ISSUE 44 JAN 2017 A Risk Management Newsleer for Hospital Authority Healthcare Professionals RISK ALERT Risk Mitigation Strategy Surgical Instrument / Material Removal i n this issue Risk Mitigation Strategy Surgical instrument / material removal Sentinel Events (SEs) (Q3 2016) Retained instruments / material Inpatient suicide Gas embolism Serious Untoward Events (SUEs) (Q3 2016) Global Sharing Withdrawing insulin from pen devices Local Sharing Specimen container with NEW security seal Surgeon is responsible for confirming that the drain is not caught by sutures before the whole wound is closed and dressed. A simple way is to shiſt the drain a lile bit. This will also ensure smooth removal of drain in due course. Dr K Y PANG, HKEC Dep SD (Q&S) / PYNNEU Cons Surgeon’s Advice on Drain Management Check for completeness of surgical instrument / material upon removal Perform imaging if there are doubts of retained fragment / segment of the removed item Document details of removed surgical instrument / material
Transcript
ISSUE 44 JAN 2017A Risk Management Newsletter for Hospital Authority Healthcare Professionals
RISK ALERT
Risk Mitigation StrategySurgical Instrument / Material Removal
in this issueRisk Mitigation StrategySurgical instrument / material removalSentinel Events (SEs) (Q3 2016) Retained instruments / material Inpatient suicideGas embolism
Serious Untoward Events (SUEs) (Q3 2016)Global SharingWithdrawing insulin from pen devicesLocal SharingSpecimen container with NEW security seal
Surgeon is responsible for confirming that the drain is not caught by sutures before the whole wound is closed and dressed. A simple way is to shift the drain a little bit. This will also ensure smooth removal of drain in due course.
Dr K Y PANG,HKEC Dep SD (Q&S) / PYNNEU Cons
Surgeon’s Advice on Drain Management
Check for completeness of surgical instrument / material upon removal
Perform imaging if there are doubts of retained fragment / segment of the removed item
Document details of removed surgical instrument / material
SENTINEL EVENTS
Distribution of SUE in the last four quartersDistribution of SE in the last four quarters
Asymmetry of medical knowledge between doctors and patients: incidents are no exemption
During the insertion of a chest catheter into the pleural cavity of a young patient with empyema, the catheter broke and part of it was retained. The complication was noted immediately and managed properly. Healthcare professionals understand that the above incident is a known complication and not a “sentinel event”. However, despite repeated explanation, the parents were still enraged and decided to disclose the incident to the press. It is generally appreciated that when it comes to medical knowledge, there is a big gap between healthcare professionals and patients. Patients need our adequate explanation and guidance to understand a diagnosis and make informed decisions on disease management. The same holds true for medical incidents. Nonetheless, when there is an adverse event or adverse outcome, communication often becomes harder as patients and their families are likely to have less trust and more skepticism about their doctor or treatment rendered. For “complications” where there is no error on our part, like the incident described above, the healthcare team may not feel the need or be adequately prepared to explain the incident in detail. Consequently, misunderstanding occurs more readily. We should keep in mind that asymmetry of medical knowledge applies to incidents as well. Hence, to avoid being misunderstood, we need to be more alert in our communication with the patients or their families after an incident, even though the incident is not due to error of our practice.
Dr Tony MAKService Director (Quality & Safety), Kowloon West Cluster
A guide wireDoctor A inserted a central venous catheter (CVC) in the operating theatre under the supervision of Doctor B.Doctor B was distracted by patient’s changing condition.Resistance was encountered during blood aspiration and flushing the main CVC lumen.No counting of guide wire was performed at the end of procedure. Doctor B and nurses assumed the guide wire was removed by Doctor A. Doctor B documented “guide wire removed intact” in the computer system.The retained guide wire was discovered on post-operative chest X-ray.The guide wire was removed under fluoroscopic guidance.
Contributing factors:1. Non-compliance with CVC insertion guideline on guide wire removal.2. Unclear role and accountability of staff on CVC insertion procedure.
Recommendations:1. Reinforce strict compliance with CVC insertion guideline.2. Define clearly the role and responsibility of staff on CVC insertion procedure.3. Check the removal of guide wire timely and sign on the checklist by designated staff.
