Growth hormones / IGF POS-001-034 ABS~bK~OF ~ D ~ I N (~0W'J~ ~[][~'4[][~ ~ 110 (~0~'~t BQ[~3NE I~.,F, AS][lq~ ~ ]1%1 TYPE I DIA~rlC P ~ P.F~Ob~HK~*, G . ~ , /dD~ ~mm~S0N* , H.'][~'~** * Dep,~.~,,~,, ~ of Woai~ne II, Division of Endocrinology & MeL..~I"~,~-,,; UDi'~,al"siL-y of Vio"~ , ~tria ** Ludwig Bol,-~,.-,,,,~ I.ustitar.e for Clinical Eo~kx:r'inlog~ via~a, ~,stria S,o,ooe (o~) has been im#'h--~,',~ in the paO',ogemsis of se~ral ~',,,-,~ ~ ,.L,,_,.,.ic diaber.ic complicatinos. T, type I diabetic par{o.r_q elevated basal Cl]-levelsam well am increased GB responses to ~ stimuli have been reported. In a recent: study we fo,.-d S~LZ-i~ca~Zly hld~- m responses to ~ l~.,,~e releasing ho*mo~ ((~E) in p ~ beal~hy wum~ ~han in age m~x~ed beal~y ram*. ~ £c~s of i,e~st to mea~ m responses to ~Im 1-44 (l~g body weight; [.v.) in 22 female (age 3~_2 years) aM in 32 mnle type I diabetic p~rR (ag~ 29+_2years). Basal ~ l~Is were s~z-{C~czmgly hi~ in f~male ~ in male type I diabetic r~P,r~ (2.2 ng/ml, QI:0.8 Qg~, Q3:4.4 n~ml vs. 0.5 ng~, QI:0.2 ~ml; Q3:1.2 ng~; p~O.O001) "~. In contrast to our f~-di-Z~ ~ in hRal~ ~zdi@$~l~,~l levels after sr{nz,latlon wi~h ~ ~=peak ~ level - basal G~ level) were si~lar in female toldmale type I diabetic pat{onr_~ ~:17.6 n~nd, QI:7.3 n~ml, Q3:34.1 ng/nd vs. 18.6 ng]ml, QI:8.6 n~ml, Q3:27.5 n~ml; N.S.)**. Both in f~male and male type I diabetic pa~n~s Ix) S'~,n~Hc.~ corz'el:~t"in,:l bel:v,~IAG[l ~ eSUr~wHnl or testosgeroflel~%~Is could be estab]/shed. ~ data d~m~ting ~ ab~e of ~ dlff~ in ~ ~ to O~m in ~ype I diabetic p~r~ ~ ~ e~a~ of ~ abnmmal regulation of 6H s~xetion in diabetes melli~s. * Lamg I, Schernrhan~r G, P ~ P, Kurz P., Stephems(n ~ Templ H, 1987 J ~ I ~ i Metab 65:535 **Results are #~as me medinn value the lower (QI) and the upper quard/e (Q3). POS-001-035 GROWTH HORMONE SECRETION AND SLEEP BEHAVIOUR DURING HYPER- AND HYPOGLYCEMIC NIGHTS IN TYPE-I-DIABETICS. H WALTER, I FAERBER, I KARG, H SCHULZ, H MEHNERT III. Med. Dept. City Hospital Munich-Schwabing, Munich, FRG There is accumulating evidence that sleep-induced growth hormone (HGH) secretion causes the dawn phenomenon. Increased HGH levels are found during hyperglycemia in type I diabetics. We studied HGH secretion pattern and sleep behaviour (SB) in 8 male, C-peptide negative type I diabetics (24.3 + 5.4 y of age, 6.7 + 4.1 y of D.m.) in a sleep laboratory setting (EEG, EOG, ECG7 EMG, actogramm) in--random order during 2 separate nights: hyperglycemia (BG 150-250 mg/dl) and induced hypo- glycemia (BG < 50 mg/dl). Blood was drawn every 15 min. and analysed for BG, FFA, insulin, HGH, cortisol, glucagon and adrenalin. The sleep was characterised by a polygraphic sleep stage scoring. 8 age matched healthy males served as controls. There were no significant differences in SB (duration, efficiency, stages) in the 2 groups. Inspite of elevated baseline HGH levels (2.3+1.1 ng/ml) sleep induced HGH secretion and pattern was not increased in diabetics in the hyperglycemic night. In contrast to the waking state no typical EEG pattern could be detected during nocturnal hypoglycemia in diabetic patients. Disturbances or interruption of sleep (EEG) was related to the increase of catecholamines. Our data indicate, that in type I diabetics there is an intact, not exaggerated response of HGH in- duced by ~-sleep inspite of hyperglycemia. This explains the day to day variation of the dawn phenomenon. Sleep behaviour is not disturbed by the hypoglycemia it- self but by the process of counterregulation, which only causes a shift in sleep stage. This accounts for the fact, that nocturnal hypoglycemia is often overslept by diabetic patients. $94
Transcript
Growth hormones / IGF
POS-001-034 ABS~bK~ OF ~ D ~ IN (~0W'J~ ~[][~'4[][~ ~ 110 (~0~'~t BQ[~3NE I~.,F, AS][lq~ ~ ]1%1 TYPE I DIA~rlC P ~
