130
Health and Personality Among Army Officers

Health and Personality
Among Army Officers

The role of personality and physical fitness as mediators between life events stressors and illness among middle-ranking army officers.
W.H. HALL
Submitted in partial fulfilment of the requirements of the degree of Masters of Clinical Psychology, in the Department of Psychology, Australian National University, 1986

For Anne Jane and Kate

DECLARATION
I declare that this sub-thesis reports my original work, that no part of it has been previously accepted or presented for the award of any degree or diploma by any university, and to the best of my knowledge no material previously published or written by another person is included, except where due acknowledgement is given.
The findings and views expressed are the results of the author's research studies and are not to be taken as the official opinion or policy of the Department of Defence (Army Office).
Table of Contents
ACKNOWLEDGEMENTSABSTRACTCHAPTER 1 INTRODUCTION
1.1 Background1.2 Life Events Stressors1.3 A Life Events Stressors Model1.4 The Life Events Stressors-Illness
Relationship1.5 Moderator Variables1.6 Personality Hardiness1.7 Physical Fitness1.8 The Present Study
CHAPTER 2 METHODCHAPTER 3 RESULTSCHAPTER 4 DISCUSSIONREFERENCESAPPENDICES
A Letter to Subject PoolB Modification of the Life Events
InventoryC Life Events Inventory and Life Change
ScalingsD Seriousness of Illness Rating ScaleE Instrument to Measure Psychophysiological
Re sponseF Hardiness TestG Measurement of Physical FitnessH Physical Fitness Assessment Worksheet
Page
iii
145
89101516 19 27 39 50
74
76
93102
108110116123

ii
ACKNOWLEDGEMENTS
The assistance and advice of the following are gratefully acknowledged:
Dr Mark Dickerson, whose considerate yet unobtrusivemethod of supervision proved an ideal foil for my own style.
Major General W.B. James, recently Director GeneralArmy Health Services, for suggesting the research topic and supporting its carriage.
Lieutenant Colonel P.N. Drake-Brockman, Commanding Officer 1st Psychological Research Unit, for providing administrative and technical support.
Terry Thurbon, Colleen McBain and Noel Hewitt, for providing the many hands which made the work 1ighter.
The officers who gave so generously of their time to participate in the study.

iii
Abstract
This study examined the independent and additive effects of personality hardiness and physical fitness as moderators in the life events stressors-illness relationship among middle-ranking army officers (N=96). Self-report measures of hardiness, life events stressors, psychophysiological response and illness were obtained. A physiological measure of fitness (maximum oxygen uptake) was employed.
The results provided support for claims that personality hardiness and its three components (commitment, challenge and control) buffered against illness, and suggested that officers who were low on both hardiness and fitness were more susceptible to reporting a history of illness than officers high on one or both of the variables. No relationship was found between reports of life events stressors and psychophysiological response. Implications for the Army's system of physical training tests were also discussed.

1
In recent years the topic of stressor-related illness has reached pre-eminence in the Western world. A proliferation of books, sound and video recordings, agencies, 'health-farms', consultants, cults, communes and professionals have been spawned in an attempt to combat the effects of the stressors inherent in modern society. The trend in early research was to concentrate on those persons who succumbed to illness in the face of stressors. However, as there are many persons who are subjected to the same stressors but do not fall victim to illness, the current emphasis in life events stressors-illness research has shifted to variables which moderate against the effects of the stressors. The present study provides a selective review of this area of research and examines the joint mediating effects of personality and physical fitness among middle-ranking army officers.
Background
One of the earliest recorded observations of an association between stressors and illness is attributed to Hippocrates who reported that specific emotional states appeared to bring on physical symptoms (Levine, cited in Goldberg and Comstock, 1976). Through the centuries there has been an abundance of clinical observations supporting Hippocrates' contention, however the controlled scientific investigation of the apparent relationship had its roots in the studies of Cannon and Myers little more than fifty years ago.

2
In his research Cannon monitored the relationship between stimuli associated with emotional arousal (pain, hunger and the major emotions) and changes in physiological processes. From these observations he proposed:
the strong emotions, as fear and anger, are rightly interpreted as the concomitants of bodily changes which may be of utmost service in subsequent action. These bodily changes are so much like those that occur in pain and fierce struggle that, as early writers on evolution suggested, the emotions may be considered as foreshadowing the suffering and intensity of actual strife. On this general basis, therefore, the bodily alterations attending violent emotional states would, as organic preparation for fighting and possible injury, naturally involve the effects which pain itself would produce. And increased blood sugar, a larger output of adrenalin, an adapted circulation, greater number of red corpuscles and rapid clotting would all be favourable to the preservation of the organism that could best produce them' (cited in Dohrenwend & Dohrenwend, 1974, p.2).
Much credit for the clinical application of Cannon's findings that stimuli associated with emotional arousal can cause changes in basic physiological processes falls to Myers. He postulated that the normal, mundane events of day-to-day life, as well as the catastrophic, contributed to basic physiological changes developing into pathological conditions. It followed

3
that a central theme to his teachings was the belief that an examination of important events in a patient's life formed part of the clinical diagnostic pattern for various somatic and psychological disorders.
Myers' work stimulated considerable interest and research effort directed at establishing links between life events stressors and specific illnesses. In numerous studies relationships were reported between these stressors and a diversity of disorders affecting the eye, airways, stomach, colon, muscles, joints, skin, genitals and cardio-vascular system (cf. Dohrenwend & Dohrenwend, 1974).
Despite this welter of inquiry, not until Selye was there a concerted attempt to superimpose a theoretical framework on the relationship. Selye's theory emerged from his physiological studies in which he used noxious stimuli with animals. His General Adaptation Syndrome (GAS) model provided an explanation of the physiological processes which are activated in order that an adaptation may be made to a noxious stimulus . He postulated that any noxious stimulus produced an increased physiological response characteristic of the GAS (e.g., increased adrenal cortical hormones) which in turn caused a lowering of the body's resistance and 'wearing' effects on body organisms. If the adaptive responses were prolonged or defective, illness would occur, depending on the weakness of various organs. Thus Selye provided a ready framework for later proponents of theories which emphasised a general susceptibility to illness (versus susceptibility to specific illnesses) in response to life events

4
Stressors. Although subsequent research (cf. Cohen, 1979) has questioned some of the assumptions underlying Selye's model, it remains central to much of the life events stressors-illness research.
Selye's research with noxious stimuli was expanded to include experiments in which stimuli represented a range of connotations. The results indicated increases in physiological responses regardless of the desirability of the stimuli (cf. Cohen, 1979), thus suggesting that positive as well as negative life events resulted in physiological activity which may be a precursor to illness.
Life Events Stressors
Holmes and Rahe and their colleagues synthesized many of the early findings in their investigations of the relationships between life events stressors and illness of all types. The assumption underlying their work was that adapting to any change was stressful and that the cumulative effects of stress increased the risk of illness (Holmes & Rahe, 1967). A life event was defined as being stressful if it caused change in, and demanded readjustment of, an average person's normal routine. The magnitude of the change associated with each event was determined using the techniques of psychophysics. The early research culminated in the production of the instruments which have been the cornerstones of studies in this area of research:

5
the Schedule of Recent Events (a list of 43 commonly occurring life events); and the Social Readjustment Rating Scale (a scaling for the magnitude of change associated with each of the above events).
Studies which employed these instruments have found life events stressors to be related to sudden cardiac death; myocardial infarction; pregnancy and birth complications; chronic illness; tuberculosis; multiple sclerosis; diabetes and a range of less serious disorders (cf. Sarason & Sarason, 1984). The correlations reported, however, have been typically less than 0.30 (cf. Rabkin & Struening, 1976). These studies are claimed as support for Holmes & Masuda's (1974) contention that life events stressors increase susceptibility to illness of all types. In addition, the measures have been shown to sustain their power within a number of populations across race, nationality and culture.
A Life Events Stressors - Illness Model
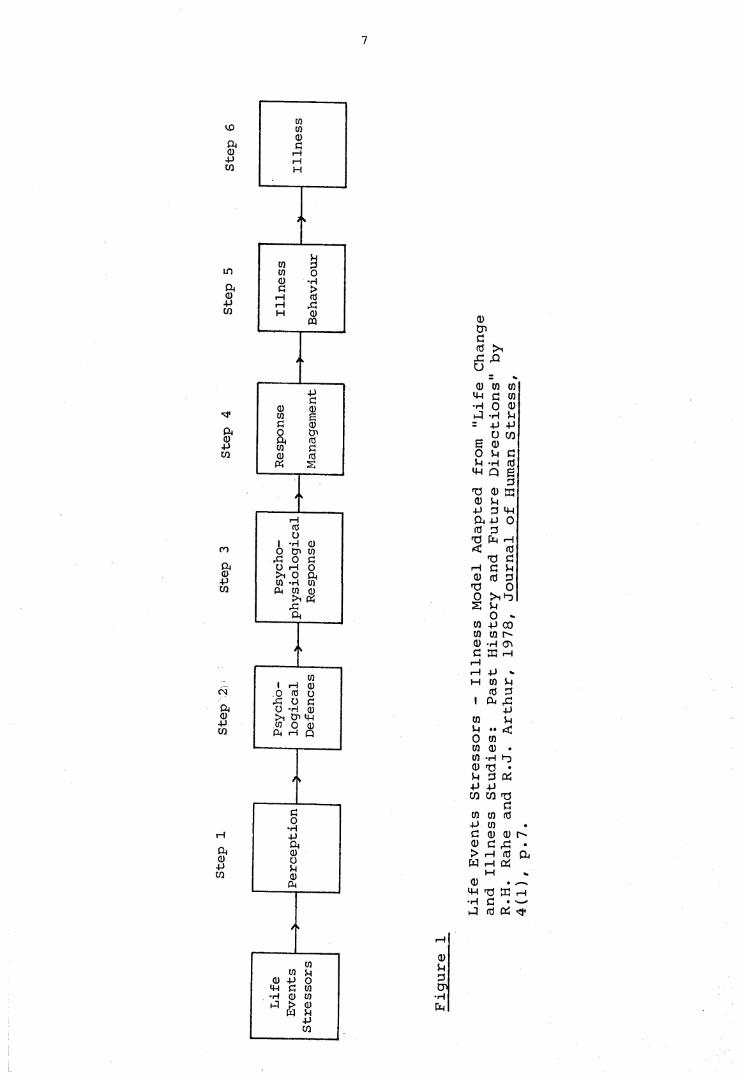
The work of Holmes and Rahe and their colleagues was posited on a linear life change - illness model (Rahe, 1974; Rahe & Arthur, 1978) expanded from Selye's basic model. An adaptation of the model is in Figure 1. The model conceptualized the relationship between life events stressors and subsequent illness in six steps with a series of filters between exposure to the stressors and diagnosis of illness.

6
Step 1 incorporates the effects of the perceptive set of the individual in attaching significance to an event. Factors which may contribute to life events being perceived as stressors at this step include past experiences/ social support and biographic assets. The concept parallels Lazarus' (1966) 'appraisal': if the person possesses the resources to overcomethe threat, to restructure the event positively or fails to perceive that danger exists, then the effects of the stressors will be minimized.
The role of psychological defence mechanisms (such as denial, displacement, repression, reaction formation and isolation) in moderating against the effects of the stressors is contained in Step 2 of the model. The range of psychophysiological responses is accommodated in Step 3.Included are those responses of which the individual is aware (e.g., mood shifts, headache, muscle tension) as well as those responses which are generally outside the individual's awareness (e.g., elevated lipids, elevated blood pressure, hypoglycaemia). Step 4 includes those responses an individual makes in an attempt to manage the effects of the psychophysiological symptoms in Step 3. Strategies may include muscle relaxation, physical exercise, medications or situational adjustments. In Step 5 illness behaviour adopted by the individual is considered: theindividual recognises symptoms and may select a sick role (absenteeism from work, consultation with a medical practitioner, adherence to a treatment plan). The final step involves the individual's illness being diagnosed and recorded by a medical practitioner as an illness.
7
C0
p02
in
ft(UP03
aa)p02
ro
P02
CM
ft0P02
rH
ft<up02
>i tr> p
02CnGfO > 1
jc , &o
02 CO CO P G co •H o 02P P P = P P
O C/2
P P fd P Q E
GT3 02 f t 02 p PGP ft P O <0 G
T3 f t P<c <0
f t C P G P 02 fd G
f t O0 > i f t £ P
O - C0 p co co co 02 P 02 G EC P pp P «•H CD P
<0 G1 f t p
PCO P P <O to CO 02 •CO P i-o02 f t •P G f tP PC/3 C/3 f t
Cco co idP coC 02 02 C"*02 C G •k* p cd f t f t P f t
p02 • —
P d G p •H G • — 1f t cd f t
r-H
0PGCn
•Hft

8
The Life Events Stressors - Illness Relationship
Psychophysiological response has been regarded as a precursor of both psychosomatic (e.g., Horowitz, 1976) and physical (e.g., Rahe, 1974) illness. Rahe and his co-workers (Rahe & Arthur, 1978) found the correlation between life events stressors and psychophysiological response (Step 3 on the model) to be approximately 0.30; and the correlation between psychophysiological response and subsequent illness (Step 6) to be approximately 0.24. However the correlation across the total pathway (between life events stressors and illness) fell to 0.12. Although all correlations were statistically significant (jd<.01), less than 2% of the variance was explained. Although an individual's exposure to life events stressors was found to be moderately related to psychophysiological symptomatology, many who exhibited symptoms did not seek medical consultation.
As numerous studies of the life events stressors- illness relationship have reported consistently that associations are typically below 0.30 (cf. Rabkin & Struening, 1976), the attention of recent studies has turned to the bulk of the population who are exposed to life events stressors but do not succumb to illness. In terms of Rahe's model, researchers have attempted to identify factors which cause individuals to scatter at various steps along the pathway and so refrain from becoming illness statistics despite their having been exposed to lifeevents stressors.

9
Moderator Variables
Certain variables contribute to individual differences in responses following exposure to life events stressors. These variables have been dubbed 'moderator variables', 'buffers' and 'mediators'. In the current report the terms will be interchanged and will represent those variables which contribute to the maintenance of health in the face of life events stressors. The variables include physiological or constitutional strengths, social resources and certain psychological characteristics.
The existence of these variables has been posited by Lazarus (1966) with his concept of 'appraisal'; Antonovsky (cited in Ganellan & Blaney, 1984) who suggested that individuals possessed 'resistance resources'; and by Selye (1976) who claimed .... it is especially true that, in our life events, the
stressor effects depend not so much upon what we do, or what happens to us, but on the way we take it' (p. 370). The following list of examples taken from the literature is far from exhaustive: a well functioning immunological system; a familyhistory that is free from genetically linked diseases; a history of pre-existing illness; marital status; income; support of friends, neighbours or spouse; close community ties; the absence of Type A characteristics; an internal locus of control; psychological needs for sensation and arousal seeking; fit between person and work role; intelligence; norms governing illness behaviour; and health practices such as exercise (cf. Cohen, 1979; Kobasa, 1982b; Kobasa & Puccetti, 1983; Sarason & Sarason, 1984) .

