Review Health related quality of life in head and neck cancer treated with radiation therapy with or without chemotherapy: A systematic review Jonathan Klein, Jonathan Livergant, Jolie Ringash ⇑ Department of Radiation Oncology, University of Toronto, Princess Margaret Hospital, Toronto, ON M5G 2M9, Canada article info Article history: Received 20 December 2013 Received in revised form 23 January 2014 Accepted 27 January 2014 Available online 18 February 2014 Keywords: Head and neck neoplasms Squamous cell carcinoma Radiotherapy Chemoradiotherapy Quality of life Questionnaires Systematic reviews summary Health-related quality of life (HRQoL) is a subjective measure of patients’ experience of disease and treatment. We systematically reviewed the literature to identify high quality manuscripts reporting HRQoL outcomes in adults with squamous cell carcinoma of the head and neck (HNSCC) treated with an organ-sparing curative regimen of radiation therapy with or without chemotherapy. Assessments were performed independently by two reviewers; a third reviewer resolved disputes. High quality reports were reviewed in detail to identify trends in HRQoL outcomes. MEDLINE and EMBASE searching yielded 276 distinct reports, plus 24 added via hand search. Of these, 53 met eligibility criteria and 18 were deemed high quality reports on the basis of a quality assessment tool. HRQoL declines after treatment but recovers to baseline levels, generally within 12 months. However, xerostomia-related HRQoL deficits may remain long-term. Combined chemoradiotherapy showed a trend toward worse HRQoL compared with RT alone. Intensity modulated radiotherapy (IMRT) yields better HRQoL compared with conventional or three-dimensional conformal radiotherapy. Baseline HRQoL may independently predict local-regional control and overall survival. Future research should incorporate HRQoL into phase III trials. However, adequate effort and journal space must be afforded to the HRQoL results of these studies to ensure proper reporting methods are followed, allowing clinicians to incorporate HRQoL into patient counseling and clinical decision making. Ó 2014 Elsevier Ltd. All rights reserved. Introduction Treatment of squamous cell carcinoma of the head and neck (HNSCC) frequently requires multi-modality intervention involv- ing surgical, medical, and radiation oncology. With improvements in radiation therapy (RT) and chemotherapy, organ-conserving treatments are increasingly employed to preserve speech, swal- lowing, and other regional functions [1]. Traditionally, treatment evaluation has focused on objective measures like survival time, tumor recurrence, or standardized toxicity grading by health professionals [2–4]. While important, these measures do not directly reflect the patient’s experience of their disease, treatment, or changes in their sense of wellbeing. The World Health Organization defines health-related quality of life (HRQoL) as a construct affected by patients’ ‘‘physical health, psychological state, level of independence, social relationships, and their relationships to salient features of their environment [5]’’. It has been incorporated into cancer research to reflect pa- tients’ experiences of their illness and treatment [6]. Information from physicians about expected HRQoL outcomes will better equip patients ‘‘to actively participate in the medical decisions concern- ing their care [2]’’. HRQoL can be severely affected by HNSCC and its treatment since social and emotional interactions are largely dependent on structural and functional integrity of organs of the head and neck [7]. Standardized tools have been developed to measure both gen- eral HRQoL aspects (e.g. effects on social interaction, appetite loss, or depression) and concerns specific to certain disease sites (e.g. dysphagia, speech deficits, or facial numbness for HNSCC patients) [8]. The most commonly used HNSCC-specific instruments in pub- lished reports include [9]: the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire (QLQ-C30 and HN-35 module) [10,11], University of Washington http://dx.doi.org/10.1016/j.oraloncology.2014.01.015 1368-8375/Ó 2014 Elsevier Ltd. All rights reserved. ⇑ Corresponding author. Address: Department of Radiation Oncology, Princess Margaret Hospital, 610 University Avenue, Toronto, ON M5G 2M9, Canada. Tel.: +1 (416) 946 2919; fax: +1 (416) 946 6561. E-mail addresses: [email protected](J. Klein), jonathan.livergant@ rmp.uhn.on.ca (J. Livergant), [email protected](J. Ringash). Oral Oncology 50 (2014) 254–262 Contents lists available at ScienceDirect Oral Oncology journal homepage: www.elsevier.com/locate/oraloncology
Jonathan Klein, Jonathan Livergant, Jolie Ringash ⇑Department of Radiation Oncology, University of Toronto, Princess Margaret Hospital, Toronto, ON M5G 2M9, Canada
a r t i c l e i n f o
Article history:Received 20 December 2013Received in revised form 23 January 2014Accepted 27 January 2014Available online 18 February 2014
Keywords:Head and neck neoplasmsSquamous cell carcinomaRadiotherapyChemoradiotherapyQuality of lifeQuestionnairesSystematic reviews
s u m m a r y
Health-related quality of life (HRQoL) is a subjective measure of patients’ experience of disease andtreatment. We systematically reviewed the literature to identify high quality manuscripts reportingHRQoL outcomes in adults with squamous cell carcinoma of the head and neck (HNSCC) treated withan organ-sparing curative regimen of radiation therapy with or without chemotherapy. Assessmentswere performed independently by two reviewers; a third reviewer resolved disputes. High qualityreports were reviewed in detail to identify trends in HRQoL outcomes. MEDLINE and EMBASE searchingyielded 276 distinct reports, plus 24 added via hand search. Of these, 53 met eligibility criteria and 18were deemed high quality reports on the basis of a quality assessment tool.
HRQoL declines after treatment but recovers to baseline levels, generally within 12 months. However,xerostomia-related HRQoL deficits may remain long-term. Combined chemoradiotherapy showed a trendtoward worse HRQoL compared with RT alone. Intensity modulated radiotherapy (IMRT) yields betterHRQoL compared with conventional or three-dimensional conformal radiotherapy. Baseline HRQoLmay independently predict local-regional control and overall survival. Future research should incorporateHRQoL into phase III trials. However, adequate effort and journal space must be afforded to the HRQoLresults of these studies to ensure proper reporting methods are followed, allowing clinicians toincorporate HRQoL into patient counseling and clinical decision making.
� 2014 Elsevier Ltd. All rights reserved.
Introduction
Treatment of squamous cell carcinoma of the head and neck(HNSCC) frequently requires multi-modality intervention involv-ing surgical, medical, and radiation oncology. With improvementsin radiation therapy (RT) and chemotherapy, organ-conservingtreatments are increasingly employed to preserve speech, swal-lowing, and other regional functions [1].
Traditionally, treatment evaluation has focused on objectivemeasures like survival time, tumor recurrence, or standardizedtoxicity grading by health professionals [2–4]. While important,these measures do not directly reflect the patient’s experience oftheir disease, treatment, or changes in their sense of wellbeing.
The World Health Organization defines health-related quality oflife (HRQoL) as a construct affected by patients’ ‘‘physical health,psychological state, level of independence, social relationships,and their relationships to salient features of their environment[5]’’. It has been incorporated into cancer research to reflect pa-tients’ experiences of their illness and treatment [6]. Informationfrom physicians about expected HRQoL outcomes will better equippatients ‘‘to actively participate in the medical decisions concern-ing their care [2]’’.
HRQoL can be severely affected by HNSCC and its treatmentsince social and emotional interactions are largely dependent onstructural and functional integrity of organs of the head and neck[7]. Standardized tools have been developed to measure both gen-eral HRQoL aspects (e.g. effects on social interaction, appetite loss,or depression) and concerns specific to certain disease sites (e.g.dysphagia, speech deficits, or facial numbness for HNSCC patients)[8]. The most commonly used HNSCC-specific instruments in pub-lished reports include [9]: the European Organization for Researchand Treatment of Cancer (EORTC) Quality of Life Questionnaire(QLQ-C30 and HN-35 module) [10,11], University of Washington
J. Klein et al. / Oral Oncology 50 (2014) 254–262 255
Quality of Life Questionnaire [12] (UWQOL), and FunctionalAssessment of Cancer Therapy Head and Neck Cancer question-naire (FACT-H&N) [13,14]. These instruments are all availableand validated in multiple languages [15–22].
