Guidelines for Lowering Lipids to ReduceCoronary Artery Disease Risk:
A Comparison of Rosuvastatin withAtorvastatin, Pravastatin, and
Simvastatin for Achieving Lipid-Lowering Goals
James Shepherd, MB, ChB, PhD, Donald B. Hunninghake, MD, Philip Barter, MD, PhD,James M. McKenney, PharmD, and Howard G. Hutchinson, MD
Both the National Cholesterol Education Program(NCEP) Adult Treatment Panel (ATP) III and the SecondJoint Task Force of European Societies guidelines haveestablished low-density lipoprotein (LDL) cholesterolgoals for lipid-lowering treatment to reduce the risk ofcoronary artery disease. Data from 3 trials that com-pared rosuvastatin 10 mg (n � 389) with atorvastatin10 mg (n � 393) and 2 trials that compared rosuvastatin10 mg (n � 226) with pravastatin 20 mg (n � 252)and simvastatin 20 mg (n � 249) were pooled sepa-rately to compare the achievement of LDL cholesterolgoals over 12 weeks of treatment in hypercholester-olemic patients. Noncomparative pooling of rosuvasta-tin 10 mg results from all 5 trials (n � 615) showed that80% achieved NCEP ATP III goals and 81% achieved theEuropean goal of <3.0 mmol/L. Compared with ator-vastatin 10 mg, significantly more patients treated with
rosuvastatin 10 mg achieved their ATP III (76% vs 53%)and European (82% vs 51%) goals (p <0.001). Also, incomparisons with simvastatin 20 mg and pravastatin 20mg, 86% of patients treated with rosuvastatin 10 mgachieved ATP III goals, compared with 64% of simvas-tatin-treated patients and 49% of pravastatin-treatedpatients (p <0.001). The proportions of patients whoachieved the European goal were 80%, 48%, and 16%for rosuvastatin 10 mg, simvastatin 20 mg, and prava-statin 20 mg, respectively, in this comparison (all p<0.001). A total of 71% of patients treated with rosuva-statin 10 mg who had triglyceride levels >200 mg/dLmet both their LDL cholesterol and their non–high-den-sity lipoprotein cholesterol goals. �2003 by ExcerptaMedica, Inc.
Am J Cardiol 2003;91(suppl):11C–19C
Both the National Cholesterol Education Program(NCEP) Adult Treatment Panel (ATP) III guide-
lines1 and the Second Joint Task Force of EuropeanSocieties guidelines2 emphasize the need to addressglobal risk in individuals at risk for coronary arterydisease (CAD). Dyslipidemia clearly constitutes a ma-jor risk factor for CAD. Risk in individuals withdyslipidemia, however, is modulated by the presenceof additional risk factors. Authors of both sets ofguidelines have struggled with the need to define risks
for the purposes of prevention and treatment decisionsin a manner that both reflects the multifactorial natureof risk and increases the ease of guideline interpreta-tion and implementation. Much remains to be learnedabout risks, and more work is needed to derive guide-lines for CAD prevention that can be easily interpretedand readily implemented in clinical practice.
Much also remains to be done to improve theadoption of and adherence to existing guidelines inclinical practice. Failure to use guidelines appropri-ately may put patients in jeopardy of increasedmorbidity and mortality. Both the ATP III and theEuropean guidelines include lipid-lowering goalsand specify when to initiate lipid-modifying thera-py.1,2 In both sets of guidelines, lowering highlevels of low-density lipoprotein (LDL) cholesterolis recognized as a key target for reducing risk.However, various analyses have shown that therates of achievement of LDL cholesterol–loweringgoals in clinical practice are poor, despite the avail-ability of drug therapy such as 3-hydroxy-3-meth-ylglutaryl coenzyme A reductase inhibitors (statins)that reduce LDL cholesterol and have clearly beenshown to reduce CAD risk.3–5
From the Department of Pathological Biochemistry, Royal Infirmary,University of Glasgow, Glasgow, Scotland (JS); the Departments ofPharmacology and Medicine (Cardiovascular Division), University ofMinnesota, Minneapolis, Minnesota, USA (DBH); the Royal AdelaideHospital, Adelaide, Australia (PB); National Clinical Research, Rich-mond, Virginia, USA (JMM); and AstraZeneca LP, Wilmington, Dela-ware, USA (HGH).
