32
2008 Management of Trachoma i n the Northern T erri tory www.nt.gov.au/health DEPARTMENT OF HEALTH AND FAMILIES Centre for Disease Control Guidelines fo r
2008 Management of Trachomain the Northern Territory
www.nt.gov.au/health
D E PA RT M E N T O F H E A LT H A N D FA M I L I E S
Centre for Disease Control
Guidelines for

First Edition 1998Second Edition 2008
Further copies available from: Darwin: DiseaseControl ph89228044Katherine: DiseaseControl ph89739049EastArnhem: DiseaseControl ph89870359TennantCreek: DiseaseControl ph89624259AliceSprings DiseaseControl ph89517540
Preparedin2008bytheCentreforDiseaseControl
CommentsarewelcomeandshouldbedirectedtotheTrachomaProjectcoordinatorat:
CentreforDiseaseControlDepartmentofHealthandFamiliesGPOBox721AliceSpringsNT0871
I
GuidelinesforTreatmentofTrachomaintheNorthernTerritory
Contents
1 Background........................................................................................ 12 Prevalence of trachoma in the NT.................................................... 23 Natural history of trachoma.............................................................. 24 Trachoma transmission .................................................................... 35 Trachoma diagnosis .......................................................................... 3 Table 1 WHO five sign grading system ......................................................................... 3 Table 2 WHO Simplified Trachoma Grading Card ........................................................ 4
6 Trachoma Control Program .............................................................. 6
6.1 The World Health Organisation SAFE Strategy ............................................. 66.2 Community Engagement and Consent ........................................................... 67 Training............................................................................................... 78 Surveillance ....................................................................................... 79 Screening ........................................................................................... 89.1 Equipment required........................................................................................... 89.2 Screening Procedure ........................................................................................ 89.3 Everting the upper eyelid.................................................................................. 910 Trachoma prevalence ...................................................................... 1010.1 How to measure trachoma prevalence .......................................................... 1010.2 Coverage .......................................................................................................... 1011 Post screening ................................................................................. 1012 Management of trachoma ............................................................... 1112.1 ‘S” - Surgery and followup ............................................................................. 1112.2 ‘A’ - Antibiotics ................................................................................................. 1112.2.1 Prevalence ≥10% in children aged <10 years with no obvious clustering .......... 1212.2.2 Prevalence ≥10% in children aged <10 years with strong obvious household
clustering .................................................................................................................. 1212.2.3 Prevalence <10% in children aged <10 years ........................................................ 1212.2.4 Prevalence 20% or more in children aged <10 years ............................................ 12 Table 3 Recommended antibiotic treatment and trachoma screening frequency ... 1312.2.5 Azithromycin ............................................................................................................. 13 Table 4. Dose for weight chart ....................................................................................... 1412.2.6 Azithromycin for children under 6 months of age ................................................ 1412.2.7 How much azithromycin to order............................................................................ 1412.3 ‘F’ - Face Washing (clean faces) .................................................................... 1512.4 ‘E’ - Environmental Health .............................................................................. 15

II
DEPARTMENTOFHEALTHANDFAMILIES
13 Data management............................................................................ 1514 Useful health promotion resources ............................................... 16References ............................................................................................ 16Appendix 1 ............................................................................................ 17Useful ResourcesAppendix 2 ............................................................................................ 18AZITHROMYCIN FOR TRACHOMA. Information for health care providersAppendix 3 ............................................................................................ 20Form 1Community summary form for screening of children with active trachomaAppendix 4 ............................................................................................ 21Form 2Community summary form for treatment with azithromycinAppendix 5 ............................................................................................ 22Form 3Community summary form for trachoma control activities implementedAppendix 6 ............................................................................................ 23 Form 4Trichiasis in Aboriginal and Torres Strait Islander adultsAppendix 7 ............................................................................................ 24 Annex 1Individual data collection form for active trachoma screeningAppendix 8 ............................................................................................ 25Annex 2Individual data collection form for trichiasis in Aboriginal and Torres Strait Islander adults

III
GuidelinesforTreatmentofTrachomaintheNorthernTerritory
TheGuidelines for Management of Trachoma in the Northern Territory, 2008 are basedon the Communicable Disease NetworkAustralia (CDNA),Guidelines for the public health management of trachoma in Australia 2006.1TheCDNAguidelinesprovideaminimumbestpractice framework for themanagement of trachoma.TheNorthernTerritory trachomaworkingpartyadaptedthenationalguidelinestoreflecttheuniqueneedsoftheNorthernTerritory.
TheNorthernTerritorytrachomamanagementguidelinesdiffer fromtheCDNAguidelines inthefollowingways.
1. Azithromycinantibiotic treatment is recommended forallcasesandhouseholdscontactsoftrachomaincludingbabies<6monthsofage.
2. Childrenunder6monthsofagewhoreceiveazithromycin,shouldbeactivelyfollowedupat1weekand4weekstoobserveforadverseeffects.
3. Incommunitieswhere the rateof trachoma is>20%, re-treatmentwithazithromycinafter6monthsisstronglyencouraged.
Trachoma management in the Northern Territory 2008.
What’s new?
1. Trachomascreeningshouldbeconductedannuallyaspartof theHealthySchoolAgeKidsscreening.
2. Facialcleanlinessshouldbeobservedandrecordedaspartoftrachomascreening.3. Therecommendedantibiotictreatmentandtrachomascreeningfrequencyhasbeenupdated.4. Inareaswheretrachomaisendemicadultsaged40-54yrsshouldbescreenedevery2years
fortrichiasisandthose>55yearsshouldbescreenedannuallyfortrichiasisaspartoftheadulthealthcheck.
5. Azithromycin antibiotic treatment is recommended for all cases and household contacts oftrachoma,includingbabies<6monthsofage.
6. Incommunitieswhere the rateof trachoma is20%ormore, re-treatmentwithazithromycinafter6monthsisrecommended.
7. Facewashinghealthpromotionprogramsareapriority.8. CentreforDiseaseControlcollectsandmaintainsaminimumdatasetfortrachoma.9. Healthserviceprovidersinvolvedintrachomamanagementshouldbeassessedascompetent
inthediagnosisandmanagementoftrachoma.

