Growth in Inuit children exposed to polychlorinated biphenyls and lead during fetal development and childhood Renée Dallaire a , Éric Dewailly b , Pierre Ayotte b , Nadine Forget-Dubois a , Sandra W. Jacobson c , Joseph L. Jacobson c , Gina Muckle a,n a École de psychologie, Université Laval and Centre de recherche du CHU de Québec, Québec City, QC, Canada b Département de médecine sociale et préventive, Université Laval and Centre de recherche du CHU de Québec, Québec City, QC, Canada c Department of Psychiatry and Behavioral Neurosciences, Wayne State University School of Medicine, Detroit, MI, USA article info Article history: Received 17 December 2013 Received in revised form 20 June 2014 Accepted 23 June 2014 Keywords: Fetal growth Child growth Polychlorinated biphenyls Lead Inuit abstract Background: Because of their geographical location and traditional lifestyle, Canadian Inuit children are highly exposed to polychlorinated biphenyls (PCBs) and lead (Pb), environmental contaminants that are thought to affect fetal and child growth. We examined the associations of these exposures with the fetal and postnatal growth of Inuit children. Methods: We conducted a prospective cohort study among Inuit from Nunavik (Arctic Québec). Mothers were recruited at their first prenatal visit; children (n ¼290) were evaluated at birth and at 8–14 years of age. Concentrations of PCB 153 and Pb were determined in umbilical cord and child blood. Weight, height and head circumference were measured at birth and during childhood. Results: Cord blood PCB 153 concentrations were not associated with anthropometric measurements at birth or school age, but child blood PCB 153 concentrations were associated with reduced weight, height and head circumference during childhood. There was no association between cord Pb levels and anthropometric outcomes at birth, but cord blood Pb was related to smaller height and shows a tendency of a smaller head circumference during childhood. Interpretation: Our results suggest that chronic exposure to PCBs during childhood is negatively associated with skeletal growth and weight, while prenatal Pb exposure is related to reduced growth during childhood. This study is the first to link prenatal Pb exposure to poorer growth in school-age children. & 2014 Elsevier Inc. All rights reserved. 1. Introduction Several environmental contaminants have been suspected of having effects on the growth of fetuses and children. Polychlori- nated biphenyls (PCBs) are a group of persistent, lipophilic con- taminants that were used as heat transfer fluids in transformers until 1970s. They are still detected in children's blood at low levels and have been identified as endocrine disruptors that could interfere with fetal and postnatal development (Cocchi et al., 2009, Casals-Casas and Desvergne, 2011). Children are particularly vulnerable to these contaminants due to their physiological immaturity and the transplacental transfer that occurs during the fetal period (Grandjean, 2008). Whereas the effects of prenatal PCB exposure on fetal growth remain controversial (Govarts et al., 2010, El Majidi et al., 2013), no previous study has investigated the relations of pre- and post-natal PCB exposure to the growth of school-age children. Lead (Pb) intoxication in children has been related to stunted growth in previous studies (Schwartz et al., 1986, Ballew et al., (1999)). Although Pb concentrations in the environment have been steadily decreasing since the ban of Pb-based paints and leaded fuel (Levin et al., 2008), children are still exposed to that Pb, particularly in families with low socioeconomic status (Liu et al., 2012) and in developing countries (Falk, 2003). Because Pb is stored in bone, the fetal period is a sensitive window of exposure due to maternal resorption from bone during pregnancy (Tellez- Rojo et al., 2004). Few studies have investigated the effects of low level postnatal Pb exposure on child growth (Frisancho and Ryan, 1991, Kim et al., 1995, Ignasiak et al., 2006), and only one study has evaluated the relation of postnatal growth to in utero exposure (Gardner et al., 2013). Inuit children in Nunavik are more exposed to PCBs than their southern Quebec counterparts due to their geographical location Contents lists available at ScienceDirect journal homepage: www.elsevier.com/locate/envres Environmental Research http://dx.doi.org/10.1016/j.envres.2014.06.023 0013-9351/& 2014 Elsevier Inc. All rights reserved. Abbreviations: BMI, body mass index; DHA, docosahexaenoic acid; FIML, full information maximum likelihood; n-3 PUFAs, n-3 polyunsaturated fatty acids; Pb, lead; PCBs, polychlorinated biphenyls; SES, socioeconomic status n Correspondence to: Centre de recherche du CHU de Québec, 2875 Boul. Laurier, Bureau 600, Québec (QC), Canada, G1V 2M2. Fax: þ1 418 654-2726. E-mail address: [email protected](G. Muckle). Environmental Research 134 (2014) 17–23
Transcript
Growth in Inuit children exposed to polychlorinated biphenyls andlead during fetal development and childhood
Renée Dallaire a, Éric Dewailly b, Pierre Ayotte b, Nadine Forget-Dubois a,Sandra W. Jacobson c, Joseph L. Jacobson c, Gina Muckle a,n
a École de psychologie, Université Laval and Centre de recherche du CHU de Québec, Québec City, QC, Canadab Département de médecine sociale et préventive, Université Laval and Centre de recherche du CHU de Québec, Québec City, QC, Canadac Department of Psychiatry and Behavioral Neurosciences, Wayne State University School of Medicine, Detroit, MI, USA
a r t i c l e i n f o
Article history:Received 17 December 2013Received in revised form20 June 2014Accepted 23 June 2014
Background: Because of their geographical location and traditional lifestyle, Canadian Inuit children arehighly exposed to polychlorinated biphenyls (PCBs) and lead (Pb), environmental contaminants that arethought to affect fetal and child growth. We examined the associations of these exposures with the fetaland postnatal growth of Inuit children.Methods: We conducted a prospective cohort study among Inuit from Nunavik (Arctic Québec). Motherswere recruited at their first prenatal visit; children (n¼290) were evaluated at birth and at 8–14 years ofage. Concentrations of PCB 153 and Pb were determined in umbilical cord and child blood. Weight, heightand head circumference were measured at birth and during childhood.Results: Cord blood PCB 153 concentrations were not associated with anthropometric measurements atbirth or school age, but child blood PCB 153 concentrations were associated with reduced weight, heightand head circumference during childhood. There was no association between cord Pb levels andanthropometric outcomes at birth, but cord blood Pb was related to smaller height and shows a tendencyof a smaller head circumference during childhood.Interpretation: Our results suggest that chronic exposure to PCBs during childhood is negativelyassociated with skeletal growth and weight, while prenatal Pb exposure is related to reduced growthduring childhood. This study is the first to link prenatal Pb exposure to poorer growth in school-agechildren.
& 2014 Elsevier Inc. All rights reserved.
1. Introduction
Several environmental contaminants have been suspected ofhaving effects on the growth of fetuses and children. Polychlori-nated biphenyls (PCBs) are a group of persistent, lipophilic con-taminants that were used as heat transfer fluids in transformersuntil 1970s. They are still detected in children's blood at low levelsand have been identified as endocrine disruptors that couldinterfere with fetal and postnatal development (Cocchi et al.,2009, Casals-Casas and Desvergne, 2011). Children are particularlyvulnerable to these contaminants due to their physiologicalimmaturity and the transplacental transfer that occurs duringthe fetal period (Grandjean, 2008). Whereas the effects of prenatal
PCB exposure on fetal growth remain controversial (Govarts et al.,2010, El Majidi et al., 2013), no previous study has investigated therelations of pre- and post-natal PCB exposure to the growth ofschool-age children.
