CHAPTER - III HEALTH PLANNING IN MAHARASHTRA STATE 3.1 INTORDUCTION Located in the north centre of peninsula of India, with the command of Arabian Sea, Marathi speaker occupied, ranking in second position in case of population (census 2001) and ranking in third position in case of area Maharashtra is the leading state of the Indian Republic. According to census 2001, Maharashtra population was 9.69 crore, the percentage of urban population in the State was 42.6 and Maharashtra was second most urbanised state after Tamil Nadu. At the same time out total of the population, 57.6 per cent people were residing in 43722 villages. The present chapter deals with the constitutional provision of public health expenditure, health infrastructure in the state and its impact on health indicators especially with the reference of rural area of Maharashtra State. 3.2 PUBLIC HEALTH SYSTEM AT STATE GOVERNMENT LEVEL A State Health Department, being one degree nearer the individual citizen, has greater authority than any other jurisdiction and a more intimate relation to local health departments that the Central government. 1 According to Constitution of India health is the subject of the state government. The Directive Principles of the Indian Constitution enunciate that, “the state shall regard the raising of the level of nutrition and the standard of living of its people and the improvement of public health as among its primary duties”
Transcript
CHAPTER - III
HEALTH PLANNING IN
MAHARASHTRA STATE
3.1 INTORDUCTION
Located in the north centre of peninsula of India, with the command of
Arabian Sea, Marathi speaker occupied, ranking in second position in case of
population (census 2001) and ranking in third position in case of area
Maharashtra is the leading state of the Indian Republic. According to census
2001, Maharashtra population was 9.69 crore, the percentage of urban
population in the State was 42.6 and Maharashtra was second most urbanised
state after Tamil Nadu. At the same time out total of the population, 57.6 per
cent people were residing in 43722 villages.
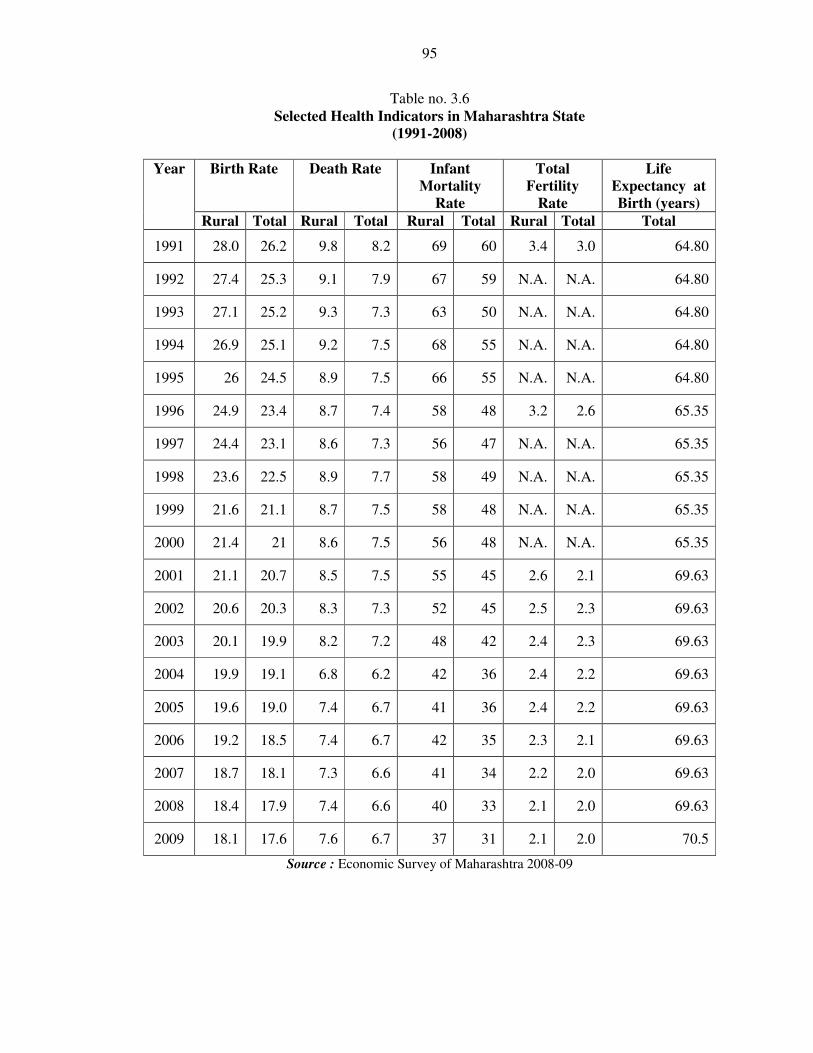
The present chapter deals with the constitutional provision of public
health expenditure, health infrastructure in the state and its impact on health
indicators especially with the reference of rural area of Maharashtra State.