HRQoL research for all cancer sites has proliferated. However,evaluating published data requires established standards forassessing the quality of these studies both in terms of conductand reporting [23]. Two groups (Efficace et al. [24] and Sprangerset al. [25]) contemporaneously developed criteria reflecting highquality reporting of a HRQoL study. We used a tool combiningthese criteria to evaluate the studies in this review.
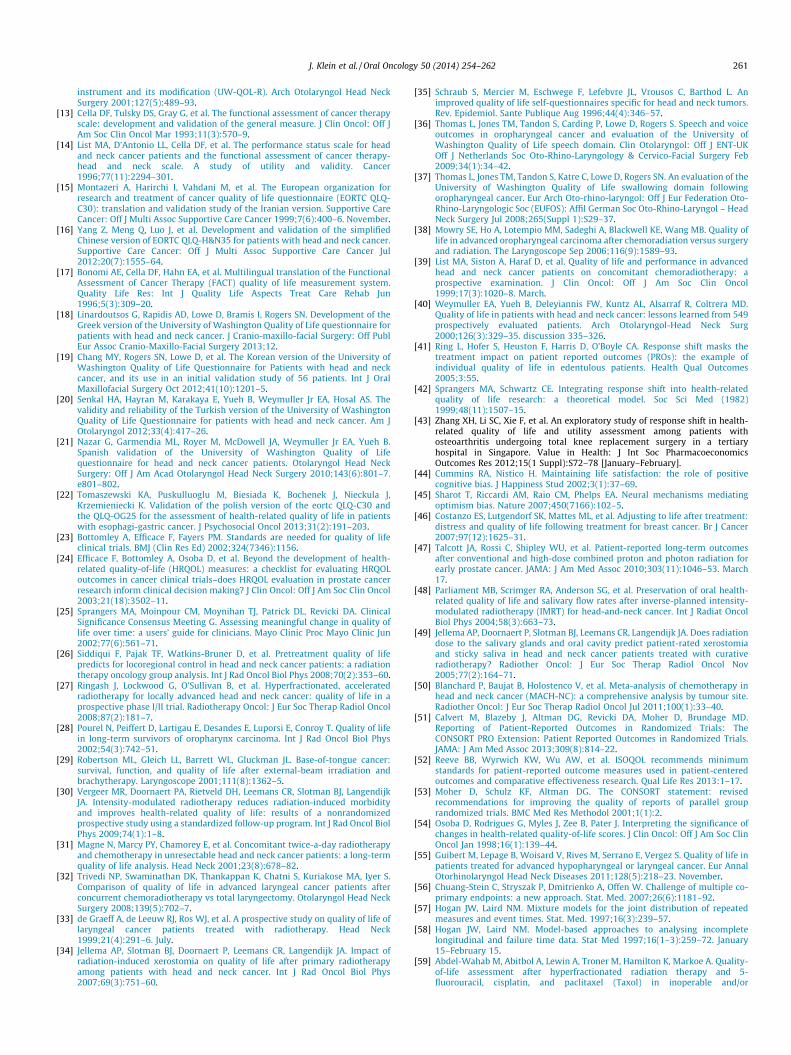
The NCIC-Clinical Trials Group (NCIC-CTG) was a pioneer instudying HRQoL within phase III cancer treatment trials. The NCICHRQoL committee has proposed a taxonomy outlining three majorways a HRQoL assessment can add value to clinical trials: by help-ing determine the best treatment, improving understanding of pa-tients’ experiences, or improving clinical trials methods. Thesegroupings are further subdivided into eight non-exclusive divisionsthat can be used to classify the contribution of individual trials tothe overall HRQoL literature [6]. We applied this taxonomy to thehigh-quality studies identified by our review.
No previous systematic review of the HRQoL literature forHNSCC has assessed the overall quality of HRQoL reporting. Wesystematically reviewed the literature using a hybrid qualityassessment tool. We also assessed the added value of high-qualitypapers using the NCIC-CTG taxonomy. We then synthesized the re-sults to provide a qualitative overview of the effect of organ-con-serving treatment on HRQoL and suggested future directions forHRQOL research in HNSCC.
Methods
Literature search
We searched the EMBASE and MEDLINE electronic databasesfrom their inceptions until 2012 using the following strategy: Med-ical subject heading (MeSH) categories ‘‘quality of life’’ and ‘‘headand neck neoplasms’’ and ‘‘carcinoma’’ and either ‘‘radiotherapy’’or textword ‘‘radiation’’, excluding the terms ‘‘esophagus,’’ ‘‘thy-roid,’’ ‘‘sarcoma,’’ ‘‘lymphoma,’’ and ‘‘melanoma.’’ The search waslimited to research performed on adult humans and published inEnglish.
Eligibility assessment
Electronic search results were combined and duplicates re-moved. We reviewed these papers to assess their eligibility forinclusion in our study. Eligible studies were published in Englishand included adult participants prescribed a non-surgical treat-ment course (neck dissection was permitted) with curative intent,including radiotherapy dose of �50 Gy, of whom greater than 50%had been diagnosed with HNSCC (i.e. excluding melanoma, lym-phoma, nasopharyngeal carcinoma, esophageal cancer, thyroidcancer, etc). HRQoL data was prospectively acquired and a vali-dated HRQoL tool used.
One reviewer (JK) performed the eligibility assessment and dis-cussed equivocal cases with a second reviewer (JL). Disagreementswere resolved first by consensus; a third reviewer (JR) adjudicatedpersistent disagreements.
We reviewed the titles of all studies and eliminated those withtitles indicating ineligibility. Reference lists of the assessed studieswere also reviewed to find appropriate studies that had beenmissed by the electronic search. We then reviewed the abstractsof the remaining studies to determine eligibility, or the whole textif sufficient information could not be gleaned from the abstract.
Quality assessment
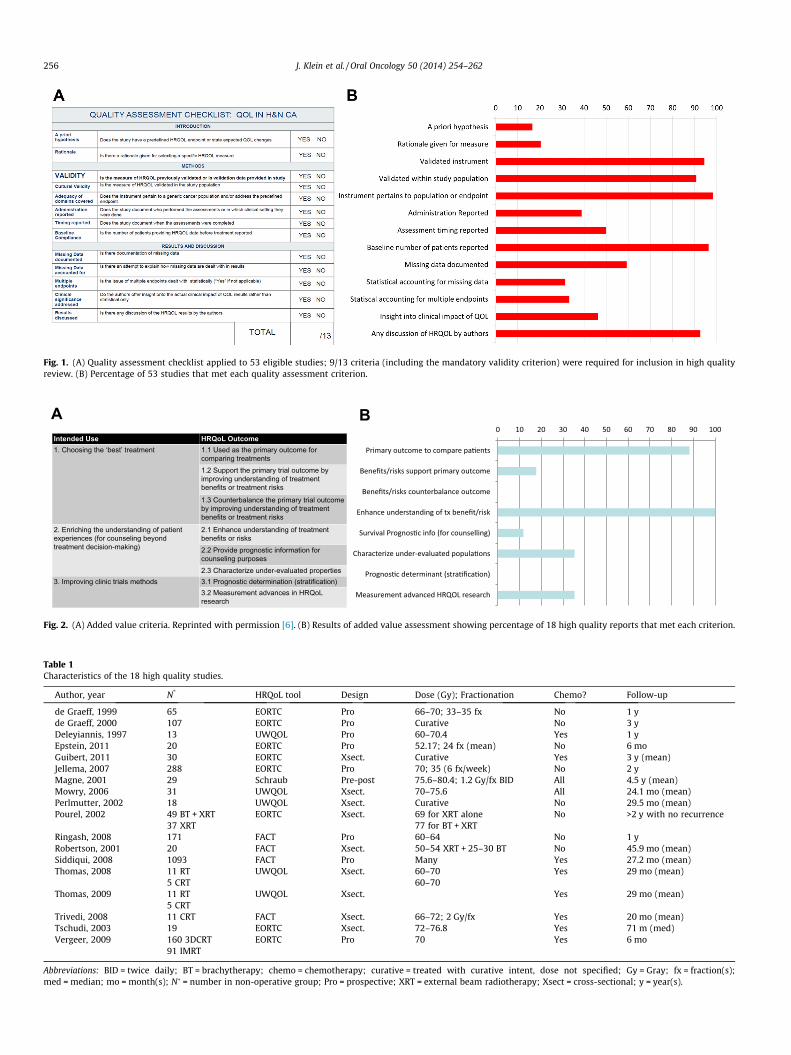
We developed a 13-item tool, shown in Fig. 1a, to assess thequality of HRQoL reporting by combining the quality assessmentcriteria from Efficace et al. [24] with those from Sprangers et al.[25] Efficace et al. defined a high quality paper as meeting 8 outof 11 criteria. We determined, a priori, that fulfillment of 9 out ofour 13 criteria, including mandatory fulfillment of the ‘‘validity’’criterion, merited inclusion.