Crestor is a registered trademark of the AstraZeneca group ofcompanies. Research discussed in this article was supported by Astra-Zeneca.
Address for reprints: James Shepherd, MB, ChB, PhD, Departmentof Pathological Biochemistry, University of Glasgow, Royal Infirmary,Castle Street 84 C4, Glasgow G4 0SF, Scotland. E-mail: [email protected].
In the EUROASPIRE II study,3 conducted from1999 to 2000, 5,556 patients from 15 Europeancountries had their status reviewed after hospital-ization for CAD. In 58.3% of patients, total choles-terol levels remained above the therapy initiationthreshold and goal of 5.0 mmol/L. Only 60.8% ofthe patients reported that they were receiving lipid-lowering medication. Among these patients, 50.6%had total cholesterol levels below the goal, whereasamong patients not receiving medication, 27.7%had levels below the goal.
Other studies in high-risk patients have shownsimilar results.4,6,7 Fonarow et al6 assessed datafrom 138,001 patients with acute myocardial infarc-tion (MI) who were discharged from hospitals par-ticipating in the National Registry of MyocardialInfarction–3 in 1998 to 1999. The investigatorsfound that only 31.7% of patients received lipid-lowering medications at hospital discharge. Simi-larly, Sueta et al4 assessed data from 48,586 coro-nary disease patients in an outpatient quality assur-ance program and found that only 39% werereceiving lipid-lowering therapy and only 25%achieved an LDL cholesterol goal of �100 mg/dL.
The Lipid Treatment Assessment Project (L-TAP), conducted in 1996 to 1997, assessed ATP IILDL cholesterol goal achievement rates in dyslipid-emic patients treated in US primary care practicesin the top tertile of frequent prescribers of lipid-lowering medications.5 Overall, 84.6% of these4,888 patients received treatment with lipid-lower-ing drugs, and of those receiving treatment, 39%had reached their LDL cholesterol goal. Amongthose receiving drug therapy, LDL cholesterol goalswere achieved by 68% of patients with a goal of�160 mg/dL, 37% with a goal of �130 mg/dL, and18% with a goal of �100 mg/dL. Most of thepatients who failed to achieve LDL cholesterolgoals had LDL cholesterol levels above the treat-ment initiation thresholds defined in the ATP IIguidelines. The L-TAP investigators observed thathigh doses of lipid-lowering medication were usedinfrequently. They suggested that the failure toachieve treatment goals despite the wide use oflipid-lowering treatment meant that either these pa-tients were receiving inadequate treatment or thedrug treatments themselves were inadequate.
Failure to titrate lipid-lowering medication ade-quately may also play a role in the failure to achievelipid-lowering goals. Drugs that reduce LDL cho-lesterol sufficiently at initial doses may thus be ofconsiderable usefulness in this regard. In recentyears, several studies have assessed the ability ofstatin therapy to help patients achieve guidelineLDL cholesterol goals.8 –10 For example, in theAtorvastatin Comparative Cholesterol Efficacy andSafety Study (ACCESS),10 hypercholesterolemicpatients received 1 of 5 statins (atorvastatin, fluva-statin, lovastatin, pravastatin, or simvastatin) ini-tially at starting doses and subsequently at titrateddoses to enable patients to achieve ATP II LDLcholesterol goals. Treatment with atorvastatin, con-
sidered to be the most effective statin in reducingLDL cholesterol, resulted in the highest rates ofboth goal achievement at the starting dose and goalmaintenance during dose titration. Additionally, al-though titration to higher doses of any statin en-abled more patients to reach LDL cholesterol goals,the percentage reduction in LDL cholesterolachieved with the starting dose was strongly corre-lated with percentage of patients maintaining goallevels at the end of the 54-week study.
It is important to note that although increasedeffectiveness in achieving guideline goals is a valu-able attribute of lipid-lowering medications such asstatins, guideline recommendations should not berigidly or unthinkingly applied without clinicaljudgment. Full knowledge of the patients’ statusand provision of good care must take precedenceover guideline recommendations, and safety is aparamount consideration in the choice of CAD pre-vention strategies.
