55
> HealthyBlue Dual/Triple Option Provider Manual

>HealthyBlue Dual/Triple Option Provider Manual
HealthyBluePROVIDERMANUAL
TableofContents
Welcome to HealthyBlue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
HealthyBlue: How it Works . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4HealthandWellnessEvaluationHealthy Action PlanHealthandWellnessRequestforInformationLetterPlanOptions
Membership & Product Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9HealthSavingsAccount(HSA)andHealthReimbursementArrangement(HRA)Plans
HealthyBlue Identification Cards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Referral Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15PCPReferralProcessSpecialistReferralProcessServicesNotRequiringaReferralExtended(Standing)Referrals
Authorizations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18ServicesRequiringAuthorizationServicesNotRequiringanAuthorizationIn-NetworkversusOut-of-NetworkProviders
Arranging for Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20RoleofthePCPRoutineOfficeVisitsEmergencyRoomServicesHospitalServicesBenefits,ExclusionsandLimitationsAwayFromHomeCareLaboratoryServicesObstetrics&Gynecology
Appeals Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Administrative Functions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45ChangeinPrivilegesWebResources
Important Addresses and Telephone/Fax Numbers . . . . . . . . . . . . . . . . . . . . . . . . 48
Frequently Asked Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
PerthetermsoftheParticipationAgreement,allprovidersarerequiredtoadheretothepoliciesandprocedurescontainedinthismanual,asapplicabletoeachtypeofprovider.
2
HealthyBluePROVIDERMANUAL
Welcome to HealthyBlue
Astheprimarycareprovider(PCP)*,youknowourmembers’healthcareneedsbetterthananyone.Youarealsointhebestpositiontoprovidecoordinatedcareandmakekeyjudgmentsregardingthemembers’health.CareFirstBlueChoice,Inc.(CareFirstBlueChoice)ispleasedtointroduceHealthyBlue,anewproductwithapositiveapproachtohealthcarethatfostersandrewardshealthylifestylesandpromotesastrong,trustingrelationshipbetweenyouandyourpatients.
HealthyBlueproductsaredesignedtorewardCareFirstBlueChoicememberswhoworkcloselywiththeirproviderstobetterunderstandandmonitortheircare.Withyourguidance,memberswillbegintotakeanactiveroleinmaintainingahealthylifestyleandworktowardimprovedhealth.
ThismanualwillassistyouincaringforCareFirstBlueChoicememberswhoelecttoparticipateinHealthyBlue.Enclosedyouwillfindadministrativeguidelines,sampleformsandmore.
Pleasenote:
● Thismanualwillbeupdatedifproceduralchangesaremadeinourongoingeffortstoimproveourservice.
● Thespecificsofamember’shealthbenefitsvaryandmaydifferfromtheproceduresoutlinedinthismanual.It is important to note that the referral process for HealthyBlue is different than BlueChoice HMO. Please refer to the Referrals section for more information.
IfyouhaveanyquestionsorwouldlikeadditionalinformationaboutHealthyBlue,pleasecallaProviderServicesRepresentativeat202-479-6560 or 800-842-5975.
*TopracticeasanindependentPCP,NPsmustbecertifiedbytheirrelevantapprovedNationalCertificationBoardandmeetalllicensingcertificationguidelinesofthestateinwhichtheNPpractices.NPsmustalsofileanattestationthattheyhaveawrittencollaborativeagreementwithaphysicianofthesamespecialtywhoisingoodstandinginthesameCareFirstprovidernetworks.
3
HealthyBluePROVIDERMANUAL
HealthyBlue: How it Works
FollowingenrollmentintheHealthyBlueproduct,memberswhoelectedtoparticipatewillhavetocompleteaHealthAssessmentandscheduleaPrimaryCareProvider(PCP)visittoconductaHealthandWellnessEvaluationatnoout-of-pocketcostforthemember.
ThefollowingtypesofCareFirstBlueChoicepractitionersarerecognizedasHealthyBlueprimarycareproviders(PCPs):
● FamilyPractice
● GeneralPractice
● InternalMedicine
● Pediatrics
● Geriatrics
Note for OB/GYN physicians: IfyouareaCareFirstBlueChoiceparticipatingOB/GYNwhoagreestoactasPCPforamember,givethememberaletterstatingyourdecisiontoserveasherPCP.ThelettershouldincludeyourCareFirstBlueChoiceprovidernumberandthemember’sidentificationnumber.ThemembershouldsubmitthelettertoCareFirstMemberServicesforprocessing.
4
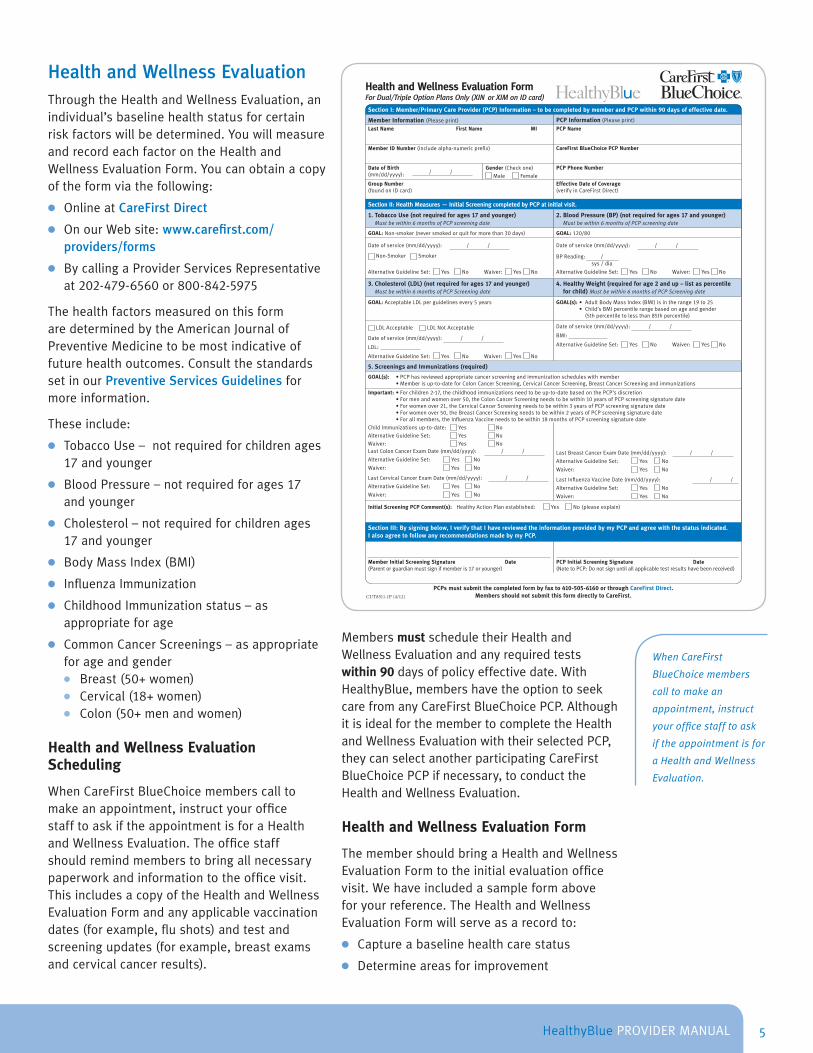
Health and Wellness EvaluationThroughtheHealthandWellnessEvaluation,anindividual’sbaselinehealthstatusforcertainriskfactorswillbedetermined.YouwillmeasureandrecordeachfactorontheHealthandWellnessEvaluationForm.Youcanobtainacopyoftheformviathefollowing:
● OnlineatCareFirst Direct
● OnourWebsite:www .carefirst .com/providers/forms
● BycallingaProviderServicesRepresentativeat202-479-6560or800-842-5975
ThehealthfactorsmeasuredonthisformaredeterminedbytheAmericanJournalofPreventiveMedicinetobemostindicativeoffuturehealthoutcomes.ConsultthestandardssetinourPreventive Services Guidelinesformoreinformation.
Theseinclude:
● TobaccoUse–notrequiredforchildrenages17andyounger
● BloodPressure–notrequiredforages17andyounger
● Cholesterol–notrequiredforchildrenages17andyounger
● BodyMassIndex(BMI)
● InfluenzaImmunization
● ChildhoodImmunizationstatus–asappropriateforage
● CommonCancerScreenings–asappropriateforageandgender
● Breast(50+women) ● Cervical(18+women) ● Colon(50+menandwomen)
Health and Wellness Evaluation Scheduling
WhenCareFirstBlueChoicememberscalltomakeanappointment,instructyourofficestafftoaskiftheappointmentisforaHealthandWellnessEvaluation.Theofficestaffshouldremindmemberstobringallnecessarypaperworkandinformationtotheofficevisit.ThisincludesacopyoftheHealthandWellnessEvaluationFormandanyapplicablevaccinationdates(forexample,flushots)andtestandscreeningupdates(forexample,breastexamsandcervicalcancerresults).
MembersmustscheduletheirHealthandWellnessEvaluationandanyrequiredtestswithin 90 daysofpolicyeffectivedate.WithHealthyBlue,membershavetheoptiontoseekcarefromanyCareFirstBlueChoicePCP.AlthoughitisidealforthemembertocompletetheHealthandWellnessEvaluationwiththeirselectedPCP,theycanselectanotherparticipatingCareFirstBlueChoicePCPifnecessary,toconducttheHealthandWellnessEvaluation.
Health and Wellness Evaluation Form
ThemembershouldbringaHealthandWellnessEvaluationFormtotheinitialevaluationofficevisit.Wehaveincludedasampleformaboveforyourreference.TheHealthandWellnessEvaluationFormwillserveasarecordto:
● Captureabaselinehealthcarestatus
● Determineareasforimprovement
HealthyBluePROVIDERMANUAL
Section I: Member/Primary Care Provider (PCP) Information – to be completed by member and PCP within 90 days of effective date.
Member Information (Please print) PCP Information (Please print)
Last Name First Name MI PCP Name
Member ID Number (include alpha-numeric prefix) CareFirst BlueChoice PCP Number
Date of Birth(mm/dd/yyyy): / /
Gender (Check one)
Male Female
PCP Phone Number
Group Number (found on ID card)
Effective Date of Coverage (verify in CareFirst Direct)
Section II: Health Measures — Initial Screening completed by PCP at initial visit.
1. Tobacco Use (not required for ages 17 and younger) Must be within 6 months of PCP screening date
2. Blood Pressure (BP) (not required for ages 17 and younger) Must be within 6 months of PCP screening date
GOAL: Non-smoker (never smoked or quit for more than 30 days) GOAL: 120/80
Date of service (mm/dd/yyyy): / /
Non-Smoker Smoker
Alternative Guideline Set: Yes No Waiver: Yes No
Date of service (mm/dd/yyyy): / /
BP Reading: / sys / dia
Alternative Guideline Set: Yes No Waiver: Yes No
3. Cholesterol (LDL) (not required for ages 17 and younger) Must be within 6 months of PCP Screening date
4. Healthy Weight (required for age 2 and up – list as percentile for child) Must be within 6 months of PCP Screening date
GOAL: Acceptable LDL per guidelines every 5 years GOAL(s): • Adult Body Mass Index (BMI) is in the range 19 to 25 • Child’s BMI percentile range based on age and gender
(5th percentile to less than 85th percentile)
LDL Acceptable LDL Not Acceptable
Date of service (mm/dd/yyyy): / /
LDL:
Alternative Guideline Set: Yes No Waiver: Yes No
Date of service (mm/dd/yyyy): / /
BMI:
Alternative Guideline Set: Yes No Waiver: Yes No
5. Screenings and Immunizations (required)
GOAL(s): • PCP has reviewed appropriate cancer screening and immunization schedules with member • Member is up-to-date for Colon Cancer Screening, Cervical Cancer Screening, Breast Cancer Screening and immunizations
Important: • For children 2-17, the childhood immunizations need to be up-to-date based on the PCP’s discretion • For men and women over 50, the Colon Cancer Screening needs to be within 10 years of PCP screening signature date • For women over 21, the Cervical Cancer Screening needs to be within 3 years of PCP screening signature date • For women over 50, the Breast Cancer Screening needs to be within 2 years of PCP screening signature date • For all members, the Influenza Vaccine needs to be within 18 months of PCP screening signature date
Child Immunizations up-to-date: Yes No
Alternative Guideline Set: Yes No
Waiver: Yes NoLast Colon Cancer Exam Date (mm/dd/yyyy): / /
Alternative Guideline Set: Yes No
Waiver: Yes No
Last Breast Cancer Exam Date (mm/dd/yyyy): / /
Alternative Guideline Set: Yes No
Waiver: Yes No
Last Cervical Cancer Exam Date (mm/dd/yyyy): / /
Alternative Guideline Set: Yes No
Waiver: Yes No
Last Influenza Vaccine Date (mm/dd/yyyy): / /
Alternative Guideline Set: Yes No
Waiver: Yes No
Initial Screening PCP Comment(s): Healthy Action Plan established: Yes No (please explain)
Section III: By signing below, I verify that I have reviewed the information provided by my PCP and agree with the status indicated. I also agree to follow any recommendations made by my PCP.
Member Initial Screening Signature Date(Parent or guardian must sign if member is 17 or younger)
PCP Initial Screening Signature Date(Note to PCP: Do not sign until all applicable test results have been received)
Health and Wellness Evaluation FormFor Dual/Triple Option Plans Only (XIN or XIM on ID card)
PCPs must submit the completed form by fax to 410-505-6160 or through CareFirst Direct. Members should not submit this form directly to CareFirst.CUT8511-1P (4/12)
When CareFirst
BlueChoice members
call to make an
appointment, instruct
your office staff to ask
if the appointment is for
a Health and Wellness
Evaluation.
5
HealthyBluePROVIDERMANUAL
● DevelopaHealthyActionPlantopromotehealthylifestyles
IfthememberdoesnotbringtheHealthandWellnessEvaluationFormtotheinitialofficevisit,youcanaccesstheformviathefollowing:
● OnlineatCareFirst Direct
● OnourWebsite:www .carefirst .com/providers/forms
● BycallingaProviderServicesRepresentativeat202-479-6560or800-842-5975
Besuretoconfirmthemember’seffectivedateandeligibilitypriortofillingouttheHealthandWellnessEvaluationForm.Theformmustbecompletedduringyourmember’sevaluationvisitandreturnedtoCareFirstBlueChoicewithin120 daysofthemember’seffectivedate,otherwisethememberwillnotbeeligibletoreceiveanincentive.
Ifthememberhascompletedtherequiredscreenings,immunizationsandhealthmeasureswithintheprevioussix(6)months,youmaydeterminethatanofficevisitisnotnecessarytocompletetheHealthandWellnessEvaluationForm.However,allareasoftheinitialscreeningsectionmustbecompletedandbothyouandthemembermustsigntheformregardlessofwhetheranofficevisitisrequired.
Toavoiddelaysinprocessingthemember’sincentive,besurethattheformisfilledoutinitsentirety–includingsignatures,updatesoncancerscreeningsandchildhoodimmunizations.Signingthisformindicatesthatyouhavereviewedtheresultswiththememberandagreewithwhatisreported.Any form received by CareFirst BlueChoice without proper signatures (provider and member) will be considered incomplete and will be returned.
Initial Evaluation Screening
AsyoucompletetheHealthandWellnessEvaluationForm,recordtheoutcomesofthescreenings,immunizationsandbaselinehealthfactorsintheInitial Screeningsection.Also,besuretomeasureanddiscussthehealthfactorswithmemberstodeterminetheirbaselinehealthstatus.AllfieldsoftheHealthandWellnessEvaluationFormmustbecompleted.
TocomplywiththeHealthInsurancePortabilityandAccountabilityAct(HIPAA)regulationsfora
“bonafidewellnessprogram,”youcanallowforanalternativestandard/guideline(orwaiverofinitialgoal/standard)foranymemberforwhomitisunreasonablydifficultduetoamedicalconditionoritismedicallyinadvisabletosatisfytheinitialstandard/guideline.
Check“Waiver”or“AlternativeGuidelineSet”intheboxesprovidedforeachHealthMeasuretoindicatethatthememberhasmettheacceptableguidelines.Detailsonallwaiversoralternativestandards/guidelinesshouldbeprovidedinthecommentssection(s)oftheform.
● By checking “Waiver”youarereportingthatthememberdoesnothavetomeetalternativestandards/guidelines
● By checking “Alternative Guideline Set” youarerequiredtoprovideanewgoalforthemembertomeetatthetimeofaclinicallyappropriatereevaluation
Examplesofawaiveroralternativestandard/guidelineinclude:
● WaivingaBodyMassIndex(BMI)readingduetopregnancy
● Compliancewithalow-cholesteroldietforindividualswithgeneticallyhighcholesterol
When completing the Health and Wellness Evaluation Form, please remember the following goals as they relate to the member’s cancer screening and immunization health status:
● Memberisup-to-dateforappropriatecancerscreeningsbasedonage/gender
● Memberisup-to-dateforinfluenza
● Memberisup-to-dateonchildimmunizationsbasedonage
● PCPhasreviewedappropriatecancerscreeningandimmunizationscheduleswithmember
ConsultourPreventive Services Guidelinesfordetailsonappropriatestandards.
Note:SubmitCPT® code 99420whenyoufileareimbursementclaimforcompletingtheinitialevaluationscreeningportionoftheHealthandWellnessEvaluationFormanddiscussingtheresultswiththemember,alongwithotherservicesrendered.Thereimbursementiscalculatedinthesamemannerasanofficevisit.
Submit the Health and Wellness Evaluation
6

HealthyBluePROVIDERMANUAL
Form using one of the following methods:
1. UploadtoCareFirst Direct: ● Scantheformandsaveitin.JPG,.PDFor
.TIFFformat ● ClickUploadEvaluationFormtosendthe
documentfromyourcomputerOR
2. Faxto:410-505-6160or800-354-8205
Healthy Action PlanAHealthy Action Planisanagreementbetweenthememberandproviderandshouldbedevelopedifthememberdoesnotmeetthenationalguidelines(identifiedas“Goal”ontheHealthandWellnessEvaluationForm)duringtheinitialscreening.Weencourageyoutoworkwiththemembertodevelopacustomizedplanthatincludesrecommendationsformeasuresthatneedre-evaluationtohelpthemembermeetthegoalsontheHealthandWellnessEvaluationForm.TheHealthy Action Plan servesasaguidetoshowmembershowtoachieveandmaintainhealthy,long-termoutcomes.
TheHealthy Action PlanshouldalsoincludeatimeframeforwhenthememberisexpectedtoreturnforaClinicallyAppropriateRe-Screening.Inordertoqualifyforaprogramincentive,themember’sHealthy Action Planmustbedevelopedandtheclinicallyappropriatere-screeningmusttakeplacepriortotherenewaldate.
Formoreinformationonthehealthmeasuresandinstructionsforprovidingpreventivecare,consultourPreventive Services Guidelines .
Clinically Appropriate Re-Screening
TheClinically Appropriate Re-ScreeningisnecessaryifyoudeterminethatthememberdoesnotmeetorexceedhealthymeasuresbasedonthestandardssetinourPreventive Services Guidelines.Membersmustcompletethisprocesstobeeligibleforprogramincentives.There-screeningwillalsobeusedtocheckthestatusoftheHealthy Action Plan atthetimeageeduponbythePCPandthemember.
Submitting the Form:
● Ifyouconductboththeinitialevaluationscreening,andthere-screening,pleasecomplete,signandsubmitboththeInitialandRe-Screeningsectionsoftheform.
● Youmaydecidetoeithertestonlythosemeasuresforthegoalsthememberdidnotreachorre-testallmeasuresagain.However,youmustbesuretofullycompletebothsectionsoftheHealthandWellnessEvaluationForm.
● Makesureallsectionsoftheform,forboththeinitialscreeningandthere-screeningresults,arecompletedbeforesubmittingtheformviaCareFirst Directorbyfax(410-505-6160or800-354-8205),eveniftherearenochanges.
● Bothyouandthemembermustsignthere-screeningsectionoftheHealthandWellnessEvaluationFormtoindicatethatyoubothreviewedtheformandagreewiththemeasuresrecorded.
● UsetheexistingclaimssubmissionprocesstofileaclaimforreimbursementoftheHealthandWellnessEvaluationFormalongwithotherservicesrendered.
● MembersmayrequestacopyoftheHealthandWellnessEvaluationFormfortheirrecords.
● OnlyaCareFirstBlueChoicePCPcansubmittheformtoCareFirstBlueChoice.
Note:SubmitCPT® code 99420whenyoufileareimbursementclaimforcompletingthere-screeningportionoftheevaluationformanddiscussingtheresultswiththemember,alongwithotherservicesrendered.Thereimbursementiscalculatedinthesamemannerasanofficevisit.
Submit the Health and Wellness Evaluation Form using one of the following methods:
1. UploadtoCareFirst Direct: ● Scantheformandsaveitin.JPG,.PDFor
.TIFFformat ● ClickUploadEvaluationFormtosendthe
documentfromyourcomputerOR
2. Faxto:410-505-6160or800-354-8205
For more information
on the health measures
and instructions for
providing preventive
care, click here to view
our Preventive Services
Guidelines .
7
HealthyBluePROVIDERMANUAL
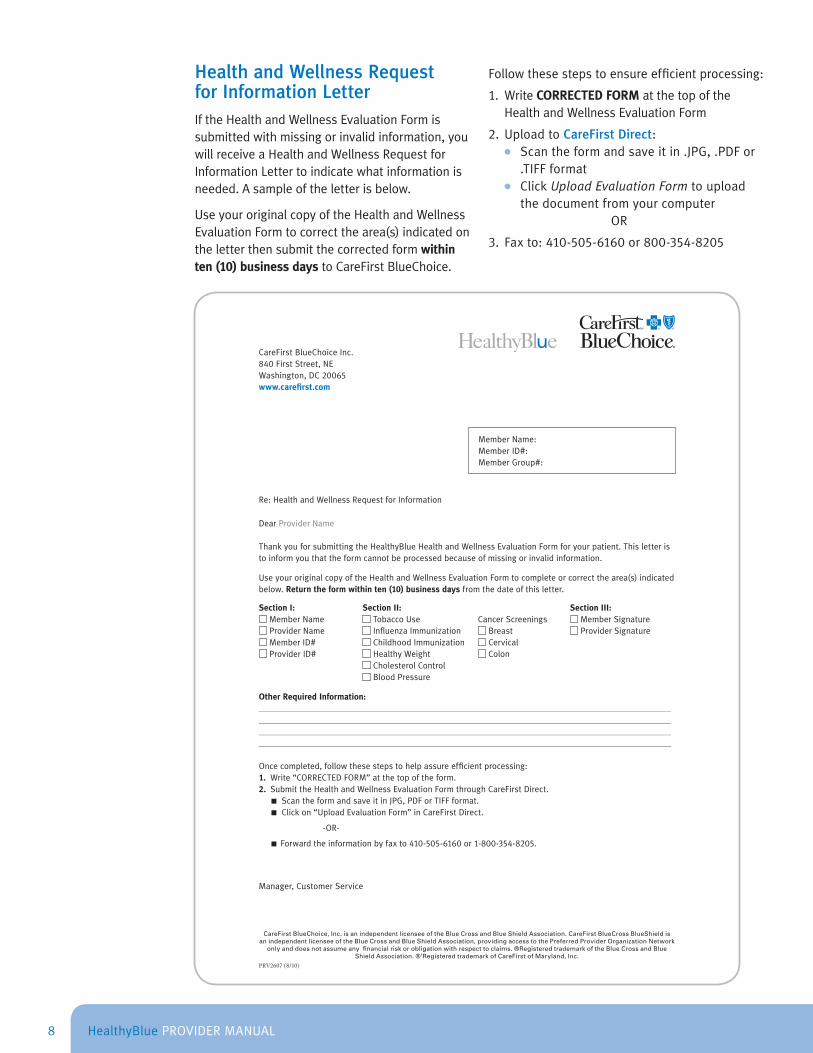
Health and Wellness Request for Information LetterIftheHealthandWellnessEvaluationFormissubmittedwithmissingorinvalidinformation,youwillreceiveaHealthandWellnessRequestforInformationLettertoindicatewhatinformationisneeded.Asampleoftheletterisbelow.
UseyouroriginalcopyoftheHealthandWellnessEvaluationFormtocorrectthearea(s)indicatedontheletterthensubmitthecorrectedformwithin ten (10) business daystoCareFirstBlueChoice.
Followthesestepstoensureefficientprocessing:
1. WriteCORRECTED FORMatthetopoftheHealthandWellnessEvaluationForm
2. UploadtoCareFirst Direct: ● Scantheformandsaveitin.JPG,.PDFor
.TIFFformat ● ClickUpload Evaluation Formtoupload
thedocumentfromyourcomputerOR
3. Faxto:410-505-6160or800-354-8205
CareFirst BlueChoice, Inc. is an independent licensee of the Blue Cross and Blue Shield Association. CareFirst BlueCross BlueShield is an independent licensee of the Blue Cross and Blue Shield Association, providing access to the Preferred Provider Organization Network
only and does not assume any fi nancial risk or obligation with respect to claims. ®Registered trademark of the Blue Cross and Blue Shield Association. ®’Registered trademark of CareFirst of Maryland, Inc.
PRV2607 (8/10)
CareFirstBlueChoiceInc.840FirstStreet,NEWashington,DC20065www.carefi rst.com
MemberName:MemberID#:MemberGroup#:
Re:HealthandWellnessRequestforInformation
DearProviderName
ThankyouforsubmittingtheHealthyBlueHealthandWellnessEvaluationFormforyourpatient.Thisletteristoinformyouthattheformcannotbeprocessedbecauseofmissingorinvalidinformation.
UseyouroriginalcopyoftheHealthandWellnessEvaluationFormtocompleteorcorrectthearea(s)indicatedbelow.Return the form within ten (10) business days fromthedateofthisletter.
Section I: Section II: Section III:MemberName TobaccoUse CancerScreenings MemberSignatureProviderName InfluenzaImmunization Breast ProviderSignatureMemberID# ChildhoodImmunization CervicalProviderID# HealthyWeight Colon
CholesterolControlBloodPressure
Other Required Information:_____________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________
Oncecompleted,followthesestepstohelpassureefficientprocessing:1 . Write“CORRECTEDFORM”atthetopoftheform.2 . SubmittheHealthandWellnessEvaluationFormthroughCareFirstDirect. ■ScantheformandsaveitinJPG,PDForTIFFformat. ■Clickon“UploadEvaluationForm”inCareFirstDirect.
-OR-
■ Forwardtheinformationbyfaxto 410-505-6160or1-800-354-8205.
Manager,CustomerService
8