Q3 2016
2 3
Always count the used guide wire before ending the procedure.
Please make use of the Procedure Safety Checklist.
OthersCoil wire fragments A patient underwent LEFT hip arthroplasty for osteoarthritis (OA) hip.While inserting the second screw, surgeon discovered that the detachable flexible drill shaft was bent.Nurse checked the instrument and suspected the outer coil wire of the drill shaft was broken. However, both surgeon and staff from supplier believed that the drill shaft was structurally intact.Surgeon performed a visual inspection of surgical field but could not find any broken fragment.Surgeon decided not to do X-ray examination due to concern of infection risk.There was no written documentation on the broken detachable flexible drill shaft in the operation record.
Contributing factors:1. No explicit procedure to confirm retention of any broken part of instrument during intraoperative period.2. Low awareness on potential risk of broken instrument.
Recommendations:1. Formulate a standard procedure on performing intraoperative imaging for all suspected broken instruments. 2. Delineate the roles and responsibilities of team members in managing broken instrument during intraoperative period.3. Remind orthopaedic surgeons to reinforce the practice of examining broken instruments with due diligence instead of only performing visual checking on surgical field.
In Q3 2016, a total of 3 inpatients (2 male and 1 female aged between 19 and 96) committed suicide.
Among them, two had psychiatric illness and 1 was recently diagnosed of cancer.
All 3 patients committed suicide whilst on home leave. One jumped from height, one ingested some insecticide and one stabbed himself.
Post-operative X-ray revealed 3 pieces of coil wire fragments in patient’s proximal femur.
Normal drill shaft
Bent drill shaft
Distribution of inpatient suicidecases in the last four quarters
6home leave
4inpatient
2missing
Q3 2016
4 5
Retained Instruments / Material
The RCA panel members acknowledged the following:1. The healthcare team providing ECMO care was appropriately trained. 2. Department guidelines for circuit priming and crisis management of ECMO therapy were being followed. 3. Changing the venous and arterial cannulae and circuit during crisis management of ECMO therapy in a totally ECMO-dependent patient was a difficult and major decision.
4. Timely incident reporting and quarantine of involved equipment / instrument / consumable should be enforced to enable subsequent investigation.
Gas bubbles were noted in extracorporeal membrane oxygenation (ECMO) circuitPatient was admitted to Cardiac Care Unit (CCU) for severe acute myocardial infarction (AMI).In cardiac catheterisation laboratory, patient had cardiac arrest and was resuscitated. ECMO support was initiated.Percutaneous coronary intervention (PCI) revealed LEFT main artery stenosis. Three drug-eluting stents were inserted.In Intensive Care Unit (ICU), there were 3 episodes of low ECMO flow with line chattering. The healthcare team repeatedly conducted systematic checking to look for possible causes.After being supported by ECMO for 3 hours, patient developed hypotension. Drop in ECMO flow was noted. Doctor suspected pump failure and switched to hand-cranking. Gas bubbles were noted in the ECMO system. The venous and arterial cannulae were clamped immediately. Patient’s condition was managed as a case of gas embolism crisis. New ECMO system was set up with new venous and arterial cannulae inserted. The ECMO flow resumed satisfactory afterwards. However, patient’s condition deteriorated and patient was certified death the same day.
Gas Embolism
Recommendations on critical points of operation:
1. Staff should be vigilant on and respond swiftly to patient’s changing condition.
2. Simulation training and sharing should be conducted to enhance staff awareness in recognising and managing both air in ECMO circuit and air embolism in ECMO patient.
3. Staff training on ECMO circuit priming should be reinforced. Competency of individual nurses on ECMO circuit priming should be assessed before they were allowed for independent practice.
SERIOUS UNTOWARD EVENTS
6 7
Of the 16 SUE cases reported in Q3 2016, 15 were medication error and 1 was patient misidentification. The medication error cases involved giving known drug allergen to patients (3), dangerous drug (2), insulin (4), inotrope (1), general anaesthetic agent (1) and others (4).
Of the 3 known drug allergen cases, 1 developed mild symptoms which subsided after treatment. The other two cases had no allergic reaction.
