37
Health and Social Policy: Time to Reshift the Paradigm? Will Ross, M.D. Associate Dean for Diversity Associate Professor of Medicine Washington University School of Medicine June 11, 2008
| Date post: | 30-Dec-2015 |
| Category: |
Documents |
| Upload: | yasir-mcpherson |
| View: | 38 times |
| Download: | 1 times |

Health and Social Policy: Time to Reshift the Paradigm?
Will Ross, M.D.
Associate Dean for DiversityAssociate Professor of Medicine
Washington University School of Medicine
June 11, 2008

Objectives
• Identify the benefits and limitations of the WHO definition of health
• Debate the roles of genetics and social forces in perpetuating health disparities
• Promote a health model that embraces an ecological approach to reducing health disparities
Is it the right time for a paradigm shift?

Thinking about the campaign for the presidential election in 2008, what two issues would you most like to hear the presidential candidates talk about? (open-ended, top 4 responses shown)
44% 43%
38%
44%
35%
26%
21%
30%
38%
30%
18%
13%
18%21%
9%12% 12%
17%
13%
18%
0%
10%
20%
30%
40%
50%
Mar-07 Jun-07 Aug-07 Oct-07 Dec-07
Iraq
Health care
Economy
Immigration
Note: Adds up to more than 100% due to multiple responses. Source: Kaiser Health Tracking Poll: Election 2008
Is Health Care Breaking Through as a Political Issue?

Disparities in Healthcare Quality*