HealthyBluePROVIDERMANUAL
Membership & Product Information
ThefollowingsectionprovidesinformationontheHealthyBluebenefitdesignandincludessamplebenefitchartsforyourreference.Itisimportanttonotethatthechartsarefordescriptivepurposesonlyanddonotrepresentbenefitdesignsacrossplanoptions/jurisdictions.IfmembershavequestionsregardingtheirHealthyBluebenefits,pleaseaskthemtocontactMemberServicesatthenumberlocatedonthebackoftheirHealthyBlueIdentificationCard.
Plan Options Throughpurposefulbenefitdesignsandmemberfinancialincentives,HealthyBlue’svalue-basedthree-optionbenefitstructureshowshowyoucanbestadvisememberstogetthemostcost-effectivecarewhentheyneedit.MemberscanhaveeitheraDualOptionorTripleOptionprogram.Inaddition,membersreceivefullcoverageforcertaingenericdrugsusedtopreventchronicdiseases,includingcholesterol,asthma,depression,hypertensionanddiabetes.
Option 1: Access through a CareFirst BlueChoice PCP:InOption1,amember’scareandreferralsarecoordinatedthroughtheprimarycareprovider(PCP)withintheCareFirstBlueChoiceprovider
network(specialist,hospitalorotherprovider)andalowerout-of-pocketcostisincurredorinthecaseofpreventativeservices,thereisnochargeatall.
Option 2: Access directly to other providers in the CareFirst BlueChoice network without PCP referral:Option2requiresthatthememberreceivescarewithintheCareFirstBlueChoicenetworkbutdoesn’trequirethatthecarebeprovidedorcoordinatedthroughthePCP.Thememberwillpayhigherout-of-pocketcosts,whilestillreceivingpreventiveservicesatnocharge.
Option 3: Access to out-of-network providers anywhere in the United States:Option3providesmemberswiththeflexibilitytoreceivecareoutsideoftheCareFirst
9

HealthyBluePROVIDERMANUAL
BlueChoicenetworkthroughthePreferredProviderOrganization(PPO)NetworkorOut-of-Networkentirely,butwillhavethehighestout-of-pocketcostswiththepreventiveservicesrequiringthedeductiblebemetfirst,withacopay/coinsurance.1
Health Savings Account (HSA) and Health Reimbursement Arrangement (HRA) PlansThosemembersinCareFirstBlueChoice’sHealthyBlueBlueFundorCompatibleHSAhealthplanscanelecttoestablishaHealthSavingsAccount(HSA),whichallowsthemtousetax-freedollarstopayforqualifiedmedicalexpenses.TheHealthReimbursementArrangement(HRA)planisavailabletomembersintheHealthyBlueBlueFundHRAandCompatibleHRAplans.TheHRAallowsmemberstouseemployer-depositedfundsfromaspendingaccounttopayforqualifiedmedicalexpenses.
ThebenefitsummaryontheprecedingpagesisasamplebenefitdesignforanHRAeligibleproduct.AllHSAqualifiedplans(BlueFundandCompatible)andsomeHRAqualifiedplans(BlueFundandCompatible)havethedeductibleapplytoallservices,exceptforpreventiveservicesthatincludepreventiveadultvisits,well-childcare,andcertaincancerscreeningsthatarenocosttothemember.
MemberswhoaccesscareunderOption3mayberesponsibleforhigherdeductiblesandcopays/coinsurance.ForIndividualDualOptionHSAaccountswedonotprovidecoverageforout-of-networkservices,thereforemembersshouldonlyvisitaCareFirstBlueChoiceprovider.
HealthyBlue
Option Option1MemberCostSharing
=$
Option2MemberCostSharing
=$$
Option3MemberCostSharing
=$$$
Network CareFirstBlueChoiceNetwork
CareFirstBlueChoiceNetwork
PreferredProviderOrganization(PPO)
Network(nobalancebilling)
Out-of-Network(possiblebalance
billing)
Referral Required for Specialist?
Yes No No
This chart is for descriptive purposes and does not represent benefits across plan options/jurisdictions.
1InMarylandsmallgroups,thewell-childcarevisitsdonotrequirethedeductibletobemetfirstandonlyhavea$10copay.
10
HealthyBluePROVIDERMANUAL
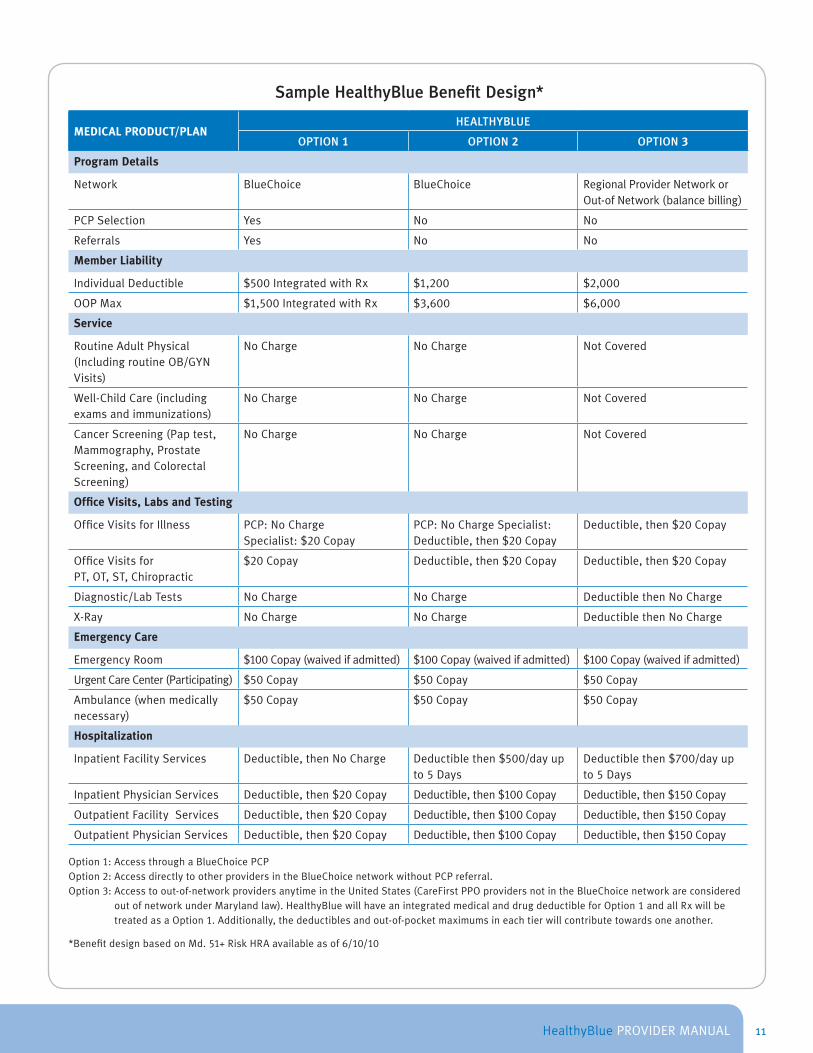
Sample HealthyBlue Benefit Design*
MEDICAL PRODUCT/PLANHEALTHYBLUE
OPTION 1 OPTION 2 OPTION 3
Program Details
Network BlueChoice BlueChoice RegionalProviderNetworkorOut-ofNetwork(balancebilling)
PCPSelection Yes No No
Referrals Yes No No
Member Liability
IndividualDeductible $500IntegratedwithRx $1,200 $2,000
OOPMax $1,500IntegratedwithRx $3,600 $6,000
Service
RoutineAdultPhysical(IncludingroutineOB/GYNVisits)
NoCharge NoCharge NotCovered
Well-ChildCare(includingexamsandimmunizations)
NoCharge NoCharge NotCovered
CancerScreening(Paptest,Mammography,ProstateScreening,andColorectalScreening)
NoCharge NoCharge NotCovered
Office Visits, Labs and Testing
OfficeVisitsforIllness PCP:NoChargeSpecialist:$20Copay
PCP:NoChargeSpecialist:Deductible,then$20Copay
Deductible,then$20Copay
OfficeVisitsforPT,OT,ST,Chiropractic
$20Copay Deductible,then$20Copay Deductible,then$20Copay
Diagnostic/LabTests NoCharge NoCharge DeductiblethenNoCharge
X-Ray NoCharge NoCharge DeductiblethenNoCharge
Emergency Care
EmergencyRoom $100Copay(waivedifadmitted) $100Copay(waivedifadmitted) $100Copay(waivedifadmitted)
UrgentCareCenter(Participating) $50Copay $50Copay $50Copay
Ambulance(whenmedicallynecessary)
$50Copay $50Copay $50Copay
Hospitalization
InpatientFacilityServices Deductible,thenNoCharge Deductiblethen$500/dayupto5Days
Deductiblethen$700/dayupto5Days
InpatientPhysicianServices Deductible,then$20Copay Deductible,then$100Copay Deductible,then$150Copay
OutpatientFacilityServices Deductible,then$20Copay Deductible,then$100Copay Deductible,then$150Copay
OutpatientPhysicianServices Deductible,then$20Copay Deductible,then$100Copay Deductible,then$150Copay
Option1:AccessthroughaBlueChoicePCPOption2:AccessdirectlytootherprovidersintheBlueChoicenetworkwithoutPCPreferral.Option3:Accesstoout-of-networkprovidersanytimeintheUnitedStates(CareFirstPPOprovidersnotintheBlueChoicenetworkareconsidered
outofnetworkunderMarylandlaw).HealthyBluewillhaveanintegratedmedicalanddrugdeductibleforOption1andallRxwillbetreatedasaOption1.Additionally,thedeductiblesandout-of-pocketmaximumsineachtierwillcontributetowardsoneanother.
*BenefitdesignbasedonMd. 51+RiskHRAavailableasof6/10/10
11
HealthyBluePROVIDERMANUAL
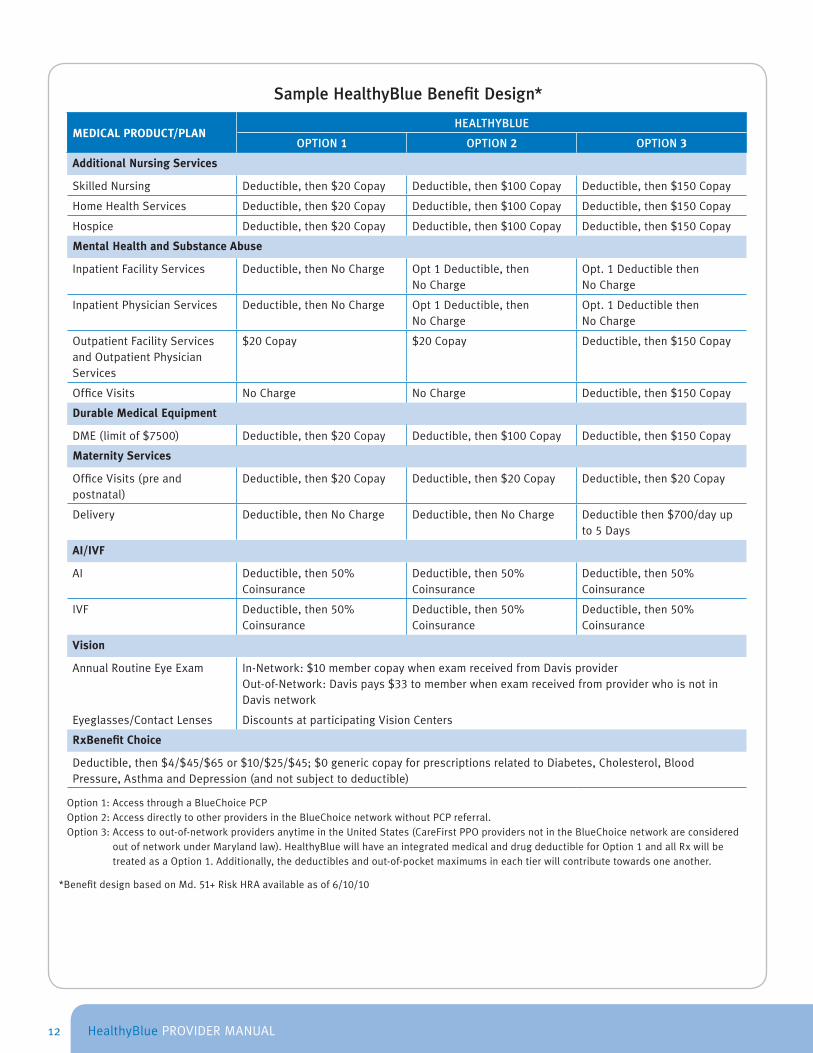
Sample HealthyBlue Benefit Design*
MEDICAL PRODUCT/PLANHEALTHYBLUE
OPTION 1 OPTION 2 OPTION 3
Additional Nursing Services
SkilledNursing Deductible,then$20Copay Deductible,then$100Copay Deductible,then$150Copay
HomeHealthServices Deductible,then$20Copay Deductible,then$100Copay Deductible,then$150Copay
Hospice Deductible,then$20Copay Deductible,then$100Copay Deductible,then$150Copay
Mental Health and Substance Abuse
InpatientFacilityServices Deductible,thenNoCharge Opt1Deductible,thenNoCharge
Opt.1DeductiblethenNoCharge
InpatientPhysicianServices Deductible,thenNoCharge Opt1Deductible,thenNoCharge
Opt.1DeductiblethenNoCharge
OutpatientFacilityServicesandOutpatientPhysicianServices
$20Copay $20Copay Deductible,then$150Copay
OfficeVisits NoCharge NoCharge Deductible,then$150Copay
Durable Medical Equipment
DME(limitof$7500) Deductible,then$20Copay Deductible,then$100Copay Deductible,then$150Copay
Maternity Services
OfficeVisits(preandpostnatal)
Deductible,then$20Copay Deductible,then$20Copay Deductible,then$20Copay
Delivery Deductible,thenNoCharge Deductible,thenNoCharge Deductiblethen$700/dayupto5Days
AI/IVF
AI Deductible,then50%Coinsurance
Deductible,then50%Coinsurance
Deductible,then50%Coinsurance
IVF Deductible,then50%Coinsurance
Deductible,then50%Coinsurance
Deductible,then50%Coinsurance
Vision
AnnualRoutineEyeExam In-Network:$10membercopaywhenexamreceivedfromDavisproviderOut-of-Network:Davispays$33tomemberwhenexamreceivedfromproviderwhoisnotinDavisnetwork
Eyeglasses/ContactLenses DiscountsatparticipatingVisionCenters
RxBenefit Choice
Deductible,then$4/$45/$65or$10/$25/$45;$0genericcopayforprescriptionsrelatedtoDiabetes,Cholesterol,BloodPressure,AsthmaandDepression(andnotsubjecttodeductible)
Option1:AccessthroughaBlueChoicePCPOption2:AccessdirectlytootherprovidersintheBlueChoicenetworkwithoutPCPreferral.Option3:Accesstoout-of-networkprovidersanytimeintheUnitedStates(CareFirstPPOprovidersnotintheBlueChoicenetworkareconsidered
outofnetworkunderMarylandlaw).HealthyBluewillhaveanintegratedmedicalanddrugdeductibleforOption1andallRxwillbetreatedasaOption1.Additionally,thedeductiblesandout-of-pocketmaximumsineachtierwillcontributetowardsoneanother.
*BenefitdesignbasedonMd. 51+RiskHRAavailableasof6/10/10
12

HealthyBluePROVIDERMANUAL
HealthyBlue Identification Cards
TheHealthyBluemembershipidentification(ID)cardprovidesimportantinformationaboutthemember’sbenefitprogram,includingcopaymentamount,authorizationtelephonenumbersandtheclaimssubmissionaddress.
Sample HealthyBlue Triple Option ID Card
13

HealthyBluePROVIDERMANUAL
Sample HealthyBlue Dual Option ID Card
BelowarethedescriptorcodesontheHealthyBlueIDcards:
DESCRIPTOR CODE NARRATIVES
PCP PrimaryCareProvider
S Specialist
ER EmergencyRoomco-paymentamount
RX PrescriptionDrugPlan
DH HMODentalProgram
DN IndemnityDentalProgram
XIM DualOptionPrefix
XIN TripleOptionPrefix
Important Note:Open AccessisnotwrittenontheHealthyBlueidentificationcards(ID),however,allHealthyBlueproductshavetheOpen Accessfeature.
MemberswhoseekcarewithoutareferralmaydosounderOption2orOption3,whereapplicable.
ThosewhoseekcareusingbenefitsinOption 2aresubjecttohigher deductiblesandcopays/coinsurance.ThoseseekingcareusingOption 3 .benefitsaresubjecttothehighest deductibles andcopays/coinsurance.
Remember to Verify Eligibility
PossessionofamembershipIDcarddoes notguaranteecurrenteligibilityforHealthyBluebenefits.UseCareFirst DirectorcallFirstLineat202-479-6560or800-842-5975toverifyeligibilityandbenefitinformationbeforecareisrendered.
14
HealthyBluePROVIDERMANUAL
Referral Process
ThefollowingsectionoutlinestheHealthyBlueReferralProcess.ItisimportanttonotethatwithHealthyBlue,thePCPcoordinatestheentirereferralprocess.AnyreferralssubmittedtoCareFirstBlueChoiceonbehalfofHealthyBluemembersmustbedonebythePCP.ThissectionalsoprovidesinformationonservicesthatdonotrequirereferralsundertheHealthyBlueproduct.
PCP Referral ProcessHealthyBluerequiresthePCPtotakethefollowingstepstocoordinatethereferralprocessformembersandspecialists:
● Completethereferral
● SubmitthereferraltoCareFirstBlueChoiceforHealthyBluemembers
● Givethememberacopyofthereferraltotaketothespecialistvisit
WiththeHealthyBlueOption1benefit,areferralisrequiredformemberstoseeaCareFirstBlueChoicespecialist.WiththeOption2benefit,memberswhoseeaCareFirstBlueChoicespecialistwithoutareferralwillbesubjecttohigherdeductiblesandcopays/coinsurance.
MemberswiththeOption3benefitcanutilizethePPOnetworkorseekcarefromanout-of-network,non-participatingproviderwithoutareferral,howevertheseservicesmaybesubjecttothehighestdeductiblesandcopays/coinsurance.
ThePCPmustmailtheoriginalreferralto:
MailAdministratorP.O.Box14116Lexington,Ky.40512-4116
15
HealthyBluePROVIDERMANUAL
Thefollowinginformationshouldbeincludedonthereferralform:
● Member’sname,dateofbirthandmemberIDnumber
● PCP’sname,phonenumberandCareFirstBlueChoiceprovideridentificationnumber
● Thedatethereferralwasissuedandthe“validuntil”date
● Thediagnosisorchiefcomplaint(stating“follow-up”or“evaluation”isnotsufficient)
● Thenumberofvisitsallowed(ifthisisleftblank,thedefaultnumberofvisitswillbethree)
● Thespecialist’snameandCareFirstBlueChoiceprovideridentificationnumber.
Specialist Referral ProcessThePCPmustensurethatthememberunderstandstowhomheorsheisbeingreferred,thenumberofvisitsallowed(limitedtoamaximumofthree(3)visits)andthetimelimit(validfor120daysfromthedateofissuance)toseekspecialistservices.Specialistsshouldonlyperformtheserviceslistedonthereferralform.Thisincludesauthorizingprocedures,testsandothermedicalservices.The specialist may also refer the member to another CareFirst BlueChoice provider specialist for the same condition for which the initial referral was obtained.
Example: APCPrefersamembertoanorthopedicspecialistforanankleinjury.Theorthopedicspecialistmayreferthemembertoaphysicaltherapistforcarebutonlyfortheankleinjury,theconditionforwhichtheoriginalreferralwaswritten.
Important Note: Services for a new or different condition require an additional referral from the PCP.
IfaparticularproviderorspecialistisnotlistedintheCareFirst BlueChoice Provider Directory,callProviderInformation&Credentialingat410-872-3500or877-269-9593todeterminewhethertheproviderorspecialistparticipatesintheCareFirstBlueChoicenetwork.
Services Not Requiring a ReferralThefollowingservicesdonotrequireawrittenreferral:
● Emergencycareorfollow-upcareafteremergencysurgery
● CoveredservicesrenderedbyaCareFirstBlueChoiceMentalHealthandSubstanceAbuseServicesprovider,includinginpatientfacilityservices,inpatientprofessionalservices,medicationmanagementservices,methadonemaintenanceservices,residentialcrisisfacilityservices,residentialcrisisprofessionalservicesandpartialhospitalizationservices
● Coveredservicesprovidedbyafree-standingCareFirstBlueChoiceradiologistoffice
● CoveredservicesprovidedbyaCareFirstBlueChoicelaboratory
● CovereddiagnostictestingrenderedbyaCareFirstBlueChoiceprovider
● ProstateCancerscreening,ColorectalCancerscreening,BreastCancerscreening,ChlamydiascreeningtestsandHumanPapillomavirusscreeningtestsperformedbyCareFirstBlueChoiceproviders
● Well-childcare,adultpreventivecareandimmunizationsperformedbyCareFirstBlueChoiceproviders
● AmbulatorySurgicalCenters(ASC),AmbulatorySurgicalFacilities
● RoutineobstetricandgynecologicalcarewhenperformedbyaCareFirstBlueChoiceproviderinanofficesetting
● CoveredservicesrenderedbyaCareFirstBlueChoiceproviderophthalmologistfordiagnosisandtreatmentofmedicalconditionsoftheeye
● RoutinevisionexamsbyparticipatingDavisVision(800-783-5602)optometrists
● Visitstoanurgentcarecenter
● CoveredservicesrenderedbyCareFirstBlueChoicelimitedservicesimmediatecarecenters
● CertainprostheticsprovidedbyCareFirstBlueChoiceproviders
16
HealthyBluePROVIDERMANUAL
● DiabeticsuppliesprovidedbyCareFirstBlueChoiceproviders
● Servicesformembersoverage65,whohaveprimarycoveragethroughMedicarePartBandtheirMedicarebenefitshavenotbeenexhausted
Extended (Standing) Referrals
PCPsmayissueanextended,orstanding,referralforaCareFirstBlueChoicememberwhorequiresspecializedcareoveralongperiodoftime.Membersarealloweduptooneyearofunlimitedspecialistvisitsthroughastandingreferralifallofthefollowingcriteriaaremet:
● Memberhasalife-threatening,degenerative,chronicand/ordisablingconditionordiseaserequiringspecializedmedicalcare
● Afterconsultingwiththespecialist,youdeterminewhetherthememberneedscontinuingspecializedcare
● Specialisthasexpertiseintreatingthemember’sconditionandisaparticipatingpractitioner
Ifnecessary,PCPsmaymodifyastandingreferraltolimitthenumberofvisitsortheperiodoftimeforwhichvisitsareapproved.Inaddition,thereferralmayrequirethespecialisttocommunicateregularlywiththePCPregardingthemember’streatmentandhealthstatus.
CareFirstBlueChoicealsoallowsreferralstoallergists,hematologistsoroncologiststobevalidforuptooneyear.Forotherlife-threatening,degenerative,chronicand/ordisablingconditionordiseasesrequiringspecializedmedicalcare,callCaseManagementat410-605-2623or888-264-8648forauthorization.
Anyfollow-upcareprovidedinthespecialist’sofficefollowingthemember’sdischargefromthehospitalrequiresareferral.
Laboratory/Radiology
LabCorp®requisitionformsthatincludethemember’sidentificationnumbermustbeusedwhenorderinglabtestingordirectingmemberstoadrawingstation.SomeexceptionsmayapplyinWesternMarylandandontheEasternShore.
ReferralsareneverrequiredforLabCorp®.ObtaininglaboratoryservicesfromavendorotherthanLabCorp®willresultincoverageattheOption3benefitlevelformembers.
AcompletelistofparticipatinglaboratoryandradiologyfacilitiescanbefoundintheCareFirst BlueChoice Provider Directory.
17
HealthyBluePROVIDERMANUAL
Authorizations
ThefollowingsectionprovidesimportantinformationabouttheCareFirstBlueChoiceHealthyBlueauthorizationprocess.ItisimportanttonotewhichservicesrequireauthorizationsandhowtosecureauthorizationsbeforerenderingcareundertheHealthyBlueproduct.
Services Requiring AuthorizationCallCareManagementat866-PRE-AUTH(773-2884)toobtainallnecessaryauthorizations.Whentheadmittingprovidercallsthehospitaltoscheduleaninpatientorout-patientprocedure,hemustprovidethehospitalwiththefollowinginformation:
● Thenameandtelephonenumberoftheadmittingproviderorsurgeon
● Adiagnosiscode
● AvalidCPTcodeand/ordescriptionoftheprocedurebeingperformed
Authorizationisrequiredforthefollowingservicespendingverificationofeligibilityrequirementsandcoverageunderthemember’sHealthyBluebenefitplan:
● Anyservicesprovidedinasettingotherthanaprovider’soffice,exceptforCareFirstBlueChoicelabandradiologyfacilities,andfreestandingambulatorysurgery/carecenters
● Allinpatienthospitaladmissionsandhospital-basedoutpatientambulatorycareprocedures
● Alldiagnosticorpreoperativetestinginahospitalsetting
● Chemotherapyorintravenoustherapyinasettingotherthanapractitioner’sofficeandbilledbyaproviderotherthanthepractitioner
18