Two reviewers (JK, JL) independently reviewed the publicationsand recorded the quality criteria that were met (or not) by each.Again, disagreement was resolved by consensus; a third reviewer(JR) resolved persistent disagreements.
Data extraction and review
For papers meeting 9 of 13 quality criteria, we recorded thenumber of participants, radiotherapy and chemotherapy regimens,study design, HRQoL outcomes, and relevant discussion themes.
Added value
We next assessed the value added by the high quality articlesusing the NCIC-CTG taxonomy, shown in Fig. 2a [6]. Articles werejudged in each category independently, so a study could add valuein one or many categories. As before, two independent reviewersassessed each study and disagreement was resolved by consensus;a third reviewer (JR) resolved persistent disagreements. Wedefined an under-evaluated population as including only a singledisease site and stage (or stage grouping such as ‘‘advanced’’), anon-standard RT schedule or technique, or a specific prognostic,socio-economic or geographic group.
Results
Literature search
EMBASE and MEDLINE searches returned 179 and 157 papers,respectively. After eliminating duplicates, 276 distinct papersremained in the database. Title review eliminated 151 studies.Review of references yielded an additional 24 papers. A total of149 were assessed in detail for eligibility.
Eligibility and quality assessment
Of 149 papers assessed, 53 papers met all inclusion criteria.Quality assessment found 18 papers meeting the required 9/13quality criteria.
Fig. 1b shows the percentage of the 53 eligible studies meetingeach quality criterion. Well-reported criteria included discussion ofHRQoL, reporting the baseline number of included patients, andwhether a validated instrument pertaining specifically to the pop-ulation or endpoint being studied was used. Conversely, fewer than20% of the studies stated an a priori hypothesis or provided anyspecific rationale for selecting the HRQoL questionnaire they usedover other validated tools.
Characteristics of the included studies are shown in Table 1.Three different study designs were used: ‘‘prospective’’ studies inwhich HRQoL was measured at predefined endpoints in a patient’scancer journey (e.g. baseline, 6 months later, 1 year, etc.); ‘‘pre-post’’ in which HRQoL was measured for all patients at baselineand then compared with a cross sectional HRQoL assessment ofresponding patients at a fixed time; and ‘‘cross-sectional’’ whichmeasured HRQoL at a single time point without baseline data.
A B 0 10 20 30 40 50 60 70 80 90 100
Primary outcome to compare pa�ents
Benefits/risks support primary outcome
Benefits/risks counterbalance outcome
Enhance understanding of tx benefit/risk
Survival Prognos�c info (for counselling)
Characterize under-evaluated popula�ons
Prognos�c determinant (stra�fica�on)
Measurement advanced HRQOL research
Intended Use HRQoL Outcome 1. Choosing the ‘best’ treatment 1.1 Used as the primary outcome for
comparing treatments 1.2 Support the primary trial outcome by improving understanding of treatment benefits or treatment risks
1.3 Counterbalance the primary trial outcome by improving understanding of treatment benefits or treatment risks
2. Enriching the understanding of patient experiences (for counseling beyond treatment decision-making)
2.1 Enhance understanding of treatment benefits or risks 2.2 Provide prognostic information for counseling purposes 2.3 Characterize under-evaluated properties
3. Improving clinic trials methods 3.1 Prognostic determination (stratification) 3.2 Measurement advances in HRQoL research
Fig. 2. (A) Added value criteria. Reprinted with permission [6]. (B) Results of added value assessment showing percentage of 18 high quality reports that met each criterion.
Fig. 1. (A) Quality assessment checklist applied to 53 eligible studies; 9/13 criteria (including the mandatory validity criterion) were required for inclusion in high qualityreview. (B) Percentage of 53 studies that met each quality assessment criterion.
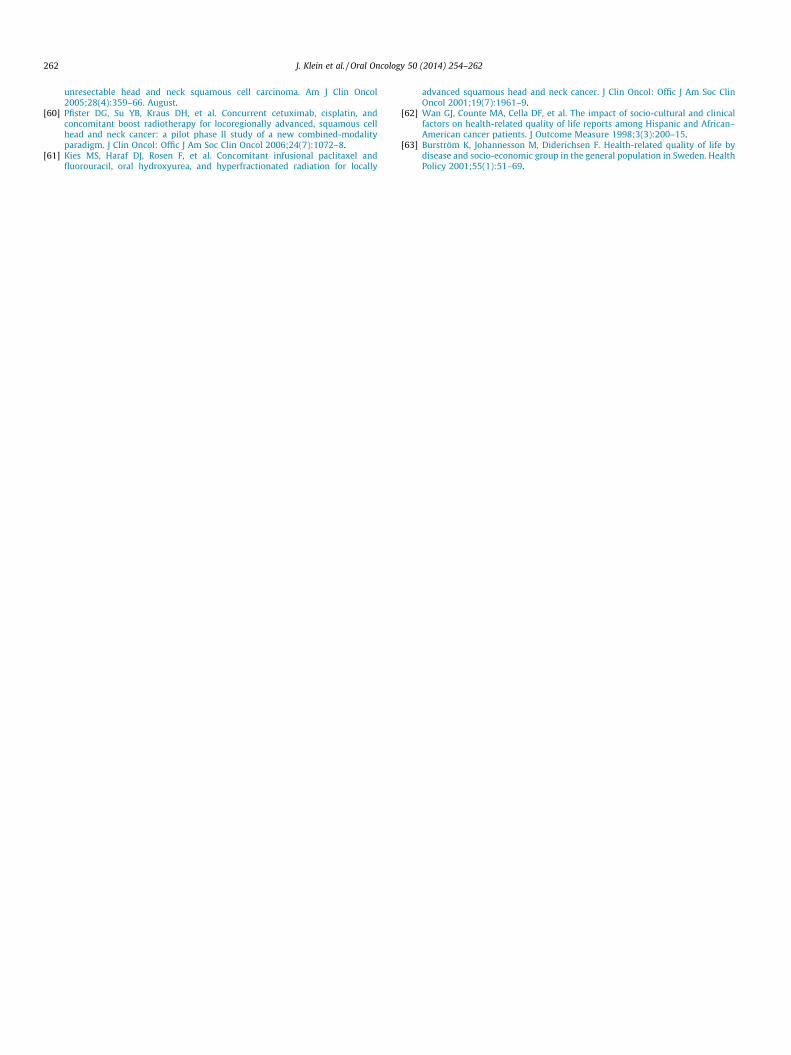
Table 1Characteristics of the 18 high quality studies.
de Graeff, 1999 65 EORTC Pro 66–70; 33–35 fx No 1 yde Graeff, 2000 107 EORTC Pro Curative No 3 yDeleyiannis, 1997 13 UWQOL Pro 60–70.4 Yes 1 yEpstein, 2011 20 EORTC Pro 52.17; 24 fx (mean) No 6 moGuibert, 2011 30 EORTC Xsect. Curative Yes 3 y (mean)Jellema, 2007 288 EORTC Pro 70; 35 (6 fx/week) No 2 yMagne, 2001 29 Schraub Pre-post 75.6–80.4; 1.2 Gy/fx BID All 4.5 y (mean)Mowry, 2006 31 UWQOL Xsect. 70–75.6 All 24.1 mo (mean)Perlmutter, 2002 18 UWQOL Xsect. Curative No 29.5 mo (mean)Pourel, 2002 49 BT + XRT EORTC Xsect. 69 for XRT alone No >2 y with no recurrence
37 XRT 77 for BT + XRTRingash, 2008 171 FACT Pro 60–64 No 1 yRobertson, 2001 20 FACT Xsect. 50–54 XRT + 25–30 BT No 45.9 mo (mean)Siddiqui, 2008 1093 FACT Pro Many Yes 27.2 mo (mean)Thomas, 2008 11 RT UWQOL Xsect. 60–70 Yes 29 mo (mean)
5 CRTTrivedi, 2008 11 CRT FACT Xsect. 66–72; 2 Gy/fx Yes 20 mo (mean)Tschudi, 2003 19 EORTC Xsect. 72–76.8 Yes 71 m (med)Vergeer, 2009 160 3DCRT EORTC Pro 70 Yes 6 mo
91 IMRT
Abbreviations: BID = twice daily; BT = brachytherapy; chemo = chemotherapy; curative = treated with curative intent, dose not specified; Gy = Gray; fx = fraction(s);med = median; mo = month(s); N� = number in non-operative group; Pro = prospective; XRT = external beam radiotherapy; Xsect = cross-sectional; y = year(s).
