#HASummit14 Session #7: How Mayo Clinic Standardized Care Across 22 Emergency Departments Pre-Session Poll Question Do you work in some capacity in or for your ED(s)? a) Yes b) No c) Not applicable Christopher S. Russi, DO, FACEP Assistant Professor of Emergency Medicine Mayo Clinic College of Medicine Rochester, MN
Transcript
#HASummit14
Session #7:How Mayo Clinic Standardized Care Across
22 Emergency Departments
Pre-Session Poll Question
Do you work in some capacity in or for your ED(s)?
a) Yesb) Noc) Not applicable
Christopher S. Russi, DO, FACEPAssistant Professor of Emergency Medicine
Mayo Clinic College of MedicineRochester, MN
#HASummit14
Poll Question #2
2
What is your role in your ED(s)?
a) Physician
b) Physician / Admin (Medical Director)
c) Admin
d) Advanced Practice Provider (APP)
e) APP / Admin
f) Nurse
g) Nurse / Admin
h) Not applicable
#HASummit14
De
gre
es o
f in
teg
rati
on
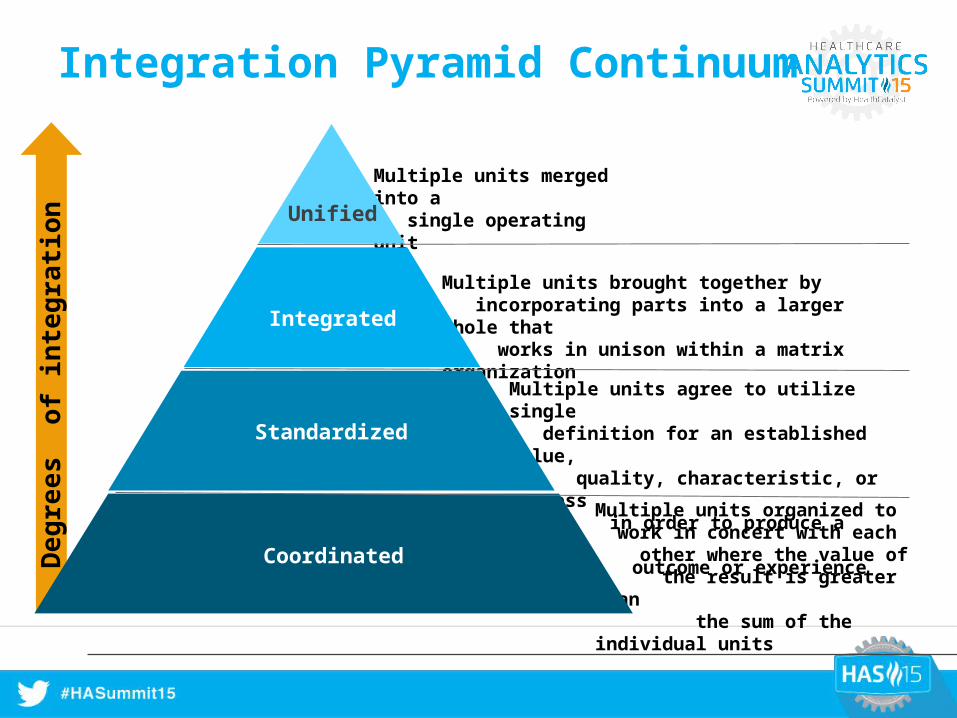
Multiple units organized to work in concert with each other where the value of the result is greater than the sum of the individual units
Multiple units agree to utilize single definition for an established value, quality, characteristic, or process in order to produce a uniform outcome or experience
Multiple units brought together by incorporating parts into a larger whole that works in unison within a matrix organization
Multiple units merged into a single operating unitUnified
Integrated
Standardized
Coordinated
Integration Pyramid Continuum
#HASummit14
Why Integrate?
Affordable Care Act
Changes in Medicare reimbursement (probable commercial payer reductions as well)
Expansion of Medicaid
Leverage the “value equation”
Need to operate clinically in a synchronous fashion• “Working differently” to reduce cost and improve quality• Examples:
Patellar fracture transfer Direct admissions Best practice dissemination
Migraine management Keeping patients local
#HASummit14
A Gift?
June 2012
Enterprise Integration Summit / Announcement
• Suddenly we owned 21 Community Emergency Departments
• Thanks, now what?