The ATP III guidelines1 differ from previousguidelines in that more patients are identified asneeding more aggressive LDL cholesterol lowering.In contrast with the ATP II guidelines, the ATP IIIguidelines include patients with diabetes and with-out CAD in the highest risk category and use Fra-mingham scoring of 10-year CAD risk to identifypeople who have �2 risk factors and who should bereceiving more aggressive therapy or be classifiedas high risk. Also, the definition of the major riskfactor of low levels of high-density lipoprotein(HDL) cholesterol was raised from �35 to �40mg/dL. As a result of these changes, it is estimatedthat 36 million people aged 20 to 79 in the USpopulation should be eligible for therapeutic life-style changes plus drug therapy based on ATP IIIguidelines.11 This represents a 140% increase in thenumber of patients eligible for drug therapy overthat based on ATP II guidelines. The lower goal of�100 mg/dL for many patients may make goalattainment even more difficult and emphasizes therequirement for effective LDL cholesterol reductionto achieve treatment goals.
The objective of the pooled analyses reported be-low was to assess achievement of LDL cholesterolgoals, from 2 major sets of guidelines currently in use,by hypercholesterolemic patients treated with rosu-vastatin 10 mg, atorvastatin 10 mg, simvastatin 20 mg,or pravastatin 20 mg.
METHODSThe first 12 weeks of 5 trials were prospectively
designed so that data could be pooled to determinethe effect of starting doses of rosuvastatin calcium(Crestor; licensed to AstraZeneca from Shionogi &Co., Ltd., Osaka, Japan) on lipid parameters inpatients with hypercholesterolemia (LDL choles-terol �160 and �250 mg/dL, triglycerides �400mg/dL). Three of these trials included comparisonsof rosuvastatin 10 mg with atorvastatin 10 mg, and
12C THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 91 (5A) MARCH 6, 2003
2 other trials included comparisons of rosuvastatin10 mg with simvastatin 20 mg and pravastatin 20mg. Details regarding these trials and the lipidresults are reported elsewhere.12,13
For this analysis of the percentages of patientswho achieved NCEP ATP III LDL cholesterolgoals, patients were classified into 3 risk categories,with goals of �100, �130, and �160 mg/dL ac-cording to the NCEP ATP III guidelines.1 Patientswho had CAD, CAD risk equivalents (such asother clinical forms of atherosclerotic disease ordiabetes), or multiple risk factors that conferred a10-year risk of �20% had an LDL cholesterol goalof �100 mg/dL. Those patients who had �2 riskfactors but a 10-year risk of �20% had an LDLcholesterol goal of �130 mg/dL, and those with �2risk factors had an LDL cholesterol goal of �160mg/dL. The European goal is �116 mg/dL (�3.0mmol/L), regardless of risk.2 For the European goalanalysis, patients were automatically identified ashigh risk if they had CAD, diabetes, or a familyhistory of premature CAD or peripheral vasculardisease. Additional patients were identified ashigh risk if they had a CAD risk �20% over 10years or if their risk would exceed 20% if projectedto 60 years of age. Calculations of this risk werebased on charts published by the Second Joint TaskForce of European and other Societies on CoronaryPrevention.2
Overall noncomparative effects of rosuvastatin10 mg on goal achievement after 12 weeks of treat-ment were summarized by using the rosuvastatin 10mg data from all 5 trials. To avoid the potential forselection bias, comparisons between drug treat-ments were made only between groups of patientsrandomized within the same trials. Therefore, thepooled comparisons of rosuvastatin with atorvasta-tin included only the rosuvastatin-treated patientsfrom the 3 trials that included atorvastatin, and thecomparisons of rosuvastatin with simvastatin andpravastatin included only the rosuvastatin-treatedpatients from the 2 trials that included simvastatinand pravastatin. Statistical comparisons between ro-suvastatin and the other drug treatments were con-ducted using a logistic regression model. Data werefrom the intention-to-treat population who received�1 dose of drug and had a baseline and �1 post-baseline measurement. Measurements of serumLDL cholesterol levels were done at weeks 2, 6, 10,and 12. The last observation made was carriedforward to be included in the 12-week analysis ifpatients withdrew from the trial before the 12-weekmeasurement.