256 J. Klein et al. / Oral Oncology 50 (2014) 254–262
Fig. 3. Change in mean HRQoL domain scores over 1 year assessed by FACT-H&N.Reprinted with permission [27].
J. Klein et al. / Oral Oncology 50 (2014) 254–262 257
Added value
The type of value added by the 18 studies was assessed and issummarized in Fig. 2b. All 18 enhanced general understanding ofHRQoL in HNSCC patients and 16 assessed HRQoL as the primaryoutcome. None provided prognostic information for stratificationor showed that HRQoL results counterbalanced the primary studyoutcome.
Two studies reported correlation between HRQoL outcomes andsurvival, providing prognostic information for patient counseling.Based on 1,000 patients from two RTOG phase III trials, Siddiquiet al. [26] concluded that HRQoL assessed by the FACT-H&N ques-tionnaire is an independent predictor of local-regional control, butnot overall survival. HRQoL was a better prognostic factor thanKarnofsky Performance Scale. However, Ringash et al. [27] foundthat baseline HRQoL by FACT-H&N independently predicted sur-vival, reporting a hazard ratio for death of 0.61 for patients in theupper quartile of baseline HRQoL compared with the second-high-est quartile.
Seven high quality reports studied under-evaluated popula-tions. Pourel et al. [28] studied long term HNSCC survivors, includ-ing patients treated with brachytherapy (BT) plus external beamRT (EBRT) together. Robertson et al. [29] also studied BT combinedwith EBRT. Vergeer et al. [30] studied intensity modulated RT(IMRT). Magne et al. [31] and Ringash et al. [27] studied patientsreceiving altered fractionation RT. Deleyiannis et al. [2] focusedon advanced (Stage III and IV) disease of the oropharynx. Trivediet al. [32] studied a population of stage III/IV laryngeal cancer pa-tients in India.
Effect of radiation therapy on HRQoL
We found that overall HRQoL scores decline from baseline afterRT and generally return to baseline levels after around one year.However, specific HRQoL domains may not follow the sametrajectory.
De Graeff et al. [33] reported significant initial HRQoL deficits inphysical functioning, cough, social eating, dysphagia, taste/smell,dry mouth, and sticky saliva. All except the latter three domainsrecovered to baseline levels at 12 months. Emotional functioningconsistently improved over time and other measured domainsdid not change significantly. Deleyiannis et al. [2] reported a de-cline in composite HRQoL scores on the UWQOL instrument overthe first 6 months after treatment with an improvement over thenext six months. However, the composite scores at 12 months re-mained significantly worse than at baseline.
Another study by De Graeff et al. [7] reported on 107 patientswho had lived at least 3 years without recurrence after treatment.By one year after treatment, most HRQoL domains had returned tobaseline levels and remained there. The major decline in quality oflife occurs just after treatment; HRQoL gradually improves afterthis initial decline, even over many years. The authors concludedthat the impact of the disease in long term survivors seems less se-vere than is often assumed.
Epstein et al. [8] administered the EORTC QLQ-C30 question-naire just before treatment, immediately afterward and again6 months later. They showed an immediate decline after treatmentwith a gradual improvement to 6 months, although overall HRQoLat 6 months remained below the pre-treatment rating. Specific do-mains that remained significantly worse than baseline at 6 monthsincluded social functioning, fatigue, dyspnea, nausea/vomiting,constipation and financial difficulties.
Ringash et al. [27] demonstrated a decline from baseline to sixmonths after treatment in overall head-and-neck related HRQoL,measured by the FACT-H&N questionnaire, followed by animprovement from 6 to 12 months. However, other HRQoL
domains did not decline at 6 months: emotional and functionalHRQoL improved over the first six months after treatment, whilesocial and physical functioning showed a trend to improvement.These changes are shown in Fig. 3.
Both Vergeer et al. [30] and Jellema et al. [34] reported thatHRQoL from xerostomia significantly worsened at the end of radi-ation treatment, with no observed improvements after 12 months(Vergeer) or 24 months (Jellema). Vergeer observed this patternboth in patients treated with 3D conformal RT (3D-CRT) and IMRT.
Though the general decline-and-recover HRQoL trajectory held,when Pourel et al. [28] compared patients who had survived atleast 24 months after treatment with either EBRT and BT or EBRTalone, to that of an age-and-gender-matched control group with-out cancer using EORTC-QLQ30, both treated groups showed sig-nificant deficits in emotional, social, and overall HRQoL comparedwith the controls. The authors concluded that in long-term HNSCCsurvivors ‘‘emotional and social functioning remain profoundly im-paired’’ compared with people who have never had cancer.
Effect of radiation technique on HRQoL
In a comparative (but non-randomized) study using EORTCQLQ-H&N35, Vergeer et al. [30] demonstrated statistically signifi-cant reductions in patient-reported xerostomia with IMRT com-pared with conventional 3D-CRT after treatment and at 3 weeks,6 months and 12 months following treatment. At 6 months post-treatment, 67% of patients treated with 3D-CRT reported moderateor severe xerostomia compared with 41% of patients treated withIMRT. HRQoL scores reported by IMRT patients were significantlybetter than the 3D-CRT group in the global, cognitive and social do-mains as well as the symptom-specific metrics of pain, swallowing,and social eating.
Pourel et al. [28] did not show clinically significant differencesin HRQoL measured by EORTC QLQ-H&N35 between long term sur-vivors (2–9 years) treated with EBRT versus BT and EBRTcombined.
Two studies used non-standard fractionation in their treatmentplans. Jellema et al. [34] conducted a prospective study in whichpatients received 70 Gy in 35 fractions, with six fractions deliveredper week instead of the standard five. They reported a significantcorrelation between xerostomia severity and global HRQoL, fati-gue, insomnia, and all functioning scales.
Fig. 4. Pretreatment and post-treatment composite University of WashingtonQuality-of-Life (UW-QOL) questionnaire scores. Reprinted with permission [40].
258 J. Klein et al. / Oral Oncology 50 (2014) 254–262
In Magne et al’s. [31] cross-sectional study, 29 patients treatedfor stage IV HNSCC completed a French-language HRQoL question-naire developed and validated by Schraub [35] at the end of theirchemoradiotherapy (chemoRT), and again by mail between 2 and7 years after treatment (mean 4.5 years). They had been prescribeda hyperfractionated and accelerated regimen of 75.6–80.4 Gy di-vided into 1.2 Gy per fraction delivered twice daily with concur-rent chemotherapy. At the end of chemoRT, 97% experiencedmoderate or severe xerostomia; 55% still reported these symptomson the follow-up questionnaire. Psychological issues and pain ratesfell 10-fold over the follow up period. However, other symptoms,like taste, had not improved significantly since treatment.
Effect of adding chemotherapy to radiation therapy on HRQoL
Only two included papers [36,37] (both describing the samestudy) reported HRQoL data both on groups of patients treatedwith RT alone and with chemoRT. Of the 77 patients assessed withthe UWQOL questionnaire, 11 were treated with RT alone and 5with chemoRT (treatment for the remaining 61 included surgery).A non-significant trend to worse speech- and swallowing-relatedHRQoL was found in the chemoRT group compared with RT alone.
