Resuscitate Cardiac Catheterization Coding: 14 Include all information and follow the rules New Face of Patient Collections: 48 Front desk collections and post-claim payment Build a Better HIPAA Toolkit: 58 Five preventive steps show voluntary compliance www.aapc.com HEALTHCARE BUSINESS MONTHLY Coding | Billing | Auditing | Compliance | Practice Management November 2014 Your Guide to Pediatric Critical Care
Transcript
Resuscitate Cardiac Catheterization Coding: 14 Include all information and follow the rules
New Face of Patient Collections: 48 Front desk collections and post-claim payment
Build a Better HIPAA Toolkit: 58 Five preventive steps show voluntary compliance
Amp up your accuracy. Save time. Get more code sets and medical reference data and policies. Reduce denials.
Do it all with digital coding tools from Optum360™. Paired with the extensive expertise that your coding professionals bring to the table, our digital resources make the work easier, more accurate and more streamlined for your organization.
WHEN YOU TURN IT UP WITH digitAl coding tools.
EncoderPro.com for physicians and payersQuickly and easily access the content of 37 Optum360 code books in one place, with a few clicks of your mouse. Boost productivity and first-pass payment. Streamline coding and prep for ICD-10. optumcoding.com/transition
OPTPRJ5784 | SPRJ1758 | June 2014
RevenueCyclePro.com for facilitiesSimplify your research efforts with reference data compiled in one comprehensive, online problem-solving tool. Maximize your coding compliance efforts and minimize rejected and denied claims. Increase efficiency across the entire hospital revenue cycle. optumcoding.com/transition
Add-on modules Customize your online digital coding subscriptions with the tools that your office needs the most. Choose from, among others:
• CPT® Changes provides the official AMA rationales for every new, revised and deleted CPT code and guideline for the CPT code set from 2006 through the current year.
• I-10 Map Manager provides forward and backward mapping between ICD-9-CM and ICD-10-CM to get you ready in spite of industry indecision.
Check out how comprehensive digital coding tools from Optum360 can address your coding needs. Call 1-800-464-3649, option 1, for a customized demo.
Amp up Your coding cApAbilities todAY.
Call: 1-800-464-3649, option 1
Visit: optumcoding.com/transition
CPT is a registered trademark of the American Medical Association.
5784_optum360_eSolutions_BC advantage_ad.indd 1 6/18/14 9:40 AM
www.aapc.com November 2014 3
Amp up your accuracy. Save time. Get more code sets and medical reference data and policies. Reduce denials.
Do it all with digital coding tools from Optum360™. Paired with the extensive expertise that your coding professionals bring to the table, our digital resources make the work easier, more accurate and more streamlined for your organization.
WHEN YOU TURN IT UP WITH digitAl coding tools.
EncoderPro.com for physicians and payersQuickly and easily access the content of 37 Optum360 code books in one place, with a few clicks of your mouse. Boost productivity and first-pass payment. Streamline coding and prep for ICD-10. optumcoding.com/transition
OPTPRJ5784 | SPRJ1758 | June 2014
RevenueCyclePro.com for facilitiesSimplify your research efforts with reference data compiled in one comprehensive, online problem-solving tool. Maximize your coding compliance efforts and minimize rejected and denied claims. Increase efficiency across the entire hospital revenue cycle. optumcoding.com/transition
Add-on modules Customize your online digital coding subscriptions with the tools that your office needs the most. Choose from, among others:
• CPT® Changes provides the official AMA rationales for every new, revised and deleted CPT code and guideline for the CPT code set from 2006 through the current year.
• I-10 Map Manager provides forward and backward mapping between ICD-9-CM and ICD-10-CM to get you ready in spite of industry indecision.
Check out how comprehensive digital coding tools from Optum360 can address your coding needs. Call 1-800-464-3649, option 1, for a customized demo.
Amp up Your coding cApAbilities todAY.
Call: 1-800-464-3649, option 1
Visit: optumcoding.com/transition
CPT is a registered trademark of the American Medical Association.
5784_optum360_eSolutions_BC advantage_ad.indd 1 6/18/14 9:40 AM
[contents]■ Coding/Billing ■ Auditing/Compliance■ Practice Management
[continued on next page]
18 Capture All of What Oncology Costs Your Practice
Janice G. Jacobs, CPA, CPC, CPCO, CCS, ROCC
51 What Auditors Wish You Knew Lisa Jensen, MHBL, FACMPE, CPC
22 Dear John: Does Manipulation Under Anesthesia Require Fixation? John Verhovshek, MA, CPC
25 On the Cover: Your Guide to Pediatric Critical Care Holly Cassano, CPC
■Practice Management36 Procure the Best Management Report Jim Strafford, CEDC, MCS-P
40 Hire and Retain Excellent Coding Staff: Part 2 By Pam Brooks, CPC, CPC-H
44 Streamline Your Revenue Cycle: Part 3 Linda Martien, CPC, CPC-H, CPMA
48 Recognize the New Face of Patient Collections Mary Pat Whaley, FACMPE, CPC
■Auditing/Compliance51 What Auditors Wish You Knew Lisa Jensen, MHBL, FACMPE, CPC
57 Ask the LAB: Mixing Clinical and Financial Data in the Patient Portal Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO
58 Building a HIPAA Toolkit
Stacy Harper, JD, MHSA, CPC
14
40
58
On the Cover: Let Holly Cassano, CPC, guide you through the many factors that play into proper coding of pediatric critical care services. Cover design by Tina M. Smith.
6 Healthcare Business Monthly
Volume 1 Number 11 November 1, 2014Healthcare Business Monthly (ISSN: 23327499) is published monthly by AAPC, 2480 South 3850 West, Suite B, Salt Lake City UT 84120-7208, for its paid members. Periodicals Postage Paid at Salt Lake City UT and at additional mailing office. POSTMASTER: Send address changes to: Healthcare Business Monthly c/o AAPC, 2480 South 3850 West, Suite B, Salt Lake City UT 84120-7208.
Go Green!Why should you sign up to receive Healthcare Business Monthly in digital format?
Here are some great reasons:
• You will save a few trees.
• You won’t have to wait for issues to come in the mail.
• You can read Healthcare Business Monthly on your computer, tablet, or other mobile device-anywhere, anytime.
• You will always know where your issues are.
• Digital issues take up a lot less room in your home or office than paper issues.
Go into your Profile on www.aapc.com and make the change!
November 2014
www.aapc.com November 2014 7
Letter from Member Leadership
“ By Failing to Prepare, You Are Preparing to Fail”
— Benjamin Franklin
In 1990, while shopping at a grocery store near his home in Texas, an elderly man had a life threatening arrhythmia and col-
lapsed on the floor. Two bystanders imme-diately went to his rescue, initiating cardio-pulmonary resuscitation (CPR). Thanks to their quick thinking and preparedness, the man’s life was saved. This story is of particular importance to me not only because I am a doctor, but because the elderly man in this story was my father. Everyone understands the importance of being prepared and knowing what to do in a crisis, but did you know there is a difference between the two?
Enhance Your LearningScientists say the skills you learn through actual application are retained far longer and become significantly more automat-ic than acquired knowledge. I don’t know if the people who saved my father’s life had actually practiced the life saving techniques they used on him, but I suspect they did. Of all the skills you can acquire, I believe knowing techniques to save lives are some of the most valuable. Because I feel so strong-ly about this, earlier this year I arranged for onsite training at ZHealth Publishing for the American Heart Association Heartsav-er® CPR AED (automatic external defibril-lator) class.
Make a Difference When Called OnToday, it’s common to see AEDs in airports, schools, churches, recreational centers, and other public areas. These devices are very high tech and actually talk the responder through the steps of using them. But when someone’s life hangs in the balance, the
difference between what you know and what you have prac-ticed can make the critical difference in saving a life. As healthcare pro-fessionals, I know many of you are cer-tified in this type of training. If you are not, or you have let your certification lapse, I encourage you to attend a class or take a refresh-er course. This sort of training is a great thing for local chap-ters to offer mem-bers.As a doctor, a son, and a father, I know this one thing to be true: You never know when you’ll be called upon to act in a moment of crisis. Being properly prepared will empow-er you with the ability to make a difference in someone’s life.
The Same Goes for CodingWhile at the recent AAPC regional con-ference in Chicago, the importance of be-ing prepared rang even more true while I was listening to Rhonda Buckholtz, CPC, CPMA, CPC-I, CENTC, CGSC, COB-GC, CPEDC, talk about the upcoming ICD-10 implementation. She explained that many providers across the country are preparing for the upcoming ICD-10 con-version by initiating the process of dual cod-ing (coding for both ICD-9-CM and ICD-10-CM).
The reason for dual coding is simple: Know-ing and doing are two very different things. Imagine trying to drive a car or ride a bicycle by merely reading a book. It’s virtually im-possible. For learning processes that involve both skill and knowledge, you must experi-ence them before you can master them. Pro-viders who put their knowledge on the line and take up the challenge of dual coding will see a significant increase in the accura-cy and quality of their coding come Octo-ber 1, 2015. It pays to be prepared.Take care,
David Dunn, MD, FACSCIRCC, CCVTC, CCC, CPC-H, CCS, RCCPresident, National Advisory Board
ZHealth staff taking the Heartsaver® CPR AED class.
8 Healthcare Business Monthly
Letters to the Editor
Not All Payers Allow MDM Points in Addition to Professional BillingThe clinical ECG coding example in “Charge Up Your ECG Doc-umentation” (August 2014, page 16) assigns three points for “or-der and read of EKG” (e.g., data reviewed), ultimately leading to the selection of a level five emergency department evaluation and management (E/M) service (99285 Emergency department vis-
it for the evaluation and management of a patient, which requires these 3 key com-ponents within the constraints imposed by the urgency of the patient’s clinical condi-tion and/or mental status: A comprehen-sive history; A comprehensive examina-tion; and Medical decision making of high complexity). The same provider also re-ports 93010 Electrocardiogram, routine ECG with at least 12 leads, interpreta-tion and report only for ECG interpreta-tion and report.Note that not all payers will allow you
to capture the test interpretation twice (once as an element of the E/M, and again as a professional service). For example, Novitas Solutions clarifies that you should not assign credit in the data re-view section of medical decision-making (MDM) if the provider is separately billing the professional component of a test:
If the provider is billing separately for the interpretation of a test in the radiology and/or medicine section of the
CPT, then that same physician should not take credit for the independent visualization of that test in the Amount and/or Complexity of Data Reviewed Section of the Medical Decision Making key component of an E/M … If the provider is not billing separately for the inter-pretation of the test or the test was performed by anoth-er provider and that physician is independently visualiz-ing the test, then the provider may take credit for the in-dependent visualization of that test in the Amount and/or Complexity of Data Reviewed Section of the Medical Decision Making key component of an E/M.
Whether you may assign credit in the data review section of MDM when the provider separately bills for the professional component of a test is a matter of payer interpretation and policy, as further explained in this Frequently Asked Question from the American College of Emergency Physicians (ACEP) website:
Q: If I bill for an ECG or X-ray interpretation, can I also count this service (assign a point) in the Evaluation and Management Medical Decision-Making (MDM) value as listed on the MDM table in the CMS distributed Marshfield Clinic tool for review of images/tracings?
A: On a basic level, there is the potential for 3 “points” in the CMS-suggested Medical Decision Making (MDM) audit scoring in the area of Amount and/or Complexity of Data to Be Reviewed for radiology/cardiology/lab and other diagnostic services. One point is assigned for order-ing the study and using the results for patient evaluation/management. Two points are available for the direct vi-sualization of the tracing/film/specimen.
www.aapc.com November 2014 9
Please send your letters to the editor to: [email protected] Letters to the Editor
It is possible to give credit for the single point assigned for ordering of the study in addition to billing for the inter-pretation of the test. It is the latter 2 points that raise some question and are discussed in this scenario. This scoring system is derived from a CMS-suggested audit scoring sheet widely distribute nationwide.
The discussion revolves around the fine point of wheth-er the complexity of data to be reviewed is an assessment of service separate from the work of the interpretation of the test. If these are separate, then the 2 points can be giv-en in addition to billing for the interpretation of the test. CPT addresses this issue by noting that the interpretation of diagnostic tests is not included in the levels of E&M services. On the other hand, Medicare seems to differen-tiate between a “report” and a “review” in respect of bill-ing and getting credit under the complexity of data sec-tion of the MDM. In that there is no specific clarification on this issue and payment policies do differ, you are ad-vised to contact your local carrier for advice.
Bottom Line: Know your individual payers’ rules before taking credit for independent visualization of at test in the Amount and/or Complexity of Data Reviewed Section of MDM when the pro-vider is billing separately for the interpretation of that same test.Marcy Stavely, CPC, CPC-I
Different Take on “Patient Not Present” BillingI was having a discussion with one of my coworkers and fellow coders about the article “Billing Rules Change When the Patient Isn’t Present” (August 2014, pages 22-23), and I wanted to follow up with additional comments.I often have seen evaluation and management (E/M) codes re-ported for family meetings (as the article suggests). In a tightly run office, where mistakes are rare, I don’t have a problem with it. But I have encountered many situations where billing special-ists or charge posters, not paying close enough attention, bill ser-vices to insurance companies that should be patient-only. There would be no way for the third-party payer to know that the service was not provided for the patient, but on behalf of the patient with-out the patient present. This is why I try to “foolproof” the situa-tion, when possible. I would not use a CPT® code or an ICD-9-CM code for this type of service. I would create a code for my practice management soft-ware, such as “FAMILY,” that does not bill to third-party payers. Most electronic health records and practice management software have the ability to set a procedure code as “bill patient only.” If a
practice wanted to use an E/M code, I would still recommend us-ing a dummy ICD-9-CM code, and not the patient’s actual diag-nosis, as a “fail safe,” in case the charge found its way to an insur-ance company. If you do bill a “patient not present” visit for a Medicare benefi-ciary using a CPT® E/M code, I contend that use of an Advanced Beneficiary Notice (ABN) would be necessary because E/M codes are covered services when supported by a medically necessary di-agnosis. I have submitted a question to our MAC to see if I can get an official opinion.Karen D. Hill, CPC, CPB, CPMA, CMB
Avoid Menisectomy/ Repair ConfusionI read with interest “Understand Modifier 59 and NCCI Bun-dling” (September 2014, pages 20-22), but I must dispute the in-formation provided in Example 1, for several reasons:1. The example states that an orthopedic surgeon performs an
arthroscopic medial and lateral meniscal repair; however, the CPT® code referenced, 29880 Arthroscopy, knee, surgical; with meniscectomy (medial AND lateral, including any menis-cal shaving) including debridement/shaving of articular carti-lage (chondroplasty), same or separate compartment(s), when per-formed, describes arthroscopic medial and lateral menisecto-my. Meniscal repair is reported using 29883 Arthroscopy, knee, surgical; with meniscus repair (medial AND lateral).
2. National Correct Coding Initiative (NCCI) edits for this coding scenario (29880 and 29877) are irrelevant. Per a 2012 revision to the CPT® manual, 29877 Arthroscopy, knee, surgi-cal; debridement/shaving of articular cartilage (chondroplasty) is inherently bundled to 29880 and 29881 Arthroscopy, knee, surgical; with meniscectomy (medial OR lateral, including any meniscal shaving) including debridement/shaving of articu-lar cartilage (chondroplasty), same or separate compartment(s), when performed.
3. Prior to the code descriptor change/CPT® revision men-tioned above, and although NCCI did include an edit with an indicator of “0” for the code combination 29880 and 29877, NCCI chapter 4 guidelines direct coders to report chondroplasty using G0289 Arthroscopy, knee, surgical, for re-moval of loose body, foreign body, debridement/shaving of artic-ular cartilage (chrondroplasty) at the time of other surgical knee arthroscopy in a different compartment of the same knee, if per-formed in a separate compartment with another surgical ar-throscopic knee procedure.
Ruby Woodward, BSN, CPC, COSC, CSFAC
10 Healthcare Business Monthly
The success of local chapters is dependent on local chapter member participation and the willingness of members to lead their chapter. One essential of-
ficer position is secretary: the historian who keeps an accurate re-cord of your chapter’s events. The secretary promotes efficient and effective communications between chapter members, officers, and AAPC’s national office.As secretary for a local chapter, your responsibilities will include:• Preparing and publishing chapter meeting minutes - A
copy of the minutes must be uploaded to AAPC’s national office within 10 days of the meeting or event. Minutes should include speaker information, the topic, and length of education. Posting the minutes on the local chapter’s section of AAPC’s forum page keeps members apprised of all meeting discussions.
• Providing sign-in sheets for all chapter meetings - Within 10 days following a meeting or event, a copy of the sign-in sheet should be given to the chapter treasurer and education officer. The original sheet must be given to the chapter president. Meeting attendance forms can be found at www.aapc.com/documents/LC_meetingattendancesheet.pdf.
• Maintaining a list of all active chapter members - As secretary, you should encourage members to update contact information on the AAPC website to ensure the list is current. You also should verify that the email distribution list contains all new chapter members. The member list can be found at www.aapc.com/MemberArea/Chapters/chapterLeaders.aspx.
• Proctoring at least one certification exam during your one year tenure. The first step, of course, is to get your chapter to host an exam.
• Being an active participant - To guarantee a successful,
seamless, and functional chapter, the secretary must collaborate with other chapter officers to make sure the chapter moves forward in a positive and professional manner, in line with the mission and vision of our profession. Along with the other chapter officers, the secretary should help monitor and respond to local chapter forum posts.
If most of these responsibilities describe your passion and sound like something you would like to do, reach out to one of the current of-ficers and nominate yourself to serve as the next secretary for your chapter. Or nominate a friend who fits the bill.
Small Chapters May Need to Combine PositionsIf your chapter does not have enough volunteers, the roles of sec-retary and treasurer can be combined and staffed by one person. In this case, the secretary/treasurer is required to co-sign on local chapter checking accounts and to retain financial and non-finan-cial records in accordance with Chapter 5, Section 10 of the Local Chapter Handbook, available at https://aapcmarketing.s3.amazonaws.com/localchapters/2014LC_handbook.pdf.
Come Out SwingingDon’t be intimated. Let your chapter know you have the clerical and people skills to be a successful secretary. Everyone is rooting for you to succeed. Don’t hesitate to ask fellow officers for guidance and sup-port when needed. You will be glad you stepped up to the plate. Good leadership begins with you!
Faith C.M. McNicholas, RHIT, CPC, CPCD, PCS, CDC, has experience in various solo and group practice medical specialties. She is assistant editor for American Academy of Dermatol-ogy’s (AAD) Derm Coding Consult, and a contributor for Association of Dermatology Managers/Administrators (ADA/M) Newsletter and Journal of Dermatology Nurses Association (JDNA). McNicholas presents at AAD annual and summer meetings, AAPC regional conferences, ADA/M
and JDNA annual meetings, and AAD monthly webinars and regional symposia. She is an ICD-10-CM/PCS expert and approved trainer, and past president, president-elect, and secretary of Des Plaines, Illinois local chapter.
Becoming Chapter Secretary Is the “Write” Thing to DoDetail-oriented, accurate record keeper, and good communicator makes for a successful secretary.
The secretary promotes efficient and effective communications between chapter members, officers, and AAPC’s national office.
www.aapc.com November 2014 11
Local Chapter Handbook
Red Rover, Red Rover, Send Members Right Over!Fitting in local chapter meetings when you lead a busy life can be challenging. Work, family, friends, hobbies, chores — the list of other things to do is endless. You may be lucky enough to have an employer who lets you attend chapter meetings during work hours (thank you, kind employer!). Most of us don’t have that luxury, how-ever. If you’re in that category, and looking for ways to squeeze lo-cal chapter meetings into your busy schedule, consider the follow-ing tips and tricks: • Schedule it: Write meeting dates on your calendar or send
yourself an appointment reminder, so you can plan around it in advance. Often, chapters hold monthly meetings on the same day of the week, at the same time each month, making advance planning easier.
• Stick to it: Don’t let other things crop up and crowd out this important opportunity to network with your peers, gain free continuing education units, and learn more about your craft.
• Speak up: If you are having a hard time attending chapter meetings because the time or day conflicts with other
activities in your life, talk with your chapter officers. If enough people need the time changed, the officers may be able to accommodate the request. If you’re a chapter officer and have noticed low or dropping chapter attendance, ask your members via a survey or at a meeting what days and times work best for them.
• Switch: If the day and time of your chapter does not work for your schedule, and the chapter is unable to move the meeting time, look around to see if there is another chapter close by that you could join.
• Take a stand: If your employer does not allow you to attend a meeting on the clock, explain to him or her that meetings enable you to expand your knowledge, and improve your job performance.
Don’t miss another opportunity to attend a meeting and receive and/or share the information, resources, and connections necessary to ex-cel in this industry.
By Erin Andersen, CPC, CHC
12 Healthcare Business Monthly
AAPC Member FeatureBy Michelle A. Dick
Paying it Forward, One Stitch at a TimeWhen the Hardship Scholarship fund needed help, a quilt maker was there.
The AAPC Chapter Association’s Hardship Scholarship fund has been a charity that former Treasurer Judy Wilson, CPC, CPC-H, CPCO, CPPM, CPC-P, CPB, CPC-I, CANPC, CMRS, holds dear to her heart. Donated funds come from members to help other hardwork-ing, active members retain their cre-dentials during times of financial hardship. When Wilson found out that her positive actions affect-ed AAPC National Advisory Board (NAB) member, Jeanne Ger-shman’s, CPC, CPC-H, CEMC, decision to donate a quilt to the fund, it was heartfelt. Gershman’s decision to donate her quilt was made at the Nash-ville, Tennessee AAPC HEALTHCON. “At one of the last con-ferences, I heard someone mention that the contributions for the hardship fund were lower than usual,” Gershman said. “I ap-proached Judy and Brenda and asked if they thought we could do a quilt raffle that would raise funds.”
A Kind Act Comes Back TenfoldWilson recalls talking to former AAPC Chapter Association Chair Brenda Edwards, CPC, CPB, CPMA, CPC-I, CEMC, at HEALTHCON about how to get people to give to the Hardship Scholarship fund. “During that time,” Wilson said, “Jeanne Ger-shman told me that my encouraging her to apply for the AAPC Chapter Association and NAB is why she is a NAB officer now, and she would like to donate the quilt for us to raffle off to help the scholarship fund.” Gershman even paid to mail the quilt to Wil-son’s office in Virginia Beach.“I was so touched that she would make something so beautiful, that I know took a great deal of time, and then give it to help raise money for the Hardship Scholarship fund,” Wilson said. “Re-
member: You never know how your words will effect what some-one does. It is so true that the kindness you show to others will only come back greater.”Gershman remembered the effect Wilson had on her at a Chicago conference. “I was impressed with the enthusiasm that I saw in the board members,” Gershman said. “I approached Judy and asked her if she thought I would have a chance of becoming an officer on either the AAPC Chapter Association or NAB.”Wilson recalls the conversation. “We start talking and I knew she would be a great fit to represent the AAPC going forward,” she said. “I told her she should apply.” Her encouragement prompted Gershman to apply for both boards, and she was chosen for NAB.
