Chapter 65 Regeneration of Epidermis from Adult Human Keratinocyte Stem Cells Ariane Rochat, Nicolas Grasset, Franc ¸ois Gorostidi, Ste ´phanie Lathion and Yann Barrandon Laboratory of Stem Cell Dynamics, School of Life Sciences, Ecole Polytechnique Fe´de´rale Lausanne and Department of Experimental Surgery, Lausanne University Hospital, 1015 e Lausanne, Switzerland Chapter Outline Introduction 768 Keratinocyte Stem Cells of the Skin 768 Clonogenic Keratinocytes with Different Capacities for Multiplication 769 Clonal Conversion 770 Stem Cell Therapy 771 Transplantation of Keratinocyte Stem Cells in Extensive Burn Wounds 772 Regeneration of Epidermis 774 Clinical Indications of Keratinocyte Stem Cells 775 Future Development 776 Economic Value 776 Conclusion 777 Acknowledgments 777 References 777 Keratinocyte stem cells together with hematopoietic stem cells have the longest record in cell therapy. Howard Green and colleagues pioneered stem cell therapy of the skin in the early 1980s, and gene therapy of hereditary disabling skin diseases using genetically corrected kera- tinocyte stem cells has recently become a reality. Since Terminology Clonal conversion. Conversion of a holoclone to a mer- oclone or to a paraclone irreversible under normal condi- tions; affected by culture conditions and age. Holoclone. (Gk holos whole þ Gk kloˆn growing) Colony- forming cell with tremendous growth potential (up to 180 divisions), whose progeny forms almost exclusively growing colonies. Meroclone. (Gk mero part þ Gk kloˆn growing) Colony- forming cell whose growth potential is lower than the growth potential of an holoclone but superior to 15 divisions; forms growing and aborted colonies. Paraclone. (Gk para akin þ Gk klo ˆn growing) Colony- forming cell committed to a maximum of 15 divisions; forms only aborted colonies. Green and colleagues’ seminal publication in 1984, thousands of extensively burned patients have been transplanted worldwide with cultured autologous kerati- nocyte stem cells. The emergency situation of extensive third degree burn wounds necessitates a massive ex vivo expansion of autologous keratinocyte stem cells that must be achieved in the shortest time possible from a small skin biopsy. Successful stem cell engraftment has permitted the lives of many patients to be saved by permanently reconstituting a functional epidermal barrier. Neverthe- less, many challenges remain. Stem cell engraftment is variable for unknown reasons; the functionality and the aesthetic appearance of the regenerated skin must improve, possibly through the use of composite grafts associating dermal and keratinocyte stem cells. Sweat glands and hair follicles must also be regenerated and the pigmentation of the skin controlled. It is thus essential to thoroughly comprehend the cellular and molecular mechanisms involved in skin morphogenesis and fetal wound healing, in epidermal renewal and dermal remod- eling. In parallel, it is crucial to master costs to make keratinocyte stem cell-based products more affordable. Only then will stem cell therapy become a major thera- peutic option in dermatology and reconstructive surgery. Handbook of Stem Cells, Two-Volume Set. DOI: http://dx.doi.org/10.1016/B978-0-12-385942-6.00065-2 Copyright Ó 2013 Elsevier Inc. All rights reserved. 767
Transcript
Chapter 65
Regeneration of Epidermis from AdultHuman Keratinocyte Stem Cells
Ariane Rochat, Nicolas Grasset, Francois Gorostidi, Stephanie Lathion and Yann BarrandonLaboratory of Stem Cell Dynamics, School of Life Sciences, Ecole Polytechnique Federale Lausanne and Department of Experimental Surgery,
Lausanne University Hospital, 1015 e Lausanne, Switzerland
Ha
Co
Chapter Outline
Introduction 768
Keratinocyte Stem Cells of the Skin 768
Clonogenic Keratinocytes with Different Capacities
for Multiplication 769
Clonal Conversion 770
Stem Cell Therapy 771
Transplantation of Keratinocyte Stem Cells in
Extensive Burn Wounds 772
Terminology
Clonal conversion. Conversion of a holoclone to a mer-
oclone or to a paraclone irreversible under normal condi-
forming cell with tremendous growth potential (up to 180
divisions), whose progeny forms almost exclusively growing
colonies.
Meroclone. (Gk mero part þ Gk klon growing) Colony-
forming cell whose growth potential is lower than the growth
potential of an holoclone but superior to 15 divisions; forms
growing and aborted colonies.
Paraclone. (Gk para akin þ Gk klon growing) Colony-
forming cell committed to a maximum of 15 divisions; forms
only aborted colonies.
ndbook of Stem Cells, Two-Volume Set. DOI: http://dx.doi.org/10.1016/B978-0-12-385942-6.00
pyright � 2013 Elsevier Inc. All rights reserved.
Regeneration of Epidermis 774
Clinical Indications of Keratinocyte Stem Cells 775
Future Development 776
Economic Value 776
Conclusion 777
Acknowledgments 777
References 777
glands and hair follicles must also be regenerated and thepigmentation of the skin controlled. It is thus essential to
Keratinocyte stem cells together with hematopoietic stemcells have the longest record in cell therapy. HowardGreen and colleagues pioneered stem cell therapy of theskin in the early 1980s, and gene therapy of hereditarydisabling skin diseases using genetically corrected kera-tinocyte stem cells has recently become a reality. Since
Green and colleagues’ seminal publication in 1984,thousands of extensively burned patients have beentransplanted worldwide with cultured autologous kerati-nocyte stem cells. The emergency situation of extensivethird degree burn wounds necessitates a massive ex vivoexpansion of autologous keratinocyte stem cells that mustbe achieved in the shortest time possible from a small skinbiopsy. Successful stem cell engraftment has permitted thelives of many patients to be saved by permanentlyreconstituting a functional epidermal barrier. Neverthe-less, many challenges remain. Stem cell engraftment isvariable for unknown reasons; the functionality and theaesthetic appearance of the regenerated skin mustimprove, possibly through the use of composite graftsassociating dermal and keratinocyte stem cells. Sweat
thoroughly comprehend the cellular and molecularmechanisms involved in skin morphogenesis and fetalwound healing, in epidermal renewal and dermal remod-eling. In parallel, it is crucial to master costs to makekeratinocyte stem cell-based products more affordable.Only then will stem cell therapy become a major thera-peutic option in dermatology and reconstructive surgery.