P.F~Ob~HK~*, G . ~ , /dD~ ~mm~S0N* , H. ' ] [~ '~* * * Dep,~.~,,~,, ~ of Woai~ne II, Division of Endocrinology & MeL..~I"~,~-,,; UDi'~,al"siL-y of Vi o"~ , ~tria ** Ludwig Bol,-~,.-,,,,~ I.ustitar.e for Cl in ica l Eo~kx:r'inlog~ v i a ~ a , ~ , s t r i a
S,o,ooe (o~) has been im#'h--~,',~ in the paO',ogemsis o f s e ~ r a l ~',,,-,~ ~ ,.L,,_,.,.ic diaber.ic complicatinos. T, type I d iabe t i c par{o.r_q elevated basal Cl]-levels am well am increased GB responses to ~ stimuli have been reported. In a recent: s tudy we fo,.-d S~LZ-i~ca~Zly h l d ~ - m responses to ~ l ~ . , , ~ e r e l ea s ing ho*mo~ ( (~E) in p ~ beal~hy wum~ ~han in age m~x~ed beal~y ram*. ~ £ c ~ s of i,e~st to mea~ m responses to ~Im 1-44 (l~g body weight; [.v.) in 22 female (age 3~_2 years) aM in 32 mnle type I diabetic p~rR (ag~ 29+_2 years). Basal ~ l~Is were s~z-{C~czmgly hi~ in f~male ~ in male type I diabetic r~P,r~ (2.2 ng/ml, QI:0.8 Qg~, Q3:4.4 n~ml vs. 0.5 ng~, QI:0.2 ~ml; Q3:1.2 ng~; p~O.O001) "~. In contrast to our f~-di-Z~ ~ in hRal~ ~zdi@$~l~,~l levels after sr{nz,latlon wi~h ~ ~=peak ~ level - basal G~ level) were si~lar in female told male type I diabetic pat{onr_~ ~:17.6 n~nd, QI:7.3 n~ml, Q3:34.1 ng/nd vs. 18.6 ng]ml, QI:8.6 n~ml, Q3:27.5 n~ml; N.S.)**. Both in f~male and male type I diabetic pa~n~s Ix) S'~,n~Hc.~ corz'el:~t"in,:l bel:v,~IAG[l ~ eSUr~wHnl or testosgerofle l~%~Is could be estab]/shed. ~ data d~m~ting ~ ab~e of ~ dlff~ in ~ ~ to O~m in ~ype I diabetic p~r~ ~ ~ e~a~ of ~ abnmmal regulation of 6H s~xetion in diabetes melli~s.
* Lamg I, Schernrhan~r G, P ~ P, Kurz P., Stephems(n ~ Templ H, 1987 J ~ I ~ i Metab 65:535 **Results are #~as me medinn value the lower (QI) and the upper quard/e (Q3).
POS-001-035 GROWTH HORMONE SECRETION AND SLEEP BEHAVIOUR DURING HYPER- AND HYPOGLYCEMIC NIGHTS IN TYPE-I-DIABETICS.
H WALTER, I FAERBER, I KARG, H SCHULZ, H MEHNERT III. Med. Dept. City Hospital Munich-Schwabing, Munich, FRG
There is accumulating evidence that sleep-induced growth hormone (HGH) secretion causes the dawn phenomenon. Increased HGH levels are found during hyperglycemia in type I diabetics. We studied HGH secretion pattern and sleep behaviour (SB) in 8 male, C-peptide negative type I diabetics (24.3 + 5.4 y of age, 6.7 + 4.1 y of D.m.) in a sleep laboratory setting (EEG, EOG, ECG7 EMG, actogramm) in--random order during 2 separate nights: hyperglycemia (BG 150-250 mg/dl) and induced hypo- glycemia (BG < 50 mg/dl). Blood was drawn every 15 min. and analysed for BG, FFA, insulin, HGH, cortisol, glucagon and adrenalin. The sleep was characterised by a polygraphic sleep stage scoring. 8 age matched healthy males served as controls. There were no significant differences in SB (duration, efficiency, stages) in the 2 groups. Inspite of elevated baseline HGH levels (2.3+1.1 ng/ml) sleep induced HGH secretion and pattern was not increased in diabetics in the hyperglycemic night. In contrast to the waking state no typical EEG pattern could be detected during nocturnal hypoglycemia in diabetic patients. Disturbances or interruption of sleep (EEG) was related to the increase of catecholamines. Our data indicate, that in type I diabetics there is an intact, not exaggerated response of HGH in- duced by ~-sleep inspite of hyperglycemia. This explains the day to day variation of the dawn phenomenon. Sleep behaviour is not disturbed by the hypoglycemia it- self but by the process of counterregulation, which only causes a shift in sleep stage. This accounts for the fact, that nocturnal hypoglycemia is often overslept by diabetic patients.
$94
POS-001-036 PARADOXICAL GROWTH HORMONE(GH) RESPONSES TO THYROTROPIN- AND LUTENIZING-HORMONE-RELEASING HORMONE(TRH AND LHRH) AND DOPAMINE ANTAGONISTS IN NON-INSULIN DEPENDENT DIABETES MELLITUS (NIDDM): PARTICIPATION OF DIABETIC CONTROL AND RETINOPATHY.
K.YASUDA, M.KITADA*, E.GOSHIMA*, N.TAKEDA, M.HAYASHI, S.GOTO, K.AOYAMA, K.MIURA Department of Medicine, Glfu University, Gifu 500, and Matsunami Hospital*, Glfu 501-61, Japan.