HealthyBluePROVIDERMANUAL
●
●
●
●
●
●
●
●
●
●
●
Durablemedicalequipment(DME)foradiagnosisotherthanasthmaanddiabeteswhenprovidedbyacontractedvendorotherthanNetworkHealthServices(NHS)/NeighborCare
Follow-upcareprovidedbyanon-participatingpractitionerfollowingdischargefromthehospital,withtheexceptionoffollow-upcarefollowingemergencysurgery
Hemodialysis(unlessperformedinaparticipatingfree-standingfacility)
Homehealthcare,homeinfusioncareandhomehospicecarewhenprovidedbyacontractedvendorotherthanNHS/NeighborCare
Inpatienthospicecare
Nutritionalservices(exceptfordiabetesdiagnosis)
Prostheticsandorthoticswhenbilledbyanancillaryprovider,suchasaDMEorsupplyvendor
Radiationoncology(exceptwhenperformedatcontractedfreestandingcenters)
Skillednursingfacilitycare
Treatmentofinfertility(notavailableinDCandVA)
Habilitativeservicesforchildren(MDandDConly)
Note: AuthorizationfromCareManagementisrequiredfortheaboveservices,evenifthememberhasotherprimaryhealthcoverage,suchascommercialcoverage.
Necessary Information
ThehospitalwillprovidethefollowinginformationtoCareManagementforservicesrequiringauthorization:
● Member’sname,addressandtelephonenumber
● Member’sHealthyBlueidentificationnumber
● Member’sdateofbirthandgender
● Member’srelationshiptosubscriber
● Attendingprovider’sname,provideridentificationnumber,addressandtelephonenumber
● Admissiondateandsurgerydate,ifapplicable
●
●
Admittingdiagnosisandprocedureortreatmentplan
Otherhealthcoverage,ifapplicable
Services Not Requiring an AuthorizationAnyserviceperformedataparticipatingfreestandingambulatorysurgical/carecenterorwhenMedicareistheprimarycoveragedoesnotrequireanauthorization.
● EmergencyRoomvisits
● Outpatientservicesnotperformedinahospitaloutpatientdepartment
● Rehabilitationservices
● Spinalmanipulationservices
● Cardiacrehabilitationservices
● Routinematernityadmissions
● Methadonemaintenancetreatment
● DMEimmediateneedsitems
In-Network versus Out-of-Network ProvidersProvidersandspecialistsintheCareFirstBlueChoicenetworkareconsideredin-networkforHealthyBlueOption1andOption2.Memberswhoseekcarein-networkwillreceivethehighestlevelofbenefitswhileloweringtheirout-of-pocketcosts.
ProvidersandspecialistsinanyCareFirstPreferredProviderOrganization(PPO)networkoranynon-participatingproviderareconsideredout-of-network.Ifmemberschooseanout-of-networkprovidertheywillreceiveOption3benefits,whichcouldresultinthehighestdeductible,copay/coinsurance.MemberswiththeDualOptionHSAproductareonlyeligibleforcoveragewithaCareFirstBlueChoiceprovider.
19

HealthyBluePROVIDERMANUAL
Arranging for Care
Thefollowingsectionprovidesinformationonallaspectsofmembercare,fromofficevisitstobenefitguidelines.
Role of the PCPCareFirstBlueChoicerecognizesthatthereisnoonebettersuitedtocoordinatemembers’carethanthePCP.WhenPCPsandmembershavealongstandingmutuallybeneficialrelationship,membersaremoreinclinedtorelyontheirPCP’scounseltomaintainahealthylifestyle.ThiscollaborativerelationshipisattheheartofHealthyBlueandisessentialtoachievingsuccessful,long-term,healthyresults.
WithHealthyBlue,PCPsareattheforefrontofmembers’care.PCPsareinthebestpositiontomakekeyjudgmentsabouttheirmembers’care,includingwhenspecialistsareneededandwhichparticularspecialiststorefermemberstowhentheyseekadditionalcare.
HealthyBluerecognizespractitionersinthefollowingmedicalspecialtiesasPCPs:
● FamilyPractice
● GeneralPractice
● InternalMedicine
● Pediatrics
● Geriatrics
Note for OB/GYN physicians: IfyouareaCareFirstBlueChoiceparticipatingOB/GYNwhoagreestoactasPCPforamember,givethememberaletterstatingyourdecisiontoserveasherPCP.ThelettershouldincludeyourCareFirstBlueChoiceprovidernumberandthemember’sidentificationnumber.ThemembershouldsubmitthelettertoCareFirstMemberServicesforprocessing.
20

HealthyBluePROVIDERMANUAL
EachHealthyBluememberselectsaCareFirstBlueChoicePCPuponenrollmentinHealthyBlueandreceivesaHealthyBlueidentificationcardwiththePCP’snameonit.
IfaPCPnolongerwishestobeamember’sPCP,theprovidermustverifythatheisthecurrentPCP,andnotifyProviderServicesinwriting,priortonotifyingthemember.Sendcorrespondenceto:
MailAdministratorP.O.Box14114Lexington,Ky.40512-4114
AdditionallythePCPmustgivethemember30daysnoticepriortoreleasinghim/herfromcare.AmemberservicesrepresentativewillhelpthememberselectanewPCP.
IfamemberchoosestochangePCPs,themembermustcalltheselectedprovider’sofficetoconfirmthatthePCPparticipateswithCareFirstBlueChoiceandisacceptingnewpatients.ThemembercannotifyMemberServicesofthechangeatwww .carefirst .com/myaccount.Requestsreceivedonorbeforethe20thofthemonthwillbeeffectiveonthefirstdayofthefollowingmonth.Requestsreceivedafterthe20thwillbeeffectiveonthefirstdayofthesecondmonthfollowingtherequest.
Forexample:ChangesreceivedonorbeforeJanuary20willbeeffectiveFebruary1.ChangesreceivedonJanuary21 willbeeffectiveMarch1.NewcardswillbeissuedafterthePCPchangeisprocessed.
Back-up Coverage
WhenthePCPisnotavailabletoprovideservicetomembers,arrangementsmustbemadeforeffectivecoveragethroughanotherpractitionerwhoisaCareFirstBlueChoicePCP.Thecoveringpractitionermustindicateonthepaperclaimform“coveringfor[Dr.’sname]”whensubmittingtheclaimtoCareFirstBlueChoice.
After Hours Care
ThePCPcoveringphysiciansreferencedabovemustprovidetelephoneaccess24hoursaday,sevendaysaweektorespondappropriatelytomembersandotherprovidersconcerning
afterhourscare.Theuseofrecordedphonemessagesinstructingmemberstoproceedtotheemergencyroomduringoff-hoursisnotanacceptablelevelofcareforCareFirstBlueChoicemembersandshouldnotbeused.
Open/Closed Panel
AsstatedinthePhysicianParticipationAgreement,youmaycloseyourpaneltonewmemberswithatleast60dayspriorwrittennoticetoProviderInformationandCredentialing,providedyourpanelincludesatleast200CareFirstBlueChoicemembers.Anasterisk(*)indicatingaclosedpanelwillbeplacedbesidethePCP’snameinthenextprintingoftheproviderdirectory.
Ifyouwishtoacceptanewmemberintoaclosedpanel,youmustnotifyProviderInformationandCredentialinginwriting.Whenyouelecttoreopenyourpaneltonewmembers,writtennotificationisrequired.RequestsforopeningandclosingapanelcanbefaxedtoProviderInformationandCredentialingonyourletterheadto410-872-4107or866-452-2304.
Routine Office VisitsAnnualhealthexaminations,well-childvisitsandotherservicesforthepreventionanddetectionofdiseasearecoveredbenefits.*TheHealthyBlueproductpromotespreventivehealthservicesandCareFirstBlueChoicehasadoptedpreventivehealthrecommendationsapplicabletoourmembers.Examinationssolelyforthepurposesofemployment,insurancecoverage,schoolentryandsportsorcampadmissionaregenerallynotcoveredandshouldbechargedinfulltothemember.Immunizationsrequiredsolelyforforeigntravelaregenerallynotcovered.
PerthetermsoftheParticipationAgreement,non-symptomaticvisits,suchaspreventivecareorroutinewellness,appointmentsshouldbescheduledwithin4weeks.
Note: TheHealthandWellnessEvaluation,alongwithanynecessarytests,musttakeplacewithin 90 daysofthemember’seffectivedate.Boththeinitialevaluationandtheclinicallyappropriatere-screeningareconsideredpreventivevisitsand
shouldbebilledappropriately.
If a PCP no longer wishes
to be a member’s PCP,
the provider must verify
that he is the current
PCP, and notify Provider
Services in writing, prior
to notifying the member.
Send correspondence to:
Mail Administrator
P.O. Box 14114
Lexington, Ky.
40512-4114
*IfamemberaccessescareinOption3therewillbeout-of-pocketcostsfortheservicesrendered.Certaingenericmedicationswillstillbeatnochargeforthemember
21
HealthyBluePROVIDERMANUAL
Emergency Room Services
In-Area Emergencies
Participatingprovidersortheircoveringprovidersarecontractuallyobligatedtobeavailablebytelephone24hoursadaysevendaysaweekshouldCareFirstBlueChoicememberscall911foranylife-threateningemergencies.Membersmaycalltheirprimarycareprovider(PCP),FirstHelp,our24-hourmedicaladvicelineand/orthespecialistinurgentsituations.Membersmayarriveattheemergencyroomoneoffourways:
● PCPorspecialistreferral
● FirstHelpreferral
● Self-referral
● Ambulance
Allmedicallynecessaryemergencyandurgentservicesarecoveredatthesamebenefitlevelregardlessoftheprovider.Priorauthorizationisnotneededforemergencyroomservices.
Referred to Emergency Room by PCP or Specialist
MembersareencouragedtocontacttheirPCPand/orspecialisttoseekguidanceinurgentoremergencymedicalconditions.WhenaPCPorspecialistrefersamembertotheemergencyroom(ER),theERprofessionalswilltriage,treatandbillintheircustomarymanner.AnauthorizationnumberorwrittenreferralfromthePCPorspecialistisnotrequired.
Referred to Emergency Room by FirstHelp
WhenFirstHelp(202-479-6560or800-842-5975)refersamembertotheERfortreatment,theERprofessionalswilltriage,treatandbillintheircustomaryfashion.AnauthorizationnumberorwrittenreferralfromFirstHelpisnotrequired.
Emergency Room Self-Referral
Whenamemberself-referstoanemergencyroom,theprofessionalsshouldtriagethemember.Iftheconditionisdeemedemergent,treatmentisrenderedandtheserviceisbilled.Anauthorizationnumberorwrittenreferralisnotrequired.Pleaserememberthatallsubsequentfollow-upcaremustbeprovidedorcoordinatedbythemember’sPCPorauthorizedbyCareManagement(866-773-2884).
Iftheconditionisdeemedanon-emergency,theemergencyroomprofessionalsshouldencouragethemembertocallhisPCP,specialistorFirstHelpforadviceregardingtreatmentattheappropriatelevelofcare.Professionalservicesshouldbebilledappropriately.
Ambulance
Ifthememberarrivesattheemergencyroombyambulance,theERprofessionalstriage,treatandbillintheircustomarymanner.Anauthorizationnumberorwrittenreferralisnotrequired.
Out-of-Area Emergencies
Itisthemember’sresponsibilitytonotifyCareFirstBlueChoicewithin24hoursafterreceivingout-of-areacare.
Emergency Hospital Admissions
WhenemergencyroomprofessionalsrecommendanemergencyadmissionofaCareFirstBlueChoicemember,theyshouldcontactthemember’sPCPorspecialist,asappropriate.Themember’sprovideristhenexpectedtocommunicatetheappropriatetreatmentforthemember.ThehospitalisrequiredtocontactCareManagementbyfollowingtheEmergencyAdmissionAuthorizationProcesstoverifyand/orsecureauthorization.
In-Area Authorization Process
Thehospitalisresponsibleforinitiatingin-areaauthorizationforallemergencyadmissions.CareManagement(866-773-2884) mustreceivetheauthorizationrequestwithin48hoursafteranemergencyadmissionoronthenextbusinessdayfollowingtheadmission,whicheverislonger.Thisincludesanymedical/surgicalorobstetricaladmissions.
Medicalinformationforacutehospitalcaremustbereceivedbytelephonethenextbusinessdayaftertherequestforauthorizationismade.Ifthememberhasbeendischarged,thehospitalmustprovidemedicalinformationtoCareManagementwithin5businessdays.Failuretoprovidetherequestedinformationmayresultinadenialofauthorizationduetolackofinformation.
22
HealthyBluePROVIDERMANUAL
Out-of-Area Authorization Process
Inthecaseofanout-of-areaemergencyadmission,itisthemember’sresponsibility,ifpossible,tonotifyCareManagementwithin24hoursoftheadmission.
Hospital Services
Authorization Process
Thehospitalisresponsibleforinitiatingallrequestsforauthorizationforinpatientadmissions.However,whentheadmittingproviderscallthehospitaltoscheduleinpatientprocedures,theymustprovidethehospitalwiththefollowinginformation:
● Adiagnosiscode
● AvalidCPTcodeand/ordescriptionoftheprocedurebeingperformed
● Thenameandtelephonenumberoftheadmittingproviderorsurgeon
Theadmittingprovidermustcallthehospitalatleastfivebusinessdayspriortoallelectiveadmissions,exceptwhenitisnotmedicallyfeasibletodelaytreatmentduetothemember’smedicalcondition.CareFirstBlueChoicewillcontacttheadmittingprovider’sofficeifadditionalinformationisneededbeforeapprovingtheauthorization.
Failuretonotifythehospitalwithinthistimeframemayresultinadelayordenialoftheauthorization.
CareManagement(866-773-2884)willobtaintheappropriateinformationfromthehospitalandeitherforwardthecasetotheUtilizationReviewSpecialist(URS)orcertifyaninitiallengthofstayforcertainspecifiedelectiveinpatientsurgicalprocedures.TheURSmustreviewarequestforapreoperativeday.On-sitehospitalreview(concurrentreview)isperformedatselectedhospitalsandonacase-by-casebasis.
Ifthedateforanelectiveadmissionchanges,CareManagementmustbenotifiedbythehospitalassoonaspossible,butnolaterthanonebusinessdaypriortotheadmission.Lackofnotificationmayresultinadenialofauthorization.
Preoperative Testing Services
Preoperativelaboratoryservicesauthorizedinthehospitalsettingareasfollows:
● Typeandcrossmatchingofblood
● Laboratoryservicesforchildrenundertheageofeight
AllotherpreoperativetestingmustbeprocessedbyLabCorp®orperformedatparticipatingfreestandingradiologycenters.SomeexceptionsapplyinWesternMarylandandontheEasternShore.
Hospitalist Services Available
CareFirstBlueChoiceoffersavoluntary,diagnosis-specifichospitalistprogramtomembersinselectedhospitalsthroughanagreementwithMDxL,acompanythatspecializesinemergencyinpatientandoutpatientcare.
InpatientcarerequiresthehospitaltoobtainauthorizationfromCareManagement(866-773-2884).MDxLprovideshospitalistservicestomemberswhoareadmittedtoahospitalthroughtheemergencyroom.Ourprogramisofferedatthefollowinghospitals:
● DoctorsCommunityHospital–Lanham,Md.
● HolyCrossHospital–SilverSpring,Md.
● LaurelRegionalHospital–Laurel,Md.
● MontgomeryGeneralHospital–Olney,Md.
● PrinceGeorge’sHospitalCenter–Cheverly,Md.
● ShadyGroveAdventistHospital–Rockville,Md.
● SouthernMarylandHospitalCenter–Clinton,Md.
● SuburbanHospital–Bethesda,Md.
● WashingtonAdventistHospital–TacomaPark,Md.
Hospitalistscoordinatethemember’stestsandspecialtycare,communicatewiththemember’sPCPandinsuranceprovidersandplanthemember’sdischarge,homecare,hospiceorassistedlivingarrangement.
23
HealthyBluePROVIDERMANUAL
Discharge Planning Process
Thehospitalorattendingproviderisresponsibleforinitiatingadischargeplanasacomponentofthemember’streatmentplan.Thehospital,underthedirectionoftheattendingprovider,shouldcoordinateanddiscussaneffectiveandsafedischargeplanwithCareManagementandeachmemberand/orfamilymemberassoonafteradmissionaspossible.Dischargeneedsshouldbeassessedandadischargeplandevelopedpriortoadmissionforelectiveadmissions.
Referralstohospitalsocialworkers,long-termcareplanners,dischargeplannersorhospitalcasemanagersshouldbemadepromptlyafteradmissionandcoordinatedwithCareManagement.
Anappropriatedischargeplanshouldinclude:
● Fullassessmentofthemember’sclinicalconditionandpsychosocialstatus
● Level,frequencyandtypeofskilledservicecareneeds
● Verificationofmember’scontractualhealthcarebenefits
● ReferraltoaCareFirstBlueChoiceparticipatingprovider,ifneeded
● Alternativefinancialorsupportarrangements,ifbenefitsarenotavailable
Outpatient Hospital Services
Authorizationisrequiredforalloutpatientservices,includinglaboratoryandradiologyperformedinahospitalsetting.Youmustperformorarrangeallpre-operativeservicesforyourmembers.SomeexceptionsmayapplyinWesternMarylandandontheEasternShore.
Notethefollowing:
● Thehospitalisresponsibleforinitiatingallrequestsforauthorizationforoutpatientservices(e.g.,surgery,false-labor/observation).
● Ifauthorizationcriteriaaremet,authorizationwillbeissued.Inaddition,thecallerwillbeinstructedwhetherthememberisaccessingin-networkorout-of-networkbenefits.Therewillbeinstancesinwhichthememberwillbedirectedtoamoreappropriatenetworkproviderforcertainservices(i.e.,laboratory,radiologicalservices).
Iftheadmissiondateforanoutpatientelectiveprocedurechanges,thehospitalmustnotifyCareManagement(866-773-2884)assoonaspossible,butnolaterthanonebusinessdaypriortotheprocedure.Lackofnotificationmayresultintheclaimbeingdenied.
Disease Management
DiseaseManagementprograms,suchasthosefordiabetesandasthma,identifymemberswithpotentiallylong-termconditionsandoffereducationaboutandmanagementoftheirdiseasesthatwillsignificantlyimpacttheirmedicaloutcomeandqualityoflife.
ThefollowingimpactconditionsareapartoftheDiseaseManagementoffering:
● Asthma
● Diabetes
● Heartfailure
● Coronaryarterydisease
● ChronicObstructivePulmonaryDisease(COPD)
CallCaseManagementat410-605-2623or888-264-8648toobtainmoreinformationortoreferamembertotheoncologyprogram.
Case Management Care Coordination
CaseManagementisdesignedtoidentify,asearlyaspossible,memberswhorequiremoreinvolvedcoordinationofcareduetoacatastrophic,chronic,progressiveorhighriskacuteillness.CaseManagementcoordinatestheuseofhealthcarebenefitstocreateaplanofcarethatmaximizesbenefitseffectivelywithoutcompromisingthequalityofcare.Refermemberswhowouldbenefitfromtheseservicesassoonastheyareidentified.
CaseManagementinterventionisappropriateformemberswiththefollowingconditions:
● Catastrophic,progressive,chronicorlife-threateningdiseases
● Continuouscareduetoacatastrophiceventoranacuteexacerbationofachronicillness
● Extendedacutecarehospitalizations
● Repeathospitaladmissionswithinalimitedtimeperiod
TheCaseManagerpreparesandcoordinatesacareplanincollaborationwiththemember,his/
24