Skin is a complex organ whose main function is to protectthe body from environmental hazards. The skin of verte-brates is covered with scales, feathers or hairs that contributeto protection, tactile sensation, thermoregulation, and cam-ouflage. Furthermore, skin participates in body homeostasis,for instance through water balance in the frog or vitamin Dsynthesis in the human. Most importantly, the appearance ofthe skin shapes emotional and social attitudes. In humans, itis best illustrated by the social impact of skin diseases or badscarring (hypertrophic scars, keloids) and the plethora ofadvertisements for beautiful skin and eternal youth, somecosmetics even claiming efficacy via stem cells.
Skin of an adult human represents about 16% of thebody weight and measures 1.7 m2. It is composed of threelayers that are, from the skin surface: the epidermis, thedermis, and the subcutis. The epidermis is a stratified,keratinized and self-renewing squamous epithelium incontinuity with the skin appendages, i.e. the hair follicles,the sebaceous glands, and the sweat glands (Figure 65.1).The epidermis contains several specialized cell typesthat all contribute to body protection. Keratinocytes ofectodermal origin represent 90% of the epidermal cellsand are responsible for renewal, cohesion, and barrierfunction of the epidermis. Melanocytes of neural crestorigin are pigment-producing cells responsible for UVprotection and the color of skin, whereas neuroepithelialMerkel cells are involved in signal transduction, andLangerhans and epidermal T cells of hematopoieticorigin in immunological defense. The epidermis receivesits nutrients from the highly vascularized dermis,a connective tissue that contains fibroblasts producingproteoglycans, collagen, and elastic fibers. The dermis isresponsible for the mechanical properties of the skin and is
FIGURE 65.1 Depth of burns. First-degree burns heal spontaneously
without a scar; second-degree burns heal with a scar. Third-degree burns
do not heal and may necessitate the transplantation of autologous split-
thickness skin grafts and autologous cultured keratinocyte stem cells
depending on the extent of the burns.
separated from the epidermis and the epidermal append-ages by a complex basement membrane. The subcutismainly contains adipocytes (fat cells) and is involved inthermoregulation and lipid storage. The skin is also highlyinnervated with numerous free nerve endings in theepidermis and specialized nerves endings in the dermis.Altogether, skin contains more than twenty-five speciali-zed cell types originating from at least six different stemcells (Brouard and Barrandon, 2003). Most importantly,the skin is constantly remodeled. In humans, the epidermisis renewed on average every 3 weeks and scalp hairfollicles undergo cycles of growth, regression and restabout twenty-five times in a lifetime. Similarly, the dermisconstantly remodels and produces new collagen fibers toreplace old fibers.
KERATINOCYTE STEM CELLSOF THE SKIN
Several stem cells with differing functions are includedunder the generic term of keratinocyte stem cells. Strictlyspeaking, they are all tissue stem cells that self-renew(Lajtha, 1979) and generate keratinocytes, i.e. keratin-containing epithelial cells that will ultimately terminallydifferentiate to form the squamous layers of the stratifiedepithelium. Keratinocyte stem cells are present in skin,the ocular surface (conjunctiva and cornea), the oral cavity,the esophagus, the vagina and anal canal. In skin, cumu-lative evidence demonstrates that unipotent (single-lineage) and multipotent (multiple-lineage) keratinocytestem cells coexist (Gambardella and Barrandon, 2003;Blanpain and Fuchs, 2009). Unipotent keratinocyte stemcells reside in the basal layer of epidermis (Barrandon andGreen, 1987), whereas multipotent stem cells are located inhair follicles (Oshima et al., 2001; Blanpain and Fuchs,2009) and sweat glands (our unpublished observations).In the mouse, multipotent keratinocyte stem cells arelocated in the upper constant region of hair follicles, i.e. inthe bulge region and its vicinity (Jaks et al., 2010). They areidentified as label retaining cells (LRC) (Taylor et al., 2000)or by the expression of different cell surface markers(e.g. CD34, Lgr5, Lgr6, Lrig1 and MTS24) (Jaks et al.,2010). In human epidermis, keratinocyte stem cells arethought to express high levels of b1 and a6 integrin and lowlevels of CD71 (transferrin receptor) when analyzed byflow cytometry (Jones and Watt, 1993; Tani et al., 2000),but it is still impossible to identify a stem cell on a histo-logical section of epidermis. In human epidermal append-ages, multipotent stem cells are located in the upper regionof the hair follicle below the sebaceous glands (Rochatet al., 1994) and in sweat glands and sweat ducts(our unpublished results). Most importantly, multipotentstem cells can migrate out of hair follicles or sweat glands
769Chapter | 65 Regeneration of Epidermis from Adult Human Keratinocyte Stem Cells
to adopt an epidermal fate to repair a wounded epidermis(Al-Barwari and Potten, 1976; Argyris, 1976; Claudinotet al., 2005; Blanpain and Fuchs, 2009). If we betterunderstand the cell hierarchy and the signaling pathwaysinvolved in epidermal and hair follicle homeostasis in themouse (Watt, 2001; Watt et al., 2008; Blanpain and Fuchs,2009), a lot remains to be learned in the human. Lineagetracing experiments in the mouse have clearly demon-strated that a stem cell only renews a tiny portion ofepidermis (Ghazizadeh and Taichman, 2001; Clayton et al.,2007; Doupe et al., 2010), suggesting that billions of stemcells are necessary to renew 1.7 m2 of human epidermis.Most importantly, human keratinocyte stem cells have theremarkable ability to extensively proliferate and self-renewin cell culture (Rheinwald and Green, 1975; Barrandon andGreen, 1987; Rochat et al., 1994; Pellegrini et al., 1998).This unique property is at the origin of stem cell therapy inskin (O’Connor et al., 1981; Gallico et al., 1984). Whencultured under appropriate conditions, e.g. onto a feederlayer of lethally irradiated mouse 3T3-J2 cells as describedby Rheinwald and Green (1975), keratinocyte stem cellsdivide on average every 16 to 20 hours and form progres-sively growing colonies that can be serially subculturedfor many weeks. Colonies will ultimately fuse to forma confluent stratified epithelium that can be detached fromthe culture vessel and transplanted. When the culturesystem of Rheinwald and Green is used at its best, it ispossible to isolate enough keratinocyte stem cells froma small skin biopsy to generate vast amounts of differen-tiated keratinocytes for long periods of time. As anexample, our laboratory routinely uses a strain of humandiploid keratinocytes (YF29) isolated more than 25 yearsago from the foreskin of a newborn.
