35
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None
Management of Heart Failure
and Cardiomyopathies in
Pregnancy
Professor Sanjay Sharma
Disclosures: None
Cardiovascular disease in pregnancy is increasing in the Western World.
0.2-3% of all pregnancies in industrialised countries are complicated by cardiovascular disease.
Increasing prevalence of ischaemic heart disease due to advancing age of first pregnancy.
Congenital heart disease is the most frequent cardiovascular disease present during pregnancy (75-82%).
Heart failure complicates 4.6 per 100,000 pregnancies
Epidemiology of Cardiac Disease In Pregnancy
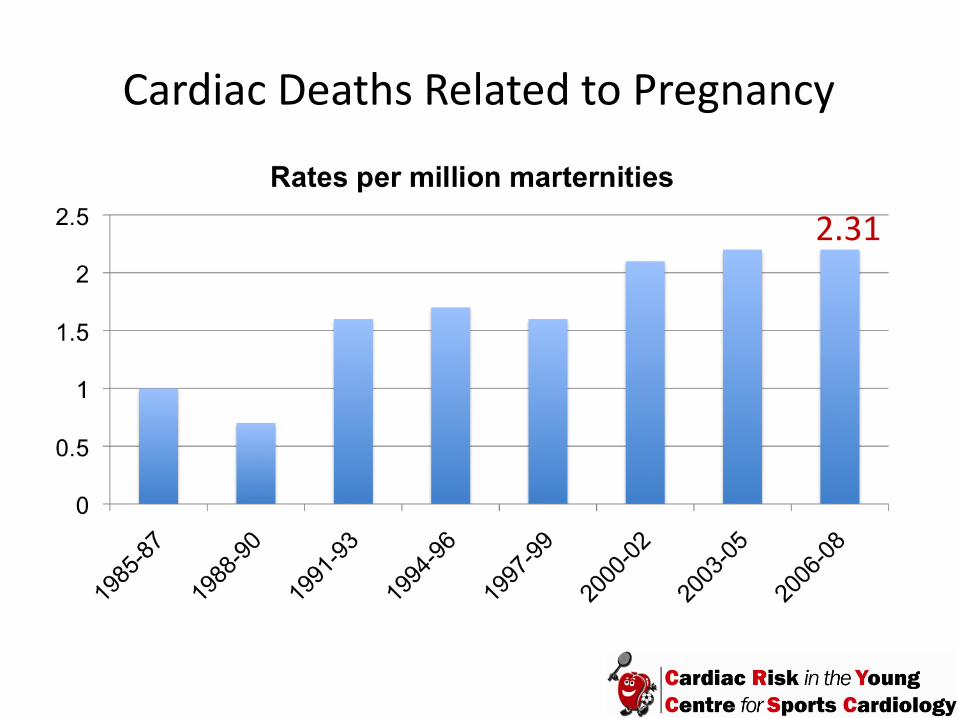
Cardiac Deaths Related to Pregnancy
2.31
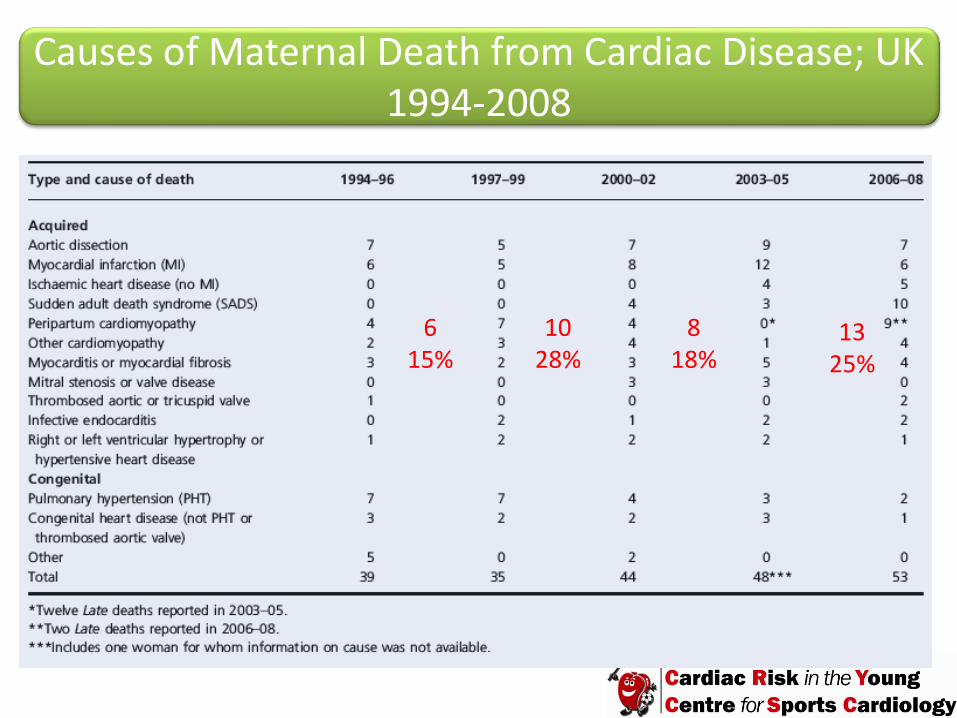
Causes of Maternal Death from Cardiac Disease; UK 1994-2008
13 25%
6 15%
10 28%
8 18%