The Gift that Keeps GivingWhen Healthcare Business Monthly contacted Gershman about featuring her quilt for this article, she humbly explained that she did it to fill a need. “I am a bit embarrassed,” she said. “This was just done because there was a need.” Gershman had been a local chapter officer for Providence, Rhode Island, for three years pri-or and was unable to run for office again. She said she really en-joys being involved in her local chapter and saw the quilt as a way to continue contributing. “This is my way of sharing my passion for quilting and using it to serve other people in need,” Gersh-man said.The quilt not only helped others, but it bolstered Gershman’s quilting skills. “On a personal note, it really improved my self-con-fidence and level of achievement,” she said.There may be more quilts donated in the future. “If the raffle pro-ceeds are enough to cover what I have personally put into the quilt, I am willing to do this yearly,” Gershman said. “I would donate my time, material, and enthusiasm for the cause.” She added that she hopes this encourages others to donate.
Michelle A. Dick is executive editor at AAPC.
Hardship Scholarship Fund Helps Members in Crisis
Chapters or members may donate to this great cause by mailing a check or money order,
payable to the “AAPCCA Hardship Scholarship Program,” to:
AAPCCA Hardship Scholarship Program 2480 South 3850 West, Suite B Salt Lake City, UT 84120
We Can Help You!
Admitting you need help is never easy. Asking for help is even harder. But you’ve worked hard to get where you are and have studied countless hours for your credentials. When it’s a harsh reality that you can’t make ends meet, we want to help you during this stress-ful time. The generosity of others enables us
to help those who cannot afford membership dues and other AAPC branded goods and services related to certification.
To see the rules for the Hardship Scholarship fund and get answers to frequently asked questions, go to www.aapc.com/MemberArea/Chapters/scholarship.aspx.
NewarkNEW JERSEYDec. 8–9
Las VegasNEVADADec. 11–12
BaltimoreMARYLANDDec. 11–12
San AntonioTEXASDec. 15–16
CPT® Changes 2015 and ICD-10-CM Workshops
When you think December, think learning with the American Medical Association.
Visit “Training & Events” at amastore.com to learn more and register. Or call (800) 882-3000 to learn about group pricing and student discounts.
*Promotion code can only be applied toward the full rate. Offer expires Nov. 22, 2014.
Healthcare Business Monthly readers save $75. Register with promo code FQW.
DAY 1: CPT® CHANGES 2015
Get the insider’s view to the process, rationale and application for more than 500 changes to the CPT® 2015 code set. If you can’t attend Symposium, then you want to attend this workshop.
Receive a free copy of CPT® 2015 Professional Edition and CPT® Changes 2015 at the event. Earn CEUs.
Full rate: $545
DAY 2: ICD-10-CM
Learn how to prepare, code and document properly for ICD-10-CM in a separate full-day workshop. Study now to make an effective transition on Oct. 1, 2015.
Receive a free copy of ICD-10-CM 2015 at the event. Earn CEUs.
Full rate: $545
TWO-DAY PACKAGE
Or make it a two-day learning experience and attend both sessions.
Following the rules will ensure proper coding and reimbursement.Cardiac catheterization is performed to diagnose coronary ar-tery disease, valvular heart disease, angina (chest pain), conges-tive heart failure, and certain congenital (present at birth) heart conditions. Ensure your providers are correctly reimbursed for these diagnostic techniques by understanding what these proce-dures involve and the requirements for coding them.
Understand the Procedure During cardiac catheterization, a small, flexible tube called a catheter is placed into a blood vessel in the patient’s arm, groin (upper thigh), or neck, and advanced through the aorta into the heart. The tip of the catheter can be placed in various parts of the heart, or advanced to the coronary arteries. This is followed by an injection of contrast dye through the catheter into the ar-teries. This test, coronary angiography, allows the physician to locate blockages in the coronary arteries.The dye can show whether a waxy substance called plaque has built up inside the coronary arteries. Fatty deposits may devel-op in childhood and continue to thicken and enlarge through-out life. Atherosclerosis (a buildup of plaque in the inner lining of an artery, causing it to narrow or become blocked) is the most common form of coronary artery disease.
Break Down the Catheterization CodesTo better understand catheter placement code assignment, we’ll review several key codes and guidelines.
93451 Right heart catheterization including measurement(s) of oxygen saturation and cardiac out-put, when performed
• The catheter is advanced through the inferior or superior vena cava into the right atrium, then into the right ventricle, pulmonary artery, and pulmonary capillary wedge positions for pressure measures.
• Swan-Ganz catheter, a flow-directed catheter, should not be reported with 93503 Insertion and placement of flow directed catheter (eg, Swan-Ganz) for monitoring purposes with any right heart catheterization procedure. Report 93503 when the Swan-Ganz is placed for monitoring purposes only.
• To report right atrial angiography or right ventricular angiography, assign add-on code 93566 Injection procedure during cardiac catheterization including imaging supervision, interpretation, and report; for selective right ventricular or right atrial angiography (List separately in addition to code for primary procedure) to 93451, 93453, 93456, 93457, 93460, 93461 and congenital heart disease (CHD) catheterizations.
• Other codes that include a right heart catheterization are 93453, 93456, 93457, 93460, and 93461. Do not report 93451 separately with any of these codes.
93452 Left heart catheterization including intraprocedural injection(s) for left ventriculography, im-aging supervision and interpretation, when performed
• Documentation should indicate crossing of the aortic valve, and that the pressures are from inside the left heart chamber.
• Code 93452 includes imaging supervision and interpretation for left ventricular or left atrial angiography.
• Other codes that include a left heart catheterization are 93453 and 93458-93461. Do not report 93452 separately with any of these codes.
93453 Combined right and left heart catheterization including intraprocedural injection(s) for left ventriculography, imaging supervision and interpretation, when performed
• Code 93453 includes all left heart catheterization components, including the function of the mitral valves, aortic valves, and aortic valve regurgitation.
• For right and left heart catheterization with coronary angiography, refer to 93460.
• For bypass graft angiography, use 93461 (description follows).
www.aapc.com November 2014 15
Cardiac Catheterization
CODING/BILLING
93454 Catheter placement in coronary artery(s) for coronary angiography, including intraprocedur-al injection(s) for coronary angiography, imaging supervision and interpretation
• The coronary arteries arise from the aorta just above the aortic valve, so the physician can place the catheter into the coronary arteries without entering the heart.
• When the physician uses injections for guidance only, do not separately code the injection.
Bypass graft catheterization codes include:
93455 Catheter placement in coronary artery(s) for coronary angiography, including intraprocedur-al injection(s) for coronary angiography, imaging supervision and interpretation; with cathe-ter placement(s) in bypass graft(s) (internal mammary, free arterial, venous grafts) including intraprocedural injection(s) for bypass graft angiography
93457 Catheter placement in coronary artery(s) for coronary angiography, including intraprocedur-al injection(s) for coronary angiography, imaging supervision and interpretation; with cathe-ter placement(s) in bypass graft(s) (internal mammary, free arterial, venous grafts) including intraprocedural injection(s) for bypass graft angiography and right heart catheterization
93459 Catheter placement in coronary artery(s) for coronary angiography, including intraprocedural injection(s) for coronary angiography, imaging supervision and interpretation; with left heart catheterization including intraprocedural injection(s) for left ventriculography, when per-formed, catheter placement(s) in bypass graft(s) (internal mammary, free arterial, venous grafts) with bypass graft angiography
93461 Catheter placement in coronary artery(s) for coronary angiography, including intraprocedur-al injection(s) for coronary angiography, imaging supervision and interpretation; with right and left heart catheterization including intraprocedural injection(s) for left ventriculography, when performed, catheter placement(s) in bypass graft(s) (internal mammary, free arterial, venous grafts) with bypass graft angiography
• Coronary artery bypass grafts include vein grafts, internal mammary artery grafts, and free arterial grafts.
• When the origin of any of these grafts is engaged, you should assign a code that includes bypass graft catheterization.
• Internal mammary artery (non-grafted) injection (to determine whether it’s suitable for use in future bypass surgery) is coded as a bypass graft catheterization, even though the artery has not yet been grafted.
Appropriately Apply Add-onsIntravascular ultrasound (IVUS) is an additional technique that may be employed during a cardiac catheterization. IVUS uses a computer and a transducer to transmit ultrasonic sound for direct visualization and measurements of the inside of blood vessels, and may assist the physician in selecting an appropri-ate treatment. Report IVUS with add-on codes 92978 Intra-vascular ultrasound (coronary vessel or graft) during diagnostic evaluation and/or therapeutic intervention including imaging su-pervision, interpretation and report; initial vessel (List separate-ly in addition to code for primary procedure) and 92979 Intravas-cular ultrasound (coronary vessel or graft) during diagnostic eval-uation and/or therapeutic intervention including imaging super-vision, interpretation and report; each additional vessel (List sep-arately in addition to code for primary procedure). Claim the cor-
Answer Five Questions Before Coding 1. Which set of CPT® codes apply? There are two sets of
cardiac catheterization codes: One for congenital heart disease, and one for all other conditions.
Caution: Do not use congenital codes (93530-93533) if the patient’s only congenital anomaly is coronary arteries, patient foramen ovale, mitral valve prolapse, or bicuspid aortic valve: These types of anomalies are very common.
2. Which side(s) of the heart was the catheterization per-formed on: right, left, right and left, or only the coronary arteries?
Tip: When a study is performed for a congenital anomaly, the right side of the heart will almost always be studied.
3. What technique was used? A retrograde (opposite the direction of blood flow) approach is performed most often for coronary arteries and left heart catheterizations. The antegrade (in the same direction of blood flow) approach is more common for right heart catheterization.
4. Were there any add-on procedures?
5. What was the place of service? For example, are you
coding for professional component billing (modifier 26 Profes-sional component) or the hospital Outpatient Prospective Payment System, which assigns codes to a payable ambulatory payment classification?
CODI
NG/B
ILLI
NG
Cardiac Catheterization
onary IVUS codes one time per vessel, even if multiple exams are performed in a vessel.Other potential add-on procedures with cardiac catheter place-ment include:• Suparavalvular aortography +93567 Injection procedure
during cardiac catheterization including imaging supervision, interpretation, and report; for supravalvular aortography (List separately in addition to code for primary procedure) describes positioning a catheter in the aortic root and injecting contrast. The resulting angiograms show the aortic valve, the aortic root, and the ascending aorta.
• Pulmonary angiography +93568 Injection procedure during cardiac catheterization including imaging supervision, interpretation, and report; for pulmonary angiography (List separately in addition to code for primary procedure) describes passing a catheter through the right atrium into the right ventricle, and then into the main pulmonary artery or one of its branches. Report this add-on code in addition to 93451, 93453, 93456, 93457, 93460, 93461, and CHD heart catheterization codes.
Watch Out for Bundled ServicesThe following services are included in cardiac catheterizations and are not coded separately:• Local anesthesia and moderate sedation • Insertion, positioning, repositioning, and removal of
catheters into the coronary arteries and/or left and/or right heart
• Mapping angiography performed to place the catheters• Recording of pressures in the heart chambers and blood
vessels
• Angiography for closure device placement• Evaluation and interpretive report
Do not assign a separate injection code for a type of injection that is already included in the catheterization code.
Coding Examples Show the WayConsider the following examples of proper coding for catheter placement.Example 1: A critically ill patient requires continuous cardi-ac monitoring. In the intensive care unit, a Swan-Ganz catheter is inserted into the jugular vein and advanced through the right atrium, right ventricle, and pulmonary artery to a wedged posi-tion. Blood samples are taken, pressures and recordings are ob-tained, and the catheter is left in place for continuous monitor-ing for two days.Because the catheter is placed for monitoring only, correct cod-ing is 93503. Example 2: A 6-French sheath and catheter is inserted into the right femoral artery and a catheter is advanced to the left ventri-cle. Ventriculography is performed using power injection of con-trast agent. Pressures in the left heart are obtained. Additionally, the coronary arteries are selected and imaged.In this case, correct coding is 93458 Catheter placement in coro-nary artery(s) for coronary angiography, including intraprocedural injection(s) for coronary angiography, imaging supervision and inter-pretation; with left heart catheterization including intraprocedur-al injection(s) for left ventriculography, when performed for left ven-triculography.Example 3: A 7-French sheath and catheter is inserted into the right common femoral artery. The catheter is advanced through the inferior or superior vena cava into the right atrium, into the
right ventricle, and then into the pul-monary artery.Because this is a right heart catheteriza-tion, the appropriate code is 93451.
Educate Physicians About Documentation RequirementsAll coding must be supported by the documentation in the medical record. To improve your chances of selecting the appropriate cardiac catheter code, and of gaining the best possible appro-priate reimbursement, educate your providers to document all pertinent in-formation, including:
• History (e.g., acute myocardial infarction), medical necessity, and reason for repeat diagnostic studies after prior angiography/computed tomography/magnetic resonance angiography (angio/CT/MRA)
• Vascular access sites: à Arm (becoming more popular, less recovery time) à Groin (upper thigh: most common, requires 2-6 hours
of bed rest) à Neck
• Vessels catheterized, describing the catheter tip location, and any variant anatomy
• Heart pressures and chambers entered, injected, and imaged
• Vessels injected, the areas imaged (for medical necessity), with interpretation of findings (e.g., Is it a chronic total occlusion (CTO)?), along with specific documentation of degree stenosis and exact locations of the treated lesions
• Interventions performed, and any complications or additional treatments provided
• Specific devices and specialty supplies used during the procedure
Source: Adapted from ZHealth Publishing with permission.
Lynn Stuckert, LPN, CPC, CPMA, has 30 years of experience in large multi-specialty clinics and hospital systems as a nurse, chart auditor, educator, compliance manager, and medical writer. She has held offices for AAPC’s City of Palms Chapter, Fort Meyers, Florida, and the Health Management Association of Southwest Florida.
To discuss this article or topic, go to www.aapc.com
Do not assign a separate injection code for a type of injection
that is already included in the catheterization code.
■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
■ CODING/BILLING
Capture All of What Oncology Costs Your Practice
By Janice G. Jacobs, CPA, CPC, CPCO, CCS, ROCC
Billing relies on documentation to reflect time, resources, and complexity of services accurately.
www.aapc.com November 2014 19
Oncology
CODING/BILLING
Oncology practices are continually challenged to gain appropriate reimbursement for services performed, resources used, and drugs dispensed. Let’s address potential billing, coding, and documen-tation problems where lack of understanding can adversely affect practice revenue.
Recognize Unique CircumstancesA medical oncologist typically will see a cancer patient multiple times throughout the treatment process (beginning with the ini-tial consultation, cancer staging, and care plan coordination), and often for years afterward. An oncologist also might help the pa-tient make the decision to move from treatment to palliative care, coordinating a care plan developed to assure comfort and quali-ty of life. Due to the complexity of cancer-related cases and the risk involved in treatment, the oncologist’s medical decision-making is typical-ly very high, and the time involved in managing patients is sig-nificant. Oncologists often express frustration when faced with coding guidelines that do not seem to reflect the level of services they provide, and may find it difficult to accept that certain fol-low-up visits with critically (or terminally) ill patients qualify only for a low-level evaluation and management (E/M) service. How-ever, when a patient is in the middle of chemotherapy, and no ad-verse reactions are reported or no new complaints are noted, the visit would not merit a high level just because there is a cancer di-agnosis. There are, however, situations exclusive to oncology where addi-tional services may be captured and billed, such as adverse reac-tions to treatment. Appropriate charge capture of these services will ensure that physicians are appropriately compensated for their services during chemotherapy administration.Physicians should bill codes that accurately reflect the time, re-sources, and complexity of services they and their staff provide for managing significant adverse drug reactions. Examples of ad-ditional billing opportunities for chemotherapy patient manage-ment for patients having adverse reactions are:• When a patient experiences an adverse reaction to drugs
during a chemotherapy session that requires physician intervention, you may report an E/M service in addition to the chemotherapy administration services.
• When a patient experiences an adverse reaction to drugs during a chemotherapy session, but had already seen the physician prior to treatment for an unrelated problem, the physician may bill for the significant drug reaction visit. The total time, resources, and complexity of the physician’s interaction with the patient may justify a higher E/M level
than the original, separately identifiable E/M service. • When a patient experiences an adverse reaction to drugs
during a chemotherapy session, the physician may be able to bill for prolonged services, depending upon how much time is spent face-to-face with the patient. The encounter must be documented and time clearly noted. Additionally, the physician must spend at least 30 minutes with the patient to justify billing for prolonged services.
• When a patient experiences a life-threatening, adverse reaction to drugs during a chemotherapy session, the physician may be able to bill for critical care services in addition to other services, if the physician’s work involves at least 30 minutes of face-to-face management of the patient’s life-threatening condition.
ExampleA patient presents for chemotherapy. Prior to treatment, she sees the oncologist for an assessment of a rash that erupted over her chest following a previous session. The oncologist assesses the rash and prescribes a topical cream. An established patient level 2 E/M (99212 Office or other outpatient visit for the evaluation and man-agement of an established patient, which requires at least 2 of these 3 key components: A problem focused history; A problem focused ex-amination; Straightforward medical decision making.) is charged. During the subsequent chemotherapy administration, the patient experiences heart palpitations and shortness of breath. The oncol-ogist is called to perform a comprehensive exam of the respiratory and cardiovascular systems, and orders a portable EKG and chest X-ray. Due to the additional provided services beyond the assess-ment and treatment of the rash, you may now report a level 4 E/M (provided that the additional services are clearly documented).
Capture All Services RenderedIt’s important to accurately and completely document and code chemotherapy administration services, so you also can properly bill for the resources and supplies consumed. Inadequate docu-mentation of these services will inevitably lead to a decrease in rev-enue, due to claim rejections or denials and missed opportunity.To ensure your practice is compensated for the services rendered, be sure to address the documentation issues that can result in im-proper charge capture and billing, such as proper documentation of infusion start and stop times. Without start and stop times, it’s not possible to establish that a drug infusion lasted more than 15 minutes. Infusion services lasting 15 or fewer minutes are reported with intravenous (IV) push codes (96409 Chemotherapy adminis-tration; intravenous, push technique, single or initial substance/drug or 96374 Therapeutic, prophylactic, or diagnostic injection (speci-
20 Healthcare Business Monthly
fy substance or drug); intravenous push, single or initial substance/drug). Infusion services lasting longer than 15 minutes are report-ed with time-based infusion codes.Start and stop times are required to determine the appropriate concurrent or sequential code assignment, as well as additional billable infusion time beyond the first hour of the infusion. Absent start and stop time documentation will result in the lowest level of chemotherapy administration service being billed.
ExampleAn oncology patient presents for chemotherapy infusion. Docu-mentation indicates that three drugs are administered: vincristine, a chemotherapeutic drug, with a start time of 11:00 a.m.; ondan-setron, an anti-emetic, with a start time of 11:15 a.m.; and meth-otrexate, a chemotherapeutic drug, with a start time of 11:35 a.m. Without clear documentation of the stop times, it’s impossible to determine the appropriate CPT® code assignments. From an au-diting perspective, it’s assumed that all three drugs were admin-istered in less than 15 minutes, and IV push codes would be as-signed.• 96409 - for the initial IV push • +96375 - Therapeutic, prophylactic, or diagnostic injection
(specify substance or drug); each additional sequential intravenous push of a new substance/drug (List separately in addition to code for primary procedure) for additional sequential IV push of a new substance
• +96411 - Chemotherapy administration; intravenous, push technique, each additional substance/drug (List separately in addition to code for primary procedure) for additional chemotherapeutic substance/drug, IV push technique.
The same example, with stop times, is:• Vincristine start 11:00 a.m., stop 11:10 a.m. - 96409 • Ondansetron start 11:15 a.m., stop 11:35 a.m. - +96367
Intravenous infusion, for therapy, prophylaxis, or diagnosis (specify substance or drug); additional sequential infusion of a new drug/substance, up to 1 hour (List separately in addition to code for primary procedure)
• Methotrexate start 11:35 a.m., stop 12:30 p.m. - +96417 Chemotherapy administration, intravenous infusion technique; each additional sequential infusion (different substance/drug), up to 1 hour (List separately in addition to code for primary procedure)
Billing Anemia as a Side EffectAnemia, a common side effect of chemotherapy, must be treated during the course of therapy. The provider should document the specific type of anemia to meet medical necessity requirements when billing for anemia drugs during the course of treatment. In addition to the infusion and injection codes, the claim form must include the proper HCPCS Level II code for the anemia drug ad-ministered and a minimum of two ICD-9-CM codes: one for the anemia, and one or more for the underlying condition that caused the anemia.The exception to this rule is antineoplastic chemotherapy induced anemia, which has its own code, 285.3 Antineoplastic chemother-apy induced anemia. Always check your local coverage determi-nations (LCDs), and national coverage determinations (NCDs) for updated medical necessity guidelines related to anemia due to chemotherapy.
Examples• A patient undergoing chemotherapy is diagnosed with
“anemia induced by chemotherapy.” ICD-9-CM coding is 285.3. This code does not require an E code because the source of the anemia is named as the cause in the description of the code. This is usually a short-term anemia, and isn’t considered aplastic.
• A patient undergoing chemotherapy is diagnosed with “aplastic anemia due to chemotherapy.” ICD-9-CM coding is 284.89 Other specified aplastic anemias. An E code from the Table of Drugs and Chemicals is required to specify the drug that is the source of the anemia.
• A cancer patient is diagnosed with “anemia due to a neoplastic disease.” ICD-9-CM coding is 285.22 Anemia in neoplastic disease. In this case, the source of the anemia is the disease, not the treatment of the neoplasm.
To discuss this article or topic, go to www.aapc.com
Charge Capture of Correct UnitsIf chemotherapy drugs are hard-coded into a charge description master (CDM) or fee schedule, cross check the administered che-motherapy drug units against how that drug is set up in the office billing system. The maximum allowable fee per unit is based on the HCPCS Level II description of the chemotherapy drug. Er-rors are often made and drugs are frequently under-billed because they are hard coded with a unit of one. Example: For single-dose vials, bill the total amount of the drug contained in the vial(s), including partial vials. Based on the unit definition for the HCPCS Level II code, reimbursement is made based upon the total number of units contained in the vial.Multiple units also may be billed over the course of a treatment, or over the course of a single day. It’s important not only to cap-ture multiple units per day, but also multiple units per treatment. Example: A patient may receive up to 275 mg of epirubicin HCI per day, but the HCPCS Level II code (J9178 Injection, epirubicin
HCI, 2 mg) used to report the drug only covers 2 mg. This is why it’s very important that the proper number of units be document-ed, captured, and billed. CDMs and fee schedules should be reviewed annually to ensure that the line items and units accurately reflect the HCPCS Lev-el II descriptions. Training and education for clinicians and tech-nicians is imperative to ensure proper charge capture. Implement ongoing auditing and monitoring to identify and remediate sys-temic issues before they result in long-term revenue losses.