3.2 PUBLIC HEALTH SYSTEM AT STATE GOVERNMENT
LEVEL
A State Health Department, being one degree nearer the individual
citizen, has greater authority than any other jurisdiction and a more intimate
relation to local health departments that the Central government. 1According to
Constitution of India health is the subject of the state government. The
Directive Principles of the Indian Constitution enunciate that, “the state shall
regard the raising of the level of nutrition and the standard of living of its
people and the improvement of public health as among its primary duties”
72
(Article 47). After the making health policy for health by central government, it
is the responsibility of the state government to execute the policy. In this
direction the implementation, surveillance and providing technical assistance at
local level are functions to be accomplished by the state governments. To
provide medical services and public health facilities to the people are the main
functions of the state governments, in it includes the Hospitals, pharmaceuticals
and similar services. Due to decentralisation of democracy, Zila Parishad
provides all kinds of health services to the rural area, while in the urban area it
is the responsibility of Municipal Corporation. For the convenience of study
the public health scheme is divided into two parts, 1. Environmental Health
Services and 2. Personal Health services. The local government performs these
functions on behalf of state governments.
1. Environmental Health Services
In order to control and eradicate epidemics and other diseases, sanitation
services played a vital role. The state government did not perform this kind of
work directly, however, the local governments have to accomplish this work.
Environmental Health Services include the services such as public sanitation
services. The state government provides medical and health, guidance and
surveillance related, help to all local governments.
2. Personal Health Services
The purpose of environmental health is to bring about conditions that
will promote health and prevent diseases. The concept of environment includes
water supply, disposal of wastes, and housing, personal hygiene and disease
control. Personal health services refer to the health services where people
benefited individually by the health services. It includes the Maternal and Child
Health Services, School Health Programmes, etc. At the same time it includes
the hospitals, doctors, nurses and paramedical staff who treat the patients. In
case of rural area the state government deputed the functions like
environmental health services to the Village Panchyat, while the personal
health services were deputed to the Zila Parishad.
73
3.3 HEALTH ADMINISTRATION IN THE
MAHARASHTRA STATE
In all States, the management sector comprises of the State Ministry of
Health and A Director of Health. The State Health Ministry is headed by the
Minister of Health and Family Welfare who is elected by the people. The
Health Secretary is usually a senior I.A.S. Officer. The Health Ministry deals
mainly with administration, and policy decisions, approval of plans, finance
and Budget. The Health Directorate is headed by the Directorate of Health
Services. He is the chief technical adviser to the State Government on health
matters. The Director of Health Services has several assistants who are MCH,
Family Welfare, Nutrition, Communicable Diseases and Health Education.
Functions of the State Health Director
The functions of the State Health Director are given below:
1. Formulating the plan for health services, directing the approved health
programmes and evaluating them.
2. Rendering preventive services and curative health services
3. Supervision of PHCs through the organisation of District Health Services
4. Control of milk and food sanitation and adulteration
5. Execution of central government health programmes e.g. MCH and Family
Welfare
6. Recruitment of personnel for rural health services
7. Training of P.H. Nurses, Sanitarians, Health Assistants and Health Workers,
(former ANMs).