DEPARTMENTOFHEALTHANDFAMILIES
1
1 Background
Trachomaisacontagiousinfectionoftheeye,causedbythebacteriaChlamydia trachomatis.TheserovarofChlamydiathatcausestrachomaisslightlydifferentfromthegenitalserovar.
Repeated trachoma infection causes scarringof theeyelidand in-turnedeyelashes (trichiasis),whichleadtoblindnessifnottreatedwithsurgery.Blindnessfromtrachomaisentirelypreventable.
Trachomawaseradicated frommost parts ofAustralia by the1930s.Despite improvements inhealthservicedelivery, trachomaremainsendemic inmanyIndigenouscommunitiesacross theNorthernTerritory(NT).AustraliaistheonlydevelopednationwhereendemictrachomaisfoundinIndigenouspeople.
AustraliaisasignatorytotheWorldHealthOrganization(WHO)GlobalEliminationofTrachomaby2020andhasrecentlyintroducedseveralnewstrategiestoeradicatetrachoma.TheNationalTrachomaSurveillanceandReportingUnitwasestablishedtomonitortheprevalenceandeffectoftrachomamonitoringprograms.In2006,theCommunicableDiseasesNetworkAustralia(CDNA)publishedGuidelines for the public health management of trachoma in Australia.1TheseguidelinesproviderecommendationstoensureconsistencyintrachomacontrolprogramsacrossAustralia.
The CDNA national trachoma guidelines recommend that government run regional populationhealthunitsberesponsiblefortrachomacontrol.IntheNT,theCentreforDiseaseControl(CDC)provides training, assistance and coordination of trachoma control programs.Government andnon-governmentprimaryhealthcareservicesmayaccessadviceandassistanceinthedetectionandmanagementoftrachomawhenrequired.
CurrentprevalencedataforactivetrachomaintheNTisincomplete(Figure1).TheextenttowhichtrachomaisbothscreenedandmanagedvariesacrosstheNT.TheCDCcanassistcommunitiesacrosstheNTtocoordinatetheireffortstoeliminatethispreventabledisease.
To monitor the prevalence and effectiveness of trachoma management in the NT, summarytrachomadataisbeingcollectedandmaintainedbyCDC.Remotecommunitieswillreceivetimelyfeedbackofdatafollowingtrachomascreeningandtreatmentprograms.Thisdatawillassistintheevaluationoftrachomacontrolprograms.Asthedatadoesnotuseindividualnames,confidentiallywillbemaintained.
TheseguidelinesfortrachomamanagementintheNTareadaptedfromtheCDNAGuidelines for the public health management of trachoma in Australia1,2006.Theydonotprecludehealthservicesorcommunitiesimplementingcontrolstrategiesoverandabovewhatisrecommendedhere.
GuidelinesforTreatmentofTrachomaintheNorthernTerritory
2
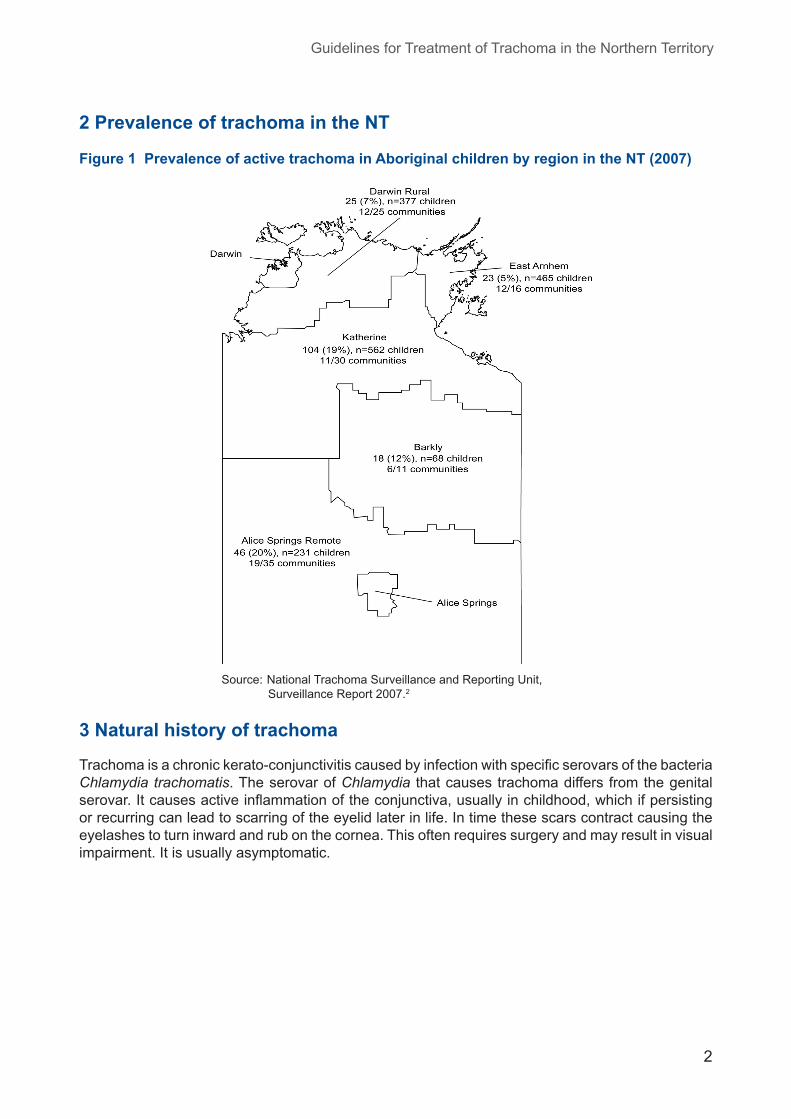
2 Prevalence of trachoma in the NT
Figure 1 Prevalence of active trachoma in Aboriginal children by region in the NT (2007)
Source: NationalTrachomaSurveillanceandReportingUnit,SurveillanceReport2007.2
3 Natural history of trachoma
Trachomaisachronickerato-conjunctivitiscausedbyinfectionwithspecificserovarsofthebacteriaChlamydia trachomatis.TheserovarofChlamydia thatcausestrachomadiffersfromthegenitalserovar.Itcausesactiveinflammationoftheconjunctiva,usuallyinchildhood,whichifpersistingorrecurringcanleadtoscarringoftheeyelidlaterinlife.Intimethesescarscontractcausingtheeyelashestoturninwardandrubonthecornea.Thisoftenrequiressurgeryandmayresultinvisualimpairment.Itisusuallyasymptomatic.

DEPARTMENTOFHEALTHANDFAMILIES
3
4 Trachoma transmission
Themainsourceoftrachomainfectionisinfectedeyesecretionsinpersonswithtrachoma.
Theactive infectivestagesof trachoma(trachomatous inflammation- follicularand intense)areusuallyfoundinchildren.
Thereisnoanimalreservoirfortrachoma.
Routesoftransmissioninclude:
• directeyetoeyespread(egwhileplayingorsharingabed)• fingers• indirectspreadthroughsharingtowels,pillowsetc• eyeseekingflies• coughingandsneezing.
Trachomaprevalencevariesbetweenandwithincommunities.Withincommunities it isstronglyclusteredbyhouseholds.Withinhouseholds,itisclusteredbysleepingrooms.
Trachomaoccursmorecommonlyindrydustyenvironments.Itisassociatedwithovercrowding,reducedavailabilityanduseofwater,inadequatewastedisposalandhighnumberofflies.1
5 Trachoma diagnosis
Trachomaisaclinicaldiagnosis.
TheWHOhasdevelopedasimple5signgradingsystemfordiagnosisandassessmentoftrachoma(seeTable1).Toensureconsistency,thissystemshouldbeusedintrachomacontrolprogramsintheNT.
Table 1 WHO five sign grading system
TF Trachomatous inflammation-follicular
5ormorefolliclesintheuppertarsalconjunctiva.Folliclesmustbemorethan0.5mmindiameter.
TI Trachomatous inflammation-intense
Pronouncedinflammatorythickeningofthetarsalconjunctivawhichobscuresmorethanhalfofthenormaldeeptarsalvessels.
TS Trachomatous conjunctival-scarring
Visiblescarsintheuppertarsalconjunctiva.
TT Trachomatous trichiasis
Atleast1eyelashrubsontheeyeball,orevidenceofrecentremovalofinturnedlashes.
CO Corneal opacity Visiblecornealopacityoverthepupilwhichissodensethatatleastpartofthepupilmarginisblurredthroughtheopacity.
Source:WorldHealthOrganization,19873
Eachsignisindividuallygradedasbeingpresentorabsent.Oneormoresignscanandusuallydo,occurtogether.Table2providesfurtherdescriptionofthesigns.

GuidelinesforTreatmentofTrachomaintheNorthernTerritory
4
Table 2 WHO Simplified Trachoma Grading Card
The normal everted upper lidThenormalconjunctivacoversthefirmpartoftheuppereyelid,overthecentral2/3.Itdoesnotincludethecornersortheroundededgeofthetarsalplate.The normal conjunctiva is pink, smooth, thinand transparent. Over the whole area of thetarsal conjunctiva there are normally largedeep-lyingbloodvesselsthatrunvertically.
TF Trachomatous inflammation-FollicularThe presence of 5 or more follicles in the upper tarsal conjunctiva.
Folliclesareroundswellingsthatarepalerthanthe surrounding conjunctiva, appearing white,greyoryellow.Folliclesmustbeatleast0.5mmindiametertobeconsidered.
TI Trachomatous inflammation-IntensePronounced inflammatory thickening of the tarsal conjunctiva that obscures more than half of the normal deep tarsal vessels.Thetarsalconjunctivaappearsred,roughandthickened.Thereareusuallynumerousfollicles,whichmaybepartiallyortotallycoveredbythethickenedconjunctiva.
Note:Eye conditions that can be mistaken for folliclesSmall scars can bemistaken for follicles but are sharp edged and not round aswith follicles.Degenerativedeposits includeconjunctivalconcretions thatareyellowishmasseswithclearcutedges,orcyststhatappearasclearbubblesintheconjunctiva.Thesecanbemistakenforfollicles.