Janice G. Jacobs, CPA, CPC, CPCO, CCS, ROCC, is a director at IMA Consulting. She has over 25 years of healthcare industry experience including hospital accounting and audit-ing, inpatient, outpatient and professional fee coding, and compliance and revenue cycle management. Prior to IMA, Jacobs was a director in Huron’s Healthcare Compliance and Investigations Practice, where she worked on academic medical centers. Jacobs is a fre-
quent speaker at industry trade shows. She is a member of the Scranton, Pennsylvania local chapter.
Oncology
CODING/BILLING
Oncologists often express frustration when faced with coding
guidelines that do not seem to reflect the level of services provided.
Not an EM calculator, this tool includes audit elements for documentation not just the coding elements
Easy access hot keys allow for efficient and fast auditing
Fully integrated work queue allows for multiple audits to be worked on simultaneously with the ability to manage them
Sophisticated reporting capabilities with summary reports and scoring
22 Healthcare Business Monthly
■ DEAR JOHN
Have a Coding Quandary? Ask JohnDoes Manipulation Under Anesthesia Require Fixation?
QMay we report CPT® 23700 Manipulation under anes-thesia, shoulder joint, in-cluding application of fixa-tion apparatus (dislocation excluded) if no fixation de-vice is used? Does anesthesia, in this instance, mean gener-al anesthesia?
AThe short answers to your questions are “Yes” and “Yes.” The American Medical Association’s
(AMA) CPT® Assistant has addressed both questions on separate occasions.
May 2009; Volume 19: Issue 5Question: Is it appropriate to report CPT code 23700 for ma-nipulation of the shoulder joint under anesthesia if a fixation apparatus is not utilized?Answer: Yes. Utilization of a fixation apparatus is not re-quired in order to report CPT code 23700.
April 2005; Volume 15: Issue 4Question: Is it appropriate to report CPT code 23700, Manipulation under anesthe-sia, shoulder joint, including application of
fixation apparatus (dislocation excluded), when general anesthesia is not used?Answer: CPT® code 23700 is intended to be reported for the manipulation only when performed under general anesthesia. The code descriptors, which include the phrase “requiring anesthesia” or “under anesthe-sia,” indicate that the work involved in that specific procedure requires the use of gener-al anesthesia; therefore, it would not be ap-propriate to report code 23700 if general an-esthesia is not provided.
If you have a coding-related question for AAPC’s Healthcare Business Monthly, please contact John Verhovshek, managing editor, at [email protected].
To discuss this article or topic, go to www.aapc.com
Available Benefits Include:
Are you taking advantage of your
MEMBERB E N E F I TS?
Healthcare Business Resources Comprehensive EducationDiscounted Products & ServicesUnparalleled Networking Opportunities
International RecognitionSavings on Hundreds of National BrandsInvaluable Access to Jobs
Voraxaze® New Technology Add-on Payment (NTAP) ExtendedReceive up to an additional 50% payment on your MS-DRG submission.*
For the treatment of toxic plasma methotrexate concentrations (>1 micromole per liter) in patients with delayed methotrexate clearance due to impaired renal function
DISCLAIMER* Procedure coding should be based upon medical necessity and procedures and supplies provided to the patient. Coding and reimbursement information is provided for educational purposes and does
not assure coverage of the specifi c item or service in a given case. This information makes no guarantee of coverage or reimbursement of fees. Contact a local Medicare Fiscal Intermediary, Carrier, or CMS for specifi c information regarding coverage, coding, and payment. To the extent that cost information is submitted to Medicare, Medicaid, or any other reimbursement program to support claims for services or items, there is an obligation to accurately report the actual price paid for such items, including any subsequent adjustments.
ICD-9-CM=International Classifi cation of Diseases, Ninth Revision, Clinical Modifi cation. NTAP=New Technology Add-on Payment policy provides additional payments for cases with high costs involving eligible new technologies while preserving some of the incentives under the average-
based payment system. The payment mechanism is based on the cost to hospitals for the new technology and is determined on a case-by-case basis. Under 42 CFR §412.88 Medicare pays the lesser of 50 percent of the cost in excess of the full DRG payment or 50 percent of the cost of the technology. If the actual costs of a NTAP case exceed the DRG payment by more than the estimated costs of the new technology, Medicare payment is limited to the DRG payment plus 50 percent of the estimated costs of the new technology.2
Selected Safety Information �Serious allergic reactions, including anaphylactic reactions, may occur
� The most common adverse reactions (incidence ≥1%) with Voraxaze® are paresthesias, fl ushing, nausea and/or vomiting,hypotension, and headache
Indication and Limitations of Use �Voraxaze® is indicated for the treatment of toxic plasma methotrexate concentrations (>1 micromole per liter) in patientswith delayed methotrexate clearance due to impaired renal function1
�Voraxaze® is not indicated for use in patients who exhibit the expected clearance of methotrexate (plasma methotrexate concentrations within 2 standard deviations of the mean methotrexate excretion curve specifi c for the dose of methotrexate administered) or those with normal or mildly impaired renal function because of the potential risk of subtherapeutic exposureto methotrexate1
References: 1. Voraxaze® [prescribing information]. Brentwood, TN: BTG International Inc. March 2013. 2. New Medical Services and New Technologies. February 2014. http://cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/newtech.html.
Please see brief summary of prescribing information on adjacent page.Please see full prescribing information, including important safety information, at www.voraxaze.com.
VORAXAZE® (glucarpidase) For Injection, for intravenous use Initial U.S. Approval: 2012
Brief Summary of Prescribing Information. For complete Prescribing Information, consult official package insert.
INDICATIONS AND USAGE
Indication VORAXAZE (glucarpidase) is indicated for the treatment of toxic plasma methotrexate concentrations (>1 micromole per liter) in patients with delayed methotrexate clearance due to impaired renal function.
Limitation of Use VORAXAZE is not indicated for use in patients who exhibit the expected clearance of methotrexate (plasma methotrexate concentrations within 2 standard deviations of the mean methotrexate excretion curve specific for the dose of methotrexate adminis-tered) or those with normal or mildly impaired renal function because of the potential risk of subtherapeutic exposure to methotrexate.
CONTRAINDICATIONS None
WARNINGS AND PRECAUTIONS
Serious Allergic Reactions Serious allergic reactions occurred in less than 1% of patients [see Adverse Reactions].
Monitoring Methotrexate Concentration/Interference with Assay Methotrexate concentrations within 48 hours following administration of VORAXAZE can only be reliably measured by a chromatographic method. DAMPA (4- deoxy-4-amino-N10-methylpteroic acid) is an inactive metabolite of methotrexate resulting from treatment with VORAXAZE. DAMPA interferes with the measurement of methotrexate concentration using immunoassays resulting in an erroneous measurement which overestimates the methotrexate concentration. Due to the long half-life of DAMPA (t1/2 of approximately 9 hours), measurement of methotrexate using immunoassays is unreliable for samples collected within 48 hours following VORAXAZE administration.
Continuation and Timing of Leucovorin Rescue Continue to administer leucovorin after VORAXAZE. Do not administer leucovorin within 2 hours before or after a dose of VORAXAZE because leucovorin is a substrate for VORAXAZE [see Drug Interactions]. For the first 48 hours after VORAXAZE, administer the same leucovorin dose as given prior to VORAXAZE [see Warnings and Precautions]. Beyond 48 hours after VORAXAZE, administer leucovorin based on the measured methotrexate concentration. Do not discontinue therapy with leucovorin based on the determination of a single methotrexate concentration below the leucovorin treatment threshold. Therapy with leucovorin should be continued until the methotrexate concentration has been maintained below the leucovorin treatment threshold for a minimum of 3 days. Continue hydration and alkalinization of the urine as indicated.
ADVERSE REACTIONS Serious allergic reactions, including anaphylactic reactions, may occur. The most common adverse reactions (incidence >1%) with VORAXAZE are paraesthesias, flushing, nausea and/or vomiting, hypotension, and headache.
Clinical Trials Experience Because clinical trials are conducted under controlled but widely varying conditions, ad-verse reaction rates observed in clinical trials of VORAXAZE cannot be directly compared to
rates in the clinical trials of other drugs and may not reflect the rates observed in practice.The evaluation of adverse reactions in patients treated with VORAXAZE is confounded by the population in which it was studied, patients with toxic plasma methotrexate levels due to impaired renal function. Adverse reactions related to toxic methotrexate levels due to prolonged methotrexate clearance include myelosuppression, mucositis, acute hepatitis, and renal dysfunction and failure. The safety of VORAXAZE is based on data from 290 patients who were treated in 2 single-arm, open-label, multicenter trials enrolling patients who had markedly delayed methotrexate clearance secondary to renal dysfunction. Patients with osteosarcoma were eligible for these studies if the plasma methotrexate concentration was greater than 50 μmol/L at 24 hours, greater than 5 μmol/L at 48 hours, or greater than 2 standard deviations above the mean methotrexate elimination curve at least 12 hours after methotrexate administra-tion and there was a 2-fold or greater increase in serum creatinine above baseline. All other patients were eligible for these studies if the plasma methotrexate level was greater than 10 μmol/L more than 42 hours after the start of the methotrexate or the plasma level was greater than 2 standard deviations above the mean methotrexate excretion curve at least 12 hours following methotrexate and the serum creatinine was greater than 1.5 times the up-per limit of normal or the creatinine clearance was less than 60 mL/min at least 12 hours following methotrexate administration. Study 1, conducted by the National Cancer Institute (NCI), enrolled 184 patients; safety information is available for 149 patients. VORAXAZE was given at a dose of 50 Units/kg as an intravenous injection over 5 minutes. Patients with pre-VORAXAZE methotrexate concentrations >100 μmol/L were to receive a second dose of VORAXAZE 48 hours after the first dose. The protocol specified that patients continue receiving intravenous hydration, urinary alkalinization and leucovorin, and that leucovorin administration be adjusted to ensure that it was not administered within two hours before or after VORAXAZE. In Study 1, VORAXAZE-related adverse reactions were collected on a flow sheet with a daily log of adverse reactions characterized as “glucarpidase toxicity.” Additional safety information was collected from clinical re-cords submitted by treating physicians. This information was abstracted and categorized using the National Cancer Institute (NCI) “Common Terminology Criteria for Adverse Events” (CTCAE) version 3 scale. The Study 1 population enrolled patients with a median age of 18 years (1 month to 85 years); 63% were male, and the underlying malignancies were osteosarcoma/sarcomas in 32%, and leukemia or lymphoma in 63% of patients. One (n=106) or 2 (n=30) doses of VORAXAZE were administered intravenously; the number of doses was not specified in 13 patients. Doses ranged from 18 to 98 Units/kg, with a median dose of 49 Units/kg. Study 2 is an ongoing expanded access program. At the time of data cut-off, 243 patients were enrolled and safety data was available for 141 patients. VORAXAZE was given at a dose of 50 Units/kg as an intrave-nous injection over 5 minutes. The criterion for allowing patients to receive a second glucar- pidase dose was not specified in the protocol. The protocol specified that patients continue receiving intravenous hydration, urinary alka-linization and leucovorin, and that leucovorin administration be adjusted to ensure that it was not administered within two hours before or after VORAXAZE. Study 2 enrolled patients with a median age of 17 years (6 months to 85 years); 64% were male, and the underlying malignancies were osteogenic sarcoma in 32%, and leukemia or lymphoma in 62% of patients. One (n=122) or 2 (n=18) doses of VORAXAZE were administered intravenously; the number of doses was not
specified for 1 patient. Doses ranged from 6 to 189 Units/kg, with a median dose of 50 Units/kg. In Study 2 only VORAXAZE-related adverse reactions were collected and severity was graded according to NCI CTCAE version 3. Among the 290 patients included in the safety evaluation of VORAXAZE, there were 8 deaths within 30 days of VORAXAZE exposure that were not related to progressive disease. Twenty-one of 290 patients (7%) experienced adverse reactions that were assessed as related to VORAXAZE. Most were Grade 1 or 2 events. One patient experienced related Grade 3 flushing. The most common related adverse reactions that were not hematologic, hepatic or renal events were paresthesia, flushing, and nausea and/or vomiting, which each occurred in 2% of patients (Table 1).
Table 1: Per Patient Incidence of Grade 1 and 2 Adverse Reactions Assessed as Possibly, Probably, or Definitely Related to VORAXAZE Excluding Hematologic, Hepatic, or Renal Adverse Reactions
1This incidence includes the following terms: flushing, feeling hot, burning sensation. 2One of these reactions was classified as Grade 3 in severity.
Immunogenicity As with all therapeutic proteins, there is potential for immunogenicity. In clinical trials, 121 patients who received one (n=99), two (n=21), or three (n=1) doses of VORAXAZE were evaluated for anti-glucarpidase antibodies. Twenty-five of these 121 patients (21%) had detectable anti-glucarpidase anti-bodies following VORAXAZE administration, of which 19 received a single dose of VORAXAZE and 6 received two doses of VORAXAZE. Antibody titers were determined using a bridging enzyme-linked immunosorbent assay (ELISA) for anti-glucarpidase antibodies. Neutralizing antibodies were detected in 11 of the 25 patients who tested positive for anti-glucarpidase binding antibodies. Eight of these 11 patients had received a single dose of VORAXAZE. However, the development of neutralizing antibodies may be underreported due to lack of assay sensitivity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of incidence of antibodies to VORAXAZE with the incidence of antibodies to other products may be misleading.
DRUG INTERACTIONS
Use of VORAXAZE with Leucovorin Leucovorin is a substrate for VORAXAZE. Do not administer leucovorin within 2 hours before or after a dose of VORAXAZE. No dose adjustment is recommended for the continu-ing leucovorin regimen because the leucovorin dose is based on the patient’s pre-VORAXAZE methotrexate concentration [see Warnings and Precautions].
Other Substrate Interference Other potential exogenous substrates of VORAXAZE may include reduced folates and folate antimetabolites.
USE IN SPECIFIC POPULATIONS
Pregnancy Pregnancy category C. There are no adequate and well controlled studies with VORAXAZE in pregnant women and animal reproduction studies have not been conducted with VORAXAZE. Therefore, it is not known whether VORAXAZE can cause fetal harm when administered to a pregnant woman. VORAXAZE should be given to a pregnant woman only if clearly needed.
Nursing Mothers It is not known if VORAXAZE is excreted in hu-man milk. Because many drugs are excreted in human milk, caution should be exercised when VORAXAZE is administered to a nursing woman.
Pediatric Use The effectiveness of VORAXAZE in pediatric patients was established in Study 1. Of the 22 patients in the efficacy dataset in Study 1, 12 were pediatric patients with ages ranging from 5 to 16 years. Three of the six pediatric patients with a pre-VORAXAZE methotrexate concentration of 1-50 μmol/L achieved a rapid and sustained clinically important reduction (RSCIR) in plasma methotrexate concentration, while none of the six pediatric patients with a pre-VORAXAZE methotrexate concentration >50 μmol/L achieved a RSCIR.The pooled clinical safety database for VORAXAZE included data for 147 patients from 1 month up to 17 years of age. No overall differences in safety were observed between these patients and adult patients.
Geriatric Use Of the total number of 290 patients in clinical studies of VORAXAZE, 15% were 65 and over, while 4% were 75 and over. No overall differences in safety or effectiveness were observed between these patients and younger patients.
Renal Impairment No dose adjustment of VORAXAZE is recommended for patients with renal impairment.
Hepatic Impairment No specific studies of VORAXAZE in patients with hepatic impairment have been conducted.
OVERDOSAGE There are no known cases of overdose with VORAXAZE.
Adverse Reaction N= 290 n (%)
Paresthesias 7 (2%)
Flushing1,2 5 (2%)
Nausea/Vomiting 5 (2%)
Headache 2 (1%)
Hypotension 2 (1%)
Blurred Vision 1 (<1%)
Diarrhea 1 (<1%)
Hypersensitivity 1 (<1%)
Hypertension 1 (<1%)
Rash 1 (<1%)
Throat irritation/ Throat tightness 1 (<1%)
Tremor 1 (<1%)
Manufactured by: BTG International Inc. Brentwood, TN 37027 U.S. License No. 1861
Distributed by: BTG International Inc. West Conshohocken, PA 19428
VORAXAZE® is a registered trademark of Protherics Medicines Development Ltd. BTG and the BTG roundel logo are registered trademarks of BTG International Ltd.
www.aapc.com November 2014 25■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
CODING/BILLING ■
Proper documentation and coding of critical care services depend not only on the Centers for Medicare & Medicaid Services (CMS)
and CPT® guidelines, but also the payer (individual payers may have unique critical care requirements). To help ensure you are reporting these services correctly, you must have a solid understanding of pe-diatric critical care codes, including when to use them and when it’s more appropriate to use the standard, time-based critical care codes 99291-99292.Note: CMS rules may apply for a child on Medicaid. Best practice is to check with the Medicaid carrier to see if it follows CMS/CPT® rules.
Location Matters Less than You ThinkCritical care services usually are provided in a critical care area, such as a coronary care unit (CCU), intensive care unit (ICU), or the emergency department (ED); however, critical care services may be
provided in any location, as long as the care meets the definition of critical care. Likewise, just because a patient is in the ICU, CCU, neonatal intensive-care unit (NICU), etc., does not mean you can report critical care. Merely “rounding” to check vitals and to docu-ment that an otherwise stable patient is on a ventilator does not meet critical care requirements.
Indicators of Critical CareSeveral key performance indicators (KPI) are required to report crit-ical care. Both the illness or injury and the treatment provided must meet critical care requirements. Clinical reassessments and docu-mentation must support the aggregated critical care time for patients over 5 years old, including:• A complete itemization of the physician’s ongoing interval
assessments of the patient’s condition
Your Guide to Pediatric Critical Care
By Holly Cassano, CPC
When choosing codes, factor in age, time, CMS, CPT®, and bundling rules.
COVER
26 Healthcare Business Monthly
CODI
NG/B
ILLI
NG
Pediatric Critical Care
• Any impairments of organ systems based on all relevant data available to the physician (e.g., metabolic changes and diagnostic results)
• The rationale and timing of interventions• Patient response to treatment
Pediatric Critical Care DefinedPediatric critical care codes are reported per day. If a provider from the same group or specialty rounds on the patient later in the day, he or she cannot bill another critical care code for a patient young-er than 5 years of age. The applicable code sets include:
Neonatal critical care 28 days or younger99468 Initial inpatient neonatal critical care, per day, for the evaluation and management of a critically
ill neonate, 28 days of age or younger
99469 Subsequent inpatient neonatal critical care, per day, for the evaluation and management of a crit-ically ill neonate, 28 days of age or younger
ExampleA term infant is born after a normal pregnancy, labor, and deliv-ery. The infant has significant respiratory distress and requires NICU admission with intubation and mechanical ventilation. The neonatologist places an umbilical arterial line. Chest X-ray reveals a pneumothorax. The neonatologist additionally places a chest tube. Correct coding is 99468-25 Significant, separately identifiable evaluation and management service by the same physician or other qualified health care professional on the same day of the procedure or other service and 32551 Tube thoracostomy, includes connection to drainage system (eg, water seal), when performed, open (separate pro-cedure). Endotracheal intubation (31500 Intubation, endotracheal, emergency procedure) and umbilical artery catheterization (36660 Catheterization, umbilical artery, newborn, for diagnosis or therapy) are bundled with 99468, which represents initial inpatient neona-tal critical care for a patient 28 days or younger. Modifier 25 is ap-
pended to the critical care code to alert the payer of a significant separately identifiable evaluation and management (E/M) service by the same physician on the same day as another service.
Pediatric critical care 29 days–24 months99471 Initial inpatient pediatric critical care, per day, for the evaluation and management of a critically
ill infant or young child, 29 days through 24 months of age
99472 Subsequent inpatient pediatric critical care, per day, for the evaluation and management of a crit-ically ill infant or young child, 29 days through 24 months of age
ExampleA former 25-week gestation infant, now 45 days old, remains ventilator dependent. Today, he has increased ventilatory re-quirements and his perfusion is poor. The provider suspects ac-quired sepsis. The provider performs a bladder aspiration and lumbar puncture, obtains a blood culture, and begins a course of antibiotics.
Critical Care TipIf the patient is stable, take critical care off the table.If the provider documents “patient is stable,” critical care was not performed. Only if lifesaving interventions (and other CPT® and CMS requirements) are performed and documented may you report critical care. If the provider is “rounding and checking vitals,” the services do not meet the criteria for critical care. Instead, report the appropriate inpatient code for provided services.
www.aapc.com November 2014 27
CODING/BILLING
Pediatric Critical Care
Correct coding is 99472, which describes subsequent inpatient global critical care code for a patient who is older than 29 days but younger than 24 months. The bladder aspiration and lumbar puncture are bundled into the critical care.
Pediatric critical care 2-5 years99475 Initial inpatient pediatric critical care, per day, for the evaluation and management of a critically
ill infant or young child, 2 through 5 years of age
99476 Subsequent inpatient pediatric critical care, per day, for the evaluation and management of a crit-ically ill infant or young child, 2 through 5 years of age
ExampleA 5-year-old girl is in a motor vehicle accident, causing blunt trau-ma to her left side, resulting in splenic laceration, rib fractures, flail chest on the left, and acute respiratory failure. The pediat-ric critical care physician should report 99475 for initial inpatient critical care.On day two of her hospital stay, the child develops infiltrates in the left chest and left pleural effusion on chest radiograph. She goes into respiratory arrest and is ventilated. The pediatric critical care physician reports 99476 for subsequent inpatient critical care; all other services are bundled into the critical care.When reporting critical care services for patients over 5 years of age, use time-based critical care codes:
Critical care for patients over 5 years99291 Critical care, evaluation and management of the critically ill or critically injured patient; first 30-
74 minutes
+99292 each additional 30 minutes (List separately in addition to code for primary service)
Proper documentation of time is essential to correctly reporting 99291 and 99292. Use 99291 to report the first 30-74 minutes of critical care and +99292 to report additional 30-minute blocks of time beyond the first 74 minutes of critical care, as shown in Table A.
Table A
Total Duration of Critical Care Appropriate CPT® Codes
Less than 30 minutes 99232, 99233, or other appropriate E/M code
30 - 74 minutes 99291 x 1
75 - 104 minutes 99291 x 1 and 99292 x 1
105 - 134 minutes 99291 x 1 and 99292 x 2
135 - 164 minutes 99291 x 1 and 99292 x 3
165 - 194 minutes 99291 x 1 and 99292 x 4
194 minutes or longer 99291 - 99292 as appropriate
For example, for critical care time of 76 minutes, report 99291. For critical care time of 110 minutes, report 99291 for the first hour and 99292 x 1 for the additional 36 minutes. Critical care time less than 30 minutes is not reported using critical care codes. Any service less than 30 minutes must be reported using the ap-propriate ED, inpatient, or other code that best reflects provid-ed services.
