33
Harm Reduction in Action: Understanding and Applying Harm Reduction Practices and Principles Maryland Rehabilitation Conference 2021 Laura Bartolomei-Hill, LCSW-C
Harm Reduction in Action: Understanding and Applying Harm Reduction
Practices and PrinciplesMaryland Rehabilitation Conference 2021
Laura Bartolomei-Hill, LCSW-C
About me• Social Worker in Baltimore City - combination of outpatient
services, substance use services, harm reduction outreach, and emergency department assessments
• Trainer/consultant on the Behavioral Health Administration’s brain injury partnership grant
• On the advisory board of the Baltimore Harm Reduction Coalition
• Personal history of brain injury and outpatient TBI treatment
2
Objectives
• Make connections between harm reduction, opioids, overdose, and brain injury
• Contextualize cultural attitudes around drug use
• Introduce harm reduction tools and strategies
• Participate in small group discussions and debrief
3

Getting on the same pageDefinitions

Opioid Overdose • A negative health event directly caused by taking too great an amount
of an opioid or opioids, alone or in combination with other
substances.
• Opioids can suppress breathe.
• Suppressed respiration can lead to to unconsciousness, coma, brain
injury, and death
• Surviving an overdose depends on restoring respiratory function and
getting enough oxygen (naloxone, rescue breathing)5
Overdose During the PandemicDrug-related deaths were increasing before the pandemic. The pandemic has complicated the response and likely contributed to a worsening crisis. Overdose deaths increased by over 15% in 2020 over 2019.• Disruptions in in-person treatment, Narcotics Anonymous /Alcoholics
Anonymous meetings, and other medical and mental health programs
• Worsening life stressors, including housing, employment, childcare, food, access to health insurance and medical care
• Social distancing means that people are alone more often and fewer people may be around to respond to an overdose
• Restricted migration/trade patterns have made the drug supply less predictable
6
Types of brain injury
7
Traumatic Brain Injury (TBI) - Defined
TBI is an insult to the brain caused by an external physical force, such as a: banging your head, fall, motor vehicle accident, assault, sports related incident.
Acquired Brain Injury (ABI) - Defined
ABI is an insult to the brain that has occurred after birth, such as: TBI, stroke, near suffocation, infections in the brain, anoxia, and opioid overdose(s)
Both types of brain injury can be chronic, and get worse with age.
Overdose as a brain injury
• The frontal lobe is highly susceptible to brain hypoxia (reduced oxygen)
• Frontal lobe damage leads to potential loss of executive functions which are often required to participate, engage, and thrive in treatment
• As a result of frontal lobe damage, survivors of overdose may have issues with noncompliance, poor follow through, or a lack of engagement
• Decreased ability to participate and engage in treatment puts these individuals at increased risk for relapse
8
Cumulative impact
9
Cumulative impact - A subsequent brain injury can take longer to
resolve and the individual may experience more severe symptoms.
• What does this mean for people who overdose multiple times? Or who
regularly have “near” overdoses, which can involve oxygen deprivation to
the brain?
Opioids & Brain Injury Individuals with co-occurring brain injury and SUD may choose to use drugs to feel good or to relieve pain. (e.g post traumatic headaches, orthopedic injuries, heterotrophic ossification )
Individuals with co-occurring brain injury and drug use should have access to resources to use drugs more safely, to treatment programs that accommodate their individual needs, and to non-judgmental health care and service providers. (Programs should be brain injury informed)
10
Harm Reduction
Harm reduction is a philosophy and set of practices applied to promote safety associated with culturally stigmatized behaviors, such as drug use and sex work.
Harm reduction is practiced on two levels: the interpersonal, where we change our routines, share suggestions, and gather and distribute tools for increasing safety, and the institutional, where we change policy and systems to support safety and decrease violence and marginalization.
Source: Baltimore Harm Reduction Coalition
11
Harm Reduction on the interpersonal level
Gather and distribute resources and supplies to increase individual safety. Examples include:
• Naloxone distribution• Syringe service programs• Safer sex kits• Overdose prevention sites
12
Harm Reduction on the Institutional levelChange policies and organizational practices to decrease violence and create a safer, less harmful environment. Examples include:
● Advocating for increased access to quality health care, including behavioral health, for the entire community
● Re-considering severity of punishments for individual behaviors, including drug use and sex work
● Assessing how your agency or organization may perpetuate stigma and make an action plan to change the practices and culture
13
Asking why?Contextualizing approaches to drug use
What are the harms or risks of drug use?
15
What are the harms or risks of drug use?- Death- Cognitive impairment- Physical dependence- Memory loss- Financial issues
- Discharge from program- Incarceration - Lose your housing- Lose your job- ???
16

What are the harms or risks of drug use?- Death- Cognitive impairment- Physical dependence- Memory loss- Financial issues- Discharge from program- Incarceration - Lose your housing- Lose your job- ???
17
How many of these harms and
risks are CREATED or
WORSENED by our social and
cultural response to drug use?

