37
Haematemesis Lent 2007
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | helen-allen |
| View: | 213 times |
| Download: | 0 times |

Haematemesis
Lent 2007

The case: Mr J O’F
• 48 year old jockey (divorced, no recent wins).
• Presents at 2am with a big haematemesis
• Unable to give a history

On examination……• Shocked: b.p. 90/60, P120
• Short (5’5”); Thin arms and legs
• Spider naevi
• Pale yellow sclerae
• Veins visible coming out from the navel
• Liver palpable plus mass in LUQ
• Abdomen distended with shifting dullness
• Fetid breath

Spider naevus

Yellow scleri

Which way do the veins go?

What is the lump in the LUQ?

Why is the abdomen distended?

Why is the breath fetid and why is he vomiting blood?

Common causes of haematemesis• Peptic ulcer: gastric or duodenal
• Acute gastric erosions/gastritis
• Carcinoma of the stomach
• Mallory-Weiss syndrome
• Oesophageal varices

So what might be happening in our patient?
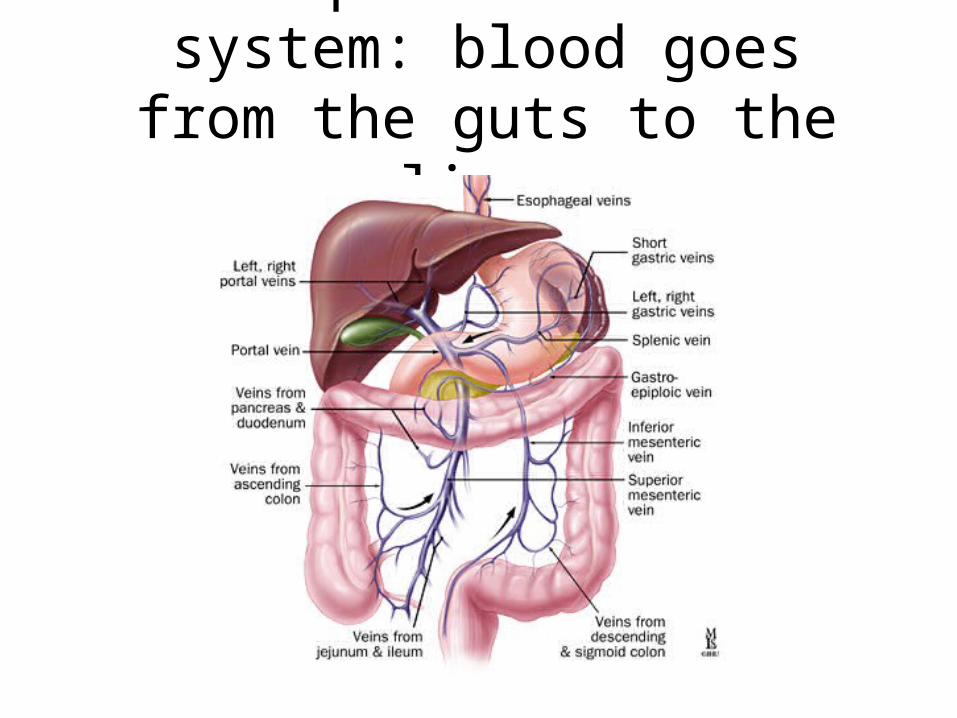
The portal venous system: blood goes from the guts to the liver
Hepatic portal vein pressure
Pressure = output (flow) x resistance, so..
pressure increases due to an increase in flow or resistance

What might cause an increase in resistance?

Increase in portal pressure:
• A blocked portal vein: thrombosis or tumour
• Liver disease: cirrhosis, tumour, infection (e.g schistosomiasis)