Effect of combined chemoradiotherapy on HRQoL
Ten of the 18 reports included patients treated with chemoRT(see Table 1). However, five of these did not report HRQoL sepa-rately for the RT alone and chemoRT groups and so could not in-form about differences in outcome.
Three studies [31,32,38] gave all their organ-conservation pa-tients chemoRT. Trivedi et al. [32] performed a cross-sectionalstudy using the FACT-H&N on 11 patients treated for advanced lar-yngeal cancer. Worst HRQoL domains were voice quality and drymouth, as 9 out of 11 chemoRT patients rated these domains as‘‘bad’’ (defined as scores 62 on the 0-to-4 point scale of FACT-H&N). The domains ranked most often as ‘‘good’’ (scores <2) werebreathing (10/11) and communication (9/11).
Magne et al’s. [31] cohort consisted of long term survivors whohad received chemotherapy and a hyperfractionated RT regimenand who filled out a second HRQoL between 3 and 7 years aftertreatment. Nearly all the patients had reported moderate or severexerostomia at the end of their CRT and over half (55%) still hadthese symptoms at the time of their second questionnaire. Mowryet al. [38] analyzed 31 patients with locally-advanced HNSCC of thelarynx or orpharynx (11 stage III, 13 stage IV) treated withchemoRT using the UWQOL questionnaire in a cross-sectionaldesign. The UWQOL questionnaire separates each HRQoL domaininto a set of discrete responses assigned equally-spaced pointvalues on a 0–100 scale, with 100 representing normal function.After mean follow up of 11 months (range 3–111 months), 93% ofpatients reported overall ‘‘fair’’ (40 points) or higher HRQoL, with48% reporting ‘‘good’’ HRQoL (P60). Only saliva-related HRQoLshowed a difference between the disease sites; no differences wereseen for overall HRQoL or domains such as taste, swallowing, andchewing.
Discussion
Effect of RT and ChemoRT on HRQoL
Past HRQoL studies have demonstrated a general trend, as dem-onstrated in Fig. 4: HRQoL tends to decline following treatmentand then gradually improve [39,40]. Whether HRQoL returns tothe baseline level, and when, differs by domain, population, andinstrument. This trend was confirmed by several studies in our
review, including those by Deleyiannis et al. [2], Epstein et al. [8],De Graeff et al. [7], and Ringash et al [27].
Emotional HRQoL did not follow the general decline-and-re-cover trend, and actually improved over the first year after treat-ment, as shown by both Ringash et al. [27] and de Graeff et al.[33]. Conversely, xerostomia-related HRQoL reaches a nadir atthe end of RT. Xerostomia, sticky saliva and diminished taste canbe long lasting or even permanent, as demonstrated by Vergeeret al. [30] and Jellema et al. [34].
While successful treatment and recovery from acute toxicitycertainly accounts for some improvement in HRQoL over time, cop-ing mechanisms like ‘‘response shift’’ may also contribute. In thisphenomenon, patients adjust their perception of pre-treatmentHRQoL and their judgment of ‘‘acceptable’’ HRQoL as a result oftheir disease and treatment experience [41–43]. Once the initialturmoil of treatment and toxicity has passed, patients grow accus-tomed to their new life and perceive it to be ‘‘normal.’’ HRQoLrecovery may also be influenced by ‘‘optimism bias’’ [44] wherebypatients report high HRQoL secondary to overestimating theirchances of achieving an optimal outcome once they begin to seeimprovement after treatment [45].
Patients may report that HRQoL returns to baseline levels de-spite wide differences in cosmesis or function if compared to un-treated people. Pourel et al.’s control-matched analysis showedthat long-term survivors continued to demonstrate deficits in emo-tional, social, and overall HRQoL compared with patients whonever had cancer. This unique control-matched design suggeststhat HRQoL may never return to the level enjoyed by patientswhen they were cancer free. Oncologists commonly counsel pa-tients about this ‘‘new normal’’ [46,47] noting that while theymay notice a sharp decline in HRQoL, the effects of treatment aresuch that, with time, patients rate their HRQoL similarly or betterthan at baseline.
Xerostomia is a persistent cause of diminished HRQoL in HNSCCpatients [34,48] for which a dose-response relationship has beendemonstrated [49]. Advanced RT techniques like IMRT were devel-oped with the intent to reduce dose to normal tissues comparedwith 3D-CRT while still delivering ablative doses to cancer [48].Vergeer’s non-randomized study confirmed this finding, showingthat patients treated with IMRT reported better HRQoL overalland related symptoms like pain, swallowing, and eating comparedwith 3D-CRT.
J. Klein et al. / Oral Oncology 50 (2014) 254–262 259
ChemoRT is the standard of care for locally-advanced HNSCCsuitable for organ-conserving management; concurrent treatmentusing a platinum-based agent is the dominant reported approach[50]. Chemotherapy toxicity, such as nausea/vomiting, myelosu-pression, neurotoxicity (e.g. parasthesias and tinnitus) andnephrotoxicity could significantly contribute to patients’ HRQoLexperience.
Available chemoRT studies show similar decline-and-recoverHRQoL patterns to those of other cohorts. Xerostomia also remainsa major factor with chemoRT. Deleyiannis et al. [2] showed a differ-ence between salivary HRQoL between patients with oropharynxand larynx cancer, likely reflecting the closer proximity of oropha-ryngeal disease to the parotid and other major salivary glands lead-ing to higher exposure to ablative radiation doses. However, otherdomains potentially affected by a lack of saliva (e.g. taste, swallow-ing, chewing, etc.) did not show different HRQoL scores betweenthe two groups in this study.
The lack of proper studies comparing patients treated withchemoRT and RT alone makes drawing conclusions about theadditional effect of chemotherapy on HRQoL difficult. One study,described in two separate papers by Thomas et al. [36,37], includedsmall subgroups treated with RT and chemoRT without surgery.Despite the small subgroup size and lack of discussion about theseresults, the study generated a hypothesis that chemoRT leads toworse speech- and swallowing-related HRQoL.
The results of Siddiqui et al. [26], suggesting that baselineHRQoL predicts overall survival and Ringash et al. [27], suggestingthat HRQoL predicts local control, are particularly exciting and fur-ther research should explore the relationship between HRQoLmeasures and survival outcomes. HRQoL may be a better predictorof survival than physician-reported Karnofsky Performance Status,as shown by Siddiqui et al, because HRQoL derives from thepatient’s own assessment of their condition, which may moreaccurately reflect the burden of morbidity on the patient from theirdisease than is evident to an external observer.
Further comparative studies with HRQoL outcomes and suffi-cient sample size are warranted to inform clinicians and patientsabout the trade-offs inherent in the choice between RT alone andchemoRT, as well as the effects of different fractionation schedules.These studies might particularly focus on patients with good prog-nosis or older patients, groups in whom the survival rationale forchemoRT may be less clear.
HRQoL assessment in HNSCC remains non-standardized, andthe designs of most reports were more appropriate for ‘‘hypothesisgeneration’’ than ‘‘hypothesis testing.’’ Formulation and testing ofspecific hypotheses will facilitate the availability of clinicallyrelevant data to inform patient decision-making. More data fromprospective, randomized clinical trials using validated HRQoLinstruments and adequate reporting practices is urgently needed.
Quality of HRQoL reporting
Advances in HRQoL data will be achieved only if reporting ofHRQoL studies is adequate. Future studies should particularly focuson those criteria not well reported to date. The ConsolidatedStandards of Reporting Trials (CONSORT) PRO extension found thatof nearly 800 randomized controlled trials (RCTs) which studiedpatient-reported outcomes (PROs) only 50% specifically reporteda hypothesis, 28% documented missing data and strategies toaccount for it, and 64% discussed the clinical context of the PRO[51]. Our analysis showed similar areas of poor reporting: declar-ing an a priori hypothesis (17%), proper statistical accounting formissing data or multiple endpoints (31% and 35%, respectively),and discussion of clinical relevance of the HRQoL findings (46%).Elucidation of the procedure for HRQoL assessment (38%) and
rationale for choosing a specific HRQoL assessment tool (19%) werealso not widely reported in our review.