The CPT®/CMS Rundown on Critical CareCPT® and CMS critical care definitions vary. CPT® specifies, “A critical illness or injury in which one or more vital organ systems is impaired such that there is a high probability of imminent or life threatening deterioration in the patient’s condition.” Evidence that criteria were met must be present in the medical record with the physician’s attestation that critical care was provided. CMS not only requires the illness or injury to be of an urgent or emergent nature, but there must be the added inclusion of high-
When reporting 99291-99292, the critical care clock stops when performing non-bundled, separately billable procedures.
28 Healthcare Business Monthly
level treatment(s) and interventions to satisfy critical care criteria:• CMS criteria for critical care is not met if the emergency
physician does not prescribe any pharmacological intervention.
• CMS criteria for critical care is met if other acute interventions (intubation, etc.) are provided as necessary during the course of care.
• CMS critical care is not met if the patient only receives coordination of care and interpretation of studies and is admitted or discharged.
CMS gives several examples that do not satisfy the criteria because medical necessity was not met, or the patient does not have a criti-cal care illness or injury and is not eligible for critical care payment:• Patients are admitted to a critical care unit because no other
hospital beds were available.• Patients are admitted to a critical care unit for close nursing
observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose).
• Patients are admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit.
Be Careful Not to UnbundleCPT® and CMS consider several services to be included (bundled) in critical care time when performed during the critical portion of the service by the same physician(s) providing critical care. Do not report these services separately. Both CPT® and CMS bundle the following services into critical care codes 99291 and 99292: • Interpretation of cardiac output measurements (93561,
For pediatric critical care for patients under 5 years of age (99468, 99469, 99471, 99472, 99475, and 99476), CPT® and CMS con-sider several additional services to be included in critical care time when performed during the critical portion of the service by the same physician(s) providing critical care.All services included in codes 99291-99292, as well as the follow-ing, which may be reported by facilities only:• Administration of blood/blood components (36430,
36440)• Administration of intravenous fluids (96360-96361)• Administration of surfactant (94610)• Bladder aspiration, suprapubic (51100)• Bladder catheterization (51701, 51702)• Car seat evaluation (94780-94781)• Catheterization umbilical artery (36660)• Catheterization umbilical vein (36510)• Central venous catheter, centrally inserted (36555)• Endotracheal intubation (31500)• Lumbar puncture (62270)• Oral or nasogastric tube placement (43752)• Pulmonary function testing, performed at the bedside
(94375)• Initial and subsequent care provided to a critically ill infant
or child• Other hospital care or intensive care services by same group
or individual done on same day the patient was transferred to initial neonatal/pediatric critical care
• Readmission to critical unit on same day (subsequent care)CMS further specifies the relevant time frame for bundling to in-clude the entire calendar day for which critical care is reported, rather than limiting the time to the period the patient is critically ill or injured during that calendar day, as CPT® does.
Bill Separately Reportable ServicesWhen reporting 99291-99292, the critical care clock stops when performing non-bundled, separately billable procedures. Al-though not an exhaustive list, examples of common, separately re-portable procedures that may be performed for a critically ill or in-jured patient over 5 years old include: • Cardiopulmonary resuscitation (92950)• Endotracheal intubation (31500)• Central line placement (36555, 36556)• Intraosseous placement (36680)• Tube thoracostomy (32551)
Pediatric Critical Care
CODI
NG/B
ILLI
NG
Critical Care TipIf food is on the table, the patient is stable.One would be hard pressed to explain how a critically injured or ill patient is able to consume a meal during the interventions required to report critical care. If the patient consumes a meal during the course of care, he or she was not “critical.” Default to a high level ED code, or the appropriate inpatient code to report provided services.
www.aapc.com November 2014 29
To discuss this article or topic, go to www.aapc.com Pediatric Critical Care
• Temporary transvenous pacemaker (33210)• ECG with at least 12 leads w/interpretation and report only
(93010)• Electrical cardioversion (92960)• Services performed by a transferring individual prior to
transfer of the patient to a different individual in a different group (99221-99233, 99291-99292, 99460-99462, 99477-99480)
• Services provided by another individual in another group receiving a patient transferred to a lower level of care (99231-99233, 99478-99480)
• Services provided by an individual transferring a patient to a lower level of care (99231-99233, 99291-99292)
ExampleA neonatologist is asked to assume care for a 6-year-old boy in re-spiratory arrest. She spends 90 minutes providing critical care ser-vices to stabilize the child, including endotracheal intubation and placement of a central line.Correct coding is 99291, 99292, 31500, and 36556. Because the boy is 6 years old, the time-based critical care codes are appropri-
ate. The intubation (31500) and central line placement (36556 In-sertion of non-tunneled centrally inserted central venous catheter; age 5 years or older) are not bundled into critical care, and may be re-ported separately.CMS and CPT® indicate that time is critical to the mission of ac-curately reporting critical care services, and providers must ensure that they clearly report time for these services in the medical re-cord. Coders and billers must be able to extract the aggregate time to report the appropriate critical care codes. Make sure your pro-viders are documenting accordingly. For more information on critical care services, refer to MLN Mat-ters® article MM5993, available on the CMS website at:w w w.cms.gov/Outreach-and-Education/Medicare-Learning-Net work-MLN/MLNMattersArticles/downloads/MM5993.pdf.
Holly Cassano, CPC, is CEO of ACCUCODE Consulting, LLC, and has worked in practice management, coding, auditing, teaching, blogging, and consulting for multiple specialties for the past 18 years. She writes for codingcertification.org, Tactical Management, Inc., Justcoding.com, Advance for Health Information Professionals, and others. Cassano is a member of the Tampa, Florida, local chapter, for which she has served two terms as an officer. You can reach her at [email protected] and follow her on Twitter@hollycassano.
CODING/BILLING
AAPC Coder
800-626-2633 | aapc.com/coder
The premier online coding tool from the largest coding credentialing organization
“I find the CMS 1500 claim edit checker to be the most helpful tool ever created by coding-mankind. I also love the fact that everything is in one place: LCD, NCCI edits, Fee Schedule, etc.” - Vanessa M.
Earn up to 20 CEUs with your annual subscription
Start your FREE 30-day trial today
30 Healthcare Business Monthly ■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
A&P Tip
The paranasal sinuses are four sets of air-filled sacs located within the bones of the skull and face, centered on the nasal cavity. They serve to lighten the weight of the head, to humidify and heat inhaled air, and to increase the resonance of speech.
The four sets of air-filled sacs are:
• Maxillary - the largest of the paranasal sinuses and lie behind the eyes in the maxillary bone. They are pyramid shaped, with the base along the nasal wall and the roof in the floor of the orbit.
• Frontal - funnel shaped and located in the frontal bone above the eyes in the forehead.
• Sphenoid - originate in the sphenoid bone at the center of the skull behind the ethmoid sinuses. They reach their full size by the late teenage years.
• Ethmoid - pyramid shaped and located in the ethmoid bone. There are between six and 12 on each side of the nose, and are separated by a thin septum.
Sinusitis is inflammation of the sinuses, occurring from an infection due to a virus, bacteria, or fungus. Most sinus infec-
tions are caused by a virus. Other causes include allergies, structural issues within the nasal cavity, pollutants, and a week immune system. Sinusitis affects an estimated 35 million people, with close to 16 million office visits a year.
Symptoms of sinusitis may include:
• Drainage of thick, yellow or greenish discharge from the nose or down the back of the throat
• Nasal obstruction or congestion• Pain and swelling around the eyes, cheeks, nose, or forehead• Reduced sense of smell and taste• Ear pain• Cough• Sore throatClinical documentation for sinusitis should include:
• Anatomical location – Maxillary, frontal, ethmoidal, sphenoidal, or pansinusitis (inflammation of all the sinuses on one or both sides of the nose)
• Temporal parameters – Acute (less than four weeks),
subacute (four to 12 weeks), chronic (more than 12 weeks with or without acute exacerbation), recurrent (four or more acute episodes per year)
• Contributing factors - Smoking, while not part of the code for sinusitis, should be documented to assign addi-tional codes, when applicable.
Documentation should indicate if the patient has or had:
• Exposure to environmental tobacco smoke• History of tobacco use• Occupational exposure to environmental tobacco smoke• Tobacco dependence • Tobacco useIf more than one sinus is affected, but not all (pansinusitis), the codes for other sinusitis are assigned according to whether the condition is acute, recurrent, or chronic.
We offer group discounts and reporting capabilities!We can also create or host custom courses for your employees!
Providing Quality Education at Affordable Prices
™CodingWebU.com
(484) 433-0495
We are the only program that provides interactive training incorporating audio, text and graphics to ensure you comprehend the information being taught. You will receive live updates as codes change and content is added.
You always have access to the most current information, even if you purchased the course five years ago.
2014 Annual Coding Scenarios!
Courses Starting at $30Specialty Coding - Chart Auditing - Evaluation and Management - OB/GYN
Revenue Management - Medical Terminology - Anatomy - Physiology
2015 ANESTHESIA CODING RESOURCES
Obtain proper payment for anesthesia services with these coding resources developed by the authority in anesthesia – the American Society of Anesthesiologists.
n 2015 Relative Value Guide®: A Guide for Anesthesia Valuesn 2015 CROSSWALK®: A Guide for Surgery/Anesthesia CPT® Codesn 2015 Reverse CROSSWALK® on CD-ROM: A guide that lists the CPT anesthesia codes and cross references all applicable CPT procedure codes
Order nowasahq.org/codesmart
Call: (847) 825-5586 | Promo code: CE15
14-147
ORDER
32 Healthcare Business Monthly
Healthcare Business News
Be Leery of Pharmaceutical Discount Coupons
September 18, the Office of In-spector General (OIG) issued a Special Advisory Bulletin (SAB), “Pharmaceutical Manufactur-er Copayment Coupons,” and an Office of Evaluations and Inspec-tions (OEI) report, “Manufacturer Safeguards May Not Prevent Co-payment Coupon Use for Part D
Drugs.” The bulletin and report discuss the potential for an-ti-kickback issues for pharmaceutical companies and phar-macies associated with offering co-payment and/or discount coupons.The SAB defines co-payment coupons as “any form of direct support offered by a manufacturer … to reduce or eliminate out-of-pocket costs.”According to the OIG, as addressed in the OEI report and the SAB, when offering “copayment coupons” or discounts re-
lated to pharmaceutical therapies, there “is the potential for these coupons to induce both physicians and patients to use more-expensive brand-name drugs when less-expensive and equally effective generic options are available.” OIG’s SAB ex-pressed apprehension that:
… the continued use of copayment coupons with-out the implementation of effective mechanisms to prevent their use by federal program beneficiaries, improved reliability of claims edits, and other solu-tions to make the coupons “universally identifiable,” creates risk under the federal Anti-Kickback Statute (AKS) (42 U.S.C. § 1320a-7b(b)).
What Does this Mean for Your Practice?Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO, of AAPC’s National Advisory Board, Legal Adviso-ry Board, and AAPC Ethics Committee says:
While not directly applicable to physicians, AAPC members who work for physicians might need to be aware of the compliance risks associated with these coupons in the event that drug reps attempt to sup-
An example of a drug coupon on internetdrugcoupons.com
Continuing education. Any time. Any place. ℠
Be with the family and earn CEUs!
Need CEUs to renew your CPC®? Stay in town. At home. Use our CD courses anywhere, any time, any place. You won’t have to travel, and you can even work at home.
• From the leading provider of interactive computer-CD courses with preapproved CEUs
• Finish at your own speed, quickly or leisurely • Just 1 course earns as many as 18.0 CEUs • CD-ROM (Windows) or Cloud-CD™ (Win/Mac) • No annoying timeouts. No expiring passwords.
Finish a CD in a couple of sittings, or take it a chapter a day — you choose. So visit our Web site to learn more about CEUs, the convenient way!
Our coding courses / CEU line-up: • Dive Into ICD-10 (18 CEUs) • E/M from A to Z (18 CEUs) • Primary Care Primer (18 CEUs) • E/M Chart Auditing & Coding (16 CEUs) • Demystifying the Modifiers (16 CEUs) • Medical Coding Strategies (15 CEUs) • Walking Through the ASC Codes (15 CEUs) • Coding with Heart (Cardiology) • Elements of ED Coding (11 CEUs)
Easily affordable with EasyPayments! www.HealthcareBusinessOffice.com/easypay.htm
(Most courses can also earn CEUs with AHIMA.
See our Web site.)
www.aapc.com November 2014 33
Healthcare Business News
ply the practice with such coupons as an incentive to physicians to order more costly drugs. Even if this doesn’t occur, knowledge of this issue might help prepare members for potential questions by patients seeking these coupons.
OIG also warns pharmacies that accepting manufacturer’s coupons from federal program beneficiaries may result in liability under AKS, the beneficiary inducement Compre-hensive Medical Plan, and the federal False Claims Act (31 U.S.C. § 3729).
Healthcare Financial Relationships More TransparentSeptember 30, the Centers for Medicare & Medicaid Ser-vices (CMS) launched the Open Payments website (http://cms.gov/openpayments/). As a provision of the Patient Protection and Affordable Care Act, Open Payments is a federally run pro-gram that collects information about financial relationships with physicians and hospitals, and makes it available to the
public. According to the Open Pay-ments website, “These relationships can include money for research ac-tivities, gifts, speaking fees, meals, or travel.”The Open Payments website’s goal is to increase payment transparency for research through its database. The records are organized into three categories:• General payments• Research payments • Physician ownership and investments
According to the data from August 1, 2013 to December 31, 2013, manufacturers made 4.4 million payments to 546,000 physicians and 1,360 teaching hospitals. CMS withheld about one-third of the data for the launch due to inaccuracy of some payment records.
Source: Modern Healthcare, Jaimy Lee, “Open Payments Website Launches,” September 30
As displayed on http://cms.gov.openpayments
Enos training will help you learn to code E/M with confidence, avoid RAC audits, and maximize your reimbursement by better choosing the right level of service. Learn at your own pace and retake the course whenever you wish. The course pays for itself.
We offer eLearning, webinars, chart audits, and any services we can to help you minimize your risk and maximize your reimbursement. So, what are you waiting for? You can’t afford NOT to take this course!
For course information, go to www.EnosMedicalCoding.com
Maximize Reimbursement
&Minimize RiskYou may be missing out on $30 to $50 per claim
NAMAS has “THE” conference for you!
6th ANNUAL
Auditing & Compliance Conference 2014
http://namas.co/events/namas-conference
December 7-9, 2014 • Grove Park Inn in Asheville, NC
S ince I passed my certification, I have attended each NAMAS conference. The information I receive during these conferences is invaluable. I continue to receive confirmation that I’m auditing correctly, yet receive education on issues I’ve never
audited before.”— Dolly Perrine, CPMA
As a health care professional working in
compliance, auditing and administration, concerns
surrounding audits are everywhere — don’t panic,
we have you covered! Don’t miss this opportunity
to attend a conference with the industry leaders in
the areas of auditing and compliance.
• Elin Baklid-Kunz
• John Burns
• Frank Cohen
• Shannon DeConda
• James Dunnick, M.D.
• David Glaser
• Maggie Mac
• Lynn Merz
• Robert Liles
• Kathy Pride
• Sara San Pedro
• Don Self
• Regan Tyler
Noted national speakers include:
Sponsored by:Topics and full course descriptions are now available
in the full agenda on our website: www.NAMAS.co
www.aapc.com November 2014 35
AAPC is now accepting applications for new Na-tional Advisory Board (NAB) members to serve in 2015–2018. If becoming an NAB member is something you’re considering, here’s what you need to know.
Who Is the NAB?The NAB is a voluntary, non-voting board cre-ated to help advise AAPC leadership on industry related issues, trends, and member needs, as well as to enthusiastically promote and support and mission of AAPC. They also serve the purpose of providing a voice for the general membership to AAPC, listening to member feedback, and re-laying that information to AAPC.The board is comprised of 20 members: 16 of which will be selected from eight geographic regions and four officers. Officers consist of a president, president-elect, secretary, and member relations. The board works closely with AAPC CEO Jason VandenAkker and AAPC Liaison Rhonda Buckholtz, CPC, CPMA, CPC-I, CENTC, CGSC, COBGC, CPEDC, vice president of ICD-10 Training and Education. For more information about NAB members, go to the AAPC website at: www.aapc.com/AboutUs/national-advisory-board.aspx.
What Are the Responsibilities?The NAB’s main responsibility is to the mem-bership and to AAPC to “Uphold a Higher Stan-dard.” They have a commitment to participate in monthly conference calls, steering committees, and attend the annual NAB fall retreat.
Serving at ConferenceThe NAB also provides large support at AAPC’s National Conference, HEALTHCON. Board members work closely with the AAPC confer-ence team to support attendees at registration, assist with general AAPC/conference related questions, and provide support for speakers. It is a fabulous bonding experience as board mem-bers work together to help make HEALTH-CON the great success it is.
Moving AAPC ForwardThe NAB plays an integral part in the forward motion of AAPC by continually sharing new ideas, opinions, and promoting the recruitment
of new members. They work with the national organization of AAPC for the betterment of the entire membership and healthcare community.
Committing to Three YearsNAB serves with a three-year commitment of service. The next term begins April 2015 at HEALTHCON in Las Vegas and runs until the national conference in 2018. At the end of each term, four board members stay on as officers to serve another three years.
Application ProcessIf this sounds like something you’re interested in, consider submitting an application. Here’s the process:1. Each interested member will be asked to
complete an application form and to sub-mit letters of recommendation. The appli-cations will be available on AAPC’s website November 1, 2014.
2. All required paperwork must be received in the national office (Salt Lake City) by December 31, 2014.
3. AAPC management and current NAB officers will review all applications and make final selections by the beginning of February 2015.
4. The new NAB members will be notified by mid-February 2015.
Newly selected NAB members need to be avail-able to attend 2015 HEALTHCON in Las Ve-gas, Nevada, March 29 – April 1. For details on each step, conference attendance, and the appli-cation, go to the AAPC website at: https://www.aapc.com/AboutUs/national-advisory-board.aspx.
What NAB Members Have to SayNAB Member Relations Officer Nancy Clark, CPC, CPC-H, CPB, CPMA, CPC-I, had this to say about her time serving on the board:One of my favorite responsibilities on the NAB is to “work” the AAPC conferences. This usually involves arriving around 6 a.m. and assisting wherever needed. Just a few of my duties have included assisting in registra-tion, introducing and helping speakers, and organizing the AAPC Feud. I enjoy the op-portunity to meet members from different re-
gions and hear their concerns. I also love the feeling of accomplishment we share with the very dedicated AAPC staff at the end of the day — no matter how tired we are!
The reason I applied back in 2010 was the ap-pealing thought of giving back and doing more for the coding community. It has been one of the most rewarding adventures in my career and it just keeps getting better. Are you ready to be the voice of your peers? if so, please give some thought to joining me and the other new officers on the board.
Jaci Johnson, CPC, CPMA, CEMC, CPC-H, CPC-I, is president-elect of NAB. She teaches PMCC and manages a national client list, providing compliance monitoring for provider documentation. Johnson is past president of the Richmond, Virginia, local chap-ter and Virginia’s Coder of the Year in 2006.
NAB MESSAGE
Send in Your NAB Applications
By Jaci Johnson, CPC, CPMA, CEMC, CPC-H, CPC-I
NAB: David Dunn, Jaci Johnson, Maryann Palmeter, Nancy Clark, Jeanne Gershman, Susan Edwards, Michael Miscoe, Yvonne Dailey, M. Colleen Mescall, Erica Cousin, Sylvia Partridge, Virginia Outlaw, Angela Clements, Stacy Harper, Ann Bina, Chandra Stephenson, Cynthia Swanson, Rhonda Zollars, Ida Landry, Melissa Tescher
photo by Rachel Momeni
36 Healthcare Business Monthly
Procure the Best Management Report
By Jim Strafford, CEDC, MCS-P
Key performance indicators will help you generate a true picture of practice revenue.
Since I began my career in revenue cycle management, formerly called accounts receivable (A/R) management, reporting capac-ity and functionality have increased exponentially. Back then, a billing cycle manager could access a very basic package of reports to measure billing and collection effectiveness. Custom reporting was minimal, and usually required a request to the information technology department and a lengthy wait.
Fast Forward 30 YearsToday’s practice manager is faced with a daunting menu of stan-dard and custom reports from multiple sources, including bill-ing systems and reporting middleware. Yet, practice manage-ment/revenue cycle reports are often underutilized and not ana-lyzed effectively.For example, a practice my company reviewed recently had un-dergone an expensive billing system upgrade, but was not receiv-ing key reports. We contacted the software vendor and found out that the reports were available, but weren’t accessed by the billing office. In another review, a large, multi-site practice was receiv-ing minimal reporting from the hospital central billing office — despite the hospital having a multi-million dollar billing system.As a revenue cycle manager or practice manager, you’d probably like a single report to provide the data and metrics you need to de-termine billing and collection effectiveness and trends. I’ll provide some tips to build this report, starting with basic billing and col-lections metrics — referred to in 2014 as key performance indica-tors (KPIs) or the revenue cycle spreadsheet.
Basic Revenue CycleThe report will track KPI by month. Let’s start with April as the first month, as shown in Table 1. Note that all metrics on this re-port are by date of entry (DOE). This would be the date charges/payment/adjustments were posted to the billing system.
■ PRACTICE MANAGEMENT
■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
Note: Besides KPI reports by DOE metrics, there are also re-ports by date of service (DOS), which are very useful for track-ing cash flow from a given DOS; however, the resulting metrics can be confusing. I’ll cover this type of report in a future issue of Healthcare Business Monthly.
Analyze the NumbersA/R: This is the total amount of charges that are not yet resolved by payment, adjustment, or write off to bad debt.Charges: This is the total charges billed for the month.Adjustments: This is the total charges adjusted from the A/R. This typically represents amounts that will not be paid due to managed care and other payer contracts.Volume: This is the total volume of services rendered and billed with CPT® or HCPCS Level II codes for a given month. It is some-times called “services of procedures.”Payments: This is all payments posted from payers and self-pay patients for a given month.Collections: This is the amount of unpaid claims, usually self-pay, that have been moved from the active A/R to collections. This should mean these unpaid claims have been moved to a third-par-ty collection agency or internal collections office.
Ending A/R: This is the result of all of the above transactions for a given month (April) on the A/R.
Six Month Revenue CycleKPIs give a general feel for the basic practice metrics in a month. Considered alone, they tell the practice manger very little about the revenue cycle performance. To shed light on revenue cycle per-formance, you must spread these metrics over time. Table 2 shows six months of KPIs.