HealthyBluePROVIDERMANUAL
herPCP,otherprovidersandfamily.TheCaseManagerwillensurethatthecareplaniswithinthemember’sexistingbenefits.
ContactCaseManagementat410-605-2623or888-264-8648ifyouareinterestedintheirservices,ortoreferamember.
Benefits, Exclusions and Limitations
Covered Services and Benefit Guidelines
CareFirstBlueChoiceexpectsthatallproviderswhoperformlaboratoryorimagingtests,atanysitewillobtainand/ormaintaintheappropriatefederal,state,andlocallicensesandcertifications,training,qualitycontrolsandsafetystandardspertinenttothetestsperformed.
AdditionalinformationaboutcoveredservicesandbenefitsguidelinesisavailableintheMedical Policy Reference Manual,thePolicysectionandtheBasicClaimAdjudicationPolicyConceptssection(pg.15)oftheGeneral Information Manual.Ifyouhaveadditionalquestions,contactaProviderServicesrepresentativeat202-479-6560or800-842-5975.
VisitCareFirst DirectorcallFirstLine(202-479-6560or800-842-5975)todeterminethemember’seligibilityandlevelofcoveragepriortoadministeringthefollowingservices.
Abortion
AnauthorizationfromCareManagementisrequiredtoperformanabortioninahospitalsetting.Itisnotrequiredifperformedinaprovider’soffice.Benefitsforabortionsarenotavailableunderallprograms.
Allergy
Allergyservicesrequireawrittenreferral.Youmayissuealong-standingreferralforallergyservices.Allergyconsultation,injections,testingandserumaregenerallycovered.PCPsmayadministerallergyinjectionsandmustmaintainappropriateemergencydrugsandequipmentonsite.
Alternative Therapies
OptionsandBlue365arediscountprogramsthatoffermembershealthandwellnessinformation,support,andservices,inadditiontospecialsavings.Note:Referralsarenotneededfortheseprograms.
Discountsinclude:
● Acupuncture
● Chiropracticcare
● Eldercareservices
● Fitnesscenters
● Hearingcareservices
● Laservisioncorrection
● Mailordercontactlenses
● Massagetherapy
Ambulance
Ambulanceservicesinvolvetheuseofspecially-designedandequippedvehiclestotransportillorinjuredmembers.Benefitsforambulanceservicesareprovidedformedicallynecessaryambulancetransport.ServicesmustbeauthorizedthroughCareManagement,exceptinemergencysituations.
Emergencyambulanceservicesareconsideredmedicallynecessarywhenthemember’sconditionissuchthatanyotherformoftransportationwouldbemedicallycontraindicatedandendangerthemember’shealth.Formoreinformation,pleaserefertotheadministrativeservicessectionoftheMedical Policy Reference Manual.LookintheTableofContentsforMedicalPolicy 10.01.005,AmbulanceServices.
Anesthesia
CareFirstBlueChoiceprovidesbenefitsforanesthesiachargesrelatedtocoveredsurgicalproceduresandforpainmanagement.Authorizationforanesthesiaduringsurgeryisincludedintheauthorizationforthesurgery.AreferralfromthePCPisrequiredforpainmanagementservicesrenderedinaprovider’soffice.
Formoreinformationaboutreportinganesthesiaservices,refertoanesthesiapoliciesinSection9oftheMedical Policy Reference Manual.
25
HealthyBluePROVIDERMANUAL
Procedure Codes – CardiologyPROCEDURE CODE EFFECTIVE DATE PROCEDURE CODE EFFECTIVE DATE
76825 addedpriorto1/1/08 78469 addedpriorto1/1/08
76826 addedpriorto1/1/08 78472 addedpriorto1/1/08
76827 addedpriorto1/1/08 78473 addedpriorto1/1/08
76828 addedpriorto1/1/08 78478 invalidasof1/1/08
78414 addedpriorto1/1/08 78480 invalidasof1/1/08
78428 addedpriorto1/1/08 78481 addedpriorto1/1/08
78445 addedpriorto1/1/08 78483 addedpriorto1/1/08
78451 added1/1/08 78491 addedpriorto1/1/08
78452 added1/1/08 78492 addedpriorto1/1/08
78453 added1/1/08 78494 addedpriorto1/1/08
78454 added1/1/08 78496 addedpriorto1/1/08
78455 invalidasof1/1/08 78990 invalidasof1/1/08
78456 addedpriorto1/1/08 A9500 addedpriorto1/1/08
78457 addedpriorto1/1/08 A9501 added1/1/08
78458 addedpriorto1/1/08 A9502 addedpriorto1/1/08
78459 addedpriorto1/1/08 A9503 addedpriorto1/1/08
78460 invalidasof1/1/08 A9505 addedpriorto1/1/08
78461 invalidasof1/1/08 A9508 addedpriorto1/1/08
78464 invalidasof1/1/08 A9510 addedpriorto1/1/08
78465 invalidasof1/1/08 A9600 addedpriorto1/1/08
78466 addedpriorto1/1/08 A9700 addedpriorto1/1/08
78468 addedpriorto1/1/08
Refer to your current
CPT® code book for
descriptions.
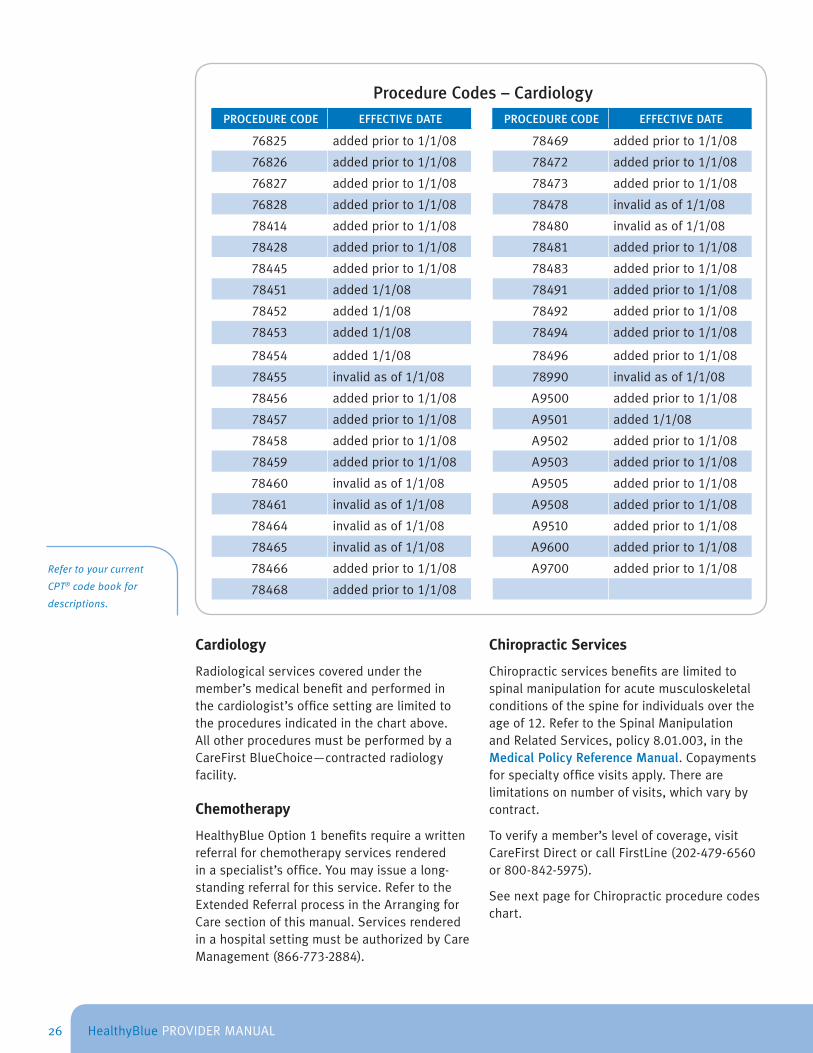
Cardiology
Radiologicalservicescoveredunderthemember’smedicalbenefitandperformedinthecardiologist’sofficesettingarelimitedtotheproceduresindicatedinthechartabove.AllotherproceduresmustbeperformedbyaCareFirstBlueChoice—contractedradiologyfacility.
Chemotherapy
HealthyBlueOption1benefitsrequireawrittenreferralforchemotherapyservicesrenderedinaspecialist’soffice.Youmayissuealong-standingreferralforthisservice.RefertotheExtendedReferralprocessintheArrangingforCaresectionofthismanual.ServicesrenderedinahospitalsettingmustbeauthorizedbyCareManagement(866-773-2884).
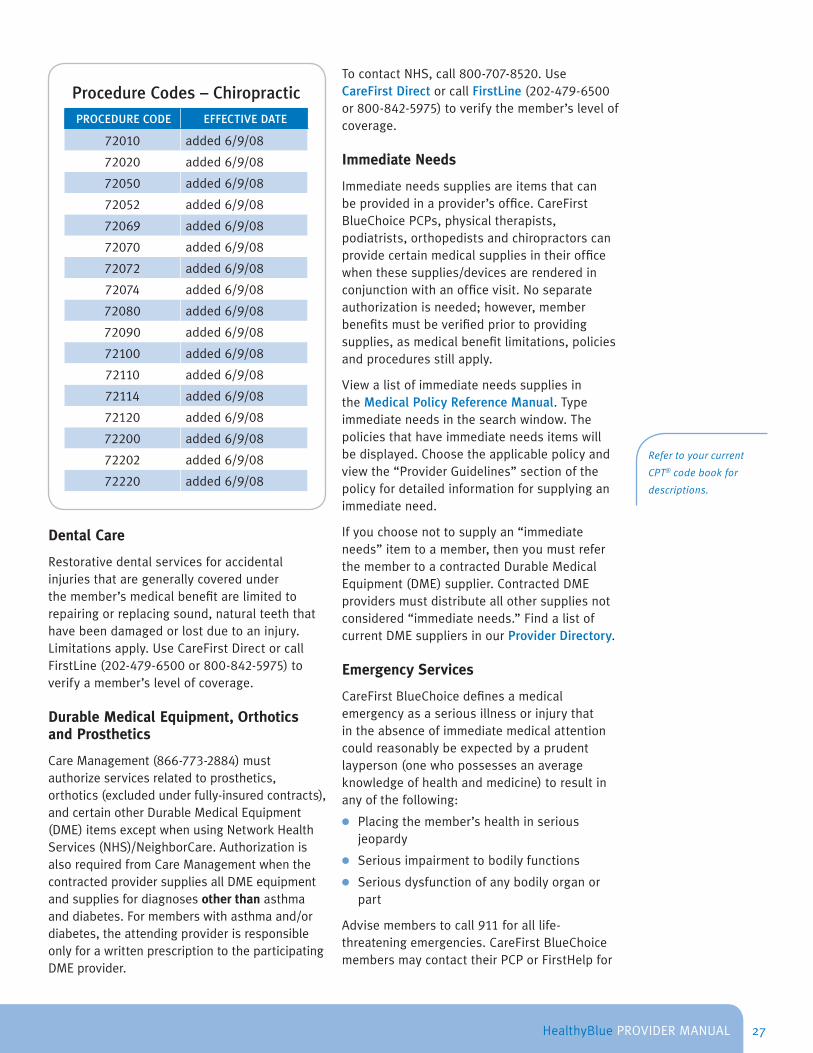
Chiropractic Services
Chiropracticservicesbenefitsarelimitedtospinalmanipulationforacutemusculoskeletalconditionsofthespineforindividualsovertheageof12.RefertotheSpinalManipulationandRelatedServices,policy8.01.003,intheMedical Policy Reference Manual.Copaymentsforspecialtyofficevisitsapply.Therearelimitationsonnumberofvisits,whichvarybycontract.
Toverifyamember’slevelofcoverage,visitCareFirstDirectorcallFirstLine(202-479-6560or800-842-5975).
SeenextpageforChiropracticprocedurecodeschart.
26
HealthyBluePROVIDERMANUAL
Procedure Codes – ChiropracticPROCEDURE CODE EFFECTIVE DATE
72010 added6/9/08
72020 added6/9/08
72050 added6/9/08
72052 added6/9/08
72069 added6/9/08
72070 added6/9/08
72072 added6/9/08
72074 added6/9/08
72080 added6/9/08
72090 added6/9/08
72100 added6/9/08
72110 added6/9/08
72114 added6/9/08
72120 added6/9/08
72200 added6/9/08
72202 added6/9/08
72220 added6/9/08
Dental Care
Restorativedentalservicesforaccidentalinjuriesthataregenerallycoveredunderthemember’smedicalbenefitarelimitedtorepairingorreplacingsound,naturalteeththathavebeendamagedorlostduetoaninjury.Limitationsapply.UseCareFirstDirectorcallFirstLine(202-479-6500or800-842-5975)toverifyamember’slevelofcoverage.
Durable Medical Equipment, Orthotics and Prosthetics
CareManagement(866-773-2884)mustauthorizeservicesrelatedtoprosthetics,orthotics(excludedunderfully-insuredcontracts),andcertainotherDurableMedicalEquipment(DME)itemsexceptwhenusingNetworkHealthServices(NHS)/NeighborCare.AuthorizationisalsorequiredfromCareManagementwhenthecontractedprovidersuppliesallDMEequipmentandsuppliesfordiagnosesother thanasthmaanddiabetes.Formemberswithasthmaand/ordiabetes,theattendingproviderisresponsibleonlyforawrittenprescriptiontotheparticipatingDMEprovider.
TocontactNHS,call800-707-8520.UseCareFirst DirectorcallFirstLine(202-479-6500or800-842-5975)toverifythemember’slevelofcoverage.
Immediate Needs
Immediateneedssuppliesareitemsthatcanbeprovidedinaprovider’soffice.CareFirstBlueChoicePCPs,physicaltherapists,podiatrists,orthopedistsandchiropractorscanprovidecertainmedicalsuppliesintheirofficewhenthesesupplies/devicesarerenderedinconjunctionwithanofficevisit.Noseparateauthorizationisneeded;however,memberbenefitsmustbeverifiedpriortoprovidingsupplies,asmedicalbenefitlimitations,policiesandproceduresstillapply.
ViewalistofimmediateneedssuppliesintheMedical Policy Reference Manual.Typeimmediateneedsinthesearchwindow.Thepoliciesthathaveimmediateneedsitemswillbedisplayed.Choosetheapplicablepolicyandviewthe“ProviderGuidelines”sectionofthepolicyfordetailedinformationforsupplyinganimmediateneed.
Ifyouchoosenottosupplyan“immediateneeds”itemtoamember,thenyoumustreferthemembertoacontractedDurableMedicalEquipment(DME)supplier.ContractedDMEprovidersmustdistributeallothersuppliesnotconsidered“immediateneeds.”FindalistofcurrentDMEsuppliersinourProvider Directory.
Emergency Services
CareFirstBlueChoicedefinesamedicalemergencyasaseriousillnessorinjurythatintheabsenceofimmediatemedicalattentioncouldreasonablybeexpectedbyaprudentlayperson(onewhopossessesanaverageknowledgeofhealthandmedicine)toresultinanyofthefollowing:
● Placingthemember’shealthinseriousjeopardy
● Seriousimpairmenttobodilyfunctions
● Seriousdysfunctionofanybodilyorganorpart
Advisememberstocall911foralllife-threateningemergencies.CareFirstBlueChoicemembersmaycontacttheirPCPorFirstHelpfor
Refer to your current
CPT® code book for
descriptions.
27
HealthyBluePROVIDERMANUAL
instructionsormedicaladvice.Ifthemember’smedicalconditionseemslessserious,theemergencyprovidermayelecttodirectthemembertoreceivecareatoneofthefollowinglocations:
● ThePCP’soffice
● Anotherparticipatingprovider’soffice(writtenreferralmayberequired)
● Anurgentcarecenter
Copaysaregenerallyrequiredforemergencyservices;however,thecopayiswaivedifthememberisadmittedtothehospital.
Youoryourcoveringprovideriscontractuallyobligatedtobeavailablebytelephone24hoursaday,7daysaweekformemberinquiries.Theuseofrecordedphonemessagesinstructingmemberstoproceedtotheemergencyroomduringoff-hoursisnotanacceptablelevelofcareforCareFirstBlueChoicemembersandshouldnotbeused.
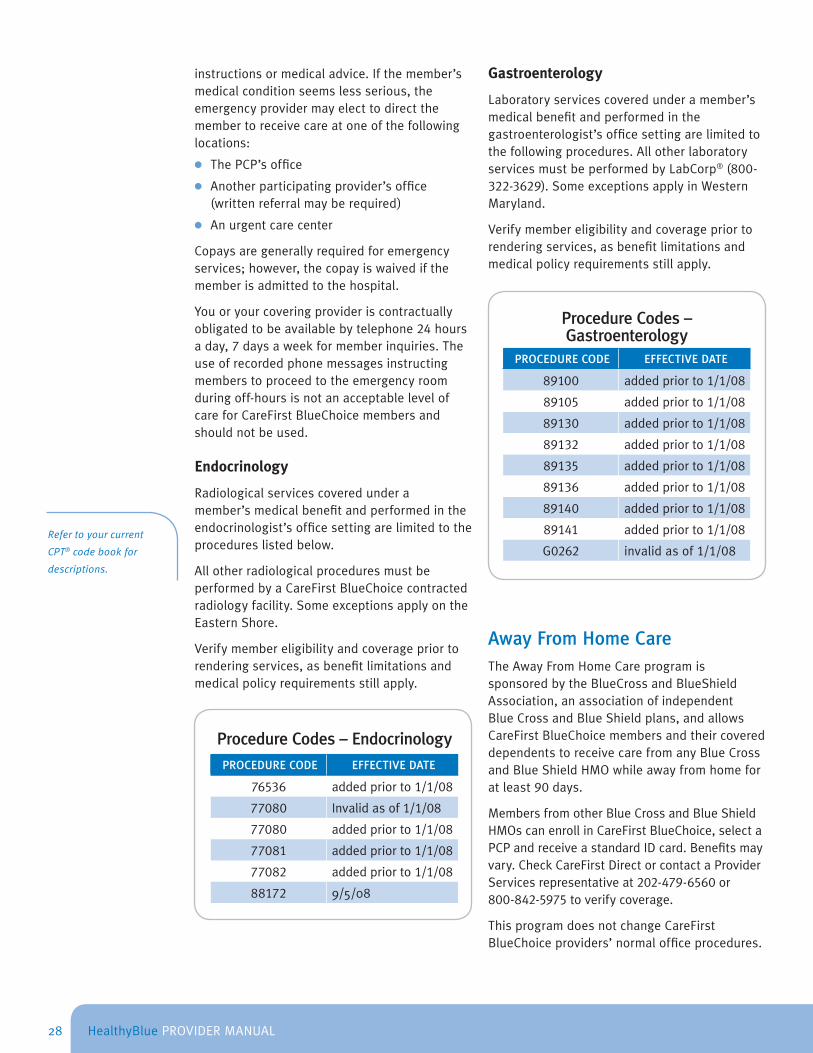
Endocrinology
Radiologicalservicescoveredunderamember’smedicalbenefitandperformedintheendocrinologist’sofficesettingarelimitedtotheprocedureslistedbelow.
AllotherradiologicalproceduresmustbeperformedbyaCareFirstBlueChoicecontractedradiologyfacility.SomeexceptionsapplyontheEasternShore.
Verifymembereligibilityandcoveragepriortorenderingservices,asbenefitlimitationsandmedicalpolicyrequirementsstillapply.
Refer to your current
CPT® code book for
descriptions.
Procedure Codes – EndocrinologyPROCEDURE CODE EFFECTIVE DATE
76536 addedpriorto1/1/08
77080 Invalidasof1/1/08
77080 addedpriorto1/1/08
77081 addedpriorto1/1/08
77082 addedpriorto1/1/08
88172 9/5/08
Gastroenterology
Laboratoryservicescoveredunderamember’smedicalbenefitandperformedinthegastroenterologist’sofficesettingarelimitedtothefollowingprocedures.AllotherlaboratoryservicesmustbeperformedbyLabCorp®(800-322-3629).SomeexceptionsapplyinWesternMaryland.
Verifymembereligibilityandcoveragepriortorenderingservices,asbenefitlimitationsandmedicalpolicyrequirementsstillapply.
Procedure Codes – Gastroenterology
PROCEDURE CODE EFFECTIVE DATE
89100 addedpriorto1/1/08
89105 addedpriorto1/1/08
89130 addedpriorto1/1/08
89132 addedpriorto1/1/08
89135 addedpriorto1/1/08
89136 addedpriorto1/1/08
89140 addedpriorto1/1/08
89141 addedpriorto1/1/08
G0262 invalidasof1/1/08
Away From Home CareTheAwayFromHomeCareprogramissponsoredbytheBlueCrossandBlueShieldAssociation,anassociationofindependentBlueCrossandBlueShieldplans,andallowsCareFirstBlueChoicemembersandtheircovereddependentstoreceivecarefromanyBlueCrossandBlueShieldHMOwhileawayfromhomeforatleast90days.
MembersfromotherBlueCrossandBlueShieldHMOscanenrollinCareFirstBlueChoice,selectaPCPandreceiveastandardIDcard.Benefitsmayvary.CheckCareFirstDirectorcontactaProviderServicesrepresentativeat202-479-6560or800-842-5975toverifycoverage.
ThisprogramdoesnotchangeCareFirstBlueChoiceproviders’normalofficeprocedures.
28
HealthyBluePROVIDERMANUAL
Guest Membership Program
TheguestmembershipprogramissponsoredbytheBlueCrossandBlueShieldAssociation,anassociationofindependentBlueCrossandBlueShieldplans.TheprogramallowsCareFirstBlueChoicemembersandtheircovereddependentstoreceivecarefromanyBlueCrossandBlueShieldHMOwhileawayfromhomeforatleast90days.
MembersfromotherBlueCrossandBlueShieldHMOscanenrollinCareFirstBlueChoice,selectaPCPandreceiveastandardIDcard.Benefitsmayvary;itisimportanttoverifythemember’scoverageatCareFirstDirectorcontactProviderServices.ThisprogramdoesnotchangeCareFirstBlueChoiceproviders’normalofficeprocedures.
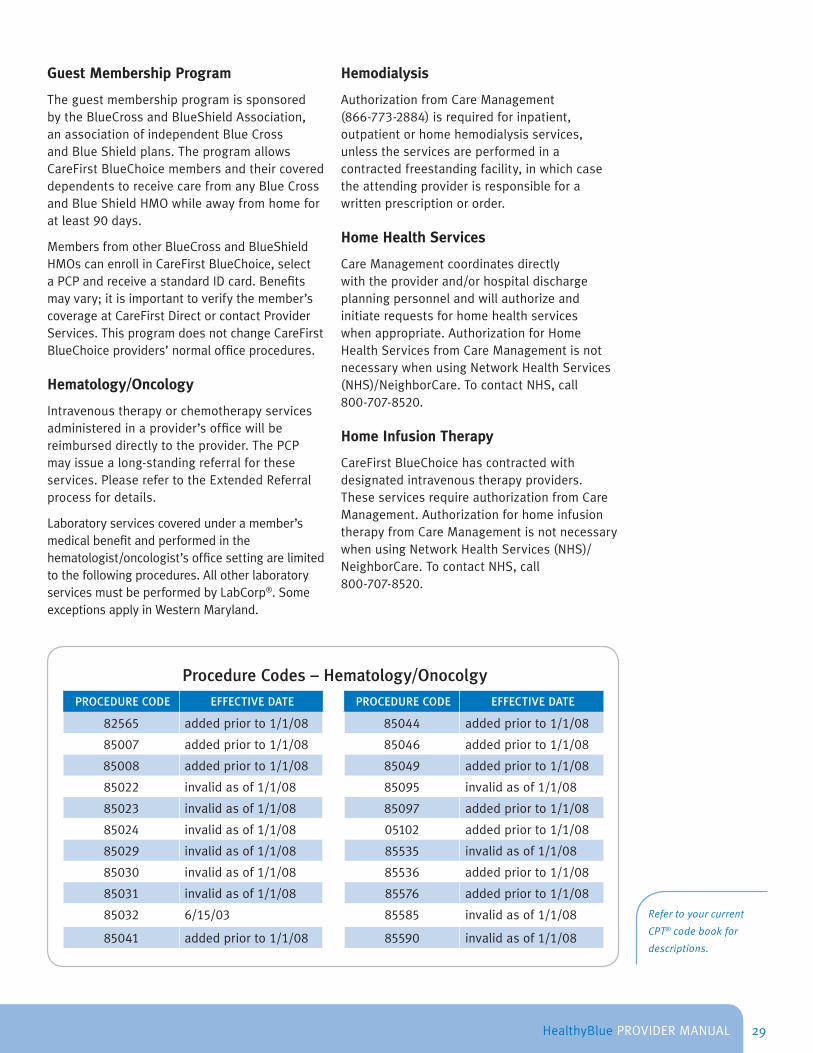
Hematology/Oncology
Intravenoustherapyorchemotherapyservicesadministeredinaprovider’sofficewillbereimburseddirectlytotheprovider.ThePCPmayissuealong-standingreferralfortheseservices.PleaserefertotheExtendedReferralprocessfordetails.
Laboratoryservicescoveredunderamember’smedicalbenefitandperformedinthehematologist/oncologist’sofficesettingarelimitedtothefollowingprocedures.AllotherlaboratoryservicesmustbeperformedbyLabCorp®.SomeexceptionsapplyinWesternMaryland.
Hemodialysis
AuthorizationfromCareManagement(866-773-2884)isrequiredforinpatient,outpatientorhomehemodialysisservices,unlesstheservicesareperformedinacontractedfreestandingfacility,inwhichcasetheattendingproviderisresponsibleforawrittenprescriptionororder.
Home Health Services
CareManagementcoordinatesdirectlywiththeproviderand/orhospitaldischargeplanningpersonnelandwillauthorizeandinitiaterequestsforhomehealthserviceswhenappropriate.AuthorizationforHomeHealthServicesfromCareManagementisnotnecessarywhenusingNetworkHealthServices(NHS)/NeighborCare.TocontactNHS,call800-707-8520.
Home Infusion Therapy
CareFirstBlueChoicehascontractedwithdesignatedintravenoustherapyproviders.TheseservicesrequireauthorizationfromCareManagement.AuthorizationforhomeinfusiontherapyfromCareManagementisnotnecessarywhenusingNetworkHealthServices(NHS)/NeighborCare.TocontactNHS,call800-707-8520.
Procedure Codes – Hematology/OnocolgyPROCEDURE CODE EFFECTIVE DATE PROCEDURE CODE EFFECTIVE DATE
82565 addedpriorto1/1/08 85044 addedpriorto1/1/08
85007 addedpriorto1/1/08 85046 addedpriorto1/1/08
85008 addedpriorto1/1/08 85049 addedpriorto1/1/08
85022 invalidasof1/1/08 85095 invalidasof1/1/08
85023 invalidasof1/1/08 85097 addedpriorto1/1/08
85024 invalidasof1/1/08 05102 addedpriorto1/1/08
85029 invalidasof1/1/08 85535 invalidasof1/1/08
85030 invalidasof1/1/08 85536 addedpriorto1/1/08
85031 invalidasof1/1/08 85576 addedpriorto1/1/08
85032 6/15/03 85585 invalidasof1/1/08
85041 addedpriorto1/1/08 85590 invalidasof1/1/08
Refer to your current
CPT® code book for
descriptions.
29