RESULTSOverall effects of rosuvastatin 10 mg on LDL choles-
terol goal achievement: Results were obtained from615 patients who received rosuvastatin 10 mg (389in trials that compared rosuvastatin with atorvasta-tin plus 226 in trials that compared rosuvastatin
with simvastatin and pravastatin). Overall, rosuva-statin 10 mg reduced LDL cholesterol by 47%, froma mean baseline of 186 mg/dL,12 and 80% of pa-tients receiving rosuvastatin achieved their ATP IIILDL cholesterol goals (Table 1). Almost half ofthese patients (43%) had an LDL cholesterol goal of�100 mg/dL, and 61% of these patients achievedthis goal (Table 1). Similarly, 81% achieved theEuropean goal of �3.0 mmol/L (�116 mg/dL).Most of these patients (77%) were defined as at highrisk of CAD according to European guidelines, andthe percentage of these high-risk patients whoachieved the goal of �3.0 mmol/L was nearly iden-tical to that of the overall group.
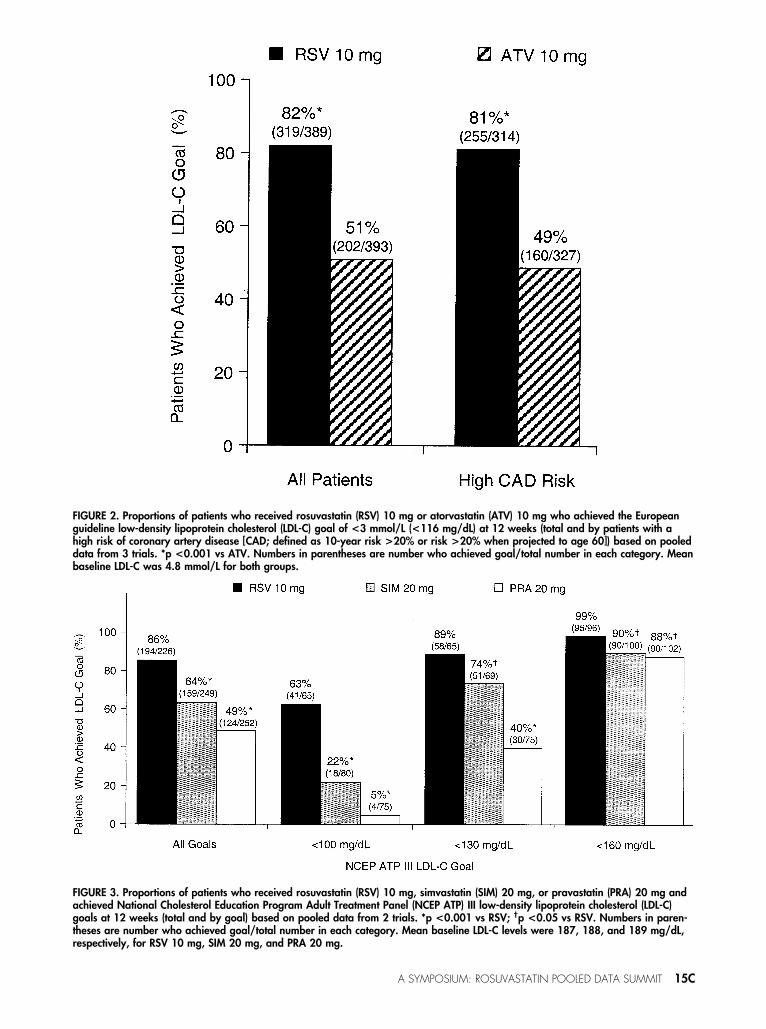
Comparison of rosuvastatin 10 mg with atorvastatin10 mg: The pooled data results from the 3 trials thatcompared rosuvastatin 10 mg with atorvastatin10 mg showed that significantly more patients whoreceived rosuvastatin 10 mg (76%) than those whoreceived atorvastatin 10 mg (53%) achieved theirATP III LDL cholesterol goals (p �0.001) (Figure1). Differences in goal achievement rates weremost evident among patients who had an LDL cho-lesterol goal of �100 mg/dL. In this group of pa-tients, 60% of those who received rosuvastatin10 mg reached their goal, compared with only 19%of patients who received atorvastatin 10 mg(Figure 1). Also, significantly more patients whoachieved rosuvastatin 10 mg (82%) than thosewho received atorvastatin 10 mg (51%) achievedthe European goal of �3.0 mmol/L (p �0.001)(Figure 2).