Medication Error
3
7
31
1
3
2
1
13
1
1
5
Q4 2015 Q1 2016 Q2 2016 Q3 2016
penicillin NSAID paracetamol others
Number of known drug allergen cases
From 2014-16, of the 11 reported known drug allergen cases related to Ketorolac (Toradol®), 3 (27%) had developed anaphylaxis and 1 (9%) had respiratory failure requiring intubation.
Ketorolac is a non-steroidal anti-inflammatory drug (NSAID)A patient with known history of NSAID allergy attended Accident and Emergency Department for abdominal pain.Intramuscular injection of Ketorolac was prescribed and administered.Patient developed severe anaphylaxis with respiratory distress requiring intubation and ICU admission.
GENERIC NAME: KetorolacBRAND NAME: Toradol®
Ketorolac is a NSAID
Colchicine was prescribed for prolonged duration A 75-year-old patient had history of chronic kidney disease and gout. Short duration of colchicine was prescribed for acute gouty attack as an inpatient treatment.Three days later, patient’s condition improved. Colchicine was discontinued.While prescribing discharge medication, doctor inadvertently prescribed colchicine 0.5mg twice daily for 32 days. Patient took the medications as instructed.One month later, patient was admitted for viral gastroenteritis and was found to have symptoms and signs of colchicine toxicity (myopathy, renal impairment and liver impairment).
Case highlight 1
Case highlight 2
Colchicine has a narrow therapeutic window and is extremely toxic if overdosed. Patients at particular risk of toxicity are those with renal or hepatic impairment, gastrointestinal or cardiac disease, and patients at extremes of age.
Drug Safety Update Nov 2009, vol 3 issue 4:5
6 7
GLOBAL SHARING
Withdrawing Insulin from Pen DevicesHon. Assoc. Prof. William CHUI, HKWC CSC(PHAR)
Patient Safety Alert issued by NHS Improvement on 16 Nov 2016
“… If insulin extracted from a pen or cartridge is of higher strength, and that is not considered in determining the volume required, it can lead to a significant and potentially fatal overdose….”
“… extracting insulin from pen devices or cartridges is dangerous and should not happen. Organizations should ensure staff are trained and competent in using insulin pens ... Staff, … should be routinely provided with safety needles and access to equipment capable of safely removing and disposing of used insulin pen needles...”
Reference: NHS Improvement Patient Safety Alert - Risk of severe harm and death due to withdrawing insulin from pen devices
Current Situation in HA Hospitals:Insulin syringe (U-100) may be used to draw insulin from insulin penfill cartridge or pen device.Pen needle may not be available in all wards for insulin pen device.Pen needle may be removed from insulin pen device using artery forceps.Risk of recapping & needle stick injury may not be well recognised.
Specialty Advisory Group (Endocrinology) had recommended the good practice of insulin administration by pen device as follows:
Insulin coming in pen device must be administered with the original pen needle. Patients should be encouraged to administer insulin pen device by themselves as far as possible.When using insulin pen device, nurses should use safety device together with the pen device to prevent needle stick injury.
EDITORIAL BOARDEditor-in-Chief: Dr N C SIN, CM(PS&RM), HAHO
Board Members: Dr K Y PANG, Dep SD(Q&S), HKEC; Dr Osburga P K CHAN, SD(Q&S), KCC; Dr Petty LEE, P(CPO), HAHO;Mr Fred CHAN, SM(PS&RM), HAHO; Dr Venus SIU, SM(PS&RM), HAHO; Dr C M LAM, M(PS&RM), HAHO;
Ms Katherine PANG, M(PS&RM), HAHOAdvisor: Dr Lawrence LAI, HOQ&S Honorary Senior Advisor
Suggestions or feedback are most welcome. Please email us through HA intranet at address: HO Patient Safety & Risk Management
Specimen Container with NEW Security SealAlthough painstaking as some may describe - root cause analysis (RCA) is necessary in incident management. The prime objective of RCA is to exhaustively identify all possible loopholes that may give rise to an incident. Rational avoidance of calculated risks is the hallmark of learning entity.