In response to the poor reporting of PROs, two publishedstatements have outlined best practices. The International Societyfor Quality of Life Research (ISOQOL) suggested minimum stan-dards for PRO instruments, which include translation into multiplelanguages, ease of use for patients and investigators, publishedguidelines for interpretation of results (i.e. what is a ‘‘high’’ or‘‘low’’ score), and published evidence of the PRO tool’s validity,reliability, and responsiveness to changing outcomes [52]. TheCONSORT PRO extension suggested guidelines for reporting PROsin the context of RCTs, indicating that manuscripts should identifythe PRO as primary or secondary outcome, specify a hypothesis,provide evidence of instrument validity and reliability, explainstatistical approaches to deal with missing data and discussPRO–specific limitations and the generalizability of study findings[51,53].
The HRQoL questionnaires used by the studies in our review(e.g. EORTC, FACT, UWQOL) are widely-used, well-validated, andmeet the ISOQOL recommendations. Our analysis was based onquality criteria that predated the CONSORT PRO-specific sugges-tions. However, they were very similar to those suggested by CON-SORT. Identification of the PRO as a primary or secondary endpointwas incorporated into our added value analysis, while the otherfactors were included in the quality assessment procedure.
Reports often omitted such critical procedural details as whoperformed the assessment, how, and where. These are importantdetails; HRQoL instruments frequently use a recall period of oneweek or more, even though momentary experience (e.g. havingjust received bad news) could influence reporting. Similarly, per-ceived authority figures such as physicians or nurses could unin-tentionally influence patients to report either too positively(social desirability bias) or negatively (attention seeking). A pa-tient’s comfort level with their surroundings (e.g. at home or inhospital) could also influence HRQoL reporting. Detailed descrip-tion of the HRQoL assessment method will permit appropriatecomparison between studies.
Authors should also explain why a given HRQoL assessment toolwas chosen over alternatives (e.g. because it was validated in a cer-tain language or used in previous studies of similar patients) as re-sults are not directly comparable across different questionnaires.Also, since the composition of a study cohort can limit the general-izability of the findings, future studies should include well-definedinclusion criteria, recruit a more homogenous group of patients(e.g. stage, disease site, age, etc.), and perform assessments at stan-dard timepoints.
Discussion of the clinical impact of HRQoL findings deservescloser attention in publications. Most commonly, authors reportedonly numerical HRQoL results and assessed only statistical signifi-cance. However, consideration of whether or not observed differ-ences or changes in scores are large enough to be clinicallyrelevant is also necessary.
A few of the studies we identified did attempt to provide thiscontext. Pourel et al. [28] interpreted their results according to pre-viously published, instrument-specific interpretation criteria forthe EORTC QLQ-C30, as suggested by Osoba et al. [54] Mowryet al. [38] interpreted their results on the UWQOL using categoriesthe UWQOL developers established by anchoring scores to externalcriteria, allowing for better standardization of responses betweenpatients with similar HRQOL deficits. For example, when askingabout saliva function, the possible responses were ‘‘no saliva,’’‘‘too little saliva,’’ ‘‘less than normal, but adequate,’’ and ‘‘normal.’’
Proper statistical accounting for missing data or multiple end-points was also lacking in our review. The HRQoL questionnairesask large numbers of questions (FACT-H&N: 39, EORTC QLQ-H&N35: 35, UWQOL: 13) [11,12,14], generating several dozen data
260 J. Klein et al. / Oral Oncology 50 (2014) 254–262
points. Reporting scores for multiple domains increases the proba-bility of finding a statistically significant outcome simply bychance. If all outcomes are of interest, the standard 0.05 p-valuefor statistical significance is inappropriate and must be adjusted.However, many reports we reviewed simply maintained the stan-dard p < 0.05 threshold. Guibert et al.’s [55] study accounted wellfor multiple endpoints, setting their significance limit atp < 0.0015. However, a preferred strategy is to allow a pre-specifiedhypothesis to drive the choice of a primary HRQoL endpoint.
Patient availability can also bias results. Ringash et al. [27] dem-onstrated a correlation between baseline HRQoL and survival, sopatients with poor baseline HRQoL may selectively ‘‘drop out’’ ofprospective studies if they die sooner or cannot attend for appoint-ments. Alternately, patients with good HRQoL outcomes may beless motivated to present for follow up if they feel they do not re-quire medical attention. Rigorous accounting for all patients as-sessed at baseline is critical to properly analyze the effect oflosing patients to follow up. As well, methods to maximize patientcompliance with follow up procedures can minimize the bias frommissing patients. An extreme example of these problems is pre-sented by the ‘‘cross-sectional’’ or ‘‘pre-post’’ study design in whicha convenient sample of surviving, disease-free, accessible andresponding patients are included in HRQoL post-treatment analy-ses, with or without baseline data.
We found only two studies that accounted for this bias. In addi-tion to the study mentioned above, Siddiqui et al. [26] statisticallyestimated (imputed) missing data, and showed that their resultsdid not significantly change whether the imputed data were in-cluded or not. Detailed discussion of strategies to account for miss-ing patients or multiple-endpoint studies is beyond the scope ofthis review, but interested readers are referred to reviews by Offenet al. [56] and Hogan et al. [57,58].
Our literature search identified several potentially high-impactreports that did not pass quality assessment [39,59–61]. Sincestudy quality can be assessed only according to what is reported,many studies labeled ‘‘low quality’’ may have employed excellentmethods, but were unable to adequately report methodology andHRQoL results. Many high-impact studies report their HRQoL re-sults in the same manuscript as primary outcomes like survivaland toxicity. Journal word limits may leave inadequate space toproperly report on HRQoL. Potential solutions include permittinga higher word count in publications that address both survivaland HRQoL outcomes, or simultaneous publication of companionreports with one focused on survival data and the other on HRQoL.Realizing this goal would, however, require high impact journals toequally prioritize HRQoL with survival and toxicity outcomes.
Added value
The NCIC-CTG added value taxonomy was initially developedfor phase III clinical trials. Cross-sectional design, used by half ofthe studies included in this review, has many limitations, but espe-cially cannot be used as prognostic information for patient coun-seling or stratification. Future research should add HRQoLassessments to phase III or large phase II studies to correlateHRQoL with survival and toxicity data.
Seven study cohorts met our broad definition of ‘‘under-evaluated populations’’. These reports generally investigated theHRQoL effects of non-standard RT techniques like BT or alteredfractionations, although Pourel et al. studied long term survivors.More investigation is warranted into the HRQoL outcomes ofprognostic groups like HPV-positive patients or those withcommon comorbidities (e.g. diabetes mellitus). Most of the highquality reports studied patients in North American or Europeanacademic hospitals with HNSCC of several stages and primary sites.Only Trivedi et al studied a population in a different geographic
region (India). However, since HRQoL is a subjective measurement,it is affected by cultural, social, and economic factors, so specificcultural, language or geographic groups may indeed be under-evaluated [62,63].
Better understanding of HRQoL in specific patient populations,particularly those underrepresented in the literature, will helpdevelop tools to advise individual patients on HRQoL outcomesand increase the scope for trials specifically aimed at improvingHRQoL.
Conclusions
We identified 53 reports describing HRQoL in patients withHNSCC treated with radiation therapy with or without chemother-apy that met our eligibility criteria; 18 of these met quality report-ing standards. Detailed review confirmed a pattern of HRQoLdecline after treatment, with a return to, or near to, baseline levelswithin approximately 1 year in many domains. Improvement overtime may be in part related to patient adaptation or ‘‘responseshift.’’ IMRT may improve HRQoL compared with 3D-CRT. Thecurrent literature is lacking comparative research on the effect ofadding chemotherapy to radiation therapy on HRQoL in HNSCCpatients, though trends to worse HRQoL with chemoRT wereshown. Baseline HRQoL may be predictive of survival. Conclusionsrelated to underevaluated populations were limited.
More prospective HRQoL data from phase III and large phase IItrials is needed to determine the relative effects on HRQoL ofdifferent treatment strategies, including chemotherapy plus RT,and to confirm the prognostic value of HRQoL. Published reportsrequire sufficient journal space to meet HRQoL reporting standardsfor data to add value and contribute meaningfully to the overallunderstanding of HNSCC and its clinical management.
Conflict of interest statement
None declared.