FIGURE 65.2 Clonogenic keratinocytes with different capacities for
multiplication. A single cell is isolated with a Pasteur pipette and culti-
vated onto a feeder layer of irradiated 3T3-J2 cells. If a clone forms, it is
subcultured while in exponential growth. The number and shape of
colonies on the indicator dishes determine the clonal type of the founding
cell. The progeny of a holoclone generates large, progressively growing
colonies; the progeny of a meroclone generates a mixture of large,
progressively growing colonies and aborted colonies; and that of a para-
clone generates only aborted colonies or no colony. The proportion of
young skin mostly contains holoclones and meroclones, and old skin
contains mainly meroclones and paraclones.
Clonogenic Keratinocytes with DifferentCapacities for Multiplication
The growth potential of human multiplying keratinocytes isbest evaluated by clonal analysis, which can be performedwith cells freshly isolated from skin or with culturedcells (Barrandon and Green, 1987). It is best to choosea cell-friendly cloning technique to minimize cell stressand avoid fluorescent activated cell sorting that greatlydiminishes cloning efficiency. In our hands, isolation ofindividual single cells under direct vision remains the mostgentle and efficient technique. A single cell experimenttypically includes the isolation and culture of 100e200individual cells, yielding 30e120 clones depending on thestarting material (biopsy or culture) (Barrandon and Green,1985, 1987). Briefly, each single cell is isolated with anelongated Pasteur pipette under a dissecting microscopebefore it is carefully deposited at the center of a Petri dishcontaining lethally irradiated 3T3-J2 cells (the size of the
culture vessel can vary from a 96-well plate to a 175 cm2
flask). After 7 days of culture, each dish is carefullysearched for the presence of a clone under an invertedmicroscope. Each clone is then enzymatically dissociatedto obtain a single cell suspension, which is inoculated intoseveral indicator dishes (usually 2� 100-mm size Petridishes) containing lethally irradiated 3T3-J2 cells. After 12days of cultivation, cultures are fixed and stained withRhodamine B before they are examined under a dissectingmicroscope (Figure 65.2). Three types of colonies areeasily distinguished:
1. Growing colonies that are large and round witha smooth perimeter and that mostly contain small cells.These colonies can be subcultured many times and areformed by keratinocytes with significant growthpotential.
2. Aborted colonies that are small with an irregular shapeand that contain large, flattened differentiated squame-like cells. These colonies cannot be subcultured and areformed by cells with restricted growth potential.
3. Mixed colonies with a jagged perimeter that containareas of intermingled small and large differentiatedcells. These colonies can only be subcultured a limited
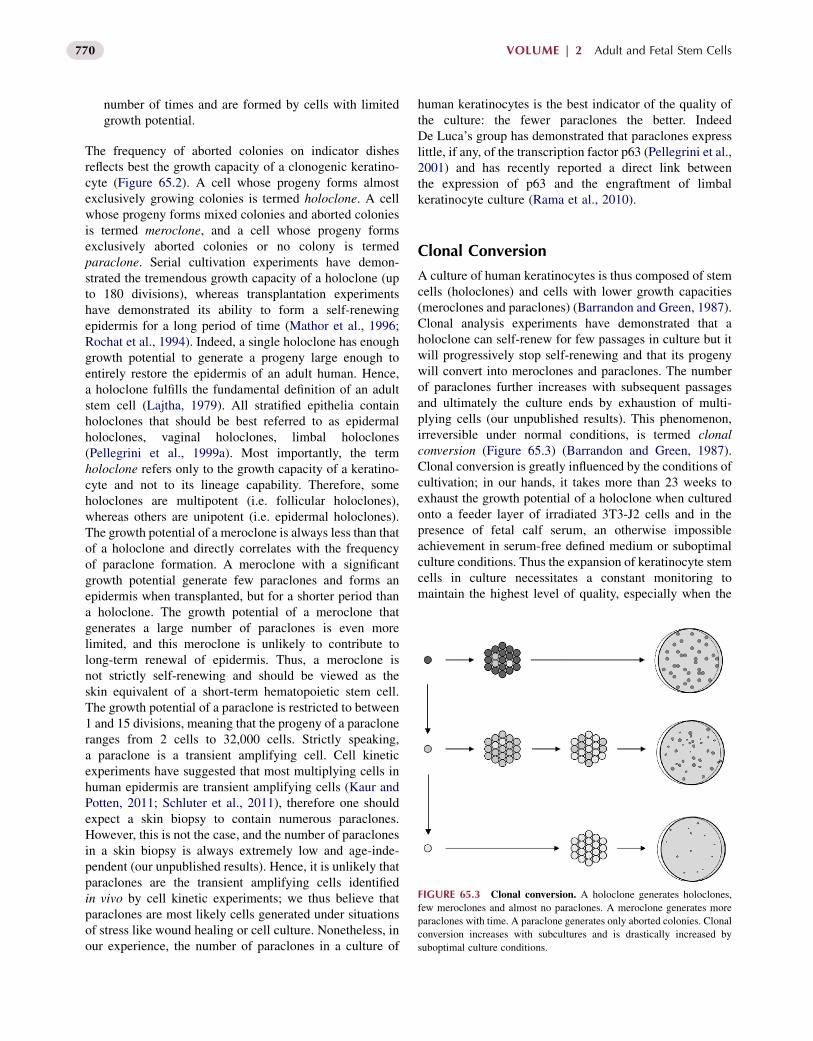
FIGURE 65.3 Clonal conversion. A holoclone generates holoclones,
few meroclones and almost no paraclones. A meroclone generates more
paraclones with time. A paraclone generates only aborted colonies. Clonal
conversion increases with subcultures and is drastically increased by
suboptimal culture conditions.
770 VOLUME | 2 Adult and Fetal Stem Cells
number of times and are formed by cells with limitedgrowth potential.