HealthyBluePROVIDERMANUAL
Hospice Care
Memberswithlifeexpectanciesofsixmonthsorlessmaybeeligibleforhospicecare.CallCareManagementforauthorization.AuthorizationforhospicecarefromCareManagementisnotnecessarywhenusingNetworkHealthServices(NHS)/NeighborCare.TocontactNHS,call800-707-8520.
House Calls
WhenaproviderdeterminesthatahousecallisnecessaryfortreatingaCareFirstBlueChoicemember,copayisrequired.Basedonprovider’sspecialty,collecttheappropriatecopaylistedonthemember’sHealthyBlueIDcard.Areferralisrequiredforaspecialisttovisitthehome.UsetheappropriateEvaluation&Managementhomevisitprocedurecode.
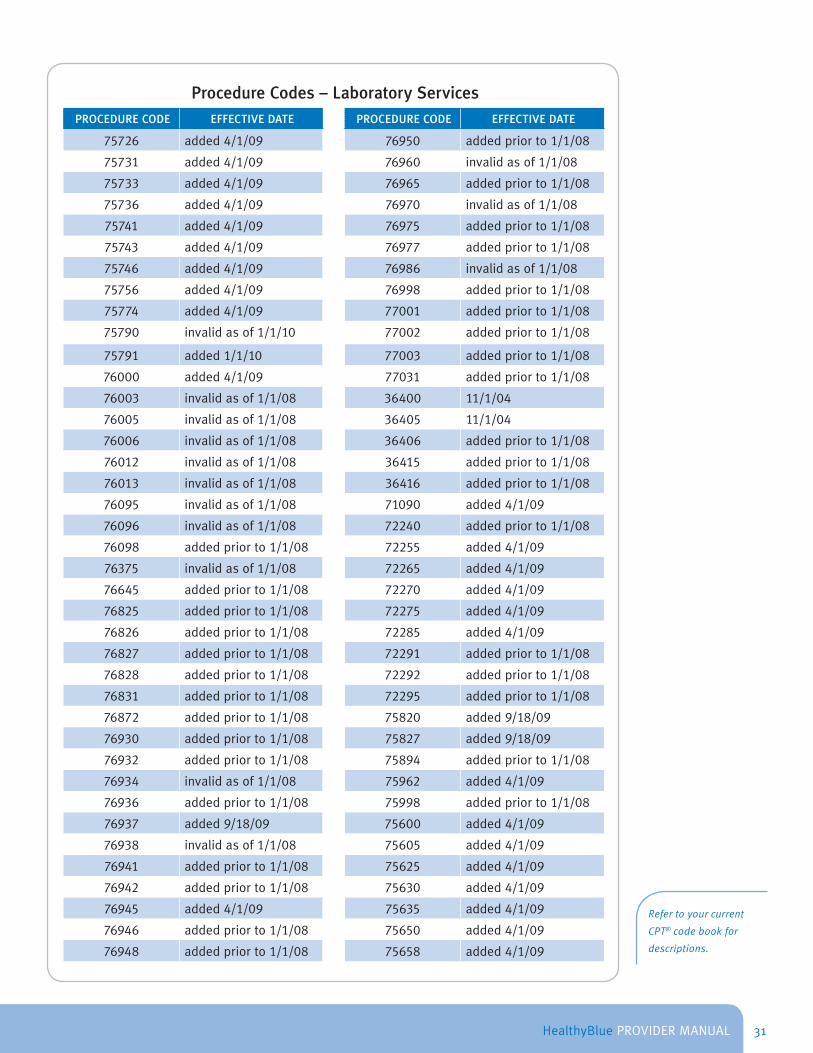
Laboratory ServicesPCPsandspecialistsarerequiredtouseLaboratoryCorporationofAmerica(LabCorp®)foroutpatientlaboratoryservicesthatarenotlistedonthechartbeginningonpage31.Therequiredlaboratoryrequisitionformsmustaccompanylabspecimenscollectedintheprovider’soffice.TherequisitionformmustincludethemembershipIDnumberexactlyasitappearsontheIDcard.Indicatethemember’sinsurancecompanyasCareFirstBlueChoice.PCPsmayalsorefermemberstodesignateddrawingsiteswiththerequiredlaboratoryrequisitionforms.
CallLabCorp®at 800-322-3629toobtaincopiesoftherequisitionform.
RefertotheProvider DirectoryorcallLabCorp®fordesignatedlocations.Laboratoryservicescoveredunderamember’smedicalbenefitandperformedinthePCPorspecialist’sofficesettingarelimitedtotheprocedurecodeslisted.AllotherlaboratoryservicesmustbeperformedbyLabCorp®.SomeexceptionsapplyinWesternMaryland.
WithHealthyBluelaboratoryservicesperformedinanoutpatienthospitalsettingrequirepriorauthorizationwithOption1,butnotinOption2or3.Membersmaybesubjectedtohigherdeductiblesand/orcopaysinOption2.CareFirstmemberswhoseeklaboratoryservicesatafacilityotherthanLabCorp®inOption3maybesubjecttothehighestdeductiblesandcopays/coinsurance.
ProviderswhoperformlaboratoryservicesintheirofficeshouldmaintaintheappropriatelevelofClinicalLaboratoryImprovementAmendmentscertification.FormoreinformationonCLIA,pleasevisithttp://www .fda .gov/cdrh/clia/.
Verifymembereligibilityandcoveragepriortorenderingservices,asbenefitlimitationsandmedicalpolicyrequirementsstillapply.
Mental Health/Substance Abuse Services
MagellanBehavioralHealthServices(800-245-7013)administersallmentalhealthandsubstanceabusebenefitsforCareFirstBlueChoicemembers.
30
HealthyBluePROVIDERMANUAL
Procedure Codes – Laboratory ServicesPROCEDURE CODE EFFECTIVE DATE PROCEDURE CODE EFFECTIVE DATE
75726 added4/1/09 76950 addedpriorto1/1/08
75731 added4/1/09 76960 invalidasof1/1/08
75733 added4/1/09 76965 addedpriorto1/1/08
75736 added4/1/09 76970 invalidasof1/1/08
75741 added4/1/09 76975 addedpriorto1/1/08
75743 added4/1/09 76977 addedpriorto1/1/08
75746 added4/1/09 76986 invalidasof1/1/08
75756 added4/1/09 76998 addedpriorto1/1/08
75774 added4/1/09 77001 addedpriorto1/1/08
75790 invalidasof1/1/10 77002 addedpriorto1/1/08
75791 added1/1/10 77003 addedpriorto1/1/08
76000 added4/1/09 77031 addedpriorto1/1/08
76003 invalidasof1/1/08 36400 11/1/04
76005 invalidasof1/1/08 36405 11/1/04
76006 invalidasof1/1/08 36406 addedpriorto1/1/08
76012 invalidasof1/1/08 36415 addedpriorto1/1/08
76013 invalidasof1/1/08 36416 addedpriorto1/1/08
76095 invalidasof1/1/08 71090 added4/1/09
76096 invalidasof1/1/08 72240 addedpriorto1/1/08
76098 addedpriorto1/1/08 72255 added4/1/09
76375 invalidasof1/1/08 72265 added4/1/09
76645 addedpriorto1/1/08 72270 added4/1/09
76825 addedpriorto1/1/08 72275 added4/1/09
76826 addedpriorto1/1/08 72285 added4/1/09
76827 addedpriorto1/1/08 72291 addedpriorto1/1/08
76828 addedpriorto1/1/08 72292 addedpriorto1/1/08
76831 addedpriorto1/1/08 72295 addedpriorto1/1/08
76872 addedpriorto1/1/08 75820 added9/18/09
76930 addedpriorto1/1/08 75827 added9/18/09
76932 addedpriorto1/1/08 75894 addedpriorto1/1/08
76934 invalidasof1/1/08 75962 added4/1/09
76936 addedpriorto1/1/08 75998 addedpriorto1/1/08
76937 added9/18/09 75600 added4/1/09
76938 invalidasof1/1/08 75605 added4/1/09
76941 addedpriorto1/1/08 75625 added4/1/09
76942 addedpriorto1/1/08 75630 added4/1/09
76945 added4/1/09 75635 added4/1/09
76946 addedpriorto1/1/08 75650 added4/1/09
76948 addedpriorto1/1/08 75658 added4/1/09
Refer to your current
CPT® code book for
descriptions.
31

HealthyBluePROVIDERMANUAL
Procedure Codes – Laboratory ServicesPROCEDURE CODE EFFECTIVE DATE PROCEDURE CODE EFFECTIVE DATE
75660 added4/1/09 84830 addedpriorto1/1/08
75662 added4/1/09 85002 addedpriorto1/1/08
75665 added4/1/09 85007 addedpriorto1/1/08
75671 added4/1/09 85013 addedpriorto1/1/08
75676 added4/1/09 85014 addedpriorto1/1/08
75680 added4/1/09 85018 addedpriorto1/1/08
75685 added4/1/09 85021 invalidasof1/1/08
75705 added4/1/09 85023 invalidasof1/1/08
75710 added4/1/09 85024 invalidasof1/1/08
75716 added4/1/09 85025 addedpriorto1/1/08
75722 added4/1/09 85027 addedpriorto1/1/08
75724 added4/1/09 85095 invalidasof1/1/08
77032 addedpriorto1/1/08 85102 invalidasof1/1/08
77071 addedpriorto1/1/08 85610 addedpriorto1/1/08
78800 added4/1/09 85651 addedpriorto1/1/08
78801 added4/1/09 86308 addedpriorto1/1/08
81000 addedpriorto1/1/08 86315 invalidasof1/1/08
81001 addedpriorto1/1/08 86403 addedpriorto1/1/08
81002 addedpriorto1/1/08 86580 addedpriorto1/1/08
81003 addedpriorto1/1/08 86585 invalidasof1/1/08
81015 addedpriorto1/1/08 86588 invalidasof1/1/08
81020 addedpriorto1/1/08 86759 addedpriorto1/1/08
81025 addedpriorto1/1/08 87081 addedpriorto1/1/08
81050 addedpriorto1/1/08 87177 addedpriorto1/1/08
82044 8/1/05 87205 addedpriorto1/1/08
82247 addedpriorto1/1/08 87208 invalidasof1/1/08
82250 invalidasof1/1/08 87210 addedpriorto1/1/08
82270 addedpriorto1/1/08 87211 invalidasof1/1/08
82272 1/6/06 87220 addedpriorto1/1/08
82274 1/6/06 87430 addedpriorto1/1/08
82438 addedpriorto1/1/08 87449 addedpriorto1/1/08
82570 8/1/05 87450 addedpriorto1/1/08
82757 addedpriorto1/1/08 87451 addedpriorto1/1/08
82948 addedpriorto1/1/08 87480 added6/15/03
82962 addedpriorto1/1/08 87510 added6/15/03
83014 addedpriorto1/1/08 87797 addedpriorto1/1/08
83026 addedpriorto1/1/08 87804 addedpriorto1/1/08
83036 addedpriorto1/1/08 87807 addedeffective4/10/09
83037 3/7/08 87880 addedpriorto1/1/08
Refer to your current
CPT® code book for
descriptions.
32

HealthyBluePROVIDERMANUAL
Procedure Codes – Laboratory Services(CONTINUED)
PROCEDURE CODE EFFECTIVE DATE
88170 invalidasof1/1/08
87510 added6/15/03
87797 addedpriorto1/1/08
87804 addedpriorto1/1/08
87807 addedeffective4/10/09
87880 addedpriorto1/1/08
88171 invalidasof1/1/08
88171 invalidasof1/1/08
88382* 12/4/09
89100 addedpriorto1/1/08
89105 addedpriorto1/1/08
89130 addedpriorto1/1/08
89132 addedpriorto1/1/08
89135 addedpriorto1/1/08
89136 addedpriorto1/1/08
89140 addedpriorto1/1/08
89141 addedpriorto1/1/08
89190 addedpriorto1/1/08
89220 addedpriorto1/1/08
89230 addedpriorto1/1/08
89350 invalidasof1/1/08
89360 invalidasof1/1/08
*ApprovalofthiscodeappliesonlytoDermatopathologiststhataretrainedandcertifiedtoperformMohsmicrographicsurgery.
Nephrology
Laboratoryservicescoveredunderamember’smedicalbenefitandperformedinthenephrologist’sofficesettingarelimitedtotheproceduresbelow.AllotherlaboratoryservicesmustbeperformedbyLabCorp®.SomeexceptionsapplyinWesternMaryland.
UseCareFirstDirectorcallFirstLine(202-429-6500or800-842-5975)toverifymembereligibilityandcoveragepriortorenderingcare,asbenefitlimitationsandmedicalpolicyrequirementsstillapply.
Nutritional Services
AuthorizationfornutritionalservicesmustbeissuedbyCareManagementunlessamemberisdiagnosedwithdiabetesandservicesarerenderedinanofficesetting.ThePCPmustprovideawrittenreferraltoaparticipatingprovider,whennutritionalservicesarerenderedinanofficesettingtoamemberdiagnosedwithdiabetes.
Obstetrics & GynecologyObstetricalcaremaybeprovidedbyaparticipatingOB/GYNwithoutawrittenreferralfromthePCP.ThehospitalmustcontactCareManagementthedayofdeliveryorthenextbusinessdaytoobtainthenecessaryauthorizationforthefacility.
Procedure Codes – NephrologyPROCEDURE CODE EFFECTIVE DATE PROCEDURE CODE EFFECTIVE DATE
75710 5/9/2008 75902 5/9/2008
75790 5/9/2008 75978 5/9/2008
75791 added1/1/10 75982 invalidasof8/1/2009
75820 5/9/2008 76937 addedpriorto1/1/08
75822 5/9/2008 81001 addedpriorto1/1/08
75825 5/9/2008 81003 addedpriorto1/1/08
75827 5/9/2008 81005 addedpriorto1/1/08
75894 5/9/2008 81007 addedpriorto1/1/08
Refer to your current
CPT® code book for
descriptions.
33

HealthyBluePROVIDERMANUAL
Admissionsforpre-termlabororotherobstetricalcomplicationsrequireanadditionalauthorization.Ifthenewbornrequiresadditionalservicesoranextendedstayduetoprematurityoranycomplicationsofbirth,aseparateauthorizationwillberequired.
Reporting for Obstetrical Services
Foradditionalinformationaboutreportingmaternityservices,visitourMedical Policy Reference ManualandconductasearchforGlobal Maternity Care (4.01.06A).YoumayalsofindinformationintheBasicClaimAdjudicationPolicyConceptssection(pg.15)oftheGeneral Information Manual.
Obstetrical Radiology/Laboratory Services
Obstetricalultrasoundscoveredbythemember’smedicalbenefitandperformedintheOB/GYN’sofficesettingarelimitedto:
● OnebaselinefetalultrasoundfordiagnosiscodesV22-V22.2or650
● Anymedicallynecessarydiagnosticfetalultrasound
Otherradiology,laboratoryandothernotedservicescoveredunderthemember’smedicalbenefitandperformedintheOB/GYN’sofficesettingarelimitedtothefollowingprocedures.AllotherradiologyandlaboratoryservicesmustbeperformedbyLabCorp®oraCareFirstBlueChoicecontractedradiologyfacility.SomeexceptionsapplyinwesternMarylandandontheEasternShore.
Foradditionalinformation,refertotheBasicClaimAdjudicationPolicyConceptssection(pg.15)oftheGeneral Information Manual.
Amniocentesis/Chorionic Villus Sampling (CVS)
AnauthorizationfromCareManagementwillberequirediftheamniocentesisisperformedinahospitalsetting.Iftheamniocentesisisperformedintheofficesetting,CareManagementauthorizationisnotnecessary.AllspecimensmustbesubmittedtoLabCorp®forprocessing.
CVSproceduresrequireanauthorizationfromCareManagement,whetherperformedinahospitalorinyouroffice.Allspecimensmustbe
submittedtoLabCorp®forprocessing,unlessprocedureisperformedinahospitalsetting.SomeexceptionsapplyinWesternMaryland.
Genetic Testing/Counseling (excludes Amniocentesis)
Genetictestingandcounselingperformedinaspecialist’sofficerequiresawrittenreferral,unlessthespecialistisanOB/GYN.Genetictestingandcounselingperformedinasettingotherthanaparticipatingprovider’sofficewillrequireanauthorizationfromCareManagement.AlllabworkmustgotoLabCorp®forprocessing.PleasecontactFirstLine(202-479-6560or800-842-5975)oruseCareFirst Directtoverifyamember’slevelofcoverage.SomeexceptionsapplyinWesternMaryland.
Maternal and Child Home Assessment
Apostpartumhomevisitisavailableforamaternalandchildhomeassessmentbyahomehealthnurse.Thehomevisitmaybeperformedafterthemotherandchildaredischargedfromthehospital:
● Lessthan48hoursfollowinganuncomplicatedvaginaldelivery
● Lessthan96hoursfollowinganuncomplicatedC-Section
● Uponproviderrequest
CareManagementmustauthorizethepostpartumhomevisit.Thepostpartumhomevisitwillconsistofacompleteassessmentofthemotherandbaby.Testsforphenylketonuria(PKU)orbilirubinlevelsarealsoincludediforderedbytheprovider.Ifmorevisitsaremedicallyindicated,anadditionalauthorizationfromCareManagementwillberequired.
Infertility Services
Teststhatrelatetoestablishingthediagnosisofinfertility(e.g.,semenanalysis,endometrialbiopsy,postcoitalandHSG-hysterosalpingogram)donotrequireanauthorizationfromCareManagementwhenperformedinanofficesetting.AllspecimensmustgotoLabCorp®forprocessing.SchedulethesetestswithLabCorp®priortorenderingservices.
Treatmentofinfertility(excludedinDCandVA),includingartificialinsemination(AI)and
34