• Urgent need to make a Division
• EMERGENT need to improve staffing
• No idea of the magnitude of what we just were gifted
#HASummit14
Emergency Medicine in the MCHSBackground
1992 – 1st site: Decorah
• Contract services (county-owned facility)
Next 21 years
• 78 communities served
• 21 EDs (Regional Structure)
‒ 10 Critical Access (CA) sites
‒ 3 contract services
‒ 2 Level-3 trauma centers, 1 Level-2
‒ ~ 320,000 annual visits*
• 2nd largest workforce in MCHS
#HASummit14
#HASummit14
Enthusiasm Redirected
NIH KL2 Scholar
• Interested in developing a severe sepsis / septic shock treatment protocol transcending community to receiving centers
Slam on the brakes…
Why am I here?
• Non-data and analytic approach
#HASummit14
How do we Integrate? Where do we begin?
• 22 distinct cultures / personalities
• Geographically and economically disperse
• Variable provider (sometimes absent) workforce
• Siloed recruiting, salaries, administration, and privileges
• Staffing CRISIS
• Focus on PEOPLE
‒ Wrong people = No engagement = NO integration
#HASummit14
Poll Question #3
10
Do you have locum tenens routinely staffing your EDs?
a) Yes
b) No
c) Not applicable
#HASummit14
Immediate Strategy & Tactics
• Road Trip – Invest in knowledge acquisition and relationship building
• Salary Standardization / Correction
• Right tools in place
• EM Leadership Team / Medical Directors
• Develop people
• Eliminate locums
#HASummit14
My Job
• Rapid evolution from the start
• Vision and Strategy
• Recruitment
• Salary / Comp standardization
• Advocacy at the C-Suite
• Practice standardization
• Education
#HASummit14
Early Projects / Successes
Large, functional, productive Division
Centralized Recruiting Process
• 18 hires in two years
‒ $75K savings / FTE locum offset
‒ Heavy use of the CA position
Bedside US
APP Fellowship
‒ $210K saving / FTE physician offset
Create a shared staffing model (Mobile Workforce)
• Web-based scheduling software
• Singular privileging form
#HASummit14
Early Projects / Successes
• Demonstrate Value of EM
‒ Reduced Transfers
‒ Reduction of Oncall need for Ortho / Anesthesia
• Standardized Salary / Benefits
• Move to a salary model
• Midwest APP Medical Director
• Logix Health Implementation
‒ $2.2m realized + $8m estimate NOI increase
• Nursing Standardized Education / Training
• Fairmont & Red Wing ED Redesign
#HASummit14
Future Projects
• Begin to standardize approaches to emergent conditions
• qPath (US billing)
• Match providers to volume and acuity
‒ The APP transition
• Develop a Midwest quality team
‒ Singular focus
• Annual meeting / education event?
#HASummit14
Lessons Learned
16
1. Take a hard look at the current workforce. You may need to make substantial investments to correct issues.
2. Hire those with “fire in the belly.” Those who are enthusiastic and believe in your mission should be your hiring focus.
3. Put the right leaders in the right places.
4. Doing the “right thing” is ok in the absence of supportive data/analytics. Don’t be paralyzed.
#HASummit14
Analytic Insights
AQuestions &
Answers
17
#HASummit14
Choose one thing…
18
Write down one thing will you do differently after hearing this presentation
#HASummit14
Thank You
19
#HASummit1420
Session Feedback Survey
1. On a scale of 1-5, how satisfied were you overall with this session?
10) Is Big Data a Big Deal…or Not?Dale Sanders, Senior Vice President, Health CatalystRichard Proctor, General Manager, Global Healthcare & Life Sciences, Hortonworks
11) Partners Healthcare Analytic Strategy for bundled Payments and Risk ManagementSreekanth Chaguturu, MD, Vice President for Population Health Management, Partners HealthCareHelen Chan, Senior Manager, Business Planning, Partners HealthCare
12) Sneak Peek: Improving Patient Engagement and Outcomes with Predictive AnalyticsGregory A. Spencer, MD, CMO & CMIO, Crystal Run HealthcareLouis G. Cervone, Jr., Director of Business Intelligence, Crystal Run Healthcare
13) How a Pioneer ACO is Using Analytics to Change Heart FailureSpencer H. Kubo, MD, CMO of BioControl Medical, United Heart &Vascular Clinic, Allina Integrated Medical Network
14) Entering Shared Risk for Community Hospitals Through Physician EngagementGreg Stock, CEO, Thibodaux Regional Medical CenterMark F. Hebert, MD, FACS, Surgical Specialist, Thibodaux Regional Medical Center
15) Panel – Children’s Hospitals: “Tike-mares”…Are the Monsters Under the Bed For Real?