10
More recently studies have sought to establish the effect of various combinations of variables in buffering against illness. Pearlin, Lieberman, Menaghan and Mullen (1981) reported that social support and coping behaviour moderated the negative effects of stressful job events on mental health; Kobasa, Maddi and Puccetti (1982) found independent and additive buffering effects from personality and exercise; Kobasa, Maddi and Zola (1983) reported Type A characteristics increased general illness but other personality variables buffered against illness; and Kobasa and Puccetti (1983) found that personality variables and perceived boss support buffered against illness, perceived family support increased symptomatology, and social assets made no impact on health status.
Personality Hardiness
Kobasa's (1979b) concept of personality hardiness as a buffer against the effects of life events stressors on illness was based on the integration of an existentialist theory of personality (cf. Kobasa & Maddi, 1977) with various empirical leads from social psychological, developmental and personality research (cf. Kobasa, 1982b).
Existentialism's emphasis on persons as beings-in-the-world who do not carry around a set of static internal traits, but rather continuously and dynamically construct personality through their actions, suits the personality-in-situation emphasis of

11
the personality and stress question. Second, existentialism portrays life as always changing and therefore inevitably stressful. The mission of existentialists has been to describe how best to confront, utilize and shape this life. Unfortunately more space has been devoted to depicting how persons have failed in the struggle rather than succeeded. But it is recognised, on philosophical and psychological grounds, that persons can rise to the challenges of their environment and turn stressful life events into possibilities or opportunities for personal growth and benefit. Three existential concepts appear especially relevant to this optimistic orientation: commitment,control and challenge. Together these comprise the personality style of hardiness (Kobasa, 1982b, p.6).
Commitment (versus alienation) refers to an individual's ability to believe in the truth, importance and interest value both of one's self and one's actions. Committed persons involve themselves fully in a wide range of life: work,family, interpersonal relationships and social institutions. Their orientation is one of vigorousness rather than vegetativeness. They have a sense of purpose in life; are able to recognise goals and priorities; and have confidence in their abilities to make decisions and maintain values. Conversely, persons who are alienated from themselves reflect 'a lack of involvement with (their) distinctive skills, sentiments, and values and a passive attitude towards personal decision making and goal setting' (Kobasa, Maddi & Puccetti, 1982, p. 396).
12
Those alienated from work display 1 a general sense of meaninglessness, apathy, detachment... and a lack of personal investment in that area of life involving socially productive occupation' (Kobasa, Maddi & Puccetti, 1982, p. 397).
Commitment is based in a sense of community: committedpersons are able to draw on the knowledge that they can turn to others when they are in difficulty, as well as being aware that others are depending on them to persevere in trying times. Thus committed persons have both the skills and determination to cope successfully with stressors. According to Antonovsky (cited in Kobasa, 1982b) the possession of a sense of accountability to others is the prime social resource for coping with the effects of stressors.
Control is possibly the single personality characteristic which has attracted more attention from researchers than any other. Its efficacy as a buffer against the effects of stressors has been indicated in numerous field and laboratory studies (cf. Lefcourt, 1980; Kobasa, 1982b). Control reflects the belief of persons that their lives can be influenced by the self, rather than being at the mercy of external forces such as fate, chance or powerful outsiders. Persons with control assume responsibility for events in their lives; perceive many life events stressors as predictable consequences of their own decisions and actions; and feel confident of their ability to manipulate events to their own advantage. Their orientation is one of meaningfulness rather than nihilism. Averill (1973) asserted that persons with control possess a 'coping repertoire'

13
(a cluster of responses that can be summoned in reaction to life events stressors); and as well as having confidence in being able to cope effectively on their own initiative, they possess the ability to perceive most events as integral to their own life plans.
Challenge is based on the assumption that change rather than stability is the norm. Persons with this characteristic view life events stressors as opportunities for personal development rather than as threats to security; they seek new and stimulating experiences actively; they are well rehearsed in responding to the unexpected; they are familiar with their environment and attuned to the resources available to them to minimize the effects of the stressors; and they are typically flexible, tolerant and candid. Thus they are well equipped to appraise the threat of the most unexpected life events stressors. In contrast, persons lacking in the challenge dimension value safety, stability and predictability.
Kobasa (1979b) demonstrated the possible buffering effects of personality hardiness in a retrospective study of executives identified as being high on life events stressors.The findings indicated that those executives in the high life events stressors - low illness group achieved scores on measures of hardiness that were significantly higher than the scores of executives in the high life events stressors - high illness group. Subsequent investigations appear to have overcome the methodological flaws inherent in the initial retrospective study and so have established the prospective buffering effect of hardiness on illness.

14
In one study (Kobasa, Maddi & Khan, 1982) illness was monitored for two years subsequent to the measurement of life events stressors and hardiness. The study controlled for the possible confounding effects of existing illness symptoms. The results indicated that life events stressors increased illness, while hardiness decreased it. In addition, the illness buffering effects of hardiness were greatest when life events stressors mounted. It was found in a second, similar study (Kobasa, Maddi & Courington, 1981) that constitutional predisposition, as an independent variable, was unrelated to hardiness thus demonstrating that hardiness was not merely a reflection of the incidence of illness suffered by a person's natural parents. Results of the study also confirmed that hardiness reduced illness while life events stressors and constitutional predisposition were found to increase it.
The buffering effects of hardiness have been shown to be relevant in several populations in addition to executives discussed above, viz.,: lawyers (Kobasa 1982b); army officers(Kobasa, cited in Kobasa, 1982b); and gynaecology patients (Kobasa & Hill, cited in Kobasa, 1982b).
In terms of Rahe's model it is conceptualized that the effect of personality hardiness is to moderate between life events stressors and psychophysiological response (cf. Kobasa, 1982a; Kobasa & Puccetti, 1983). In so doing hardiness adds to the moderating effects of other variables which buffer against the effects of the stressors. Hardiness facilitates a person's ability to perceive, evaluate and cope with stressors in a manner

15
which will successfully resolve the situation created by the stressors. 'The coping styles of hardy persons reflect their belief in their own effectiveness as well as their ability to make good use of other human and environmental resources. Coping for them consists of turning stressful events into possibilities and opportunities for their personal development and that of others around them' (Kobasa & Puccetti, 1983, p.840). Thus personality hardiness diminishes the debilitating effects on the organism associated with the need for continuous readjustment.
Physical Fitness
There has been considerable expenditure on the promotion of physical fitness as a buffer against illness, particularly in the area of cardio-vascular disorders. Studies have demonstrated that physical fitness programmes have contributed to reducing health care costs, reducing sick leave, and improving morale and productivity (cf. O'Connell & Price, 1982). Other studies have shown that adequate physical activity (including exercise and manual labour) will promote efficiency in a number of cardio-vascular functions; enable many previously incapacitated persons to resume a more active life style; and decrease the probability of heart attack, particularly in highly stressed groups such as business executives (cf. Paffenbarger & Hale, 1975; Epstein, Miller, Stitt & Morris, 1976; Paffenbarger, Wing & Hyde, 1978; Everett, 1979).

16
The effects of maintaining a reasonable level of fitness are to increase cardiac efficiency, curb heart rate and minimize arhythmia; increase fibromolytic activity; and promote coronary arterial circulation (cf. Paffenbarger & Hale, 1975; Epstein et al., 1976). Conversely, a lack of physical activity is associated with arhythmia and other indicators of circulatory impairment. Although the mechanics involved in fitness buffering against illness in the face of life events stressors are not established, a possible explanation may lie in the laboratory findings of McCaul, Solomon & Holmes (1979). The physiological strategy of paced respiration was found to be effective in reducing levels of arousal and anxiety for subjects in stressful situations. In terms of Rahe's model, persons with higher levels of fitness have less intense psychophysiological response in the face of life events stressors and thus are less likely to succumb to illness.
The Present Study
The present study examined both the independent and additive effects of personality hardiness and physical fitness as moderators of the effects of life events stressors.
A sample of middle-ranking army officers was chosen for the study. As well as being subjected to the stressors inherent in belonging to the profession of arms, the officers were at a stage in their careers where many might be expected to be subject to additional stressors as they made important decisions

17
regarding their future lives. Events which might impinge on the group included restriction on chances for further promotion; the desire to provide geographical stability for their children during secondary schooling; the financial benefits that accrue when a wife resumes her career as children become more independent; and the changes which occur when the familiar regimental and mess life are replaced by the more impersonal environment of high-rise office accommodation and integration into the civilian community. These events were viewed against the backdrop that indicated many of the officers would have qualified for retirement (pension) benefits and were at an age where they could readily commence a second career.
Hardiness has been shown to be a particularly discriminating instrument for use in studies of variables which moderate against illness in groups of professionals (including army officers) who are subjected to high levels of life events stressors (cf. Kobasa, 1982b). Additionally, as the population was one in which a formalized physical fitness regimen was accepted, the opportunity existed to examine the buffering effects that would accrue from adherence to the regimen.
Two retrospective investigations reported in the literature are fundamental to the current study. Using a sample of 157 lawyers Kobasa (1982a) found that personality buffered against the report of psychophysiological response and illness. Exercise (measured by self-report questionnaire as the number of hours per week spent in aerobic exercise) had no such buffering effect. In a similar study of 137 executives, Kobasa, Maddi and

18
Puccetti (1982) used a rating scale to quantify self-reports of exercise. Results indicated that personality hardiness and exercise buffered individually and additively against illness.
In the present study it was anticipated that the buffering effects of hardiness and fitness would operate discretely. Hardiness was expected to mediate against illness by facilitating the person's ability to perceive, evaluate and cope with stressors in a manner which would diminish the potency of the stressor. In contrast, fitness was expected to mediate against the intensity of the psychophysiological response to stressors, thus weakening the vital link in the life events stressors-illness relationship.

19
METHOD
Subj ects
A random sample of 130 male, middle-ranking army officers stratified for age, rank and work location was selected as the subject pool for the study. All subjects were serving in Army staff appointments in the Australian Capital Territory region. From this pool 105 subjects participated in the study; 16 were unavailable for administrative reasons (absence on duty or leave, work commitments for the duration of the study); and nine elected not to participate in the study. The sample size was reduced to 96 by the non-return of protocols (4) and the return of protocols after the data were processed (5).
Procedure
The original pool of 130 officers was mailed a composite questionnaire with a covering letter from the senior preventative medicine officer soliciting co-operation in the study. Participation was both voluntary and anonymous. A copy of the covering letter is at Appendix A. The questionnaire comprised the following measures:
1. Life events stressors for the immediately preceding 12 months period.

20
2. History of illness and psychophysiological response for the immediately preceding 12 months period.
3. Personality hardiness.
4. Demographic variables.
Each subject was invited to contact the researcher to make an appointment to attend a medical centre to undertake a submaximal test of physical fitness. There was a routine follow-up by telephone of all subjects who had failed to contact the researcher within 10 days of the despatch of questionnaires. Subjects with medical contra-indications were exempted from this facet of testing. To assist with the maintenance of anonymity, at the conclusion of the fitness testing subjects were presented with a record of their results and requested to mail both these results and their completed questionnaires to the researcher. A pre-addressed envelope was provided for administrative convenience.
Measures
Life Events Stressors
The Life Events Inventory (Tennant and Andrews, 1976), modified to accommodate population specific items, was used as the measure of life events stressors. This inventory was developed to embrace the two major principles on which the life

21
events-illness nexus had been posited : the magnitude of the change produced by the event (Holmes & Rahe, 1967) and the degree of emotional distress it caused (Paykel, Prusoff & Uhlenhuth, 1971). The 67 items in the inventory are grouped into eight broad categories. Tennant and Andrews (1976) provided a life change scaling and a distress scaling for each inventory item based on a survey of 151 Australian adults (78 males and 73 females). The sample was biased towards the upper socio-economic groups .
To maintain consistency with previous studies using the personality measure 'hardiness' as a mediator between life events stressors and illness, the concept of life change scalings was adopted for the present study in preference to the concept of distress scalings.
A group of eight army members not included in the subject pool was consulted to determine population specific life events for inclusion in the Life Events Inventory and to confirm the deletion of inapplicable items. As a result of the consultation 16 items were deleted from the inventory and 21 items selected for inclusion.
The 21 items which were added to the inventory were included in a questionnaire together with instructions for rating the amount of readjustment associated with each event in comparison with the index item 'marriage'. The instructions issued were those used in the development of the Social Readjustment Rating Scale (Holmes & Rahe, 1967, p 213). A copy

22
of the questionnaire was mailed to 200 middle-ranking army- officers sampled from the same population on a similar basis to, but exclusive of, the 130 officers in the subject pool. A covering letter from the researcher solicited co-operation in the survey. A pre-addressed envelope was provided to facilitate the return of completed protocols.
Respondents' ratings for individual items were summed and the mean value for each item calculated. The life change scaling for each event was determined pro-rata, on the basis of the ratio between the arbitrary value assigned to the index item (marriage) in the questionnaire, and the same item's scaling provided by Tennant and Andrews, ie. 500:59.
The details of the modification of the Life Events Inventory are at Appendix B. The modified Life Events Inventory and life change scalings used in the study are at Appendix C.
An inspection of the population specific scalings revealed no unexpected values. Being passed over for promotion and the submission of resignation from the Army were perceived as the events requiring the most readjustment. These events were subordinate only to Tennant and Andrews' scalings of events associated with death of an immediate family member and marriage/ divorce. At the lower end of the range was the requirement to make frequent work related trips of short duration. This event corresponded to the adjustment necessary following a significant positive change in financial status.

23
Psychophysiological Response
The measure of psychophysiological response used was the list of 16 physical and mental symptoms commonly associated with reactions to stressors developed by Kobasa (1982a) . The instrument, based on a sample of 75 adult male professionals, was found to have sound internal consistency (co-efficient alpha .85) and test-retest reliability (.80 after two weeks). Its validity as an indicator of health was shown by its significant correlation with reported illness (r = 0.35, £_ < .05).
In the present study subjects indicated the frequency with which each symptom was experienced in the 12 months preceding the study (zero = not at all; 1 = a little; 2 = quite a bit; and 3 = frequently). The list of symptoms and instructions to subjects are at Appendix E. A subject's psychophysiological response score was the sum of the responses to each item.
I1lness
A modified form of the Seriousness of Illness Rating Scale (Wyler, Masuda & Holmes, 1967) was used to measure the occurrence of diagnosable illness among subjects. This instrument is a self-report checklist of 126 common diagnosable illnesses. A severity scaling for each illness was obtained by asking a sample of medical practitioners and lay persons to rate

24
each in terms of seriousness. This scale has been used frequently in stress and illness studies (cf. Dohrenwend & Dohrenwend, 1974). Its reliability and validity as a complete listing of illnesses and an accurate set of seriousness scalings has been established by Wyler, Masuda and Holmes (1970).
Following consultation with senior Army medical officers, items deemed inappropriate for the study's population were deleted from the scale. These deletions included female specific illnesses and illnesses with age of onset sufficient to preclude military enlistment.
The modified scale with disease items in rank, order of seriousness and with associated seriousness of illness scales is at Appendix D.
Personality Hardiness
Personality hardiness was measured by the current generation Hardiness Test (3. R. Maddi, personal communication, June 14, 1985). This test has been well established as a measureof the degree of resistance afforded by personality against the negative effects of life events stressors on health (cf. Kobasa, 1979b, 1982b; Kobasa, et al., 1981; Kobasa, Maddi & Khan,1982; Kobasa, Maddi & Puccetti, 1982). As well as a composite hardiness score, the test provided scores on dimensions of commitment, control and challenge. The 50 item Hardiness Test is at Appendix F.