• The evidence is “overwhelming”• Disparities exist even when insurance status,
income, age, and severity of conditions are comparable
• Minorities are less likely than whites to receive needed services
• Disparities contribute to worse outcomes in many cases
• Differences in treating heart disease, cancer, & HIV infection partly contribute to er death rates for minorities
*Unequal Treatment: Confronting Racial and Ethnic Disparities in Healthcare, 2002.

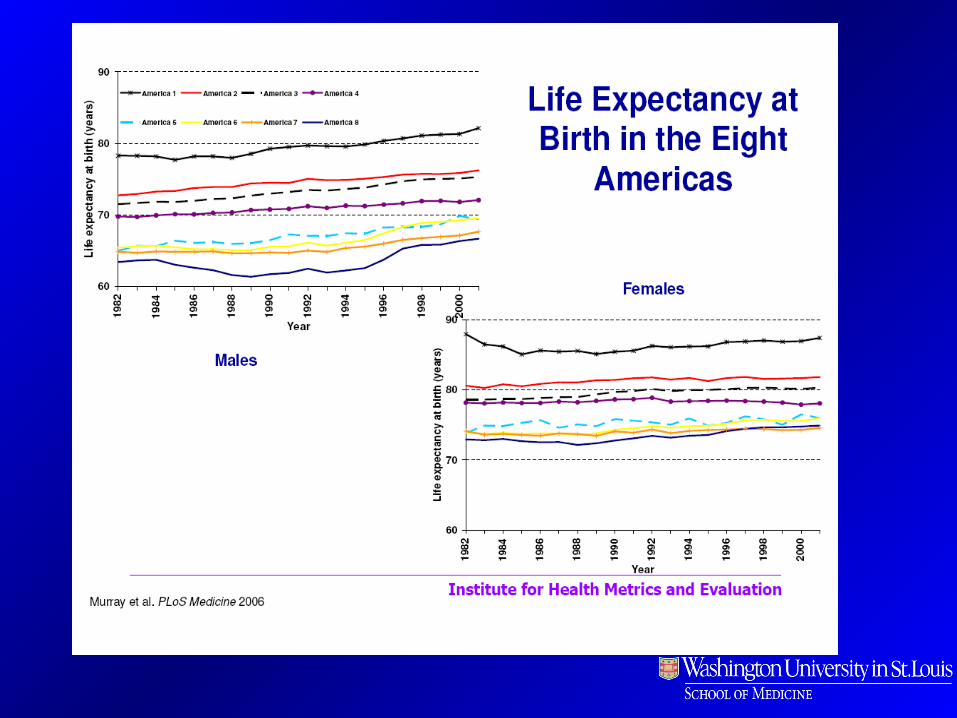
Eight Americas: Investigating Mortality Disparities Across Races, Counties, and Race-Counties in the United States
Christopher J.L. Murray, MD, DPhilInstitute Director, Institute for Health Metrics and Evaluation Professor of Global Health, University of Washington
Majid Ezzati, Ph.D. Associate ProfessorHarvard School of Public Health
Institute for Health Metrics and EvaluationSeptember 12, 2006
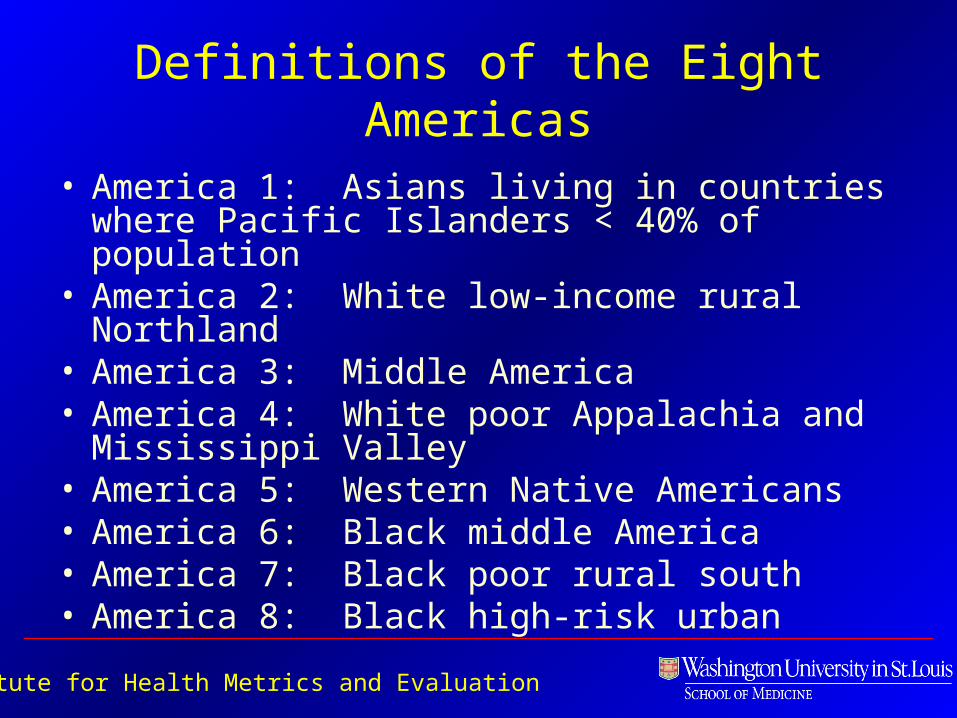
Definitions of the Eight Americas
• America 1: Asians living in countries where Pacific Islanders < 40% of population
• America 2: White low-income rural Northland• America 3: Middle America• America 4: White poor Appalachia and Mississippi
Valley• America 5: Western Native Americans• America 6: Black middle America• America 7: Black poor rural south• America 8: Black high-risk urban
Institute for Health Metrics and Evaluation

