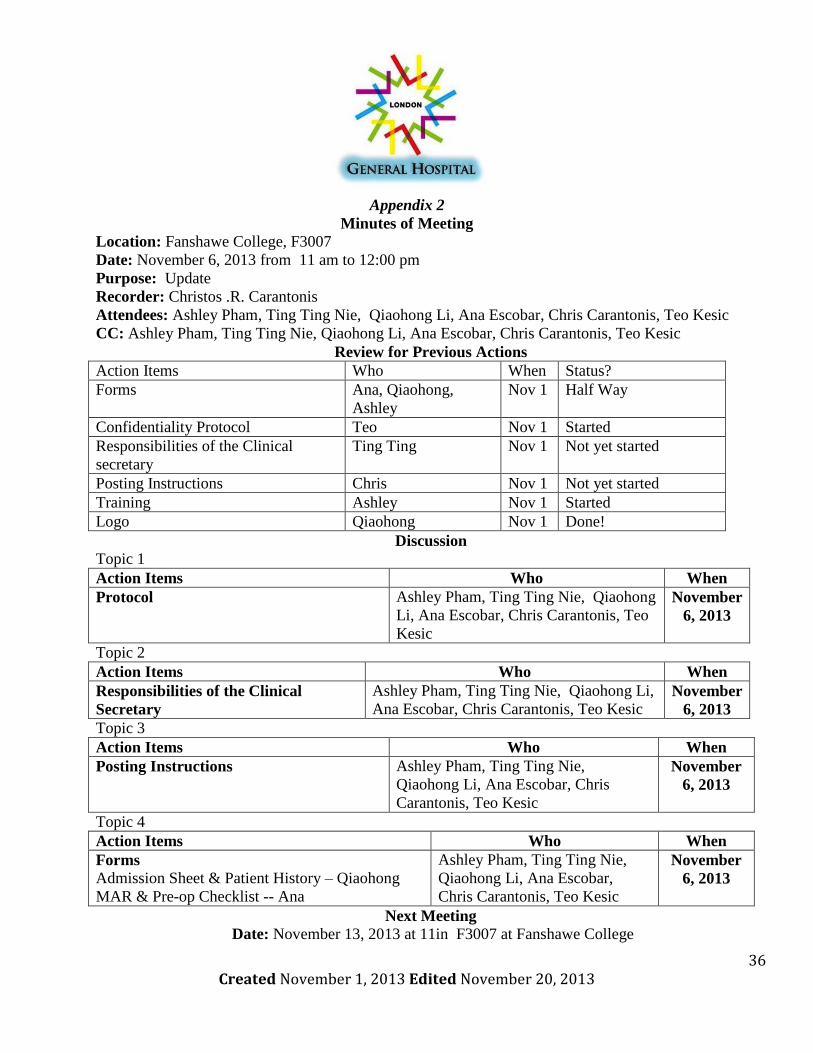
Appendix 2
Minutes of Meeting
Location: Fanshawe College, F3007
Date: November 6, 2013 from 11 am to 12:00 pm
Purpose: Update
Recorder: Christos .R. Carantonis
Attendees: Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic
CC: Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic
Review for Previous Actions
Action Items Who When Status?
Forms Ana, Qiaohong,
Ashley
Nov 1 Half Way
Confidentiality Protocol Teo Nov 1 Started
Responsibilities of the Clinical
secretary
Ting Ting Nov 1 Not yet started
Posting Instructions Chris Nov 1 Not yet started
Training Ashley Nov 1 Started
Logo Qiaohong Nov 1 Done!
Discussion
Topic 1
Action Items Who When
Protocol Ashley Pham, Ting Ting Nie, Qiaohong
Li, Ana Escobar, Chris Carantonis, Teo
Kesic
November
6, 2013
Topic 2
Action Items Who When
Responsibilities of the Clinical
Secretary
Ashley Pham, Ting Ting Nie, Qiaohong Li,
Ana Escobar, Chris Carantonis, Teo Kesic November
6, 2013
Topic 3
Action Items Who When
Posting Instructions Ashley Pham, Ting Ting Nie,
Qiaohong Li, Ana Escobar, Chris
Carantonis, Teo Kesic
November
6, 2013
Topic 4
Action Items Who When
Forms
Admission Sheet & Patient History – Qiaohong
MAR & Pre-op Checklist -- Ana
Ashley Pham, Ting Ting Nie,
Qiaohong Li, Ana Escobar,
Chris Carantonis, Teo Kesic
November
6, 2013
Next Meeting
Date: November 13, 2013 at 11in F3007 at Fanshawe College

37 Created November 1, 2013 Edited November 20, 2013
Appendix 3
Minutes of Meeting
Location: Fanshawe College, F3007
Date: November 7, 2013 at 10 am to 12 pm
Purpose: Update
Recorder: Qiaohong Li
Attendees: Ashley Pham, Ana Escobar, Chris Carantonis, Ting Ting Nie , Qiaohong Li ,Teo Kesic
CC: Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic
Review for Previous Actions
Action Items Who When Status?