25
Physical Fitness
Maximum oxygen uptake (V02 max) was selected as the measure of physical fitness as it is correlated with cardiacoutput, myocardial oxygen consumption and blood flow. Given thevariations in age, levels of fitness and health of the subjectpool a procedure for estimating VO2 max from a submaximal test was adopted.
The cycle ergometer was selected as the test instrument. The technique involved is simple, the oxygen uptake can be predicted with greater accuracy than for any other type of exercise and, within limits, the mechanical efficiency is independent of body weight (Astrand & Rodahl, 1977).
Subjects completed a nine minute continuous multi-stage exercise test on the cycle ergometer in which they were required to attain three stable heart rate-workload responses. An electro-cardiograph was used to monitor heart rate during the test. The details of testing are at Appendix G.
For each subject the estimate of VO2 max was corrected for age, body weight and sex using the principles of Astrand (1960). Scores were expressed in terms of millilitres of oxygen per kilogram of body weight per minute. The details of this computation are at Appendix G. Subjects with medical contra-indications were exempted from this phase of testing and, a priori, allocated to the 'low fitness' group for data analysis.

26
Demographie Variables
The questionnaire included items which indexed age, marital status, smoking, work performance appraisal and result in the most recent Army physical training test (PTT) series.

RESULTS
Sample Characteristics
The 96 male subjects ranged in age from 30 to 54 years, with a mean of 39.2 years; 89.6% were married; and 26% were smokers. The sample had a mean height of 175cm and a mean weight of 79kg.
Ten subjects were exempted from the submaximal test of physical fitness because of medical contra-indications. Data from this phase of testing were split at the median to yield high and low fitness groups. The 10 subjects exempted from the fitness testing were assigned a priori to the low fitness group. Six subjects who were unavailable for administrative reasons during the period of fitness testing were assigned randomly to the high and low fitness groups.
1. Approval to conduct the study was conditional upon theauthor's non-reporting of data regarding individual life events, psychophysiological response or illness; and the deletion of Items 12, 14, 17 and 18 of themodified Life Events Inventory from the analysis ofdata.

28
Characteristics of Life Events Stressors, Psychophysiological Response and Illness
The scores for life events stressors ranged from 9 to 454 with a mean of 163.66 and a standard deviation of 92.1. The mean score corresponded to the occurrence of several significant events during the previous year.
The psychophysiological response scores ranged from zero to 30 with a mean of 4.32 and a standard deviation of 4.36. The small value for the mean and the large positive skewness (3.61) indicated that the majority of subjects reported few symptoms commonly associated with reaction to stressors.
Scores on the illness measure ranged from zero to 4741 with a mean of 811.14 and a standard deviation of 683.65. The mean score corresponded to the occurrence of a significant disorder and several minor illnesses during the previous year (e.g., hepatitis, hay fever, sore throat, common cold).
The Pearson product moment correlation between life events stressors and illness was 0.23 (jo = 0.12). This indicated that although some subjects reported illness in association with life events stressors, others reported one- without the other thus confirming the wide range of individual differences in the relationship. There was no correlation between life events stressors and psychophysiological response (r = 0.02). The correlation between illness and

29
psychophysiological response was 0.70 (jd = .001). This indicated that a significant number of subjects who reported diagnosable illness also reported a history of physical and psychological symptoms commonly associated with reactions to stressors.
Characteristics of Hardiness and Fitness
The scores on the hardiness measure ranged from 43.14 to 90.11 with a mean of 75.19, a standard deviation of 8.34 and skewness of -0.87. The mean and skewness scores were comparable to corresponding scores for a normative population (N = 1734;M = 72.49; skewness = -0.92), (S.R. Maddi, personalcommunication, November 27, 1985). The range and standarddeviation of scores in the present study were more constricted than with the normative group (Range = 21.1 to SD = 12.28).
The following characteristics were exhibited by scores on the three components of hardiness:
1 . Challenge : M = 33.37; SD = 5 . 1
2 . Commitment: M = 37.76; SD = 5.61
3. Control : M = 41.55; SD = 4.24

30
The scores on the fitness test (n_ = 80) ranged from22.5 to 70.5 with a mean of 37.54 and a standard deviation of9.47. When compared to normative data (Fitness Testing andExercising with the Repco Cycle Ergometer, 1972) the VO2 max scores ranged from low to very high, with the mean score fallingwithin the average band for the normative group.
Quartile splits were made with V02 max scores for those subjects who completed both the fitness test and the Army'sPTT (n_ = 75). These two measures of fitness were found to becorrelated significantly ( x2 = 18.63, df = 9, £ < .05).However, of those with VO2 max scores in the bottom 25% of the sample, 5 (6.67%) obtained results in the highest category offitness on PTT ('A' level pass). A further 7 (9.33%) obtained'B' level passes. In all, 14 subjects (18.67%) in the bottom 50%on VO2 max scores achieved 'A* level passes on PTT.Conversely, only one subject in the top 50% on VO2 max scorereported a PTT result which was other than an 'A1 or *B' levelpass (a 'C' level pass).
A chi-square test indicated that there were notsignificant differences between quartile splits on VO2 max scores across the three main elements of the Army : combat arms,support arms, services ( X2 = 6.89, df = 9).

31
Correlations of Life Events Stressors, Hardiness, Fitness and Demographics
There was no correlation between hardiness and fitness(r-jo, = -0.06). Similarly there was no pattern of relationship between these two moderator variables and demographics. The onesmall but significant correlation was between work performance appraisal and personality hardiness (r = 0.18, £ < .05). The trend was for more hardy individuals to be assessed by their superiors as being more competent in their work performance. Given that only one of the correlations between moderator variables and demographics reached a level of significance, the indication is that the effectiveness of the moderators could not have been attributed to demographics. The details of the interrelationships are summarized in Table 1.

32
Table 1
Interrelationships of Life Events Stressors, Hardiness,
Fitness and Demographics (N = 96)
Demographic
variables
Life events
stressors Hardiness Fitness
Age r = -0.03 r = 0.04 rb = “0 • 2 2
Marital status rpbi = 0 -05 rpbi = -0.03 in. r—i
50 II4-1
II P
CslX
Smoking rpbi = rPbi = -0 -11 X2 = 0.9,
df=l
Work performance
appraisal r = 0.08 r = 0.18a X2 = 0.77,
d f=2
a £ <-05
Analysis of Psychophysiological Response Data
Further analysis of psychophysiological response data
was suspended because a. there was no relationship between this
variable and life events stressors; and b. there was a marked
lack of normality in the distribution of the psychophysiological
response scores .

33
Illness as a Function of Life Events Stressors, Hardiness and Fitness
The distributions of scores of the independent variables (life events stressors, hardiness and fitness) were split at the medians to yield high and low categories. Mean illness scores were calculated for each category and the significance of the difference between means tested with the t. statistic. The results summarized in Table 2 indicated a significant difference between the mean illness scores for the high life events stressors-low hardiness group and the low life events stressors-low hardiness group {t_ = 2.23, df = 45,£ <.05). This suggested that those subjects who were less hardy were more likely to report a history of illness as life events stressors mounted. The results did not indicate that the level of physical fitness mediated significantly against the report of illness.

34
Table 2
Mean Illness as a Function of Life Events
Stressors, Hardiness and Fitness
Classification Mean Illness t n
High life events stressors
Low hardiness3 1148.59 ) 1.5 22
High hardiness 791.35 ) d f=46 26
Low fitness 973.31 ) 0.12 19
High fitness 943.14 ) d f=46 29
Low life events stressors
Low hardiness3 641.96 ) 0.36 25
High hardiness 694.61 ) d f=46 23
Low fitness 717.83 ) 0.07 19
High fitness 616.54 ) d f=45 28
Difference between these means significant (t_ - 2.23,
df=4 5 , 2. < • 2)5 )

35
The distributions of the three independent variables and the dependent variable (illness) were split at the medians to yield high and low categories. The correlations between life events stressors and illness scores, controlled for the effects of high and low hardiness, and high and low fitness are in Table 3. The results indicated a significant relationship between life events stressors and illness for the group of subjects in the low hardiness - low fitness group. The relationship was not significant for other categories.Apparently those subjects who were neither hardy nor physically fit were more likely to report a history of illness.
Table 3
Comparison of Life Events Stressors and Illness Frequency in Relation to Level of Fitness within High and Low Hardiness Groups
Classification n_ " Chi-Square value
High hardinessHigh fitness Low fitness
Low hardinessHigh fitness 28 X2= 1.45 df = 1Low fitness 19 Fisher's exact test = 0.05
25 x2 = r-CN df = 124 x2 = 0.12 df = 1

36
Multiple Regression with Illness as the Dependent Variable
A hierarchical stepwise regression analysis of life events stressors, hardiness and fitness on illness was conducted. The analysis was repeated with the three hardiness components (commitment, control and challenge) substituted for the composite hardiness score. The analyses summarized in Tables 4 and 5 indicated that in each instance the best combination of predictors of reported illness was the hardiness composite (or three hardiness components) and life events stressors. In the first regression equation personality hardiness made the greatest contribution to the prediction of reported illness (R = 0.18), with life events stressors adding a change in R of 0.06. In the second equation the hardiness component 'commitment' contributed the greatest amount to the prediction of reported illness (R^ = 0.10), followed in order by life events stressors (change in r2 of 0.05); challenge (change in r2 of 0.05); and control (change in R^ of 0.04). The level of physical fitness was not a significant predictor of reported history of illness.

37
Table 4
Hierarchical Stepwise Regression of Life Events Stressors, Hardiness and Fitness on Illness (N = 96)
Variable R2 B F £
Hardiness 0.18 -0.36 20.12 .0000Life events stressorsFitness3 (Constant)
0.24 1.89
3173.55
14.76 .0000
Variable did not reach 0.05 level of significance necessary for inclusion in equation.
Note: Durbin-Watson test 1.92

38
Table 5
Hierarchical Stepwise Regression of Life Events Stressors, Commitment, Control, Challenge and Fitness on Illness
Variable R2 B F R
Commitment 0.10 -1.75 10.70 .0015Life events stressors 0.15 1.70 8.39 .0004Challenge 0.20 -2.73 7.67 .0001Control 0.24 -1.32 7.01 .0001Fitnessa(Constant) 2595.57
a Variable did not reach 0.05 level of significance necessaryfor inclusion in equation.
Note: Durbin-Watson test = 1.9

39
DISCUSSION
As expected, those officers who reported higher incidences of life events stressors also reported correspondingly higher incidences of illness. The moderately strong correlation obtained (r = 0.23, p_ <.05) was consistent with those reported in the majority of similar studies (cf. Rabkin & Struening,1976). The pattern is, however, different from that observed by Kobasa (cited in Kobasa, 1982b) in a study of 75 US Army captains and majors. In the US sample an unusually strong relationship was found between life events stressors and illness (r = 0.58,2. <.001). This sample also displayed a level of hardiness lower than those displayed by two other groups of professionals (executives and lawyers) and, distinctively, the challenge component was associated with increased symptomatology.Apparently those US officers for whom safety, stability and predictability were deemed important were less suscepitble to illness than those officers who perceived changes as stimulating and opportunities for personal development.
Kobasa speculated that these patterns may have been attributable to the US Army's alleged difficulties in maintaining an all-volunteer force, and a lack of clarity in the Army's goals and purpose following the Vietnam war. The differences in patterns of life events stressors-illness relationships observed between different professional groups prompted Kobasa (1982b) to suggest that the unique structures and processes of the professions also contributed to the relationship. The results of

40
the present study appeared to support this suggestion, both in terms of the life events stressors-hardiness-illness relationship, and in the degree to which organisation specific life events stressors contributed to the overall stressor scaling. By way of example, being passed over for promotion was perceived by Australian Army officers as the organisation specific life events stressor which required the greatest amount of readjustment. For the officers promotion to the rank of major had been virtually automatic, however the chances of further promotion were pre-determined by the rank structure of the organisation to be in the order of 2:5 (beyond major) and 1:4 (beyond lieutenant colonel). Thus it was pre-ordained that a substantial majority of officers would be subjected to the organisation specific life events stressor perceived as requiring the greatest amount of readjustment. Accordingly Rahe's model should accommodate the characteristics of both the population under study and the organisational climate in which its members operate as mediators in the life events stressors-illness relationship.
The prediction that reported higher incidences of life events stressors would be associated with correspondingly higher levels of reports of psychophysiological response was not substantiated. Thus for the officers the report of psychophysiological response was not seen as a precursor to illness associated with life events stressors. The strong correlation between reports of psychophysiological response and illness (r = 0.70, jd = .001) suggested that officers experienced psychophysiological response in association with

41
illness irrespective of degree of life events stressors. The results also provided further validation of Kobasa's instrument as an indicator of health.
An explanation of this pattern of results may be found in Mechanic's (1976) concept of illness behaviour. Social psychological variables, including group norms and ideology, which influence the degree to which individuals will admit to symptomatology or illness may apply to officers. As a group they may readily report symptoms associated with diagnosable illness that prompt a consultation with a medical practitioner, but postpone reporting psychophysiological response or deny interpreting these symptoms as precursors of illness. To report psychophysiological response in the face of life events stressors may be contrary to officer ideology.
An alternative explanation would suggest that the officers who have survived to reach middle-rank level are those who have successfully cultured a range of stressor resistance resources. Thus the report of a low incidence of symptoms commonly associated with reactions to stressors may be a reflection of an attribute distinctive to army officers of this seniority.
The expectation that hardiness and each of its three components mediated against the report of illness was fulfilled. Additionally, the mediating effect of hardiness was found to be greatest when reported life events stressors mounted. An explanation of the manner in which hardiness operated as a