8. Promotion of health education and nutrition programmes
9. Collection of vital statistics
10. Co-ordination of health with other Ministries of the State, with the Central
Health Ministry and with voluntary agencies.
74
3.4 HEALTH ORGANISATION
Medical Services in Maharashtra States was organised in the beginning
of the 19th
century. The year 1942 was considered an important landmark
regarding more recent origin of Health Services. Till recently the Medical and
Public Health Department were functioning independently of each other at the
State, Divisional and District levels. The Medical Department was under the
Surgeon General and the Public health Department worked under the Director
of Public Health.
The Medical Department looked after curative medical care as well as
Medical Education including training of medical and para-medical medical
personnel and the Public Health Department was in-charge of preventive health
services and family planning. Thus the responsibility for Medical Care and
Education on the one hand and that for Medical Care in rural areas, control of
communicable diseases, maternal and child health education on the other, was
clearly divided into two separate and independent compartments. To achieve
proper coordination in total health care and to avoid duplication of efforts and
overlapping of work an integration of these two services became necessary.
Government took steps in this direction and from 1970,1 the post of Director of
Public Health was abolished and the post of Director of Health Services was
created with Headquarters at Bombay to control both Medical and Public
Health Services in the State excluding Medical Education and Research.
Similarly the post of ‘Surgeon General’ was abolished and instead the post of
Director of Medical Education and Research was created.
The Director of Health Services is assisted by five Joint Directors of
Health Services, two being stationed at Bombay and the other three at Pune.
Out of the three Joint Directors at Pune one looks exclusively after Family
Planning, Maternal and Child Health and School health work. Further, the
Deputy Directors of Medical Services and Deputy Directors of Public Health
Services were changed to Deputy Directors of Health Services (Bombay).
Besides the Joint Directors of Health Services, there is a Deputy Director of
Health Services. The whole State, at the Divisional Level, has been divided
75
into Seven Circles for convenience of administration and each Circle is in-
charge of a Deputy Director of Health Services.
All the health related functions are performed by the minister of health.
These functions are performed by the Urban Development Minister through the
local governments instead of Minister of Health. In case of urban area Urban
Development Minister surveys the work of Municipal Corporation and
Corporation. There is also a Health Officer in the corporation to carry out the
health programmes. The Ministry of Health provides technical guidance to
them, but cannot interfere in the work or directly supervise them. This is same
in the case of rural area. The health officer of the Zila Parishad and their
assistant health officer carry out the health programmes through the health staff.
HEALTH BODIES
3.4.1 STATE HEALTH MISSION
Recognizing the importance of health in the process of economic and
social development and improving the quality of life of our citizen particularly
of poor and vulnerable section of the population the central government has
resolved to launch the National Rural Health Mission to carry out the necessary
architectural correction in the basic health care delivery system. The mission
adopts a synergic approach relating health to the determinant of good health
viz. segment of nutrition, sanitation, hygiene and safe drinking water. It also
aims at mainstreaming the Indian system of medicines to facilitate health care.
The plan of action includes increasing public expenditure on health,
reducing regional imbalances in health infrastructure, pooling resources
integration of organizational structure, optimization of health management
decentralization of district management of health programs, community
participation, ownership of assets induction of management and financial
personnel into the district health system and operationalization of community
health center into functional hospital meeting Indian public health standard in
each block of the state.
76
The implementation of the National Rural Health Mission with
architectural correction was under active consideration of the Government of
Maharashtra. In this regard Government of Maharashtra has passed the
following resolution:
Resolution: Government is pleased to constitute a State Health Mission on the
lines of the National Rural Health Mission. Composition of mission is as
follows:
Hon. Chief Minister is the Chairperson, Hon. Dy. Chief Minister is Co.
chairperson, and Hon. Minister Public Health is Dy. Chairman. Hon.