References
[1] Marur S, Forastiere AA. Head and neck cancer: changing epidemiology,diagnosis, and treatment. Mayo Clinic Proc Mayo Clinic 2008;83(4):489–501.
[2] Deleyiannis FW, Weymuller Jr EA, Coltrera MD. Quality of life of disease-freesurvivors of advanced (stage III or IV) oropharyngeal cancer. Head Neck Sep1997;19(6):466–73.
[3] Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy OncologyGroup (RTOG) and the European Organization for Research and Treatment ofCancer (EORTC). Int J Rad Oncol Biol Phys 1995;31(5):1341–6.
[4] Trotti A, Colevas AD, Setser A, et al. CTCAE v3.0: development of acomprehensive grading system for the adverse effects of cancer treatment.Seminars Rad Oncol Jul 2003;13(3):176–81.
[5] Organization WH. WHOQOL: measuring quality of life. Geneva: WHO; 1997.[6] Au HJ, Ringash J, Brundage M, et al. Added value of health-related quality of life
measurement in cancer clinical trials: the experience of the NCIC CTG. ExpertRev Pharm Outcomes Res Apr 2010;10(2):119–28.
[7] de Graeff A, de Leeuw JR, Ros WJ, Hordijk GJ, Blijham GH, Winnubst JA. Long-term quality of life of patients with head and neck cancer. Laryngoscope Jan2000;110(1):98–106.
[8] Epstein JB, Robertson M, Emerton S, Phillips N, Stevenson-Moore P. Quality oflife and oral function in patients treated with radiation therapy for head andneck cancer. Head Neck May 2001;23(5):389–98.
[9] Ojo B, Genden EM, Teng MS, Milbury K, Misiukiewicz KJ, Badr H. A systematicreview of head and neck cancer quality of life assessment instruments. OralOncol 2012;48(10):923–37.
[10] Bjordal K, Hammerlid E, Ahlner-Elmqvist M, et al. Quality of life in head andneck cancer patients: validation of the European Organization for Researchand Treatment of Cancer Quality of Life Questionnaire-H&N35. J Clin Oncol:Off J Am Soc Clin Oncol 1999;17(3):1008–19. March.
[11] Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization forResearch and Treatment of Cancer QLQ-C30: a quality-of-life instrument foruse in international clinical trials in oncology. J Natl Cancer Inst1993;85(5):365–76.
[12] Weymuller Jr EA, Alsarraf R, Yueh B, Deleyiannis FW, Coltrera MD. Analysis ofthe performance characteristics of the University of Washington Quality of Life
J. Klein et al. / Oral Oncology 50 (2014) 254–262 261
instrument and its modification (UW-QOL-R). Arch Otolaryngol Head NeckSurgery 2001;127(5):489–93.
[13] Cella DF, Tulsky DS, Gray G, et al. The functional assessment of cancer therapyscale: development and validation of the general measure. J Clin Oncol: Off JAm Soc Clin Oncol Mar 1993;11(3):570–9.
[14] List MA, D’Antonio LL, Cella DF, et al. The performance status scale for headand neck cancer patients and the functional assessment of cancer therapy-head and neck scale. A study of utility and validity. Cancer1996;77(11):2294–301.
[15] Montazeri A, Harirchi I, Vahdani M, et al. The European organization forresearch and treatment of cancer quality of life questionnaire (EORTC QLQ-C30): translation and validation study of the Iranian version. Supportive CareCancer: Off J Multi Assoc Supportive Care Cancer 1999;7(6):400–6. November.
[16] Yang Z, Meng Q, Luo J, et al. Development and validation of the simplifiedChinese version of EORTC QLQ-H&N35 for patients with head and neck cancer.Supportive Care Cancer: Off J Multi Assoc Supportive Care Cancer Jul2012;20(7):1555–64.
[17] Bonomi AE, Cella DF, Hahn EA, et al. Multilingual translation of the FunctionalAssessment of Cancer Therapy (FACT) quality of life measurement system.Quality Life Res: Int J Quality Life Aspects Treat Care Rehab Jun1996;5(3):309–20.
[18] Linardoutsos G, Rapidis AD, Lowe D, Bramis I, Rogers SN. Development of theGreek version of the University of Washington Quality of Life questionnaire forpatients with head and neck cancer. J Cranio-maxillo-facial Surgery: Off PublEur Assoc Cranio-Maxillo-Facial Surgery 2013;12.
[19] Chang MY, Rogers SN, Lowe D, et al. The Korean version of the University ofWashington Quality of Life Questionnaire for Patients with head and neckcancer, and its use in an initial validation study of 56 patients. Int J OralMaxillofacial Surgery Oct 2012;41(10):1201–5.
[20] Senkal HA, Hayran M, Karakaya E, Yueh B, Weymuller Jr EA, Hosal AS. Thevalidity and reliability of the Turkish version of the University of WashingtonQuality of Life Questionnaire for patients with head and neck cancer. Am JOtolaryngol 2012;33(4):417–26.
[21] Nazar G, Garmendia ML, Royer M, McDowell JA, Weymuller Jr EA, Yueh B.Spanish validation of the University of Washington Quality of Lifequestionnaire for head and neck cancer patients. Otolaryngol Head NeckSurgery: Off J Am Acad Otolaryngol Head Neck Surgery 2010;143(6):801–7.e801–802.
[22] Tomaszewski KA, Puskulluoglu M, Biesiada K, Bochenek J, Nieckula J,Krzemieniecki K. Validation of the polish version of the eortc QLQ-C30 andthe QLQ-OG25 for the assessment of health-related quality of life in patientswith esophagi-gastric cancer. J Psychosocial Oncol 2013;31(2):191–203.
[23] Bottomley A, Efficace F, Fayers PM. Standards are needed for quality of lifeclinical trials. BMJ (Clin Res Ed) 2002;324(7346):1156.
[24] Efficace F, Bottomley A, Osoba D, et al. Beyond the development of health-related quality-of-life (HRQOL) measures: a checklist for evaluating HRQOLoutcomes in cancer clinical trials–does HRQOL evaluation in prostate cancerresearch inform clinical decision making? J Clin Oncol: Off J Am Soc Clin Oncol2003;21(18):3502–11.
[25] Sprangers MA, Moinpour CM, Moynihan TJ, Patrick DL, Revicki DA. ClinicalSignificance Consensus Meeting G. Assessing meaningful change in quality oflife over time: a users’ guide for clinicians. Mayo Clinic Proc Mayo Clinic Jun2002;77(6):561–71.
[26] Siddiqui F, Pajak TF, Watkins-Bruner D, et al. Pretreatment quality of lifepredicts for locoregional control in head and neck cancer patients: a radiationtherapy oncology group analysis. Int J Rad Oncol Biol Phys 2008;70(2):353–60.
[27] Ringash J, Lockwood G, O’Sullivan B, et al. Hyperfractionated, acceleratedradiotherapy for locally advanced head and neck cancer: quality of life in aprospective phase I/II trial. Radiotherapy Oncol: J Eur Soc Therap Radiol Oncol2008;87(2):181–7.
[28] Pourel N, Peiffert D, Lartigau E, Desandes E, Luporsi E, Conroy T. Quality of lifein long-term survivors of oropharynx carcinoma. Int J Rad Oncol Biol Phys2002;54(3):742–51.
[29] Robertson ML, Gleich LL, Barrett WL, Gluckman JL. Base-of-tongue cancer:survival, function, and quality of life after external-beam irradiation andbrachytherapy. Laryngoscope 2001;111(8):1362–5.
[30] Vergeer MR, Doornaert PA, Rietveld DH, Leemans CR, Slotman BJ, LangendijkJA. Intensity-modulated radiotherapy reduces radiation-induced morbidityand improves health-related quality of life: results of a nonrandomizedprospective study using a standardized follow-up program. Int J Rad Oncol BiolPhys 2009;74(1):1–8.
[31] Magne N, Marcy PY, Chamorey E, et al. Concomitant twice-a-day radiotherapyand chemotherapy in unresectable head and neck cancer patients: a long-termquality of life analysis. Head Neck 2001;23(8):678–82.