42
mediator can be seen in an adaptation of Kobasa's (1979b, p.9) illustration of the processes involved in an encounter with a typical life events stressor. In the present context the example is of an officer being posted to a different type of job in a new location.
Whether hardy or not, the officer will anticipate and experience the changes that will be consequences of the posting, such as learning to work with new superiors and subordinates, establishing his family in new accommodation in a new neighbourhood, and coping with the demands of a new job. The hardy officer will approach the necessary readjustments in his life with a clear sense of his values, goals and capabilities, and a belief in their importance (commitment to, rather than alienation from self); and a strong tendency towards active involvement with his environment (vigorousness rather than vegetativeness). Rather than passively acquiesce to the posting, the hardy officer involves himself actively in his new situation using his inner resources to make it his own. He maintains an unshakeable sense of meaningfulness of the posting in terms of his general career and life plans (meaningfulness rather than nihilism). The posting also represents a change which can be developmentally stimulating for his family. An internal (rather than external) locus of control allows the hardy officer to accept the posting with the recognition that although it may have been initiated at a higher level, the actual course it takes is dependent on how he handles it. Thus he is actively involved in the consequences of the posting rather than a passive victim of change. In contrast, the less hardy officer will react to his

43
posting with less sense of personal resource, more acquiescence, greater meaninglessness and a conviction that the change has been determined externally with no possibility of control on his part. In this context it is understandable that the hardy officer will also tend to perceive the posting as a less significant life events stressor than would the less hardy officer.
In the present study all three components of hardiness had a mediating effect against illness. The component which contributed most to the mediating effect was commitment (R.2 = 0.10). Thus the officers who were less likely to report a history of illness were those who had the ability to believe in the truth, importance and interest value of what they were doing (cf. Maddi, 1967; Maddi, cited in Kobasa, 1982b). This ability is reflected in the tendency to involve themselves fully across the spectrum of life situations including family, career, interpersonal relationships and social institutions. Interestingly, hardiness was found to correlate with officers' work performance appraisals (r = 0.18, jd <.05). As well as mediating against illness, hardiness appeared to be positively associated with characteristics which contribute to success in a military career. The application of the hardiness concept to performance assessment and predictive instruments may be worthy of further study.
A limitation of the present study is that prospective interpretation has to be inferred as all data were collected at the same time. Although, as discussed previously, the

44
prospective buffering effects of hardiness can be gauged from two studies (Kobasa et ai., 1981; Kobasa, Maddi & Khan, 1982) aprospective replication of the current study is required to confirm that causal relationships hold for a population of army officers.
The prediction that fitness would be a significant buffer between life events stressors and illness across the total sample was not substantiated. These findings appeared contrary to popularly held beliefs regarding health and fitness and the bulk of literature on the benefits of exercise as a mediator against illness (cf. Paffenbarger & Hale, 1975; Epstein et al., 1976; Paffenbarger et al., 1978; Everett, 1979; O'Connell &Price, 1982) .
Several possible explanations for the findings emerge. Firstly, the result may be an artefact of the methodology. The study was a retrospective one in which all measurements were taken at a single time. There is a possibility of inaccuracies in the recall of occurrences of illness in the previous 12 months. However it is contended that the officers in the study were more aware than most of the occurrence and severity of personal illness. They are subjected routinely to annual medical examinations; each is assigned an employment category on the basis of medical classification; and such matters as promotion and employment prospects are affected by this classification. Additionally, Kobasa (1982b) cited studies showing agreement between self-report of illness and physicians diagnoses ranging from 82% to 93% with a mean of 89%. The question of the

45
relationship between the current level of physical fitness and history of illness is more vexed. It may be argued that those officers who have experienced illness in the recent past have, either on their own initiative or in response to a medical practitioner's prescription, engaged actively in exercise in order to raise their level of fitness as part of their recuperative regimen and/or to provide a buffer against the possible future onset of illness.
Alternatively it may be argued that those officers who maintained a high level of fitness were more sensitive to fluctuations in body functioning and suffered more disruption to their health regimens by dysfunction. Hence they were more likely to be aware of, seek treatment for and thus report a history of illness. For the less fit group minor ailments would assume less significance than for the fit group. As the distress of illness assumed less importance, there may have been greater denial of the existence of dysfunction, or its presence may have gone undetected for a longer period. As a consequence the degree of illness reported by the less fit group may have been underestimated .
A third explanation may stem from the belief that only exercise over a long period of time mediates against illness. Paffenbarger et al., (1978) found that those adult males who have maintained a physically active life since childhood showed significantly more benefit from current exercise than those who have only commenced exercise as adults. In this regard there was homogeneity in the officer group: all had a record over a

46
considerable number of years of participating in strenuous physical activity and of routinely contesting Army PTT. The fitness regimens followed in their years as young officers may have developed predispositions which buffered against the effects of life events stressors, irrespective of the level of fitness maintained in later life.
A fourth possible explanation may lie in the role fitness played in the officers' health regimens. In a study of 842 adults Harris and Guten (1979) found that the most prevalent form of health protective behaviour was concerned with nutrition, food and eating conditions (71% of the sample), followed in order by sleep, rest and relaxation (46%); exercising, physical activity and physical recreation (36%); and contact with the health system (19%). If officers attached similar importance to fitness in their health-protective behaviour, it is expected that there would have been a consequential diminution in the role of fitness as a buffer against illness.
Although fitness was found not to mediate against illness across the total sample, those officers who were low on both hardiness and fitness were significantly more likely to report a history of illness than those high on either one or both variables. Apparently in the group of officers who were less hardy, a higher level of fitness compensated for the lack of hardiness in buffering against illness. As the effects of hardiness as a mediator against illness appeared to increase as life events stressors mounted, there would seem to be merit in officers maintaining a reasonable level of fitness to minimize susceptibility to illness associated with lack of hardiness.

47
The results in the present study did not accord with the findings in either of the similar studies reported by Kobasa (1982a) , and Kobasa, Maddi and Puccetti (1982). The current results, based on a more rigorous measure of physical fitness, suggested the role of fitness as a buffer against illness was not as universal for the officer group as for the executive group. However a relationship was reported which was not apparent in the sample of lawyers.
The current study has provided support for claims that hardiness buffers against illness and suggested that those army officers who are low on both hardiness and fitness are more susceptible to reporting a history of illness. A prospective replication of the study is required as the next stage of research in order to confirm these findings and attribute causality in relationships.
As predicted, personality hardiness and physicalfitness were unrelated (r^ = -0.06). These findings are consistent with those of Kobasa, Maddi and Puccetti (1982). Somehardy officers apparently include the maintenance of a reasonablelevel of fitness as part of their regimens but clearly there areothers who do not accept this course.
The Army PTT is currently used as a method of assessing the level of fitness maintained by officers. The results of the present study raised doubts regarding the validity of this method of assessment. Although PTT results correlated positively with a physiological measure of fitness, VO2 max, (n. = 75,
48
= 18.63, df = 9, p <.05) a proportion of the group wasmisclassified. Even if some allowance is made for variations inskill on individual test items, there would still appear to be areasonable number of officers who achieved 'superior' results onPTT despite having lower levels of physical fitness in comparisonwith both their peers and the population at large. There were6.67% of the officers in the bottom 25% on VO2 max scores who obtained 'A' level passes and a further 9.33% who obtained 'B‘level passes. A total of 18.67% of officers in the bottom 50% ofthe sample on VO2 max scores achieved 'A' level passes.
These results suggested some less fit officers may have subjected themselves to undue strain and thereby placed themselves unnecessarily at risk physically in order to achieve higher level PTT results. A review of the current PTT policies would appear prudent, with particular emphasis being directed towards the identification, monitoring and, if necessary, the protection of officers in the 'at risk' categories.
Tnis study has confirmed both the utility of personality hardiness as a mediator against illness and its independence from physical fitness and demographic variables. Additionally, the contributions made to the life events stressors-illness relationship by the characteristics of the population under study and the organisational climate in which its members operate were highlighted.

49
If, as Kobasa (1979a) contends, hardiness is a personality style that is learned, there appears to be scope for studies which seek to isolate learning experiences and organisational structures which will develop, promote and sustain hardiness. The incorporation of the hardiness concept into organisational theory would be a positive step towards mediating against the effects of inevitable life events stressors. For example, an organisation could assist its executives buffer against illness by adopting policies which foster a sense of purpose and active involvement (commitment rather than alientation); a quest for novelty and challenge (rather than familiarity and security); and a feeling that the executives have the power to exercise control over their own lives (rather than being controlled externally).
The notion of fostering personality hardiness as a buffer against life events stressors flies in the face of widely held beliefs regarding the management of the effects of stressors. Many of these beliefs are based on the premises that illness is the inevitable consequence of exposure to these stressors; these stressors must be avoided or at least minimized; and rest and relaxation are primary life goals. The present study calls these beliefs into question. The incidence of illness associated with life events stressors is small; stressors can be encountered successfully, and moderators can be developed to offset the effects of the stressors.

50
REFERENCES
Adair, A.R . (1984). Shortfalls in the Australian Army physicaltraining tests system. Combat Arms, 4_, 43-44.
Andrews, G., & Tennant, C. (1978). Editorial: Life event stressand psychiatric illness. Psychological Medicine, 8_,545-549.
I
Astrand, I. (I960). Aerobic work capacity in men and women with special reference to age. Acta Physiologica Scandinavia,49 (Suppl. 169), 1-92.
Astrand, P-0., & Rodahl, K. (1977). Textbook of work physiology♦ New York : McGraw-Hill.
Astrand, P-0., & Ryhming, I. (1954). A nomogram for calculation of aerobic capacity (physical fitness) from pulse rate during submaximal work. Journal of Applied Physiology,7_, 218-221.
Averill, J.R. (1973). Personal control over aversive stimuli and its relationship to stress. Psychological Bulletin, 80, 286-303.
Beehr, T.A . (1983). Relationship of the Life Experiences Survey to internal/external control, social desirability, and work-related satisfaction. Psychological Reports, 52,467-472.

51
Betz, B.J. & Thomas, G.B. (1979). Individual temperament as a predictor of health or premature disease. The Johns Hopkins Medical Journal, 144 ( 3) , 81-89.
Blackinton, J.G. (1981). Locus of control and moods as affected by aerobic exercise. Dissertation Abstracts International, 42_(05), 20423-20433.
Bonds, A.G. (1980). The relationship between self-concept andlocus of control and patterns of eating, exercise and social participation in older adults. Dissertation Abstracts International, 4] (04), 1397A.
Bryant, B.K., & Trockel, J.F. (1976). Personal history ofpsychological stress related to locus of control orientation among college women. Journal of Consulting and Clinical Psychology, 44(2), 266-271.
Byrne, D.G. (1981). Type A behaviour, life-events and myocardial infarction : Independent or related risk factors? BritishJournal of Medical Psychology, 54, 371-377.
Byrne, D.G. (1984). Personal assessments of life-event stress and the near future onset of psychological symptoms.British Journal of Medical Psychology, 57, 241-248.
Cobb, S., & Rose, R.M. (1973). Hypertension, peptic ulcer, and diabetes in air traffic controllers. JAMA, 224(4) ,489-492.

52
Cohen, F. (1979). Personality, stress, and the development of physical illness. In G.C. Stone, F. Cohen, & N.E. Adler (Eds.), Health Psychology ; A Handbook (pp. 77-111).San Francisco : Jossey-3ass Publishers.
Cooley, E.J., & Keesey, J.C. (1981). Moderator variables in life stress and illness relationship. Journal of Human Stress,7_( 3 ) , 35-40.
Corbin, D.E. (1982). Psychological and physical aspects of self-perceived health status among older adults.Dissertation Abstracts International, 43_(06), 1842A.
Cunningham, J. (1980). The effects of exercise and relaxation training upon psychological variables in coronary heart patients. Dissertation Abstracts International, 4_1_(06) , 23133-2314B.
D'Amato, K.R. (1981/1982). The effects of cardiovascularefficiency on psychological and physiological variables in women. Dissertation Abstracts International, 43(01),244B.
Dembroski, T.M., Weiss, S.M., Shields, J.L., Haynes, S.G., &Feinlab, M. (Eds.). (1978). Coronary prone behaviour.New York : Springer-Verlag.
Denney, D.R., & Frisch, M.B. (1981). The role of neuroticism in relation to life stress and illness. Journal ofPsychosomatic Research, 25(4), 303-307.

53
Directorate-General of Air Force Health Services. (Undated). Personal Health - Aerobic power assessment (Health Services Circulars - Environmental Health 5-3). Canberra: Royal Australian Air Force.
Dodge, D.L., & Martin, W.T. (1970). Social stress and chronic illness. Notre Dame : University of Notre Dame Press .
Dohrenwend, B.P. (1961). The social psychological nature of stress : A framework for causal inquiry. Journal of Abnormal and Social Psychology, 62_(2), 294-302.
Dohrenwend, B.P., & Dohrenwend, B.S. (1969). Social status and Psychological disorder : A causal inquiry. New York : Wiley-Interscience.
Dohrenwend, B.S., & Dohrenwend, B.P. (Eds.). (1974). Stressfullife events : Their nature and effects. New York :John Wiley & Sons.
Dohrenwand, B.S., & Dohrenwend, B.P. (1978). Some issues inresearch on stressful life events. The Journal of Nervous and Mental Disease, 166(1) , 7-15.
Dohrenwend, B.S., Dohrenwend, B.P., Dodson, M., & Shrout, P.E. (1984). Symptoms, hassles, social supports, and life events: Problem of confounded measures. Journal ofAbnormal Psychology, 9^(2), 222-230.

54
Doty, D.A . (1981/1983). Moderator variables of the effects ofstressful life events. Dissertation Abstracts International, 43_(07), 23323.
Epstein, L., Miller, G.J., Stitt, F.W., & Morris, J.N. (1976). Vigorous exercise in leisure time, coronary risk factors, and resting electrocardiogram in middle-aged civil servants. British Heart Journal, 38, 403-409.
Everett, M.D. (1979). Strategies for increasing employees' level of exercise and physical fitness. Journal of Occupational Medicine, 2J (7), 463-467.
Fairbank, D.T., & Hough, R.L. (1979). Life event classifications and the event-illness relationship. Journal of Human Stress , 5_(3 ) , 41-47.
Finlay-Jones, R.A., & Murphy, E. (1979). Severity ofpsychiatric disorder and the 30-item General Health Questionnaire. British Journal of Psychiatry, 134,609-616.
Fitness testing and exercising with the Repco cycle ergometer. (1972). Melbourne : Repco.
Floria, D.L. (1982/1983). The impact of health locus of control and health value on self-care health behaviour.Dissertation Abstracts International, 43_(07), 2153B.

55
Freeman, Z. (1985). Stress, type-A behaviour and infarction.
The Medical Journal of Australia, 142, 5-6.
Ganellen, R.J. & Blaney, P.H. (1984). Hardiness and social
support as moderators of the effects of life stress.
Journal of Personality and Social Psychology, 47(1),
156-163.
Gilbert, L.A. (1976). Situational factors and the relationship
between locus of control and psychological adjustment.
Journal of Counseling Psychology, 23_(4), 302-309.
Gilbert, L.A., & Mangelsdorff, D. (1979). Influence of
perceptions of personal control on reactions to stressful
events. Journal of Counseling Psychology, 26(6),473-480.
Goldberg, D.P. (1972). The detection of psychiatric illness by
questionnaire. London : Oxford University Press.
Goldberg, E.L., & Comstock, G.W. (1976). Life events and
subsequent illness. American Journal of Epidemiology,
104(2), 146-158.
Goldberg, E.L., & Comstock, G.W. (1980).
Epidemiology of life events : Frequency in general
populations. American Journal of Epidemiology, 111(6),
736-752.