DEPARTMENTOFHEALTHANDFAMILIES
5
Table 2 continued. WHO Simplified Trachoma Grading Card
TS Trachomatous ScarringThe presence of scarring in the tarsal conjunctiva.Scarsareeasilyvisibleaswhite lines,bands,or sheets in the tarsal conjunctiva. They areglisteningandfibrousinappearance.Scarring,especially diffuse fibrosis, may obscure thetarsalbloodvessels.
TT Trachomatous TrichiasisAt least 1 eyelash rubs on the eyeball.Evidence of recent removal of inturnedeyelashesshouldalsobegradedastrichiasis.
CO Corneal OpacityEasily visible corneal opacity over the pupil.The pupil margin is blurred viewed throughthe opacity. Such corneal opacities causesignificantvisualimpairment(lessthan6/18or0.3 vision), and therefore visual acuity shouldalsobemeasuredifpossible.
AdaptedfromTheWorldHealthOrganizationsimplifiedtrachomagradingclassificationsystem.Source:WorldHealthOrganization,1987.3
GuidelinesforTreatmentofTrachomaintheNorthernTerritory
6
6 Trachoma Control Program
6.1 The World Health Organization SAFE Strategy
TheWhoGlobalEradicationofTrachomaby2020initiative,recommendstheimplementationoftheSAFEstrategyfortheeffectivecontroloftrachoma.Thisincludes:
• Surgery–surgicalcorrectionfortrichiasis • Antibiotics-antibiotictreatmentofcasesandcontactsofactivetrachoma • Facial Cleanliness–promotecleanfacestoreducespreadofinfection • Environmental Health– improvewateraccess, toilethygieneandsanitation,wasteandflycontrolandpromoteactivitiesthatreduceovercrowding.
6.2 Community engagement and consent
Communityengagementisanessentialpartoftrachomamanagement.Consultationwithcouncils,healthboardsandotherkeycommunitymembersregardingtrachomacontrolisaprerequisitetoimplementingtheSAFEstrategy.Thisshouldoccurannuallybeforeschoolscreening,toensureinformed consent is obtained. Community assistance should be sought for improved hygienemeasures,face-washingprogramsandwiththelogisticsofazithromycinadministration.
Acommunityengagementprocessisrecommendedwithaholisticapproach.
Keystepsintheplanningprocess.
1. Consultwithkeystakeholders.2. Determinecommunityprioritiesregardingtrachoma.3. Buildrelationships.4. Informthecommunityofhealthrisksoftrachomaandtheneedforaneradicationprogram.5. Inform the community about thedifferencebetweeneradicationprogramsandother health
programs.6. Allowthecommunitytomakeinformedchoices.
Keystakeholdersmayinclude:
• School• CommunityCouncil• ChildcareCentre• CommunityEnvironmentalHealthOfficers• AgedCareFacility• Elders• Women’sCentre• HealthAdvisoryBoard• CommunityHealthCentre.

DEPARTMENTOFHEALTHANDFAMILIES
7
7 Training
TheCDNAGuidelines for the public health management of trachoma in Australia1recommendthatallhealthprofessionalsinvolvedintrachomacontrolreceiveongoingtraininginthediagnosisandmanagementoftrachoma.
CDCconductstraininginallaspectsoftrachomacontrol.
Thisincludes:
• communityconsultationandengagement• recognitionoftrachoma• trachomagrading• eyelideversion• obtainingconsent• organisingatreatmentprogram• healthpromotionactivities.
IntheNT,CDCrecommendsthatallhealthprofessionalsinvolvedintrachomacontrolbeassessedascompetentinthediagnosisandmanagementoftrachoma.
ContactyournearestCDCforinformationontrainingoptions.
8 Surveillance
IntheNT,screeningfortrachomaisconductedannuallyaspartoftheHealthySchoolAgeKidsProgram(HSAK).ForinformationorassistancewithHealthySchoolAgeKidsscreening,contacttheMaternal, Child andYouth Health team in your region. Screening for trachomamay occuroutsidetheHSAKprogram,accordingtocommunitypreference.
Theprevalenceof trachoma incommunities isdeterminedbyscreeningallschoolagechildrenforactivetrachoma.Toensurethereportedprevalenceoftrachomaisaccuratethecoverageofscreening should be at least 80% of the target group, ie. 80% of all school age children.Theabsoluteminimum targetgroup forscreening foractive trachoma isall childrenaged5-9yearslivingincommunities/townswheretrachomaisendemic.
Ideally,allchildrenaged1-4yearsshouldalsobeexamined,asthehighestprevalenceofactivetrachomaisusuallyfoundinthepreschoolchild.
Ifactivetrachomaisfoundduringscreening,appropriatecontrolmeasuresmustbeimplemented.
Independentprimaryhealthcareservicesmayhavetrachomacontrolprogramsinplace.Checkwithyourorganisation’spublichealthcoordinatorregardingthetrachomaprogram.
Ideally,trachomacontrolprogramsshouldbeconductedonaregionallevel.Screeningandtreatmentatapopulationlevelisthebestmethodtodecreasetheprevalenceoftrachoma.Treatmentatapopulationlevelreducesthepoolofinfectioncirculatinginthecommunity.Wherepossibleavoidscreeningandtreatingisolated,individualcasesoftrachoma.
CDCisabletoassistwiththescreeningandsurveillanceoftrachoma,contactyourregionalCDCformoreinformation.

GuidelinesforTreatmentofTrachomaintheNorthernTerritory
8
9 Screening
9.1 Equipment required
• Binocluarloupes,x2.5magnification• Penlighttorch• Orangestickorapplicatorstick• Soapandwateroralcoholbasedhandwash• Rubbishdisposalbags• Datacollectionform(seeAppendix3forsample)• Pens• WHOsimplifiedtrachomagradingchart• Seating.
9.2 Screening procedure
• Eacheyemustbeassessedseparately.• Binocluarloupes(X2.5)andadequatelightingareessential.• Washhandswithsoapandwateroralcoholbasedhandwash,rinseoffhandwash.
• Signsmustbeclearlyseenfortrachomatobereportedaspresent.• Refer to the WHO simplified trachoma grading card for a colouredpictorialguidetotrachomagrading.
• Observeandrecord facialcleanliness (Is there ‘sleep’,dirtorcrustingaroundtheeyes?).Cleanfaceisdefinedastheabsenceofdirtorcrustingonthecheeksandforehead.
• Examinefortrichiasis,eitherin-turnedeyelashesorpreviouslyremovedlashes. To check for this the upper lid needs to be pushedupwardsslightly,toexposethelidmargins.
• Examinethecorneaforopacities(CO).• Everttherightuppereyelid,examineandrecordthepresenceofTF,TIandTSinareashown.
• Everttheleftuppereyelid,examineandrecordthepresenceofTF,TIandTSinareashown.