The frequency of aborted colonies on indicator dishesreflects best the growth capacity of a clonogenic keratino-cyte (Figure 65.2). A cell whose progeny forms almostexclusively growing colonies is termed holoclone. A cellwhose progeny forms mixed colonies and aborted coloniesis termed meroclone, and a cell whose progeny formsexclusively aborted colonies or no colony is termedparaclone. Serial cultivation experiments have demon-strated the tremendous growth capacity of a holoclone (upto 180 divisions), whereas transplantation experimentshave demonstrated its ability to form a self-renewingepidermis for a long period of time (Mathor et al., 1996;Rochat et al., 1994). Indeed, a single holoclone has enoughgrowth potential to generate a progeny large enough toentirely restore the epidermis of an adult human. Hence,a holoclone fulfills the fundamental definition of an adultstem cell (Lajtha, 1979). All stratified epithelia containholoclones that should be best referred to as epidermalholoclones, vaginal holoclones, limbal holoclones(Pellegrini et al., 1999a). Most importantly, the termholoclone refers only to the growth capacity of a keratino-cyte and not to its lineage capability. Therefore, someholoclones are multipotent (i.e. follicular holoclones),whereas others are unipotent (i.e. epidermal holoclones).The growth potential of a meroclone is always less than thatof a holoclone and directly correlates with the frequencyof paraclone formation. A meroclone with a significantgrowth potential generate few paraclones and forms anepidermis when transplanted, but for a shorter period thana holoclone. The growth potential of a meroclone thatgenerates a large number of paraclones is even morelimited, and this meroclone is unlikely to contribute tolong-term renewal of epidermis. Thus, a meroclone isnot strictly self-renewing and should be viewed as theskin equivalent of a short-term hematopoietic stem cell.The growth potential of a paraclone is restricted to between1 and 15 divisions, meaning that the progeny of a paracloneranges from 2 cells to 32,000 cells. Strictly speaking,a paraclone is a transient amplifying cell. Cell kineticexperiments have suggested that most multiplying cells inhuman epidermis are transient amplifying cells (Kaur andPotten, 2011; Schluter et al., 2011), therefore one shouldexpect a skin biopsy to contain numerous paraclones.However, this is not the case, and the number of paraclonesin a skin biopsy is always extremely low and age-inde-pendent (our unpublished results). Hence, it is unlikely thatparaclones are the transient amplifying cells identifiedin vivo by cell kinetic experiments; we thus believe thatparaclones are most likely cells generated under situationsof stress like wound healing or cell culture. Nonetheless, inour experience, the number of paraclones in a culture of
human keratinocytes is the best indicator of the quality ofthe culture: the fewer paraclones the better. IndeedDe Luca’s group has demonstrated that paraclones expresslittle, if any, of the transcription factor p63 (Pellegrini et al.,2001) and has recently reported a direct link betweenthe expression of p63 and the engraftment of limbalkeratinocyte culture (Rama et al., 2010).
Clonal Conversion
A culture of human keratinocytes is thus composed of stemcells (holoclones) and cells with lower growth capacities(meroclones and paraclones) (Barrandon and Green, 1987).Clonal analysis experiments have demonstrated that aholoclone can self-renew for few passages in culture but itwill progressively stop self-renewing and that its progenywill convert into meroclones and paraclones. The numberof paraclones further increases with subsequent passagesand ultimately the culture ends by exhaustion of multi-plying cells (our unpublished results). This phenomenon,irreversible under normal conditions, is termed clonalconversion (Figure 65.3) (Barrandon and Green, 1987).Clonal conversion is greatly influenced by the conditions ofcultivation; in our hands, it takes more than 23 weeks toexhaust the growth potential of a holoclone when culturedonto a feeder layer of irradiated 3T3-J2 cells and in thepresence of fetal calf serum, an otherwise impossibleachievement in serum-free defined medium or suboptimalculture conditions. Thus the expansion of keratinocyte stemcells in culture necessitates a constant monitoring tomaintain the highest level of quality, especially when the
771Chapter | 65 Regeneration of Epidermis from Adult Human Keratinocyte Stem Cells
cells are aimed for cell therapy. A parameter that impactsclonal conversion is the age of the donor. As stated earlier,the number of paraclones in the primary culture initiatedfrom the skin biopsy is age-independent but it becomesstrongly age-dependent when the cells are subcultured(Barrandon and Green, 1987; Pellegrini et al., 1998).Indeed, subcultures from old donors contain many moreparaclones than those of young donors and consequentlycannot be maintained for as long. Hence, the formation ofparaclones reflects an age-related phenomenon that cangreatly impact the cultivation strategy for cell therapy.Indeed, clonal conversion can adversely affect engraft-ment (“take”) of cultured epithelium autografts and thelong-term renewal of the generated epithelium (Ramaet al., 2010).
STEM CELL THERAPY
In 1975, Rheinwald and Green reported in a seminal paperthe cultivation of human keratinocytes using a feeder layerof lethally irradiated mouse Swiss 3T3-J2 cells and envi-sioned a potential application for the treatment of extensiveskin defects (Rheinwald and Green, 1975). It took 8 moreyears of intensive work before Green and colleaguessuccessfully transplanted cultured autologous keratinocytesonto a human (O’Connor et al., 1981; Gallico et al., 1984).This period was paved with several landmarks, includinguse of the enzyme dispase to detach the cultured epitheliumas a transplantable homogenous sheet (Green et al., 1979)and the demonstration that cultured human keratinocytescan generate an epidermis when transplanted onto athymicmice (Banks-Schlegel and Green, 1980). Since then, thetechnology has been used worldwide to treat thousands ofextensively burned patients (Gallico et al., 1984; Kumagaiet al., 1988; De Luca et al., 1989; Munster et al., 1990;Teepe et al., 1990; De Luca et al., 1992; Haith et al., 1992;Rue et al., 1993; Hickerson et al., 1994; Meuli andRaghunath, 1997; Paddle-Ledinek et al., 1997; Pellegriniet al., 1999b; Carsin et al., 2000; Ronfard et al., 2000;Oshima et al., 2002; Chester et al., 2004; De Luca et al.,2006; Hernon et al., 2006; Wood et al., 2006a,b; Sood et al.,2009, 2010; Cirodde et al., 2011). Green’s method tocultivate transplantable keratinocytes is extremely efficientand it is possible to initiate cultures from tiny skin biopsies,individual hair follicles and even from a single keratinocytestem cell (Barrandon and Green, 1985, 1987; Rochat et al.,1994) but it is critical to properly monitor culture condi-tions. This is best accomplished by using reference strainsof human keratinocytes, the growth characteristics of whichare well known. Indeed, we systematically test lots ofserum, supplements, or growth factors in a colony-formingassay using a reference strain to determine to what extentthe ratio of growing colonies (stem cells and close progeny)to aborted colonies (paraclones) is affected. We believe that
the culture of keratinocyte stem cells necessitates a strictadherence to instructions and that fiddling with protocols inan uncontrolled manner rarely results in improving theperformance of the culture but rather results in deleteriousconsequences, like enhanced clonal conversion, rapidexhaustion of stem cells, and failure of engraftment. Forinstance, 3T3-J2 cells are best grown in the presence ofbovine serum, and switching to fetal bovine serum isa common mistake with damaging consequences on thequality of the feeder cells. The use of a feeder layer oflethally irradiated mouse Swiss 3T3-J2 cells and serumremains a requirement for successful keratinocyte stem celltherapy (Rheinwald and Green, 1975) and to our knowl-edge, no clinical success has been obtained with cellsgrown in defined medium or other conditions. Neverthe-less, the use of cells of animal origin (xenotransplantation)can theoretically induce adverse reactions and transmitpathogens, though the risk is significantly minimized if oneuses 3T3-J2 cells originating from a master bank that testednegative for a battery of pathogens according to regulatoryaffairs guidelines. Animal serum, widely used in thebiotechnology industry, is also a potential hazard throughthe induction of adverse reactions to foreign proteins andthe transmission of pathogens. Again, the risk is minimal ifone purchases lots of serum with traceable origin for whichthe manufacturer maintains a master file in accordance withregulatory affairs guidelines. It is worth emphasizing thatno adverse reaction to 3T3-J2 cells and serum has beenreported in the thousands of patients treated with kerati-nocyte stem cells cultivated according to Rheinwald andGreen.