What would happen if the portal venous pressure increases?
(Portal hypertension)
In portal hypertension..
• Portal flow slows
• Vessels dilate due to back-pressure
• Flow may go elsewhere: anastomoses open up:
At the base of the oesophagus
At the umbilicus
At the haemorrhoidal plexus
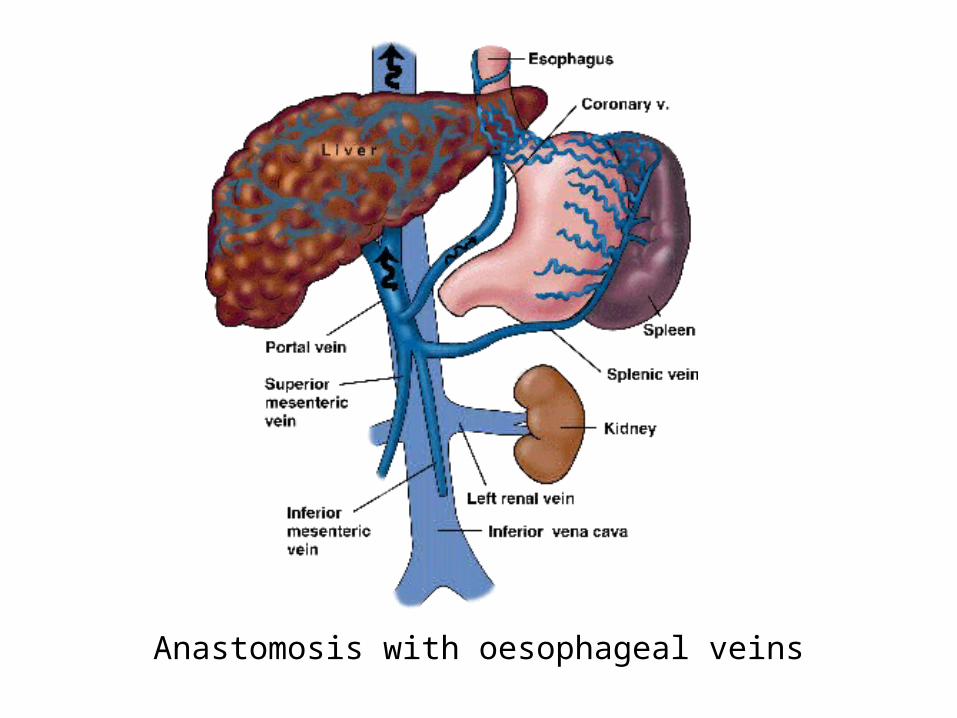
Anastomosis with oesophageal veins

What is the umbilicus?
Umbilicus: insertion site of umbilical cord: 2 arteries and one
vein


In adult life:
• The umbilical arteries- become the obliterated umbilical arteries in the medial umbilical ligaments
• The umbilical vein- becomes the ligamentum teres in the falciform ligament
THIS BECOMES PATENT IN PORTAL HYPERTENSION

The caput Medusa
And what causes ascites?

Ascites: fluid in the peritoneal cavity
• May be transudate due to increased portal pressure
• May be exudate of actively secreted fluid due to inflammation or tumour
• May be exacerbated by low protein levels due to poor liver function

So what has happened to to Mr J O’F?

The clinical picture suggests:
• Signs of portal hypertension
• Hepatosplenomegaly
• ascites
• Large haematemesis, probably from oesophageal varices
• Underlying cause?


How would you manage this case?

management
• Rescuscitaion
• Hb, X-match blood, U&Es, LFTs
clotting studies
• Investigation: endoscopy; imaging
• Treatment: stop the bleeding; address the underlying problem

endoscopy

Treatment of varices:
• Medical: IV vasopressin; octreotide
• Ligation; banding
• Sclerotherapy
• Balloon tamponade

banding

The Sengstaken-Blakemore tube
And the outcome?

Prognosis from bleeding varices
• Patients who have bled once from esophageal varices have a 70% chance of rebleeding
• Approximately one third of further bleeding episodes are fatal.
• Risk of death highest during the first few days after the bleeding episode and decreases slowly over the first 6 weeks.









![Gr-ale“Groove” - Nottingham CAMRA Gr-ale flyer[1].pdf · 2012-06-18 · Live music featured throughout the festival! PUB THURS FRI SAT SUN ForestTavern 8pm-11pm 9pm-2am 7pm-2am](https://static.documents.pub/doc/80x56/5e966058218379793b13f614/gr-aleaoegroovea-nottingham-gr-ale-flyer1pdf-2012-06-18-live-music-featured.jpg)