[32] Trivedi NP, Swaminathan DK, Thankappan K, Chatni S, Kuriakose MA, Iyer S.Comparison of quality of life in advanced laryngeal cancer patients afterconcurrent chemoradiotherapy vs total laryngectomy. Otolaryngol Head NeckSurgery 2008;139(5):702–7.
[33] de Graeff A, de Leeuw RJ, Ros WJ, et al. A prospective study on quality of life oflaryngeal cancer patients treated with radiotherapy. Head Neck1999;21(4):291–6. July.
[34] Jellema AP, Slotman BJ, Doornaert P, Leemans CR, Langendijk JA. Impact ofradiation-induced xerostomia on quality of life after primary radiotherapyamong patients with head and neck cancer. Int J Rad Oncol Biol Phys2007;69(3):751–60.
[35] Schraub S, Mercier M, Eschwege F, Lefebvre JL, Vrousos C, Barthod L. Animproved quality of life self-questionnaires specific for head and neck tumors.Rev. Epidemiol. Sante Publique Aug 1996;44(4):346–57.
[36] Thomas L, Jones TM, Tandon S, Carding P, Lowe D, Rogers S. Speech and voiceoutcomes in oropharyngeal cancer and evaluation of the University ofWashington Quality of Life speech domain. Clin Otolaryngol: Off J ENT-UKOff J Netherlands Soc Oto-Rhino-Laryngology & Cervico-Facial Surgery Feb2009;34(1):34–42.
[37] Thomas L, Jones TM, Tandon S, Katre C, Lowe D, Rogers SN. An evaluation of theUniversity of Washington Quality of Life swallowing domain followingoropharyngeal cancer. Eur Arch Oto-rhino-laryngol: Off J Eur Federation Oto-Rhino-Laryngologic Soc (EUFOS): Affil German Soc Oto-Rhino-Laryngol – HeadNeck Surgery Jul 2008;265(Suppl 1):S29–37.
[38] Mowry SE, Ho A, Lotempio MM, Sadeghi A, Blackwell KE, Wang MB. Quality oflife in advanced oropharyngeal carcinoma after chemoradiation versus surgeryand radiation. The Laryngoscope Sep 2006;116(9):1589–93.
[39] List MA, Siston A, Haraf D, et al. Quality of life and performance in advancedhead and neck cancer patients on concomitant chemoradiotherapy: aprospective examination. J Clin Oncol: Off J Am Soc Clin Oncol1999;17(3):1020–8. March.
[40] Weymuller EA, Yueh B, Deleyiannis FW, Kuntz AL, Alsarraf R, Coltrera MD.Quality of life in patients with head and neck cancer: lessons learned from 549prospectively evaluated patients. Arch Otolaryngol-Head Neck Surg2000;126(3):329–35. discussion 335–326.
[41] Ring L, Hofer S, Heuston F, Harris D, O’Boyle CA. Response shift masks thetreatment impact on patient reported outcomes (PROs): the example ofindividual quality of life in edentulous patients. Health Qual Outcomes2005;3:55.
[42] Sprangers MA, Schwartz CE. Integrating response shift into health-relatedquality of life research: a theoretical model. Soc Sci Med (1982)1999;48(11):1507–15.
[43] Zhang XH, Li SC, Xie F, et al. An exploratory study of response shift in health-related quality of life and utility assessment among patients withosteoarthritis undergoing total knee replacement surgery in a tertiaryhospital in Singapore. Value in Health: J Int Soc PharmacoeconomicsOutcomes Res 2012;15(1 Suppl):S72–78 [January–February].
[44] Cummins RA, Nistico H. Maintaining life satisfaction: the role of positivecognitive bias. J Happiness Stud 2002;3(1):37–69.
[45] Sharot T, Riccardi AM, Raio CM, Phelps EA. Neural mechanisms mediatingoptimism bias. Nature 2007;450(7166):102–5.
[46] Costanzo ES, Lutgendorf SK, Mattes ML, et al. Adjusting to life after treatment:distress and quality of life following treatment for breast cancer. Br J Cancer2007;97(12):1625–31.
[47] Talcott JA, Rossi C, Shipley WU, et al. Patient-reported long-term outcomesafter conventional and high-dose combined proton and photon radiation forearly prostate cancer. JAMA: J Am Med Assoc 2010;303(11):1046–53. March17.
[48] Parliament MB, Scrimger RA, Anderson SG, et al. Preservation of oral health-related quality of life and salivary flow rates after inverse-planned intensity-modulated radiotherapy (IMRT) for head-and-neck cancer. Int J Radiat OncolBiol Phys 2004;58(3):663–73.
[49] Jellema AP, Doornaert P, Slotman BJ, Leemans CR, Langendijk JA. Does radiationdose to the salivary glands and oral cavity predict patient-rated xerostomiaand sticky saliva in head and neck cancer patients treated with curativeradiotherapy? Radiother Oncol: J Eur Soc Therap Radiol Oncol Nov2005;77(2):164–71.
[50] Blanchard P, Baujat B, Holostenco V, et al. Meta-analysis of chemotherapy inhead and neck cancer (MACH-NC): a comprehensive analysis by tumour site.Radiother Oncol: J Eur Soc Therap Radiol Oncol Jul 2011;100(1):33–40.
[51] Calvert M, Blazeby J, Altman DG, Revicki DA, Moher D, Brundage MD.Reporting of Patient-Reported Outcomes in Randomized Trials: TheCONSORT PRO Extension: Patient Reported Outcomes in Randomized Trials.JAMA: J Am Med Assoc 2013;309(8):814–22.
[52] Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimumstandards for patient-reported outcome measures used in patient-centeredoutcomes and comparative effectiveness research. Qual Life Res 2013:1–17.
[53] Moher D, Schulz KF, Altman DG. The CONSORT statement: revisedrecommendations for improving the quality of reports of parallel grouprandomized trials. BMC Med Res Methodol 2001;1(1):2.
[54] Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance ofchanges in health-related quality-of-life scores. J Clin Oncol: Off J Am Soc ClinOncol Jan 1998;16(1):139–44.
[55] Guibert M, Lepage B, Woisard V, Rives M, Serrano E, Vergez S. Quality of life inpatients treated for advanced hypopharyngeal or laryngeal cancer. Eur AnnalOtorhinolaryngol Head Neck Diseases 2011;128(5):218–23. November.
[56] Chuang-Stein C, Stryszak P, Dmitrienko A, Offen W. Challenge of multiple co-primary endpoints: a new approach. Stat. Med. 2007;26(6):1181–92.
[57] Hogan JW, Laird NM. Mixture models for the joint distribution of repeatedmeasures and event times. Stat. Med. 1997;16(3):239–57.
[58] Hogan JW, Laird NM. Model-based approaches to analysing incompletelongitudinal and failure time data. Stat Med 1997;16(1–3):259–72. January15–February 15.
[59] Abdel-Wahab M, Abitbol A, Lewin A, Troner M, Hamilton K, Markoe A. Quality-of-life assessment after hyperfractionated radiation therapy and 5-fluorouracil, cisplatin, and paclitaxel (Taxol) in inoperable and/or
262 J. Klein et al. / Oral Oncology 50 (2014) 254–262
unresectable head and neck squamous cell carcinoma. Am J Clin Oncol2005;28(4):359–66. August.
[60] Pfister DG, Su YB, Kraus DH, et al. Concurrent cetuximab, cisplatin, andconcomitant boost radiotherapy for locoregionally advanced, squamous cellhead and neck cancer: a pilot phase II study of a new combined-modalityparadigm. J Clin Oncol: Offic J Am Soc Clin Oncol 2006;24(7):1072–8.
[61] Kies MS, Haraf DJ, Rosen F, et al. Concomitant infusional paclitaxel andfluorouracil, oral hydroxyurea, and hyperfractionated radiation for locally
advanced squamous head and neck cancer. J Clin Oncol: Offic J Am Soc ClinOncol 2001;19(7):1961–9.
[62] Wan GJ, Counte MA, Cella DF, et al. The impact of socio-cultural and clinicalfactors on health-related quality of life reports among Hispanic and African–American cancer patients. J Outcome Measure 1998;3(3):200–15.
[63] Burström K, Johannesson M, Diderichsen F. Health-related quality of life bydisease and socio-economic group in the general population in Sweden. HealthPolicy 2001;55(1):51–69.