The conventional method to prepare transplantablekeratinocyte cultures for the treatment of extensive thirddegree burns has been reported in great detail (Gallicoet al., 1984; Pellegrini et al., 1999b; Ronfard et al., 2000).Briefly, a full-thickness skin biopsy is obtained aseptically,stored in culture medium and transferred to the laboratorywhere it is minced with scissors and treated with trypsinto obtain a single-cell suspension. Cells are then seededat a density of 2.4� 104 cells/cm2 onto a feeder layer oflethally irradiated 3T3-J2 cells (60 Gy) in mediumcontaining fetal bovine serum and supplemented withcholera toxin, hydrocortisone, insulin, and triiodothyronineaccording to published protocols (Ronfard et al., 2000).Cultures are supplemented with recombinant humanepidermal growth factor (10 ng/mL) starting at the firstmedium change. Under these conditions, clonogenic kera-tinocytes divide on average every 16 to 20 hours,and colonies quickly expand and push away the irradiatedfeeder cells, which will detach from the culture vessel.The method of cultivation selects for clonogenic keratino-cytes but some melanocytes and dermal fibroblasts canalso adhere and multiply, although at a much lower ratethan keratinocytes. Primary cultures are usually
772 VOLUME | 2 Adult and Fetal Stem Cells
subcultured while in exponential growth before confluenceor after 9 days of cultivation, whichever comes first.If primary cultures yield enough cells, cultures for trans-plantation are then initiated at a seeding density of1.2� 104 cells/cm2 and the leftover cells are frozen forfuture use. If the primary cultures do not yield enough cells,it is necessary to further expand the cell population bysetting up secondary cultures at a seeding density of1.2� 103 cells/cm2. Cells are then cultivated for no morethan a week before they are used to set up cultures fortransplantation. Under optimal conditions, a 10,000-foldexpansion is obtained within 2 to 3 weeks (Gallico et al.,1984; Pellegrini et al., 1999b; Ronfard et al., 2000).For transplantation, confluent cultured epithelia are thentreated with dispase (Green et al., 1979) or thermolysin(Germain et al., 1993) that detach the epithelium asa coherent cell sheet from the bottom of the culture vesselsand result in a significant shrinkage of the epithelium. Oncerinsed with medium, each epithelial graft is carefullymounted and clipped onto a petroleum gauze, special carebeing taken to maintain the correct polarity of the epithe-lium (i.e. the basal layer facing away from the gauze).This step of the procedure is delicate, cumbersome, tediousand demanding in manpower, especially when hundreds ofcultured epidermal grafts must be rapidly prepared. This iswhy many groups have explored alternative methods toculture keratinocytes using detachable matrices that can bearmed with various growth factors. These matrices includehuman fibrin (Ronfard et al., 1991; Kaiser et al., 1994;Zisch et al., 2001; Lorentz et al., 2011), bovine or humancollagen (Hansbrough et al., 1989; Shahabeddin et al.,1990), hyaluronic acid (Myers et al., 1997), shark proteo-glycans (Yannas et al., 1989), and various polymers(Hansbrough et al., 1993; Meana et al., 1997; Yamato et al.,2002; Nishida et al., 2004; Kumashiro et al., 2010).However, it should be emphasized that it is critical tothoroughly evaluate the effects of these matrices on kera-tinocyte stem cell fate before implementing them in a celltherapy protocol, since suboptimal culture conditions resultin enhanced clonal conversion, reduced keratinocytelifespan, and irreversible degradation of the quality of thegraft. We and other groups have demonstrated that a fibrinmatrix alleviates the need for detachment of the culturedepithelium, eliminates shrinkage and greatly facilitateskeratinocyte stem cell transplantation (Pellegrini et al.,1999b; Ronfard et al., 2000; Llames et al., 2006). Mostimportantly, a fibrin matrix considerably shortens theculture process and it is possible to generate enoughcultured epithelium autografts (CEA) to transplant theentire body of a burned adult as soon as 15 days after injury(Ronfard et al., 2000). The transplantation of small coloniesof keratinocytes (preconfluent culture) grown on a fibrinmatrix or of individual keratinocytes suspended in fibringels has been proposed (Horch et al., 1998). It may be
useful to quickly transplant small full-thickness burns or toenhance healing of superficial burn wounds. However, itremains to be demonstrated that individual cells or smallcolonies directly exposed to the hostile environment of aninflammatory grafting bed can generate an epidermalbarrier faster than a confluent and organized culture. Fibrinmatrices are also extremely useful to transplant limbalkeratinocyte stem cells to restore corneal defects (Ramaet al., 2001). Composite grafts combining autologouskeratinocytes and fibroblasts embedded in a collagen gel,a fibrin matrix, or in polymers can be useful to generatea closer-to-normal skin by enhancing the formation ofdermis (Boyce and Warden, 2002). However, it is difficultby today’s cell culture technology to obtain enough dermalfibroblasts from a small skin biopsy within the 2e3 weekperiod compatible with the transplantation of large acuteburn wounds. To alleviate this problem, several groupshave proposed the use of allogeneic dermal fibroblasts,large stocks of which can be prepared in advance. However,allogeneic fibroblasts do not permanently engraft (Briscoeet al., 1999). To our knowledge, composite autografts thatassociate autologous fibroblasts and autologous keratino-cytes are mainly used to treat small skin defects or chronicwounds, e.g., leg ulcers (Limat and Hunziker, 2002). It ishoped that progress will be made in the cultivation ofhuman fibroblasts, which will then give composite trans-plants a significant advantage.