In total 119 patients with NIDDM and 57 normal subjects, plasma GH responses to TRH(500 pg, i.v., 71 patients, mean age 55 years), LHRH(100 pg l.v., 58 patients, mean age 55 years), meto- clop=amlde(MCP, i0 mg i.v., 27 patients, mean age 52 years), and domperldone(DP, i0 mg l.v., 33 patients, mean age 53 years) were measured during 2 hours. Both TP, H and LHRH tests and also both MCP and DP tests were performed in 51 and 19 patients, respectively. Paradoxical increase in GH was defined as the response of AGH(difference of peak and basal values) above 3 ng/ml. Basal GH level was significantly higher in NIDDM(2.1 ± 1.7 ng/ml, mean ± SD) than in normal suhjects(l.6 ± 0.4). None of normal subjects except a case in DP test responded above 3 ng/ml of AGH during these tests. Mean peak GH values in NIDDM were 5.5, 5.2 ng/ml in TRH and LHRN tests, and 4.8, 5.3 ng/ml In MCP and DP tests, respectively. Incidence of paradoxical GH response were 38% (27 cases) to TRH, 41% (24 cases) to LHRH, 30% (8 cases) to MCP and 39% (13 cases) to DP. There were significant correlation between basal and peak GH values in TP, H (r=0.42, p<0.001), and In LHP, H ( r=0.68, p<0.001) tests. AGH values between TRH and LHRH tests were significantly correlated each other (r= 0.75, p<0.00i). Similar relation was also observed in AGH between MCP and DP tests ( r= 0.79, p<0.001). Fasting plasma glucose and HbAlc positively correlated to AGH In TRH (r=0.68, and 0.33, p<0.001 and 0.01, respectively) or in LHRH (r=0.55, 0.57, p<both 0.001), but not coT- related to AGH in MCP or DP test. TRH and LHRH tests were repeated in respective 9 and 16 pa- tients before and after treatments. Basal and AGH decreased in both tests after treatment. There were no significant difference of AGH or incidence of paradoxical GH response between the diabetics wlth and without retlnopathy. These results suggested the possibilities that para- doxical GH rlse during TRH and LHRH tests, and during MCP and DP tests in NIDDM were due to the slmilarmechanism, respectively, and that the former phenomenon closely related to the derangement of diabetic control.
POS-001-037 NO EVIDENCE FOR NEGATIVE FEEDBACK REGULATION OF GROWTH HORMONE SECRETION VIA SONATOMEDIN-C IN INSULIN-DEPENDENT DIABETIC PATIENTS
G.SCHERNTHANER, J.STEPHENSON, P.PIETSCHMANN Department of Medicine I I , Division of Endocrinology & Metabolism, University of Vienna, Austria
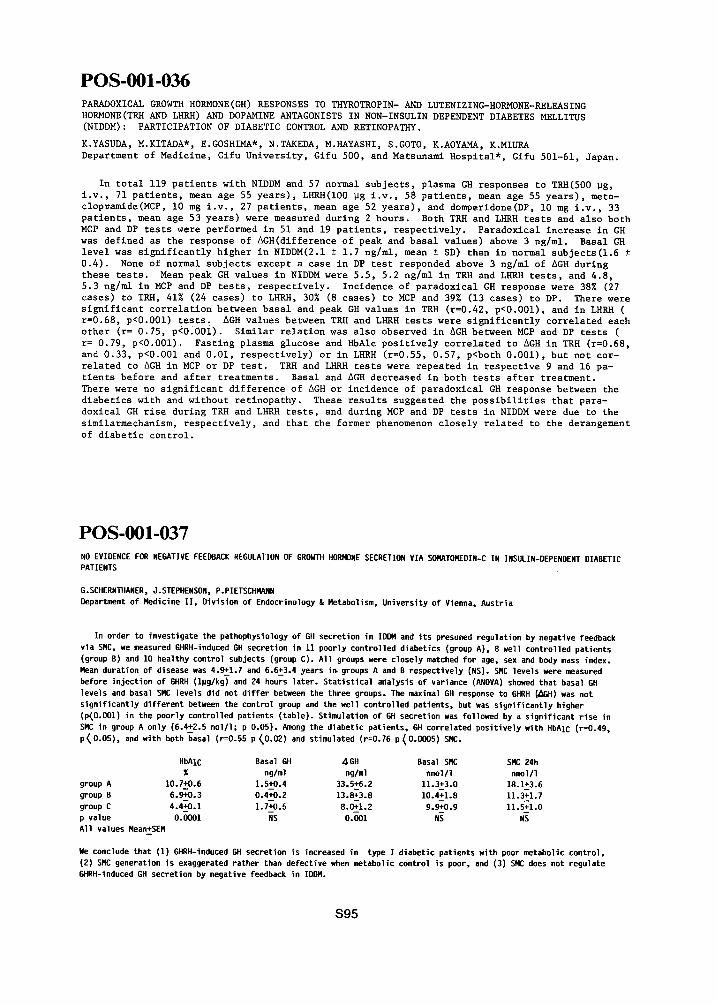
HbAIc %
group A 10.7+0.6 group B 6.9+0.3 group C 4.4+0.1 p value 0.0001 All values Mean+SEN
In order to investigate the pathophysiology of GH secretion in IDDM and i ts presumed regulation by negative feedback via SMC, we measured GHRH-induced GH secretion in 11 poorly controlled diabetics (group A), 8 well controlled patients (group B) and 10 healthy control subjects (group C). All groups were closely matched for age, sex and body mass index. Mean duration of disease was 4.9+1.7 and 6.6~3.4 years in groups A and B respectively (NSI. SMC levels were measured before injection of GHRH (lpg/kg~ and 24 hours later. Stat ist ical analysis of variance (ANOVA) showed that basal 6H levels and basal SNC levels did not d i f f e r between the three groups. The maximal GH response to GHRH (~kBH) was not s igni f icant ly di f ferent between the control group and the well controlled patients, but was s igni f icant ly higher (p~O.O01) in the poorly controlled patients (table1. Stimulation of GH secretion was followed by a signif icant r ise in SMC in group A only (6.4~2.5 no1/1; p 0.05). Among the diabetic patients, GH correlated posi t ively with HbAIc (r=0.49, p~O.OS), and with both basal (r=0.55 p (0.021 and stimulated (r=0.76 p (O.O00S) SMC.