HealthyBluePROVIDERMANUAL
Procedure Codes – Infertility ServicesPROCEDURE CODE EFFECTIVE DATE PROCEDURE CODE EFFECTIVE DATE
58323 addedpriorto1/1/08 84702 addedpriorto1/1/08
59840 addedpriorto1/1/08 84703 addedpriorto1/1/08
59841 addedpriorto1/1/08 84704 1/18/2008
59850 addedpriorto1/1/08 85610 addedpriorto1/1/08
59851 addedpriorto1/1/08 87480 addedpriorto1/1/08
59852 addedpriorto1/1/08 87510 addedpriorto1/1/08
72190, 76645, 76801,76802,76805, 76810,
76811, 76812, 76813, 76814,76815, 76816, 76817, 76818,76819, 76825, 76826, 76827,
76828, 76946, 93325
Limitedtoobstetricalservicessuchasnormaldelivery,abortion,ectopicpregnancy,miscarriageandinfertility.
74740
addedpriorto1/1/08
87660 addedpriorto 9/15/10
89240 addedpriorto1/1/08
89250 addedpriorto1/1/08
89251 addedpriorto1/1/08
89252 invalidasof1/18/2008
89253 addedpriorto1/1/08
89254 addedpriorto1/1/08
89255 addedpriorto1/1/08
10/28/2011 89256 invalidasof1/1/08
76376 9/5/2008 89257 addedpriorto1/1/08
76705, 76830, 76948
Limitedtoobstetricalservicessuchasnormaldelivery,abortion,ectopicpregnancy,miscarriage,infertilityandmedicalservices.
addedpriorto1/1/08
89258 addedpriorto1/1/08
89259 addedpriorto1/1/08
89260 addedpriorto1/1/08
89261 addedpriorto1/1/08
89264 addedpriorto1/1/08
76820, 76821
Limitedtoobstetricalservicessuchasnormaldelivery,abortion,ectopicpregnancy,miscarriageandinfertility.
3/1/2007
89268 addedpriorto1/1/08
89272 addedpriorto1/1/08
89280 addedpriorto1/1/08
89281 addedpriorto1/1/08
89290 addedpriorto 9/15/10
76856, 76857
Limitedtoinfertilityandmedicalservices.
addedpriorto1/1/08
89300 addedpriorto1/1/08
89310 addedpriorto1/1/08
89320 addedpriorto1/1/08
82670 addedpriorto1/1/08 89321 addedpriorto1/1/08
83001 addedpriorto1/1/08 89322 added1/1/08
83002 addedpriorto1/1/08 89325 addedpriorto1/1/08
84144 addedpriorto1/1/08 89329 addedpriorto1/1/08
84146, 84443, 89291 Limitedtoinfertilityonly addedpriorto1/1/08
89330 addedpriorto1/1/08
89331 added1/1/08
89352 addedpriorto1/1/08
Refer to your current CPT® code book for descriptions.
35
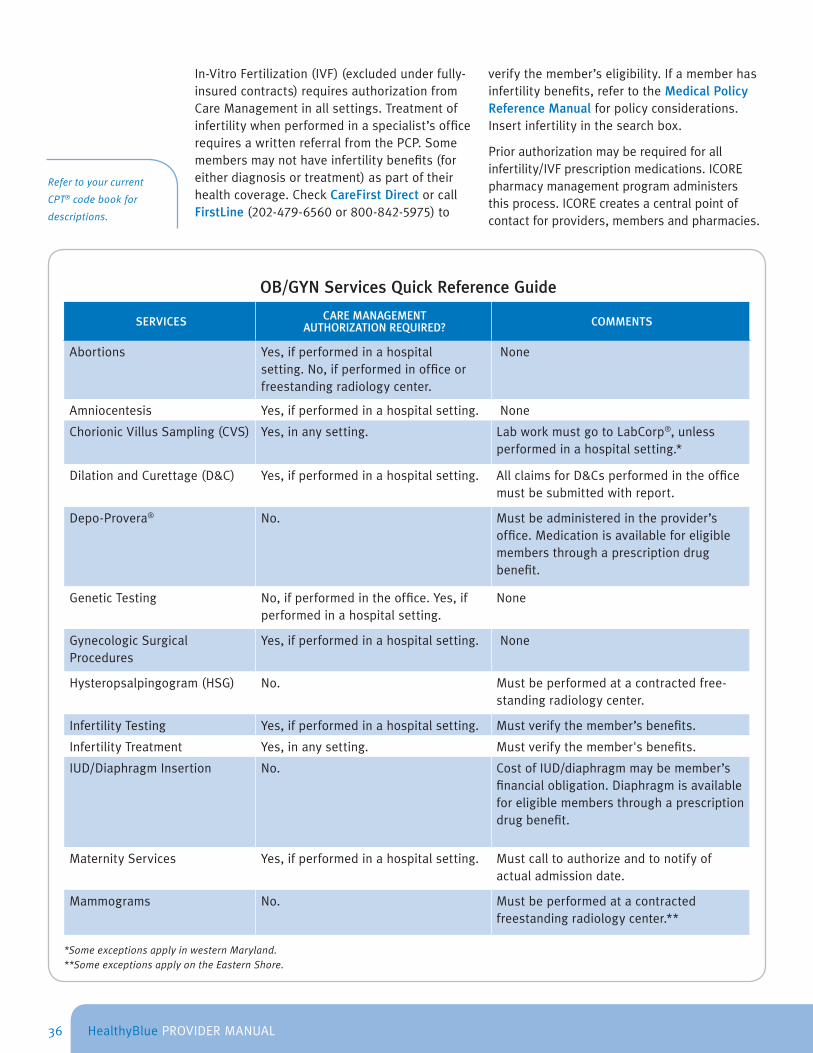
HealthyBluePROVIDERMANUAL
In-VitroFertilization(IVF)(excludedunderfully-insuredcontracts)requiresauthorizationfromCareManagementinallsettings.Treatmentofinfertilitywhenperformedinaspecialist’sofficerequiresawrittenreferralfromthePCP.Somemembersmaynothaveinfertilitybenefits(foreitherdiagnosisortreatment)aspartoftheirhealthcoverage.CheckCareFirst DirectorcallFirstLine(202-479-6560or800-842-5975)to
verifythemember’seligibility.Ifamemberhasinfertilitybenefits,refertotheMedical Policy Reference Manualforpolicyconsiderations.Insertinfertilityinthesearchbox.
Priorauthorizationmayberequiredforallinfertility/IVFprescriptionmedications.ICOREpharmacymanagementprogramadministersthisprocess.ICOREcreatesacentralpointofcontactforproviders,membersandpharmacies.
Refer to your current
CPT® code book for
descriptions.
OB/GYN Services Quick Reference Guide
SERVICES CARE MANAGEMENT AUTHORIZATION REQUIRED? COMMENTS
Abortions Yes,ifperformedinahospitalsetting.No,ifperformedinofficeorfreestandingradiologycenter.
None
Amniocentesis Yes,ifperformedinahospitalsetting. None
ChorionicVillusSampling(CVS) Yes,inanysetting. LabworkmustgotoLabCorp®,unlessperformedinahospitalsetting.*
DilationandCurettage(D&C) Yes,ifperformedinahospitalsetting. AllclaimsforD&Csperformedintheofficemustbesubmittedwithreport.
Depo-Provera® No. Mustbeadministeredintheprovider’soffice.Medicationisavailableforeligiblemembersthroughaprescriptiondrugbenefit.
GeneticTesting No,ifperformedintheoffice.Yes,ifperformedinahospitalsetting.
None
GynecologicSurgicalProcedures
Yes,ifperformedinahospitalsetting. None
Hysteropsalpingogram(HSG) No. Mustbeperformedatacontractedfree-standingradiologycenter.
InfertilityTesting Yes,ifperformedinahospitalsetting. Mustverifythemember’sbenefits.
InfertilityTreatment Yes,inanysetting. Mustverifythemember'sbenefits.
IUD/DiaphragmInsertion No. CostofIUD/diaphragmmaybemember’sfinancialobligation.Diaphragmisavailableforeligiblemembersthroughaprescriptiondrugbenefit.
MaternityServices Yes,ifperformedinahospitalsetting. Mustcalltoauthorizeandtonotifyofactualadmissiondate.
Mammograms No. Mustbeperformedatacontractedfreestandingradiologycenter.**
*Some exceptions apply in western Maryland.**Some exceptions apply on the Eastern Shore.
36
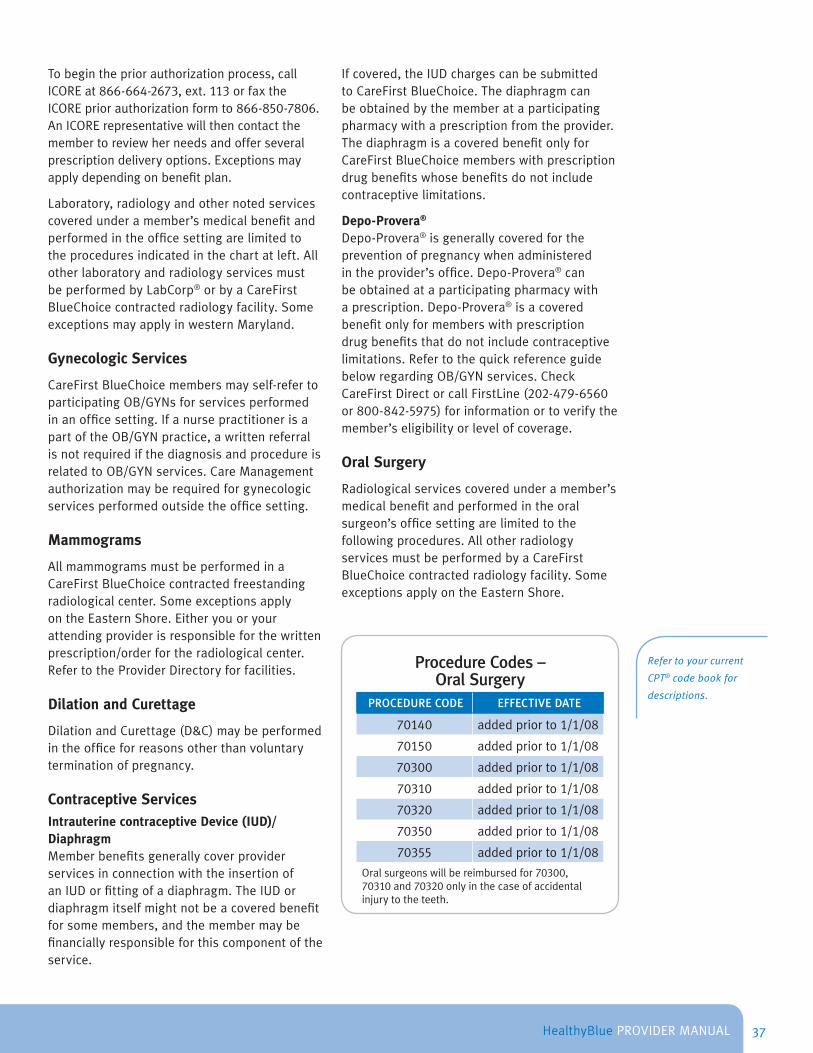
HealthyBluePROVIDERMANUAL
Tobeginthepriorauthorizationprocess,callICOREat866-664-2673,ext.113orfaxtheICOREpriorauthorizationformto866-850-7806.AnICORErepresentativewillthencontactthemembertoreviewherneedsandofferseveralprescriptiondeliveryoptions.Exceptionsmayapplydependingonbenefitplan.
Laboratory,radiologyandothernotedservicescoveredunderamember’smedicalbenefitandperformedintheofficesettingarelimitedtotheproceduresindicatedinthechartatleft.AllotherlaboratoryandradiologyservicesmustbeperformedbyLabCorp®orbyaCareFirstBlueChoicecontractedradiologyfacility.SomeexceptionsmayapplyinwesternMaryland.
Gynecologic Services
CareFirstBlueChoicemembersmayself-refertoparticipatingOB/GYNsforservicesperformedinanofficesetting.IfanursepractitionerisapartoftheOB/GYNpractice,awrittenreferralisnotrequiredifthediagnosisandprocedureisrelatedtoOB/GYNservices.CareManagementauthorizationmayberequiredforgynecologicservicesperformedoutsidetheofficesetting.
Mammograms
AllmammogramsmustbeperformedinaCareFirstBlueChoicecontractedfreestandingradiologicalcenter.SomeexceptionsapplyontheEasternShore.Eitheryouoryourattendingproviderisresponsibleforthewrittenprescription/orderfortheradiologicalcenter.RefertotheProviderDirectoryforfacilities.
Dilation and Curettage
DilationandCurettage(D&C)maybeperformedintheofficeforreasonsotherthanvoluntaryterminationofpregnancy.
Contraceptive ServicesIntrauterine contraceptive Device (IUD)/DiaphragmMemberbenefitsgenerallycoverproviderservicesinconnectionwiththeinsertionofanIUDorfittingofadiaphragm.TheIUDordiaphragmitselfmightnotbeacoveredbenefitforsomemembers,andthemembermaybefinanciallyresponsibleforthiscomponentoftheservice.
Ifcovered,theIUDchargescanbesubmittedtoCareFirstBlueChoice.Thediaphragmcanbeobtainedbythememberataparticipatingpharmacywithaprescriptionfromtheprovider.ThediaphragmisacoveredbenefitonlyforCareFirstBlueChoicememberswithprescriptiondrugbenefitswhosebenefitsdonotincludecontraceptivelimitations.
Depo-Provera®
Depo-Provera®isgenerallycoveredforthepreventionofpregnancywhenadministeredintheprovider’soffice.Depo-Provera®canbeobtainedataparticipatingpharmacywithaprescription.Depo-Provera®isacoveredbenefitonlyformemberswithprescriptiondrugbenefitsthatdonotincludecontraceptivelimitations.RefertothequickreferenceguidebelowregardingOB/GYNservices.CheckCareFirstDirectorcallFirstLine(202-479-6560 or800-842-5975)forinformationortoverifythemember’seligibilityorlevelofcoverage.
Oral Surgery
Radiologicalservicescoveredunderamember’smedicalbenefitandperformedintheoralsurgeon’sofficesettingarelimitedtothefollowingprocedures.AllotherradiologyservicesmustbeperformedbyaCareFirstBlueChoicecontractedradiologyfacility.SomeexceptionsapplyontheEasternShore.
Procedure Codes – Oral Surgery
PROCEDURE CODE EFFECTIVE DATE
70140 addedpriorto1/1/08
70150 addedpriorto1/1/08
70300 addedpriorto1/1/08
70310 addedpriorto1/1/08
70320 addedpriorto1/1/08
70350 addedpriorto1/1/08
70355 addedpriorto1/1/08
Oralsurgeonswillbereimbursedfor70300,70310and70320onlyinthecaseofaccidentalinjurytotheteeth.
Refer to your current
CPT® code book for
descriptions.
37
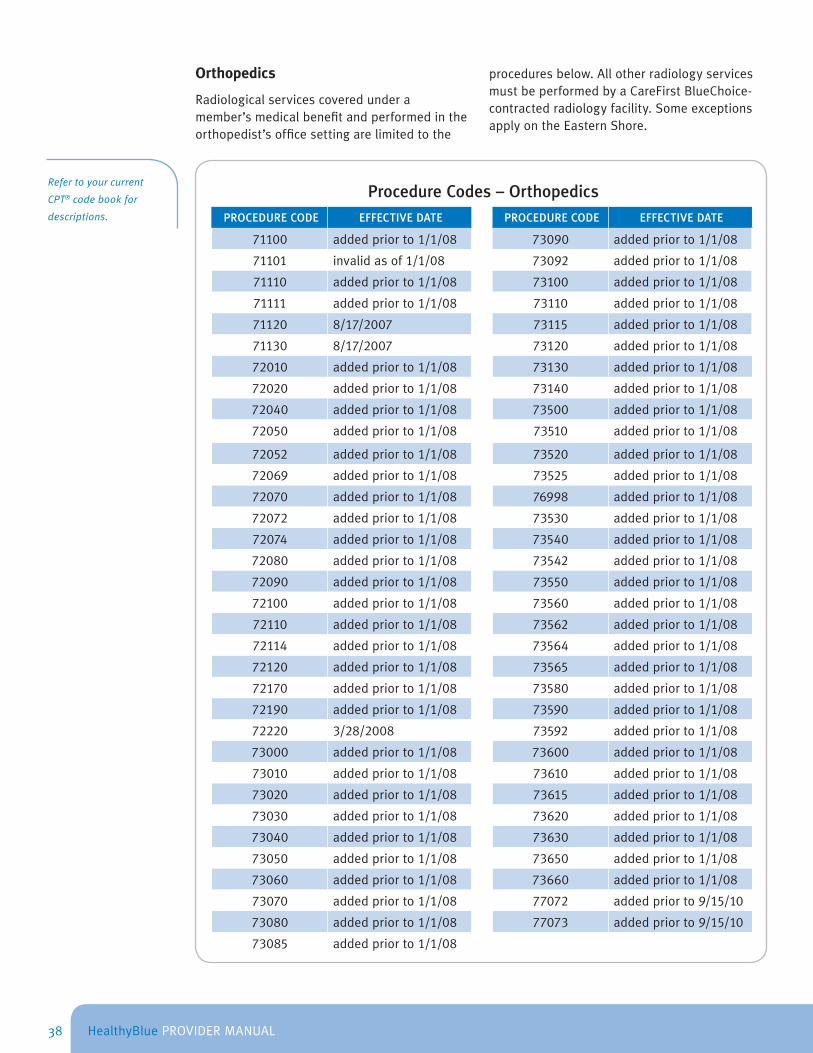
HealthyBluePROVIDERMANUAL
Orthopedics
Radiologicalservicescoveredunderamember’smedicalbenefitandperformedintheorthopedist’sofficesettingarelimitedtothe
proceduresbelow.AllotherradiologyservicesmustbeperformedbyaCareFirstBlueChoice-contractedradiologyfacility.SomeexceptionsapplyontheEasternShore.
Refer to your current
CPT® code book for
descriptions.
Procedure Codes – OrthopedicsPROCEDURE CODE EFFECTIVE DATE PROCEDURE CODE EFFECTIVE DATE
71100 addedpriorto1/1/08 73090 addedpriorto1/1/08
71101 invalidasof1/1/08 73092 addedpriorto1/1/08
71110 addedpriorto1/1/08 73100 addedpriorto1/1/08
71111 addedpriorto1/1/08 73110 addedpriorto1/1/08
71120 8/17/2007 73115 addedpriorto1/1/08
71130 8/17/2007 73120 addedpriorto1/1/08
72010 addedpriorto1/1/08 73130 addedpriorto1/1/08
72020 addedpriorto1/1/08 73140 addedpriorto1/1/08
72040 addedpriorto1/1/08 73500 addedpriorto1/1/08
72050 addedpriorto1/1/08 73510 addedpriorto1/1/08
72052 addedpriorto1/1/08 73520 addedpriorto1/1/08
72069 addedpriorto1/1/08 73525 addedpriorto1/1/08
72070 addedpriorto1/1/08 76998 addedpriorto1/1/08
72072 addedpriorto1/1/08 73530 addedpriorto1/1/08
72074 addedpriorto1/1/08 73540 addedpriorto1/1/08
72080 addedpriorto1/1/08 73542 addedpriorto1/1/08
72090 addedpriorto1/1/08 73550 addedpriorto1/1/08
72100 addedpriorto1/1/08 73560 addedpriorto1/1/08
72110 addedpriorto1/1/08 73562 addedpriorto1/1/08
72114 addedpriorto1/1/08 73564 addedpriorto1/1/08
72120 addedpriorto1/1/08 73565 addedpriorto1/1/08
72170 addedpriorto1/1/08 73580 addedpriorto1/1/08
72190 addedpriorto1/1/08 73590 addedpriorto1/1/08
72220 3/28/2008 73592 addedpriorto1/1/08
73000 addedpriorto1/1/08 73600 addedpriorto1/1/08
73010 addedpriorto1/1/08 73610 addedpriorto1/1/08
73020 addedpriorto1/1/08 73615 addedpriorto1/1/08
73030 addedpriorto1/1/08 73620 addedpriorto1/1/08
73040 addedpriorto1/1/08 73630 addedpriorto1/1/08
73050 addedpriorto1/1/08 73650 addedpriorto1/1/08
73060 addedpriorto1/1/08 73660 addedpriorto1/1/08
73070 addedpriorto1/1/08 77072 addedpriorto9/15/10
73080 addedpriorto1/1/08 77073 addedpriorto9/15/10
73085 addedpriorto1/1/08
38
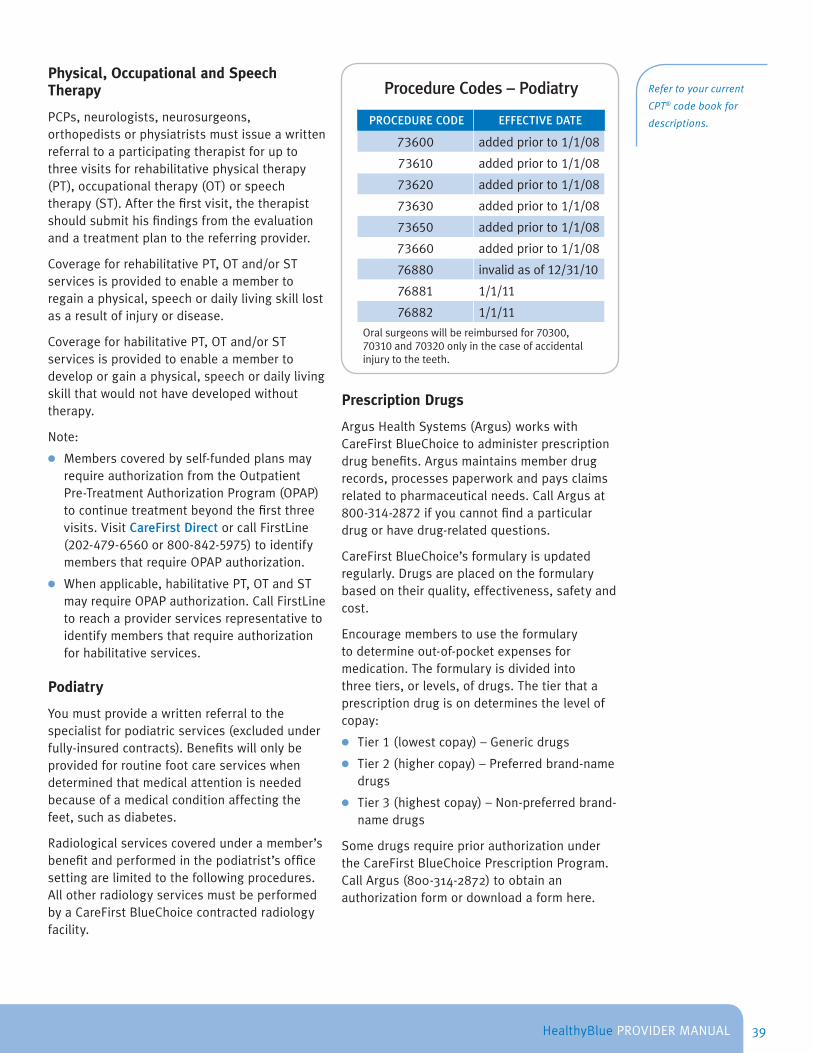
HealthyBluePROVIDERMANUAL
Physical, Occupational and Speech Therapy
PCPs,neurologists,neurosurgeons,orthopedistsorphysiatristsmustissueawrittenreferraltoaparticipatingtherapistforuptothreevisitsforrehabilitativephysicaltherapy(PT),occupationaltherapy(OT)orspeechtherapy(ST).Afterthefirstvisit,thetherapistshouldsubmithisfindingsfromtheevaluationandatreatmentplantothereferringprovider.
CoverageforrehabilitativePT,OTand/orSTservicesisprovidedtoenableamembertoregainaphysical,speechordailylivingskilllostasaresultofinjuryordisease.
CoverageforhabilitativePT,OTand/orSTservicesisprovidedtoenableamembertodeveloporgainaphysical,speechordailylivingskillthatwouldnothavedevelopedwithouttherapy.
Note:
● Memberscoveredbyself-fundedplansmayrequireauthorizationfromtheOutpatientPre-TreatmentAuthorizationProgram(OPAP)tocontinuetreatmentbeyondthefirstthreevisits.VisitCareFirst DirectorcallFirstLine(202-479-6560or800-842-5975)toidentifymembersthatrequireOPAPauthorization.
● Whenapplicable,habilitativePT,OTandSTmayrequireOPAPauthorization.CallFirstLinetoreachaproviderservicesrepresentativetoidentifymembersthatrequireauthorizationforhabilitativeservices.
Podiatry
Youmustprovideawrittenreferraltothespecialistforpodiatricservices(excludedunderfully-insuredcontracts).Benefitswillonlybeprovidedforroutinefootcareserviceswhendeterminedthatmedicalattentionisneededbecauseofamedicalconditionaffectingthefeet,suchasdiabetes.
Radiologicalservicescoveredunderamember’sbenefitandperformedinthepodiatrist’sofficesettingarelimitedtothefollowingprocedures.AllotherradiologyservicesmustbeperformedbyaCareFirstBlueChoicecontractedradiologyfacility.
Procedure Codes – Podiatry
PROCEDURE CODE EFFECTIVE DATE
73600 addedpriorto1/1/08
73610 addedpriorto1/1/08
73620 addedpriorto1/1/08
73630 addedpriorto1/1/08
73650 addedpriorto1/1/08
73660 addedpriorto1/1/08
76880 invalidasof12/31/10
76881 1/1/11
76882 1/1/11
Oralsurgeonswillbereimbursedfor70300,70310and70320onlyinthecaseofaccidentalinjurytotheteeth.
Prescription Drugs
ArgusHealthSystems(Argus)workswithCareFirstBlueChoicetoadministerprescriptiondrugbenefits.Argusmaintainsmemberdrugrecords,processespaperworkandpaysclaimsrelatedtopharmaceuticalneeds.CallArgusat800-314-2872ifyoucannotfindaparticulardrugorhavedrug-relatedquestions.
CareFirstBlueChoice’sformularyisupdatedregularly.Drugsareplacedontheformularybasedontheirquality,effectiveness,safetyandcost.
Encouragememberstousetheformularytodetermineout-of-pocketexpensesformedication.Theformularyisdividedintothreetiers,orlevels,ofdrugs.Thetierthataprescriptiondrugisondeterminesthelevelofcopay:
● Tier1(lowestcopay)–Genericdrugs
● Tier2(highercopay)–Preferredbrand-namedrugs
● Tier3(highestcopay)–Non-preferredbrand-namedrugs
SomedrugsrequirepriorauthorizationundertheCareFirstBlueChoicePrescriptionProgram.CallArgus(800-314-2872)toobtainanauthorizationformordownloadaformhere.
Refer to your current
CPT® code book for
descriptions.
39