Transplantation of Keratinocyte Stem Cellsin Extensive Burn Wounds
Burn wounds of the skin result in a rupture of the cuta-neous barrier that can have serious consequences such asloss of proteins and body fluids, infection, and death(Figure 65.1). Moreover, chronic wounds favor improperscarring and the development of skin cancers (Owens andWatt, 2003; Perez-Losada and Balmain, 2003). A first-degree burn wound affects only the epidermis and healsspontaneously without scarring; the reconstitution ofepidermal integrity results from the migration and theproliferation of keratinocytes originating from the nearbyepidermis or appendages. A second-degree burn wound,defined as superficial or deep depending on its depth,destroys the epidermis and part of the dermis. It can healspontaneously by migration of cells originating fromappendage remnants, but a permanent scar will form.A third-degree burn destroys the entire thickness of theskin (full-thickness burn). Although a tiny third-degreeburn wound can possibly heal by migration of cells fromthe surrounding unwounded skin, a large third-degree burnwound will not. The transplantation of split-thicknessautografts harvested from unburned donor sites is then theunique therapeutic option, with an added risk of infection
773Chapter | 65 Regeneration of Epidermis from Adult Human Keratinocyte Stem Cells
and improper healing of the donor sites (hypertrophicscars and keloids). Moreover, the recurrent cropping ofdonor sites can become a serious problem, especially forpatients burned over 60% of the total body surface area(TBSA). Progress in medical resuscitation and intensivecare allows patients whose skin has been almostcompletely burned to remain alive. These patients do nothave enough donor skin for conventional split-thicknessautografts and then the transplantation of autologouskeratinocyte stem cells can become life-saving (Green,1991). The transplantation of cultured keratinocyte stemcells necessitates a highly trained surgical and nursingstaff. Various surgical procedures have been developedover the years to transplant cultured epithelium autografts.CEAwere initially transplanted directly on the granulationtissue that spontaneously forms after full-thickness burnswere excised to fascia (Gallico et al., 1984). Success wasvariable, ranging from poor to excellent, and surgeonsquickly stressed that the quality of the wound bed wascrucial. In that regard, the most appreciated procedure isCuono’s method in which full-thickness burns are exciseddown to living (bleeding) tissues and temporarily covered
(A) (B)
(D) (E)
(G) (H)
FIGURE 65.4 Transplantation of human cultured epithelium autografts
degree burns. (A) Admission. (B) Excision to fascia of full-thickness thorac
temporarily covered with meshed split-thickness human cadaver allografts.
control cultured epithelia (top) and cultured epithelia grown on fibrin matrices
(G) Appearance of the same area 21 days later. Note the excellent take of both
was taken from the opposite side to that shown in panel E). (H and I) Appear
with permission from Ronfard et al. (2000).
with meshed, expanded fresh or cryopreserved split-thickness human allografts obtained from a skin bank(Cuono et al., 1986). Skin substitutes like Integra� orBiobrane� are useful alternatives to cadaver skin when thelatter is not available or cannot be used for religiousreasons. At the time of transplantation of CEA, whichusually occurs 2 to 3 weeks after the biopsy for expansionof keratinocyte stem cells is obtained, cadaver allograftsare dermabraded or tangentially excised with carefulhemostasis. CEA are then gently applied with the basalcell layer oriented toward the grafting bed. Grafts are thencovered with petroleum gauze dressings to preventdesiccation (Figure 65.4). Special care must be taken atthis step of the procedure not to damage the fragileepithelium, by avoiding sliding and displacement of thegrafts. CEA are then overlaid with bridal veil gauze,sterile dry compresses and elastic bandage (Carsin et al.,2000). Engraftment is evaluated empirically at the timeof the first dressing (“take-down”), the engrafted epithe-lium looking shiny and translucent. With time, theregenerated epithelium matures to resemble a normalepidermis (Figure 65.4 and Figure 65.5) and engraftment
(C)
(F)
(I)
. A 35-year-old woman burned by flames over 50% of her body has third-
ic and abdominal burn wounds the day after injury. (C) The excised area
(D) Appearance of the dermabraded grafting bed. (E) transplantation of
(bottom); (F) Appearance of the transplanted area 8 days later (take-down).
control (bottom) and experimental (top) cultured epithelia (the photograph
ance of same area 57 days and 4 months after transplantation. Reproduced
(A) (B)
(E) (F)
(C) (D)
FIGURE 65.5 Long term follow-up of
cultured epithelia transplanted on a fibrin
matrix. A 9-year-old boy burned by flames over
95% of his body has third-degree burns. (A) Day
of admission at Percy Burn Center a month after
injury. (B) Transplantation of cultured epithelia,
grown on a fibrin matrix, on the left arm.
(C) Appearance of the transplanted area at take-
down. (D and E) Aspect of the area transplanted
with CEA 3.5 years later. The skin is elastic when
pinched and has a smoother appearance than
the neighboring split-thickness skin autografts.
(F) Histology of the transplanted area 3.5 years
after transplantation. The epidermis is histologi-
cally normal. Note the presence of rete ridges and
a superficial neodermis with vascular arcades.
Similar results were obtained with cultured
epithelia grown in absence of fibrin. Bar: 100 mm.
Reproduced with permission from Ronfard et al.
(2000).
774 VOLUME | 2 Adult and Fetal Stem Cells
becomes easier to assess. The Cuono’s procedure hasgreatly increased the rate of CEA engraftment (“take”):successful engraftment can average 70% of the trans-planted area, and it is not unusual to obtain a 100%take (Pellegrini et al., 1999b; Carsin et al., 2000; Ronfardet al., 2000; Cirodde et al., 2011). Nevertheless, it is fair tosay that engraftment can be poor and even null. Infectionof the grafting bed is the enemy of CEA and provokesa rapid loss of the grafts. Systemic antibiotherapy andlocal antiseptics are usually used to fight infection, and itis worth noting that local antiseptics with alleged stemcell toxicity in vitro can be clinically efficient and notharmful in vivo (Carsin et al., 2000; Sood et al., 2010).Engraftment has also been associated with the age of thepatient e the younger the better e possibly reflecting stemcell aging (Barrandon and Green, 1987; Carsin et al.,2000; De Luca et al., 2006; Green, 2008). CEA performbest in areas in which shear forces or frictions are minimaland in non-weight-bearing surfaces. Fragility andblistering of CEA are commonly observed during the firstweeks following transplantation, most likely a conse-quence of a delayed maturation of the anchoring fibrilsthat anchor the regenerated epidermis onto the neodermis(Woodley et al., 1988; Compton et al., 1989). Bleeding ofthe grafting bed can also result in loss of CEA, further
emphasizing the importance of thorough hemostasis atthe time of grafting. In addition, lysis of CEA-generatedepidermis is sometimes observed a few weeks aftertransplantation, for unexplained reasons. Anothercomplication of CEA is epidermal hyperkeratosis, whichmay need repeated treatment with moisturizing and ker-atolytic ointments (Carsin et al., 2000). Wound contrac-ture can also be a problem, as observed in patients withextensive deep burns, but it seems that there is lesshypertrophic scarring with CEA than with conventionalsplit-thickness autografts (Carsin et al., 2000).