We conclude that (1) GHRH-induced GH secretion is increased in type I diabetic patients with poor metabolic control, (21SNC generation is exaggerated rather than defective when metabolic control is poor, and (31SNC does not regulate GHRH-induced GH secretion by negative feedback in IDOM.
$95
POS-001-038 SERUM GROWTH HORMONE AND IGF-I LEVELS IN PATIENTS VlTH DIABETIC RETINOPATHY AFTER TREATMENT WITH CONTINUOUS SUBCUTANEOUS INFUSION OF OCTREOTIDE
S.L.HYER, P.S.SHARP, R.A. BROOKS, J.M. BURRIN, E.M. KOHNER. Royal Postgraduate Medical School, Hammersmith Hospital, London WI2., England
Excessive GH secretion has been implicated in the development of diabetic microvascular complications. Previous attempts at suppressing 24hr GH secretion in diabetics with proliferative retinopathy using intermittent doses of octreotlde (Sandostatln), a long acting somatostatln analogue, have not been successful. In the present study, six insulin dependent diabetics (3 male, 3 female; age 24 - 45 yrs; duration 17 - 83 yrs; mean HbAI:9.86% ) with active retlnopathy (5 proliferative, I preproliferatlve) and 4 matched healthy subjects received octreotlde 500 ug / 24 hrs for 2 weeks as a" continuous subcutaneous infusion via a portable infusion pump. 24 hr GH secretlon was completely suppressed in the normal subjects whilst the patients showed significant but not complete inhibition of GH release; mean baseline area under GH curve i SEM [patients]: 209 ! 33 mU/l.hr before treatment vs 121 t 33.6 after treatment; p<0.05). Mean serum IGF-I levels in both patients and normal subjects were markedly reduced; 203 ! 25.4 ug/l (initial) vs 60 ! 10.2 after treatment; p<0.005 (patients); 183 ! 7.1 ug/l (initial) vs 73 ± 7. i after treatment ;p<O.05 (controls). Unpleasant slde-effects (diarrhoea and abdominal pain) were common in patients and control subjects. One patient lost 7kg in weight over 3 weeks. Insulin dosage was reduced by a mean of 60% in the patients with no significant change in HbAI at the end of the study. Prospective studies to investigate whether continued therapy will influence the progression of diabetic retinopathy are currently in progress.
POS-001-039 URINARY GROWTH HORMONE LEVEL IN PATIENTS WITH INSULIN DEPENDENT DIABETES MELLITUS
0 NUKADA, J HIGUCHI, M KATAYAMA, T OMURA, S KANZAKI, M FUJIMOTO, T MORIWAKE, H KIMOTO
Department of Pediatrics, Okayama University, School of Medicine, Okayama, Japan
Increased serum growth hormone(GH) level is well known in patients with insulin dependent diabetes mellitus(IDDM). Resistance to insulin therapy is partly explained by GH elevation, since GH is a major antagonist to insulin. However, GH influence has not been evaluated in daily clinic because of the difficulty in the assessment of GH level which requires multiple blood sampling or provocative tests. These invasive tests could be circumvented by a single measurement of urinary GH(U-GH). Recent advancement in enzyme immunoassay made it possible to measure U-GH which is thought to reflect mean concentration of serum GH. GH in the morning fasting urine was measured in 45 patients with IDDM,3 to 20 years of age,and 180 age and sex matched normal controls. Patients with abnormal proximal tubular function were excluded, since GH is reabsorbed there. Results were as follows: i) U-GH was elevated above the level of +2SD in 8 patients. 2) Morning fasting blood glucose was significantly higher in patients with elevated U-GH(~+2SD) compared to those with normal U-GH(within±2SD) (247+53mg/dl vs. 134±73mg/dl), as was the HbAlc (12.1+1.7% vs. 8.5±1.9%). 3) Patients with elevated U-GH required more daily insulin dose compared to those with normal U-GH ( 0.88*0.22U/Kg vs. 0.74 ±0.38U/Kg). 4) 7 Patients with multiple insulin injection therapy showed normal U-GH level. 5) Adult patients showed normal U-GH level except for one case in spite of the fact that many of them were poorly controlled. In conclusion, U-GH was elevated in patients with poorly controlled IDDM, especially those in puberty. A vicious circle may be formed in which in- adequate insulin therapy causes GH elevation that in tern worsens diabetic control. Patients with elevated GH can be easily detected by the determination of U-GH. These patients might have much better control provided that influence of GH is eliminated. Intensive insulin therapy was suggested to be effective in normalizing GH level. U-GH will be a clinically usefull index in the control and treatment of IDDM.
$96
POS-O01-040 DERANGED CARBOHYDRATE METABOLISM BEFORE AND AFTER TREATMENT OF ACROMEGALY.
N.C.THALASSINOS,I.TZAVARA,D.FILOKYPROU,CH.NIKOLOU,P.GANIA,D.IKKOS Oepartment of Endocrinology,Evangelismos Hospital,Athens,Greece.
The increased incidence of diabetes mellitus(DM)and impaired glucose tolerance(IGT)asso- ciated with acromegaly is attributed to the raised growth hormone(GH)although no agreement exists on the relationship between GH levels and DM or IGT.To investigate this relationship an oral glucose tclerance(OGTT)with simultaneous GH determinations was performed in 133 acro- megalic patients(55 males and 78 females,aged 17-72 years)before(89 patients)and after(85 patients)treatment(41 patients assessed both before and after).According to the WHO criteria the patients were classified before treatment:11 with DM(12.4%),43 with IGT(48.3%)and 35 with normal glucose tolerance,NGT(39.3%)while after treatment the classification was:13 DM(15.3%) 25 IGT(39.4%)and 47 NGT(55.3%).According to the lowest GH value(ng/ml)the patients were classified as group A(GH ~ lO),B(GH>5<10)and C(GH ~5),NGT was found before treatment in 26 of 60 group A patients(43.3%)and in 5 of 19 group B and C patients considered together(26.3%) while after treatment the corresponding figures were 11 of 26 group A patients(42.3%) 9 of 16 group B(S6.3%)and 24 of 3B group C(63.1%).It is concluded that in acromegaly the incidence of deranged carbohydrate metabolism(DM and IGT)was found(a)higher(~60%)than hither to repor- ted and(b)not related to GH values before treatment but lower in the patients with lower GH values after treatment.