Why do we think what we think about drugs?
• Self-assessment: Check in with yourself.
• What is your immediate reaction when you think about other people who use drugs?
• What is your immediate reaction when thinking about your own alcohol or drug use?
• Do you have a different immediate reaction to different substances? Why do you think that is?
• Do you feel like some drugs are “worse” than others? Why?
18

Historical Responses to Drug UseOpium Use and Restriction - late 1800s-early 1900s• Chinese practice of opium dens brought to US in 1850s• 1890: US Govt imposes a tax on opium in first narcotic restriction legislation• Mainstream newspaper stories warn of dangers of white women being “seduced” by
Chinese men and their opium Source: Opium Throughout History on PBS Frontline
• “In the late 19th century, as long as the most common kind of narcotic addict was a sick old lady, a morphine or opium user, people weren’t really interested in throwing them in jail. That was a bad problem, that was a scandal, but it wasn’t a crime. When the typical drug user was a young tough on a street corner, hanging out with his friends and snorting heroin, that’s a very different and less sympathetic picture of narcotic addiction.”
Source: David T. Courtwright, author of Dark Paradise: A History of Opiate Addiction in America.
19

Historical Responses to Drug UseHarry Anslinger and the criminalization of marijuana
• Director of the Federal Bureau of Narcotics for 32 years
• Led advocacy for the Marijuana Tax Act of 1937, which effectively made marijuana illegal
• From the 1890s-1930s, Anslinger and newspaper publisher William Randolph Hearst used racism and sensationalism to campaign for marijuana criminalization. These tabloid stories frequently linked drug use by African Americans and Mexican immigrants to sexual violence against white women.
• “There are 100,000 total marijuana smokers in the US, and most are [Black people], Hispanics, Filipinos, and entertainers. Their Satanic music, jazz and swing, results from marijuana use. This marijuana causes white women to seek sexual relations with [Black people], entertainers, and others.” - Anslinger
Source: Robert Solomon, author of “Racism and Its Effect on Cannabis Research.”
20
Historical Responses to Drug Use
• President Nixon declared a “War on Drugs” and in the 1970s, including the creation of the DEA.
• Ushered in an era of mass incarceration, mandatory minimums, and more severe sentencing.
• Although rate of drug use is similar across racial groups, Black people and Latinx people are disproportionately arrested, charged, and convicted of drug-related crimes.
21