Additional Chief Secretary is the member secretary. The State Health Mission
meets at least once in every 6 months. The business of the mission is as follow:
• Providing health system oversight
• Consideration of policy matters related with health sector (including
determinants of good health) review of progress in implementation of
NRHM.
• Inter sectoral coordination
• Advocacy measures required to promote NRHM visibility.
The state health mission was constituted on15th
October 2005
3.4.2 STATE HEALTH SOCEITY
The state health society was constituted on 24th October 2005. State
health society comprises of governing body and executive committee, which
serves in an additional managerial and technical capacity to the dept of public
health for effective implementation of NRHM / RCH II.
a) The governing body has Chief Secretary as the Chairperson, Principal
Secretary Planning Department as the co-chair person and Additional Chief
Secretary Health as the Vice-Chairperson. Mission Director is the member
secretary of the governing body. The committee has also nominated non
77
official members and representatives from development partners as members.
The business of the governing body is as follows :
• Approval /endorsement of annual state action plan for the NRHM.
• Consideration of proposals for institutional reforms in health and family
welfare sector.
• Review of implementation of annual action plan
• Inter sector coordination: all NRHM related sectors and beyond
(e.g. administrative reforms across the state)
• Status of follow up action on decision of the State Health Mission.
• Coordination with NGOs / donors / other agencies / organizations.
b) The executive body has Additional Chief Secretary Health as the
Chairperson, Commissioner Family Welfare as the Co-chair Person and
Director Health Services as the Vice-Chairperson. Mission Director is the
member secretary of the executive body. These committee has also nominated
non official members and representative from development partners as
members. The business of the executive body is as follows:
• Detailed implementation and expenditure review
• Approval of proposals from district and other implementing agencies /
district action plan
• Execution of the approved state action plan, including release of funds
for programmes at state level as per annual action plan
• Release of funds to the district health society
• Finalization of working arrangement for intra sectoral and inter-sectoral
coordination.
• Follow up action on decision of the governing body.
After sanction of state action plan by the governing body of the State
Health Society and of district plans by executive committee funds are released
through joint signature of authorized signatories.
78
3.4.3 DISTRICT HEALTH MISSION
On the lines of State Health Mission every district has a District Health
Mission headed by the Chairperson Zila Parishad and District Collector as the
Co-chairperson and Chief Executive Officer as the Mission Director. To
support the District Health Mission every district has a District Integrated
Health and Family Welfare Society and all the existing societies are merged in
it.
3.5 SOME IMPORTANT HEALTH PROGRAMMES RUN BY
PUBLIC HEALTH CARE SYSTEM IN MAHARASHTRA
STATE
To cure the disease and heal the injuries and give relief from pains to the
patients is the first responsibility of every public health center. At the same
time, execution of the various health programs deputed by the Central and State
Government is also the responsibility of public health centers. Hitherto several
measures have been undertaken by the Central and State Government to
improve the health of the people. However, The Central Government cannot
maintain an organization reaching every individual and protecting every
community with adequate service. Not only would such an organization fail;
but in this country of local government such a situation would not and should
not be tolerated. It is but slightly less absurd to expect a state.3 State
Government has successfully implemented these programs through the public
health care system. A brief account of these programs which are currently in
operation is given below :
3.5.1 FAMILY WELFARE
The family welfare program is being implemented in the State since
1957. It is a high priority program. To stabilize population and improve quality
of life is the main objective of this program. Sterilization program under family
welfare is well established in the state. During the 2008-09 there were 238.5
79
thousand sterilization operations performed with different sterilization methods
in the State, however the target (450 thousand) was not achieved.4
3.5.2 REPRODUCTIVE AND CHILD HEALTH PROGRAMME (RCH)
With an objective to improve the performance of family welfare in