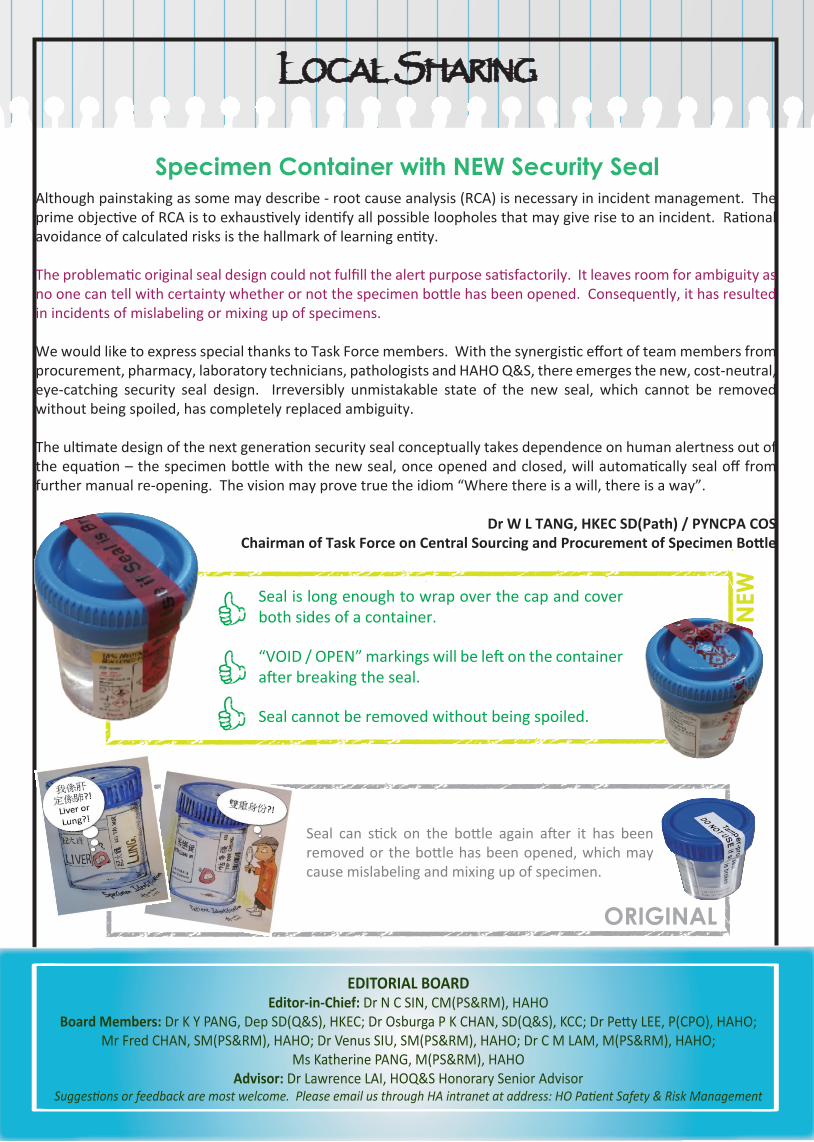
The problematic original seal design could not fulfill the alert purpose satisfactorily. It leaves room for ambiguity as no one can tell with certainty whether or not the specimen bottle has been opened. Consequently, it has resulted in incidents of mislabeling or mixing up of specimens. We would like to express special thanks to Task Force members. With the synergistic effort of team members from procurement, pharmacy, laboratory technicians, pathologists and HAHO Q&S, there emerges the new, cost-neutral, eye-catching security seal design. Irreversibly unmistakable state of the new seal, which cannot be removed without being spoiled, has completely replaced ambiguity.
The ultimate design of the next generation security seal conceptually takes dependence on human alertness out of the equation – the specimen bottle with the new seal, once opened and closed, will automatically seal off from further manual re-opening. The vision may prove true the idiom “Where there is a will, there is a way”.
Dr W L TANG, HKEC SD(Path) / PYNCPA COSChairman of Task Force on Central Sourcing and Procurement of Specimen Bottle
Seal is long enough to wrap over the cap and cover both sides of a container.
“VOID / OPEN” markings will be left on the container after breaking the seal.
Seal cannot be removed without being spoiled.
Seal can stick on the bottle again after it has been removed or the bottle has been opened, which may cause mislabeling and mixing up of specimen.