Lead (Pb) intoxication in children has been related to stuntedgrowth in previous studies (Schwartz et al., 1986, Ballew et al.,(1999)). Although Pb concentrations in the environment have beensteadily decreasing since the ban of Pb-based paints and leadedfuel (Levin et al., 2008), children are still exposed to that Pb,particularly in families with low socioeconomic status (Liu et al.,2012) and in developing countries (Falk, 2003). Because Pb isstored in bone, the fetal period is a sensitive window of exposuredue to maternal resorption from bone during pregnancy (Tellez-Rojo et al., 2004). Few studies have investigated the effects of lowlevel postnatal Pb exposure on child growth (Frisancho and Ryan,1991, Kim et al., 1995, Ignasiak et al., 2006), and only one study hasevaluated the relation of postnatal growth to in utero exposure(Gardner et al., 2013).
Inuit children in Nunavik are more exposed to PCBs than theirsouthern Quebec counterparts due to their geographical location
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/envres
Environmental Research
http://dx.doi.org/10.1016/j.envres.2014.06.0230013-9351/& 2014 Elsevier Inc. All rights reserved.
Abbreviations: BMI, body mass index; DHA, docosahexaenoic acid; FIML, fullinformation maximum likelihood; n-3 PUFAs, n-3 polyunsaturated fatty acids;Pb, lead; PCBs, polychlorinated biphenyls; SES, socioeconomic status
n Correspondence to: Centre de recherche du CHU de Québec, 2875 Boul. Laurier,Bureau 600, Québec (QC), Canada, G1V 2M2. Fax: þ1 418 654-2726.
and consumption of traditional native foods, especially marinemammal fat. Although the Stockholm Convention has banned PCBproduction and uses internationally since 2001, their persistenceand biomagnification through the Arctic marine food chain con-tinue to result in chronic dietary exposure in Inuit children(Muckle et al., 2001a, 2001b). Pb is also a contaminant of concernin this population, with the main source of exposure being the useof lead shots for hunting (Couture et al., 2012). Frequent con-sumption of marine mammals, fish and migratory birds duringinfancy and childhood is, therefore, an important source ofpostnatal exposure to these contaminants among the Inuit. Anextended duration of breastfeeding is also a significant source ofexposure to PCBs. Several health and neurobehavioral effects ofpre- and postnatal PCB and Pb exposure have already beenreported among Inuit children (Dallaire et al., 2006, Boucher etal., 2009, Boucher et al., 2012, Ethier et al., 2012). The aim of thisstudy was to evaluate the associations of pre- and postnatal PCBand Pb blood concentrations with fetal and child growth in arelatively highly exposed population.
2. Methods
2.1. Study population
Participants were 290 Inuit children residing in 14 Inuit communities of Nunavik, aregion located north of the 55th parallel, in Arctic Québec. Most participants (n¼233)were initially recruited (1993–1998) as part of a study aimed at monitoring prenatalexposure to environmental contaminants present in the marine food web (Dewailly etal., 1993). The remaining children (n¼57) were recruited (1996–2000) from the threelargest communities of the Hudson Bay coast (Puvirnituq, Inukjuak and Kuujjuarapik)as part of a study undertaken to document the effects of prenatal exposure toenvironmental contaminants on infant development (Muckle et al., 2001a, 2001b,Jacobson et al., 2008). All children were seen at birth. The combined number ofparticipants recruited for the two initial studies was 548. All families came from thesame geographical area and should be considered as coming from one populationalthough three of the largest communities were overrepresented.
Between September 2005 and February 2010, children's caregivers werecontacted by telephone, provided with information about the study protocol, andinvited to participate with their school-age children in a follow-up study. Inclusioncriteria were age between 8.5 and 14.5 years, birth weightZ2.5 kg, gestationdurationZ35 weeks, no major birth defects, neurological or chronic healthproblems affecting growth (hepatic chronic disease and asthma) and cord bloodsample collected at birth (N¼461). Participation rate was 63%. Main reasons for lossto follow-up were; children moved to another village or outside Nunavik, refusal toparticipate and inability to recontact participants. The principal caregivers (thebiological mother in 67.6% of cases) were interviewed to provide information onsociodemographic background, food insecurity, obstetrical and child medicalhistory, as well as maternal lifestyle habits, including smoking, alcohol, and druguse during pregnancy. Written informed consent was obtained from the parent ofeach participant; oral assent was obtained from each child. The study was endorsedby community stakeholders and public health authorities, approved by LavalUniversity and Wayne State University ethics committees, and conducted inaccordance with the ethical standards of 1983 Declaration of Helsinki.
2.2. Anthropometric parameters
Weight, height and head circumference were measured at birth and duringchildhood by midwives and our research nurses, respectively. Midwives and nurseswere trained to use standard measurement procedures. Newborn and child weightswere determined using a digital balance, while head circumference was measuredwith a measuring tape. Length at birth and height during childhood were measuredwith an infantometer and a stadiometer, respectively. Two measurements wereperformed for each parameter, and a third was obtained in case of a discrepan-cy45 g between the two measurements for birth weight,4500 g for weightduring childhood,40.3 cm for length and head circumference at birth, and40.5 cm for both parameters in childhood. The final value of a given growthparameter was based on the average of the two closest measurements. In addition,the body mass index (BMI) was calculated using the formula BMI¼weight(kg)/height (m)2.
2.3. Biomarkers of exposure to environmental contaminants
A blood sample (30 mL) obtained from the umbilical cord was used todetermine prenatal exposure to PCBs and toxic metals (Pb and Hg), whereas avenous blood sample (20 mL) collected from each child was used to documentexposure to these contaminants at the time of testing. In cord blood samples, totalHg concentrations were determined using cold vapor atomic absorption spectro-metry (Pharmacia Model 120; Pharmacia, Piscataway, NJ). Pb levels were deter-mined by graphite furnace atomic absorption spectroscopy, using the Zeeman-effect background correction (PerkinElmer model ZL 4100; PerkinElmer, Norwalk,CT). Total Hg and Pb concentrations in children blood samples were determined byinductively coupled plasma mass spectrometry (ICP-MS) using a Perkin-Elmer SciexElan 6000 and a PE DRC II instruments for Pb and Hg determination, respectively.We verified that tubes used for blood collection and storing of samples were free ofanalytically significant lead contamination.
The 14 most prevalent PCB congeners (International Union of Pure and AppliedChemistry numbers 28, 52, 99, 101, 105, 118, 128, 138, 153, 156, 170, 180, 183 and187) were measured in purified cord and child plasma extracts using gaschromatography/mass spectrometry. The system used for the latter was an Agilent6890 Network gas chromatograph (Wilmington, DE) equipped with an Agilent7683 series automatic injector and an Agilent 5973 Network mass spectrometer.The gas chromatograph was fitted with an Agilent 60 m DB-XLB column (0.25 mmi.d, 0.25 μm film thickness). The carrier gas was helium and the injection volumeswere 3 mL in splitless mode for the first fraction and 2 mL in splitless mode for thesecond fraction. The mass spectrometer was operated in selected ion monitoringmode, using negative chemical ionization with CH4 (99.97%) as reagent gas. Limitsof detection (LOD) in cord samples were 0.2 mg/L for Hg and Pb, and 0.02 mg/L forPCB congeners. LOD for children samples were 0.1 mg/L for Hg, 0.002 mg/dL for Pband o0.05 mg/L for all PCB congeners except PCB 52 (0.15 mg/L). These analyseswere performed at the Laboratoire de Toxicologie, Institut National de Santé Publiquedu Québec (Québec, QC, Canada).