DEPARTMENTOFHEALTHANDFAMILIES
9
9.3 Everting the upper eyelid
• Sitdirectlyinfrontoftheperson• Askthepersontolifttheirchinandlookdown• Hold theeyelashesbetween thumband thefirst fingergentlypulltheeyelidforwardtobreakthesuctionandstretchthelidalittle
• Placeaclean,gentleinstrumentsuchasanapplicatorstick,ortheindexfingerofyourotherhandabovethecrease on the upper eyelid.Push downgently, pulltheeyelidoutandupoverthefingerorstick
• Steady theevertedeyelid, removestickorfingerandexamineforTF,TI,TS
• Askthepersontokeeplookingdown• Whenyouhavefinished,gentlyre-everttheeyelid• Recordyourfindings
DiagramsfromCRANAClinicalProceduresManualforremoteandruralpractice2001.4

GuidelinesforTreatmentofTrachomaintheNorthernTerritory
10
10 Trachoma prevalence
Publichealthactivitiesaimedatassistingcommunitiestoeliminatetrachomawillvarydependingontheprevalenceoftrachomainthecommunity.Therefore,itisimportanttoknowhowmuchactivetrachomathereisinthecommunity.Wedothisbymeasuringtheprevalenceoftrachoma.
The trachoma prevalence is used to determine the public health response to trachoma incommunities.
10.1 Measuring trachoma prevalence to determine public health response
• Followingthehealthyschoolagekidsscreening(ortrachomascreening),identifythenumberofchildren<10yearsscreenedandthenumberofchildren<10yearswhohavetrachoma.
• Calculateprevalenceoftrachomabyusingfollowingformula:
Numberofchildren<10yearsscreenedwhohavetrachomaNumberofchildren<10yearsscreened
10.2 Coverage
The coverage is used tomeasure the true extent of disease in a community. In this instance,itmeasureshowmanyschoolagechildrenwerescreenedcompared tohowmanyschoolagechildrenwholiveinthecommunity.
Thecoverageis:
TotalnumberofschoolagechildrenscreenedfortrachomaTotalnumberofschoolagechildrenwholiveinthecommunity
Toensureprevalenceoftrachomaisaccuratelyreportedthecoverageofscreeningshouldbeatleast80%ofthetargetgroup,ie.80%ofschoolagechildren.Theabsoluteminimumtargetgroupforactivetrachomaisallchildrenaged5-9yearslivingincommunities/townswheretrachomaisendemic.
11 Post screening
1. Calculatethetrachomaprevalenceandcoverage.2. Determinethetargetgroupfor treatment, thismayvarydependingontrachomaprevalence
(seeTable3).3. Plottrachomacasesonacommunitymaptodetermineifclusteringispresent.4. DiscusstrachomaprevalencewithyourregionalCDC.5. Liaisewithlocal/communitymedicalofficer,andPublicHealthCoordinator.6. Providetimelyfeedbacktofamiliesandthecommunity.7. LiaisewiththeCouncil,school,preschool,Healthcentreandchildcarecentreaswellasother
importantstakeholdersincommunity.8. Alltreatmentofchildrenmustbeconductedwithparentalorguardianconsent.Iftreatmentis
conductedatschool,writtenparentalconsentisrequired.
X100
X100

DEPARTMENTOFHEALTHANDFAMILIES
11
9. Discusstreatmentandhealthpromotionactivitieswithcommunitystakeholders.10.Aregionalapproachtotrachomacontrolisaneffectivestrategyinhighlymobilecommunities.
Liaisewithsurroundingcommunitieswhereappropriate.11. Determineadatetotreattargetgroup.12. Aimtocompletethetreatmentphaseover2weeks.13.Orderazithromycin(seeTable12.2.7).
12 Management of trachoma
TrachomamanagementintheNorthernTerritoryisbasedontheWHOSAFEstrategy.1
12.1 ‘S” - Surgery and followup
Thechronicsequelaeoftrachoma,trachomatousconjunctival-scarring,trichiasis,cornealopacityandblindness,occursinadults.
Theremovalofeyelashes(epilation)isnotrecommendedotherthanasatemporarymeasurewhilewaitingforsurgery,aseyelashesmaycausefurtherdamagewhentheyregrow.Epilationshouldbedonecarefullyusinggoodlightingandmagnificationloupes.Allpatientswithtrichiasisshouldbereferredtoaneyespecialistassoonaspossible.
Surgical interventionof trichiasisstops theeyelashes from rubbingagainst thecornea,causingcornealopacityandsubsequentblindness.
Surgerydoesnotalwayspreventtrichiasisinthefuture,astheremainingscartissuemaycontractand turnothereyelashes inward.Annual reviewpostsurgery is recommended todetect furthertrichiasis.
Inareaswhere trachomaor trichiasis isendemic,adultsaged40-54yearsshouldbescreenedevery2yearsandthose55+yearsshouldbescreenedannuallyfortrichiasisasapartofahealthyadultcheck.Healthservicesneedtoensurethataprocessisinplacefortimelysurgicalreferralandtreatmentofpeoplewithtrichiasis.
Adultswithtrachomascarringand/ortrichiasisshouldhavetheireyesexaminedannuallyaspartofthehealthyadultchecktodetectearlychanges.Theyshouldbeofferedcorrectivesurgerybeforetheyexperiencecornealopacity.Wherepractical, theyshouldbeplacedon thehealth centre’srecallsystem.
12.2 ‘A’ - Antibiotics
Antibioticisthe‘A’componentoftheSAFEstrategy.Theaimofantibiotictherapyistoreducetheprevalenceandintensityofactivetrachomainfection,preventingthedevelopmentofscarringandblindness.
Whentheprevalenceoftrachomaincommunitiesin1to9yearoldsis10%orhigher,theWHOrecommendationofcommunity-basedtreatmentiseasierandmoreeffective.
Thereforeiftheprevalenceoftrachomainchildren1-9yearsisover10%communitywidetreatmentisrecommendedunlessstrongfamilyclusteringisseenwhenfamilybasedtreatmentofallchildrenandalltheirhouseholdcontactsisindicated.

GuidelinesforTreatmentofTrachomaintheNorthernTerritory
12
Azithromycinistherecommendedtreatmentforallpeoplediagnosedwithtrachomaaswellasalltheirhouseholdcontacts(seeTable3,p13).
A household contact is anyone who is living and/or sleeping in the house.
12.2.1. Prevalence ≥10% in children aged <10 years with no obvious clustering
• Thesecommunitiesshouldbetargetedfortreatmentwithsingle-doseazithromycin.• Theaimistodecreasethereservoirofactivetrachomabytreatingallchildreninthecommunityupto14yearsofageandalltheirhouseholdcontacts.
• Healthpromotionactivitiesmustbeincludedinthepublichealthresponse.
12.2.2. Prevalence ≥10% in children aged <10 years with strong obvious household clustering
• Casesareobviouslyclusteredwithin1ormorehouseholds.• Healthstaffcaneasilyidentifyallhouseholdcontactsofcases.• Household treatmentwith single dose azithromycin for all people living and sleeping in thehousewithachildwithtrachoma.
• Healthpromotionactivitiesshouldbeincludedinthepublichealthresponse.
12.2.3. Prevalence <10% in children aged <10 years
• Treatallcasesandallhouseholdcontactswithsingle-doseazithromycin.• Healthpromotionactivitiesshouldbeincludedinthepublichealthresponse.
SeeTable3,p13.
12.2.4. Prevalence 20% or more in children aged <10 years
Incommunitieswhere trachomaprevalence is20%ormorere-treatmentwithazithromycinat6monthsisrecommeded.Re-screeningatthisstageisnotnecessary.ContactyourregionalCDCforassistance.
TheNationalTrachomaSurveillanceandReportingUnit(NTRSU)definehyperendemictrachomaasaprevalenceofactivetrachomaof20%ormore.5Currentliteraturesuggeststhere-treatmentofhyperendemictrachomawithazithromycinat6monthssignificantlyreducesocularchlamydiainfectionandthechanceofre-infectioninacommunity.6,7,8,9

DEPARTMENTOFHEALTHANDFAMILIES
13
Table 3. Recommended antibiotic treatment and trachoma screening frequencyTrachomaprevalenceinscreenedchildrenaged<10years
Treatmentofcasesofactivetrachomaa(TF,TI)
Treatmentforhouseholdcontactscofcaseswithactivetrachomaa
Communitytreatmenta
Screeningfrequency
≥10%withnoobviousclustering
Single-doseazithromycinb
Single-doseazithromycinbtoallhouseholdcontactsc.
Single-doseazithromycinbtoallchildrenupto14yearsofage.
Annual
≥10%And casesareobviouslyclusteredwithinseveralhouseholdsAnd healthstaffcaneasilyidentifyallhouseholdcontactscofcases
Single-doseazithromycinb
Single-doseazithromycinbtoallhouseholdcontactsc.
Nil Annual
<10% Single-doseazithromycinb
Single-doseazithromycinbtoallhouseholdcontactsc.
Nil Annual
<5% Single-doseazithromycinb
Single-doseazithromycinbtoallhouseholdcontactsc.
Nil Annual
<5%for5consecutiveyears
Single-doseazithromycinb
Single-doseazithromycinbtoallhouseholdcontactsc.
Nil Ceasescreening
a Antibiotictreatmentofcasesandcommunitymembersshouldbecompletedwithin2weeksofscreening.bAzithromycindoseis20mg/kg,uptoamaximumdoseof1000mg.cahouseholdcontactisdefinedasanyonewhoislivingandsleepinginthehouse.Source:Guidelines for Public Health Management of trachoma in Australia CDNA2006.1
12.2.5 Azithromycin
• Azithromycin orally as a single dose 20mg/kg (maximumdose 1000mg) is the treatment ofchoice(Table4).
• Ifazithromyciniscontraindicated,discussalternativetreatmentwithyourlocalmedicalofficer.
Preparation:40mg/mlpowdertobereconstitutedwithwater,or500mgtablet.
Administration:orallyasasingledose.