10
1
3
3
4
4
4
5
7
9
50
0 20 40 60
Other
Doxorubicin
Substance abuse
Connective tissue disease
Peripartum
HTN
HIV
Infiltrative
IHD
Myocarditis
Idiopathic
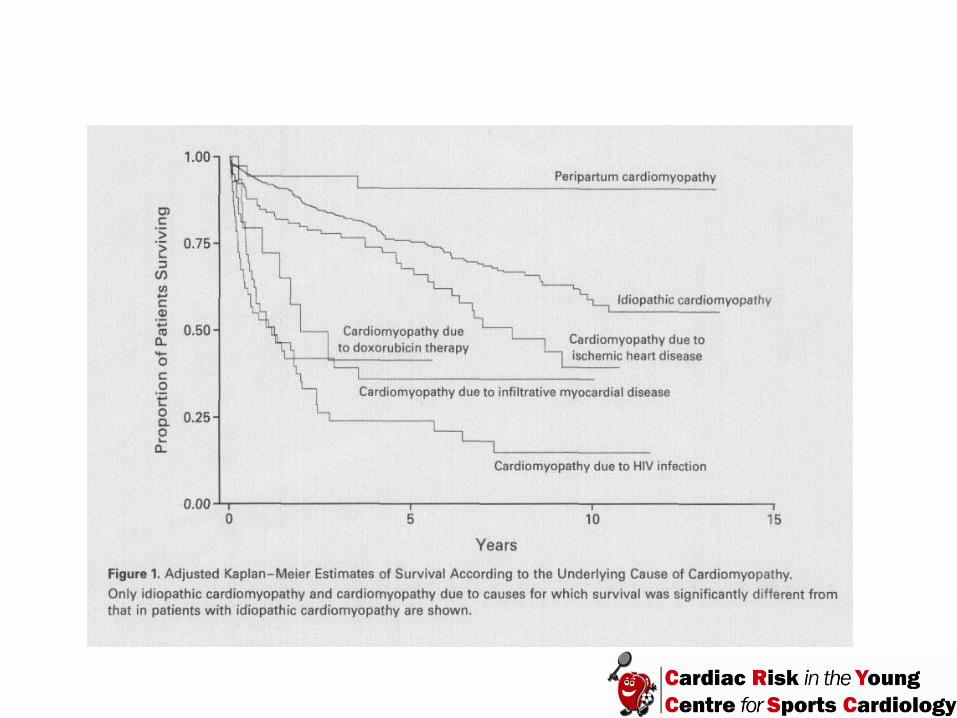
% Felker M et al NEJM 2000
Causes of Cardiomyopathy in Pregnancy

STRESSES Increased plasma volume (30-50%) Increased stroke volume Increased heart rate Increased myocardial oxygen consumption Auto-transfusion during uterine involution Hypercoagulability
Impact of the Pregnancy Related Changes in Cardiovascular Physiology in Patients with Impaired Cardiac Function
CONSEQUENCES
IMPAIRED FUNCTION
Pulmonary congestion Acute decompensated cardiac failure Arrhythmias Systemic thrombo-embolism DEATH