Plasma PCB 153 concentration, expressed on a lipid basis, was selected as asingle marker for exposure to the mixture of PCBs found in the Arctic environment,because it is the prevailing PCB congener and is highly correlated with the othercongeners (Muckle et al., 2001a, 2001b).
2.4. Other laboratory analyses
Cholesterol, triglycerides, phospholipids and n-3 polyunsaturated fatty acids(n-3 PUFAs) were determined in cord plasma samples. In addition, hemoglobin,ferritin, and vitamins A and D were quantified in child plasma samples. Analyticalprocedures are provided in Supplemental Material.
2.5. Control variables
The following potential confounding variables were documented: (1) childcharacteristics: sex, duration of gestation, duration of breastfeeding, age of child attesting, as well as Hg, vitamin and hemoglobin concentrations in child blood;(2) characteristics of biological mothers: pre-pregnancy maternal weight (kg),height (cm), age at delivery, parity; (3) maternal characteristics at child follow-up:education (years), marital status (single vs. married/living with partner), socio-economic status (SES) (Hollingshead, 1975) (the score includes the occupationalstatus of the principal caregiver and, when relevant, the secondary caregiver whowas either the child's biological father or mother's partner in 77.3% of cases), andfood insecurity of the family (yes/no, refers to having experienced at least 1 daywithout food during the month prior to the interview); (4) cord plasma levels ofthe omega-3 fatty acid docosahexaenoic acid (DHA); and (5) other prenatalexposures: cord Hg, maternal smoking (yes/no), alcohol use (yes/no), and illicitdrug use (yes/no). Prenatal exposure to tobacco, alcohol and illicit drugs as well asbreastfeeding durationwere retrospectively documented at 11 years of age for mostparticipants (n¼233) and through prenatal interview (for substance use) and 1-month postnatal interviews (for substance use and breastfeeding) for the remain-ing mothers.
2.6. Statistical analysis
Preliminary multiple regression analysis at each testing time allowed for theidentification of relevant confounders for each anthropometric parameter sepa-rately at birth and at 11 years. Covariates were initially retained as potentialconfounders if they were correlated with outcomes with pr0.20. All covariateswere found to be associated with outcomes at p valuer0.20 were first includedtogether in multiple regression models to assess their confounding influence andthen removed using a backward procedure, starting with the least significantassociation with the outcome. Covariates modifying the β associated with a givencontaminant by at least 10% were retained in the final models. Sex and age of childat follow-up as well as food insecurity were included in all models (see the figures'notes for a complete list of the covariates retained for each outcome). Interaction
R. Dallaire et al. / Environmental Research 134 (2014) 17–2318
terms between PCB 153 and Pb, as well as with gender and breastfeeding statuswere tested in full models. All the interaction terms were not significant.
Contaminant concentrations, weight, BMI, and head circumference at 11-yearas well as duration of breastfeeding were all log-transformed to improve normalityof distributions. Path analyses were conducted to model the longitudinal relationsbetween exposure variables and growth outcomes in newborns and in children.This method simultaneously estimates all the regression and correlation coeffi-cients specified in models with more than one dependent variable.
Path models were estimated using the Mplus 5.21 software. Missing data weretaken into account with the full information maximum likelihood (FIML) estimator,which represents a state-of-the-art method for estimating models with missingdata (Graham, 2009). The FIML estimator fits the model tested with all dataavailable for each participant so that any participant with at least one valid datapoint is retained for analyses. In our sample, the proportion of missing data rangedfrom 0% to 25% (see Table 1). A 2-tailed p-valueo0.05 was considered statisticallysignificant. The coefficients reported in the figures are standardized regressioncoefficients (unstandardized estimates are available from the authors).
3. Results
Descriptive statistics are presented in Table 1. Most women wereyoung at delivery, low in socioeconomic status, and cigarettesmokers; half had consumed alcohol at least once during pregnancy.Six percent of the children were born before 37 weeks of gestation.The mean age of children at follow-up was 11 years. At follow-up, thesocioeconomic status of the mother continued to be low, and foodinsecurity was reported by almost 40% of interviewed women. Levelsof contaminants were higher at birth than during childhood. A
comparison of the children participating in the 11-year follow-upwith the children who did not on anthropometrics, exposure andsocioeconomic characteristics showed few differences. The childrenwho participated in the follow-up showed slightly longer length atbirth (average difference¼0.48 cm, p¼0.02), slightly lower pre-pregnancy maternal weight (average difference¼2.23 kg, p¼0.02),and were more exposed to mercury prenatally (average difference(geometric means)¼2.33 ug/L, po0.001).
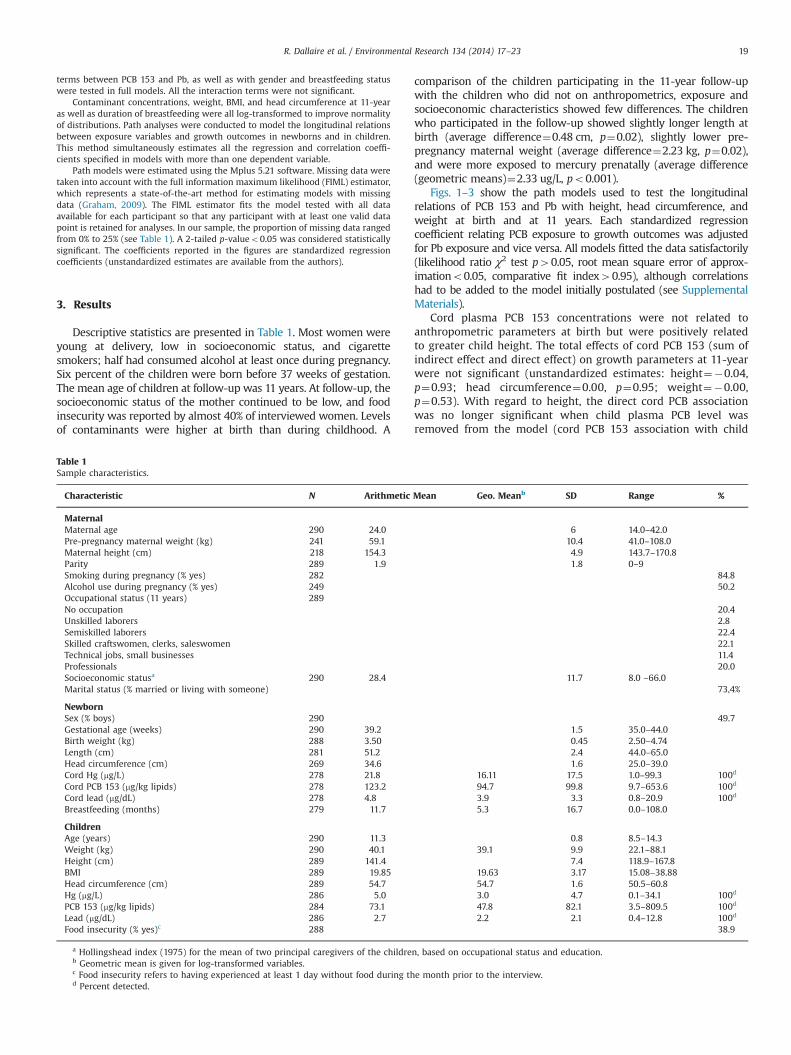
Figs. 1–3 show the path models used to test the longitudinalrelations of PCB 153 and Pb with height, head circumference, andweight at birth and at 11 years. Each standardized regressioncoefficient relating PCB exposure to growth outcomes was adjustedfor Pb exposure and vice versa. All models fitted the data satisfactorily(likelihood ratio χ2 test p40.05, root mean square error of approx-imationo0.05, comparative fit index40.95), although correlationshad to be added to the model initially postulated (see SupplementalMaterials).