Analyze the NumbersTable 2 provides a much more educated representation of what is happening with your practice revenue. Let’s analyze KPI individ-ually over the six-month reporting period.A/R: There are A/R fluctuations, but no dramatic changes. Re-search a major increase or reduction in A/R.Charges: Charges range from a low of $42,000 in May to a high of $71,000 in July. Why is there a $29,000 increase between May and July? It could be because we are the Beachcomber Urgent Care Center, and summer is peak season. If this is the trend every year, this would be expected. But what if your practice doesn’t have those types of seasonal shifts? Could it be that the coding depart-ment had a backlog in May, and dug their way out over the sum-mer? Investigate it further.Volume: Volume of rendered services is relatively consistent with charge trends; however, in May charges were down $8,000 from April, even though volume increased by 100. This could be be-cause the practice sees fewer acute patients in May compared to
April. If that isn’t the case, could it be a new provider joined the practice in May, whose docu-mentation isn’t adequate, result-ing in a lower average charge? Determine the reasons for the metrics shift and remedy them.Adjustments: The adjustments, mostly insurance allowances that the practice accepts based on contracts with payers, range from $9,000 to $19,000. Overall, they appear consistent with charges and payments. Payments: Payments range from a low of $21,000 in June to a high of $37,000 in October. In using a KPI spreadsheet, you can see the impact of increased charges in July and August on pay-ments in August and September. Payments of $21,000 in June ap-pear low based on the charges. Consider drilling down into this metric. There are a few possibilities. There may have been a pay-ment postings backlog in June. Sometimes, large payments come late in a month and are not included in the month-end totals. You might reconcile deposits with payments (do this monthly) to see if this is an issue. Or maybe there was a shift in payer mix. This will require more specific metrics showing payments by payer.Collections: Accounts that moved to this status ranged from a low of $2,500 in August to a high of $8,200 in September. Collec-tions status needs to be monitored carefully. Often, management controls transfer to collections status, especially in smaller prac-tices. There could be good reason for this variance; for instance, in
house collectors are following up and the manager does not want to send the accounts to a more expensive collection agency. The decrease can also mean the person who manages the transfer to collections was busy, and many uncollectable accounts remained in the active A/R instead of being worked aggressively in collec-tions. I have seen this issue many times in our consulting practice.Ending A/R: From an accounting point of view, the beginning and ending A/R should reconcile each month. With automated systems, this typically is not an issue, but it’s a good idea to contin-uously watch the A/R to determine if there are major increases or unexplained decreases. An A/R decrease should be a good thing, reflecting collection improvement and efficiency. But that is not always the case: A large transfer of accounts to collections status could also decrease A/R.
Use KPI Spreadsheets to Identify IssuesA KPI spreadsheet allows a manager to spot trends in charges, pay-ments, adjustments, collections, and A/R that can’t be identified by reviewing month-end or year-to-date metrics only. With im-
… you’d probably like a single report to provide the data and metrics you need to determine billing and collection effectiveness and trends.
www.aapc.com November 2014 39
Management ReportTo discuss this article or topic, go to www.aapc.com
provements in databases and reporting, this type of report should be available from most billing software packages. If you’re not re-ceiving one, request it!These spreadsheets can be very useful in identifying revenue cycle issues, but to pin-point and resolve issues, more data is neces-sary. There are many other reports in most billing packages, from “aging” to various production reports. Consider using addi-tional performance indicators to make your KPI spreadsheet the best management re-port.Coming up: We’ll look at additional perfor-mance indicators and the metrics for average charge, adjustments, payments by payer, and decreased A/R in greater detail in an upcom-ing issue of Healthcare Business Monthly.
Jim Strafford, CEDC, MCS-P, has more than 30 years’ experience as a consultant, manager, and educator in all phases of medical coding, billing, compliance, and re-imbursement. He is published, with expertise in on emergency department revenue cycle and coding is-
sues. Strafford is the principle at Strafford Consulting Services and a member of the Philadelphia, Pennsylvania local chapter.
NOW EMR STANDS FOREVENMOREREVENUEFOR BILLERS
Have providers who hate their EMR?
Who are still stuck using paper charts?
Who risk penalties because their EMR is not MUII certified?
Introduce them to OneTouch, an EMR that looks familiar,
runs faster, is flexible and future-proof. An EMR that works equally
well on mobile phones, iPads, and desktops. One that doesn’t
require a scary amount of time or money to implement.
OneTouch will simplify their lives and
add revenue to your bottom line.
Let OneTouch pay you
for referrals!
Learn More at OneTouchEMR.com/AAPC1.800.4.1.TOUCH • 10100 N. Central Expressway, Suite 250 • Dallas, TX 75231
■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
Hire and Retain Excellent Coding StaffPart 2: Keep top talent in your practice.
By Pam Brooks, CPC, CPC-H
Last month, we talked about how to find and hire the best coders for your practice (See “Hire and Retain Excellent Coding Staff:
Part 1,” Healthcare Business Monthly, October, pages 42-45). Let’s now consider how to retain your exceptional employees.
Start on the Right FootAfter you’ve found the ideal candidate for a coding position in your practice, there’s still more work to do to make sure your em-ployee’s first few months (and next several years) are successful, productive, and worry-free.
TrainOne of the biggest complaints new employees have is insufficient training. In addition to the usual orientation, such as an intro-duction to staff and showing them to their desk, new employees need safety training, a review of policies and procedures (includ-ing where to find them), a separate review of the organization’s HIPAA policy, and if possible, a workplace ergonomic assessment to prevent repetitive motion injuries.
MonitorCheck in with the new employee periodically during the first few weeks to see how things are going. Solicit feedback from the new hire’s co-workers to help gauge his or her progress. Use manage-ment reports to track productivity. Communicate often during the early days to answer questions, provide support and encour-agement, correct mistakes, and make suggestions.
ReviewPerform random audits of the new coder’s work to check for accu-racy. Be sure to document carefully both progress and problems, so if you must release the new employee before the end of his or her probationary period, you have a clear record to support the termi-nation. Schedule a 90-day review, and make plans for continued success beyond that time.
Long-term Success Requires Continued EncouragementAfter the initial 90 days, employee support consists of more than
just an annual review. One way to keep employees for the long term is to provide rewards.“Reward” doesn’t always have to mean money. In fact, most em-ployees appreciate perks that aren’t linked to money. Employees want to be acknowledged for the good work they’ve done. They want a pleasant working environment. They want great managers and engaged co-workers. It’s a manager’s job to make sure these re-wards are possible. This can be accomplished in a number of ways.
Employees appreciate flexible, family-friendly jobs. Everyone has a life outside of work. Enable a flexible work day by promot-ing teamwork. That way, if one employee needs to leave early for a parent-teacher conference, his or her absence won’t derail the en-tire staff ’s productivity.
Keep coders up to date on changes in the industry. Providing continuing education, workshop opportunities, continuing edu-cation unit (CEU) dollars, tuition reimbursement, and other ed-ucational incentives is a great way to keep your staff current, en-gaged, and loyal. Sending staff to national or regional conferences is probably the most effective way to provide education, a wonder-ful benefit, lots of CEUs, and a reward for a job well done.
Provide opportunities for staff development. For example:• Support employee participation in AAPC local chapters,
and even pay them to attend meetings.• Arrange for employees to take a course to learn a new
software application.• Provide employees with the opportunity for a workshop in
effective communication.• Find out what your employees’ career goals are and offer
your assistance in helping them to meet those goals.• Use your education budget to provide group training
or workshop subscriptions. If you’re a not-for-profit organization, you may qualify for education grants for your employees.
• Tap into local resources by contacting your community hospital and taking advantage of employee education offerings.
• Allow your staff to job shadow in other departments or offices and cross-train everyone so you’re covered in emergencies. This will ensure everyone knows office operations and understands a variety of work to keep them engaged.
• Ask your physicians to mentor staff and share their expertise.
Provide a comfortable workspace. One that allows your new employee enough room to work without unwanted drama or pol-itics, a freezing-cold office, or other distractions. It’s the manag-er’s job to make sure the work environment is conducive to hap-py employees.
Appreciate coders for the work they do. This is often the single most important factor when it comes to job satisfaction. If employ-ees consistently perform in an outstanding manner, but receive no acknowledgement from management, it won’t be long before they perform outstandingly for someone else.
Challenge employees with interesting projects. But don’t mi-cromanage their efforts. Allow them to take ownership of their work, and provide them with the ability to make decisions about how that work is performed and completed. Set the bar high: As employees excel and improve, they’ll strive to work smarter and more efficiently. Identify their strengths and allow them to use those strengths where they are most valuable.
Act like a manager. Employees want a leader who is accessible, fair, responsive, and honest. They want managers to hold people accountable for their work, and to be consistent with policies and procedures. They want to trust that confidences are not shared. Managers must be able to think objectively and decide wheth-er problems in the work place were caused by themselves, rather than their employees.
Keep morale high. Morale is the intangible “feel good” emotion in the workplace that can be enhanced or destroyed by managers who fail to value their staff. There are many low-cost and creative ways to reward staff and build morale in the workplace.
For example:• Schedule “breakfast days” on occasion. Bring in morning
casseroles and coffee, for example, just because.• Introduce a more relaxed environment by having jeans day
or casual Friday from time to time, if your organization allows it.
• Initiate a “Coders’ Night Out,” where the staff gets together at a local restaurant for drinks and appetizers after work.
• Have theme days, such as Cinco de Mayo, where everyone dresses up and you put out food and decorations in line with the theme.
• Encourage the team to work together on a volunteer project such as United Way, Habitat for Humanity, or a 5K run/walk for charity.
• Celebrate birthdays, weddings, and new babies.• Take walks together at lunch (no work talk along the way).
Encourage the team to work together on a volunteer project like
United Way, Habitat for Humanity, or a 5K run/walk for charity.
42 Healthcare Business Monthly
Hire and Retain
PRAC
TICE
MAN
AGEM
ENT
To discuss this article or topic, go to www.aapc.com
• Provide free yoga sessions during mid-day lunch breaks.
Above all, listen to your employees. Welcome suggestions, comments, and even criticism. No manager can know and do everything. Staff members are the subject matter experts. They do the work, and they know when something is not working.Acknowledging excellent employees is easy. Acknowledging employees who are struggling takes some effort, but if you be-gin to provide them with positive feedback, allow them some flexibility, and challenge them to do their best, the results can be amazing.
Money Still TalksMoney is always a good incentive. Pay your staff what the market says they should be paid. The adage “you get what you pay for” is frequently true. Employees who are willing to work for peanuts might just give peanuts in return. So ante up and make sure everyone’s being paid what they’re worth. Otherwise, it will cost 1.5 - 2.5 times their salary (depending on what study you look at) over the year to replace them.Employee benefits are almost expected in the healthcare industry. A decent benefit package is not only a great incentive, but may be a requirement in the current healthcare environment. Encourage wellness programs to keep costs down. Hiring excellent coding staff, developing current staff ’s skills, and retaining those top-notch coders for the long term is a process that can lead to an outstanding workplace and a well-functioning coding department. It’s a process that starts with understanding the job, selecting the right people, and mentoring and supporting those people once they’re in place. Rewarding your excellent staff is a reward in itself!
Pam Brooks, CPC, CPC-H, is the coding manager at Wentworth Douglass Hospital in Dover, New Hampshire. She supervises a staff of multi-specialty coders and has devel-oped a team of medical auditors and educators, surgical specialty coders, and documen-tation improvement specialists. Brooks first started in a mental health billing office and moved into practice management of an eating disorders practice. She earned a Bachelor
of Science degree in Adult Education and Workplace Training from Granite State College and is completing a master’s in Health Administration from St. Joseph’s College, Maine. Brooks is a member of the Seacoast-Do-ver local chapter and sits on the AAPC Chapter Association board of directors for Region 1. She is a frequent contributor and speaks throughout New England and nationally regarding coding and career development topics.
If employees consistently perform in an outstanding manner, but receive no acknowledgement from management, it won’t be long before they perform outstandingly for someone else.
Ask the Legal Advisory BoardFrom HIPAA’s Privacy Rule and anti-kickback statute, to compliant coding, to fraud and abuse, there are a lot of legal ramifications to working in healthcare. You almost need a lawyer on call 24/7 just to help you make sense of all the new guidelines. As luck would have it, you do! AAPC’s Legal Advisory Board (LAB) is ready, willing, and able to answer your legal questions. Simply send your health law questions to [email protected] and let the legal professionals hash out the answers. Select Q&As will be published in Healthcare Business Monthly.
Sinusitis that lasts four to 12 weeks is considered …a. Acuteb. Subacutec. Chronicd. Recurrent
Check your answer on page 65. Take this monthly quiz, in addition to AAPC’s ICD-10 Anatomy and Pathophysiology advanced training, to prepare for the increased clinical specificity requirements of ICD-10-CM. To learn more about AAPC’s ICD-10 training, go to www.aapc.com to download AAPC’s ICD-10 Service Offering Summary.
Rhonda Buckholtz, CPC, CPMA, CPC-I, CENTC, CGSC, COBGC, CPEDC, is vice president of ICD-10 Training and Education at AAPC.
■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
■ PRACTICE MANAGEMENT
Are you charging for every service you perform? If your practice is like most, the answer is probably “No.” Many estimates suggest a significant portion of annual practice revenue is lost because practices simply do not bill for services and procedures that pro-viders perform.
Keep CurrentThe charge ticket (a.k.a. the encounter sheet or superbill) is the beginning of the revenue cycle. In a perfect world, every provid-er would have a certified coder follow him or her around to assist with coding for every patient. This may not be possible in the real world, but providers can have an updated charge ticket for every setting in which they work.The key word is updated. Many practices or departments don’t take the time to update the charge ticket every year (or more often, when necessary, such as when you have a new payer contract). Yet, the charge ticket is one of the most important tools your practice or department will use. Your superbill should list current CPT® and ICD-9-CM codes to reflect the majority of the services you provide. This allows providers to communicate to the office staff and, by extension, allows office staff to communicate with payers the services being provided and why those services are necessary.
Ensure Complete Charge CaptureCharge capture means that all encounters, and all the services and procedures provided, are accounted for. The medical practi-tioner should use pre-numbered encounter forms for office/clinic visits and other encounters. Most practice management systems
can produce customized encounter forms and can track encoun-ters within the system. Your practice or department should insist on having editing capabilities for the encounter form(s), if they are generated from the system. This saves system support costs and al-lows for timely encounter form edits.Written policies and procedures should identify who is responsible for entering and maintaining the various services and procedures on the form. To capture the diagnoses, the encounter form may include pre-coded diagnoses (usually the top 25 to 50 for the prac-tice or department). Update the encounter form as often as neces-sary to reflect correct, current diagnoses, services, and procedure codes. If your practice or department can customize the encoun-ter form on the management system, collaborate with the pro-viders on a design that will ensure accurate information capture.It’s important for the medical record to support diagnoses, ser-vices, and procedures, and that visit circumstances and types are marked on the encounter form (e.g., new patients versus estab-lished patients, preventive visits, consultations, etc.). Perform in-ternal audits (five to 10 records per provider, per month, at a min-imum) to compare the documentation in the medical record with what has been captured on the encounter form, and maintain the written results. Immediately share the findings from audits with providers, and offer education, as needed.In most practices, the bulk of the services provided are captured with evaluation and management (E/M) codes. Because Medi-care beneficiaries constitute a significant segment of many prac-tices, and because Medicare-covered preventive services (and the G codes that must be used to bill for them) are growing in num-ber, these should be included on your superbill, as should consul-
By Linda Martien, CPC, CPC-H, CPMA
www.aapc.com November 2014 45
Revenue Cycle
PRACTICE MANAGEM
ENT
tations codes (99241–99245 and 99251-99255) for non-Medi-care patients. Teleconference consultation codes (certain HCPCS Level II G codes) may be reported to Medicare, and also should be included.It’s more difficult to track charge capture of a medial practitioner’s non-office encounters. Inpatient and outpatient encounters at the hospital, as well as nursing home visits, account for the majority of non-office encounters. Charges can include hospital inpatient care, observation stay care, consultations, surgeries and other pro-cedures, and test or study interpretation and reports. Work closely with the providers and personnel in the non-office setting to de-velop a method to capture non-office charges. Hospital computer systems can generate a provider’s surgery schedule, ancillary out-patient schedules, and inpatient census. Constant monitoring is necessary to avoid losing non-office charges.
Keep Track of All Charge TicketsTo ensure you receive all the charge tickets from your providers, supply each with a set of unique, sequentially numbered charge tickets. You can design the charge tickets to fit into a small book they can carry with them. Office staff should ensure all numbers are in sequence when the tickets are delivered. If a charge ticket is missing, staff should alert the provider. Have each provider keep a log, in which the charge ticket series for each day can be entered. That way, a missing ticket can be identified easily.Be sure your providers are trained to use the charge tickets, to capture all billable services. You can’t expect charges to be cap-tured accurately if providers are unclear about the purpose of the
tickets. Consider vaccines, for example: Can you charge 90460-90461 Immunization administration through 18 years of age via any route of administration, with counseling by physician or other qual-ified health care professional... in addition to the vaccine supply? Only if the provider counsels regarding the vaccine (i.e., side ef-fects, benefits, contraindications, etc.). If your practice dispens-es vaccines regularly, your practitioners should be knowledgeable about the rules.
Electronic Superbill/Charge TicketSuperbills are the backbone of your medical practice’s financial dealings, and any labor and cost reductions in this area can affect your future immensely. It’s no surprise that electronic superbills are something to be excited about. They’re designed to save your practice time, money, and labor. Paper superbills, still common-ly used today, represent more work and require more time to en-ter charges for billing. Paper superbills also boast a larger margin of human error. Electronic superbills mean less guesswork as to which CPT® codes were circled, or missing partially circled codes. Bad coding equals bad superbill, and vice versa.Make no mistake: There’s considerable money at stake with bad superbills. The American Academy of Ophthalmology’s website offers a few real life cases, including a scenario where a surgeon’s staff coded all laser treatments using the same CPT® code. The ini-tial loss of revenue was nearly $700, but was much greater when surgeries beyond the scope of the audit were considered.
Source: “Costly Coding Errors,” American Academy of Ophthalmology (www.aao.org/yo/newsletter/200810/article01.cfm)
Paper superbills, still commonly used today, represent more work
and require more time to enter charges for billing.
To discuss this article or topic, go to www.aapc.comRevenue Cycle
PRAC
TICE
MAN
AGEM
ENT
EHRs Ease Charge CaptureProper coding with an electronic health record (EHR) means you should always have a proper (paperless) superbill. EHR tem-plates and superbills provide the platform necessary for daily use of codes. Automating charge capture via your EHR leads to more ac-curate, higher levels of E/M coding. Your EHR may automatically suggest codes at the time of the patient encounter, based upon the content present in the physician’s patient progress note.
ICD-10 May Prompt You to Go PaperlessThe switch to ICD-10 is looming, whereby superbills will become the standard daily code use. Electronic superbills can help you make the switch. Because ICD-10 code descriptions sometimes take up significant space on a standard letter-sized form, printing fractions of superbills will be tedious and time-consuming. Early on, in discussions about transitioning to the ICD-10 superbill, it was estimated a current two-page superbill (front and back) would require up to 20 pages with ICD-10’s expanded specificity. In fact, when going over the case of one hospital on her team, Gayl Kirkpatrick of 3M Health Information Systems Consulting Services recently noted in a Government Health IT article, “We took a two-page superbill in ICD-9 and translated that into ICD-10. It became a 48-page superbill.” (www.govhealthit.com/blog/icd-10-superbill-will-superbills-survive-icd-10-implementation?page=10) Multiple page encounter forms are impractical and costly, leading some to believe ICD-10 will make the superbill obsolete. But for most, the logical choice lies in converting to an EHR.
Superbill Summary• Update charge tickets at least annually.• Perform training to staff and providers after updates to
avoid errors and misunderstandings.• Use sequentially numbered charge tickets for each provider
and each type of encounter they perform.• Log charge tickets for each provider as a series for each
day, identify any missing charge tickets, and report to the provider.
• Decide if modifiers should be “hard coded” (linked to the code on the charge ticket or charge master), or if they will be added manually by the coder or health information management department.
• Start looking now at ICD-10 transition for your charge tickets.
Encourage consistent communication between the coder, data-entry, office and billing staff, and providers. Everyone should be comfortable in going to each other with questions about charges and their coding.
Linda Martien, CPC, CPC-H, CPMA, is director of reimbursement at Cytomedix, and brings her 30-plus years of experience in coding, billing, auditing, management, and con-sulting to the table. She is a member of the AAPC Chapter Association board of directors for 2014-2017, and is a past member and officer of the National Advisory Board. She also has held various officer positions for Columbia and Jefferson City, Missouri, local chapters.
Early on, in discussions about transitioning to the ICD-10 superbill, it was estimated a current two-page superbill (front and back) would require up to 20 pages with ICD-10’s expanded specificity.
www.aapc.com November 2014 47
Sydney Romanof, CPCWHY I CODE
For 25 years, I dabbled in college, raised kids, and self-trained in secretarial and computer tasks. I had a “jack of all trades and master of none” kind of education.
With my kids pretty much out on their own, it was time for me to focus on myself. I wanted a career that was not niche-market dependent and was fairly impervious to economic decline. Healthcare was a perfect choice. None of my self-taught clerical skills were connected to healthcare (with the exception of organizing my kids’ doctor visits), however. I knew this would be an uphill climb.
First Step: Map Your CourseI tried to find the right job to fit my personality (I’d rather not work with the public), my skills (I’m tech-savvy), and my quirks (I’m a bit geeky and enjoy detailed research). I looked into jobs like nuclear medicine technician, radiology assistant, and sonography technician. In my search, I came across a coding exam preparatory course. I researched coding and workforce demands, and it looked pretty good, so I went for it.
Second Step: Get CertifiedAbout halfway through the course, I realized I was the only one in the class who wasn’t already in some sort of healthcare job. Yikes! I studied harder. My instructor did not discourage me; “cold turkey” is not the usual way to become a certified coder, but it’s achievable. I kept studying, and with momentum and pride, I passed the exam.
Third Step: Get Your Foot in the DoorI found out that my new wall art didn’t include the job experience that all the help wanted ads demanded, so I kept my day job, searched for internship positions, attended AAPC local chapter meetings, and I offered myself to be an unpaid volunteer coder to get experience and a foot in the door, anywhere. After 10 months, I got a break.
Climb HigherI learned so much in those seven months at an orthopedics group. When I had a little hands-on experience, I applied for a job in the town where my grandson (Oh, and his parents!)
lives. Although I didn’t have the one year’s experience they wanted, I got the position.
My duties were more problem-solving and research-oriented, and soon led to a coding supervisor promotion. It’s stimulat-ing and challenging, and a perfect fit for me. I investigate and fix denied claims, work out methods for a smoother work-flow, and I am a resource for residents and providers.
This year, I serve as local chapter secretary, and I’m excited about its possibilities. Working in a teaching hospital, I aim to become more involved in new resident coding training and information support for a wider range of specialists.
How Can NAMAS Help You With Auditing & Compliance?
Webinars that include CEU approval for specialty certifications and Core CPCy & CPMAy
Forum for all of your Auditing & Compliance needs
Trends and information on the Auditing & Compliance Industry
Ask-the-Auditor Access
Discounts on Products & Services
Quarterly Free Newsletter specific to Auditing & Compliance
In the past, collections in medical practices fo-cused predominantly on insurance collections because insurers paid the greater portion of the physician’s fee. Thirty-five years later, the pen-dulum has swung from the insurance compa-ny paying anywhere from 80-100 percent of the physician fee to the patient being responsi-ble for a minimum of 30 percent (up to 100 per-cent) of the charges. The industry is facing the most significant change in reimburse-ment since the introduction of the co-pay in the 1980s. New ideas and tools are needed to manage the change successfully.