POS-O01-041 HIGH DOSE HGH THERAPY FOR RECCURENT HOUSSAY'S PHENOMENON IN A COMPLETE GH DEFICIENCY AND IDDM.
PATIENT WITH
O.MORI*, M.KODAMA, T.YAZAWA, T.KAMIJO, H.TOMITA, and M.OGAWA, Department of Pediatrics, School of Medicine, Nagoya University, Nagoya, 466, Japan.
The pathological conditions of both GH and insulin deficiency in children are not only extremely rare, but also of significant interest in studying the interaction between GH and glucose metabolism. We have experienced a patient diagnosed as isolated GH deficiency with IDDM. The patient was a Japanese boy aged 16 years. The typical Houssay's phenomenon was observed during infancy. Insulin treatment could not be initiated to correct the hyperglycemia, because of reccurent hypoglycemia and insulin hypersensitivity. Standard doses of HGH therapy ( 0.5 IU/Kg/W ) was adopted when the boy was 7 years old. HGH administration caused exaggerated hyperglycemia and ketosis instead of disappearance of Houssay's phenomenon. Therefore, insulin therapy was required and dose of insulin increased to the usual level for IDDM. Control of diabetes was fairly good during 7 years with combined therapy of standard doses of HGH and insulin, but after 7 years severe hypoglycemic attacks ocurred reccurently, so that insulin therapy could not to be continued. From repititive hormonal examination, etiology of hypoglycemia were interpreted as reccurent Houssay's phenomenon. Procedures of IVH were needed to control blood glucose levels for about 1.5 years, high dose of HGH ( 2.0 IU/kg/W ) successfully controlled the intractable hypoglycemia without any serious side effects, on the contrary, other trials including high dose hydrocortisone were of no use. In conclusion, high dose HGH therapy was the only successful choice for treatment of intractable Houssay's phenomenon in a patient with GH and insulin deficiency.
S97
POS-001-042 INCREASED MYOCARDIAL CONTRACTILITY FOLLOWING GROWTH HORMONE ADMINISTRATION IN NORMAL MAN. AN ECHOCARDIOGRAPHIC STUDY.
CHRISTIANSEN JS, THUESEN L, ORSKOV H, HENNINGSEN P Second University Clinic of Internal Medicine and University Department of Cardiology, Aarhus Kommunehospital, DK-8OOO Aarhus C, Denmark.
Cardiac function was studied by echocardiography in I I normal subjects before subcutaneous growth hormone administration ( f i r s t control), after l week of subcutaneous growth hormone administration and at one week after stopping subcutaneous growth hormone administration (second control). Plasma growth hormone was 1.4 ng/ml and 4.5 ng/ml respectively at the f i r s t two examinations. Compared to the f i r s t and second control situations heart rate increased by 9% (p < O.l) and 15% (p < O.Ol), fractional shortening of the l e f t ventricle by 8% (p < 0.02) and 9% (p < O.Ol), and mean circumferential shortening velocity by 10% (p < 0.05) and 14% (p < O.Ol) respectively. Mean arter ia l blood pressure was unchanged.
Thus, in man an increase in plasma growth hormone up to levels comparable to those seen in type l diabetics during conditions of poor metabolic control is followed by enhancement in myocardial contract i l i ty . We therefore suggest that growth hormone might contribute to the increase of myocardial cont rac t i l i ty ear l ier described in type l diabetic patients with no c l in ical signs of microvascular disease.
POS-001-043 GROWTH HORMONE CAUSES MEAL CARBOHYDRATE INTOLERANCE NOT ONLY BY DECREASING GLUCOSE UPTAKE BUT ALSO BY IMPAIRING THE POSTPRANDIAL HEPATIC RESPONSE.
R RIZZA, E KRYSHAK, P BUTLER Endocrine Research Unit, Mayo Clinic and Foundation, Rochester, MN U.S.A.
Previous studies have shown that growth hormone (GH) decreases both insulin induced suppression of hepatic glucose release (GR) and the stimulation of glucose uptake (GU) in fasting man. However, the mechanism by which GH impairs postprandial glucose tolerance is unknown. To determine the contribution of changes in GR, gluconeogenesis (GN), initial sDlanchnic glucose clearance (SGC), and GU to the GH induced alterations in meal tolerance, subjects ingested an isotopically labeled solid mixed meal during a 12 hour growth hormone infusion (4 uo/kq/min) and a 12 hour saline infusion. Fasting GH was greater (p<O.Ol) during the growth hormone infusion (26+3 vs 3+1 ng/ml) as were glucose (94+1 vs 85+1 mg/dl), insulin (14+2 vs 7+1 pU/ml), and C-pept~de (2~2+0.3 vs 1.4+0.2 ng/ml). Aft-er meal iEgestion, growth hormone-infusi~caused a greater increment (p-~O.O01) in glucose (92+14 vs 55+8 mg/dl/6h), insulin (i0.0+1.3 vs 5.1+0.9 mU/ml/6h), and C-peptide (1.3+0.1 vs 0.8--+0.1 ~g/ml76h) than did saline. DespiTe hyperglycemia and hyperinsulinemia, the grea~er postpraEdial glucose excursion with growth hormone could be totally ascribed to lower GU (181+18 vs 230+28 mg/kg/2h, p<O.02) during the first 2 hours postprandial. GR, GN, and SGC did not -aiffer durlng growth hormone and saline infusions. However, when glucose concentrations during saline were matched to those present during the growth hormone infusion by a supplemental intravenous glucose infusion, not only was postprandial glucose uptake far lower (p<O.05) during growth hormone than saline infusion (428+35 vs 735+73 mg/kg/6h) but also suppression of GR (-168+21 vs -436+71 mg/!<g/6h) was clearl~ less (p<O-~05). In summary, the hyperglycemia and hyperTnsulinemia~resent during growth hormone excess obscures growth hormone induced alterations in postprandial hepatic response. However, when glucose and insulin concentrations are matched, growth hormone has a clearly demonstrable effect on the liver. These studies indicate that in addition to decreasing glucose uptake, growth hormone also impairs meal carbohydrate tolerance by increasing postprandial hepatic glucose release.