Comparison of rosuvastatin 10 mg with simvastatin20 mg and pravastatin 20 mg: Pooled data resultsfrom the 2 trials that compared rosuvastatin 10 mgwith simvastatin 20 mg and pravastatin 20 mgshowed that 86% of patients treated with rosuva-statin 10 mg met their ATP III LDL cholesterolgoals (Figure 3). In contrast, significantly fewerpatients treated with simvastatin 20 mg (64%) orpravastatin 20 mg (49%) met their goals(p �0.001). Additionally, significantly more pa-tients treated with rosuvastatin 10 mg than thosetreated with simvastatin 20 mg or pravastatin 20 mgmet their goals, regardless of the goal (p �0.05)(Figure 3). Finally, significantly more patientstreated with rosuvastatin 10 mg (80%) achieved theEuropean goal of �3 mmol/L compared with thosetreated with simvastatin 20 mg (48%) or pravastatin20 mg (16%) (p �0.001) (Figure 4).
Achievement of NCEP ATP III LDL cholesterol andnon-HDL cholesterol goals in patients with triglycerides>200 mg/dL: In the NCEP ATP III guidelines, non-HDL cholesterol is identified as a secondary targetin patients who have triglyceride levels �200 mg/dL. Non-HDL cholesterol levels represent the sumof LDL and other atherogenic lipoproteins that aretriglyceride rich. According to the ATP III guide-lines,1 meeting LDL cholesterol goals is the firstgoal of therapy, but patients with higher triglycer-
A SYMPOSIUM: ROSUVASTATIN POOLED DATA SUMMIT 13C
ides should also meet a goal for lowering non-HDLcholesterol levels, which was set at 30 mg/dL abovetheir LDL cholesterol goals. Therefore, the goalsfor non-HDL cholesterol levels are �130 mg/dL,
�160 mg/dL, and �190 mg/dL, respectively, ac-cording to the patient’s risk of CAD.
Overall, 182 of 615 hypercholesterolemic patientstreated with rosuvastatin 10 mg also had baseline
TABLE 1 Effects of Rosuvastatin 10 mg on Low-Density Lipoprotein Cholesterol (LDL-C)and Achievement of LDL-C Goals After 12 Weeks of Treatment (Pooled Data from 5Trials [N � 615])
Pooled Analysis Results(N � 615)
Mean (SD) baseline LDL-C 186 (19) mg/dL (4.8 mmol/L)Mean (SD) LDL-C at 12 wk 98 (29) mg/dL (2.5 mmol/L)Median LDL-C at 12 wk 94 mg/dL (2.4 mmol/L)Mean (SE) % change in
LDL-C from baseline�47 (0.6)
Patients who achieved ATP III goals, % (n)All patients 80 (491/615)Goal �100 mg/dL 61 (161/264)Goal �130 mg/dL 89 (119/134)Goal �160 mg/dL 97 (211/217)
Patients who achieved European goal of�3.0 mmol/L, % (n)
All patients 81 (500/615)High risk for CAD* 80 (380/475)
*As defined by the European guidelines.2
FIGURE 1. Proportions of patients who received rosuvastatin (RSV) 10 mg or atorvastatin (ATV) 10 mg and achieved National Choles-terol Education Program Adult Treatment Panel (NCEP ATP) III low-density lipoprotein cholesterol (LDL-C) goals at 12 weeks (all goalsand by individual goal) based on pooled data from 3 trials. *p <0.001 vs ATV. Numbers in parentheses are number achieving goal/total number in each category. Mean baseline LDL-C levels were 186 mg/dL for RSV 10 mg and 187 mg/dL for ATV 10 mg.
14C THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 91 (5A) MARCH 6, 2003
FIGURE 2. Proportions of patients who received rosuvastatin (RSV) 10 mg or atorvastatin (ATV) 10 mg who achieved the Europeanguideline low-density lipoprotein cholesterol (LDL-C) goal of <3 mmol/L (<116 mg/dL) at 12 weeks (total and by patients with ahigh risk of coronary artery disease [CAD; defined as 10-year risk >20% or risk >20% when projected to age 60]) based on pooleddata from 3 trials. *p <0.001 vs ATV. Numbers in parentheses are number who achieved goal/total number in each category. Meanbaseline LDL-C was 4.8 mmol/L for both groups.