56
Goldman, L. (1984, September). Heart disease and type Abehaviour : Is there really a connection? Modern Medicine of Australia, pp. 87-88.
Gottlieb, B.H. (1983). Social support as a focus for integrative research in psychology. American Psychologist, 38(3), 278-287.
Guilford, J.P., & Fruchter, B. (1978). Fundamental statistics in psychology and education (6th ed .). Auckland: McGraw-Hill.
Harris, D.M., & Guten, S. (1979). Health-protective behaviour : An exploratory study. Journal of Health and Social Behaviour, 20, 17-29.
Henderson, A.S. (1984). Interpreting the evidence on social support. Social Psychiatry, 19, 49-52.
Henderson, S., Byrne, D.G., & Duncan-Jones, P. (1981). Neurosis and the social environment. Sydney : Academic Press .
Heno, J.W. (1976). The relationship of psychosocial stressors (life change), locus of control and field dependence to illness susceptibility. Dissertation Abstracts I nt er national, 3_7_ (3 ) , 1476B.
Holmes, T.H., & Masuda, M. (1974). Life change and illness susceptibility. In B.S. Dohrenwend, & B.P. Dohrenwend (Eds.), Stressful life events: Their nature and effects(pp. 45-72). New York: John Wiley & Sons.

57
Holmes, T.H., & Rahe, R.H. (1967). The Social Readjustment Rating Scale. Journal of Psychosomatic Research, 11,213-218.
Horowitz, M.J. (1976). Stress response syndromes. New York : Jason Aronson.
Horowitz, M., Schaefer, C., Hiroto, D., Wilner, N., & Levin, B.(1977). Life event questionnaires for measuring presumptive stress. Psychosomatic Medicine, 39_(6), 413-431.
Howley, F.M. (1983). The transfer of healthsport behaviours of disabled persons from training program site to home community. Dissertation Abstracts International,43_(J9), 2959A-2960A.
Hull, C.H., & Nie, N.H. (1981). SPSS update 7-9. New York : McGraw Hill.
Husaini, B.A., Sc Neff, J.A. (1981). Social class and depressive symptomatology : The role of life change events and locus of control. The Journal of Nervous and Mental Disease,169(10), 638-647.
Jenkins, C.D. (1979). Psychosocial modifiers of response to stress. Journal of Human Stress, 5_(4), 3-15.

58
Jenkins, C.D., Rosenman, R.H., & Friedman, M. (1967).Development of an objective psychological test for the determination of the coronary-prone behaviour pattern in employed men. Journal of Chronic Disorders, 20, 371-379.
Jenkins, C.D., Rosenman, R.H., & Zyzanski, S.J. (1974).Prediction of clinical coronary heart disease by a test for the coronary-prone behaviour pattern. The New England Journal of Medicine, 290(23), 1271-1275.
Johnson, J.H., & Sarason, I.G. (1978). Life stress, depression and anxiety: Internal - external control as a moderatorvariable. Journal of Psychosomatic Research, 22,205-208.
Jones, J.P. (1983). The effects of increasing physical fitness level on locus of control, self concept, and reported changes in lifestyle dimensions. Dissertation Abstracts I nternational, 44 (05), 1373A.
Kessler, R.C. (1979). A strategy for studying differentialvulnerability to the psychological consequences of stress. Journal of Health and Social Behaviour, 20, 100-108.
Kessler, R.C., Price, R.H., & Wortman, C.B. (1985). Socialfactors in psychopathology: Stress, social support, andcoping processes. Annual Review of Psychology, 36,531-572.

59
King, M.G., Burrows, G.D., & Stanley, G.V. (1983). Measurement of stress and arousal : Validation of the stress/arousal adjective checklist. British Journal of Psychology, 74, 473-479.
King, M.G., Stanley, G.V., & Burrows, G.D. (1984). Stress, combat and tactical decisions. Defence Force Journal,44, 9-15.
Klecka, W.R., Nie, N.H., & Hull, C.H. (1975). Statistical package for the social sciences primer. New York : McGraw-Hill.
Kobasa, S.C. (1979a). Personality and resistance to illness. American Journal of Community Psychology, 1_ (4),413-423.
Kobasa, S.C. (1979b). Stressful life events, personality, andhealth : An inquiry into hardiness. Journal of Personality and Social Psychology, 37 (1), 1-11.
Kobasa, S.C. (1982a). Commitment and coping in stress resistance among lawyers. Journal of Personality and Social Psychology, 42 (4), 707-717.
Kobasa, S.C. (1982b). The hardy personality : Toward a socialpsychology of stress and health. In G.S. Sanders & J. Suls (Eds.), Social psychology of health and illness(pp. 3-32). Hillsdale, NJ: Lawrence Erlbaum Associates.

60
Kobasa, S.C., Hilker, R.R.J., & Maddi; S.R. (1979). Who stays healthy under stress? Journal of Occupational Medicine, 21(9), 595-598.
Kobasa, S.C., & Maddi, S.R. (1977). Existential personality theory. In R.J. Corsini (Ed.). Current personality theories (pp. 243-276). Itasca, IL : Peacock.
Kobasa, S.C., Maddi, S.R., & Courington, S. (1981). Personality and constitution as mediators in the stress - illness relationship. Journal of Health and Social Behaviour,22, 368-378.
Kobasa, S.C., Maddi, S.R., & Kahn, S. (1982). Hardiness andhealth : A prospective study. Journal of Personality and Social Psychology, 42_(1), 168-177.
Kobasa, S.C., Maddi, S.R., & Puccetti, M.C. (1982). Personality and exercise as buffers in the stress - illness relationship. Journal of Behavioural Medicine, 5_ (4), 391-404.
Kobasa, S.C., Maddi, S.R., & Zola, M .A . (1983). Type A andhardiness. Journal of Behavioural Medicine, 6_ (1)/41-51.
Kobasa, S.C.O., & Puccetti, M.C. (1983). Personality and social resources in stress resistance. Journal of Personality andSocial Psychology, 45 (4), 839-850.

61
Krantz, D.S., Grunberg, N.E., & Baum, A. (1985). Healthpsychology. Annual Review of Psychology, 36, 349-383.
Krantz, D.S., & Manuck, S.B. (1984). Acute psychophysiologicreactivity and risk of cardiovascular disease : A review and methodological critique. Psychological Bulletin, 96 (3), 435-464.
La Rocco, J.M., House, J.S., & French, J.R.P., Jr. (1980).Social support, occupational stress, and health. Journal of Health and Social Behaviour, 21, 202-218.
Langley, T.D. (1983). The relationship of success in a weight loss - fitness program and locus of control of reinforcement. Dissertation Abstracts International, 44 (05), 134 3A .
Lazarus, R.S. (1961). Adjustment and personality. New York : McGraw-Hill.
Lazarus, R.S. (1966). Psychological stress and the coping process. New York: McGraw-Hill.
Lazarus, R.S. (1967). Cognitive and personality factorsunderlying threat and coping. In M.H. Appley & R. Trumball (Eds.), Psychyological stress (pp. 151-181). New York :Appleton - Century - Crofts.

62
Lee, D.Y., Hallberg, E.T., Hassard, J.H., & Haase, R.F. (1979). Counselor-trainees1 blame-assignment and commitment to change as a function of locus of control and success and failure feedback. Journal of Clinical Psychology, 35 (4), 747-753.
Lefcourt, H.M. (1980). Locus of control and coping with life's events. In E. Staub (Ed.), Personality: Basic issues andcurrent research (pp. 200-235). Englewood Cliffs, NJ: Prentice-Hall.
Lefcourt, H.M., Martin, R.A., & Saleh, W.E. (1984). Locus of control and social support : Interactive moderators ofstress. Journal of Personality and Social Psychology,£7_ (2) , 378-389 .
Lester, D., Leitner, L.A., & Posner, I. (1983). Recent lifeevents and stress scores : An examination of the Holmes and Rahe Scale. Psychological Reports, 53, 70.
Lester, D., & Tappert, E. (1931). Subjective stress and internal - external locus of control. Perceptual and Motor Skills, 5_3, 590.
Levenson, R.W., & Ditto, W.B. (1981). Individual differences in ability to control heart rate : Personality, strategy, physiological, and other variables. Psychophysiology,18 (2), 91-100.

63
Levine, L.B. (1978/1979). The relationship between life stress, locus of control and attrition in baccalaureate nursing students. Dissertation Abstracts International, 39 (11), 5520B.
Lin, N., Simeone, R.S., Ensel, W.M., & Kuo, W. (1979). Socialsupport, stressful life events, and illness : A model and an empirical test. Journal of Health and Social Behaviour,20, 108-119.
Linn, M.W., Linn, B.S., & Harris, R. (1981). Stressful lifeevents, psychological symptoms, and psychosocial adjustment in anglo, black, and Cuban elderly. Social Science and Medicine, 15E, 283-287.
Lipkin, M. Jr., & Kupka, K. (Eds.). (1982). Psychosocialfactors affecting health. New York : Praeger.
Louhevaara, V., Ilmarinen, J., & Oja, P. (1985). Comparison of three field methods for measuring oxygen consumption. Ergonomics, 28 (2), 463-470.
Luscomb, R.L., Clun, G.A., & Patsiokas, A.T. (1980). Mediating factors in the relationship between life stress and suicide attempting. The Journal of Nervous and Mental Disease,168 (11), 644-650.
Maddi, S.R. (1967). The existential neurosis. Journal of Abnormal Psychology, 72 (4), 311-325.

64
Maddi, S.R., Hoover, M., & Kobasa, S.C. (1982). Alienation andexploratory behaviour. Journal of Personality and Social P sychology, 42 (5), 884-890.
Maddi, S.R., & Kobasa, S.C. (1981). Intrinsic motivation and health. In H.J. Day (Ed.), Advances in intrinsic motivation and aesthetics (pp. 299-321). New York : Plenum Press.
Maddi, S.R., Kobasa, S.C., & Hoover, M. (1979). An alienation test. Journal of Humanistic Psychology, 19 (4), 73-76.
Mahoney, M.J. (1978). Experimental methods and outcome evaluation. Journal of Consulting and Clinical Psychology, 46 (4), 660-672.
Manuck, S.B., Hinrichsen, J.J., & Ross, E.O. (1975a). Life stress, locus of control, and state and trait anxiety. Psychological Reports, 36, 413-414.
Manuck, S.B., Hinrichsen, J.J., & Ross, E.O. (1975b). Life stress, locus of control, and treatment seeking. Psychological Reports, 37, 589-590.
Masuda, M., & Holmes, T.H. (1978). Life events : Perceptions and frequencies. Psychosomatic Medicine, 40_(3), 236-261.

65
McCaul, K.D., Solomon, S., & Holmes, D.S. (1979). Effects of paced respiration and expectations on physiological and psychological responses to threat. Journal of Personality and Social Psychology, 37, 564-571.
McFarlane, A.H., Norman, G.R., Streiner, D.L., & Roy, R.G.(1983). The process of social stress : stable, reciprocal, and mediating relationships. Journal of Health and Social Behaviour, 24, 160-173.
Mechanic, D. (1976). Stress illness and illness behaviour. Journal of Human Stress, 2_, 2-6.
Miller, M.B. (1981/1982). Individual differences and felt stress in work. Dissertation Abstracts International,42_(0 7 ) , 3 2 24A .
Monat, A., & Lazarus, R.S. (Eds.). (1977). Stress and coping.New York : Columbia University Press.
Morgan, C.H., Jr. (1979/1980). Personality factors and stress ratings of life changes in a college population. Dissertation Abstracts International, 40_(9), 4496B .
Mueller, D.P., Edwards, D.W., & Yarvis, R.M. (1978). Stressful life events and community mental health center patients. The Journal of Nervous and Mental Disease, 166(1),16-24.

66
Nettier, G. (1957). A measure of alienation. American Sociological Review, 22_(6 ), 670-677.
Nie, N.H., Hull, C.H., Jenkins, J.G., Steinbrenner, K.,& Bent, D.H. (1975). Statistical package for the social sciences (2nd ed.). New York : McGraw-Hill.
Nowicki, S., Jr. (1978). Reported stressful events duringdevelopmental periods and their relation to locus of control orientation in college students. Journal of Consulting and Clinical Psychology, 46_(6), 1552-1553 .
Paffenbarger, R.S., Jr., Sc Hale, W.E. (1975 ). Work activity and coronary heart mortality. New England Journal of Medicine, 292, 545-550.
Paf f enbarger, R.S., Jr., Wing, A.L., Sc Hyde, R.T. (1978).Physical activity as an index of heart attack in college alumni. American Journal of Epidemiology, 108, 161-175.
Parkes, K.R. (1984). Locus of control, cognitive appraisal, and coping in stressful episodes. Journal of Personality and Social Psychology, 46_(3), 655-668.
Patterson, J.A. (1981/1982). Health beliefs and health locus of control as predictors of cardiorespiratory endurance in adults enrolled in prescriptive exercise programs. Dissertation Abstracts International, 43_(04), 1044B.

67
Paykel, E.S., Prusoff, B.A., & Uhlenhuth, E.H. (1971). Scaling of life events. Archives of General Psychiatry, 25,340-347.
Pearlin, L.I., Lieberman, M.A., Menaghan, E.G., & Mullen, J.T.(1981). The stress process. Journal of Health and Social Behaviour, 22, 337-356.
Perri, S., II. (1981/1982). The effects of an aerobics exercise program on psychological and physiological variables in the elderly. Dissertation Abstracts International, 43(01),259B.
Rabkin, J.G., & Struening, E.L. (1976). Life events, stress, and illness. Science, 194, 1013-1020.
Rahe, R.H. (1974). The pathway between subjects' recent life changes and their near-future illness reports:Representative results and methodological issues. In B.S. Dohrenwend & B.P. Dohrenwend (Eds.), Stressful life events: Their nature and effects (pp. 73-86). New York:John Wiley & Sons.
Rahe, R.H. (1979). Life change events and mental illness : An overview. Journal of Human Stress, 5_(3) , 2-10.
Rahe, R.H. (1981). Development in life change measurements :Subjective life change unit scaling. In B.S. Dohrenwend, & B.P. Dohrenwend (Eds.), Stressful life events and their contexts (pp. 48-62). New York : Academic Publications.