CARPREG Multicentre Study
562 consecutive women with heart disease
Pulmonary oedema, arrhythmia, stroke and death complicated 13% of pregnancies
Neonatal complication rate 20%
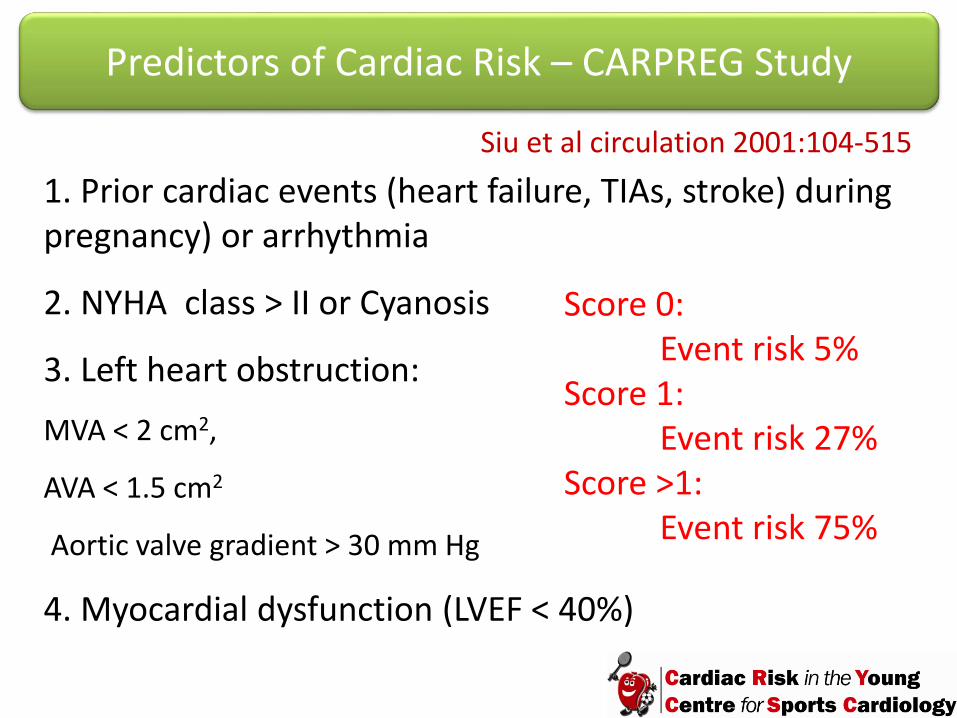
1. Prior cardiac events (heart failure, TIAs, stroke) during pregnancy) or arrhythmia
2. NYHA class > II or Cyanosis
3. Left heart obstruction:
MVA < 2 cm2,
AVA < 1.5 cm2
Aortic valve gradient > 30 mm Hg
4. Myocardial dysfunction (LVEF < 40%)
Predictors of Cardiac Risk – CARPREG Study
Score 0: Event risk 5%
Score 1: Event risk 27%
Score >1: Event risk 75%
Siu et al circulation 2001:104-515

Risk stratification and Ante-natal counselling Joint care in a multi-disciplinary setting in a specialist centre Alteration of drug therapies Requirement for anticoagulation Frequent surveillance Anticipate problems
Essentials in the Management of Women with Impaired Ventricular Function
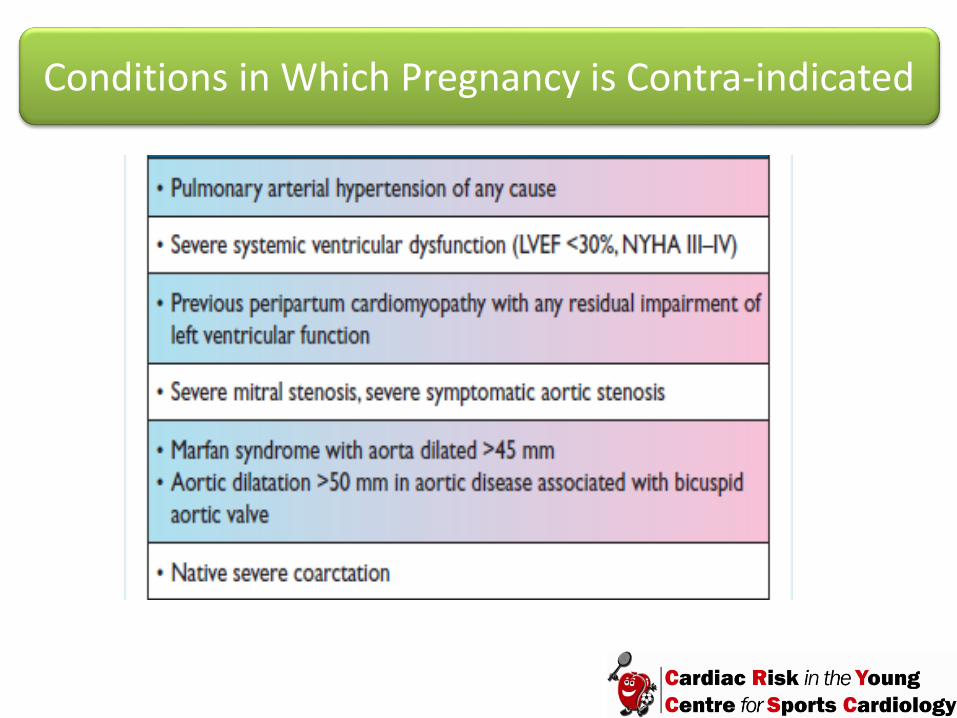
Conditions in Which Pregnancy is Contra-indicated