FIGURE 3. Proportions of patients who received rosuvastatin (RSV) 10 mg, simvastatin (SIM) 20 mg, or pravastatin (PRA) 20 mg andachieved National Cholesterol Education Program Adult Treatment Panel (NCEP ATP) III low-density lipoprotein cholesterol (LDL-C)goals at 12 weeks (total and by goal) based on pooled data from 2 trials. *p <0.001 vs RSV; †p <0.05 vs RSV. Numbers in paren-theses are number who achieved goal/total number in each category. Mean baseline LDL-C levels were 187, 188, and 189 mg/dL,respectively, for RSV 10 mg, SIM 20 mg, and PRA 20 mg.
A SYMPOSIUM: ROSUVASTATIN POOLED DATA SUMMIT 15C
FIGURE 4. Proportions of patients who received rosuvastatin (RSV) 10 mg, simvastatin (SIM) 20 mg, or pravastatin (PRA) 20 mg whoachieved the Joint European guideline low-density lipoprotein cholesterol (LDL-C) goal of <3 mmol/L (<116 mg/dL) at 12 weeks (to-tal and by patients with a high risk of coronary artery disease [CAD; defined as 10-year risk >20% or risk >20% when projected toage 60]) based on pooled data from 2 trials (*p <0.001 vs SIM and PRA). Numbers in parentheses are number who achieved goal/total number in category. Mean baseline LDL-C levels were 4.8, 4.9, and 4.9 mmol/L, respectively, for RSV 10 mg, SIM 20 mg, andPRA 20 mg.
FIGURE 5. Proportions of patients who had triglyceride levels >200 mg/dL and who achieved both low-density lipoprotein choles-terol (LDL-C) and non–high-density lipoprotein cholesterol (non–HDL-C) NCEP ATP III goals. Rosuvastatin (RSV) 10 mg and atorvastatin(ATV) 10 mg results from the 3 trials that compared RSV with ATV are shown in the first set of bars, and RSV 10 mg, simvastatin(SIM) 20 mg, and pravastatin (PRA) 20 mg results from the 2 trials that compared RSV with SIM and PRA are shown in the secondset of bars.
16C THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 91 (5A) MARCH 6, 2003
triglyceride levels �200 mg/dL, and 129 (71%) ofthese patients met both their LDL cholesterol andnon-HDL cholesterol goals. Figure 5 shows the resultsfrom the comparator pooled-data sets. Because thepatient numbers were small, no statistical analysis wasperformed. In the trials comparing rosuvastatin withatorvastatin, 66% of rosuvastatin-treated patients,compared with 32% of atorvastatin-treated patients,met both goals. In trials comparing rosuvastatin withsimvastatin and pravastatin, 80% of patients in therosuvastatin 10 mg group, 54% in the simvastatin 20mg group, and 20% in the pravastatin group met bothgoals (Figure 5).
SUMMARYThese pooled analysis results from a large num-
ber of patients show that rosuvastatin 10 mg re-duces LDL cholesterol sufficiently to allow mostpatients to achieve both NCEP ATP III and Euro-pean goals regardless of risk category. When com-pared with the usual starting doses of atorvastatin,simvastatin, and pravastatin, significantly more pa-tients reached their goals with rosuvastatin 10 mg.This ability to bring more patients to guidelinegoals at an initial dose offers the potential advan-tage of obviating the need for titration to higherdoses.
The recent Heart Protection Study14 (HPS) mayhave a substantial impact on lipid-lowering treatmentin clinical practice. In this large long-term study, statintreatment was associated with significant reductions inmajor cardiovascular events across a broad range ofbaseline and post-treatment LDL cholesterol levels,including those �100 mg/dL. These results are likelyto lead to revisions of current guidelines. Many stud-ies have shown that the low LDL cholesterol levelsassociated with the greatest risk reduction in the HPSmay be difficult to achieve, particularly in patientswith higher initial LDL cholesterol levels. In thiscontext, a drug such as rosuvastatin, which has beenshown to reduce LDL cholesterol levels sufficiently toreach the lower goal levels in a large number ofhypercholesterolemic patients, can be of considerablevalue.
Acknowledgment: The authors gratefully acknowl-edge the contributions of David A. Wood, MSc,
whose presentation on major lipid guidelines providedmuch of the foundation for the introduction of thisarticle.