$98
POS-001-044 PIRENZEPINE BLOCKS GROWTH HORMONE HYPERSECRETION IN TYPE-I-DIABETIC PATIENTS.
M.L.WAGNER*, B.WILLMS, J.ARENDS. Bad Lauterberg, West Germany
Pirenzepine (P) inhibi ts cholinergic muscarinic receptors (CMR) and is used in peptic ulcer disease (PUD) for more than ten years in Europe. As growth hormone (GH) secretion is also regulated by CMR we tested the effect of P in type-l-diabetics in view of the potential role of GH in the pathogenesis of diabetic microangiopathy. All experiments were done with C-peptide negative normal weight male type-l-diabetics with a duration of diabetes of more than one year.
In 8 patients GH secretion was stimulated by arginine infusion: Maximal concentration with placebo was 9.0~l.9ng/ml, with P (30 mg iv at -lOmin.) 1.5+_O.4ng/ml.
In 8 patients GH secretion was stimulated by a 30 min ergometer exercise at 75 W. With placebo GH increased to 9.0+l.4ng/ml, with P (30 mg iv at -lOmin) this increase was com- pletely blocked (peak 1.4+O?4ng/ml). In a third series of experiments, GH secretion was stimulated with l~g/kg bo~yweight GH re]easing factor (GRF). 30 mg P i .v . blocked the GH increase (l.2+l.4ng/ml vs. 16.0+12.9 ng/m]), where as 20 mg or lO mg only par t ia l l y inhibited GH sec~tion by 77% and 85% resp. In al l these experi- ments basal GH concentration was not depressed. II type-l-diabetics got 50 mg P oral ly at bedtime. Nocturnal GH was depressed and the dawn phenomenon was decreased (fasting blood glucose with placebo 186+lOmg/dl, with P 146+13mg/dl).
30 m~ P 9iven i .v . corresponds to a standard oral dose of 150 mg in PUD. Thus Pirenzepine can De glven on a long term basis and with this tool the growth hormone hypothesis of diabetic microangiopathy can be tested.
POS-001-045
CALCIUM INFLUX: AN INTRACELLULAR MESSAGE OF THE ACTION OF INSULIN-LIKE GROWTH FACTOR-I and II
E OGATA, I KOJIMA, H MATSUNAGA, I NISHIMOTO Fourth Department of Internal Medicine, University of Tokyo, Japan
The mode of action of insulin and insulin-like growth factors (IGFs) in cell proliferation is a matter of debate. In a series of studies, we could define that IGFs affect Balb/c 3T3 fibroblasts only in the primed competent state and lead to cell proliferation. The primed competnt state was induced by treating the fibroblasts at the Go state with PDGF and then with EGF (B.B.R.C. 142:275,1987). We could also observe a close linear relationship between the extent of agonist-induced calcium influx and that of DNA syn- thesis (J.Biol.Chem. 262:12120,1987).
In the present study, we showed that IGF-I and IGF-II act on their own receptors in Balb/c 3T3 cells as indicated by I) dose-response relationship, 2) anti-IGF II receptor antibody, and 3) affinity-labelling studies. The cal- cium channel was examind with cell-attached patch clamp method. It was defined I) voltage-independent, 2) sensitive not to dihydropyridine but to tetramethrin, and 3) cation non-selective. Evidence for the involvement of a pertussis toxin sensitive G protein(s) in the reaction between the receptors and the channel was also provided. Finally, it was shown that the cells in the primed competent state respond with cell proliferation when Ca ++ influx is induced by another means (BAY K 8644). We conclude that both IGF-I and II stimulate calcium influx in primed competent Balb/c 3T3 cells by activating a calcium-permeable cation channel via a G protein transduction system, and that calcim influx thus induced is an intracellular message of the mitogenic ac- tivity of IGFs.
$99
POS-001-046 EPIDERMAL GROWTH FACTOR STIMULATES INSULIN - LIKE GROWTH FACTOR I/SOMATOMEDIN-C PRODUCTION AND REDUCES ALKALINE PHOSPHTASE ACTIVITY IN MEDIUM OF CULTURED RAT CALVARIAE
H STRACKE, I LISSFELD and H SCHATZ Center of Internal Medicine, University of Giessen, Rodthohl 6, D-6300 Giessen, FRG
We previously ~emonstrated that insulin-like growth factor I/somatomedin-C (IGF I/SM-C) production occurs in fetal rat bone which can be stimulated by growth hormone in vitro. Since epidermal growth factor (EGF) is known to stimulate DNA synthesis in bone and in- hibits bone collagen synthesis in vitro (Canalis and Raisz, ]979) its effect on fetal rat calvariae was investigated. Methods: Rat calvariae from 21 days old embryos were cultured for 4 days without or with EGF (50 ng/lO0 ml medium). The medium was changed every day and alkaline phosphatase (AP) as well as IGF I/SM-C was measured in the culture media. Results: The controls showed an increase of AP values during the culture period, whereas the AP-activity decreased after addition of 50 ng EGF/]00 ml to the medium. IGF I/SM-C activity increased also during the culture period of the controls and was further enhanced when EGF was added to the medium. Conclusions:Since EGF stimulates IGF I/SM-C synthesis and inhibits AP-activity in fetal rat bone, EGF appears to be involved in the coupling of bone formation and bone resorption.