68
Rahe, R.H., 6c Arthur, R.J. ( 1 9 7 8 ) . Life change and illnessstudies : Past history and future directions. Journal of Human Stress, 4_(1), 3-15.
Rahe,R.H., Ryman, D.H., 6c Ward, H.W. (1980). Simplified scaling for life change events. Journal of Human Stress, 6 (4), 22-27.
Rhodewalt, F., 6c Agustsdottir. (1984). On the relationship ofhardiness to the Type A behaviour pattern : Perception of life events versus coping with life events. Journal of Research in Personality, 18, 212-223.
Ross,C.E., 6c Mirowsky, J., II. (1979). A comparison of life- event-weighting schemes : Change, undesirability, and effect-proportional indices. Journal of Health and Social Behaviour, 20, 166-177 .
Rotter, J.B. (1966). Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs : General and Applied, 80_( 1) , 1-28.
Ryckman, R.M., 6c Malikiosi, M. ( 1 9 7 4 ) . Differences in locus of control orientation for members of selected occupations. Psychological Reports, 3 4 , 1 2 2 4 - 1 2 2 6 .

69
Sarason, I.G., & Sarason, B.R. (1984). Life changes, moderators of stress, and health. In A. Baum, S.E. Taylor, & J.E. Singer (Eds.), Handbook of psychology and health : Vol. 4. Social psychological aspects of health (pp. 279-299). Hillsdale, NJ : Lawrence Erlbaum.
Schill, T., Ramanaiah, N., & Toves, C. (1982). Defensive externality and vulnerability to life stress.Psychological Reports, 51, 878.
Schoeneman, S.Z., Reznikoff, M., & Bacon, S.J. (1983).Personality variables in coping with the stress of a spouse's chronic illness. Journal of Clinical Psychology, 39(3), 430-436.
Schroeder, D.H., & Costa, P.T., Jr. (1984). Influence of life event stress on physical illness : Substantive effects or methodological flaws? Journal of Personality and Social P sychology, 46_(4), 853-863.
Seeman, M. (1959). On the meaning of alienation. American Sociological Review, 24_(6), 783-791 .
Selye, H. (1976) . The stress of life (rev. ed.) New York, : McGraw-Hill.
Simeone, R.S. (1979/1980). An examination of the effects of stressors, social support, and psychological resources on depressive symptomatology. Dissertation Abstracts International, 41(01), 415B.

70
Singer, J.L. (1984). The private personality. Personality and Social Psychology Bulletin, 10_(1), 7-30.
Solvesson-Lane, S.A-G. (1980). Life transitions : Friend or foe? Self-concept, flexibility and locus of control as moderator variables. Dissertation Abstracts International, 41 (04), 1529B.
Sonstroen, R.J., & Walker, M.I. (1973). Relationship ofattitudes and locus of control to exercise and physical fitness. Perceptual and Motor Skills, 36, 1031-1034.
Srole, L. (1956). Social integration and certain corollaries : An exploratory study. American Sociological Review, 21, 709-716.
Surwit, R.S., Shapiro, D., & Good, M.I. (1978). Comparison of cardiovascular biofeedback, neuromuscular biofeedback, and meditation in the treatment of borderline essential hypertension. Journal of Consulting and Clinical Psychology, 46_(2 ), 252-263.
Surwit, R.S., Williams, R.B., Jr., & Shapiro, D. (1982).Behavioural approaches to cardiovascular disease. New York : Academic Press.
Tausig, M. (1982). Measuring life events. Journal of Health and Social Behaviour, 23, 52-64.

71
Tennant, C., & Andrews, G. (1976). A scale to measure thestress of life events. Australian and New Zealand Journal of Psychiatry, 10, 27-32.
Tennant, C., & Andrews, G. (1978). The pathogenic quality of life events stress in neurotic impairment. Archives of General Psychiatry, 35, 859-863.
Toves, C. Schill, T., & Ramanaiah, N. (1981). Sex differences, internal - external control, and vulnerability to life stress. Psychological Reports, 49, 508.
Ursin, H. (1980). Personality, activation and somatic health : A new psychosomatic theory. In E. Levine, & H. Ursin (Eds.), Coping and health (pp. 259-279). New York : Plenum Press.
Vinokur, A., & Selzer, M.L. (1975). Desirable versusundesirable life events : Their relationship to stress and mental distress. Journal of Personality and Social Psychology, 3_2_(2), 329-337 .
Wallston, B.S., Wallston, K.A., Kaplan, G.D., & Maides, S.A.(1976). Development and validation of the Health Locus of Control (HLC) Scale. Journal of Consulting and ClinicalP sychology, 44(4), 583-585.

72
Wallston, K.A., & Wallston, B.S. (1981). Health locus ofcontrol scales. In H.M. Lefcourt (Ed.), Research with the locus of control construct : Vol. 1. Assessment methods (pp. 189-243). New York : Academic Press.
Wallston, K.A., Wallston, B.S., & De Vellis, R. (1978).Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Education Monographs, 6_(2),160-170.
Wan, T.T.H. (1982). Stressful life events, social supportnetworks and gerentological health : a prospective study.Us : Gower.
Weiman, J.B. (1980). Running as treatment for depression : A theoretical basis. Dissertation Abstracts International, 41_(0 5 ) , 1935B-1936B.
Wendt, B.R. (1982). The role of hardiness as a mediator between stress and illness among adolescents. Dissertation Abstracts International, 43_(3), 891B.
Wyler, A.R., Masuda, M., & Holmes, T.H. (1968). Seriousness of Illness Rating Scale. Journal of Psychosomatic Research, 11, 363-374.
Wyler, A.R., Masuda, M., & Holmes, T.H. (1970). Seriousness of Illness Rating Scale : Reproducibility. Journal ofPsychosomatic Research, 14, 59-64.

73
Wyler, A.R., Masuda, M., & Holmes, T.H. (1971). Magnitude of life events and seriousness of illness. Psychosomatic Medicine, 33_(2 ) , 115-122.
Zastrow, C. (1984). Understanding and preventing burn-out. British Journal of Social Work, 14 141-155.
Zimmerman, M. (1983). Weighted versus unweighted life eventscores : Is there a difference? Journal of Human Stress,9(4), 30-35.

74
Appendix A:Letter to Subject Pool
(Subject's Name)
The Chief of Personnel has approved a survey to investigate the level of physical fitness of officers serving in the Canberra region, the incidence of recent illness in the group and their opinions and attitudes to various health and social issues. The study will provide data which will enable the staff to review current policies on physical fitness and health care. The project officer is (researcher's name).
You are one of 130 officers selected randomly and invited to participate in the survey. Participation is both voluntary and anonymous: identifying data will not be recordedon survey material.
The survey comprises two phases:
a. the completion of the enclosed questionnaire; and
b. a physical fitness assessment in which your heart rate will be monitored while you pedal a cycle ergometer. This assessment will take approximately eleven minutes and be conducted at JSHC. It is recommended PT gear be worn for the assessment.
Should you agree to participate in the study please bring your completed questionnaires to JSHC when you attend for

75
your fitness assessment. An appointment for this assessment should be made with (the researcher) on (telephone number).
If you have medical restrictions which preclude your participation in the physical fitness assessment, please contact (the researcher) for instructions regarding the disposal of your completed questionnaire.
Thank you for your co-operation.

76
Appendix B:Modification of the Life Events Inventory
Table B-l
The Life Events Inventory
Life change__________________ Event_______________________________scalings
HEALTH (Men and Women)
1. You had a minor illness or injury like one needing a visit to a doctor or a couple ofdays off work. 2
2. You had a serious illness, injury or operation needing hospitalization or a month or more offwork. 16
3. A close relative had a serious illness (fromwhich they did not die). 9
(Women Only)
4. You are pregnant (with a wanted pregnancy). 26

77
Event
5. You are pregnant (with an unwanted pregnancy).
6. You had a stillbirth.
7. You had an abortion or miscarriage.
8. You had a baby.
9. Your change of life (menopause) began.
10. You adopted a child.
(Men Only)
11. Your wife had a child or you adopted a child.
BEREAVEMENT (Men and Women)
12. Your wife/husband died.
13. A child of yours died.
14. A close family member died (eg. parent, brother, etcj.
15. A close family friend or relative died (e.g., aunt, uncle, grandmother, cousin, etc.) .
Life change sealings
29
22
13
47
18
47
41
79
57
27
12

78
Life changeEvent scalings
FAMILY AND SOCIAL (if you are or were married)
16. You married. 59
17. There has been increasing serious argumentswith your wife/husband. 25
13. There has been a marked improvement in the wayyou and your wife/husband are getting on. 18
19. You have been separated from your husband/wife for more than a month because of maritaldifficulties. 29
20. You have been separated from your wife/husband for more than a month (for reasons otherthan marital difficulties). 15
21. You have got back together again after aseparation due to marital difficulties. 25
22. You began an extramarital affair. 28
23. Your wife/husband began an extramarital affair. 28
24. You have been divorced. 62

79
Life changeEvent sea lings
(If you have or had children)
25. A child of yours became engaged. 6
26. A child of yours married with your approval. 10
27. A child of yours married without yourapproval. 16
28. A child of yours left home for reasons otherthan marriage. 14
29. A child of yours entered the armed services. 10
(if you are single)
30. You became engaged or began a "steady"relationship. 17
31. You broke off your engagement. 21
32. You broke off a "steady" relationship. 18
33. You had increasing arguments or difficultieswith your fiance or steady friend. 13
FRIENDS AND RELATIVES
34. a new person came to live in your household(apart from a new baby). 20

EventLife change scalings
35. There has been a marked improvement in the way you get on with someone close to you(excluding husband and wife). 10
36. You have been separated from someone importantto you (other than close family members). 13
37. There has been serious increase in argumentsor problems with someone who lives at home (excluding husband or wife). 16
38. There has been serious problems with a close friend, neighbour or relative not living athome. B
EDUCATION
39. You started a course (ie. University, Tech.College, Business College, apprenticeshipor other occupational training course). 16
40. You changed to a different course. 11
41. You completed your training program. 27
42. You dropped out of your training program. 22
43. You studied for, or did, important exams. 13
44. You failed an important exam. 18

81
Event
WORK
45. You have been unemployed and seeking work for a month or more.
46. Your own business failed.
47. You were sacked.
48. You retired.
49. You were downgraded or demoted at work.
5d. You were promoted.
51. You began to have trouble or disagreements with your boss, supervisor or fellow workers.
52. You had a big change in the hours you worked.
53. You had a big change in the people, duties or responsibilities in your work.
54. You started in a completely different type of job.
Life change scalings
22
44
34
53
18
18
9
16
17
24
55. You had holidays for a week or more. 5

Event Life change sealings
MOVING HOUSE
56. You moved to Sydney from overseas. 48
57. You moved to Sydney from elsewhere inAustralia. 26
58. You moved house in Sydney. 11
FINANCIAL AND LEGAL
59. You had moderate financial difficulties. 10
60. You had a major financial crisis. 37
61. You are much better off financially. 23
62. You were involved in a traffic accident that carried serious risk to the health or lifeof yourself or others. 22
63. You had minor difficulties with the police orthe authorities [which has not required a court appearance (eg. speeding fine, etc.)]. 2
64. You had more important problems with the police or the authorities (leading to a courtappearance). 15
65. You had a jail sentence or were in prison. 72

83
EventLife change scalings
66. You were involved in a civil law suit(eg. divorce, debt, custody, etc.). 21
67. Something you valued or cared for greatlywas stolen or lost. 5
(from Tennant and Andrews, 1976, pp. 30-32).
Deletions
The following female specific items were deleted from the inventory: Items 4,5,6,7,8,9 & 10.
Items 39, 40, 41, 45, 46, 48, 49, 53 & 65 were deleted as they were inappropriate to the study's population.
Amendments
Gender specific instructions were amended to reflect the male population of study.
Items 56, 57 & 58 were amended from 'Sydney' to 'ACT region' to reflect the geographical location of the study's population.

84
Items 42, 44, 47, 51, 54, 55, 62, 63 & 64 were amended to reflect population specific terminology and/or circumstances. Similarly the category 'Moving House' was amended to 'Accommodation'.
Additions
The following 21 items were chosen for inclusion in theinventory:
Health
1. You were medically downgraded.
2. You failed your Physical Training Tests.
Family and Social
1. Your wife commenced paid employment.
2. A child of yours was forced to change schools.
3. A child of yours experienced significant difficulty at school.
Education
1. You started a part-time course at a civilian institution.

85
2. You were a full-time student (eg. a Staff College, Long Term Civil Schooling, etc.).
3. You attended a demanding career course (excluding Long Term Schooling).
Work
1. You have been seriously seeking civilian employment.
2. You received a poor Confidential Report (PR 19) .2
3. You submitted your resignation.
4. You were passed over for promotion.
5. Your work performance was significantly impaired by lack of resources (staff, funds, equipment, etc.).
6. You were required to make frequent work related trips of short duration (average of two trips per month as minimum).
2 . Annual performance appraisal by superior officer(s).

86
7. You were reposted.
8. You held a demanding extra-regimental appointment.
9. You held a significant honorary appointment in the community (e.g., school board, youth/sporting/social/service club or association).
Accommodation
1. You moved from your own home into rented (MQ, TRA etc.) accommodation.
2. You bought your own home.
3. You made a major extension to your dwelling.
Financial and Legal
1. A close relative had problems with the law.
Determination of Life Change Scalings
The 21 population specific items selected for addition to the inventory were included in a questionnaire together with the following instructions employed by Holmes and Rahe (1967, p. 213):

87
Social readjustment includes the amount and duration of change in one's accustomed pattern of life resulting from various life events. As defined, social readjustment measures the intensity and length of time necessary to accommodate to a life event, regardless of the desirability of this event.
You are asked to rate a series of life events as to their relative degrees of necessary readjustment. In scoring, use all of your experience in arriving at your answer. This means personal experience where it applies as well as what you have learned to be the case for others. Some persons accommodate to change more readily than others; some persons adjust with particular ease or difficulty to only certain events. Therefore, strive to give your opinion of the average degree of readjustment necessary for each event rather than the extreme.
The mechanics of rating are these: Event 1, Marriage,has been given an arbitrary value of 500. As you complete each of the remaining events think to yourself, "Is this event indicative of more or less readjustment than marriage?" "Would the readjustment take longer or shorter to accomplish?" If you decide the readjustment is more intense and protracted, then choose a proportionately larger number and place it on the line directly opposite the event in the column marked "VALUES". If you decide the event represents less and shorter readjustment than marriage then

38
indicate how much less by placing a proportionately smaller number on the opposite line. (if an event requires intense readjustment over a short time span, it may approximate in value an event requiring less intense readjustment over a long period of time). If the event is equal in social readjustment to marriage, record the number 500 opposite the event.
A random sample of 200 male, middle-ranking army officers, stratified for age, rank and work location was selected as the subject pool for the study to determine the life change scalings for the additional inventory items. These 200 officers were drawn from the same population as the 130 officers in the subject pool for the principal study, but were exclusive of this group.
A copy of the questionnaire, a pre-addressed return envelope and the following letter from the researcher soliciting co-operation in the study were mailed to each officer at his work location recorded in a departmental telephone directory:
I am conducting a survey to investigate the level of physical fitness of officers serving in the Canberra region, the incidence of recent illness in the group and their opinions and attitudes to various health and social issues. The study will provide data which will assist the staff to review current policies on physical fitness and health care. The survey has been approved by the Chief of Personnel.