Cord plasma PCB 153 concentrations were not related toanthropometric parameters at birth but were positively relatedto greater child height. The total effects of cord PCB 153 (sum ofindirect effect and direct effect) on growth parameters at 11-yearwere not significant (unstandardized estimates: height¼�0.04,p¼0.93; head circumference¼0.00, p¼0.95; weight¼�0.00,p¼0.53). With regard to height, the direct cord PCB associationwas no longer significant when child plasma PCB level wasremoved from the model (cord PCB 153 association with child
Table 1Sample characteristics.
Characteristic N Arithmetic Mean Geo. Meanb SD Range %
MaternalMaternal age 290 24.0 6 14.0–42.0Pre-pregnancy maternal weight (kg) 241 59.1 10.4 41.0–108.0Maternal height (cm) 218 154.3 4.9 143.7–170.8Parity 289 1.9 1.8 0–9Smoking during pregnancy (% yes) 282 84.8Alcohol use during pregnancy (% yes) 249 50.2Occupational status (11 years) 289No occupation 20.4Unskilled laborers 2.8Semiskilled laborers 22.4Skilled craftswomen, clerks, saleswomen 22.1Technical jobs, small businesses 11.4Professionals 20.0Socioeconomic statusa 290 28.4 11.7 8.0 –66.0Marital status (% married or living with someone) 73,4%
a Hollingshead index (1975) for the mean of two principal caregivers of the children, based on occupational status and education.b Geometric mean is given for log-transformed variables.c Food insecurity refers to having experienced at least 1 day without food during the month prior to the interview.d Percent detected.
R. Dallaire et al. / Environmental Research 134 (2014) 17–23 19
height, β¼�0.007, p¼0.88), indicating that this association waslikely due to collinearity between cord and child PCB 153 con-centrations (β¼0.40, po0.001). Child blood PCB 153 concentra-tions were related to reduced child height, head circumference
and weight, even after controlling the cord PCB 153. The pathmodel for body mass index (BMI) (β¼�0.33, po0.001) was notpresented as the association was similar to those observed withweight and height (see Supplemental Materials, Table S.1).
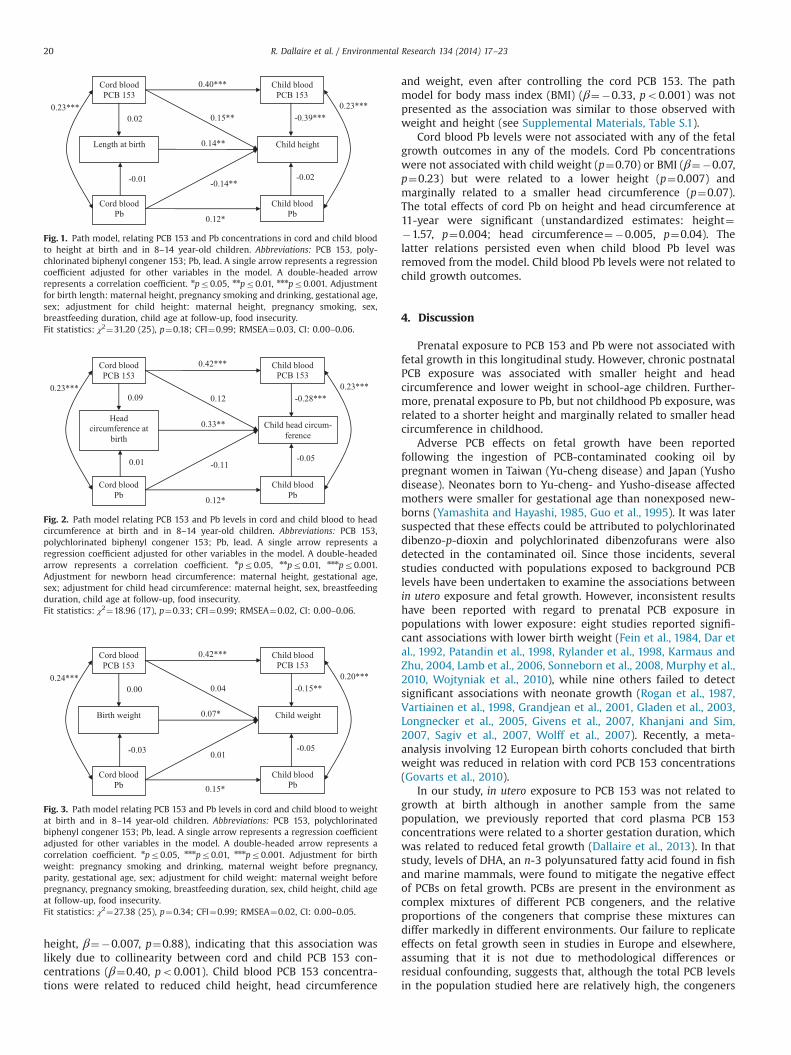
Cord blood Pb levels were not associated with any of the fetalgrowth outcomes in any of the models. Cord Pb concentrationswere not associated with child weight (p¼0.70) or BMI (β¼�0.07,p¼0.23) but were related to a lower height (p¼0.007) andmarginally related to a smaller head circumference (p¼0.07).The total effects of cord Pb on height and head circumference at11-year were significant (unstandardized estimates: height¼�1.57, p¼0.004; head circumference¼�0.005, p¼0.04). Thelatter relations persisted even when child blood Pb level wasremoved from the model. Child blood Pb levels were not related tochild growth outcomes.
4. Discussion
Prenatal exposure to PCB 153 and Pb were not associated withfetal growth in this longitudinal study. However, chronic postnatalPCB exposure was associated with smaller height and headcircumference and lower weight in school-age children. Further-more, prenatal exposure to Pb, but not childhood Pb exposure, wasrelated to a shorter height and marginally related to smaller headcircumference in childhood.