How does criminalization affect treatment services?• Goals and expectation are often set by the program, not by the client
• Traditional SUD approaches are often centered around abstinence and there are few services for people who use drugs outside of this perspective. For people in court-mandated treatment, abstinence is often mandated.
• Surveillance and monitoring through urine drug screens
• Punishment and consequences for “positive” urines
• Provider resentment toward people who continue to use drugs
22
Employment policy
The Drug Policy Alliance has identified three areas of focus related to drug use and employment:1) Pre-emptive drug testing - no evidence that pre-employment drug testing predicts on-
the-job impairment; also consider who gets drug tested most frequently (manager vs worker)
1) Discrimination based on criminal record - Consider that drug use is similar across racial groups, but that Black, Brown, and poor people are disproportionately arrested and convicted of drug crimes
1) Stigma against those with a diagnosed substance use disorder (SUD)
23
Changes in Baltimore City
• Baltimore City Mayor Brandon Scott announced during his March 2021 “State of the City” address his plans to issue an executive order stopping pre-employment drug screenings for city employees in non-safety positions.
• During his announcement, he stated, "It’s on all of us -- from our partners to our friends in labor -- to ensure City employment remains accessible to our neighbors who have been impacted by the War on Drugs."
24
Harm Reduction Tools
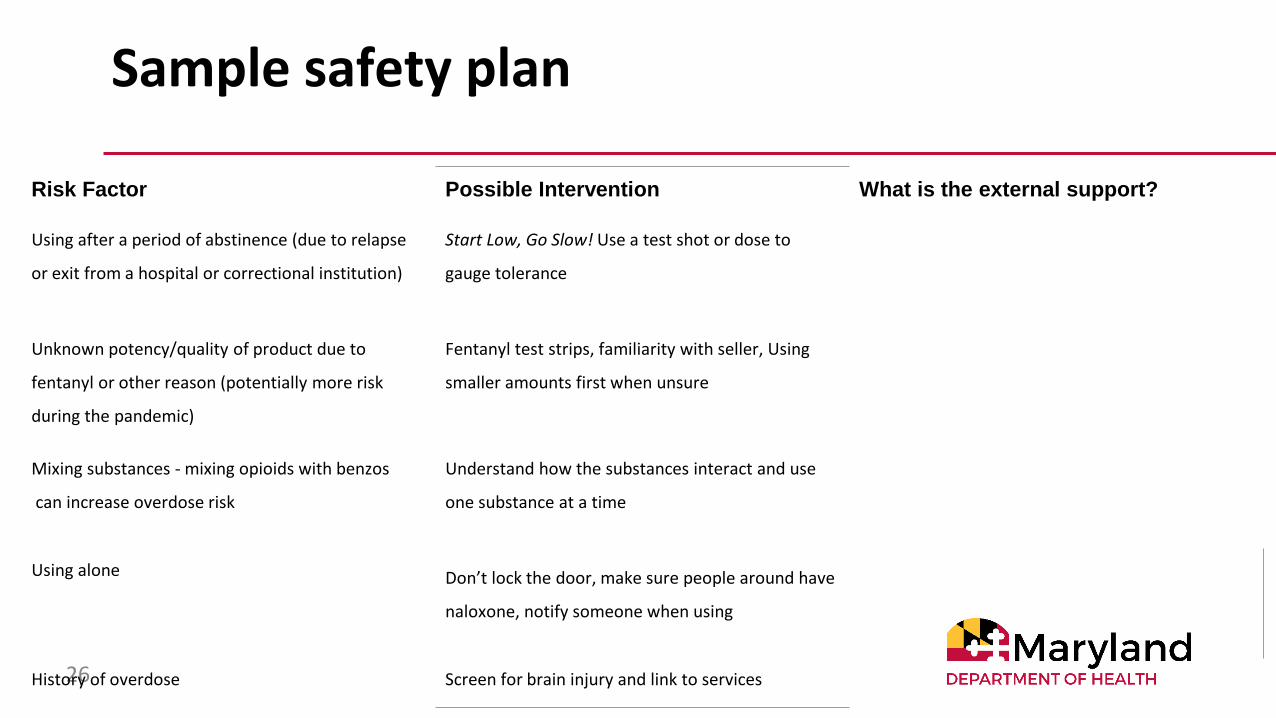
Sample safety plan
26
Risk Factor Possible Intervention What is the external support?
Using after a period of abstinence (due to relapse
or exit from a hospital or correctional institution)
Start Low, Go Slow! Use a test shot or dose to
gauge tolerance
Unknown potency/quality of product due to
fentanyl or other reason (potentially more risk
during the pandemic)
Fentanyl test strips, familiarity with seller, Using
smaller amounts first when unsure
Mixing substances - mixing opioids with benzos
can increase overdose risk
Understand how the substances interact and use
one substance at a time
Using alone Don’t lock the door, make sure people around have
naloxone, notify someone when using
History of overdose Screen for brain injury and link to services

Harm Reduction Organizational Analysis
27
How do we harm our clients: Recommended organizational responses:
Over-emphasis on abstinence leads individuals to hide or downplay drug use
Incentivize progress on individual-identified goals, remove penalties for drug use
Increase sense of shame when unable to meet unrealistic expectations
Remove requirement of attending specific # of groups, encourage and recognize variety of social supports
Place expectation for change only on the internal motivation of the individual
Improve screening for brain injury and utilize accommodations and external supports
Discharge for not meeting program rules Work with the individual to make changes to care as needed
Ignore context of racialized drug policy Validate experiences. Advocate for those in other health care settings and with law enforcement. Make space for political advocacy.
Tips from Brain Injury Providers
• Be flexible with rules, particularly around group attendance and participation. Allow for participants to take breaks as needed.
• Focus on routines and behaviors as much as on internal motivation
• Use concrete safety plans with external supports to better understand specific risk and increase safety.
28
Harm Reduction Resources in Maryland
• Syringe service programs are operational in 7 jurisdictions https://phpa.health.maryland.gov/Documents/SSP%20Guide.pdf
• Naloxone is available through 100+ certified overdose response programs (ORPs) or available at most pharmacies. Also available through the mail via the Baltimore Harm Reduction Coalition
• Additional training available through:• Baltimore Harm Reduction Coalition• Maryland Harm Reduction Training Institute
29

Small group discussions

Pick one (or both!)
1) What accommodation or practice that you can implement right now is sticking out to you?
1) What change in organizational policy, law, or regulation do you want to advocate for?
31

What we are working towards
“And that deep and irreplaceable knowledge of my capacity for joy comes to demand from all of my life that it be lived within that knowledge that such satisfaction is possible”
- Audre Lorde
32
Thank you!!!
“This project was supported, in part by grant number 90TBSG0027-01-00 from the U.S. Administration for Community Living, Department of Health and Human Services, Washington, D.C. 20201. Grantees undertaking projects with government sponsorship are encouraged to express freely their findings and conclusions. Points of view or opinions do not, therefore, necessarily represent official ACL policy.”
2021
Traumatic Brain Injury Partner Project
MD Behavioral Health Administration

