Forms Ana, Qiaohong, Ashley, Ting Ting Nov 6 Almost done
Confidentiality Protocol Teo Nov 6 Started
Responsibilities of the Clinical
secretary
Ting Ting Nov 6 Done!
Posting Instructions Chris Nov 6 Codes started
Training Ashley Nov 6 Just have to do
PowerPoint
Logo Qiaohong Nov 6 Done!
Discussion
Topic 1
Action Items Who When
Protocol Ashley Pham, Ting Ting Nie, Qiaohong
Li, Ana Escobar, Chris Carantonis, Teo
Kesic
November 7,
2013
Topic 2
Action Items Who When
Training Ashley Pham, Ting Ting Nie, Qiaohong
Li, Ana Escobar, Chris Carantonis, Teo
Kesic
November 7,
2013
Topic 3
Action Items Who When
Posting Instructions Ashley Pham, Ting Ting Nie, Qiaohong
Li, Ana Escobar, Chris Carantonis, Teo
Kesic
November 7,
2013
Topic 4
Action Items Who When
Forms
Ashley Pham, Ting Ting Nie, Qiaohong
Li, Ana Escobar, Chris Carantonis, Teo
Kesic
November 7,
2013
Next Meeting
Date: November 13, 2013, Time: 11 am – 12 pm, Location: Fanshawe College, Room Number: TBA

38 Created November 1, 2013 Edited November 20, 2013
Appendix 4
Minutes of Meeting
Location: Fanshawe College, F3007
Date: November 13, 2013
Time: 11 a.m. to 12:00 p.m.
Purpose: Update & discuss formatting
Recorder: Ting Ting Nie
Attendees: Ashley Pham, Ana Escobar, Chris Carantonis, Ting Ting Nie , Qiaohong Li ,
Regrets: Teo Kesic
CC: Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic
Review for Previous Actions
Action Items Who When Status?
Forms Ana, Qiaohong,
Ashley, Ting Ting
Nov 7 Done!
Confidentiality Protocol Teo Nov 7 Done!
Responsibilities of the Clinical
secretary
Ting Ting Nov 7 Done!
Posting Instructions Chris Nov 7 Codes- Done!
Others need to start
Training Ashley Nov 7 Done!
Logo Qiaohong Nov 7 Done!
Discussion
Topic 1
Action Items Who When
Logo and formatting Ashley Pham, Ting Ting Nie,
Qiaohong Li, Ana Escobar,
Chris Carantonis, Teo Kesic
November 13
Topic 2
Action Items Who When
Posting Instructions Ashley Pham, Ting Ting Nie,
Qiaohong Li
Ana Escobar, Chris
Carantonis, Teo Kesic
November 13
Next Meeting
Date: November 20, 2013 Time: 11 am – 12 pm Location: Fanshawe College Room Number: TBA
39 Created November 1, 2013 Edited November 20, 2013
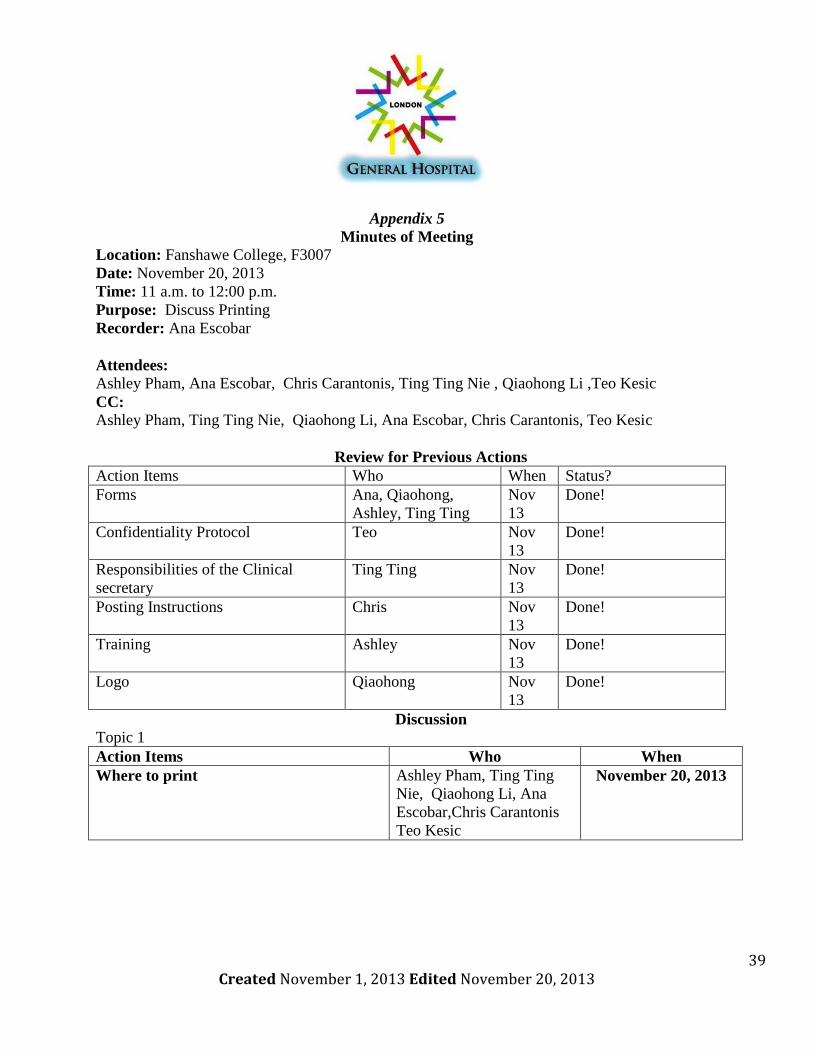
Appendix 5
Minutes of Meeting
Location: Fanshawe College, F3007
Date: November 20, 2013
Time: 11 a.m. to 12:00 p.m.