Adverse PCB effects on fetal growth have been reportedfollowing the ingestion of PCB-contaminated cooking oil bypregnant women in Taiwan (Yu-cheng disease) and Japan (Yushodisease). Neonates born to Yu-cheng- and Yusho-disease affectedmothers were smaller for gestational age than nonexposed new-borns (Yamashita and Hayashi, 1985, Guo et al., 1995). It was latersuspected that these effects could be attributed to polychlorinateddibenzo-p-dioxin and polychlorinated dibenzofurans were alsodetected in the contaminated oil. Since those incidents, severalstudies conducted with populations exposed to background PCBlevels have been undertaken to examine the associations betweenin utero exposure and fetal growth. However, inconsistent resultshave been reported with regard to prenatal PCB exposure inpopulations with lower exposure: eight studies reported signifi-cant associations with lower birth weight (Fein et al., 1984, Dar etal., 1992, Patandin et al., 1998, Rylander et al., 1998, Karmaus andZhu, 2004, Lamb et al., 2006, Sonneborn et al., 2008, Murphy et al.,2010, Wojtyniak et al., 2010), while nine others failed to detectsignificant associations with neonate growth (Rogan et al., 1987,Vartiainen et al., 1998, Grandjean et al., 2001, Gladen et al., 2003,Longnecker et al., 2005, Givens et al., 2007, Khanjani and Sim,2007, Sagiv et al., 2007, Wolff et al., 2007). Recently, a meta-analysis involving 12 European birth cohorts concluded that birthweight was reduced in relation with cord PCB 153 concentrations(Govarts et al., 2010).
In our study, in utero exposure to PCB 153 was not related togrowth at birth although in another sample from the samepopulation, we previously reported that cord plasma PCB 153concentrations were related to a shorter gestation duration, whichwas related to reduced fetal growth (Dallaire et al., 2013). In thatstudy, levels of DHA, an n-3 polyunsatured fatty acid found in fishand marine mammals, were found to mitigate the negative effectof PCBs on fetal growth. PCBs are present in the environment ascomplex mixtures of different PCB congeners, and the relativeproportions of the congeners that comprise these mixtures candiffer markedly in different environments. Our failure to replicateeffects on fetal growth seen in studies in Europe and elsewhere,assuming that it is not due to methodological differences orresidual confounding, suggests that, although the total PCB levelsin the population studied here are relatively high, the congeners
Cord blood PCB 153
Length at birth
Cord blood Pb
Child blood PCB 153
Child blood Pb
Child height
0.02
-0.01
0.40***
0.15**
0.14**
-0.14**
0.12*
-0.39***
-0.02
0.23*** 0.23***
Fig. 1. Path model, relating PCB 153 and Pb concentrations in cord and child bloodto height at birth and in 8–14 year-old children. Abbreviations: PCB 153, poly-chlorinated biphenyl congener 153; Pb, lead. A single arrow represents a regressioncoefficient adjusted for other variables in the model. A double-headed arrowrepresents a correlation coefficient. npr0.05, nnpr0.01, nnnpr0.001. Adjustmentfor birth length: maternal height, pregnancy smoking and drinking, gestational age,sex; adjustment for child height: maternal height, pregnancy smoking, sex,breastfeeding duration, child age at follow-up, food insecurity.Fit statistics: χ2¼31.20 (25), p¼0.18; CFI¼0.99; RMSEA¼0.03, CI: 0.00–0.06.
Cord blood PCB 153
Head circumference at
birth
Cord blood Pb
Child blood PCB 153
Child blood Pb
Child head circum-ference
0.09
0.01
0.42***
0.12
0.33**
-0.11
0.12*
-0.28***
-0.05
0.23*** 0.23***
Fig. 2. Path model relating PCB 153 and Pb levels in cord and child blood to headcircumference at birth and in 8–14 year-old children. Abbreviations: PCB 153,polychlorinated biphenyl congener 153; Pb, lead. A single arrow represents aregression coefficient adjusted for other variables in the model. A double-headedarrow represents a correlation coefficient. npr0.05, nnpr0.01, nnnpr0.001.Adjustment for newborn head circumference: maternal height, gestational age,sex; adjustment for child head circumference: maternal height, sex, breastfeedingduration, child age at follow-up, food insecurity.Fit statistics: χ2¼18.96 (17), p¼0.33; CFI¼0.99; RMSEA¼0.02, CI: 0.00–0.06.
Cord blood PCB 153
Birth weight
Cord blood Pb
Child blood PCB 153
Child blood Pb
Child weight
0.00
-0.03
0.42***
0.04
0.07*
0.01
0.15*
-0.15**
-0.05
0.24*** 0.20***
Fig. 3. Path model relating PCB 153 and Pb levels in cord and child blood to weightat birth and in 8–14 year-old children. Abbreviations: PCB 153, polychlorinatedbiphenyl congener 153; Pb, lead. A single arrow represents a regression coefficientadjusted for other variables in the model. A double-headed arrow represents acorrelation coefficient. npr0.05, nnnpr0.01, nnnpr0.001. Adjustment for birthweight: pregnancy smoking and drinking, maternal weight before pregnancy,parity, gestational age, sex; adjustment for child weight: maternal weight beforepregnancy, pregnancy smoking, breastfeeding duration, sex, child height, child ageat follow-up, food insecurity.Fit statistics: χ2¼27.38 (25), p¼0.34; CFI¼0.99; RMSEA¼0.02, CI: 0.00–0.05.
R. Dallaire et al. / Environmental Research 134 (2014) 17–2320
forming the PCB mixture found in the Arctic might be somewhatless toxic.
In children affected by Yu-cheng disease, growth delay wasobserved at multiple periods during childhood (Rogan et al., 1988,Guo et al., 1994). In low exposure populations, prenatal PCBexposure was associated with greater weight in children in threestudies (Hertz-Picciotto et al., 2005, Verhulst et al., 2009, Valviet al., 2012), with no association observed in one study of toddlers(Mendez et al., 2011). In moderately to highly exposed popula-tions, prenatal PCB exposure has been found to be related to lowerweight during childhood in four studies (Jacobson et al., 1990,Patandin et al., 1998 Lamb et al., 2006), although not in two(Gladen et al., 2000, Jackson et al., 2010). In recent years, somepapers have considered the role of prenatal exposure to contami-nants, including PCBs, in the etiology of obesity (Tang-Peronardet al., 2011), but to the contrary of Tang-Peronard et al. (2014) wedid not observe a positive correlation between prenatal PCB 153exposure and weight during childhood. We also observed no clearassociation of prenatal PCB exposure with skeletal growth, whichis consistent with the lack of association between these variablesreported in four studies (Jacobson et al., 1990, Gladen et al., 2000,Blanck et al., 2002, Jackson et al., 2010). However, prenatal PCBexposure was found to be related to reduced length and headcircumference through 3 months of age among infants (Patandinet al., 1998) and to greater height in 5-year-old girls (Hertz-Picciotto et al., 2005) and 17-year-old male teenagers (Lambet al., 2006).
Few studies have evaluated the relation between childhoodPCB exposure and growth. In our study, we found that blood PCBconcentrations at 11 years of age were associated with lowerweight, shorter height, smaller head circumference, and lowerBMI. Consistent with our findings, a study of 8- to 9-year-old boysin Russia reported a significant decrease in BMI, height, and heightvelocity among the most exposed children (Burns et al., 2011). Asimilar association between PCB exposure and reduced BMI butnot height, was seen in a less exposed population of Flemishadolescents (Dhooge et al., 2010). Thus, the hypothesis that PCBexposure adversely affects skeletal growth and weight duringchildhood has received some empirical support from studies withmoderately to highly exposed cohorts. One possible mechanismthat might account for these associations relates to disruption ofthyroid hormone homeostasis or bone formation by PCBs (Zoeller,2001, Cocchi et al., 2009), given that thyroid hormones areinvolved in fat metabolism and bone growth in humans (Duntas,2002, Combs et al., 2011). Another explanation might be reversecausation related to dilution of PCBs in fat tissue in heavierchildren since PCBs are lipophilic contaminants. Dilution mightcontribute to the PCB-weight association but is not likely toexplain the relation with skeletal growth.