POS-001-047 PROTEIN KINASE-A, PROTEIN K1NASE-C AND CALCIUM MAY REGULATE THE METABOLIC AND M1TOGENIC EFFECTS OF INSULIN-LIKE GROWTH FACTORS ON CHONDROCYTES
A.M. TAYLOR, D.J. MORRELL, *P. DANDONA & M.A. PREECE Depar tment of Growth and Development, Ins t i tu te of Child Health and *Depar tment of Chemical Pathology and Human Metabolism, Royal Free Hospital, London, U.K.
The possible involvement of the cyclic-AMP dependent Protein Kinase-A (PKA), Protein Kinase-C (PKC) and calcium in the regulation of the metabolic and mitogenic e f fec t s of I n s u l i n - l i k ~ r o w t h Factor-I (IGF-I) was investigated by observing the e f fec ts of the following compounds on S sulphate and 3H thymidine incorporation by monolayer cul tures of porcine ar t icular chondrocytes: (a) A PKC act ivator , phorbol es ter dibutyryl (PDBU); (b) A PKC and PKA inhibitor compound H7; (c) A calcium channel antagonist (verapamil); (d) A cyclic-AMP analogue, N v, O 2'-dibutyryl adenosine 3'5'-cyclic monophosphoric acid. PDBU, like IGF-I, s t imulated the incorporation of both sulphate and thymidine into chondrocytes. Both these e f fec t s were inhibited by the compound HT.
Verapamil inhibited IGF-I and PDBU st imulated sulphate uptake but, in contras t , enhanced IGF-I and PDBU st imulated thymidine uptake.
Cyclic-AMP dibutyryl s t imulated basal and enhanced IGF-I s t imulat ion of sulphate uptake but inhibited both basal and IGF-I s t imulated thymidine incorporation by chondrocytes.
These results suggest that the mitogenic e f fec t s of IGF-I on chondrocytes may be mediated by a PKC enzyme system independent of extracel lular calcium influx, but counter - regula ted by the cyclic-AMP dependent PKA enzyme system. The metabolic e f fec t s of IGF-I may not involve PKC activity but may be mediated by cyclic-AMP dependent PKA activity which may be dependent upon extracel lular calcium influx.
Sl O0
POS-001-048 EFFECT OF INSULIN AND INSULIN-LIKE GROWTH FACTOR-I ON DNA SYNTHESIS AND GLUCOSE METABOLISM IN SMOOTH MUSCLE CELLS FROM NORMAL AND DIABETIC RATS:
HJ A r n q v i s t , K B o r n f e l d t , R G i d l ~ f , D e p a r t m e n t o f Ir. t e r n a l Med i c i n and Pharmaco logy L i n k S p i n g U n i v e r s i t y , L i n k ~ p i n g , S w e d e n .
The e f f e c t o f i n s u l i n and i n s u l i n - l i k e g rowth f a c t o r - l ( I G F - l ) on DNA s y n t h e s i s and g l u c o s e m e t a b o l i s m were s t u d i e d in a o r t i c smooth muscle c e l l s c u l t u r e d f rom normal and s t r e p t o z o t o c i n - d i a b e t i c r a t s . l n c o r p o r a t i o n o f H - t h y m i ~ i n e i n t o DNA was measured a f t e r inc~1~at ion f o r 24h o f s u b c o n f l u e n t c e l l s w i t h H - t h y m i d i n e w h i l e a ~ u m u l a t i o n o f C -g l ucose carbon was measured a f t e r lh i n c u b a t i o n in 5 .6 mM C~glucose and i n s u l i n o r I G F - I . B o t h i n s u l i R and IGF- I were found to s t i m u l a t e ~ H - t h y m i d i n e i n c o r p o r a t i o n i n t o DNA and " ~ C - g l u c o s e carbon accumu la - t i o n in c e l l s f rom normal and d i a b e t i c r a t s . H a l f maximal e f f e c t o f IGF- I on t h y m i d i n e i n c o r p o r a t i o n was o b t a i n e d a l r e a d y a t a c o n c e n t r a t i o n o f l . l n M in c e l l s f rom normal a o r t a w h i l e the po tency o f i n s u l i n to s t i m u l a t e t h y m i d i n e i n c o r p o r a t i o n w ~ abou t l O 0 - f o l d l o w e r . T h e c o n c e n t r a t i o n e f f e c t curves f o r the s t i m u l a t i o n o f C - g l u c o s e a c c u m u l a t i o n in normal smooth muscle c e l l s were s i m i - l i a r f o r i n s u l i n and IGF- I w i t h a h a l f maximal e f f e c t o b t a i n e d a t about lOnM. There ~as no d i f f e r e n c e in the c o n c e n t r a t i o n - e f f e c t curves f o r IGF- I and i n s u - l i n on H - t h y m i d i n e i n c o r p o r a t i o n between normal and d i a b e t i c v a s c u l a r smooth muscle c e l l s . H o w e v e r d i a ~ t i c c e l l s tended to be more s e n s i t i v e f o r the e f f e c t o f i n s u l i n and IGF- I on C - g l u c o s e a c c u m u l a t i o n but the d i f f e r e n c e was not s i g n i f i c a n t . In c o n c l u s i o n DNA-syn thes is in v a s c u l a r smooth muscle c e l l s f rom normal r a t s is about l O 0 - f o l d more s e n s i t i v e f o r IGF- I than i n s u l i n w h i l e the c o n c e n t r a - t i o n - e f f e c t curves f o r g l ucose a c c u m u l a t i o n are s i m i l i a r f o r bo th hormones.