reducing maternal and infant mortality, unwanted pregnancies and thus lead to
population stabilization the Second Phase of Reproductive and Child Health
(RCH-II) was launched on 1st April, 2005 for period of five year. During the
2008-09 Rs. 224.64 crore were sanctioned and an expenditure 0of Rs. 177.16
crore was incurred under the RCH.5
3.5.3 JANANI SURAKSHA YOJANA (JSY)
The Janani Suraksha Yojana (JSY) is a modified scheme of National
Maternal Benefit Scheme. JSY is being implemented in the State since 2005-06
with objective of reducing maternal and neo-natal mortality by promoting
institutional deliveries among the poor pregnant women. Under the scheme, for
urban area, Rs. 600 and for rural area Rs. 700 is given to the beneficiary after
delivery in the institution within seven days while for home delivery an amount
of Rs. 500 is given to the beneficiaries having up to two living children. During
the 2008-09 Rs. 23.81 crore expenditure was incurred under the same scheme.6
3.5.4 NATIONAL RURAL HEALTH MISSION (NRHM)
Recognizing the importance of health in the process of economic and
social development and to improve the quality of life of its citizens National
Rural Health Mission (NRHM) was launched on 12th
April, 2005. The main
aim of NRHM is to provide accessible, affordable, accountable, effective and
reliable primary health care and bridging the gap between rural health care
through creation of a cadre of Accredited Social Health Activist (ASHA). The
mission will be an instrument to integrate multiple vertical programs along
with their funds at the district level. The programs to be integrated are existing
80
programs of health and family welfare including RCH-II; National Vector
Borne Disease Control Programs against malaria, filaria, kala azar, dengue
fever, etc.; National Leprosy Irradiation Program, National Tuberculosis
Program, National Program for Control of Blindness, Iodine Deficiency
Disorder Control Program and Integrated Disease Surveillance Project. The
NRHM also attempts to make effective integration of health determinants like
sanitation and hygiene, nutrition and safe drinking water.7
3.5.5 SCHOOL HEALTH PROGRAM
Under this programme students from I to IV standard are examined
every year and are provided free of cost medical services. For needy students
even major operations like cardiac surgeries are provided free of cost. During
2008-09 about 108.02 lakh students from 79543 schools throughout the State
were examined and primary treatment was given for illness and referral
services were provided for major illness.8
3.5.6 UNIVERSAL IMMUNIZATION
Universal Immunization Program was started in 1985-86 to achieve 100
per cent immunization and to reduce mortality and morbidity among infant and
young children due to vaccine preventable diseases such as Tuberculosis (T.B.),
diphtheria, whooping cough, tetanus, polio, measles. The immunization
programs include the vaccination like BCG, DPT, Polio, Hib, Measles, DT,
Tetanus etc. Over the period, coverage of different vaccination is increasing but
it has yet to reach the cent per cent target. During 2008-09 the State
Government has incurred an expenditure of Rs. 11.26 crore under this head.9
3.5.7 PULSE POLIO PROGRAM
The Pulse Polio Immunization Program is the largest ever conducted
program of immunization in every country across the world. In India, with
intension to eradicate polio disease from all over the country Pulse Polio
81
Immunization Program was started on 9th
December 1995. Maharashtra State
has made good progress in controlling the spread of wild polio virus in the
State. Under this programme, all children below 5 years of age are given dose
of oral polio vaccine. During 2008-09 an expenditure of Rs. 26.64 crore was
incurred for the program.
3.5.8 NATIONAL AIDS CONTROL PROGRAM (NACP)
Looking at the gravity of HIV infections in the country, Government of
India started National AIDS Control Program (NACP) in the year 1987. It is a
100 per cent centrally sponsored scheme implemented in the State through
Maharashtra State AIDs Control Society (MSACS). Monitoring HIV
supervisors, controlling STDs, controlling the spread of HIV infection from
mother to child, condom promotion, provision of antiretroviral treatment,
school aids education, AIDS telephone helpline, etc. are the major features of
NACP. 10
3.5.9 NATIONAL VECTOR BORN DISEASE PROGRAM
National Vector Born Disease Control Program (NVBDCP) is being
implemented for prevention and control of vector borne disease like Malaria,
Lymphatic Filariasis, Japanese Encephalitis (JE), Dengue, Chikungunya and
Chandipura, etc. In 2008-09, there were 165 people died due to malaria, 21
people died due to dengue and 16 people died due to chandipura disease.