HealthyBluePROVIDERMANUAL
Refer to your current
CPT® code book for
descriptions.
Procedure Codes – Pulmonology
PROCEDURE CODE EFFECTIVE DATE
71010 3/6/2006
71015 3/6/2006
71020 3/6/2006
71021 3/6/2006
71022 3/6/2006
71023 3/6/2006
71030 3/6/2006
71034 3/6/2006
71035 3/6/2006
82800 addedpriorto1/1/08
82803 addedpriorto1/1/08
82805 addedpriorto1/1/08
82810 addedpriorto1/1/08
82820 addedpriorto1/1/08
85022 invalidasof1/1/08
WithHealthyBlue,membershaveaccesstocertaingenericdrugsatnocost.Thisincludesmedicationinthefollowingclasses:
● Asthma
● Depression
● Diabetes
● Highbloodpressure
● Highcholesterol
Alistofgenericdrugsonthepreferreddruglistisavailableatwww .carefirst .com/HealthyBlue.
Pulmonology
Laboratoryservicescoveredunderamember’smedicalbenefitandperformedinthepulmonologist’sofficesettingarelimitedtotheprocedurecodesabove.AllotherlaboratoryservicesshouldbeperformedbyLabCorp®.SomeexceptionsmayapplyinWesternMaryland.
Radiology
OutpatientradiologyproceduresrenderedataparticipatingfreestandingradiologyfacilitydonotrequireawrittenreferralfromthePCP.SomeexceptionsapplyontheEasternShore.
Providersmustprovidethememberwithaprescriptionororder.PleaserefertotheProvider Directoryforanup-to-datelistingofparticipatingfacilities.
Radiologicalservicesandothernotedcodescoveredunderamember’smedicalbenefitandperformedinthePCP’sorspecialist’sofficearelimitedtotheprocedurecodes.AllotherradiologyservicesmustbeperformedbyCareFirstBlueChoicecontractedradiologyfacility.SomeexceptionsapplyontheEasternShore.
CareFirstandCareFirstBlueChoice,Inc.expectsallproviderswhoperformlaboratoryorimagingtests,atanysitetoobtainand/ormaintaintheappropriatefederal,stateandlocallicensesandcertifications,training,qualitycontrols,andsafetystandardspertinenttothetestsperformed.
Multiple Computerized Tomography (CT) Scans, Magnetic Resonance Imaging (MRI) and Magnetic Resonance Angiography (MRAs)
MultiplemedicallynecessaryCTScans,MRIsandMRAsperformedbyprofessionalprovidersataparticipatingoutpatientfacility(free-standingorhospital-based)willbereimbursedat100percentoftheallowedamount,minusapplicablecopaymentsand/ordeductiblespaidbythemember.
ThisappliestomultipleCTScans,MRIsandMRAsrenderedtothesamememberonthesamedateofservice.
Rheumatology
Radiologicalservicescoveredunderamember’smedicalbenefitandperformedintherheumatologist’sofficesettingarelimitedtotheproceduresonthefollowingpage.AllotherradiologicalproceduresmustbeperformedbyaCareFirstBlueChoicecontractedradiologyfacility.SomeexceptionsapplyontheEasternShore.
40
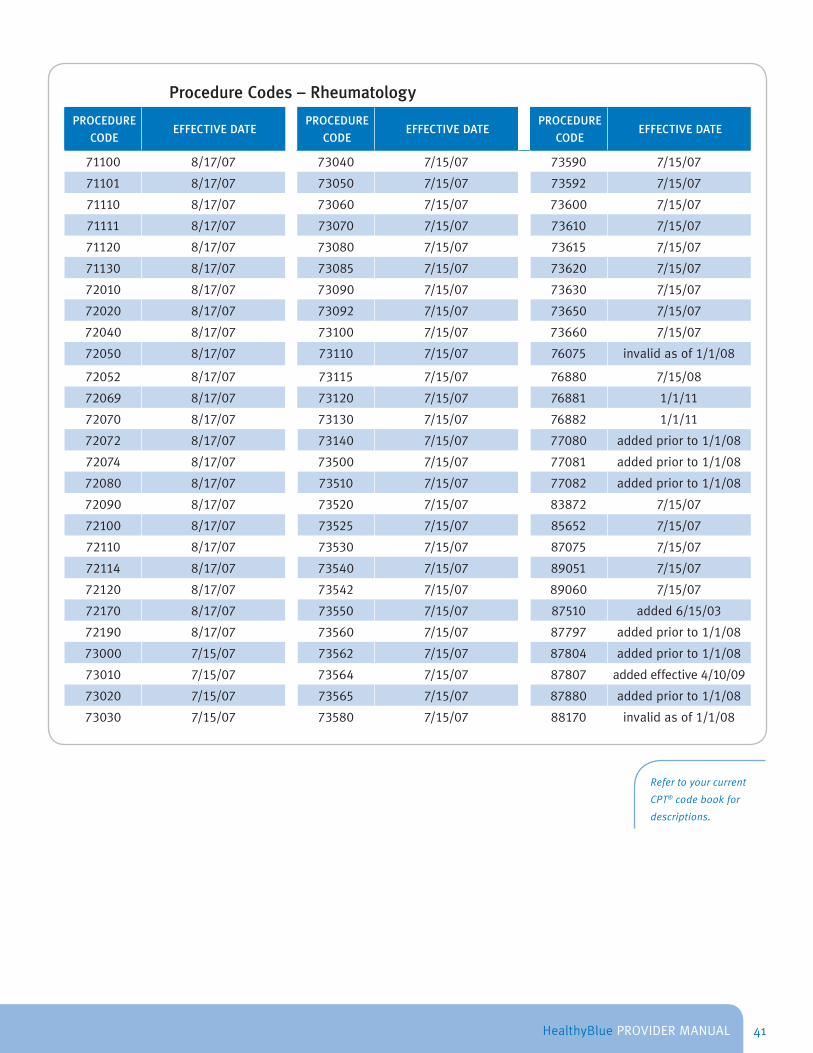
HealthyBluePROVIDERMANUAL
Procedure Codes – Rheumatology
PROCEDURE
CODEEFFECTIVE DATE
PROCEDURE
CODEEFFECTIVE DATE
PROCEDURE
CODEEFFECTIVE DATE
71100 8/17/07 73040 7/15/07 73590 7/15/07
71101 8/17/07 73050 7/15/07 73592 7/15/07
71110 8/17/07 73060 7/15/07 73600 7/15/07
71111 8/17/07 73070 7/15/07 73610 7/15/07
71120 8/17/07 73080 7/15/07 73615 7/15/07
71130 8/17/07 73085 7/15/07 73620 7/15/07
72010 8/17/07 73090 7/15/07 73630 7/15/07
72020 8/17/07 73092 7/15/07 73650 7/15/07
72040 8/17/07 73100 7/15/07 73660 7/15/07
72050 8/17/07 73110 7/15/07 76075 invalidasof1/1/08
72052 8/17/07 73115 7/15/07 76880 7/15/08
72069 8/17/07 73120 7/15/07 76881 1/1/11
72070 8/17/07 73130 7/15/07 76882 1/1/11
72072 8/17/07 73140 7/15/07 77080 addedpriorto1/1/08
72074 8/17/07 73500 7/15/07 77081 addedpriorto1/1/08
72080 8/17/07 73510 7/15/07 77082 addedpriorto1/1/08
72090 8/17/07 73520 7/15/07 83872 7/15/07
72100 8/17/07 73525 7/15/07 85652 7/15/07
72110 8/17/07 73530 7/15/07 87075 7/15/07
72114 8/17/07 73540 7/15/07 89051 7/15/07
72120 8/17/07 73542 7/15/07 89060 7/15/07
72170 8/17/07 73550 7/15/07 87510 added6/15/03
72190 8/17/07 73560 7/15/07 87797 addedpriorto1/1/08
73000 7/15/07 73562 7/15/07 87804 addedpriorto1/1/08
73010 7/15/07 73564 7/15/07 87807 addedeffective4/10/09
73020 7/15/07 73565 7/15/07 87880 addedpriorto1/1/08
73030 7/15/07 73580 7/15/07 88170 invalidasof1/1/08
Refer to your current
CPT® code book for
descriptions.
41
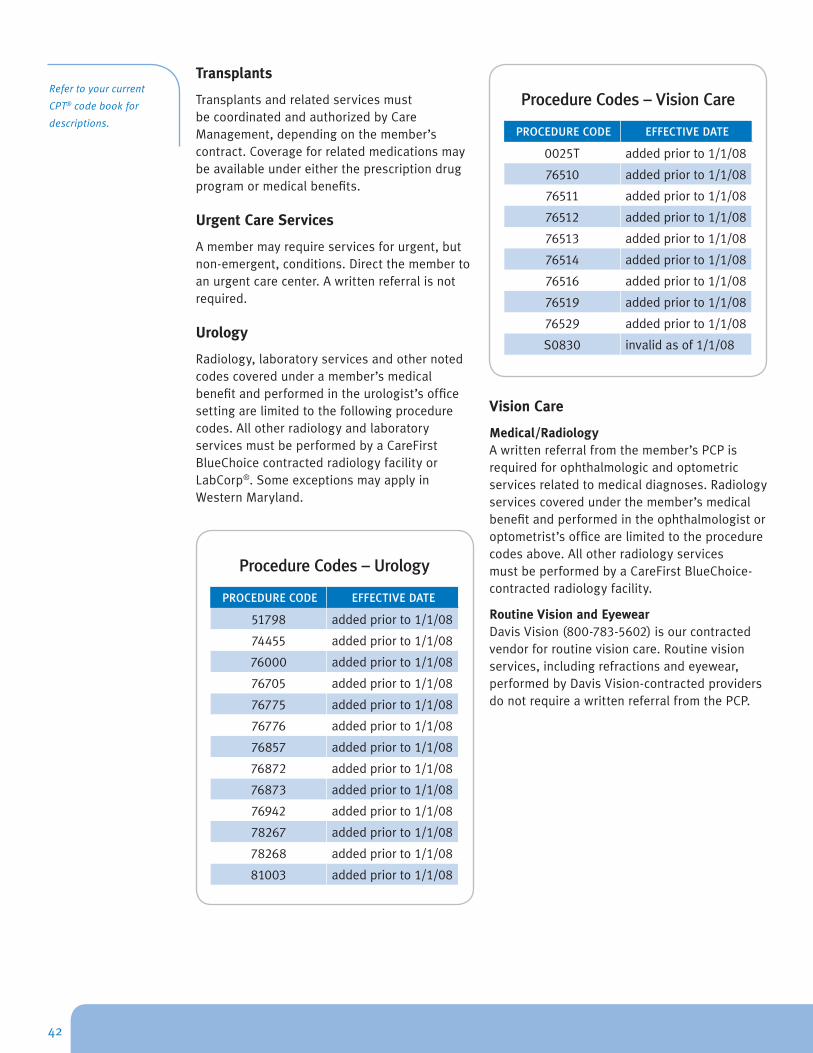
HealthyBluePROVIDERMANUAL
Refer to your current
CPT® code book for
descriptions.
Transplants
TransplantsandrelatedservicesmustbecoordinatedandauthorizedbyCareManagement,dependingonthemember’scontract.Coverageforrelatedmedicationsmaybeavailableundereithertheprescriptiondrugprogramormedicalbenefits.
Urgent Care Services
Amembermayrequireservicesforurgent,butnon-emergent,conditions.Directthemembertoanurgentcarecenter.Awrittenreferralisnotrequired.
Urology
Radiology,laboratoryservicesandothernotedcodescoveredunderamember’smedicalbenefitandperformedintheurologist’sofficesettingarelimitedtothefollowingprocedurecodes.AllotherradiologyandlaboratoryservicesmustbeperformedbyaCareFirstBlueChoicecontractedradiologyfacilityorLabCorp®.SomeexceptionsmayapplyinWesternMaryland.
Procedure Codes – Urology
PROCEDURE CODE EFFECTIVE DATE
51798 addedpriorto1/1/08
74455 addedpriorto1/1/08
76000 addedpriorto1/1/08
76705 addedpriorto1/1/08
76775 addedpriorto1/1/08
76776 addedpriorto1/1/08
76857 addedpriorto1/1/08
76872 addedpriorto1/1/08
76873 addedpriorto1/1/08
76942 addedpriorto1/1/08
78267 addedpriorto1/1/08
78268 addedpriorto1/1/08
81003 addedpriorto1/1/08
Procedure Codes – Vision Care
PROCEDURE CODE EFFECTIVE DATE
0025T addedpriorto1/1/08
76510 addedpriorto1/1/08
76511 addedpriorto1/1/08
76512 addedpriorto1/1/08
76513 addedpriorto1/1/08
76514 addedpriorto1/1/08
76516 addedpriorto1/1/08
76519 addedpriorto1/1/08
76529 addedpriorto1/1/08
S0830 invalidasof1/1/08
Vision Care
Medical/RadiologyAwrittenreferralfromthemember’sPCPisrequiredforophthalmologicandoptometricservicesrelatedtomedicaldiagnoses.Radiologyservicescoveredunderthemember’smedicalbenefitandperformedintheophthalmologistoroptometrist’sofficearelimitedtotheprocedurecodesabove.AllotherradiologyservicesmustbeperformedbyaCareFirstBlueChoice-contractedradiologyfacility.
Routine Vision and EyewearDavisVision(800-783-5602)isourcontractedvendorforroutinevisioncare.Routinevisionservices,includingrefractionsandeyewear,performedbyDavisVision-contractedprovidersdonotrequireawrittenreferralfromthePCP.
42
HealthyBluePROVIDERMANUAL
Appeals Process
ThissectionprovidesPCPswiththeinformationneededtobetterunderstandtheAppealsProcess.Refertothissectionforinformationonhowtorequestreconsiderationofaclaimsdecision.
Claims Issues
Youmayappealaclaimsdecisioninwritingwithin180daysfromthedateyoureceivedthedenial.UseaProviderInquiryResolutionForm(PIRF),sendaformalletterofmedicalnecessity,oruseCareFirst DirecttosubmitalladministrativeappealstoProviderServices.
ContactaProviderServicesrepresentative(202-479-6560or800-842-5972)regardinganinquiryorappealofaclaimpayment.Yourconcernscanoftenbehandledandresolvedthroughinformaldiscussionsandinformationgathering.Ifyourquestionsorconcernrelatestoourhandlingofaclaimorotheradministrativeaction,callanddiscussthematterwithaCareFirstBlueChoiceProviderServicerepresentative.Inmanyinstances,themattermaybequicklyresolved.
IftheinquirycannotbesatisfiedintheServiceArea,youwillbeinstructedtomaketheappealinwritingandsubmitthisinformation,alongwithyourappealreasonandanypertinentorsupportivemedicalrecords,literatureorclaimsdocumentationtoCareFirstBlueChoice.
Internal Appeal or Grievance Process
Allappealsandgrievancesmustbesubmittedinwritingandfiledwithin180daysfromthedateyoureceivedthenotificationofthedenialofbenefitsorservices.CareFirstBlueChoicemayrequireadditionalinformationfromyouorthebillingand/ortreatmentprovider.Ifyourgrievanceisregardingamedicalnecessity,cosmeticorexperimental/investigationaldenialreason,thegrievancewillbereviewedbyaproviderwhowasnotinvolvedintheinitialdenialdetermination.
43

HealthyBluePROVIDERMANUAL
Writtenappealsshouldbemailedto:
MailAdministratorP.O.Box14114Lexington,Ky.40512-4114
Thereisanemergency/expeditedappealprocessavailabletoyou.Inanexpeditedappealforurgent/emergencycare,theappealorgrievancedecisionwillbemadeassoonaspossible,andnolaterthan24hoursafterCareFirstBlueChoicereceivesthenecessaryinformationtomakeadecision.Theappealorgrievancereviewwillbecompletedbyaproviderinthesameorsimilarspecialtyasthetreatmentunderreviewandnotpartoftheoriginaldenialdecision,asappropriate.Expeditedappealsinvolvecarethathasnotyetoccurredoriscurrentlyoccurring(pre-serviceorconcurrentcare).Allappealandgrievancedecisionsareansweredinwriting.Ifthedecisionremainsadenialoftheoriginalrequest,adetailedexplanationthatreferencestherule,policyorguidelineusedtomakethedecisionwillbeincluded.
Necessary Information
Aletterdescribingthereason(s)fortheappealandtheclinicaljustification/rationaleisrequired,includingthefollowinginformation,ifpossible:
● Member’snameandidentificationnumber
● Provider’snumberortaxidentificationnumber
● Claimnumber
● Admissionanddischargedate(ifapplicable)ordate(s)ofservice
● Provider’sname
● AcopyoftheoriginalclaimorExplanationofBenefit(EOB)denialinformation
● Supportingclinicalnotesormedicalrecords(i.e.pertinentlabreports,x-rays,treatmentplans,progressnotes,etc.)
Contact a Provider
Services representative
(202-479-6560 or 800-
842-5972) regarding
an inquiry or appeal of
a claim payment. Your
concerns can often be
handled and resolved
through informal
discussions and
information gathering.
44
HealthyBluePROVIDERMANUAL
Administrative Functions
Thissectionprovidesinformationaboutouradministrativeprocedures,includingchangesinprivileges,providerreimbursementandimportanttelephonenumbers.
Web ResourcesThefollowinginformationisavailableatwww .carefirst .com:
● ThePrescription DrugssectionincludestheCareFirstformularyandinformationonpriorauthorizationrequirementsandquantitylimits.
● CareFirstMedical Policy Reference Manualhasthemostup-to-datemedicalpolicyinformationandguidelines.
● HealthyBlueseminarsandweb-basedseminarsareavailablethroughtheCenter for Provider Education & Training .
● ClaimsAdjudicationandAssociatedReimbursementPolicyinformation,includingdetailsonbillingandreimbursementguidelinesareavailableintheGeneral Information Manual.
● MedicalForms,includingtheHealthyBlueHealthandWellnessEvaluationFormareavailablefordownloadingandmore.
Change in PrivilegesYourparticipationintheCareFirstBlueChoicenetworkissubjecttothetermsofyourparticipationagreementwithCareFirstBlueChoice.Theagreementspecificallyprovidesfortheenforcementofarangeofsanctionsuptoandincludingterminationofyournetworkparticipationforreasonsrelatedtothequalityofcarerenderedtomembers,aswellasforbreachesoftheparticipationagreementitself.
AfterreviewofrelevantandobjectiveevidencesuppliedtoorobtainedbyCareFirstBlueChoice,aCareFirstBlueChoiceMedicalDirectormayelecttoreduce,suspendorterminateyourprivilegesforcause.Whenapotentialproblemwithqualityofcare,competenceorprofessionalconductisidentifiedandthereisimminentdangertothehealthofCareFirstBlueChoicemembers,theMedicalDirectormayimmediatelyterminateyourparticipation.Actions,otherthanterminationofparticipation,include:
45