1. Expert Panel on Detection, Evaluation, and Treatment of High Blood Choles-terol in Adults. Executive Summary of the Third Report of the National Choles-terol Education Program (NCEP) Expert Panel on Detection, Evaluation, andTreatment of High Blood Cholesterol in Adults (Adult Treatment Panel III).JAMA 2001;285:2486–2497.2. Second Joint Task Force. Prevention of coronary heart disease in clinicalpractice: recommendations of the Second Joint Task Force of European and otherSocieties on Coronary Prevention. Eur Heart J 1998;19:1434–1503.3. EUROASPIRE II Study Group. Lifestyle and risk factor management anduse of drug therapies in coronary patients from 15 countries: principal resultsfrom EUROASPIRE II Euro Heart Survey Programme. Eur Heart J 2001;22:554 –572.4. Sueta CA, Chowdhury M, Boccuzzi SJ, Smith SC Jr, Alexander CM, LondheA, Lulla A, Simpson RJ Jr. Analysis of the degree of undertreatment of hyper-lipidemia and congestive heart failure secondary to coronary artery disease. Am JCardiol 1999;83:1303–1307.5. Pearson TA, Laurora I, Chu H, Kafonek S. The lipid treatment assessmentproject (L-TAP): a multicenter survey to evaluate the percentages of dyslipidemicpatients receiving lipid-lowering therapy and achieving low-density lipoproteincholesterol goals. Arch Intern Med 2000;160:459–467.6. Fonarow GC, French WJ, Parsons LS, Sun H, Malmgren JA. Use of lipid-lowering medications at discharge in patients with acute myocardial infarction:data from the National Registry of Myocardial Infarction 3. Circulation 2001;103:38–44.7. Pearson TA, Peters TD. The treatment gap in coronary artery disease and heartfailure: community standards and the postdischarge patient. Am J Cardiol 1997;80:45H–52H.8. Brown AS, Bakker-Arkema RG, Yellen L, Henley RW Jr, Guthrie R, Camp-bell CF, Koren M, Woo M, McLain R, Black DM. Treating patients withdocumented atherosclerosis to National Cholesterol Education Program–rec-ommended low-density-lipoprotein cholesterol goals with atorvastatin, fluva-statin, lovastatin and simvastatin. J Am Coll Cardiol 1998;32:665–672.9. Hunninghake D, Bakker-Arkema RG, Wigand JP, Drehobl M, Schrott H, EarlyJL, Abdallah P, McBride S, Black DM. Treating to meet NCEP-recommendedLDL cholesterol concentrations with atorvastatin, fluvastatin, lovastatin, or sim-vastatin in patients with risk factors for coronary heart disease. J Fam Pract1998;47:349–356.10. Andrews TC, Ballantyne CM, Hsia JA, Kramer JH. Achieving and main-taining National Cholesterol Education Program low-density lipoprotein choles-terol goals with five statins. Am J Med 2001;111:185–191.11. Fedder DO, Koro CE, L’Italien GJ. New National Cholesterol EducationProgram III guidelines for primary prevention lipid-lowering drug therapy: pro-jected impact on the size, sex, and age distribution of the treatment-eligiblepopulation. Circulation 2002;105:152–156.12. Blasetto JW, Stein EA, Brown WV, Chitra R, Raza A. Efficacy of rosuva-statin compared with other statins at selected starting doses in hypercholester-olemic patients and in special population groups. Am J Cardiol 2003;91(suppl5A):3C–10C.13. Rader DJ, Davidson MH, Caplan RJ, Pears JS. Lipid and apolipoproteinratios: association with coronary artery disease and effects of rosuvastatincompared with atorvastatin, pravastatin, and simvastatin. Am J Cardiol 2003;91(suppl 5A):20C–24C.14. Heart Protection Study Collaborative Group. MRC/BHF Heart ProtectionStudy of cholesterol lowering with simvastatin in 20,536 high-risk individuals: arandomized placebo-controlled trial. Lancet 2002;360:7–22.
DISCUSSION
Michael H. Davidson, MD (Chicago, Illinois,USA): Every time I compare the Prospective Cardio-vascular Munster (PROCAM)1 risk scoring and the
Framingham risk scoring, used in both the AdultTreatment Panel (ATP) III and the European guide-lines, I come out with a lower PROCAM risk score. In