New Skills Are NeededPreviously, front desk staff identified the amount of the co-pay-ment on the patient’s insurance card and collected that payment. Now, front desk staff must be much more involved in collections, understand insurance concepts, and feel comfortable discussing financial policies and patient responsibility. Confidence, with-out coming off as overbearing, patronizing, or uncompassionate, is paramount to collection success. This takes training, scripting, and role-playing with staff.I don’t recommend that front desk staff do all the heavy lifting, however. Every patient coming to your practice should have heard about your financial policy at least three times before they arrive at the check-in window:• First time - when the patient schedules an appointment• Second time - when the practice confrms the appointment• Third time - snail mail, email, patient portal, or however
else your practice communicates with patientsBe sure your check-in person can answer any questions and is able to estimate the patient’s payment portion for that day’s visit.
New Technology Is NeededVery few medical practices have the wherewithal to estimate pa-tient balances without sophisticated technology. Whether it’s ap-plying the unpaid deductible to a typical office visit charge or un-derstanding out-of-network benefits for an in-office procedure, the busy front desk staff are rarely able to provide a fast answer to “What will I owe today?” (if the patient dares to ask).One technology option that is available at minimal or no cost is keeping a patient’s credit or debit card on file to charge the bal-ance owed after insurance has paid. Although an estimate of the amount due by the patient is always helpful to mentally prepare the patient, sometimes it just isn’t possible to provide this, even at the checkout desk. The hub around which credit card on file (CCoF) works is called Payment Gateway Software, which allows you to use a small swip-er to securely capture a patient’s credit card information and store it in a third-party, offsite server. The credit card information is en-crypted and stored on the web (Payment Card Industry (PCI)-compliant), and can be retrieved to charge the patient for post-in-surance claim balances, as well as recurring payments such a pay-ment plan. See Chart B for the benefits associated with using Pay-ment Gateway Software for CCoF.
A New Mind-set Is NeededThe time has come for medical practices to take a stand on patients being required to pay at time of service, or immediately after insur-
■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
■ PRACTICE MANAGEMENT
Success relies on front desk staff collections and post-claim payment strategies.
www.aapc.com November 2014 49
ance pays. For longer than I have been in medical practice man-agement, it has been taboo to talk about money with patients. It’s as if the fact that the patient has been provided a valuable service is beside the point. As you know, it’s crucial that medical practic-es be viable financially, and that means having the “money talk.”The money talk begins with a clear, understandable financial poli-cy not hidden under the stack of papers the patient signs, or buried deep in the patient portal registration process. Patients appreciate understanding exactly how your financial policy relates to their specific situation, and having the information out in the open.Succeeding in the new world of patient collections necessitates staff retraining, implementation of time-of-service and post-claim payment strategies, and a willingness to have frank conversations with your patients. Be sure you’re ready to help your practice make it in the new world of patient collections.
Note: Readers can download a free copy of Mary Pat Whaley’s preferred financial policy here: http://bit.ly/FinancialPolicy.
Mary Pat Whaley, FACMPE, CPC, is co-founder and president of Manage My Practice, a practice management consulting firm focused on solo and small medical practices. With 25+ years managing physician practices of all sizes and specialties in the private and pub-lic sectors, Whaley is a physician advocate and practice management consultant. She holds a Board Certification in Medical Practice Management and is a member of the Durham, North Carolina, local chapter.
Very few medical practices have the wherewithal to estimate
patient balances without sophisticated technology.
PRACTICE MANAGEM
ENT
Patient CollectionsTo discuss this article or topic, go to www.aapc.com
Chart A: Patient pay as a percentage of provider’s total revenue
Source: McKinsey & Co., “Patient Payment Collection: Challenges for Payers and Providers,” www.navinet.net/sites/default/files/pdf/NaviNet_Patient_Payment_Collection_WP_FINALjs.pdf
CHANGE BENEFIT
Improve cash flow Improve liquidity, stabilize finances, protect practice against 90-day grace period for exchange plans, handle high-deductible plans
Eliminate statements Reduce collection expenses, deposits, and staff work-load in posting payments
Electronic payment plans “Set it and forget it!” Secure and flexible
Eliminate manual patient refunds
Improve patient satisfaction with fast refunds, reduce practice expense
Eliminate bounced checks
Reduce collection expense (time and labor)
Reduce/eliminate deposits
All insurance payments are EFT starting January 1, 2014, with CCoF, no deposits are required
Faster check-in and -out No need to ask for payment!
■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
You’ve heard it a million times: Misus-ing modifiers will lead to trouble. Ar-ticle after article enumerate the pit-
falls of “outlier” status (i.e., reporting too many high-level evaluation and manage-ment (E/M) services). Coders are warned repeatedly against charging separately for services that are part of the global surgi-cal package (unbundling). With all the em-phasis on proper coding, you might be sur-prised to learn the most common audit finding isn’t coding related at all.
What Auditors Wish You KnewMissing records are devastating, and surprisingly common audit findings.
AUDIT/COMPLIANCE ■By Lisa Jensen, MHBL, FACMPE, CPC
52 Healthcare Business Monthly
Auditors Wish You Knew
Overcome InsufficiencyThe Medicare Fee-for-Service 2013 Improper Payment Report shows that insufficient docu-mentation errors account for a significant por-tion of improper payments from the Centers for Medicare & Medicaid Services (CMS), as shown in Table B1.Insufficient documentation may be found when submitted medical documentation is inade-quate to support payment for the billed servic-es, or a specific documentation element required for payment is missing. Other potential prob-lems may be that the medical documents sub-mitted do not contain pertinent patient facts (e.g., patient’s condition, diagnosis, etc.), or the medical documentation is illegible, has no date, is improperly signed, etc. The number one reason for insufficient docu-mentation is a missing signature. If you aren’t auditing 100 percent of your practice notes in all locations, you may not know if this deficiency applies to you. However, I am consistently sur-prised by the number of chart notes I review that lack a legible signature (or any signature at all). Payers and CMS require the medical chart doc-umentation supporting a claim contain a leg-ible and timely signature. For medical review purposes, Medicare requires the author, using a handwritten or a valid electronic signature, to authenticate the services provided and ordered. Regardless of how accurate the coding is, if the document lacks a legible signature, the entire note will be disregarded.
Tip: Auditors will appreciate if you include a signature log listing the typed or printed name of the author associated with initials or an illegible signature. The signature log can be included on the actual page where the initials or illegible signature are used, or in a separate document.
You may ask, “If an auditor notices a note is missing a signature, can I just have the provid-er add it?” The answer is: Probably not. Provid-
AUDI
TING
/COM
PLIA
NCE
To be considered valid for Medicare medical review purposes, an attesta-tion statement must be signed and dated by the author of the medical re-cord entry and must contain sufficient information to identify the patient. CMS provides a sample statement from the Medicare Program Integrity Manual 100-08, Section 3.4.1.1:
I, [print full name of the physician/practitioner], hereby attest that the medical record entry for [date of service] accurately reflects signatures/notations that I made in my capacity as [insert provider credentials, e.g., M.D.] when I treated/diagnosed the above listed Medicare bene-ficiary. I do hereby attest that this information is true, accurate, and complete to the best of my knowledge and I understand that any falsi-fication, omission, or concealment of material fact may subject me to administrative, civil, or criminal liability.
Although this is an acceptable format, CMS is neither requiring nor in-structing providers to use a certain form or format.
SAMPLE
www.aapc.com November 2014 53
Auditors Wish You Knew
ers should not add late signatures to the medi-cal record (beyond the short delay that occurs during the transcription process). If the docu-ment is missing a signature, you must include an attestation statement. If you have a valid sig-nature attestation statement and signature log, completed and provided with the medical re-cords request, auditors will have one less con-cern to audit (see the preceding page for an at-testation statement sample).A note of caution: Auditors will not accept a single attestation to cover several chart notes or a length of time. A generic statement will not suffice. For instance, “I, Dr. X hereby attest that all medical record entries for any patients I’ve ever seen accurately reflect my observations,” would not be accepted, nor inspire confidence.
AWOL Documentation = AWOL PaymentsInsufficient documentation and lack of signa-tures is one thing, but over half the providers I audit have issues with missing medical records. My experience is not unique. For instance, in the breakdown of Medicare Part B billing’s top 20 service types with highest improper pay-ments (Table B1), “Major Procedure Cardio-vascular-Other” clocks in with a 95.5 percent finding related to missing documentation.In Table B3, Part A services of “Clinic OPT” (outpatient therapy) clock in at 44.6 percent missing documentation, and in Table B2, “LSO” (lumbar support orthotics) tops the “DME” (durable medical equipment) category with a 5 percent rate of missing documentation. Woody Allen said, “Eighty percent of success is showing up.” During my 19-year career as an auditor, I’ve realized a similar truth applies to audits: Eighty percent of success is the request-ed records showing up for audit.It’s frustrating for both the provider and the au-ditor when there is a bill for a date of service, but the documentation for that date of ser-
AUDITING/COMPLIANCE
54 Healthcare Business Monthly
Auditors Wish You Knew
vice doesn’t seem to exist. Perhaps such documents end up in an alterna-tive dimension with lost car keys, mis-placed remote con-trol units, and van-ished socks from the dryer? One practice discovered a medical assistant stationed at a counter-high desk to relieve her leg and back pain using a box of chart notes to bolster the height of her footrest. In another situation, a provider was hav-ing difficulty keeping up with paperwork. The charts found their way into his trunk, never to return. How do you know if this is a problem for you? Pick 10 patients, at random, from the last two week’s schedules. Now, go on safari in your practice or facility. Is docu-mentation for all 10 visits accounted for? If not, where are they? Because you’re probably very diligent and aware of the nooks and crannies in your office, the above task probably wasn’t much of a challenge for you; but chart requests from health plans and oth-er providers most likely come to someone else in your practice or facility. Would the average employee know where to find these charts, and would the folks who manage medical records know who to ask if they couldn’t find a chart? What about chart notes from visits six years ago? Are they accessi-ble? If you’ve converted from paper charts to an electronic health record (EHR), or from one EHR to another, would you know how to find (and access) the old records?
Make Records Access a PriorityMany times, finding a missing chart isn’t a priority: The office staff member was busy, or didn’t understand the implications of a missing chart note. Those implications are serious: If the chart note isn’t present, the entire service must be refunded, and some auditors may not give you a second chance to provide missing doc-
umentation — an expensive les-son to learn.
Practices should provide training for medical record staff, and perhaps should require someone in leader-ship to review medical re-cord requests from Medi-care Advantage payers, Medicare contractors, and state/government agencies before a response is sent to
the requestor. However you make it work, ensure all med-
ical record requests are fulfilled completely. If there are missing
records, communicate it to the ap-propriate leadership/compliance per-
sonnel in the practice.
Requested Records Could Be ElsewhereYou may run into trouble when requesting documentation out-
side of the office visit note. If the medical record request seeks “all supporting documentation” of the claims billed, this is auditor-speak for, “You might find some of this elsewhere!” Here’s what this means for you:• If the claims audited are for inpatient services, does your
staff know how to access and recognize a history and physical examination, a daily encounter note, and a bedside procedure note from the facility?
• If the claims audited involved diagnostics, does your record include the visit where the diagnostic was discussed, the physical order of the diagnostic, the results, and the report?
• If the claims audited are for vaccines or injectables, are these logs kept separately from the office visits?
• If the claims audited are for initial office visits or complete physicals, are the patient medical history and review of system questionnaires stored in separate locations, such as scanned document folders?
These are examples of items that may not be contained in a single location, but must be gathered to fully satisfy the record request. If medical records staff do not know coding, they may need train-
AUDI
TING
/COM
PLIA
NCE
www.aapc.com November 2014 55
Auditors Wish You KnewTo discuss this article or topic, go to www.aapc.com
AUDITING/COMPLIANCE
ing to recognize record requests that will require documents from another location or another healthcare entity.
Coding Is Only Part of the BattleIt’s unfortunate when the very best codes have been expertly ap-plied — and perhaps the claim has already been paid — only to undergo an audit that leads to overpayment recovery. By contrast, if all the requested chart notes show up for audit, with a timely, leg-ible signature of the performing professional, the excellent coding you applied is allowed to shine.To avoid the stress of a poor audit outcome, take a peek at your practice’s documentation. A great place to start is the Medicare Claim Review Programs Guide for MR, NCCI Edits, MUEs,
CERT, and Recovery Audit Program (www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/MCRP_Booklet.pdf). This guide can give you pointers for auditing your practice and assist you in addressing documentation concerns, before a regulator addresses them for you.
Lisa Jensen, MHBL, FACMPE, CPC, is the senior manager of External Audit at Providence Health Plans in Beaverton, Oregon. She has a master’s degree in Healthcare Business Lead-ership and is a charter member of the Columbia River local chapter and credentialed since 1996. Jensen also is a member of the Medical Group Managers Association (MGMA) and attained Fellowship status in the American College of Medical Practice Executives in 2008.
It’s unfortunate when the very best codes have been expertly applied — and perhaps the claim has already been paid — only to
undergo an audit that leads to overpayment recovery.
Sophisticated medical record audit software
End-to-end, web-based auditing tools
There is a better way to manage your medical record audits.
Simplified workflow management
Targeted feedback and training modules
Audicy is a new, end-to-end, web-based system that redefines the documentation and coding review process.
Coming in January
For more information call 866-200-4157
Be Prepared: Is your organization compliance ready?
• The US Department of Justice reports $3.8 billion in 2013 settlements bringing total recoveries under False Claims Act since 2009 to over $17 billion
• In first 6 months of Fiscal Year 2014, OIG reported expected recoveries of more than $3.1 billion
- $295 million in audit receivables
- $2.83 billion in investigative receivables including $813.7 million in non-HHS receivables
Don’t become one of these statistics…
7Atlis is a simple to use, complete compliance management solution for a surprisingly affordable fee. It’s about time to meet the compliance solution you’ve been looking for.
Take a tour at 7Atlis.com or contact one of our Compliance Representatives at 1-877-835-2842 to see how we can prepare your organization.
• 2014 OIG Fraud and Abuse Control Program reports:
- Consistent $7.9 to $1 ROI—It pays to audit and investigate—So it will continue
- Exclusions of 1,720 individuals & entities from Federal health care program participation
- 465 criminal & 266 civil actions against individuals for crimes against HHS programs
www.aapc.com November 2014 57
ASK THE LAB ■
Q&A: Mixing Clinical and Financial Data in the Patient Portal
■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
Be Prepared: Is your organization compliance ready?
• The US Department of Justice reports $3.8 billion in 2013 settlements bringing total recoveries under False Claims Act since 2009 to over $17 billion
• In first 6 months of Fiscal Year 2014, OIG reported expected recoveries of more than $3.1 billion
- $295 million in audit receivables
- $2.83 billion in investigative receivables including $813.7 million in non-HHS receivables
Don’t become one of these statistics…
7Atlis is a simple to use, complete compliance management solution for a surprisingly affordable fee. It’s about time to meet the compliance solution you’ve been looking for.
Take a tour at 7Atlis.com or contact one of our Compliance Representatives at 1-877-835-2842 to see how we can prepare your organization.
• 2014 OIG Fraud and Abuse Control Program reports:
- Consistent $7.9 to $1 ROI—It pays to audit and investigate—So it will continue
- Exclusions of 1,720 individuals & entities from Federal health care program participation
- 465 criminal & 266 civil actions against individuals for crimes against HHS programs
By Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO
Be sure finances have no bearing on the clinical basis supporting patient treatment.
Q: Our practice has been communicating with patients through a patient portal, and we have run into a possible legal issue.
Suppose a patient sends a message to the practice through the portal re-garding a financial concern. The billing department (where I work) replies through the portal. Any message or question sent by the patient to the practice, or vice versa, is called a “patient case.” All patient cas-es are automatically saved into the chart, unless manually deleted. Our concern is that financial records are supposed to be separate from the medical record. Our practice manager has addressed this with the electronic health record vendor, but the vendor is unsure of what can be done to prevent the financial records from going into the med-ical record. Some of the “patient cases” have been manually deleted, but that raises the question, “Why are things being deleted from the chart?” What do you advise?
A: Based on the limited information provided, any obliga-tion to retain patient communications regarding finan-
cial issues would most likely arise through the provider’s state li-censure regulations. HIPAA is largely irrelevant to the premise of your question because it creates no duty to create health informa-tion. Once created, however, financial records/communications pertaining to patient care are included within the definition of health information, individually identifiable health information, and protected health information (see 45 C.F.R. §160.103), and are subject to the rule. There are also requirements under the se-
curity rule to preserve electronically stored heath information af-ter it has been created.Ultimately, look for a way to keep the financial communications separate from the clinical data in the patient chart, especially since they likely have no relevance to the necessity of provided servic-es. That does not mean I advocate deleting those records. Per-haps your vendor can allow you to tag communications through the portal in a way your system recognizes them as “admin” or fi-nancial records, thereby triggering automatic storage in a sepa-rate part of the chart. This would preclude improper disclosure during routine printing of clinical notations. When such segrega-tion is not possible and you are asked to provide records to a health plan, you’ll need to determine if the financial records are with-in the scope of those records necessary to serve the purpose of the carrier’s request. If not, you must prevent disclosure of those re-cords consistent with your obligations under the minimum neces-sary disclosure rule. Because such communications are not usually relevant to a carrier’s pre- and/or post-payment coverage analysis, separate storage would prevent accidental disclosure.I am concerned about your ability to delete records in your system. Be certain to only use this function consistent with your state li-censure and HIPAA record retention obligations. Where a dele-tion is permissible, it’s also good practice to keep a log of what was deleted, and why.
Michael D. Miscoe, JD, CPC, CASCC, CUC, CCPC, CPCO, serves on the AAPC’s Nation-al Advisory Board (NAB) and Legal Advisory Board (LAB), and also is AAPC Ethics Com-mittee chair. He has over 20 years of experience in healthcare coding and over 16years as a compliance expert, forensic coding expert, and consultant. He has provided expert analysis and testimony on coding and compliance issues in civil and criminal cases and his law practice concentrates on representing healthcare providers in post-payment au-
dits and with responding to HIPAA OCR issues. He speaks on a national level, and is published in national publications on a variety of coding, compliance, and health law topics. He is a member of the Johnstown, Pennsylvania local chapter.
■ Coding/Billing ■ Practice Management ■ Auditing/Compliance
Building a HIPAA ToolkitBy Stacy Harper, JD, MHSA, CPC
As of June 2013, the Office for Civil Rights (OCR) has an-nounced more than $10 million in penalties and settlements re-
lated to alleged HIPAA violations. OCR—responsible for enforc-ing HIPAA regulations—had more than 500 investigations still open at the end of 2013, all based on breach notifications alone. With the expanded enforcement under the omnibus HIPAA regu-lations that became effective September 2013, investigations, pen-alties, and settlements are expected to rise. Although the large settlement agreements announced by OCR attract attention, more significant are the thousands of investi-gations resolved by OCR where a penalty was not assessed be-cause the covered entity was found to have: 1) addressed the un-derlying cause of the breach or violation; and 2) mitigated any po-tential harm to affected individuals. Even when OCR finds that a covered entity or business associate was non-compliant with HIPAA, the investigation may be concluded through voluntary compliance, rather than financial penalty. There are a few proac-tive steps a covered entity or business associate (you) can take to improve your ability to demonstrate voluntary compliance in an investigation.
1. Prevention Goes a Long WayIt may seem simplistic to say that you can manage the risk of a breach by complying with obligations under HIPAA; however, robust compliance plans not only reduce the risk of a breach, they position your organization to respond if one arises.When a breach occurs, it does not necessarily mean you will be subject to penalties. The majority of settlement agreements an-nounced by OCR involve non-compliance beyond the breach it-self. Many of these organizations faced allegations that risk assess-ments were not performed; employees were not trained; policies and procedures were ineffective, insufficient, or missing; encryp-tion was not implemented; and/or safeguards were incomplete. In
the event a breach occurs despite compliance efforts, your com-pliance program can demonstrate voluntary compliance with the majority of HIPAA requirements, and narrow the scope of the in-vestigation to the implication of the breach itself.
2. Identify Potential Breaches in a Timely MannerOf the 101 entities that were audited for breach notification com-pliance in 2013, 31 were found to have an element of non-compli-ance related to the notification rule. Of the 31 entities with defi-ciencies, 23 had findings regarding the timeliness of notification.The breach notification rule requires that you provide necessary notification without unreasonable delay, and in no case later than 60 calendar days from the date a breach is known to the entity, or would have been known through exercise of reasonable diligence. By incorporating the “would have been known” component in the timing requirements for breach notification, HIPAA impos-es an obligation for you to implement effective policies for detect-ing potential breaches. Timely identification is accomplished pri-marily through active monitoring, mandatory reporting, and pe-riodic audits.
3. Have a Breach Response PlanBreach discovery triggers a period of heightened scrutiny for your organization. Even when notification is provided within the 60-day period, a primary question plaguing most organizations is, “What took so long?” The resolution is to improve your ability to respond appropriately, which you can do by developing a plan for the time of crisis. A breach response plan or policy usually involves describing the identification and investigation process, sending notification re-quirements applicable to the organization, and describing expec-tations to mitigate harm and prevent future incidents. The plan
Part 1: Demonstrate voluntary compliance in five preventive steps.
To discuss this article or topic, go to www.aapc.com
lays out the structure. Additionally, con-sider how your plan will be implemented:• Who will comprise the internal
team to manage the breach response?
• At what point is legal counsel involved?
• What insurance, forensics, credit monitoring, or other consultants does your organization have available?
Knowing the answers to these questions in ad-vance of a breach enables a timely, effective response.
4. Protect Individuals and Mitigate HarmThe fifth most common issue subject to corrective action by OCR in 2011, 2012, and 2013 was mitigation. Actual implemented mit-igation strategies are highly dependent on the facts of a particu-lar breach. For instance, a misdirected fax may focus on confin-ing unauthorized disclosure, such as recovery or destruction of the document, or execution of confidentiality agreements with the unauthorized recipient. A breach related to a lost, unencrypt-ed laptop, on the other hand, cannot be easily confined, and miti-gation will likely focus on protecting affected individuals against potential harm, beginning with patient notification and identi-ty theft and credit monitoring protection. Identifying potential mitigation strategies to incorporate in your breach response plan provides your team with the necessary tools to respond to a breach appropriately.
5. Learn From Your MistakesThe most important component of a breach response, and fre-quently the focus of a related investigation, is the steps an orga-
nization takes after the dust settles. A re-view of the OCR settlement agreements includes corrective action plans that de-tail your expectations to prevent a re-peat breach.In the event of a breach, the facts, vul-nerabilities, and other information
gathered during the internal investiga-tion process should be factored into your
risk analysis and risk management process-es. Every breach or similar violation presents an
opportunity for your organization to grow and to improve information protection. Ask yourself:
• Have the vulnerabilities that allowed the breach been resolved?