89
Part of the survey involves recording the views of a sample of officers regarding the effects of changes in their patterns of life. To assist in the collection of these data I would appreciate your completing the enclosed questionnaire and returning it in the envelope provided by (date).
Thank you for your co-operation.
Completed questionnaires were returned by 125 officers. Eighteen questionnaires were returned to sender undelivered.
The life change scaling for each event was determined pro rata, on the basis of the ratio between the arbitrary value assigned to the index item (marriage) in the questionnaire, and the same item's scaling provided by Tennant and Andrews (1976), ie. 500 : 59. The results of the respondents' ratings and the calculation of life change scalings are in Table B-2.
Table B-2
Calculation of Life Change Scalings (fsf=125)
Responses Life_____________________ change
Event n Sum Mean scalings
1. You were medically downgraded. 114 35111 308.0 36

90
Responses Life_________________ changeEvent n_ Sum Mean scalings
2. You failed your physicaltraining tests. 116 28738 247.7 29
3. Your wife commenced paidemployment. 122 28630 234.7 28
4. A child of yours was forced tochange schools. ' 122 40180 329.3 39
5. You have been seriouslyseeking civilian employment. 118 47235 400.3 47
6. You received a poorConfidential Report (PR19). 118 44575 377.8 45
7. You submitted yourresignation. 115 54080 470.3 55
8. You were passed over forpromotion. 115 54915 477.5 56
9. You were reposted. 122 39525 324.0 38
10. You moved from your own home into rented (MQ, TRA, etc.)accommodation. 120 39445 328.7 39
11. You bought your own home. 120 40360 336.3 40

91
Responses Life____ _______________ changeEvent n_ Sum Mean scalings
12. You started a part-time course of study at a civilianinstitution. 118 26915 228.1 27
13. You were a full-time student (e.g., a Staff College, LongTerm Civil Schooling etc.). 119 33290 279.8 33
14. You attended a demanding career course (excluding LongTerm Schooling). 119 37575 315.8 37
15. A child of yours experienced significant difficulties atschool. 121 50255 415.3 49
16. Your work performance was significantly impaired by lack of resources (staff, funds,equipment etc.). 121 40060 331.1 39
v17. You were required to make frequent work related trips of short duration (average of twotrips per month as minimum). 123 24551 199.6 24
18. You held a demanding extra- regimental appointment. 119 30281 254.5 30

92
Responses Life____________________ change
Event n_ Sum Mean scalings
19. You held a significant honorary appointment in the community (e.g., school board, youth/ sporting/social/serviceclub or association). 118 25966 220.1 26
20. You made a major extension toyour dwelling. 115 26060 226.6 27
21. A close relative had problemswith the law. 115 37820 328.9 39

93
Appendix C: Life Events Life Change
Inventory and Scalings
LIFE EVENTS SURVEY
Below is a list of events which may occur in an officer's life. In the box provided please enter the number 1 if you experienced the event in the past twelve months. If you did not experience the event in the past twelve months please leave the box blank.
Li f e change
HEALTH scalings
1. You had a minor illness or injury like oneneeding a visit to a doctor or a couple of ___days off work. I 1 2
2. You had a serious illness, injury or operation needing hospitalization or amonth or more off work. I I 16
3 . You were medically downgraded. 36

94
Li f echangescalings
4 . A close relative or friend had a seriousillness (from which they did not die). I i 9
5. Your wife had a child or you adopted achild. 41
6 . You failed your Physical Training Tests. 29
BEREAVEMENT
7. Your wife died. □ 79
8. A child o£ yours died □ 57
9* A close family member died (e.g., parent,brother, sister etc.). □ 27
A close family friend or relative died (e.g., aunt, uncle, grandparent, cousin, etc.) . □ 12
FAMILY AND SOCIAL
(if you are or were married please answer questions 11-20)
11 . □You married. 59

95
Li f echangescalings
12. There has been increasing serious argumentswith your wife. L_J 25
13. There has been a marked improvement in theway you and your wife are getting on. 1 I 18
14. You have been separated from your wife for more than a month because of maritaldifficulties. ] 29
15. You have been separated from your wife for more than a month (for reasons other than marital difficulties - e.g., course,unaccompanied posting etc.). I I 15
16. You have got back together again after aseparation due to marital difficulties. 1. 1 25
17. You began an extra-marital affair. i___1 28
18. Your wife began an extra-marital affair. 1 28
19. Your wife commenced paid employment. 1. 1 28
20. You have been divorced. 1 1 62
(if you have or had children please answer questions 21 to 27).

96
Li f echangescalings
21 .
2 2 .
23 .
24.
25.
26.
27.
28.
29.
A child of yours was forced to change schools. 39
A child of yours experienced significant difficulties at school. 49
A child of yours became engaged. 6
A child of yours married with your approval. 10
A child of yours married without your approval. 16
A child of yours left home for reasons other than marriage. 14
A child of yours enlisted in the armed services. 10
(If you are single please answer questions 28-31)
You became engaged or began a ' steady' relationship. 17
You broke off your engagement. 21
30. You broke off a 'steady' relationship. 18

97
31. You had increasing arguments ordifficulties with your fiancee or steady friend.
FRIENDS AND RELATIVES
32. A new person came to live in your household (apart from a new baby).
33. There has been a marked improvement in the way you get on with someone close to you (excluding wife).
34. You have been separated from someone important to you (other than close family members).
35. There has been serious increase inarguments or problems with someone who lives at home (excluding wife).
36. There have been serious problems with a close friend, neighbour or relative not living at home.
EDUCATION
You started a part-time course of study at □
Li f e change sealings
13
20
10
13
16
a civilian institution. 27

98
3 8 .
39.
40.
41.
42.
WORK
43.
44.
45.
46.
You were a full-time student (e.g., a Staff College, Long Term Civil Schooling etc.).
You attended a demanding career course (excluding Long Term Schooling).
You dropped out of a course (civilian or military).
You studied for, or did, important examinations.
You failed an important examination or course.
You have been seriously seeking civilian employment.
You received a poor Confidential Report (PR19).
You were 'sacked' from a posting.
You submitted your resignation □□
Li f e change sealings
33
37
22
13
18
47
45
34
55
47. You were passed over for promotion. 56

99Li f e change sealings
48. You were promoted. 1 I 18
49. You began to have trouble or disagreementswith your superior officers or peers. 1 I 9
50. Your work performance was significantly impaired by lack of resources (staff,funds, equipment etc.). L - 1 39
51. You had a big change in the hours youworked. 1 1 16
52. You were required to make frequent work related trips of short duration (average oftwo trips per month as minimum). 1 1 24
53. You were reposted. 1 1 38
54. You held a demanding extra-regimentalappointment. 1 „, 1 30
55. You moved from a regimental environment toan office environment, t I 24
56. You held a significant honorary appointment in the community (e.g., school board, youth/sporting/ social/service club orassociation). 1 1 26

100Li f echangescalings
57. You took leave/furlough for a week or nmore. I-- 1 5
ACCOMMODATION
58. You moved to the ACT region from overseas. L..1 48
59. You moved to the ACT region from elsewhere ___nin Australia. I-- I 26
60. You moved house in the ACT region. [___I H
61. You moved from your own home into rented ___(MQ, TRA etc.) accommodation. 1--1 39
n62. You bought your own home. ‘---» 40
63. You made a major extension to yourdwelling. 27
FINANCIAL AND LEGAL
64. You had moderate financial difficulties. 1 1 10
65. You had a major financial crisis. C. 1 37
66. You are much better off financially. 1 I 23

101Li f e change sealings
67. You were involved in an accident that carried serious risk to the health or lifeof yourself or others. L . -1 22
68. You had minor difficulties with police ormilitary authorities [which have not involved a civil court or court martial (e.g., speeding fine, reprimand by superior ___officer etc.)]. L -1 2
69. You had more important problems with the police or military authorities (leading toa court appearance or court martial). I 1 15
70. A close relative had problems with the1 aw. 1— ..J 3 9
71. You were involved in a civil law suit (e.g.,divorce, debt, custody etc.). 1 1 21
72. Something you valued or cared for greatlywas stolen or lost. 1 1 5
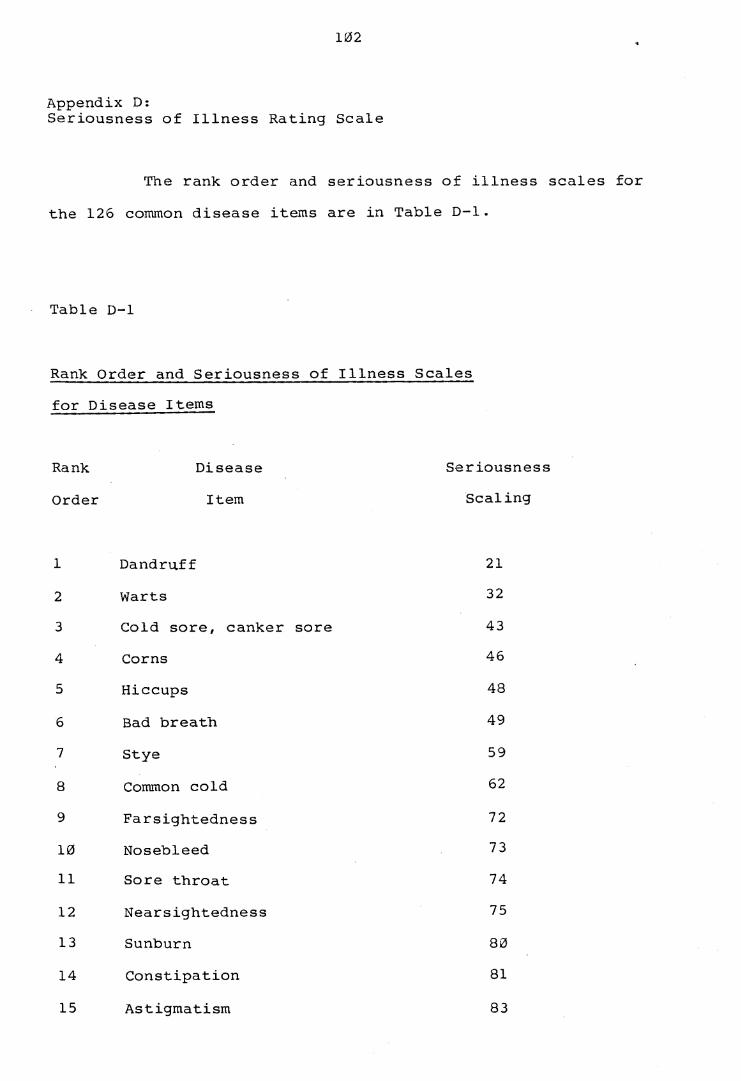
102
Appendix D:Seriousness of Illness Rating Scale
The rank order and seriousness of illness scales for the 126 common disease items are in Table D-l.
Table D-l
Rank Order and Seriousness of Illness Scales for Disease Items
Rank Disease SeriousnessOrder Item Scaling
1 Dandruff 212 Warts 323 Cold sore, canker sore 434 Corns 465 Hiccups 486 Bad breath 497 Stye 598 Common cold 629 Farsightedness 7210 Nosebleed 7311 Sore throat 7412 Nearsightedness 7513 Sunburn 8014 Constipation 8115 Astigmatism 83

1617181920212223
2425262 728293031323334353637
3839404142434445
103
Laryngitis 84Ringworm 85Headache 88Scabies 89Boil s 96Heartburn 98Acne 103Abscessed tooth 108Colourblindness 109Tonsillitis 117Diarrhoea 118Carbuncle 122Chicken pox 134Menopause 140Mumps 148Dizzines s 149Sinus infection 150Bed sores 153Increased menstrual flow 154Fainting 155Measles 159Painful menstruation 163Infection of the middle ear 164Varicose veins 173Psoriasis 174No menstrual period 175Haemorrhoids 177Hay fever 185Low blood pressure 189Eczema 204

464748495051525354555657585960616263646566676869707172737475
104
Drug allergy 206Bronchitis 210Hyperventilation 211Shingles 212Mononucleosis 216Infected eye 220Bursitis 222Whooping cough 230Lumbago 231Fibroids of the uterus 234Migraine 242
Hernia 244Frostbite 263Goitre 283Abortion 284Ovarian cyst 288Heatstroke 293Gonorrhea 296Irregular heart beats 302Overweight 309Anaemia 312Anxiety reaction 315Gout 322
Snake bite 324Appendicitis 337Pneumonia 338Depression 344Frigidity 347Burns 348Kidney infection 374

767778798081828384858687888990919293949596979999100101102103104105
105
Inability for sexual intercourse 382Hyperthyroid 393Asthma 413Glaucoma 426Sexual deviation 446Gallstones 454Arthritis 468Starvation 473Syphilis 474Accidental poisoning 480Slipped disc 487Hepatitis 488Kidney stones 499Peptic ulcer 500Pancreatitis 514High blood pressure 520Smallpox 530Deafness 533Collapsed lung 536Shark bite 545Epilepsy 582Chest pain 609Nervous breakdown 610Diabetes 621Blood clot in blood vessels 631Hardening of the arteries 635Emphysema 636T.B. 645Alcoholism 688Drug addiction 722

106
106 Coma 725107 Cirrhosis of the liver 733108 Parkinson's disease 734109 Blindness 737110 Mental retardation 745111 Blood clot in the lung 753112 Manic depressive psychosis 766113 Stroke 774114 Schizophrenia 776115 Muscular dystrophy 785116 Congenital heart defects 794117 Tumor in the spinal cord 800118 Cerebral palsy 805119 Heart failure 824120 Heart attack 855121 Brain infection 872122 Multiple sclerosis 875123 Bleeding in brain 913124 Uremia 963125 Cancer 1020126 Leukaemia 1080
On the advice of senior Army Medical officers the following items were deleted from the scale because of their lack of appropriateness for the study's population:
1. ^Colourblindness (24).
2 . Menopause (29).

107
3 .
4.
5.
6 .
7 .
8 .
9 .
10.
11.
12 .
13.
14.
Increased menstrual flow (34).
Painful menstruation (37).
No menstrual period (41).
Fibroids of the uterus (55).
Abortion (60).
Ovarian cyst (61).
Snake bite (69).
Frigidity (73).
Starvation (83).
Shark bite (95).
Mental retardation (110).
Muscular dystrophy (113).
15. Cerebral palsy (118).