Consistent with our results, Pb concentration in cord ormaternal blood during pregnancy has not been related to anthro-pometric measurements at birth in most studies (Greene andErnhart, 1991, Gonzalez-Cossio et al., 1997, Hernandez-Avila et al.,2002, Gundacker et al., 2010), but not all (Osman et al., 2000, Zhuet al., 2010, Xie et al., 2013). Also, Pb concentration in maternalurine was not related to birth weigth in newborns from Bangla-desh. Some studies have evaluated several biomarkers of Pbexposure in relation to fetal growth. Maternal tibia Pb levelsdetermined at 1 month postpartum, but not cord nor maternalblood concentrations, were associated with a lower birth weight(Gonzalez-Cossio et al., 1997), as well as decreased length andhead circumference at birth (Hernandez-Avila et al. 2002). Giventhese varying findings, it remains unclear whether prenatal Pbexposure is related to poorer fetal growth.
In our study, prenatal Pb exposure was associated with reducedheight and a tendency for smaller head circumference at school
age, whereas no associations were found between child blood Pbconcentration and child growth parameters. These results suggestthat in utero Pb exposure might have more detrimental effects onchild growth than Pb exposure during childhood. Few prospectivestudies have investigated associations between prenatal low-levelPb exposure and postnatal growth, and none have presented dataspanning such an extended time period. Three studies have foundsignificant associations between prenatal Pb exposure and lowergrowth parameters from 6 to 48 months, depending on thevariations in blood Pb levels between the pre- and postnatalperiods, with higher Pb concentrations having more detrimentaleffects (Shukla et al., 1991, Rothenberg et al., 1999, Schell et al.,2009). However, one study failed to report an association betweenpre- and postnatal exposure to Pb and growth outcomes from 0 to4 years of age (Greene and Ernhart, 1991).
Unlike other studies, our data show that Pb concentrations inInuit children are not associated with growth parameters at schoolage. Negative associations have been previously found betweenchild blood Pb concentrations and skeletal growth (Schwartz et al.,1986, Frisancho and Ryan, 1991, Kafourou et al., 1997, Ballew et al.,1999, Ignasiak et al., 2006, Yang et al., 2013) in children withhigher blood Pb concentrations than those observed in oursample. The association with weight was less clear, two studieshaving reported lower weight with increasing Pb concentrations(Schwartz et al., 1986, Ignasiak et al., 2006), whereas anotherfound a positive association between Pb dentin level and BMI (Kimet al., 1995). One possible explanation for the lack of significantnegative associations with growth in our study relates to thetiming of our Pb measurements. Because the peak exposure to Pbin children is around 2-years of age (Brody et al., 1994), we mighthave missed the appropriate postnatal window of exposure toidentify adverse effects on the child growth. Several mechanismshave been proposed to explain how Pb may interfere with skeletalgrowth. Pb has been shown (1) to inhibit the osteoblast-mediatedsecretion of two proteins involved in bone mineralization, namelyosteonectin (Klein and Wiren, 1993) and osteocalcin (Long andRosen, 1992), (2) to interfere with binding of Ca2þ by transportproteins (Sauk and Somerman, 1991), and (3) to affect growthhormone secretion (Berry et al. (2002)).
This study has several strengths. Its longitudinal design allowedus to simultaneously consider prenatal and childhood exposure toubiquitous contaminants on child growth. Furthermore, we wereable to consider the concomitant exposure to contaminants pre-sent in the diet, along with nutrients. Although numerous con-founders were considered in our analyses, substances used duringpregnancy were documented retrospectively for most children,and we controlled for food insecurity of the family rather than thecaloric intake and the physical activity of participating children. Asa result, residual confounding may have affected our estimates forweight models, but this is less likely to have affected the resultsthat were reported with skeletal growth indicators. Other limita-tions are absence of data on father characteristics and Tanner stageof the children as well as a single postnatal Pb measurement. Dueto the long half-lives of several PCB congeners (4 to 10 years)(Grandjean et al., 2008), a unique measurement of postnatal PCBconcentrations was considered adequate.
5. Conclusion
Our study supports findings from two other studies ofmoderately-exposed children indicating that chronic exposure toPCBs during childhood can adversely affect skeletal growth andbody weight. Although the absence of an effect of prenatal PCBexposure on growth suggests that the congener mixture in ArcticQuebec may be less toxic than in other locales, the PCB exposure
R. Dallaire et al. / Environmental Research 134 (2014) 17–23 21
experienced during breast-feeding (Muckle et al., 2001a, 2001b)and childhood in this population presumably accounts for theeffects seen on growth during childhood. In addition, this study isthe first to link prenatal Pb exposure to poorer growth in school-age children, providing additional evidence that there is no safeblood Pb level for pregnant women.
Funding sources
This study was funded by grants from the National Institutesof Environmental Health Sciences/NIH (R01-ES007902 toJ.L. Jacobson); Northern Contaminant Program, Indian and North-ern Affairs Canada (to G. Muckle); and the Joseph Young Sr Fundfrom the State of Michigan (to S.W. Jacobson). R. Dallaire obtaineda postdoctoral fellowship from the Canadian Institutes of HealthResearch.
Ethics
The participation of human subjects did occur after informedconsent was obtained. The research procedures were approved bythe community stakeholders and public health authorities,approved by Laval University and Wayne State University ethicscommittees, and conducted in accordance with the ethical stan-dards of the 1983 Declaration of Helsinki.
Acknowledgments
We are grateful to the Nunavik population and their organiza-tions for their participation in this research. We also thankJocelyne Gagnon, Johanne Varin, Line Roy, Alacie Pov, ChristineBouffard, Karine Poitras, Carole Vézina, Germain Lebel, EdnaLachance, Renee Sun, Brenda Tuttle, Neil Dodge and Richard Poulinfor their committed involvement in this study.
Appendix A. Supporting information
Supplementary data associated with this article can be foundin the online version at http://dx.doi.org/10.1016/j.envres.2014.06.023.
References
Ballew, C., et al., 1999. Blood lead concentration and children's anthropometricdimensions in the Third National Health and Nutrition Examination Survey(NHANES III), 1988-1994. J. Pediatr. 134 (5), 623–630.
Berry Jr., W.D., et al., 2002. Lead attenuation of episodic growth hormone secretionin male rats. Int. J. Toxicol. 21 (2), 93–98.
Blanck, H.M., et al., 2002. Growth in girls exposed in utero and postnatally topolybrominated biphenyls and polychlorinated biphenyls. Epidemiology 13 (2),205–210.
Boucher, O., et al., 2012. Prenatal methylmercury, postnatal lead exposure, andevidence of attention deficit/hyperactivity disorder among Inuit children inArctic Quebec. Environ. Health Perspect. 120 (10), 1456–1461.