GuidelinesforTreatmentofTrachomaintheNorthernTerritory
14
Table 4 Dose for weight chart
Weight Azithromycin dose
3kgto<6kg 80mg(2ml)a
6kgto<10kg 160mg(4ml)a
10kgto<15kg 240mg(6ml)a
15kgto<20kg 400mg(10ml)a
20kgto<30kg 500mg(1tablet)b
30kgto<40kg 750mg(1½tablets)b
over40kgadults 1000mg(2tablets)b
a200mg/5mlsuspensionb500mgtablet
12.2.6 Azithromycin for children under 6 months of ageAzithromyciniscurrentlylicensedfortreatmentoftrachomaininfantsover12months.However,theNationalHealthandMedicalResearchCouncilrecommendsitsuseinallinfantsforthepreventionandtreatmentofpertussisandsuggestthatitistheantibioticofchoiceinthoseunderonemonthofage.10Thereforestaffshouldfeelcomfortablerecommendingazithromycintoinfants,butinfantsunder6monthsofageshouldbereviewedat1and4weeksaftertreatmentandreportanyadverseeffectstoTrachomaCoordinatoron89516902or89516906.11
Azithromycinmaybeusedinpregnancyandlactation.ItisacategoryB1drug-usedbyalimitednumberofpregnantwomenwithoutanyincreaseinharmfuleffectsonthefetus.
TheCDNAGuidelines for the public health management of trachoma in Australiarecommendtheantibiotictreatmentprogramfortrachomabecompletedwithin2-weeksofscreeningtominimisethelikelihoodofreinfectionandtoachievehigherpopulationcoverage.
TheNationalTrachomaSurveillanceandReportingUnitmonitorsandreportsontheprevalenceofresistancetotheantibioticAzithromycin.
12.2.7 How much azithromycin to order
Age Azithromycin Syrup Azithromycin Tablets
Under5years 1bottleforevery2childrenrequiringtreatment.
5-10years 1bottleforeverychildrequiringtreatment.
10–12years 1.5bottlesforeverychildrequiringtreatment.
Over12years 1000mg=2x500mgtabletsforeachpersonrequiringtreatment.
Sometimesolderchildrenwillnotswallowtabletseveniftheyarecrushed,soitisbettertohavemoresyrup.

DEPARTMENTOFHEALTHANDFAMILIES
15
12.3 ‘F’ - Face washing (clean faces)
Ithasbeenobservedthatchildrenwithcleanfacesarelesslikelytohaveactivetrachomathanthosewithoculardischarge,nasaldischargeorfliesontheirface.12
Thereforefacialcleanlinessinchildrenshouldbepromotedbyincludingregularfacewashingaspartofaholisticpersonalhygieneprogram.Childrenshouldalsobeencouragedtobrushfliesawayfromtheirfaceandeyestoreducethespreadofinfection.
Face and hand washing may be incorporated into health promotion activities in schools andchildcarecentres.
Ifpossibleandsafe,childrenshouldbeencouragedtoswiminpools,waterholes,riversandtheocean.
12.4 ‘E’ - Environmental health
Improved environmental health and socio-economic conditions areacknowledgedasimportantfactorsinpreventingtrachoma.EnvironmentalhealthinterventionsrecommendedbyWHOinclude:
• Reducefliesinthecommunitythroughimprovingwastemanagementactivitiesinthecommunity.• Instigateappropriatehealtheducationandpromotionactivities,includinghandandfacewashingactivitiesandotherassociatedhygienetraininginappropriatecommunitysettingsegschools,women’scentres,clinic,storeandcounciloffice.
• Avoidingovercrowding.• SeekassistancefromEnvironmentalHealth,HealthPromotionandCentreforDiseaseControlforaco-ordinatedapproachoftrachomamanagement.
13 Data management
Informationobtained fromtrachomascreeningshouldbeprovided to thecommunity ina timelymanner.Alldataobtainedfromtrachomascreeningbelongstotheindividualcommunity.Assoonaspracticalafterscreeninghasoccurred,families,andotherkeystakeholdersshouldbeinformedof theresults. Indoingso,stakeholderswillbeengaged in the implementationof the treatmentprogram.
Trachomaprevalencedataisreportedbycommunity.Thesedatarepresentpublichealthsurveillanceandassistsintheevaluationoftrachomacontrolprograms.Thedatadoesnotcontainpersonalidentifyinginformation.Itisrecordedinagegroupstoidentifytheburdenofdisease.
Treatmentdataisalsoreportedinagegroups.TheNationalTrachomaSurveillanceandReportingUnit,monitorsandreportsonazithromycinresistance.
CDC is required tocollectandmaintainaminimumdataset for trachoma in theNT.TheCDNANationalTrachomaGuidelinesrecommendregionalpopulationhealthunitscollecttrachomadatainaccordancewiththeminimumnationaltrachomadataset.Thesedataarethenreportedtothenationaltrachomadatabase.SeeAppendix3.
ForassistancewithcommunityfeedbackcontactyourregionalCDCforassistance.