• Have applicable workforce members been sanctioned, terminated, or re-trained?
• Were new technologies or other safeguards implemented?• Were policies and procedures revised?• Did you document or summarize what steps were taken in
response?Demonstrate an appropriate response to the situation and your organization’s commitment to comprehensive HIPAA compli-ance by implementing these preventive measures and document-ing them.
Stacy Harper, JD, MHSA, CPC, is healthcare attorney with Lathrop & Gage, LLP. She serves on the National Advisory Board for AAPC. Harper works with healthcare providers around the country to navigate regulatory requirements such as HIPAA, data privacy and security, Stark law, anti-kickback, state licensure, and Medicare conditions of payment and participation. She is a member of the Kansas City, Missouri local chapter.
When a breach occurs, it does not necessarily mean you will be subject to penalties.
What’s in a Resume? You!Avoid the discard pile with a resume that lands you an interview.
To change careers or advance your position, you need a resume that stands out from the rest. A well written and factual resume
is a good start, but you’ll need to do more to warrant an interview in this highly competitive job market. How do you develop and write a resume to impress? Here are a few tips that I share with stu-dents in my Certified Professional Coder (CPC®) classes.
Prepare by ResearchingWriting a resume used to be a lot harder. Resources were limit-ed and finding a dependable, qualified resume writer was a chal-lenge. That’s all changed. Now, you can find numerous, free re-sources online, including interactive online templates that allow you to fill in your information, and easily print, email, or fax your resume to prospective employers. Confirm that the company to which you want to apply is a good fit for you by visiting their website and investigating other sourc-es. Who works there? What is the company’s philosophy? Famil-iarize yourself with their product or specialty, too. This research will demonstrate your interest in the company, and help you feel comfortable with your decision to join their team. It will also help you to better tailor your presentation.
Tailor Your Resume to Suit the JobAs you compose your resume, review the job description for the position you are applying for. What are the skills and qualifica-tions the employer requires? Tailor your resume to the job. If you
are applying to multiple companies, customize each resume to fit the various job descriptions. You don’t want to submit a resume de-fining qualifications of an accounts receivable position when the employer is looking to hire a receptionist.Use bold and large fonts to highlight the important items you want to stand out. Be sure your credentials are listed with your name (e.g., Sandy Smith, CPC). Put your skills and education in the fore-front (e.g., Anatomy/Physiology, billing, coding educa-tion, etc.). If the employer has to struggle to see what’s in your re-sume, they may overlook this important information, and you will find yourself in the discard pile instead of the “to be called” file. List your skills and qualifications. Keep them directed to the job description. As employers resort to electronic scanning of re-sumes, you stand a better chance of being called when you use ac-tion verbs, sometimes called “buzz words,” detailing your accom-plishments. “Maintained,” “developed,” “trained,” etc., should be included in describing your professional abilities. Showcase your greatest strengths first. Everything we do or have achieved in life contributes to our expe-rience. Always account for any time when you weren’t gainfully employed. For example:• Boy Scout or Girl Scout leader• Parent-teacher organization activities, such as decorator
for special projects, project leader, treasurer, secretary, fundraising, etc.
• Band booster parent: cook, inventory control, handling money, customer service
• Stay-at-home mom: multi-tasking, budgeting the family resources, planning vacations, etc.
• General volunteer activities and community service• Achievements and awards• Education • Work experience and tasks performed
Be sure to highlight accomplishments, such as “managed accounts payable, recovered a $10,000 mistake,” “supervised 11 employ-ees,” or “responsible for the accuracy of daily deposits, and stream-lined procedure, which saved countless man hours.” Use numbers and symbols to describe your skills, such as “Controlled the ag-ing report of $150K to 40 days.” This will make your accomplish-ments stand out for the employer to see.Whatever you do, always be truthful. And don’t forget: You are selling yourself to the employer. The employer is interested in what you can do for the business. Be clear on how you will be an asset to the employer, versus what you are seeking to fulfill your needs.
Don’t Surprise Your ReferencesIt’s a good idea to list your references on the resume, versus stating, “References available on request.” By including references, you’re showing your prospective employer you’re willing to do as much work for them as possible to get an interview, and to attain employ-ment. Be sure to contact your references and ask if you can name them on your resume.
Be Critical and Ask for OpinionsWhen developing a resume, you must be your own critic. As you proofread your completed resume, ask:• Did you identify yourself and provide contact information?• Did you organize your resume so it’s easily understood?
• Did you highlight your skills?• Did you illustrate specific qualifications pertaining to the
position you are seeking?• Did you describe your professional experiences?• Would you read past the first line?• Will you stand out from all the other potential candidates?• Based on the resume in front of you, would you hire you?
Take the time to have someone else (who can be objective) read your final draft. Although you usually know what you want to say, you may fail to say it. Another set of eyes will help you see the mer-its of your resume more clearly. Tip: Don’t depend on your word processing application’s spelling and grammar functions. Even if a word is spelled correctly, it may not be used appropriately. In fact, you might want to turn off the auto correction feature.
Include a Cover LetterA cover letter allows you to introduce yourself more informally. Start out on the right foot by addressing the letter to the person
Take the time to have someone else (who can be objective) read your final draft. Although you usually know what you
who will be reviewing your resume. “To Whom It May Concern,” says, “I don’t care enough about this job
to look up the name of the human resources director.” When you’ve got the person’s attention, use this tool to convince him or her you’re the best candidate for the job, citing tangible data as the basis of your claim. Make sure to provide the most accurate contact information, along with the best time and day to reach you easily. You don’t want your prospective employer to have to work at getting in touch with you. You may only get one chance at getting an appointment for an interview.
Never Forget to Say “Thank You”A resume is your one-of-a-kind marketing tool. Communicate to the fullest what you can do for the employer, and “knock their socks off!” Lastly, right after your initial interview, be sure to show your gratitude by sending a thank you note. You’ll soon have a lot to be thankful for!
Sharon J. Oliver, CPC, CPMA, CPC-I, is the senior in-patient coordinator for ETSU Phy-sicians and Associates, Quillen College of Medicine Department of Cardiology. She is a 30-year medical professional, a PMCC, ICD-10-CM/PCS instructor, and serves on the 2013-2016 AAPC Chapter Association board of directors. Oliver owns Medical Coding and Con-sultants, and is a member of the Johnson City, Tennessee, local chapter.
Lastly, right after your initial interview, be sure to show your gratitude by sending a thank you note. You’ll soon have a lot to be thankful for!
America’s PremierHealthcare Job Portal
Search over half a million healthcare jobs.
Visit careerhealth.com to create your free profile and find your next career.
www.aapc.com November 2014 63
NEWLY CREDENTIALED MEMBERSAbinaya Ponpandian, CPC
Alesia Irby, CPC-H
Alyssa Aschbrenner, CPC
Amanda J Hernandez, CPC, CPC-H
Amit Nagpal, CPC, CPC-H, CPC-P
Angie Knight, CPC
Anna Huffman, CPC
Ashley D’Amore Ellis, CPC
Ashok Mani, CPC
Ayesha Hampton, CPC, CPC-H
Brandy Shaw, CPC
Brenda Ritchie, CPC
Briana Primavera, CPC, CPC-H
Carla Tierney, CPC, CPC-P
Carly Arroyo, CPC
Carol Bryant, CPC
Carol Caravelli, CPC
Carol Drake, CPC-H
Carol Motley, CPC
Cassandra Juarez, CPC
Charity Green, CPC
Charnesha Mack, CPC, CASCC
Cherie Fieri, CPC, CPC-H
Christian Morris, CPC
Christina Eskins Davis, CPC
Christine Staples, CPC
Cindy Helton, CPC
Cindy Kennedy, CPC, CPC-H, CPMA
Cindy M Sanchez, CPC
Claire Herrera Melhorn, CPC, CPC-H
Courtney Thrift, CPC
Daniele DeGrandis-Kneer, CPC
Danielle Holt, CPC
Darlene Patterson, CPC
Debbie Greene, CPC
Debbie McDonald, CPC
Deborah Wilmoth, CPC
Dedra King, CPC, CPC-H
Deepa Kangalamoorthy, CPC, CPC-H
Delaine Fast, CPC
Denice Johnson, CPC
Denise Lynn Brown, CPC
Dr MadhuSudhanRao Kotha, CPC, CPC-H, CPC-P, CEDC
Edith Clark, CPC
Eric Hoang Lam, CPC
Eugene Kwak, CPC-P
Eva Clark, CPC
Farrah Dray, CPC
Gina L Clark, CPC
Gloria Jemery, CPC
Gowri T, CPC
Gretchen Hill, CPC
Gwen Holston, CPC
Haley Sutton, CPC, CPC-H
Heather Davis, CPC, CPC-H
Heather Hughes, CPC
Jackie Vasquez, CPC
Jacqueline Willett, CPC-H
Jaya Sudha, CPC
Jennifer Bolds, CPC
Jennifer Connolly, CPC
Jennifer D Thomason, CPC-H
Jennifer Helminiak, CPC
Jennifer Wright-Davis, CPC
Jerri Hampton, CPC, CPC-H
Jerry Joseph, CPC
Jessica Harless, CPC
Jessica Michele Rose, CPC
Jodi Pendergast, CPC
Julia Keenen, CPC
June Witt, CPC
Juveria Kareem, CPC
Kalicia M Hopson, CPC
Kanimozhi Parimalan, CPC
Karen Seibert, CPC
Karla Samaniego, CPC
Kathleen M Skolnick, CPC, CPC-H, CPCO, CPB, CPMA, CPPM, CPC-I
Kathleen Shapiro, CPC, CPC-H
Kathryn Siedel, CPC
Katie Pinkerton, CPC-H
Kay L Carroll, CPC, CPC-H
Kevin Timp, CPC-H
Kim Turner, CPC
Kim V Rachow, CPC, CPC-H
Kimberly L Orwig, CPC
Laura Kaminski, CPC
Laurin Grubbs, CPC
Leilani Edwards, CPC
Lena Marie Roberts, CPC
Lenore Reed, CPC
Lesa F Shields, CPC
Linda Butler, CPC
Lori Potter, CPC
Lucianne Van Vonderen, CPC
Malana Skolnick, CPC, CPC-H, CPCO, CPMA
Martha Swem Brady, CPC
Marty Lauridsen, CPC
Mary B Bonkoski, CPC
Mary Gilbreath, CPC
Mary Kulig, CPC
May Lamour, CPC
Megan Paredes, CPC
Melanie Garcia, CPC
Melisa Sallad, CPC
Melissa Pizor, CPC, CPC-H, CPCO, CPMA, CPRC
Molly F Edgington, CPC
Muthu Kumaran, CPC-H
Naomi E Clayton, CPC
Nicole Srutowski, CPC
Nirai Pandiyan Aathimoola Narayana-samy, CPC
P Darlene Payton, CPC, CPC-H
Paige Segovia, CPC, CPC-H
Pamela Ediger, CPC
Pamela L Lutze, CPC
Patti Haines, CPC
Paulette D Simmons, CPC, CPC-H
Pola L Wendt, CPC, CPC-H
Rachel Foster, CPC
Raisa Chudnovskaya, CPC
Rajeshwari Rajendran, CPC, CPC-H
Rasa Adomaityte, CPC, CPC-H
Rebecca Horton, CPC
Reneih Aziz, CPC, CPC-H
Renuka Purnima Toppo, CPC-H
Rhonda Climes, CPC
Richard Glen Wendorf, CPC, CPC-H
Rita Mauldin, CPC
Robyn Greenberg, CPC
Ronda Simmons, CPC
Sandra Jahr, CPC
Sandra West, CPC
Shajan Vp, CPC
Shannon Barker, CPC
Shannon Garza, CPC
Shannon Kathleen Dykhouse, CPC
Sharath Chandra, CPC, CPC-H
Sharon Boggs, CPC
Sharon Diane Blevins, CPC, CPC-H, CIMC
Shauna Bair, CPC
Shauna Stephens, CPC
Sheria Smith, CPC, CPC-H, CPMA
Sherry Pennington, CPC
Shirley DeHardt, CPC, CPMA
Shiva Darshan Kota, CPC, CPC-H
Sirisha Bommireddipali, CPC, CPC-H
Sithu Anirudhan, CPC-H
Soniya Kasirajan, CPC
Stacy Loftis, CPC
Stacy Sparks, CPC
Stephanie Garst, CPC, CPC-H
Stephanie Killea, CPC
Sujata Mital, CPC
Sujaya Ghosh, CPC
Susan Hubbard, CPC
Susan L McAbee, CPC, CPC-H, CPMA
Susan Lea Stovall, CPC, CPC-H
Susan Mercer, CPC
Susan Sifrit, CPC
Tabitha Lynn Barone, CPC
Terri Chambers, CPC
Theresa Gordon, CPC-P
Thulasi Dharani, CPC
Traci Jurgensen, CPC
Tracy A Collins, RN, CPC
Velda Rivard, CPC
Vijaya Babu, CPC
Wendy May, CPC
Yandi Garcia, CPC
Yolanda Thomas, CPC
ApprenticeApprenticeApprenticeAaron Keen, CPC-A
Abby Fowler, CPC-A, CPB
Abhijit Padihari, CPC-A
Aby Thankachan, CPC-A
Adrienne Floyd, CPC-A
Aileen Del Rosario, CPC-H-A
Aimee Alexander, CPC-A
Alicia Chavis, CPC-A
Alicia Johnson, CPC-A
Alison Mitchell, CPC-A
Alka Tiwari, CPC-A
Alli Arizmendez, CPC-A
Allison Malone, CPC-A
Amanda Bedeaux, CPC-A
Amanda Colby Czysz, CPC-A
Amanda Lewis, CPC-A
Amanda Lynn Whetzel, CPC-A
Amanda Peacock, CPC-H-A
Amanda Sisco, CPC-A
Amber Pietrzykowski, CPC-A
Amie Walsh, CPC-A
Amy Clemons, CPC-H-A
Amy Desserich, CPC-A
Amy Fenker, CPC-A
Ana Vazquez, CPC-A
Anand K, CPC-A
Angel Skoglund, CPC-A, CPC-H-A
Angel Smith, CPC-A
Angela Cantwell, CPC-A
Angela Cochrane, CPC-A
Angela Cromwell, CPC-A, CPC-H-A
Angela Moore, CPC-H-A
Angelic Oliveras, CPC-A
Angelina Duran, CPC-A
Angelo Gonzales Mariano, CPC-A
Anija Krisnakumar, CPC-A
Anil Barapati, CPC-H-A
Animesh Kumar, CPC-A
Ankita Sanjay Palande, CPC-A
Ann Bray, CPC-A
Ann Keiko Johiro, CPC-A
Anna Milewski, CPC-A
Annabelle Kimberly Santos, CPC-A
Anne Katrize Velasco Carlon, CPC-A
Annette Thompson, CPC-A
AnnMarie Maher, CPC-H-A
Anuja Shetkar, CPC-A
Any Laura Acuna, CPC-A
April Fields, CPC-A
April Poole, CPC-A
April Varble, CPC-A
April Wu, CPC-A
Arby Deluao, CPC-H-A
Arfat Shaikh, CPC-A
Arlene Ballesteros Inosanto, CPC-A
Arnel Pacleb Ganeb, CPC-A
Arun Kumar Duraisamy, CPC-A
Ashley Coleman, CPC-A
Ashley DeVaughn, CPC-A
Ashley Evenson, CPC-A
Ashley Hummer, CPC-A
Ashwini More, CPC-A
Audrianna Copeland, CPC-A
Ayehu Berhan Gizaw, CPC-H-A
Balannagari Siva Prasad, CPC-H-A
Balkrishna Shivaji Survase, CPC-A
Bama Ganesan, CPC-H-A
Barbara Sucha, CPC-A
Bethany Sibert, CPC-A
Betrice Dela Cruz, CPC-H-A
Betty Kuan, CPC-H-A
Beverly Miller, CPC-A
Bhagish B, CPC-A
Bhagyashree Bharambe, CPC-A
Bhavin Kumar Vadodaria, CPC-A
Bhoopal Patoori, CPC-H-A
Bhuvaneshwari C, CPC-A
Bianca Ferguson-Brown, CPC-A
Bipin Bhosale, CPC-A
Blessing Sivaraj, CPC-A
Brenda Joy Noullet, CPC-A
Brenda L Coleman, CPC-A
Briana Ickowicz, CPC-A
Bridget McCarthy, CPC-A
Bryce Wangen, CPC-A
Caitlin Capaldi, CPC-A
Camie Andrews, CPC-A
Candy Falcao, CPC-A
Candy R Marlene (Candy) R Pate, CPC-A
Caren Goss, CPC-A
Carla Effron, CPC-A
Carla Ross, CPC-A
Carmen Santana, CPC-A
Carol Chestnut Buonadonna, CPC-A
Carolyn Esham, CPC-H-A
Carrie Atkinson, CPC-A
Catherine Lerpido Obana, CPC-A
Catrina Hammond, CPC-A
Celica Ogad Salen, CPC-H-A
Charina Tiongco, CPC-A
Charli Engle, CPC-A
Charmaigne Tapar, CPC-H-A
Chasity Elliott, CPC-A
Cheryl Metzger, CPC-A
Chetan Dhadge, CPC-A
Chetan Parmar, CPC-A
Chithra Rangaswamy, CPC-H-A
Chris Fassinger, CPC-A
Christian Sales Mendoza, CPC-A
Christina Gilliam, CPC-A
Christina Marie Crawford, CPC-H-A
Christinal Shobana Priya F, CPC-A
Christine Coppock, CPC-A
Christine Dianne Gordon, CPC-A
Christine Wolff, CPC-A
Ciera Richardson, CPC-A
Cindy Larson, CPC-A
Clairissa Gillespie, CPC-A
Clariza Ramos Escueta, CPC-A
Cody Creekmore, CPC-H-A
Connie Pendley, CPC-A
Connie Akins, CPC-A
Crystal McCarter, CPC-A
Cynthia Welch, CPC-A
Daisy Evanjalin A, CPC-A
Damian Suarez, CPC-A
Damyantee Meher, CPC-A
Daniel Stephen Rodriguez, CPC-A
D’Arci Johnson, CPC-A
Darcie Gessner, CPC-A
Darryll Ruben Martinez de Castro, CPC-A
Darwin Gingco, CPC-H-A
Davetta Peterson, CPC-A
David Wolf, CPC-A
Dawn Kurelko, CPC-A
Dawn M Hall, CPC-A
Dawn Wittke CCS-P, CPC-A, CPMA
Dawne Graf, CPC-A
Dayna Kakes, CPC-A
Deanna Barber, CPC-A
Deanna Jo Chandler, CPC-A
Deanne Harris, CPC-A
Debra Gross, CPC-A
Debra Lynne Curry, CPC-A
Debra Segedy, CPC-A
Deepa Shenoy, CPC-A
Deepa Sukumar, CPC-A
Della Lloyd, CPC-A
Dena Harte, CPC-A
Denise Fralick, CPC-A
Denise Greer, CPC-A
Denise Parker, CPC-H-A
Dennis Sohn, CPC-A
Desteracy Wright, CPC-A
Devi Arunya, CPC-A
Devi Solai, CPC-A
64 Healthcare Business Monthly
NEWLY CREDENTIALED MEMBERSDheeraj Sonawane, CPC-A
Diana D’Arrigo, CPC-A
Diane Ringling, CPC-A
Dianna Dorman, CPC-A
Dipti Deshmukh, CPC-A
Divya Haridas, CPC-H-A
Divya Nair, CPC-A
Domingo Nunez, CPC-A
Donald W. Harrison, CPC-A
Donna D Robinson, CPC-A
Donna Felder, CPC-A
Donna Plencner, CPC-A
Donna-Faye Nator Mainit, CPC-A
Dr. Pallavi Yenpure, CPC-A
Dr. Vaishali Dhore, CPC-A
Dulce Armas, CPC-A
Durga P, CPC-H-A
Dusty Groff, CPC-P-A
Edward Weisman, CPC-A
Elaine Poynter, CPC-A
Elaine Regan, CPC-A
Elisabeth Louise Henry, CPC-A
Elizabeth Curbow, CPC-A
Elizabeth Garriques, CPC-A
Elizabeth Haight, CPC-A
Elizabeth Kerr, CPC-A