Regeneration of Epidermis
A cultured epithelium prepared according to Green andcolleagues is pluristratified but lacks the cornified layersindispensable for proper barrier function. However, the fullprogram of differentiation rapidly resumes after trans-plantation and proper cornified layers are normallyobserved within a week (Compton et al., 1989; Ronfardet al., 2000). Melanocytes are often observed in the basallayer of the regenerated epidermis although at a variabledensity, and the presence of Merkel cells has been reported(Compton et al., 1990). Furthermore, Langerhans cells ofhematopoietic origin rapidly invade the regenerated
775Chapter | 65 Regeneration of Epidermis from Adult Human Keratinocyte Stem Cells
epidermis. Rete ridges, vascular arcades, and elastic fibersare also observed after a few months. The formation ofa neodermis that closely resembles the papillary dermis(Figure 65.5) is certainly slow but it is unique to the graftand not observed during normal wound healing of deepwounds (Brouard and Barrandon, 2003; Compton et al.,1989; Ronfard et al., 2000). This observation stronglysuggests that dermal stem cells have been transplantedalong with the keratinocyte stem cells and that epithelio-mesenchymal interactions reminiscent of fetal woundhealing have occurred, though this hypothesis awaitsconfirmation. Most importantly, hair follicles and sweatglands are not regenerated, with consequence for thequality of life of the patients. There are several explanationsfor the non-regeneration of epidermal appendages:
1. multipotent keratinocyte stem cells are absent in adulthuman skin,
2. current culture conditions favor the epidermal lineage,and
3. the inductive signals necessary for appendagemorphogenesis are missing.
However, we and other groups have unambiguouslydemonstrated that the skin of adult mammals containsmultipotent keratinocyte stem cells with the capacity togenerate epidermis, sebaceous glands, and hair folliclesand that these stem cells can be cultured according toRheinwald and Green (Oshima et al., 2001; Blanpain et al.,2004; Claudinot et al., 2005). Therefore, the most plausibleexplanation is a lack of morphogenetic signals. Interest-ingly, it has been demonstrated that dermal papilla cellsobtained from adult human hair follicles have inductivecapacities (Reynolds et al., 1999; Driskell et al., 2011),opening the door to the regeneration of epidermalappendages.
Clinical data indicates long-term maintenance of theepidermis generated from CEA, even if there is a short-ening of telomeres in keratinocytes obtained from trans-planted patients (Counter et al., 2003). The expansion oftransplantable keratinocyte stem cells in culture represents22e23 cell doublings at the most, a small number whencompared with the overall growth potential of keratinocyte
FIGURE 65.6 Presence of holoclones in the regenerated epidermis. A b
plantation, cut in equal parts. One part was processed for histology (see Figure
and cultured as described (Barrandon and Green, 1987). Clonal analysis dem
stem cells (180 doublings). This means that transplantablekeratinocyte stem cells have plenty of growth potential leftto renew the regenerated epidermis for years (Figure 65.6).Moreover, clonal conversion affects a cell lifespan inde-pendently of the mitotic clock and the shortening of telo-meres, a difference expressed as culture shock (Sherr andDePinho, 2000). Collectively, these observations furtheremphasize that the culture of tissue stem cells aimed attherapy should be performed according to the state-of-the-art technology to minimize stress.
Clinical Indications of KeratinocyteStem Cells
Clinical indications of CEA have been extensivelyreviewed (De Luca et al., 2006; Pellegrini et al., 1998).Full-thickness burns over 60% of TBSA (total body surfacearea) remain the main indication for CEA, which haveoften been beneficial and lifesaving. CEA have also beenproposed to enhance healing of donor sites, to preventrecurrence of keloids, to cover excised giant congenitalnevi and tattoos, and during removal of basal cell carci-noma (Mohs surgery). Besides their indication in derma-tology and plastic surgery, CEA can also be indicated inurology and oral surgery, but the most impressive use ofCEA is in the treatment of corneal defects. Pellegrini andcolleagues have beautifully demonstrated that limbal ker-atinocyte stem cells (limbal holoclones) can be cultured ona fibrin matrix and transplanted onto the ocular surface torestore the integrity of the corneal epithelium (Rama et al.,2001). This approach together with elective keratoplastyhas permitted the restoration of vision in patients whosesight was greatly impaired because of corneal burn wounds(Pellegrini et al., 1997; Rama et al., 2001). Gene therapy ofhereditary disabling diseases of skin and cornea can alsobenefit from CEA. Indeed, keratinocyte stem cells of theskin or ocular surface can be successfully transduced bydefective retroviral or lentiviral vectors and engineered toexpress a protein of medical interest (Morgan et al., 1987;Mathor et al., 1996; Chen et al., 2002). For instance, thesuccessful transduction of keratinocyte stem cells isolatedfrom patients suffering from junctional or dystrophic
iopsy was obtained from the transplanted area 3.5 years after CEA trans-
65.5F), while the other one was dissociated to isolate single cells isolated
onstrated that the regenerated epidermis contained holoclones.
776 VOLUME | 2 Adult and Fetal Stem Cells
epidermolysis bullosa and xeroderma pigmentosum opensnew therapeutic avenues (Dellambra et al., 1998; Chenet al., 2002; Ortiz-Urda et al., 2002; Titeux et al., 2010;Warrick et al., 2011). Mavilio and De Luca’s groups havemade a breakthrough demonstrating the feasibility of exvivo gene therapy (Mavilio et al., 2006). The authors useda retroviral strategy to stably transduce a LAMB3 cDNAencoding laminin 5003Fb3-chain into cultured keratino-cyte stem cells (holoclones) of a patient with a rare form ofjunctional epidermolysis bullosa (JEB), a devastating skindisease characterized by skin fragility, chronic blistering,painful wounds, and the emergence of carcinomas.Genetically corrected LAMB3 CEA were then producedand transplanted to restore epidermal integrity. Masteringthe culture and transplantation of keratinocyte stem cellswas assuredly important for success, as De Luca’s grouphas thorough experience in cell therapy of burns (Pellegriniet al., 1999b) or corneal defects (Pellegrini et al., 1997).In addition, the choice to transplant chronic nonhealingwounds largely depleted in resident stem cells was criticalbecause it favored the genetically corrected stem cells overdiseased stem cells that could have otherwise migrated outof skin appendages. Importantly, the areas treated withgenetically corrected stem cells have remained healedfor years (De Luca, personal communication), unambigu-ously demonstrating stem cell engraftment.