GuidelinesforTreatmentofTrachomaintheNorthernTerritory
16
14 Useful health promotion resources
• The trachoma sickness colouring in booklet. ThisisaboutpreventionoftrachomaandwasmadebythehealthpromotionunitinKatherine.Itisaimedatschoolchildren.
• A video called “Jabbys friend. A story about trachoma”. ThiswasmadebytheKimberleyPublicHealthUnitintheHealthDepartmentofWesternAustralia,andisaimedspecificallyatAboriginalchildrenwithAboriginalcartooncharactersused togiveculturallyappropriateandentertaining information. It includes informationabout thediseaseprocessof trachomaandwaystopreventtrachoma.
• Trachoma eye sickness flipchart. ContactyourregionalCDC. • Preventing Trachoma Poster. ProducedbyWesternAustraliaHealthDept.ContactregionalCDC.
• ‘No Germs on Me’ Project.ContactregionalEnvironmentalHealthUnit.
References
1. Communicable Diseases Network Australia. Guidelines for Public Health Management of trachomain Australia. CDNA. 2006. www.health.gov.au/internet/wcms/publishing.nsf/Content/cds-cdns-pubs-trachoma.htm.
2. NationalTrachomaSurveillanceandReportingUnit.TrachomaSurveillanceAnnualReport,2007.Comm Dis Intell.2008;32(4):388-399.
3. ThyleforsB,DawsonCR,JonesBR,WestSKandTaylorHR(1987).Asimplesystemfortheassessmentoftrachomaanditscomplications.BulletinoftheWorldHealthOrganization65:477-483.
4. CouncilofRemoteAreaNursesofAustralia.ClinicalProceduresManual,2ndEdition.5. NationalTrachomaSurveillanceandReportingUnit.SurveillancereportforTrachoma,2006.Comm Dis
Intell.2007;31(4):366-374.6. LietmanT,PorcoT,Dawso,C,BlowerS.Global elimination of trachoma:How frequently shouldwe
administermasschemotherapy?Nature Medicine1999;5:572-576.7. BiebesheimerJB,HouseJ,HongKC,LakewT,AlemayehuW,ZhouZ,etal.CompleteLocaklElimination
of Infectious Trachoma from Severely Affected Communities after Six Biannual Mass AzithromycinDistributions.Ophthalmol.2009;116(11):2047-2050.
8. SolomonAW,Harding_EschE,AlexanderNDE,AguirreA,HollandM.TwoDosesofAzithromycin toEliminateTrachomainaTanzanianCommunity.N Eng J Med.2008;358(17):1870-1871.
9. CookJA.EliminatingBlindingTrachoma.N Eng J Med.2008;358(17):1777-1779.10.NationalHealthandMedicalResearchCouncil.TheAustralianImmunisationHandbook,9thed,Canberra.
AustralianGovernment;2008.p.235-236.11.SchultzR,CoffeyC,KrauseV,TaylorH,CurrieB.Treatmentoftrachomainsmallbabies.NTDisControl
Bull2007;14(4):22-23.12.WestS,MuñozB,LynchM,KayongoyaA,ChilangwaZ,MmbagaBB,TaylorHR.Impactofface-washing
ontrachomainKongwa,Tanzania.Lancet1995Mar11;345(8950):650-1.
DEPARTMENTOFHEALTHANDFAMILIES
17
Appendix 1
Useful resources
• Azithromycin fact sheet. This isuseful forproviding information topeople involvedwith thetrachomaprogramsuchassuchashealthworkers,nurses,andthehealthpromotionteam.SeeAppendix2.AlsoavailablefromCDC.
• Communicable Diseases Network Australia. Guidelines for Public Health Management oftrachomainAustralia.CanberraCDNA2006.
• CentralAustralian Rural PractitionersAssociation. CARPA Standard Treatment Manual. 4thEdition,2003.
• CouncilofRemoteAreaNursesofAustralia.ClinicalProceduresManual,2ndEdition.• EmersonPM,CairncrossS,BaileyRL,MabeyDCW(2000).Reviewoftheevidencebaseforthe‘F’and‘E’componentsoftheSAFEstrategyforTrachomaControl.Tropical Medicine and International Health 5:515-527.
• OfficeofAboriginalandTorresStraightIslanderHealth.SpecialistEyeHealthGuidelinesforuseinAboriginalandTorresStraightIslanderPopulations.Canberra:2001.
• SchultzR,CoffeyC,KrauseV,TaylorH,CurrieB.Treatmentoftrachomainsmallbabies.NTDis Control Bull 2007;14(4):22-23.
• ThePublicHealthBushBook–AresourceforworkingincommunitysettingsintheNorthernTerritory,THS1999.
• TrachomaKit.ContactregionalCDC.• TrachomaGrading –self directed learning.ACDproduced by theCentre forEyeResearchAustralia.ContactregionalCDC.
• TaylorHR.Trachoma:ABlindingScourgefromtheBronzeAgetotheTwenty-FirstCentury.EastMelbourneAustralia.CentreforEyeResearchAustralia/HaddingtonPress.2008.
• WorldHealthOrganization. Achievingcommunitysupport for trachomacontrol. Aguide fordistricthealthwork.Geneva:WHO,1995.
• WorldHealthOrganization.Futureapproachestotrachomacontrol.Reportofaglobalscientificmeeting.Geneva:June1996.
• WorldHealthOrganization.Primaryhealthcarelevelmanagementoftrachoma.Geneva:WHO,1989.
• World HealthOrganization. Trichiasis Surgery for trachoma. The bilamellar tarsal rotationprocedure.Geneva:WHO,1993.
• WorldHealthOrganization.WorldHealthOrganizationsimplifiedtrachomagradingcard.

GuidelinesforTreatmentofTrachomaintheNorthernTerritory
18
Appendix 2
AZITHROMYCIN FOR TRACHOMA
Information for health care providers
Theantibioticofchoiceforthepreventionandtreatmentoftrachomaisazithromycin.Itbelongsinthefamilyofmacrolideantibioticswhichincludeserythromycin,roxithromycinandclarithromycin.Azithromycinisbetterabsorbedfromthegastrointestinaltract,lastslongerinthebodyandgetsintothecellsbetterthantheothermacrolides.
Trachoma managementThe World Health Organization endorsed the SAFE strategy for the effective control of trachoma.
Surgery–surgicalcorrectionfortrichiasis
Antibiotics -antibiotictreatmentofcasesandcontactsofactivetrachoma
Facial Cleanliness–promotefaceandhandwashingtoreducespreadofinfection
Environmental Health–improvewateraccess,toilethygieneandsanitation,wasteandflycontrolandpromoteactivitiesthatreduceovercrowding.
Antibiotic treatment of trachomaAntibiotictreatmentoftrachomaisthoughttoreducetheprevalenceofactivetrachomainfectionandthereforepreventthedevelopmentofscarringandblindness.
Azithromycinistherecommendedtreatmentforallpeoplediagnosedwithtrachomaaswellastheirhouseholdcontacts.Ahouseholdcontactisanyonewhosleepsinthehouse.
Dosage of azithromycin
Preparation:40mg/mlpowdertobereconstitutedwithwater,or500mgtablet
Administration:orallyasasingledose20mg/kg(maximumdose1000mg)
Dose for weight chart
Weight Azithromycin dose
3kgto<6kg 80mg(2ml)a
6kgto<10kg 160mg(4ml)a
10kgto<15kg 240mg(6ml)a
15kgto<20kg 400mg(10ml)a
20kgto<30kg 500mg(1tablet)b
30kgto<40kg 750mg(1½tablets)b
over40kgadults 1000mg(2tablets)b
a200mg/5mlsuspensionb500mgtablet

