HCI Sarcoma Services Sequential Dependency of Radiotherapy for Soft-Tissue Sarcoma S Sampath TE Schultheiss YJ Hitchcock RL Randall DC Shrieve JYC Wong CTOS, Miami Beach, FL November 7, 2009
Transcript
HCI Sarcoma Services
Sequential Dependency of Radiotherapy for Soft-Tissue Sarcoma
S Sampath TE Schultheiss YJ HitchcockRL Randall DC Shrieve JYC Wong
• clinical stage• grade• histology • site• size• cause of death • race• gender• margin status • types of failures• dates of failures• surgery• RT sequence• chemotherapy
• Surgery – local tumor removal
NOS – simple excision– wide limb-sparing
resection– amputation– surgery NOS
HCI Sarcoma Services
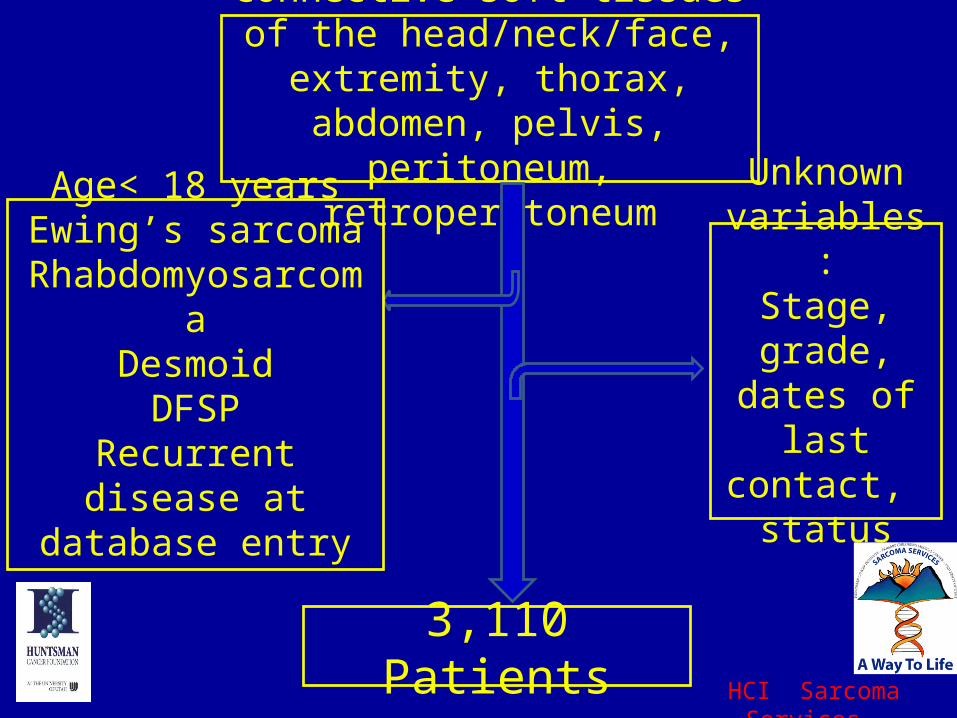
Patient Characteristics
HCI Sarcoma Services
Results• Multivariate analysis for OS for the 3,110 patients
showed RT sequence to be a significant variable in model– pre-op RT associated with improved OS compared to
post-op RT (HR 0.76, 95% CI 0.6-0.95, p<0.05)
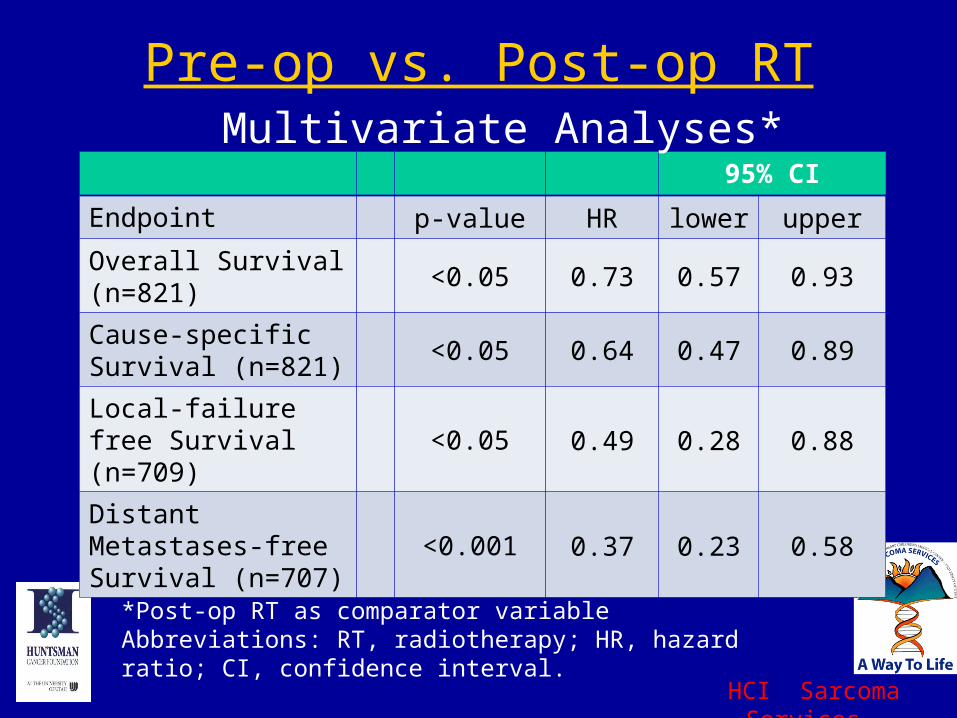
• Remainder of study consisted of 821 patients who received surgery and either pre-op or post-op RT
• Median follow-up 63 months (0-19 years)• Median RT doses: Pre-op 50.4 Gy, Post-op 60 Gy• Prognostic factors balanced
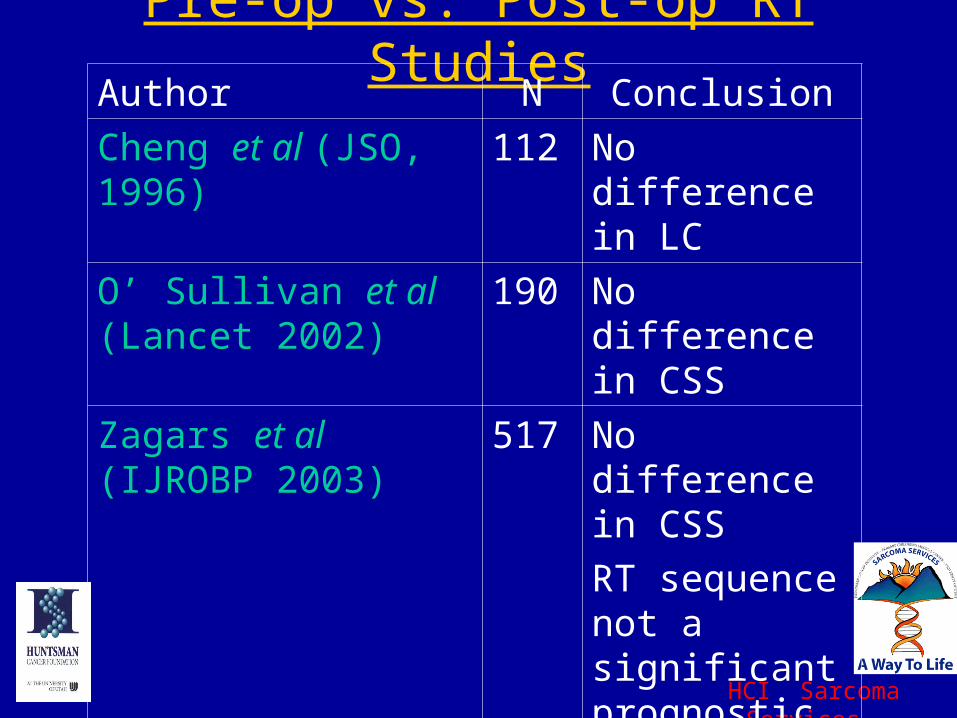