Boucher, O., et al., 2009. The relation of lead neurotoxicity to the event-relatedpotential P3b component in Inuit children from arctic Quebec. Neurotoxicology30 (6), 1070–1077.
Brody, D.J., et al., 1994. Blood lead levels in the US population. Phase 1 of the ThirdNational Health and Nutrition Examination Survey (NHANES III, 1988 to 1991).JAMA 272 (4), 277–283.
Burns, J.S., et al., 2011. Serum dioxins and polychlorinated biphenyls are associatedwith growth among Russian boys. Pediatrics 127 (1), e59–e68.
Cocchi, D., et al., 2009. Chronic treatment with polychlorinated biphenyls (PCB)during pregnancy and lactation in the rat: Part 1: Effects on somatic growth,growth hormone-axis activity and bone mass in the offspring. Toxicol. Appl.Pharmacol. 237 (2), 127–136.
Combs, C.E., et al., 2011. Thyroid hormones and bone development. MinervaEndocrinol. 36 (1), 71–85.
Couture, A., et al., 2012. Lead exposure in Nunavik: from research to action. Int. J.Circumpolar Health 71, 18591.
Dallaire, F., et al., 2006. Effect of prenatal exposure to polychlorinated biphenyls onincidence of acute respiratory infections in preschool Inuit children. Environ.Health Perspect. 114 (8), 1301–1305.
Dallaire, R., et al., 2013. Exposure to organochlorines and mercury through fish andmarine mammal consumption: associations with growth and duration ofgestation among Inuit newborns. Environ. Int. 54, 85–91.
Dar, E., et al., 1992. Fish consumption and reproductive outcomes in Green Bay,Wisconsin. Environ. Res. 59 (1), 189–201.
Dewailly, E., et al., 1993. Health status at birth of Inuit newborn prenatally exposedto organochlorines. Chemosphere 27, 359–366.
Dhooge, W., et al., 2010. Internal exposure to pollutants and body size in Flemishadolescents and adults: associations and dose-response relationships. Environ.Int. 36 (4), 330–337.
Duntas, L.H., 2002. Thyroid disease and lipids. Thyroid 12 (4), 287–293.El Majidi, N., et al., 2013. Relationship between prenatal exposure to polychlori-
nated biphenyls and birth weight: a systematic analysis of published epide-miological studies through a standardization of biomonitoring data. Regul.Toxicol. Pharmacol. 64 (1), 161–176.
Ethier, A.A., et al., 2012. Effects of environmental contaminant exposure on visualbrain development: a prospective electrophysiological study in school-agedchildren. Neurotoxicology 33 (5), 1075–1085.
Falk, H., 2003. International environmental health for the pediatrician: case studyof lead poisoning. Pediatrics 112 (1 Pt 2), 259–264.
Fein, G.G., et al., 1984. Prenatal exposure to polychlorinated biphenyls: effects onbirth size and gestational age. J. Pediatr. 105 (2), 315–320.
Frisancho, A.R., Ryan, A.S., 1991. Decreased stature associated with moderate bloodlead concentrations in Mexican-American children. Am. J. Clin. Nutr. 54 (3),516–519.
Gardner, R.M., et al., 2013. Environmental exposure to metals and children's growthto age 5 years: a prospective cohort study. Am. J. Epidemiol. 177 (12),1356–1367.
Givens, M.L., et al., 2007. Maternal exposure to polybrominated and polychlori-nated biphenyls: infant birth weight and gestational age. Chemosphere 69 (8),1295–1304.
Gladen, B.C., et al., 2000. Pubertal growth and development and prenatal andlactational exposure to polychlorinated biphenyls and dichlorodiphenyldichloroethene. J. Pediatr. 136 (4), 490–496.
Gladen, B.C., et al., 2003. Persistent organochlorine compounds and birth weight.Ann. Epidemiol. 13 (3), 151–157.
Gonzalez-Cossio, T., et al., 1997. Decrease in birth weight in relation to maternalbone-lead burden. Pediatrics 100 (5), 856–862.
Govarts, E., et al., 2010. Birth weight and prenatal exposure to Polychlorinated Biphenyls(PCBs) and Dichlorodiphenyldichloroethylene (DDE): a meta-analysis within 12European birth cohorts. Environ. Health Perspect. 120 (2), 162–170.
Graham, J.W., 2009. Missing data analysis: making it work in the real world. Annu.Rev. Psychol. 60, 549–576.
Grandjean, P., 2008. Late insights into early origins of disease. Basic Clin. Pharmacol.Toxicol. 102 (2), 94–99.
Grandjean, P., et al., 2001. Birthweight in a fishing community: significance ofessential fatty acids and marine food contaminants. Int. J. Epidemiol. 30 (6),1272–1278.
Grandjean, P., et al., 2008. Elimination half-lives of polychlorinated biphenylcongeners in children. Environ. Sci. Technol. 42 (18), 6991–6996.
Greene, T., Ernhart, C.B., 1991. Prenatal and preschool age lead exposure: relation-ship with size. Neurotoxicol. Teratol. 13 (4), 417–427.
Gundacker, C., et al., 2010. Perinatal lead and mercury exposure in Austria. Sci. TotalEnviron. 408 (23), 5744–5749.
Guo, Y.L., et al., 1995. Growth abnormalities in the population exposed in utero andearly postnatally to polychlorinated biphenyls and dibenzofurans. Environ.Health Perspect. 103 (Suppl 6), S117–S122.
Guo, Y.L., et al., 1994. Musculoskeletal changes in children prenatally exposed topolychlorinated biphenyls and related compounds (Yu-Cheng children).J. Toxicol. Environ. Health 41 (1), 83–93.
Hernandez-Avila, M., et al., 2002. Effect of maternal bone lead on length and headcircumference of newborns and 1-month-old infants. Arch. Environ. Health 57(5), 482–488.
Hertz-Picciotto, I., et al., 2005. In utero polychlorinated biphenyl exposuresin relation to fetal and early childhood growth. Epidemiology 16 (5),648–656.
Hollingshead, A.B. (1975). Four factor index of a social status. Unpublished manu-script. Yale University.
Ignasiak, Z., et al., 2006. Lead and growth status of school children living in thecopper basin of south-western Poland: differential effects on bone growth. Ann.Hum. Biol 33 (4), 401–414.
Jackson, L.W., et al., 2010. Prenatal and postnatal exposure to polychlori-nated biphenyls and child size at 24 months of age. Reprod. Toxicol. 29 (1),25–31.
Jacobson, J.L., et al., 1990. Effects of exposure to PCBs and related compounds ongrowth and activity in children. Neurotoxicol. Teratol. 12 (4), 319–326.
Jacobson, J.L., et al., 2008. Beneficial effects of a polyunsaturated fatty acid on infantdevelopment: evidence from the Inuit of Arctic Quebec. J. Pediatr. 152 (3),356–364.
R. Dallaire et al. / Environmental Research 134 (2014) 17–2322
Kafourou, A., et al., 1997. Effects of lead on the somatic growth of children. Arch.Environ. Health 52 (5), 377–383.
Karmaus, W., Zhu, X., 2004. Maternal concentration of polychlorinated biphenylsand dichlorodiphenyl dichlorethylene and birth weight in Michigan fish eaters:a cohort study. Environ. Health 3 (1), 1.