DEPARTMENTOFHEALTHANDFAMILIES
19
Azithromycin for children <6 months of age and pregnant womenAzithromyciniscurrentlylicensedfortreatmentoftrachomaininfantsover12months.However,theNationalHealthandMedicalResearchCouncilrecommendsitsuseinallinfantsforthepreventionandtreatmentofpertussisandsuggestthatitistheantibioticofchoiceinthoseunderonemonthofage.1Thereforestaffshouldfeelcomfortablerecommendingazithromycintoinfants,butinfantsunder6monthsofageshouldbereviewedat1and4weeksaftertreatmentandreportanyadverseeffectstoTrachomaCoordinatoron89516902or89516906.2
Azithromycinmaybeusedinpregnancyandlactation.ItisacategoryB1drug-usedbyalimitednumberofpregnantwomenwithoutanyincreaseinharmfuleffectsonthefetus.
Side effectsWhile not frequent some people may experience side effects including: diarrhoea, nausea, orabdominalpain.Headache,shortnessofbreath,rashorcandidainfectioncanoccurrarely.
Interactions with other medicationsAzithromycincaninterferewiththeactivityofsomeotherimportantprescriptiondrugs.
Itisimportanttoinformthepersonprescribingyouazithromycinofanyothermedicationsyouaretaking.
Trachoma screeningInregionswheretrachomaisendemictheminimumtargetgroupfortrachomascreeningischildrenaged 5-9 years. Trachoma screening should be done annually in these communities. Wherepossibletrachomamanagementprogramsshouldbeconductedataregionallevel.
Screeningand treatmentatapopulation level is thebestmethod todecrease the incidenceoftrachoma.
FormoreinformationcontactyournearestCentreforDiseaseControl.
Darwin 89228044Katherine 89739049Nhulunbuy 89870359TennantCreek 89624259AliceSprings 89517540
References 1. NationalHealthandMedicalResearchCouncil.TheAustralianImmunisationHandbook,9thed,Canberra.
AustralianGovernment;2008.p.235-236.2. SchultzR,CoffeyC,KrauseV,TaylorH,CurrieB.Treatmentoftrachomainsmallbabies.NT Dis Control
Bull2007;14(4):22-23.
GuidelinesforTreatmentofTrachomaintheNorthernTerritory
20
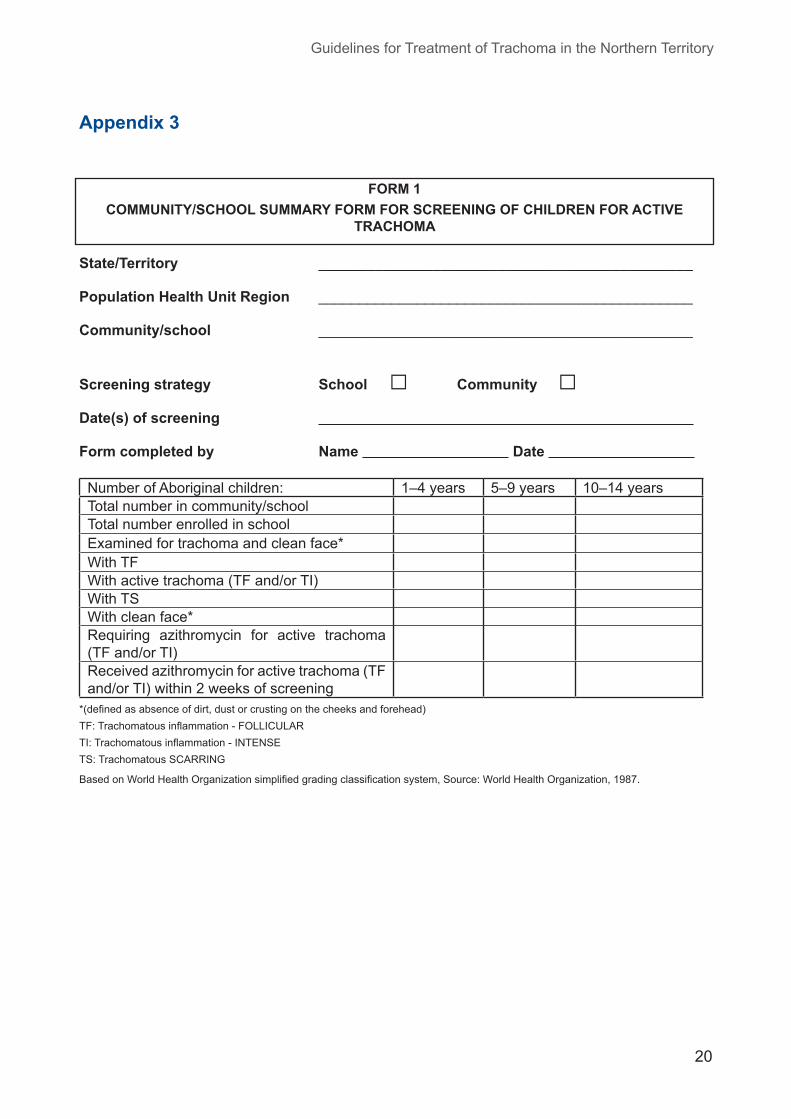
State/Territory ______________________________________________
Population Health Unit Region ______________________________________________
Community/school ______________________________________________
Screening strategy School □ Community □Date(s) of screening
Form completed by Name Date
NumberofAboriginalchildren: 1–4years 5–9years 10–14yearsTotalnumberincommunity/schoolTotalnumberenrolledinschoolExaminedfortrachomaandcleanface*WithTFWithactivetrachoma(TFand/orTI)WithTSWithcleanface*Requiring azithromycin for active trachoma(TFand/orTI)Receivedazithromycinforactivetrachoma(TFand/orTI)within2weeksofscreening
*(definedasabsenceofdirt,dustorcrustingonthecheeksandforehead)TF:Trachomatousinflammation-FOLLICULARTI:Trachomatousinflammation-INTENSETS:TrachomatousSCARRING
BasedonWorldHealthOrganizationsimplifiedgradingclassificationsystem,Source:WorldHealthOrganization,1987.
FORM 1COMMUNITY/SCHOOL SUMMARY FORM FOR SCREENING OF CHILDREN FOR ACTIVE
TRACHOMA
Appendix 3

DEPARTMENTOFHEALTHANDFAMILIES
21
State/Territory ______________________________________________
Population Health Unit Region ______________________________________________
Community/school ______________________________________________
Date(s) of screening ______________________________________________
Form completed by Name ______________________ Date______________
Date of first treatment ______________________________________________
TREATMENT STRATEGY (Tick 1 box only)The treatment strategies are based on CDNA guideline recommendations.(Tick one box only)
Prevalence≥10%inchildrenNOobviousclusteringinthecommunityTreatment strategy: Treat allAboriginal children in the community aged6
months-14 years and all household contacts aged 6monthsandover
Cases obviously clustered in several households in the communitiy and allhouseholdcontactsthatareeasilyidentifiedTreatment strategy: Treatallhouseholdcontactsaged6monthsandover
(communitywidetreatmentisnotrequired)
Prevalence<10%inchildrenPrevalence<10%but≥5%Treatment strategy: Treatallhouseholdcontactsaged6monthsandover
Prevalence<5%Treatment strategy: Treatallhouseholdcontactsaged6monthsandover
Numberofcontacts <1year
1-4years
5-9years
10-14years
15+years
RequiringtreatmentwithazithromycinTreated with azithromycin within 2 weeks of startingdistributionoftreatmentTotaltreatedwithazithromycin
Completion date of last treatment: / /
FORM 2COMMUNITY/SCHOOL SUMMARY FORM FOR TREATMENT OF HOUSEHOLD AND
COMMUNITY CONTACTS WITH AZITHROMYCIN
Appendix 4
GuidelinesforTreatmentofTrachomaintheNorthernTerritory
22
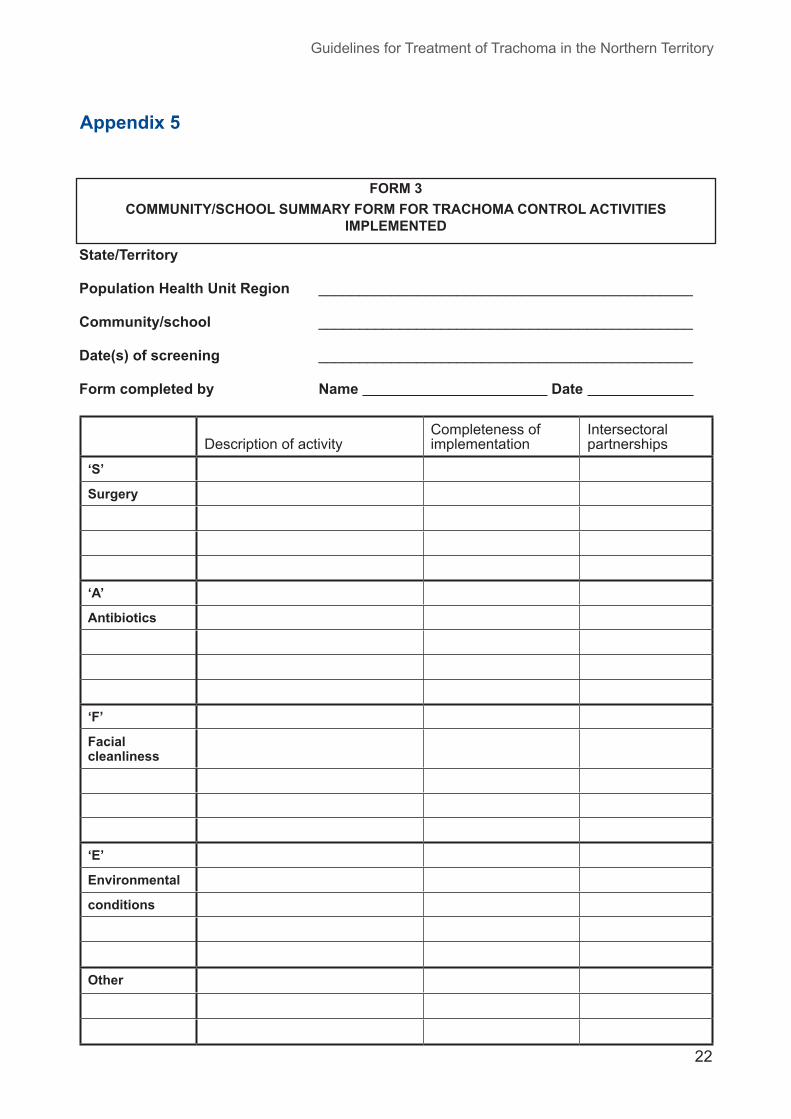
State/Territory
Population Health Unit Region ______________________________________________
Community/school ______________________________________________
Date(s) of screening ______________________________________________
Form completed by Name Date
DescriptionofactivityCompletenessofimplementation
Intersectoralpartnerships
‘S’
Surgery
‘A’
Antibiotics
‘F’
Facial cleanliness
‘E’
Environmental
conditions
Other
Appendix 5
FORM 3COMMUNITY/SCHOOL SUMMARY FORM FOR TRACHOMA CONTROL ACTIVITIES
IMPLEMENTED