Elizabeth Miller, CPC-A
Emilibeth Labrador Pantig, CPC-A
Emily Osta, CPC-A
Emmie Yee Leopoldo, CPC-A
Erica Segura, CPC-A
Erik Chang, CPC-A
Erika Frances Cahilog Ronquillo, CPC-A
Esther Chiu Yee, CPC-A
Evangelina B Steinbrenner, CPC-A
Evelyn Guerra, CPC-A
F Queen Helen Pramila, CPC-A
Fania Rosario, CPC-A
Firoz Khalife, CPC-A
Francis Valeriano Lacandola Quejano, CPC-A
Gajula Divya, CPC-A
Gale Ann Tobin, CPC-A
Gayatri Annaldas, CPC-A
Gayatri Sheth, CPC-A
Geetanjali Pawar, CPC-A
Geetha T, CPC-A
Georgia Marcum, CPC-A
Glenda Mattonen, CPC-A
Gopinath Selvarasu, CPC-A
Grace Irons, CPC-A
Gracielle Irene Guerrero Alejandro, CPC-A
Gregory Nenninger, CPC-A
Gwenda Knight, CPC-A
Haidee Litz Concepcion Baccay, CPC-A
Heather Sweat, CPC-A
Hemant Keval Khairnar, CPC-A
Hillary Moore, CPC-A
Himanshu Shekhar Rout, CPC-A
Ignacio Garcia, CPC-A
Ilam Bharathi, CPC-A
Imelda P Luft, CPC-A
Ina Kreps, CPC-A
Indira G, CPC-H-A
Jackie Lynn Banks, CPC-A
Jacqueline Sabella, CPC-H-A
Jagadish Kumar Anam, CPC-H-A
James Erwin Leones, CPC-A
James Murphy, CPC-H-A
James White Kulandai Raj, CPC-H-A
Janelle Howard, CPC-A
Janet Fearer, CPC-A, CPC-H-A
Janna Vice, CPC-A
Jasmine Jordan, CPC-A
Jayaprasad G Krishnaiah, CPC-A
Jay-jay Papina, CPC-H-A
Jayme Lopez, CPC-A
Jean May, CPC-A
Jeanette Lindquist, CPC-A
Jene’a Wilson, CPC-A
Jennie Reaume, CPC-A
Jennifer Bakkum, CPC-A
Jennifer Critchlow, CPC-A
Jennifer Fish, CPC-A
Jennifer L David, CPC-A
Jennifer Nelson, CPC-A
Jennifer Pryer, CPC-A
Jennifer Rosal Retzlaff Pinero, CPC-A
Jennifer Rose Wake, CPC-H-A
Jennifer Whittier, CPC-A
Jerin Zachariah, CPC-A
Jillian Jeffers, CPC-A
Jini Johny, CPC-A
Joan Wood, CPC-A
JoAnn Gregg, CPC-A
Joanna Birnbaum, CPC-A
Jocelyn Budzynski, CPC-A
Joe Morton, CPC-H-A
Joelene Boiano, CPC-A
John Edward Brejente, CPC-A
John Lorenz Bautista, CPC-H-A
John Martin, CPC-A
John Methgen, CPC-A
Jojo Dingal Garcia, CPC-A
Jonel Querrer, CPC-A
Jordan Karlie Wilson, CPC-A
Josha Krista Ventura Hilahan, CPC-A
Jothi Prakash R, CPC-A
Jothy A, CPC-A
Joyce Miller, CPC-A
Judy Roaden, CPC-A
Julfic Jubairali, CPC-A
Julia Pepe, CPC-A, CPC-H-A
Juliana Khubeis, CPC-A
Julie Kerstner, CPC-A
Julie Saenz, CPC-A
Julie Sewell, CPC-H-A
Juyoung Kim, CPC-A
Jyotsna Ugale, CPC-A
Kalaiarasi S, CPC-A
Kalaiselvi Periasamy, CPC-H-A
Kalaivani Dilli, CPC-A
Kanchan Pawar, CPC-A
Kara Jo Spence Dean, CPC-A
Kara Schwab, CPC-A
Karen Mercer, CPC-A
Karen Shell, CPC-A
Kassie Hefty, CPC-A
Katherine Faulkner, CPC-A
Katherine Jane Villete Beso, CPC-A
Kathleen LaShell, CPC-A
Kathleen Wilcox, CPC-A
Kathryn A Loose, CPC-A
Kathryne Mary Smith, CPC-A
Kathy Sherrill, CPC-A
Katii Sawyer, CPC-A
Kaushikrajan Manickavasagam, CPC-H-A
Kealia Huntley, CPC-A
Keertika Krishnamurthy, CPC-A
Kelley Mcandrews, CPC-A
Kelli Mckeown, CPC-A
Kelly Dockery, CPC-A
Kenda Chandler, CPC-A
Kenneth Lin, CPC-H-A
Kerry Raab, CPC-A
Ketki Kailas Ambavale, CPC-A
Khanh Thuy Vu, CPC-A
Kimberlee Talaga, CPC-A
Kimberly Crystal Lique, CPC-A
Kimberly McNamee, CPC-H-A
Kiran Pavale, CPC-A
Kirthiha Ganesan, CPC-H-A
Kolleen Herlong, CPC-A
Krishna G Vprm, CPC-H-A
Kristi Smith, CPC-A
Kristine Ann Bury, CPC-A
Kristine Graves, CPC-A
Kristine Taylor, CPC-H-A
Krunalkumar Patel, CPC-A
Kuldeep Keshav Gaikwad, CPC-A
Kylie Tantuco, CPC-H-A
Laida I Solá Suárez, CPC-A
Laura Ann Southard, CPC-A
Laura Boggs, CPC-A
Laura C Greubel, CPC-A
Laura Elizabeth Rogalsky, CPC-A
Laura Skarzynski, CPC-A
Laurel Wilcox, CPC-A
Lauren Adams, CPC-A
Lauren Park, CPC-A
Leandro Quiros, CPC-A
LeeAnn Roberge, CPC-A
Leona Bolling, CPC-A
Linda Kleinschmidt, CPC-H-A
Linda Sue Erdmann, CPC-A
Lindsay Windsbrooke Haines, CPC-A
Lisa Boyer, CPC-A
Lisa Depriest, CPC-A
Lisa Hopkins, CPC-A
Lisa Pickens, CPC-A
Lisa Selby, CPC-A
Lisa Streich, CPC-A
Lori Barger, CPC-A
Lori Hodges, CPC-A
Lori Mucha, CPC-A
Lori Smith, CPC-A
Lorren Stacy, CPC-A
Lynda Staffieri, CPC-A
Maela Toribio, CPC-A
Magda Elmoneim, CPC-A
Mahesh Dattatraya Shinde, CPC-A
Mahima Mathew, CPC-A
Malgorzata Sciesinska, CPC-A
Manikandan Ravi, CPC-A
Manimegalai Perumal, CPC-A
Manjunatha Reddy K, CPC-A
Manoj Kumar Ramagiri, CPC-H-A
Manuel Jr Goyena, CPC-H-A
Marampelli Govardhan, CPC-A
Maria E Torres, CPC-A
Maria Edessa Bautista, CPC-A
Maria Pilar Rivera, CPC-A
Maria Sowmya Paul, CPC-A
Maria Villegas, CPC-A
Mariam Mirza, CPC-A
Marissa R Cartagena, CPC-A
Marissa Reyes, CPC-A
Marites Baja Salpid, CPC-A
Mark Crowley, CPC-A
Mark Russel De Leon Catayong, CPC-A
Marla Brown, CPC-A
Marveric Ortiz, CPC-H-A
Mary Anderson, CPC-A
Mary Anitta Varghese, CPC-A
Mary Antonette Elcarte, CPC-A
Mary Brishilla Arokia Samy, CPC-A
Mary Ellen Hawf, CPC-A
Mary Ferrando, CPC-A
Mary Gilbert, CPC-A
Mary Johnson, CPC-A
Mary Ruth Rae Rivera, CPC-H-A
Mary Scott, CPC-A
Mary V Porter, CPC-A
Maureen Federice, CPC-A
Mechelle Baldridge, CPC-A
Megan C McDonald, CPC-A
Megan Huckaby, CPC-A
Megan Kollmansberger, CPC-A
Megan Slenker, CPC-A
Meily Nodal, CPC-A
Melissa Corpuz Rodulfo, CPC-A
Melissa De Graff, CPC-A
Melissa Marquez, CPC-A
Melissa Shank, CPC-A
Merlin Mathew, CPC-H-A
Merri Kaye Marcus, CPC-A
Mhildred dela Vega Molina, CPC-A
Michaelle Waters, CPC-A
Michele Davis, CPC-A
Michele Wierman, CPC-A
Michelle Lohr, CPC-A
Michelle Rene Boening, CPC-A
Mickie Baca, CPC-A
Miguel Teneza, CPC-H-A
Mike Grebner, CPC-A
Milan Mathew, CPC-A
Miranda Kyle, CPC-A
Missy Meulemans, CPC-A
Mithun Manas, CPC-A
Mohamedali K, CPC-A
Monica Maurice, CPC-A
Mukund Jawale, CPC-A
Nagasilpa Bachu, CPC-A
Nancy Ellen Depase, CPC-A
Nancy Forsberg, CPC-A
Narendra Prabhakar R, CPC-A
Narmada Mary, CPC-A
Natalie Paprocki, CPC-A
Natalie Richardson, CPC-A
Naveena LakshmiK, CPC-A
Navya Akinapally, CPC-A
Neha Kulkarni, CPC-A
Nick Tomko, CPC-A
Nicole Calcanes, CPC-A
Nicole Graveen, CPC-A, CPB
Nikki Earll, CPC-A
Nimisha P Thampi, CPC-A
Niraj Kumar Singh, CPC-A
Nisha Leelamony, CPC-A
Nishat Iqbal, CPC-A
Nithya Sundararajan, CPC-H-A
Nivin K V, CPC-A
Niyati M Gurjar, CPC-A
Ola Odewole, CPC-A
Olivia Nicole Mount, CPC-A
Omar Tristan Diego, CPC-A
Padmini Sharma, CPC-A
Page Kristine Murray, CPC-A
Pallavi Acharya, CPC-A
Pamela Crose, CPC-A
Pamela Memita, CPC-H-A
Parimala Kavala, CPC-A
Patricia Yoder, CPC-A
Patsy A Rocha, CPC-A
Paula Davis, CPC-A
Peggy Navin, CPC-A
Phyllis Ritchie, CPC-A
Poornima Nekkanti, CPC-A
Prachi Suresh Raul, CPC-A
Prajakta Nikam, CPC-A
Prakash Salimath, CPC-A
Prasanthi Maramreddy, CPC-A
Praveen Pandirla, CPC-H-A
Primiya Radha Krishnan, CPC-A
Priya George, CPC-A
Priya Yangoubam, CPC-A, CPC-H-A
Priyanka Naikwadi, CPC-A
Puja Karalia, CPC-A
Pushpa Rani P.L, CPC-A
PushpaLatha T.V., CPC-A
Rachael Lipscomb, CPC-A
Rachel Deirdre Jayne, CPC-A
Rachel E Teopaco, CPC-A
Rachel Ossino, CPC-A
Radhika G, CPC-A
Rajamanickam Revathi, CPC-H-A
Rajasekaran Tamilarasan, CPC-H-A
Rajesh P Ravikanth, CPC-H-A
Rajeswari A, CPC-H-A
Rajeswari Sundaramoorthy, CPC-H-A
RajSandeep Magapu, CPC-H-A
Raju Ankam, CPC-H-A
Rakesh Bhamare, CPC-A
Ram Arthur Tiongan, CPC-A
Ramesh N C, CPC-H-A
Ramya Selvaraj, CPC-A
Raquel Cabug, CPC-A
Ratish Nair, CPC-A
RaviChandra Verma Vallabhuni, CPC-A
Rayna Scott, CPC-A
Rebecca Hill, CPC-A
Reena A S, CPC-H-A
Regina Enriquez, CPC-A
Regina Lydia-Mary Duncan, CPC-A
Reiko Wolf, CPC-A
Rekha Prasad, CPC-A
Rekha Shivaji Sutar, CPC-A
Renee Kinsey, CPC-A
Renee Mace, CPC-A
Renee Raleigh, CPC-A
Revathy Vellaiyappan, CPC-H-A
Reynard Hirang Hilahan, CPC-A
Rhonda Williams, CPC-A
Ricki Larmour, CPC-A
Rizaldy Peleo Reyes, CPC-A
www.aapc.com November 2014 65
NEWLY CREDENTIALED MEMBERSRobert Nutz, CPC-P-A
Roberta Winters, CPC-A
Robin Moses D, CPC-H-A
Roopa Govande, CPC-A
Rosalee Campbell, CPC-H-A
Rosarie Anne Juta Pascual, CPC-A
Rowena Alonzo, CPC-A
Rupali Popat Sakhare, CPC-A
Sabrina Sampson, CPC-A
Safal Chariyampadath, CPC-A
Sai Kumar Lingala, CPC-A
Sai Varsha, CPC-A
Sajeesh Augustine, CPC-A
Salini Rajesh, CPC-A
Samantha Marie Suddath, CPC-A
Sameer Ahamed, CPC-A
Samuel Nieves, CPC-A
Samuel Stone, CPC-A
Sandra Barnette, CPC-A
Sandra Chamberlin, CPC-A
Sandra Deterville, CPC-A
Sara Hibbard, CPC-A
Sara Hoover, CPC-A
Sara Kathryn Jones, CPC-A
Sara S Howard, CPC-A
Saranya Govindan, CPC-A
Saravanan Velayutham, CPC-A
Saurabh Yadav, CPC-A
Seema Sawant, CPC-A
Shabna Najeeb Mutton, CPC-A
Shaina Stevens, CPC-A
Shani Rapaport, CPC-A
Shanna Faith Somes Torreres, CPC-A
Shannon Lindloff, CPC-A
Sharath Kanth S, CPC-H-A
Sharron Lawson, CPC-A
Shashi Mohan Bharadwaj, CPC-A
Shauna Pearson, CPC-H-A
Shavon Nickole Richmond, CPC-A
Shayna Anderson, CPC-A
Shelby Perry, CPC-A
Shelly Scott, CPC-A
Sheri Yau, CPC-A
Sherry Pfeffer, CPC-A
Sheryl A Mullendore, CPC-A
Sheryl Watson, CPC-A
Shiji Jose, CPC-A
Shirley Bailey, CPC-A
Shona Arbrouet, CPC-A
Shrikant Patil, CPC-A
Shrikant Pawar, CPC-A
Shripad Kundale, CPC-A
Shweta Mukund Zaveri, CPC-A
Shyamala Kathirvel, CPC-H-A
Sivagami Sathish, CPC-A
Sivakumar J, CPC-A
Sneha Pokiya, CPC-A
Snehal Babanrao Kapote, CPC-A
Snehali More, CPC-A
Sonia Boedigheimer de Leon, CPC-A
Sonja Peisl, CPC-A
Sreelekha J, CPC-A
Sri Ganesh Goparaju, CPC-A
Sridhar Reddy Kudumula, CPC-H-A
Srinath Hulke, CPC-H-A
Srinivasa Reddy Kunduru, CPC-H-A
Srinivasulu Kandlakunta, CPC-A
Stephanie Gannon, CPC-A
Stephanie Geary, CPC-A
Stephanie Kires, CPC-A
Stephen Crafts, CPC-A
Stephen William Pedro, CPC-A
Subashini Rajagopalan, CPC-H-A
Subramony Sriram, CPC-A
Sucheeka Bhalla, CPC-A
Sudhir Oulkar, CPC-A
Sudipta Ghosh, CPC-A
Suganya Pattabiraman, CPC-A
Sugapriya Rajagopal, CPC-A
Sunil Kharade, CPC-A
Suresh Naidu Yarra, CPC-H-A
Suriyakumari Raja, CPC-H-A
Susan Duchaine, CPC-A
Susan Suchowski, CPC-A
Sushilkumar Govande, CPC-A
Swathi Anumolu, CPC-A
Swati Gajula, CPC-A
Swati Khandwekar, CPC-A
Tamara Arias, CPC-H-A
Tami Tuttle, CPC-A
Tammy Duane, CPC-A
Tara Elaine Buerkman, CPC-A
Teresa Alferez, CPC-A
Terri Ebbinghouse, CPC-A
Theresa M Cusella, CPC-A
Thomas Ruffalo, CPC-A
Tiffany Delker, CPC-A
Timothy James Apgar, CPC-A
Tirsa Ramirez-Belloso, CPC-A
Tracy Ann Zdilla, CPC-A
Trisha Martinez, CPC-A
Trudy Martin, CPC-A
Tuhina Sharma, CPC-A
Uttara Vaiti, CPC-A
Valerie Murphy, CPC-A
Vanessa Garcia, CPC-A
Vanessa Rodrigues-Gorn, CPC-A, CPC-H-A
Varnia Casimir Bryant, CPC-A
Veeramohan Reddy Baddigum, CPC-H-A
Venkatesh Gowni, CPC-A
Vernita Russell, CPC-A
Veronica James, CPC-A
Vicki Carr, CPC-A
Victoria Lane Smith, CPC-A
Vijit Kunjir, CPC-A
Vincent Ray Regala, CPC-H-A
Vinod Mankumare, CPC-A
Virgenmina Lugaro, CPC-A
Vishal Pawar, CPC-A
Vishal Sharda, CPC-A
Vishwanath Dhorashetty, CPC-A
Vonda Butler, CPC-A
Vrushali Dhananjay Mokal, CPC-A
Weigong He, CPC-A, CPC-H-A, CPC-P-A
Wendi Cain, CPC-A
William Haydo, CPC-H-A
Yarka Karasek, CPC-A
Yesenia Castrejon, CPC-A
Yuvanjili Rajlin, CPC-A
Yvonne Vazquez, CPC-A
Zhauntae Dotson, CPC-H-A
SpecialtiesSpecialtiesSpecialtiesAdrianna Dawn Foster, CPC, CPMA
A&P Quiz Answer (from page 43)The correct answer is B.
66 Healthcare Business Monthly
Minute with a Member
Mordecai E. Mose, CPC, CPC-HSenior Surgical Coder, Baylor College of Medicine and Adjunct Instructor, DHS Coding & Billing
»» Tell us a little bit about your career — how you got into coding, what you’ve done during your coding career, what you’re doing now, etc.In December of 1991, I earned a bachelor’s degree in Applied Sciences with a concen-tration in medical records administration (MRA), which is now known as Health Information Management (HIM). To in-crease my prospects of finding a job in the MRA field, I moved from the small country town of Point Blue, Louisiana, to Houston, Texas. Armed with a four-year degree and only two semesters of clinicals experience, I was thrown into a slow economy, which was a real eye opener for a new college grad-uate. It taught me how to be more persever-ant and competitive in the job hunt, and stay focused on beginning my new career in MRA. After two months of job hunting with no results, my mother told me that the medical record director at University Medi-cal Center (where I completed my clinicals) wanted to hire me as a medical records clerk. I accepted the job. My foot was in the door and now it was up to me to make the most of my coding career.After six months as a medical records clerk, I was approached by a gentleman from LSU School of Medicine who suggested I apply for a position as a Medicaid verification rep-
resentative. I was hired for the position and, much to my surprise, began working for my college professor, who taught Legal Aspects of Healthcare. Since then, I have worked as an inpatient/outpatient coder and, for U.S. Anesthesia Partners, I worked as a patient financial counselor, an old accounts receiv-able appeals specialist, an administrative as-sistant, and a certified coding specialist II. In June 2014, I took a position as a hospi-tal coder with Victory Healthcare Systems, and I most recently have become senior sur-gical coder at Baylor College of Medicine. I am also an adjunct instructor at DHS Cod-ing & Billing Consultants.
What is your involvement with your local AAPC chapter?I attend as many local chapter meetings as I can. If I can’t attend, I have friends that I query to keep me up to date with the latest coding trends and interventions. I have at-tended a couple of the local coding sympo-siums, which I really enjoyed because of the interaction between fellow coders, HIM ad-ministrators, physicians, nurses, and state and federal CMS officials.
What AAPC benefits do you like the most?I love AAPC’s website because it’s loaded with valuable information regarding where the coding field is headed for the future. Their webinars, conferences, and online training courses also are very informative and reasonably priced to fit any style of learning.
What has been your biggest challenge as a coder?My biggest challenge has been proving my competence and knowledge as a coder — possibly due to the lack of males in this field. I’ve been coding for over 20 years, and it’s always been a female-dominated industry.
How is your organization preparing for ICD-10?I know ICD-10 will become a reality in the United States, so I asked my supervisor to purchase all the materials I needed to be-come familiar with the new code set and guidelines. I used them to help train my fel-low coders, billers, and reimbursement per-sonnel. I have taken online training mod-ules, and a hands-on AAPC-approved, eight-week training course through DHS Coding & Billing Consultants, which was very ex-citing, and helped me to pass my ICD-10-CM proficiency assessment. We are work-ing with the auditing department to provide a gap analysis to our physicians, as a primary defense against the loss of revenue.
If you could do any other job, what would it be?I would be a full-time advocate for children and adults with special needs. My wife and I have a 6-year-old son with autism, and we’ve experienced how the educational and social services systems fail to meet the basic needs of these individuals — all of whom just need a helping hand.
How do you spend your spare time? Tell us about your hobbies, family, etc.In my spare time, I enjoy cooking for my family and friends, helping my son, Mala-chi, become more acclimated to new social environments. I am also involved with the local independent film industry as an actor and stand-up comedian.
GOT A MINUTE?
Paris by Day
Vegas by NightMarch 29 - April 1, 2015
Las Vegas, NV 75+ Sessions | 18 CEUs
Conference + 3 Nights Hotel Starting at $1297 $997
Early Bird Registration Open Through January 16
healthcon.com
800-626-2633aapc.com/icd10
ICD-10 will be here in less than a yearMYTH: The Department of Health and Human Services (HHS) will grant an
extension beyond the October 1, 2015, compliance date.
FACT: HHS has no plans to extend the compliance date for implementation of ICD-10-CM/PCS; therefore, covered entities should plan to complete
the steps required to implement ICD-10-CM/PCS on October 1, 2015.
AAPC Can Help You Get ReadyTraining & Education
• Available to coders, billers, auditors, and physicians • Anatomy & Pathophysiology
• Core training: general code set
• Advanced training by specialty
• Assessment prep
• Proficiency workbooks and assessments
Clinical Documentation Improvement
• Documentation training by speciality • Two separate courses tailored to physicians and auditors/coders







































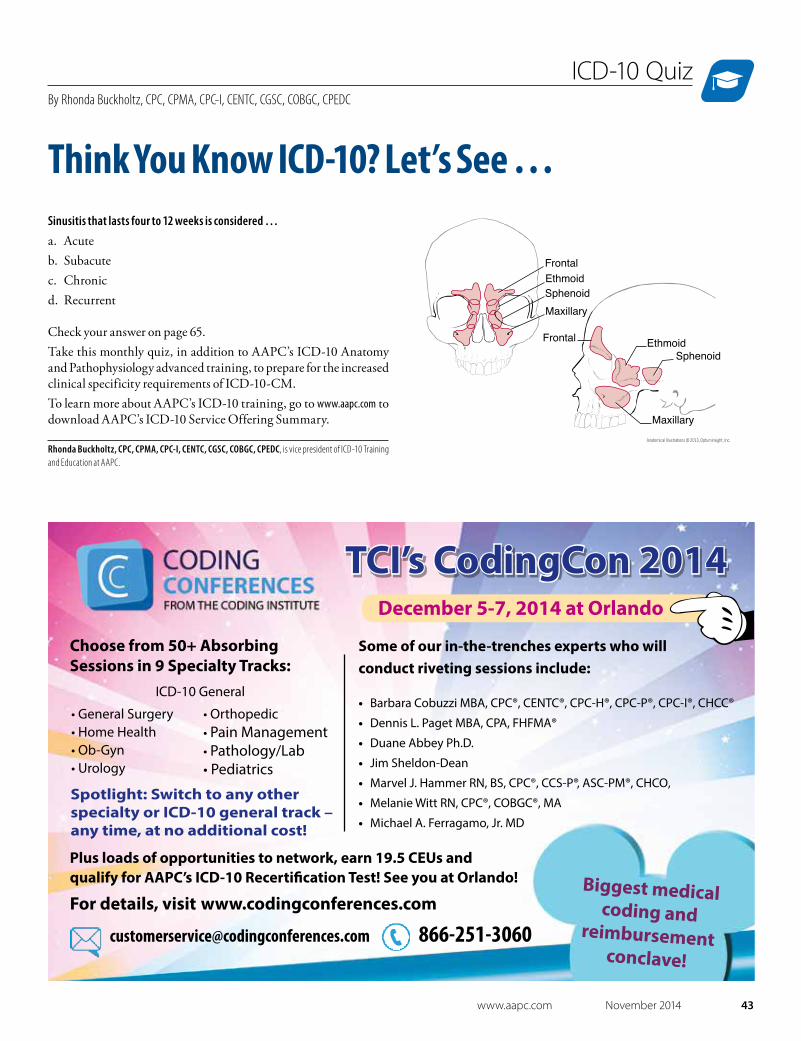





































![Table 1 [=IMG1]: ICD 9 CM Code to Identify CT … Seizure ICD‐9‐CM Code Description ICD‐9‐CM Code ICD‐10‐CM Code ICD‐10‐CM Code Description Localization‐related (focal)](https://static.documents.pub/doc/80x56/5abdd31b7f8b9a5d718c2e4a/table-1-img1-icd-9-cm-code-to-identify-ct-seizure-icd9cm-code-description.jpg)