3.5.10 INFLUENZA A (H1N1) PANDAMIC (SWINE FLU)
With the time medical science has achieved a great success in control
and eradication of various endemic and pandemic chronic diseases. However,
with the changing situation diseases also changed, some new diseases raising
their heads in society, the H1N1 disease also being one of them. During 2009,
the State faced a serious problem due to Influenza A (H1N1) popularly known
as a Swine Flu. It is an air borne disease, which spreads rapidly in the
82
community through coughing and sneezing of positive patients. So far, about
4606 people have been found H1N1 positive, 224 people have died due to this
dangerous disease. Pune region was found to be the most affected area in the
state where 123 deaths occurred due to swine flu in till 2009. The State
Government accepted different measures to prevent spread of swine flu. The
measures taken by the State are as follow:
• Medical teams are deployed at air ports, railways stations, harbors and
bus stations to screen international passengers and domestic passengers
for influenza like illness.
• To isolate and treat suspected and affected cases, the Government has
started Identified Isolation Wards (IIWs) in every district. Private
hospitals have also been involved in this activity.
• Free facility of laboratory diagnosis of H1N1 is provided at National
Institute of virology, Pune and Haffkine Institute, Mumbai.
• 142 members ‘Rapid Response Team’ (RRT) have been trained to tackle
swine flu
• Sufficient quantity of Temiflu capsule, syrups, masks, hand sanitizers
are provided.
Up to the end of November 2009, 107 IIWs and 1501 screening centers are
available in the State, 0.79 lakh suspected cases have been given Temiflu.
Along with these health programs Jeevandayi Arogya Yojana (JAY)
providing financial assistance to BPL families for major surgeries of organs,
Navsanjivani Yojana to reduce maternal mortality and infant mortality in tribal
areas, Matrutva Anudan Yojana (MAY) to provide health services to pregnant
women, antenatal care (ANC) Registration, regular health check up and to
provide required medicine to women in tribal area have been implemented in
the State.
83
3.6 EXPENDITURE ON PUBLIC HEALTH OF
MAHARASHTRA STATE
There has been no standard definition of health care expenditure. It is a
well known fact that the health status of the people is influenced by a large
number of factors and is a function of medical care, income, education, sex,
marital status, and environmental pollution etc. Given too many factors
influencing health it becomes difficult to define what items constitute health
care spending and what truly reflects health care expenditure. However, expert
on health economics have explicitly mentioned that all that activities that
primarily and significantly contribute for improving health status of the people
should be included and others should be judged on their merit. (Berman
Peter,1994)
As we know medical and health comes under the State list. Under the
revenue expenditure head developmental expenditure of state government
incurred a huge amount on the social services. Expenditure on social services
includes the heads such as education, sports, cultural, expenditure on health and
family welfare, water supply, sanitation, information and broadcasting,
SCs/STs and OBCs welfare scheme, social welfare, nutrition, etc. An
expenditure on health and family welfare is one of the most significant
elements of expenditure on social services. In order to increase health status the
state government has spent a huge fund under the head of health and family
welfare. However, India’s social services were used relatively little by the poor.
The health of the poor has improved but not as a whole. Physical access to
health services has improved but inequalities exist because of biases in locating
facilities.11
Social services policies are not comprehensive enough and the quality of
services is low. The bureaucracy is inadequate to reach the poor. Existing
capacity and resources are inadequate, particularly for education and health.12
84
Table no. 3.1
Growth Profile of Expenditure of Maharashtra State on Public Health (Rs. in crore)