Dorothy Lange’s “Migrant Mother” Collection. FSA-OWI, 1936

President Roosevelt signs Social Security Act, at approximately 3:30 pm EST on August 14, 1935

Civil rights demonstrator May 3, 1963, Birmingham, Ala.
Medical Committee for Human Rights Archive, US Health Activism History Collection Institute of Social Medicine and Community Health, Philadelphia, PA

“The time has come for an all-out world war against poverty. The rich nations must use their vast resources of wealth to develop the underdeveloped, school the unschooled, and feed the unfed. Ultimately a great nation is a compassionate nation. No individual or nation can be great if it does not have a concern for ‘the least of these’".
Rev. Dr. Martin Luther King Jr,Excerpted from his Nobel Prize Lecture,University of Oslo, December 11, 1964

President Lyndon B. Johnson signs the 1965 Social Security Amendments (Medicare and Medicaid)

Lee Celano for The New York Times, Tuesday November 6th, 2007
Hurricane Katrina
World Health OrganizationDefinition of Health1
“ . . . a state of complete physical, mental, and social well-being and not merely the
absence of disease and infirmity.”
1 The Constitution was adopted by the International Health Conference held in New York from 19 June to 22 July 1946, signed on 22 July 1946 by the representatives of 61 States (Off. Rec. Wld Hlth Org., 2, 100), and entered into force on 7 April 1948. Amendments adopted by the Twenty-sixth, Twenty-ninth, Thirty-ninth and Fifty-first World Health Assemblies (resolutions WHA26.37, WHA29.38, WHA39.6 and WHA51.23) came into force on 3 February 1977, 20 January 1984, 11 July 1994 and 15 September 2005 respectively and are incorporated in the present text.
“ . . . governments have a responsibility for the health of their peoples which can be fulfilled only by the provision of adequate health and social measures”.
But it also includes . . .
Do we have the financial resources to capitalize our
paradigm shift?
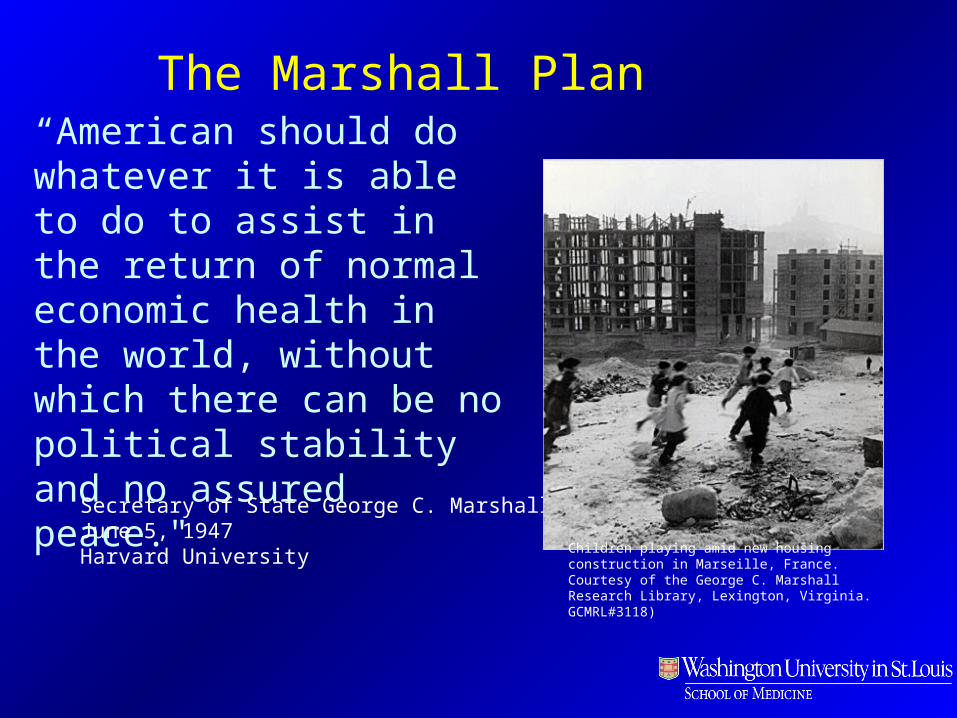
“American should do whatever it is able to do to assist in the return of normal economic health in the world, without which there can be no political stability and no assured peace."
The Marshall Plan
Secretary of State George C. MarshallJune 5, 1947Harvard University Children playing amid new housing construction in
Marseille, France. Courtesy of the George C. Marshall Research Library, Lexington, Virginia. GCMRL#3118)

"The Americans will always do the right thing - after they've exhausted all the alternatives.”
Winston Churchill

1918
1616151514
13131313131313131313121111
0
5
10
15
20
Projected
U.S. Health Expendituresas Share of GDP Expected to Rise
Through Next Decade
Expenditures as percent of gross domestic product (GDP)
Source: Center for Medicare and Medicaid Services, Office of the Actuary, 1998–2003 from CMS Health Accounts data file nhegdp03.zip available at http://www.cms.hhs.gov/statistics/nhe/default.asp; 2004–2014 published in Heffler et al., "U.S. Health Spending Projections for 2004–2014," Health Affairs Web Exclusive (February 23, 2005): W5-74–W5-85.

Higher Spending Does Not Necessarily Lead to Higher Quality
Source: Baicker and Chandra (Health Affairs 2004)
Benefits of Human Genome Project

Annualized Growth of the NIH Budget, 1971 to 2005 (The growth rates shown have been adjusted for inflation)
Loscalzo J. NEJM, 2006;354:1665-1667

As the NIH budget flattens, competition for grants escalates

“Will – Isn’t this so-called paradigm shift just a back door attempt to market a socialized medicine scheme?”


De Vogli, R. et al. J Epidemiol Community Health 2005;59:158-162
Income inequality and life expectancy at birth among industrialised countries
Less inequality More inequality