DEPARTMENTOFHEALTHANDFAMILIES
23
State/Territory ______________________________________________
Population Health Unit Region ______________________________________________
Community ______________________________________________
Date(s) of screening ______________________________________________
Form completed by Name ______________________ Date______________
NumberofAboriginaladults: <40years 40-49years 50+years
male female male female male femaleExaminedfortrichiasisWithtrichiasisInthescreeningtargetgroup(ienumberofAboriginaladultsinthescreenedagegroupincommunities/townstargetedforscreening)Inthecommunity/schoolinthescreenedagegroup(fromcensusdata)Withtrichiasiswhowereofferedanophthalmologicalconsultationwithin6monthsofthepreviousscreening
<40years 40-49years 50+years
male female male female male femalePleasereportthenumberofAboriginaladultswhounderwenttrichiasissurgeryinthepreviousyear
Appendix 6
FORM 4COMMUNITY/SCHOOL SUMMARY FORM FOR TRICHIASIS IN ABORIGINAL ADULTS

GuidelinesforTreatmentofTrachomaintheNorthernTerritory
24
This form is based on the recommendations of the CDNA Guidelines. It is for community use only and will not be collected by the National Trachoma Surveillance & Reporting Unit (NTSRU). Using this form will aid in the compilation of the data for Forms 1 & 2 that will be collected by the NTRSU.
State ______________________________________________Population Health Unit Region ______________________________________________Community ______________________________________________
Screening strategy School □ Community □Date of screening / / Name(s) of staff doing trachoma screening ____________________
NumberofAboriginalandTorresStraitIslanderchildreninschool/communityaged1-4years_____NumberofAboriginalandTorresStraitIslanderchildreninschool/communityaged5-9years_____NumberofAboriginalandTorresStraitIslanderchildreninschool/communityaged10-14years_____
Please use this form as a record for your community screening.This form can also assist you in completing the information on the community summary forms.
Reye Leye Face Azithromycin
Name Age IndigenousY/N
Sex TF TI TS TF TI TS Clean/dirty
Dategiven
Notgiven
Notrequired
*Personalinformationiscollectedforcommunityuseonly
TF:Trachomatousinflammation-FOLLICULARTI:Trachomatousinflammation-INTENSETS:TrachomatousSCARRING
BasedonWorldHealthOrganizationsimplifiedgradingclassificationsystem,Source:WorldHealthOrganization,1987
Appendix 7
ANNEX 1INDIVIDUAL DATA COLLECTION FORM FOR ACTIVE TRACHOMA SCREENING
DEPARTMENTOFHEALTHANDFAMILIES
25
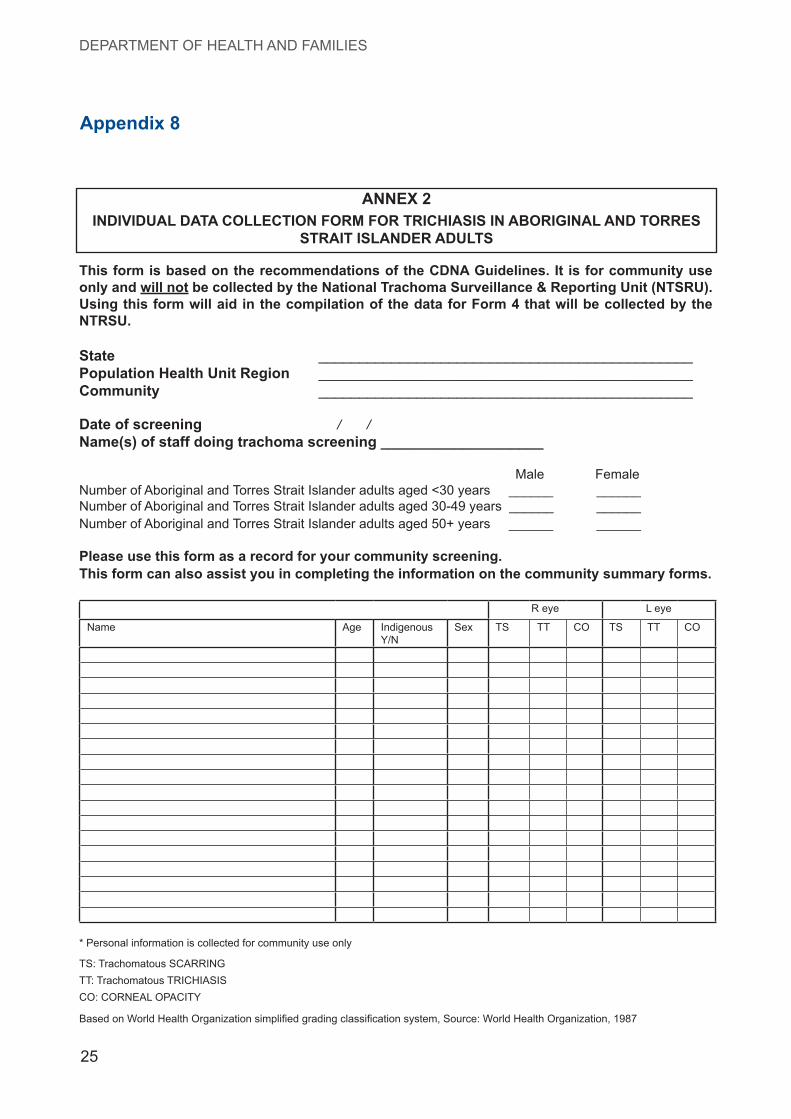
This form is based on the recommendations of the CDNA Guidelines. It is for community use only and will not be collected by the National Trachoma Surveillance & Reporting Unit (NTSRU). Using this form will aid in the compilation of the data for Form 4 that will be collected by the NTRSU.
State ______________________________________________Population Health Unit Region ______________________________________________Community ______________________________________________
Date of screening / / Name(s) of staff doing trachoma screening ____________________
Male FemaleNumberofAboriginalandTorresStraitIslanderadultsaged<30years______ ______NumberofAboriginalandTorresStraitIslanderadultsaged30-49years______ ______NumberofAboriginalandTorresStraitIslanderadultsaged50+years______ ______
Please use this form as a record for your community screening.This form can also assist you in completing the information on the community summary forms.
Reye Leye
Name Age IndigenousY/N
Sex TS TT CO TS TT CO
*Personalinformationiscollectedforcommunityuseonly
TS:TrachomatousSCARRINGTT:TrachomatousTRICHIASISCO:CORNEALOPACITY
BasedonWorldHealthOrganizationsimplifiedgradingclassificationsystem,Source:WorldHealthOrganization,1987
Appendix 8
ANNEX 2INDIVIDUAL DATA COLLECTION FORM FOR TRICHIASIS IN ABORIGINAL AND TORRES
STRAIT ISLANDER ADULTS

Guidelines for Treatment of Trachoma in the Northern Territory
26

Northern TerritoryGuidlines for Treatment of Trachoma 2008
Northern Territory Department of Health and Families
Centre for Disease Control
GPO Box 721Alice Springs NT 0871Telephone: (08) 8951 7540Facsimile: (08) 8951 7900Web: www.nt.gov.au/health

