POS-001-049 INSULIN-LIKE GROWTH FACTOR 1 CONCENTRATION IN AMNIOTIC FLUID DIFFERS IN DIABETIC AND NON-DIABETIC PREGNANCIES
A D WRIGHT,J CHAPMAN, F LAWTON, H SHAKESPEAREand H NICHOLSON Birmingham General Hospital, Birmingham Maternity Hospital, Birmingham Hospital for Women and Dudley Road Hospital, Birmingham
The role of growth factors in foetal development is receiving increasing attention. This may be of particular relevance to foetal development in diabetic women, in whom there persists an increased incidence of foetal morbidity, mortality and macrosomia. The mRNA concentration for IGF-I and IGF-II in placentae from diabetic women have been shown to be higher than in those from non-diabetic women. We have measured IGF-I concentrations in cord blood and amniotic fluid for normal and diabetic pregnancies. The purpose of the study was to determine whether there is evidence for a difference in IGF-I concentrations due to diabetes per se. Amniotic fluid and serum from cord blood were obtained at parturition. Determination of IGF-I concentration was by sensitive and specific radioimmunoaseay of the samples following acid dissociation of the hormone from the carrier protein. Cord serum IGF-I concentration from the diabetic pregnancies correlated with birth weight (p<O.05). No difference in cord serum IGF-I concentrations between the diabetic patients and controls matched for age, gestation and birth weight was detected. Amniotic fluid IGF-I concentrations showed no correlation with birth weight or gestation in either the diabetic or control groups. Amniotic fluid IGF-I concentrations, however, were significantly higher in diabetic than non-diabetic pregnancies: mean 17.96 (range 2.3-99) nmol/1 vs 4.42 (range (2-28) nmol/l p<O.O02, 2 tailed Mann-Whitney test. We conclude that cord serum IGF-I concentration in positively correlated with birth weight but does not differ between diabetic and non-diabetic pregnancies. In contrast, amniotic fluid IGF-I concentrations are higher in diabetic pregnancies than in controls. The significance of this observation is not known but implies a difference between diabetic and non-diabetic pregnancies with respect to IGF-I metabolism by the foetal-placental unit.
S101
POS-O01-050 RELEASE OF INSULIN-LIKE GROWTH FACTOE-II BY HUMAN FETAL PANCIt~S IN CULTURE.
J.M. BRYSON, B.E. TUCH, and R.C. BAXTER. Dept. of Medicine, University of Sydney and Dept. of Endocrinology, Royal Prince Alfred Hospital, Sydney, Australia.
Insulin-like Growth Factor II (IGF-II) is a growth promoting peptide thought to play a role in fetal development. We have investigated the role of IGF-II in the development of the human fetal pancreas by measuring IGF-II release during long term organ culture and relating IGF-II release to insulin release.
Human fetal pancreata (14-20 week gestational age) were obtaine~ from the therapeutic termination of pregnancy. Pancreata were diced into 1 mm- explants and cultured for 21 days with medium changed 3 times per week. Culture medium was assayed for insulin and IGF-II. IGF-II levels were measured by a sensitive radioreceptor assay developed using rat liver microsomal membranes.
IGF-II was released by the explants into the culture medium at a daily rate of 0.2-1.0 ng IGF-II/mg tissue. There was a significant increase in the daily IGF-II release (mean ~ S.D.) with gestational age, 14 weeks:0.288 ~ 0.261 ng/mg tissue (n-3), 16-17 weeks: 0.606 ~ 0.218 (n=ll), 19-20 weeks: 0.820 ~ 0.167 (n=4), (14 vs. 16-17:p-.05,14 vs 19--20:p-.021). There was a significant correlation between insulin and IGF-II release, rs0.729, p<.001, n=18.
IGF-II release was also measured after chronic exposure to 1.3uM phorbol 12-myristate 13-acetate, which causes inhibition of insulin secretion. IGF-II levels dropped significantly after 1 week in culture with the total IGF-II production/mg tissue from days 6-21 being reduced from 8.81 ~ 6.39 ng(n=6) to 1.33 ~ 0.62 ng (n=6). The correlation between insulin and IGF-II release remained significant, rs.950, p<.001, n=12.
These studies show that human fetal pancreas releases IGF-II during culture in a pattern similar to insulin release, possibly involving protein kinase C, and suggest a possible autocrine role for IGF-II in human fetal pancreas.
POS-O01-051 GROWTH HORMONE AND SOMATOMEDIN ~N DIABETIC CHILDREN WITH CROWTH FAILURE
H.ALI ASKARI,Institute pf Endocrinology and Metabolism,Tehran, Iran
To investigate the mechanism of the poor linear growth in the dibetic children , five children aged 7 to 12 years, with growth failure, and the type I diabetes of at least four years duration were studied . The heights were 3 to 9 centimeters below the third percentile of the normals , and the history indicated the slowing of the growth velocity following the appearnace of the metabolic disorder . The bone ages compared to the chronological ages showed 1/2 to 2 years delay . The basal growth hormone and its response to arginine infusion was within normal limits in all the five . The plasma somatomedin-C concentration (RIA) ranged from 0.i to 0.5 U/ml. which were either below or at the lower side of the normal range for the age and sex matched controls . In the six to twelve months following the control of the disease and the near normalization of the blood sugar all showed catch up growth and the plasma somatomedin level showed 65 to 700 percent increase. We conclude thah the poor growth in the children with IDDM could be due to the poor somatomedin generation .