HealthyBluePROVIDERMANUAL
●
●
●
●
●
Implementationofacorrectiveactionplan
Implementationofamonitoringplanrelativetobillingand/ormembersatisfaction
ClosureofPCPpanels
Suspensionwithnoticetoterminate
SpecialletterofagreementbetweenthepractitionerandCareFirstBlueChoiceoutliningexpectationsand/orlimitationofrangeofservicesthepractitionermaysupplytomembers
Tomakefinaldeterminations,theMedicalDirectorseeksadvicefromtheCredentialingAdvisoryCommittee(CAC)andmayappointotherpractitionersasadhocmemberstotheCACtoofferspecializedexpertiseinthemedicalfieldthatisthesubjectofthecaseorissuepresented.Aspartofitsinvestigation,thecommitteemayuseinformationthatmayincludechartreviewofoutpatientandinpatientcare,complaintsummaries,peer/staffcomplaintsandinterviewswiththepractitioner.
TheMedicalDirectornotifiesyouinwritingofthereason(s)fortheterminationand/orsanction,his/herrighttoappealthedeterminationandtheappealprocess.Thepractitionermayappealthedecisionbysubmittingawrittennoticewithmaterialsrelevanttothedecisionwithin30daysofbeingnotifiedofthedecision.Ifanappealisn’tfiledwithin30days,appealrightsareforfeited.
Pursuanttothelocaljurisdiction’sregulations,CareFirstBlueChoicenotifiestherelevantlicensingboardswithin10dayswhenithaslimited,reducedchangesorterminatedapractitioner’scontractifsuchactionwasforreasonsthatmightbegroundsfordisciplinaryactionbytheparticularlicensingboard.AsaqueryingagentfortheNationalPractitionerDataBank(NPDB),CareFirstBlueChoicecomplieswiththenotificationrequirements.
Quality of Care Terminations
Appealrequestsrelativetoqualityofcareterminationsarereviewedthroughahearingpanel.ThehearingpaneliscomprisedofclinicalmembersoftheCorporateQualityImprovementCommitteewhowerenotpreviouslyinvolvedinthereviewordecisionofthecase,andatleastthreepractitionerswithnoadverseeconomicinterestsconnectedtotheappealingpractitionerandsimilarexperienceintheappealing
practitioner’sexpertise(ifappropriate).
Theappealingpractitionerisnotifiedinwritingofthehearingprocess.Followingthehearing,thepanelwillmakeafinaldecisiontoaffirm,amendorreversethesanctionornetworktermination.TheMedicalDirector,inconsultationwithCareFirstlegalrepresentative(s),notifiesthepractitionerofthedecisioninwriting,providesastatementforthebasisofthedecisionandinformsthepractitionerthatthedecisionisfinalandnotsubjecttofurtherconsiderationwithCareFirstBlueChoice.
All Other Sanctions or Terminations
TheMedicalDirectorwillreconsiderappealsforallothersanctionsorterminationsonthebasisofnewinformationprovidedbythepractitioner.TheMedicalDirectormayseekrecommendationsfromtheCredentialingAdvisoryCommittee(CAC)priortomakingafinaldecision.TheMedicalDirectornotifiesthepractitionerofthedecisioninwriting,providesastatementforthebasisofthedecisionandinformsthepractitionerthatthedecisionisfinalandnotsubjecttofurtherconsiderationwithCareFirstBlueChoice.
Member to be Held Harmless
CareFirstBlueChoicewillmakepaymentstotheprovideronlyforcoveredserviceswhicharerenderedtoeligiblemembersandwhicharedeterminedbyCareFirstBlueChoicetobemedicallynecessary.AnyservicesfoundbyCareFirstBlueChoicetohavenotbeenmedicallynecessary,andineligibleforbenefits,willnotbechargedtothemember.Theprovidermaylooktothememberforpaymentofdeductiblesand/orcopaymentsorforservicesnotcoveredunderthemember’sHealthBenefitPlan.PaymentmaynotbesoughtfromthememberforanybalancesremainingafterCareFirstBlueChoice’spaymentforcoveredservicesorforservicesdeniedduetotheprovider’slackofcontractedcompliance(e.g.,lackofauthorization),unlessitistosatisfythedeductibleorcopaymentrequirementsofthemember’sHealthBenefitPlan.Theprovidershouldnotspecificallycharge,collectadepositfrom,seekcompensation,remunerationorreimbursementfromorhaveanyrecourseagainstmembersorpersonsotherthanCareFirstBlueChoiceorathirdpartypayerforcoveredservicesprovidedaccordingtotheParticipationAgreement.
46
HealthyBluePROVIDERMANUAL
Administrative Services Policy
Providerscannotrequirethepaymentofchargesaboveandbeyondcopaymentsanddeductibles.Tohelpyouevaluateyouroffice’scurrentpractices,ourpolicyisbelow.
● Participatingprovidersshallnotcharge,collectfrom,seekremunerationorreimbursementfromorhaverecourseagainstsubscribersormembersforcoveredservices,includingthosethatareinherentinthedeliveryofcoveredservices.ThepracticeofchargingforofficeadministrationandexpenseisnotinaccordancewiththeParticipationAgreementandParticipatingProviderManual.Suchchargesforadministrativeserviceswouldinclude,bywayofexample,annualorpervisitfeestooffsettheincreaseofofficeadministrativedutiesand/oroverheadexpenses,malpracticecoverageincreases,writingprescriptions,copyingandfaxing,completingreferralformsorotherexpensesrelatedtotheoverallmembermanagementandcompliancewithgovernmentlawsandregulations,requiredofhealthcareproviders.
● Theprovidermaylooktothesubscriberormemberforpaymentofdeductiblesandcopayments,orforprovidingspecifichealthcareservicesnotcoveredunderthemember’sHealthBenefitPlanaswellasfeesforsomeadministrativeservices.Suchfeesforadministrativeservicesmayinclude,bywayofexample,feesforcompletionofcertainformsnotconnectedwiththeprovidingofCoveredServices,missedappointmentfees,andchargesforcopiesofmedicalrecordswhentherecordsarebeingprocessedforthesubscriberormemberdirectly.
● Feesorchargesforadministrativetasks,suchasthoseenumeratedabove,maynotbeassessedagainstallmembersintheformofanofficeadministrativefee,butrathertoonlythosememberswhoutilizetheadministrativeservice.
Participation in Provider Reimbursement
Primary Care Practitioners and Specialists/ProvidersCareFirstBlueChoicePCPsarereimbursedonafee-for-servicebasisforbillableservices,suchasofficevisitsandprocedures.
Physician AssistantsCareFirstBlueChoicedoesnotcontractwithPhysicianAssistants(PA).CoveredservicesrenderedbyaPAareeligibleforreimbursementunderthefollowingcircumstances:
● PAisunderthesupervisionofaphysicianasrequiredbylocallicensingagencies.
● ServicesrenderedbythePAaresubmittedunderthesupervisingphysician’snameandprovidernumber.
HIPAA Compliant Codes
TocomplywiththerequirementsoftheHealthInsurancePortabilityandAccountabilityAct(HIPAA),CareFirstandCareFirstBlueChoicewilladdtheHIPAA-compliantcodesandcorrespondingreimbursementratestoyourfeeschedulewhentheyarereleasedfromAMAorCMS.Theseupdatesaremadeonaquarterlybasisthroughthecalendaryear.
In-Office Injectable Drugs Standard Reimbursement Methodology
In-OfficeInjectabledrugsarereimbursedatapercentageoftheAverageSalesPrice(ASP).In-OfficeInjectabledrugswithoutanASParereimbursedatapercentageofthelowestAverageWholesalePrice(AWP).TheASPiscalculatedbytheCentersforMedicare&MedicaidServices(CMS)andavailableatCMS .gov .TheAWPisbasedonthemostcosteffectiveproductandpackagesizeasreferencedinThomson’sRedBook.
Reimbursementforallin-officeinjectabledrugsisupdatedquarterlyonthefirstofFebruary,May,AugustandNovember.Theratesareineffectfortheentirequarterbutaresubjecttochangeeachquarter.P4OncologyandP4Rheumatologyfeeschedulesarenotincludedinthisreimbursementmethodology.
Collection of Retroactively Denied ClaimsAproviderreimbursementmaybeoffsetagainstaretroactivelydeniedclaimbyanaffiliatedcompanyofCareFirst,Inc.
47
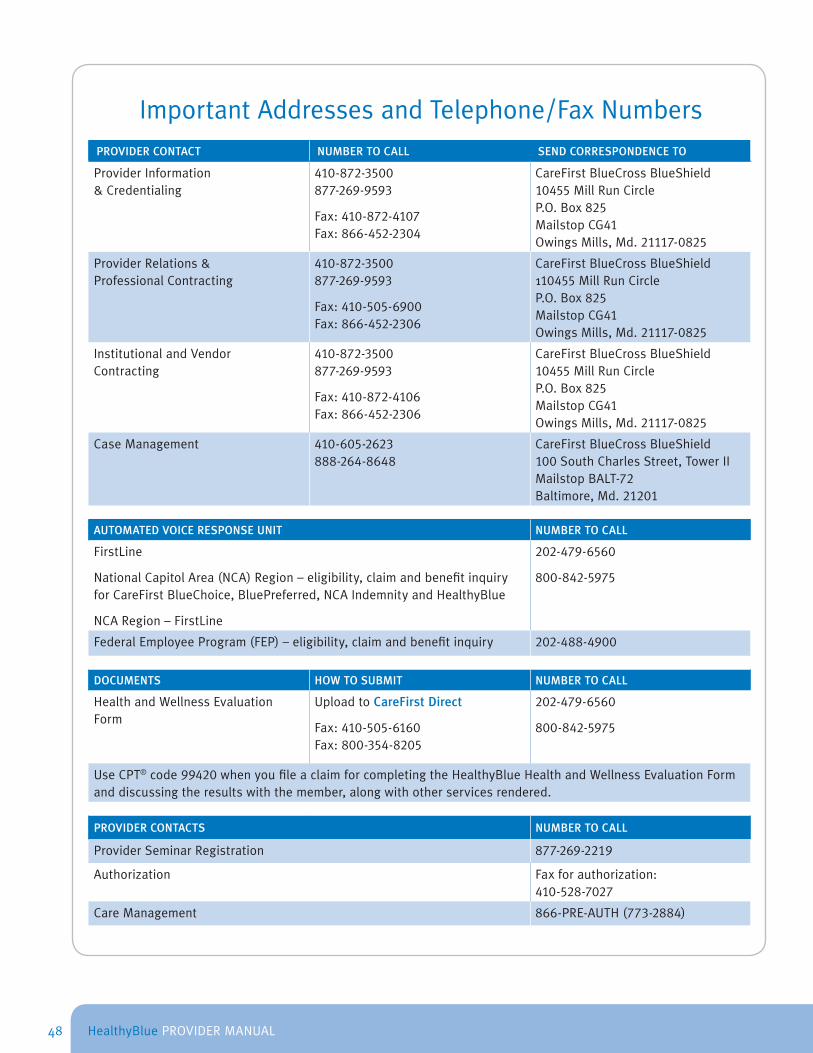
HealthyBluePROVIDERMANUAL
ImportantAddressesandTelephone/FaxNumbersPROVIDER CONTACT NUMBER TO CALL SEND CORRESPONDENCE TO
ProviderInformation&Credentialing
410-872-3500 877-269-9593
Fax:410-872-4107 Fax:866-452-2304
CareFirstBlueCrossBlueShield10455MillRunCircleP.O.Box825 MailstopCG41OwingsMills,Md. 21117-0825
ProviderRelations&ProfessionalContracting
410-872-3500 877-269-9593
Fax: 410-505-6900 Fax: 866-452-2306
CareFirstBlueCrossBlueShield110455MillRunCircleP.O.Box825 MailstopCG41OwingsMills,Md. 21117-0825
InstitutionalandVendorContracting
410-872-3500 877-269-9593
Fax:410-872-4106 Fax:866-452-2306
CareFirstBlueCrossBlueShield10455MillRunCircleP.O.Box825 MailstopCG41OwingsMills,Md. 21117-0825
CaseManagement 410-605-2623 888-264-8648
CareFirstBlueCrossBlueShield100SouthCharlesStreet,TowerIIMailstopBALT-72Baltimore,Md.21201
AUTOMATED VOICE RESPONSE UNIT NUMBER TO CALL
FirstLine
NationalCapitolArea(NCA)Region–eligibility,claimandbenefitinquiryforCareFirstBlueChoice,BluePreferred,NCAIndemnityandHealthyBlue
NCARegion–FirstLine
202-479-6560
800-842-5975
FederalEmployeeProgram(FEP)–eligibility,claimandbenefitinquiry 202-488-4900
DOCUMENTS HOW TO SUBMIT NUMBER TO CALL
HealthandWellnessEvaluationForm
UploadtoCareFirst Direct
Fax:410-505-6160 Fax:800-354-8205
202-479-6560
800-842-5975
UseCPT®code99420whenyoufileaclaimforcompletingtheHealthyBlueHealthandWellnessEvaluationFormanddiscussingtheresultswiththemember,alongwithotherservicesrendered.
PROVIDER CONTACTS NUMBER TO CALL
ProviderSeminarRegistration 877-269-2219
Authorization Faxforauthorization:410-528-7027
CareManagement 866-PRE-AUTH(773-2884)
48
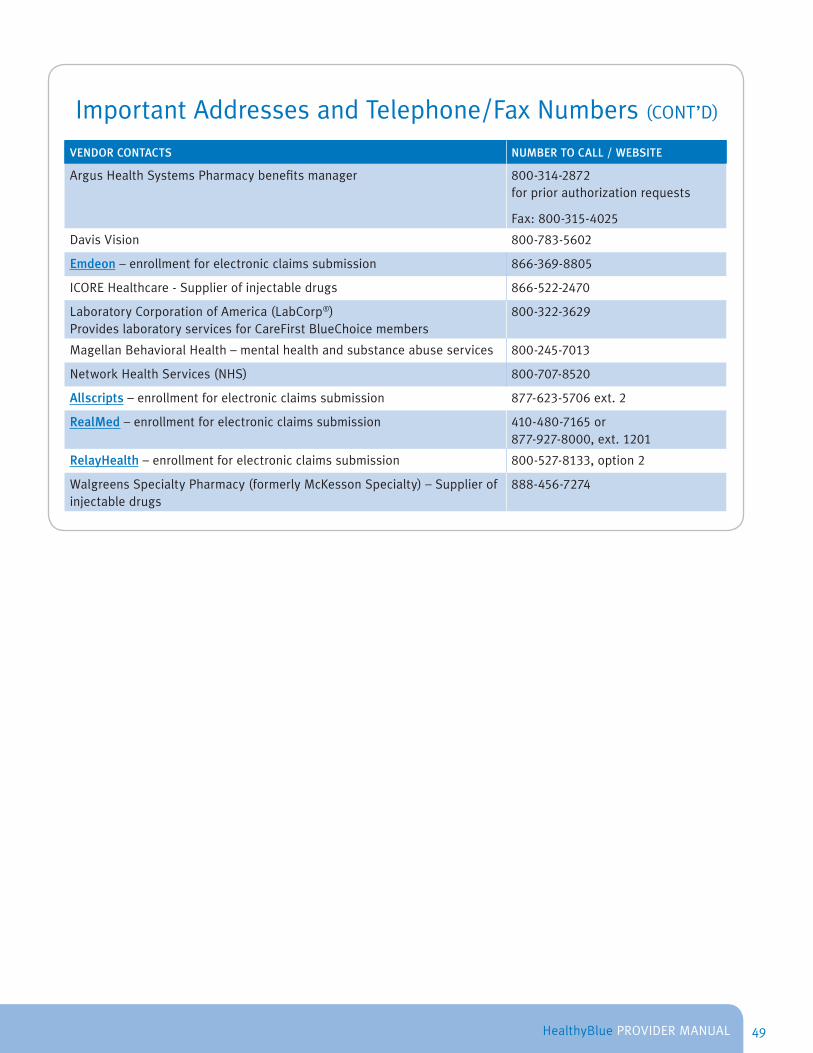
HealthyBluePROVIDERMANUAL
ImportantAddressesandTelephone/FaxNumbers(CONT’D)
VENDOR CONTACTS NUMBER TO CALL / WEBSITE
ArgusHealthSystemsPharmacybenefitsmanager 800-314-2872 forpriorauthorizationrequests
Fax:800-315-4025
DavisVision 800-783-5602
Emdeon–enrollmentforelectronicclaimssubmission 866-369-8805
ICOREHealthcare-Supplierofinjectabledrugs 866-522-2470
LaboratoryCorporationofAmerica(LabCorp®)ProvideslaboratoryservicesforCareFirstBlueChoicemembers
800-322-3629
MagellanBehavioralHealth–mentalhealthandsubstanceabuseservices 800-245-7013
NetworkHealthServices(NHS) 800-707-8520
Allscripts–enrollmentforelectronicclaimssubmission 877-623-5706ext.2
RealMed–enrollmentforelectronicclaimssubmission 410-480-7165 or 877-927-8000, ext. 1201
RelayHealth–enrollmentforelectronicclaimssubmission 800-527-8133,option2
WalgreensSpecialtyPharmacy(formerlyMcKessonSpecialty)–Supplierofinjectabledrugs
888-456-7274
49
HealthyBluePROVIDERMANUAL
Frequently Asked Questions
1 . Why is CareFirst BlueChoice offering HealthyBlue?Inanefforttoreducetherisingcostofhealthcareandenhancehealthylifestylesthroughanengagedpatient/providerrelationship,CareFirstBlueChoicedevelopedHealthyBlue.Thisnewproductisaboldapproachtohealthcarethatencouragesprimarycareproviderstoworkcloselywiththeirpatientstominimizehealthrisksinordertoachieveandmaintainhealthyoutcomes.
2. Which provider specialties are considered PCPs?HealthyBluerecognizesthefollowingspecialtiesasprimarycareproviders(PCPs):FamilyPractice,GeneralPractice,InternalMedicine,PediatricsandGeriatrics.
Note:OB/GYNswhowishtoserveasamember’sPCPmustgivethememberaletterexpressingtheirwishtoserveasthePCP.ThememberwillsubmitthelettertoMemberServices.OnceselectedasthePCP,OB/GYNswillhavethesameprivilegesasotherPCPs,includingwritingreferrals.
3. How can I tell whether my patient is eligible for HealthyBlue?Uponreviewofthemember’sHealthyBlueIDcard,useCareFirst Directtoconfirmtheireligibilityandeffectivedateofcoverage.
4. Am I required to schedule appointments within a certain timeframe?HealthyBluerequiresthattheHealthandWellnessEvaluationandapplicablescreeningsandimmunizationstakeplacewithin90daysofthemember’scontracteffectivedate.However,thePCPwillhave120daystosubmittheHealthandWellnessEvaluationFormtoCareFirst
50

HealthyBluePROVIDERMANUAL
BlueChoice.IfyoucannotmeetwiththememberintimetoconducttherequiredhealthscreeningsandfillouttheHealthandWellnessEvaluationForm,themembermayseeanotherCareFirstBlueChoiceprovider.
PerthetermsoftheParticipationAgreement,non-symptomaticvisits,suchaspreventivecareorroutinewellness,appointmentsshouldbescheduledwithin4weeks.
5. Can I verify information about my patient on the Voice Response Unit (VRU)?Yes,youcanaccesstheVRUtoobtainthemember’sbenefitinformation.
6. Where can I find more information about HealthyBlue?AdditionalinformationaboutHealthyBlueisavailableatwww .carefirst .com/healthyblue.
Health & Wellness Evaluation Form
7. What is a Health & Wellness Evaluation Form?TheHealthandWellnessEvaluationFormisusedbyaPCPtorecordtheoutcomesofrequiredhealthscreeningsandimmunizations.Theformservesasarecordtocaptureabaselinehealthstatus,determineareasforimprovement,andpromotehealthylifestylesthroughthedevelopmentofaHealthy Action Planformemberswhoneedit,basedonthegoalsoutlinedintheform.BoththePCPandthemembermustsigntheHealthandWellnessEvaluationFormbeforethePCPsubmitsittoCareFirstBlueChoice.
8. How do I get a copy of the Health & Wellness Evaluation Form?ThemembershouldbringacopyoftheformtotheirHealthandWellnessEvaluationscreening.However,iftheyforget,acopycanbeobtainedfromwww .carefirst .com/providers/forms.
9 . .Will I get reimbursed for completing the Health & Wellness Evaluation Form and submitting it?Yes,useCPT®code99420whenyoufileaclaimforcompletingtheHealthandWellnessEvaluationForm.Theofficevisitshouldbebilledappropriatelyasapreventiveservice.The
reimbursementiscalculatedinthesamemannerasanofficevisit.
10 . .How do I submit the Health & Wellness Evaluation Form for my patient?TheHealthandWellnessEvaluationFormshouldbesubmittedusingoneofthefollowingmethods:
● SubmitthroughCareFirst Direct ● ScanthisformandsaveitinJPG,PDF,or
TIFFformat ● Click“UploadEvaluationForm”
OR
● Faxto410-505-6160or1-800-354-8205
Note: Only a CareFirst BlueChoice PCP can submit the form.
11 . .How do I submit a claim for completing the Health & Wellness Evaluation Form?SubmityourclaimtoCareFirstBlueChoiceasyounormallywouldthroughthestandardclaimssubmissionprocessusingCPT®code99420toreceivereimbursementforcompletingtheHealthandWellnessEvaluationForm.
Note: Do not send the Health & Wellness Evaluation Form with your claim.
12 . .How soon should my patient schedule an appointment to complete the Health & Wellness Evaluation Form?Themembermustscheduleanofficevisitwithyouandhaveanyapplicabletestscompletedwithin90daysoftheircoverageeffectivedatetobeconsideredforprogramincentives.YoumustsubmittheHealthandWellnessEvaluationFormtoCareFirstBlueChoicewithin120daysofthemember’scoverageeffectivedate.
Note: Iftestsarerequired,enterthedatethetestwasperformedtodocumentthatthetestwasdonewithin90daysofthemember’scoverageeffectivedate.
13 . .Where can I find the Preventive Service Guidelines?ThePreventive Service GuidelinesareavailableonourWebsite.
14 . .What is a Healthy Action Plan?AHealthy Action Planisaguidethattheproviderandthememberworktogetherto
51

HealthyBluePROVIDERMANUAL
developifthememberdoesnotmeetthenationalguidelinesduringtheinitialevaluationscreening.TheHealthy Action Planservesasaguidetoshowmembershowtoachieveandmaintainhealthy,long-termoutcomes.ItshouldalsoincludeatimeframeforwhenthememberisexpectedtoreturnfortheClinicallyAppropriateRe-Screening.TheHealthy Action Planmustbedevelopedandre-measuredpriortothemember’srenewaldate.
15 . .It was necessary to put my patient on a Healthy Action Plan. How do I submit a claim for a re-evaluation if I am treating the patient for a condition?Allservicesshouldbebilledappropriatelyforthetypeofcarerendered(i.e.sick,preventive,etc.).
16 . .Can CPT® code 99420 be processed more than once a year without the claim being rejected?Yes,thecodecanbeprocessedatamaximumoftwiceayear,permember:oncefortheHealthandWellnessEvaluationandonceforthere-screening,ifnecessary.
17 . .Can I charge my patient for another office visit when they return to sign the form?Youwilldetermineifanofficevisitsisrequiredtoreviewthetestresults,finalinformationontheform,orneedtoputthememberonaHealthy Action Plan.Ifthereisnoneedforfollow-upcareorthemembercouldsimplycomeintosigntheformsoitcanbeforwardedtoCareFirstBlueChoiceandnotincuranotherofficevisitcharge.
18 . .I submitted the Health and Wellness Evaluation Form but found there was an error on the form. How do I resubmit form?AcorrectedHealthandWellnessEvaluationFormcanberesubmittedthroughCareFirst Directorfax(410-505-6160or1-800-354-8205).Write“CorrectedCopy”atthetopoftheform.
19 . .What is the difference between a waiver and an alternative standard/guideline?Awaivermeansthatthehealthmeasureisexcluded.Analternativestandard/guidelinemeansthatanewgoalisset.Youmaydeterminethatawaiverisappropriatefor
anygivenhealthmeasure(s).Youmayalsodeterminethatthemembercannotmeettheinitialstandard,andthereisnoappropriatealternativestandard/guidelinethatwillallowthemembertomeetthenationalguidelines.
20 . .How do I document a waiver or alternative standard/guideline?ThereareboxesontheHealthandWellnessEvaluationFormtoindicateifaWaiverorAlternativeGuidelinewasset.Checktheappropriatebox.Provideadditionaldetailsinthe‘Comment’sectionoftheform.
21 . .My patient had another PCP complete the Health and Wellness Evaluation. Can I conduct the re-screening?MemberswillbeencouragedtousethesamePCPtoconductboththeinitialandre-screeningvisitsandcompletetheHealthandWellnessForm.However,iftheyhavechangedPCP’sorhavechosentouseanotherproviderforthere-screening,theymaydoso.Ifpossible,membersshouldprovideyouwithacopyoftheoriginalHealthandWellnessEvaluationFormshowingtheresultsfromtheinitialvisitsoallinformationwillbeononeform.IfthisisnotpossibletheyshouldbringyouablankcopyoftheformoryoucangetacopyfromourWebsiteatwww .carefirst .com/providers/forms.
22 . .The Health and Wellness Evaluation Form was returned to me with a request for additional and/or corrected information. I already submitted my claim for the services. How should I resubmit this form?Maketheadditions/correctionsonyourcopyoftheHealthandWellnessEvaluationForm.NoteCorrected FormatthetopanduploadittoCareFirst Directorfax(410-505-6160or1-800-354-8205).Thereisnoneedtoresubmittheclaim.
23 . .My patients continue to contact me about an incentive and said that what I put on the form impacted the amount they received. Do I need to be involved with this?No,howeveritishelpfultoreviewthemember’sHealthandWellnessEvaluationFormforaccuracyifmembersareallegingthatthereisaclericalerror(comparedtoyourmedicaldocumentation),andtomaintaintimelineswithsubmissiondaterequirements.
52

HealthyBluePROVIDERMANUAL
Yourresponsibilitiesinclude:schedulingatimelyinitialevaluationandscreeningwiththemember,completingtheInitialScreeningsectionontheHealthandWellnessEvaluationFormincludingdocumentationofeachofthehealthmeasuresforthisspecificmember,yourdecisionanddocumentationontheastowhetherornotanalternativestandardorwaiverwillbeallowedasappropriate,reviewoftheformwiththememberandyourssignaturesontheformandsubmissiontoCareFirstBlueChoice.
Referral Process
24 . .As a CareFirst BlueChoice PCP, I never had to submit a referral to CareFirst BlueChoice. Why do I have to do this now?HealthyBlueencouragesyoutocoordinatethemembers’careandrequiresthatyourefermemberstoaCareFirstBlueChoicespecialistinordertohavethelowestout-of-pocketexpenses.Therefore,itisnecessaryforCareFirstBlueChoicetoreceivethereferralfromyoutoensurethatservicesareprocessedappropriatelyformembers.
25 . .How do I submit a referral to CareFirst BlueChoice?Mailreferralsto:
MailAdministratorP.O.Box14116Lexington,Ky.40512-4116
26 . .Should I use the Uniform Consultation Referral Form for submission of a referral for a HealthyBlue member?Yes,youshouldusethesameformasforotherCareFirstBlueChoicereferrals.
27 . .Why must my patient always have a referral?ReferralsfromaCareFirstBlueChoicePCPtoanotherCareFirstBlueChoiceproviderareneededformemberstoreceivethelowestout-of-pocketexpenses.Thosememberswhoseekcarewithoutareferralaresubjecttohigherdeductiblesandcopays/coinsurance.
28 . .I am a specialist with a referral from my patient’s PCP. I must send them to another provider for care on this same condition, but the referral is only for 3 visits and I know it will require more visits than this. Is it necessary for my patient to get another referral from their PCP? WithHealthyBlue,oncethenumberofvisitsexpires,thepatientmustcontactthePCPtogetanadditionalreferralformorevisits,evenifitisforthesameconditionlistedontheoriginalreferral.
29 . .My patients say they do not need a referral to schedule a visit but their membership card does not state Open Access. Can I still render services?Yes,Open AccessisnotwrittenontheHealthyBlueidentificationcards(ID),however,allHealthyBlueproductshavetheOpen Accessfeature.Memberswhoseekcarewithoutareferralmaydosohowever,theymaybesubjecthigherdeductiblesandcopays/coinsurance.
53

HealthyBluePROVIDERMANUAL
Index
AAlternativestandard/guideline6AppealsProcess43Authorizations18
BBenefitDesign11
CClinicallyAppropriateRe-Screening7
DDiseaseManagement24
EEmergencyRoomServices22
H
HealthandWellnessEvaluationForm5HealthAssessment4HealthyActionPlan7HospitalServices23
I
IdentificationCards13InitialEvaluationScreening6
L
LaboratoryServices30
P
PlanOptions9PrimaryCareProvider20
R
ReferralProcess15RoutineOfficeVisits21
S
SampleHealthyBlueBenefitDesign11Specialistservices16
W
WebResources45
54

HealthyBluePROVIDERMANUAL
From the CareFirst BlueCross BlueShield family of health care plans .
More to feel good about.840FirstStreet
Washington,DC 20065
www.carefirst.com/healthyblue
CareFirst is used as a collective reference for CareFirst BlueChoice, Inc. and CareFirst BlueCross BlueShield.
BOK5408-1S (6/12)
CareFirst BlueChoice, Inc. is an independent licensee of the Blue Cross and Blue Shield Association. CareFirst BlueCross BlueShield is an independent licensee of the Blue Cross and Blue Shield Association, providing access to the Preferred Provider
Organization Network only and does not assume any financial risk or obligation with respect to claims. ®Registered trademark of the Blue Cross and Blue Shield Association. ®’Registered trademark of CareFirst of Maryland, Inc.
55

