RT sequence not a significant prognostic factor on MVA
Kuklo et al (AJO 2005) 117 No diff. in LC
HCI Sarcoma Services
Synovial Sarcoma & Sequential Dependency
• Guadagnolo et al: IROBP 2007– 150 patients with non-metastatic SS– Pre-op RT led to an increased risk of
distant failures versus post-op RT (50% vs. 40%) but not significant
– No difference in LF or OS.
HCI Sarcoma Services
Why did Pre-op RT do better?• Hypothesis:
– Post-operative hypoxia may increase development of distant metastases(P=0.01)
– Brizel et al, Cancer Res 1996
P=0.01 pO2
>10 mm Hg
pO2
<10mm Hg
18mo. DFS 70% 35%
HCI Sarcoma Services
Criticism:“If nothing bad is ever said, then nothing good will ever get done”
• Retrospective outcomes study: – Unable to account for:
• performance status • Institutional bias of larger volume sarcoma
centers• Not always clear if grading was a 3 vs. 4 tier
– Under-reporting of chemotherapy (17%)– Heterogeneity of post-treatment follow-up
HCI Sarcoma Services
Conclusions
• Hypothesis-generating study shows that pre-op RT is associated with improved sarcoma-specific survival compared to post-op RT– Via improved local controldecreased distant
metastases– LMS, SS may be particularly advantaged
• Additional comparative or randomized studies are necessary