Despite the fact that extensive third-degree burns donot heal spontaneously and that the transplantation ofautologous cultivated keratinocytes has contributed tosaving the life of thousands of patients worldwide (Green,2008), some have questioned the origin of the healing cellsin large burns, suggesting that stem cells other thanepidermal, e.g., hematopoietic stem cells, were respon-sible for the reconstitution of epidermis. Mavilio andcolleagues’ gene therapy data, together with our datademonstrating that the cultured progeny of a single kera-tinocyte multipotent stem cell of the rat can reconstitutehair follicles and sebaceous glands for years in serialtransplantation (Claudinot et al., 2005), should definitelyclose the discussion on whether keratinocyte stemness ismaintained in culture. Another important finding ofMavilio and colleagues is that only a small number ofrecombinant keratinocyte stem cells are necessary toreconstruct an epidermis. This opens the door to thetransplantation of a genetically homogenous CEAproduced from a single transduced holoclone, in whichone can demonstrate safe integration of the recombinantprovirus. This, together with the use of a self-inactivatingshuttle vector, should further contribute to safe epidermalgene therapy (Barrandon, 2007). Though repairing theentire epidermis of an adult human by gene therapyremains a dream, the treatment of elective areas withgenetically corrected CEA, e.g., the hands in dystrophicepidermolysis bullosa patients, is certainly an option to
enhance the quality of life of patients suffering fromdisabling hereditary skin diseases.
Future Development
A promising development is the derivation of keratino-cytes from embryonic stem cells (ES), the feasibility ofwhich has been demonstrated in mouse and human byseveral groups (Coraux et al., 2003; Iuchi et al., 2006;Aberdam et al., 2007; Medawar et al., 2008; Guenou et al.,2009). Another exciting development is the derivation ofinduced pluripotent stem cells (iPS) from adult humankeratinocytes (Aasen et al., 2008), which, in combinationwith the isolation of keratinocytes from a small skinbiopsy or even a plug hair, is a powerful means ofobtaining customized iPS cell lines. However humanES- or iPS-derived keratinocytes do not seem to recapit-ulate fully the properties expected from adult keratinocytestem cells, which currently limit their interest for celltherapy. Further research to improve the culture and thetransplantation of adult keratinocyte stem cells is stillneeded, especially the development of an efficient feeder-free, serum-free culture method. It is also critical tounderstand why the engraftment of CEA is variable;however it is difficult to address the basic cellular andmolecular mechanisms controlling stem cell fate inhumans, for obvious ethical reasons, hence the necessityof a large-animal model.
Economic Value
Niche market, customized manufacturing, and highproduction costs have made it difficult for CEA tobecome a blockbuster product. For example, Epicel�,a commercial CEA is considered a Humanitarian Deviceby the FDA (www.genzyme.com) and it costs about 26US$ per cm2 (including biopsy kit, culture, and ship-ping), which prices the transplantation of a square meterof CEA at 260,000 US$. Even if the cost must becompared with that of other transplantation procedures, itremains a strong limiting factor. Personalized skin stemcell therapy is not cheap and will certainly not getcheaper, knowing that CEA are custom made in anemergency situation. Similarly, one can expect compositeCEA (mixing autologous fibroblasts and keratinocytes) tobe more expensive as they are more complex to manu-facture. Decreasing cost is certainly a challenge, but thereare routes to explore. For instance, CEA cultured ontoa fibrin matrix permits the coverage of a body surfacetwice as large as conventional CEA because of theabsence of epithelium shrinkage. Moreover they are user-friendly and easier to handle in the producing laboratoryand in the operating room.
777Chapter | 65 Regeneration of Epidermis from Adult Human Keratinocyte Stem Cells
CONCLUSION
The main challenge in ex vivo skin cell therapy is to obtaina massive expansion of the stem cells from a small skinbiopsy in the shortest time possible while preservingstemness. The culture method described by Rheinwaldand Green achieves this goal and has not been matched.Cell therapy using autologous keratinocyte stem cellscultured according to the preceding method has saved thelives of thousands of burned patients, has restored sight tovision-impaired patients, and has opened the door to exvivo gene therapy. Yet, the technology relies on a feederlayer of irradiated mouse cells and is therefore considereda xenotransplantation by regulatory affairs, which addsa significant burden to an already cumbersome approvalprocess. For this reason, one must improve the culture ofkeratinocyte stem cells (and also that of skin dermal stemcells), as well as improve and reconstruct hair follicles andsweat glands. Moreover, it is critical to improve themechanical properties and the aesthetic appearance of theregenerated skin. The answer to these challenges residesin a better understanding of the cellular and molecularevents involved in skin renewal and morphogenesis, ina better understanding of fetal and adult wound healing. Inthis regard, human embryonic stem cell lines or iPS mightbe helpful. It is also of paramount importance to studystem cell engraftment in relevant animal models, e.g., inthe pig, the skin biology of which is closer to human thanis that of rodents. In conclusion, future progress in stemcell therapy of the skin necessitates
1. continuous gains in scientific knowledge to improvestem cell engraftment and transplant functionality,
2. the development of a culture technology that meetsregulatory requirements without affecting stemness,and
3. a thorough evaluation of the economical constraint,because it can clearly affect the commercial develop-ment of skin cell therapy (Bouchie, 2002).
ACKNOWLEDGMENTS
The Ecole Polytechnique Federale Lausanne (EPFL), the Lausanne
University Hospital (CHUV), the EEC (EuroSyStem and OptiStem),
and La Fondation Enfants Papillons supported this work.
REFERENCES
Aasen, T., Raya, A., Barrero, M.J., Garreta, E., Consiglio, A.,
Gonzalez, F., et al., 2008. Efficient and rapid generation of induced
pluripotent stem cells from human keratinocytes. Nat. Biotechnol. 26,
1276e1284.
Aberdam, D., Gambaro, K., Rostagno, P., Aberdam, E., de la Forest
Divonne, S., Rouleau, M., 2007. Key role of p63 in BMP-4-induced
epidermal commitment of embryonic stem cells. Cell Cycle 6,
291e294.
Al-Barwari, S.E., Potten, C.S., 1976. Regeneration and dose-response
characteristics of irradiated mouse dorsal epidermal cells. Int. J.