Purpose: Discuss Printing
Recorder: Ana Escobar
Attendees:
Ashley Pham, Ana Escobar, Chris Carantonis, Ting Ting Nie , Qiaohong Li ,Teo Kesic
CC:
Ashley Pham, Ting Ting Nie, Qiaohong Li, Ana Escobar, Chris Carantonis, Teo Kesic
Review for Previous Actions
Action Items Who When Status?
Forms Ana, Qiaohong,
Ashley, Ting Ting
Nov
13
Done!
Confidentiality Protocol Teo Nov
13
Done!
Responsibilities of the Clinical
secretary
Ting Ting Nov
13
Done!
Posting Instructions Chris Nov
13
Done!
Training Ashley Nov
13
Done!
Logo Qiaohong Nov
13
Done!
Discussion
Topic 1
Action Items Who When
Where to print Ashley Pham, Ting Ting
Nie, Qiaohong Li, Ana
Escobar,Chris Carantonis
Teo Kesic
November 20, 2013
40 Created November 1, 2013 Edited November 20, 2013
Appendix 6

41 Created November 1, 2013 Edited November 20, 2013
Works Cited
Centers for Disease Control and Prevention (2010). “ Interim Guidance on Infection Control Measure
for 2009 H1N1 Influenza in Healthcare settings, Including Protection of Healthcare Personals”
http://www.cdc.gov/h1n1flu/guidelines_infection_control.htm
Diet.com (2013). “High-Fiber Diet”. http://www.diet.com/g/highfiber-diet
Health Canada (2012). “Canada Food Guide.” Food and Nutrition.
http://www.hc-sc.gc.ca/fn-an/food-guide-aliment/order-commander/index-eng.php
St. Joseph’s Healthcare Hamilton (2012). “What are Hospital Emergency Codes?”
http://www.stjoes.ca/default.asp?action=article&ID=1185
Thompson V.D. (2014). “Health and the Individual” Toronto: Pearson. 54-55.
Administrative and Clinical Procedures for the Canadian Health Professional.
Thompson V.D. (2014). “Health – Care Plans” Toronto: Pearson. 305.
Administrative and Clinical Procedures for the Canadian Health Professional.
Thompson V.D. (2014). “Health Information Management” Toronto: Pearson. 423-429.
Administrative and Clinical Procedures for the Canadian Health Professional.
Thompson V.D. (2014). “The Hospital Setting” Toronto: Pearson. 464.
Administrative and Clinical Procedures for the Canadian Health Professional.
Thompson V.D. (2014). “Hospital Documents and Procedures” Toronto: Pearson. 480, 488.
Administrative and Clinical Procedures for the Canadian Health Professional.
Thompson V.D. (2014). “Hospital Documents and Procedures” Toronto: Pearson. 490-491.
Administrative and Clinical Procedures for the Canadian Health Professional.
Thompson V.D. (2014). “Order Entry” Toronto: Pearson. 511, 519-520,533.
Administrative and Clinical Procedures for the Canadian Health Professional.
Thompson V.D. (2014). “Orders Related to Nutrition” Toronto: Pearson. 577-589.
Administrative and Clinical Procedures for the Canadian Health Professional.
Toronto Central Palliative Care Network (2010). “Palliative Care Common Referral From.”
http://www.ccac-ont.ca/Upload/toronto/General/Palliative_CRF_Nov2010.pdf
Web MD (2011). “Sample Meal Plan for Diabetes.” Diabetes Health Center.
http://diabetes.webmd.com/sample-meal-plan
Web MD (2013). “High Protein Diet for Weight Loss” Weight Loss & Diet Plans.
http://www.webmd.com/diet/guide/high-protein-diet-weight-loss?page=2

