Khanjani, N., Sim, M.R., 2007. Maternal contamination with PCBs and reproductiveoutcomes in an Australian population. J. Expo. Sci. Environ. Epidemiol. 17 (2),191–195.
Kim, R., et al., 1995. A longitudinal-study of chronic lead-exposure and physicalgrowth in Boston children. Environ. Health Perspect. 103 (10), 952–957.
Klein, R.F., Wiren, K.M., 1993. Regulation of osteoblastic gene expression by lead.Endocrinology 132 (6), 2531–2537.
Lamb, M.R., et al., 2006. Prenatal exposure to polychlorinated biphenyls andpostnatal growth: a structural analysis. Environ. Health Perspect. 114 (5),779–785.
Levin, R., et al., 2008. Lead exposures in US Children, 2008: implications forprevention. Environ. Health Perspect. 116 (10), 1285–1293.
Liu, J., et al., 2012. Blood lead levels and associated sociodemographic factorsamong preschool children in the South Eastern region of China. Paediatr.Perinat. Epidemiol. 26 (1), 61–69.
Long, G.J., Rosen, J.F., 1992. Lead perturbs epidermal growth factor (EGF) modula-tion of intracellular calcium metabolism and collagen synthesis in clonal ratosteoblastic (ROS 17/2.8) cells. Toxicol. Appl. Pharmacol. 114 (1), 63–70.
Longnecker, M.P., et al., 2005. Maternal levels of polychlorinated biphenyls inrelation to preterm and small-for-gestational-age birth. Epidemiology 16 (5),641–647.
Mendez, M.A., et al., 2011. Prenatal organochlorine compound exposure, rapidweight gain, and overweight in infancy. Environ. Health Perspect. 119 (2),272–278.
Muckle, G., et al., 2001a. Determinants of polychlorinated biphenyls and methyl-mercury exposure in inuit women of childbearing age. Environ. HealthPerspect. 109 (9), 957–963.
Muckle, G., et al., 2001b. Prenatal exposure of the northern Quebec Inuit infants toenvironmental contaminants. Environ. Health Perspect. 109 (12), 1291–1299.
Murphy, L.E., et al., 2010. Maternal serum preconception polychlorinated biphenylconcentrations and infant birth weight. Environ. Health Perspect. 118 (2),297–302.
Osman, K., et al., 2000. Toxic and essential elements in placentas of Swedishwomen. Clin. Biochem. 33 (2), 131–138.
Patandin, S., et al., 1998. Effects of environmental exposure to polychlorinatedbiphenyls and dioxins on birth size and growth in Dutch children. Pediatr. Res.44 (4), 538–545.
Rogan, W.J., et al., 1988. Congenital poisoning by polychlorinated biphenyls andtheir contaminants in Taiwan. Science 241 (4863), 334–336.
Rogan, W.J., et al., 1987. Polychlorinated biphenyls (PCBs) and dichlorodiphenyldichloroethene (DDE) in human milk: effects on growth, morbidity, andduration of lactation. Am. J. Public Health 77 (10), 1294–1297.
Rothenberg, S.J., et al., 1999. Pre- and postnatal lead effect on head circumference: acase for critical periods. Neurotoxicol. Teratol. 21 (1), 1–11.
Rylander, L., et al., 1998. Polychlorinated biphenyls in blood plasma among Swedishfemale fish consumers in relation to low birth weight. Am. J. Epidemiol. 147 (5),493–502.
Sagiv, S.K., et al., 2007. Organochlorine exposures during pregnancy and infant sizeat birth. Epidemiology 18 (1), 120–129.
Sauk, J.J., Somerman, M.J., 1991. Physiology of bone: mineral compartment proteinsas candidates for environmental perturbation by lead. Environ. Health Perspect.91, 9–16.
Schell, L.M., et al., 2009. Growth of infants' length, weight, head and armcircumferences in relation to low levels of blood lead measured serially. Am.J. Hum. Biol. 21 (2), 180–187.
Schwartz, J., et al., 1986. Relationship between childhood blood lead levels andstature. Pediatrics 77 (3), 281–288.
Shukla, R., et al., 1991. Lead exposure and growth in the early preschool child: afollow-up report from the Cincinnati leadsStudy. Pediatrics 88 (5), 886–892.
Sonneborn, D., et al., 2008. Prenatal polychlorinated biphenyl exposures in easternSlovakia modify effects of social factors on birthweight. Paediatr. Perinat.Epidemiol. 22 (3), 202–213.
Tang-Peronard, J.L., et al., 2011. Endocrine-disrupting chemicals and obesitydevelopment in humans: a review. Obes. Rev. 12 (8), 622–636.
Tang-Peronard, J.L., et al., 2014. Association between prenatal polychlorinatedbiphenyl exposure and obesity development at ages 5 and 7 y; a prospectivecohort study of 656 children from the Faroe Islands. Am. J. Clin. Nutr. 99 (1),5–13.
Tellez-Rojo, M.M., et al., 2004. Impact of bone lead and bone resorption on plasmaand whole blood lead levels during pregnancy. Am. J. Epidemiol. 160 (7),668–678.
Valvi, D., et al., 2012. Prenatal concentrations of polychlorinated biphenyls, DDE,and DDT and overweight in children: a prospective birth cohort study. Environ.Health Perspect. 120 (3), 451–457.
Vartiainen, T., et al., 1998. Birth weight and sex of children and the correlation tothe body burden of PCDDs/PCDFs and PCBs of the mother. Environ. HealthPerspect. 106 (2), 61–66.
Verhulst, S.L., et al., 2009. Intrauterine exposure to environmental pollutants andbody mass index during the first 3 years of life. Environ. Health Perspect. 117(1), 122–126.
Wojtyniak, B.J., et al., 2010. Association of maternal serum concentrations of 2,20 ,4,405,50-hexachlorobiphenyl (CB-153) and 1,1-dichloro-2,2-bis (p-chlorophe-nyl)-ethylene (p,p'-DDE) levels with birth weight, gestational age and pretermbirths in Inuit and European populations. Environ. Health 9, 56.
Wolff, M.S., et al., 2007. Prenatal pesticide and PCB exposures and birth outcomes.Pediatr. Res. 61 (2), 243–250.
Xie, X., et al., 2013. The effects of low-level prenatal lead exposure on birthoutcomes. Environ. Pollut. 175, 30–34.
Yamashita, F., Hayashi, M., 1985. Fetal PCB syndrome: clinical features, intrauterinegrowth retardation and possible alteration in calcium metabolism. Environ.Health Perspect. 59, 41–45.
Yang, H., et al., 2013. Effects of lead and cadmium exposure from electronicwaste on child physical growth. Environ. Sci. Pollut. Res. Int. 20 (7), 4441–4447.
Zhu, M., et al., 2010. Maternal low-level lead exposure and fetal growth. Environ.Health Perspect. 118 (10), 1471–1475.
Zoeller, R.T., 2001. Polychlorinated biphenyls as disruptors of thyroid hormoneaction. In: Fisher, L.J., Hansen, L. (Eds.), Recents Advances in the EnvironmentalToxicology and Health Effects of PCBs. University of Kentucky Press, Lexington,K.Y., pp. 265–272.
R. Dallaire et al. / Environmental Research 134 (2014) 17–23 23