108
Appendix E:Instrument to Measure Psychophysiological Response
HEALTH SURVEY
Below is a list of complaints which occur commonly in the community. Please indicate the frequency with which you have experienced each one in the past twelve months by recording a number from 0 to 3 in the box provided. A zero indicates that you had the complaint not at all; a three means you had the complaint frequently in the past twelve months.
0 = Not at all1 = A little2 = Quite a bit3 = Frequently
1. Heartburn, upset stomach or recurrent diarrhoea
2. Headaches
3. Loss of appetite
4. Dizzy spells
5. Nervousness
6. Shortness of breath
7. Trouble sleeping
□□□□□□□

109
8 .
9 .
10 .
11.
12 .
13.
14.
15 .
16 .
Irregular heartbeats
Anxiety attacks
Inability to concentrate
Sweaty palms
□□□□
Shaky hands
Stiffness in back of neck
Crying spells
Hyperventilation
Depression

110
Appendix F: Hardiness Test
PERSONAL VIEWS SURVEY
Below are some items that you may agree or disagree with. Please indicate how you feel about each one by circling a number from 0 to 3 in the space provided. A zero indicates that you feel the item is not at all true; circling a three means that you feel the item is completely true.
As you will see, many of the items are worded very strongly. This is to help you decide the extent to which you agree or disagree.
Please read all the items carefully. Be sure to answer all on the basis of the way you feel now. Don't spend too much time on any one item.
0 = Not at all true1 = A little true2 = Quite a bit true3 = Completely true
1. I often wake up eager to take up my~~life 0 1 2 3where it left off the day before.
2. I like a lot of variety in my work. 0 1 2 3
3. Most of the time, my bosses or superiors • 0 1 2 3will listen to what I have to say.

Ill
4. Planning ahead can help avoid most future 0 1 2problems.
5. I usually feel that I can change what might 0 1 2happen tomorrow/ by what I do today.
6. I feel uncomfortable if I have to make any 0 1 2changes in my everyday schedule.
7. No matter how hard I try, my efforts will 0 1 2accomplish nothing.
8. I find it difficult to imagine getting 0 1 2excited about working.
9. No matter what you do, the "tried and true" 0 1 2ways are always the best.
10. I feel that it's almost impossible to 0 1 2change my spouse's mind about something.
11. Most people who work for a living are just 0 1 2manipulated by their bosses.
12. New laws shouldn't be made if they hurt a 0 1 2person's income.
When you marry and have children you have lost your freedom of choice.
3
3
3
3
3
3
3
3
3
13. 0 1 2 3

No matter how hard you work, you never
really seem to reach your goals.
A person whose mind seldom changes can
usually be depended on to have reliable
judgement.
I believe most of what happens in life is
just meant to happen.
It doesn't matter if you work hard at your
job, since only the bosses profit by it
anyway.
I don't like conversations when others are
confused about what they mean to say.
Most of the time it just doesn't pay to try
hard, since things never turn out right
anyway.
The most exciting thing for me is my own
fantasies.
I won't answer a person's questions until I
am very clear as to what he is asking.
When I make plans I'm certain I can make
them work.

113
23 .
2 4 .
25 .
2 6 .
2 7 .
2 8 .
2 9 .
3 0 .
3 1 .
I really look forward to my work.
It doesn’t bother me to step aside for a while from something I'm involved in, if I'm asked to do something else.
When I am at work performing a difficult task I know when I need to ask for help.
It's exciting for me to learn something about myself.
I enjoy being with people who areunpredictable.
I find it's usually very hard to change a friend's mind about something.
Thinking of yourself as a free person just makes you feel frustrated and unhappy.
It bothers me when something unexpected interrupts my daily routine.
When I make a mistake, there's very little I can do to make things right again.
I feel no need to try my best at work, since it makes no difference anyway.
32. 0 1 2 3

114
33 .
34.
35.
36.
37.
38.
39.
40.
41.
42.
I respect rules because they guide me. 0 1 2 3
One of the best ways to handle most 0 1 2 3problems is just not to think about them.
I believe that most athletes are just born 0 1 2 3good at sports.
I don't like things to be uncertain or 0 1 2 3unpredictable.
People who do their best should get full 0 1 2 3financial support from society.
Most of my life gets wasted doing things 0 1 2 3that don't mean anything.
Lots of times I don't really know my own 0 1 2 3mind.
I have no use for theories that are not 0 1 2 3closely tied to the facts.
Ordinary work is just too boring to be 0 1 2 3worth doing.
When other people get angry at me, it' s 0 1 2 3usually for no good reason.
43. Changes in routine bother me. 0 1 2 3

115
44. I find it hard to believe people who tell 0 1 2 3me that the work they do is of value tosociety.
45. I feel that if someone tries to hurt me, 0 1 2 3there's usually not much I can do to tryand stop him.
46. Most days, life just isn't very exciting 0 1 2 3for me.
47. I think people believe in individuality 0 1 2 3only to impress others.
48. When I'm reprimanded at work, it usually 0 1 2 3seems to be unjustified.
49. I want to be sure someone will take care of 0 1 2 3me when I get old.
50. Politicians run our lives. 0 1 2 3

116
Appendix G:Measurement of Physical Fitness
Equipment
The following equipment was used in the measurement of physical fitness:
1. * 1Repco' HP5209 cycle ergometer with a load indicator to measure kilopond metres per minute (kpm/min). The cycle ergometer was calibrated to manufacturer's instructions.
2. 'Medtel' HS10 Cardiac Monitor.
3. 'Repco' Work Test Calculator HP5225.
4. Timing Clock.
Procedure
The testing sequence was based on the Royal Australian Air Force (RAAF) aerobic power assessment procedure. Comprehensive technical information is contained in Directorate- General Air Force Health Services (Undated). The testing procedure is summarized as follows:
1. Testing was conducted in an air conditioned room with temperature a constant 190C.

Subjects were requested to wear physical training gear .
The saddle height of the cycle was adjusted until, with the pedal shafts in the vertical position, the heel of the foot on the down pedal side rested on top of the pedal.
The cardiac monitor was attached to the subject in accordance with current RAAF practice.
The testing procedure was explained and the requirement to maintain the load indicator on the prescribed load was emphasised.
Each subject's age, weight and maximum test heart rate (MTHR) were recorded on an adaptation of the RAAF worksheet (see Appendix H). The MTHR is the age related safety limit accepted for submaximal fitness testing. Care was taken to ensure a subject's heart rate did not exceed his MTHR during testing. The range of MTHR is in Table G-l.

118
Table G-l
Maximum Test Heart Rates
Maximum test heart rate Age [beats per minute (bpm)]
26-30 16531-35 16036-40 15541-45 15046-50 14551-55 140
7• If a subject's resting heart rate was below 100 bpm thetest was commenced; if greater than 100 bpm the test was not commenced until the subject had remained at rest for an additional five minutes or until the heart rate fell below 100 bpm.
8* After a subject was given a one minute warm up andadjustment phase pedalling at 100 kpm/min, the timing clock was set and the subject instructed to pedal at an initial workload in accordance with Table G-2.
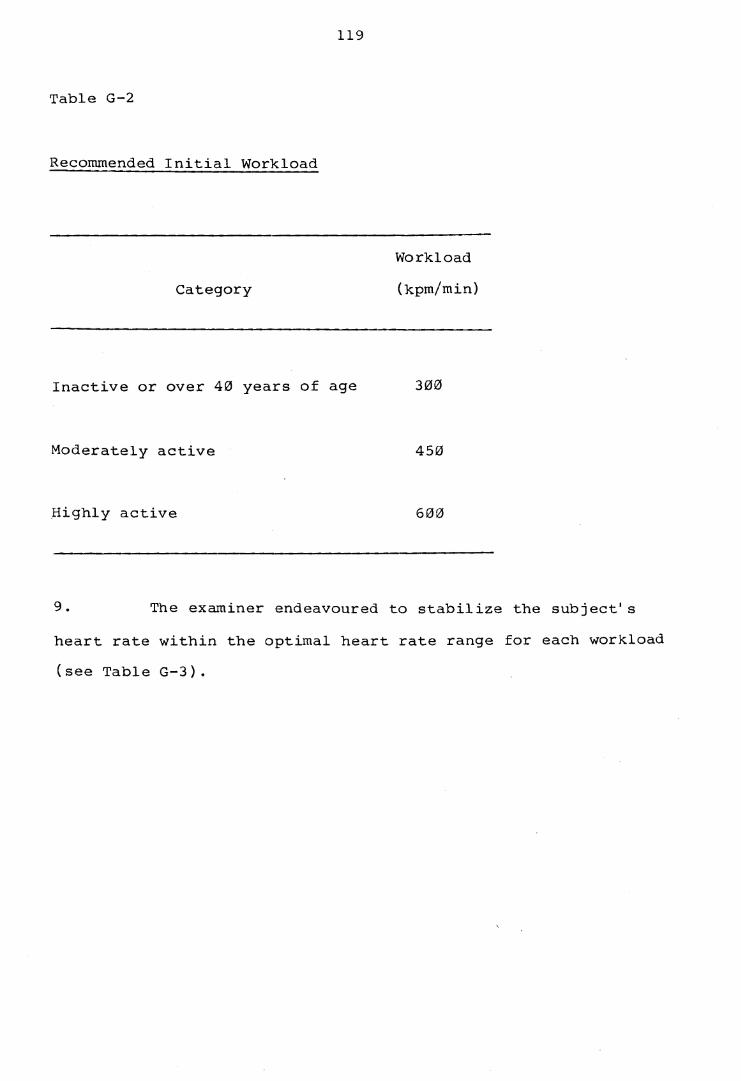
119
Table G-2
Recommended Initial Workload
WorkloadCategory (kpm/min)
Inactive or over 40 years of age 300
Moderately active 450
Highly active 600
9. The examiner endeavoured to stabilize the subject'sheart rate within the optimal heart rate range for each workload (see Table G-3).

120
Table G-3
Optimal Heart Rate Ranges for Workloads
Age Workload 1 Workload 2 Workload 3
30 105-120 125-140 145-16031-35 104-118 124-136 143-15536-40 103-116 120-134 138-15041-45 102-114 118-130 135-14546-50 101-112 116-126 130-14051-55 100-110 115-124 126-135
Tine ' stable' heart rate for each workload was recorded on the worksheet. Stability was indicated by a 5 bpm or less difference between the heart rate at the end of the second and third minutes of each workload. If the difference exceeded 5 bpm, the subject was maintained at the same workload for an additional minute.The 'stable' heart rate was the rate at the completion of the final minute for each workload.
When a stable heart rate was reached the workload was raised to a new level which was set relative to the stable heart rate and the suggested optimal heart rate ranges. Approximate workload increments based on 'stable' heart rates and optimal heart rates are in Table G-4.
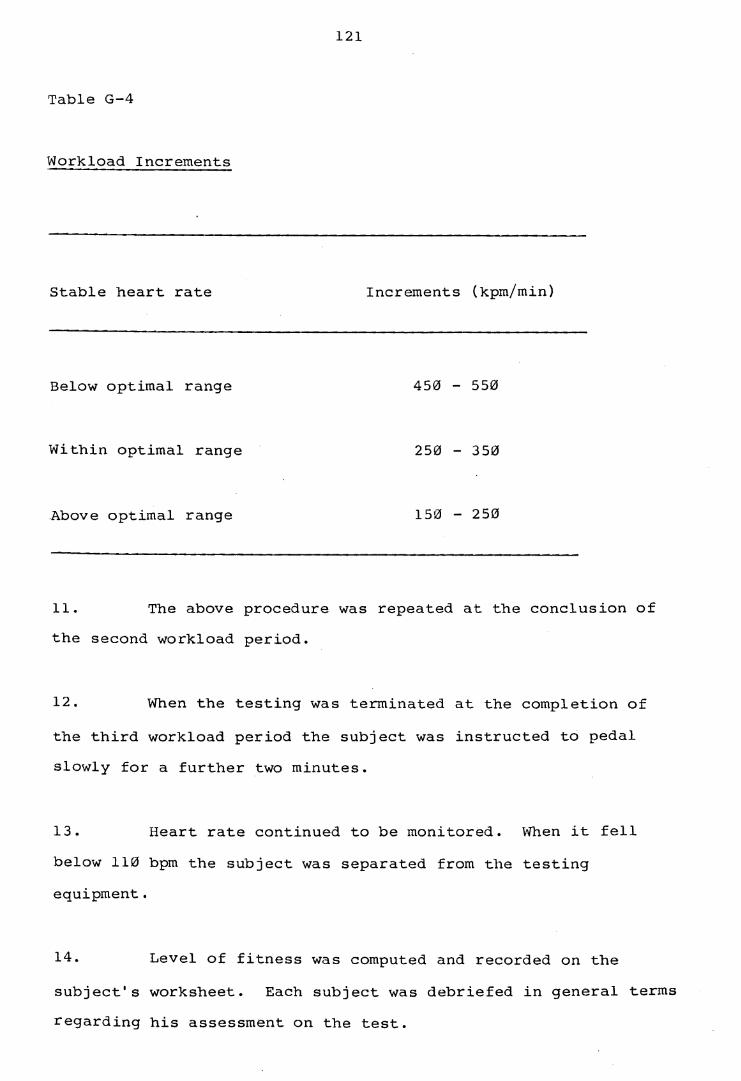
121
Table G-4
Workload Increments
Stable heart rate Increments (kpm/min)
Below optimal range 450 - 550
Within optimal range 250 - 350
Above optimal range 150 - 250
11. The above procedure was repeated at the conclusion of the second workload period.
12. When the testing was terminated at the completion of the third workload period the subject was instructed to pedal slowly for a further two minutes.
13. Heart rate continued to be monitored. When it fell below 110 bpm the subject was separated from the testing equipment.
14. Level of fitness was computed and recorded on the subject's worksheet. Each subject was debriefed in general terms regarding his assessment on the test.

122
Computation of Maximum Oxygen Uptake
At the completion of the testing the three workloads and their corresponding steady state heart rates were transferred to the Heart rate-Workload graph on the subject's worksheet. A line of best fit was extended through the points to intercept the MTHR. The workload corresponding to the MTHR intercept point was recorded as the test workload.
The 'Repco' Work Test Calculator was used to computethe predicted VO2 max for each subject. This calculator incorporates the principles of the nomogram developed by Astrand(I960) and accommodates the parameters of workload, heart rate,age, body weight and sex. On the outer, male scale the subject'sMTHR was aligned with the test workload measure; on the innerscales the subject's age and body weight measures were aligned.The VO2 max value indicated in the maximum oxygen uptake window of the calculator was recorded on the subject's worksheet.
Exemption from Fitness Testing
Subjects with medical contra-indications to fitness testing were identified by reference to their medical status at the time of testing. These subjects were exempted from this phase of the testing.

123
Appendix H:Physical Fitness Assessment Worksheet
PHYSICAL FITN ESS ASSESSMENT WORKSHEET
Weight Max Test HR
FIRST WORKLOAD
Mins W orkload Heart Rate
1
2
3
SECOND WORKLOAD
Mins Workload Heart Rate
4
5
6
THIRD WORKLOAD
Mins Workload Heart Rate
7
8
9
UJ
< 130
£< 120 I
II
. !
’/i 1 kp 1'/, 2kp 2 ’/i 3kp 3 V, 4kp
180 360 540 720 900 1080 1260 1440
Workload
kp
kpm /m in
T e s t W o rk lo a d v n ? May

