Pathways by which Socioeconomic Status Affects Health Behaviors
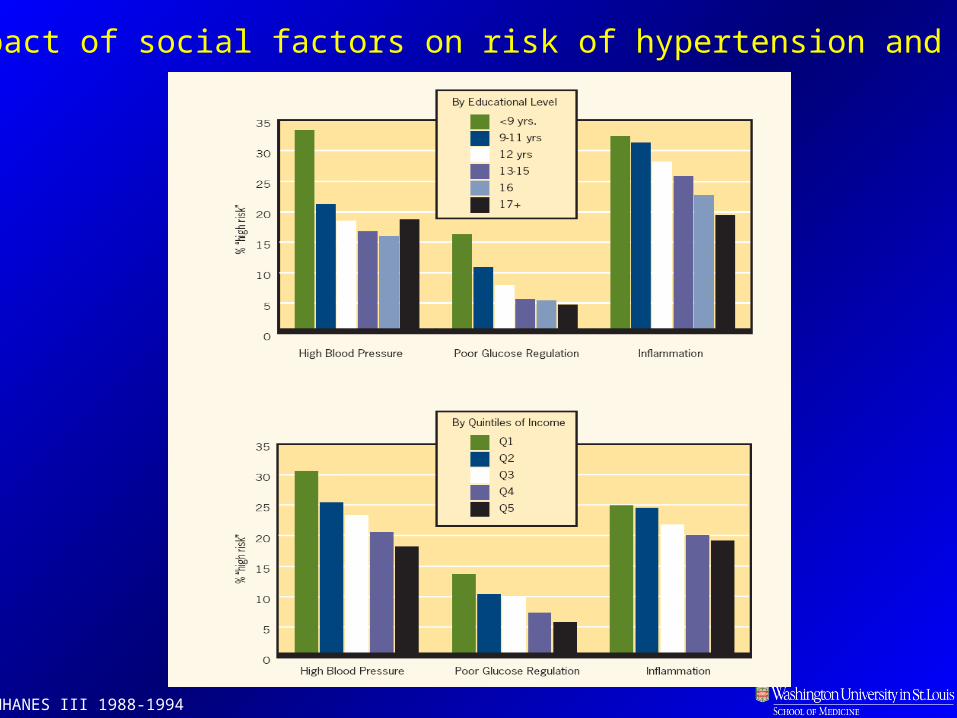
NHANES III 1988-1994
Impact of social factors on risk of hypertension and diabetes

www.macses.ucsf.edu Accessed June 5, 2008

Two kinds of policies are required to reducepremature death and eliminate health disparities:
1. Policies that impact income and wealth distribution, educational attainment and occupational mobility. Educational policies Fiscal policies Skills training policies
2. Policies that buffer individuals from the damaging conditions of living below the top rungs of the socioeconomic ladder. Policies affecting the environment Policies affecting the workplace Policies enabling healthier behaviors

• Sixty-four percent of white women ages 65 to 69 received recommended breast cancer screenings in 2004 and 2005, compared with 57% of black women, while screening rates by state ranged from 74% in Maine to 56.9% in Mississippi (Wilde Mathews, Wall Street Journal, 6/5);
• In all but two states, blacks with diabetes were less likely than whites to receive annual hemoglobin testing, and in Colorado, 66% of blacks were screened, compared with 88% of blacks in Massachusetts (New York Times, 6/5); and
Blacks nationwide had their legs amputated at about four times the rate of whites. Black residents of Louisiana, Mississippi and South Carolina had six amputations per 1,000 Medicare beneficiaries, while blacks in Colorado and Nevada had less than two per 1,000 beneficiaries (Appleby, USA Today, 6/5).
Recent study examined Medicare claims over the past two decades for evidence of racial and geographic disparities in several indicators of health care quality
Dartmouth Atlas of Healthcare, www.dartmouthatlas.com. Accessed June 6, 2008

Robert Wood Johnson Foundation Announces $300-Million Commitment to Narrow Health Disparities Across Lines of Race and Geography
June 5, 2008
Disparities in the quality of care spur nation's largest health care philanthropy to attack the problem in 14 communities across America
Aligning Forces for Quality will concentrate its resources in 14 communities across the country:
Cincinnati, Ohio Cleveland, Ohio Detroit, Mich. Humboldt County, Calif. Kansas City, Mo. Maine Memphis, Tenn. Minnesota Seattle, Wash. South Central Pennsylvania Western Michigan Western New York Willamette Valley, Ore. Wisconsin

“If you don’t know where you are going, you might wind up
somewhere else.”
Yogi Berra
Revised definition of health:
A condition of physical, mental, spiritual, and social well-being arrived at through a balance of
prevention, health education and health protection, culminating in an enhanced socially and economically
productive life.
World Health Organization, 1948Downie, Fyfe, and Tannahill, 1990Saracci, 1997

Are we ready for a paradigm shift?

In order to resolve health care disparities, we must pay attention to the broader social forces that influence
health. We must recognize that our health is intimately related to the health of our neighborhoods, and that health care should be tied to health promotion, the
formation of healthy communities that provide a safe living environment, living wage jobs, affordable
housing, and high quality schools.
Conclusion:




![Social is Open Market [Paradigm Shift]](https://static.documents.pub/doc/80x56/5482ce49b4af9f18228b461b/social-is-open-market-paradigm-shift.jpg)