‘An idiopathic cardiomyopathy presenting with heart failure secondary to left ventricular systolic dysfunction towards to the end of pregnancy or in the months following delivery. It is a diagnosis of exclusion. The LV may not be dilated but the ejection fraction is nearly always reduced below 45%.’
Peripartum Cardiomyopathy

Risk Factors for Peripartum Cardiomyopathy
Multiple Pregnancy
Pregnancy complicated by Hypertension
Multiparity Advanced
maternal age
Afro-Caribbean Race

Peripartum Cardiomyopathy
1/3000 live births May present with
acute left ventricular failure and low cardiac
output state
Diagnosis based on
echo and the absence of an
alternative cause
Rare before 36/52
More common in West Africans
? Viral myocarditis
Immune Oxidative
stress Lake salt
Selenium def
Treat with conventional heart failure therapy and
anticoagulation
50% recover 10% die within 2 years
Mortality as high as 15% in African women
0-11% require transplant
30-50% have recurrence during a subsequent
pregnancy. Advise against pregnancy in women whose LVEF has
not normalised
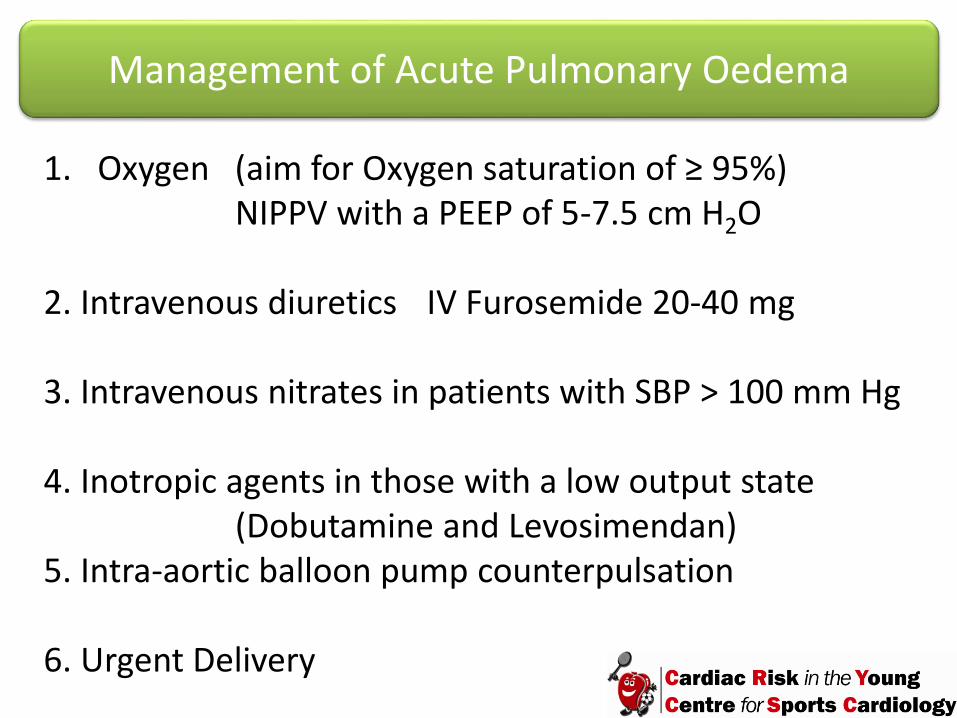
1. Oxygen (aim for Oxygen saturation of ≥ 95%) NIPPV with a PEEP of 5-7.5 cm H2O 2. Intravenous diuretics IV Furosemide 20-40 mg 3. Intravenous nitrates in patients with SBP > 100 mm Hg 4. Inotropic agents in those with a low output state (Dobutamine and Levosimendan) 5. Intra-aortic balloon pump counterpulsation 6. Urgent Delivery
Management of Acute Pulmonary Oedema
Therapeutic Options After Managing Acute Heart Failure
Pharmacotherapy Device Therapy LV Assistance Device Implantable cardioverter defibrillators ± Cardiac Resynchronisation therapy Transplantation
Loop diuretics
ACE inhibitors
Angiotensin II receptor blockers
Spironolactone
Beta-blockers
Digoxin
Nitrates
Hydralazine
PROGNOSTIC BENEFIT
Conventional Pharmacological Therapy

Loop diuretics
ACE inhibitors
Angiotensin II receptor blockers
Spironolactone
Beta-blockers
Digoxin
Nitrates
Hydralazine
PROGNOSTIC BENEFIT
Pharmacological Therapy During Pregnancy
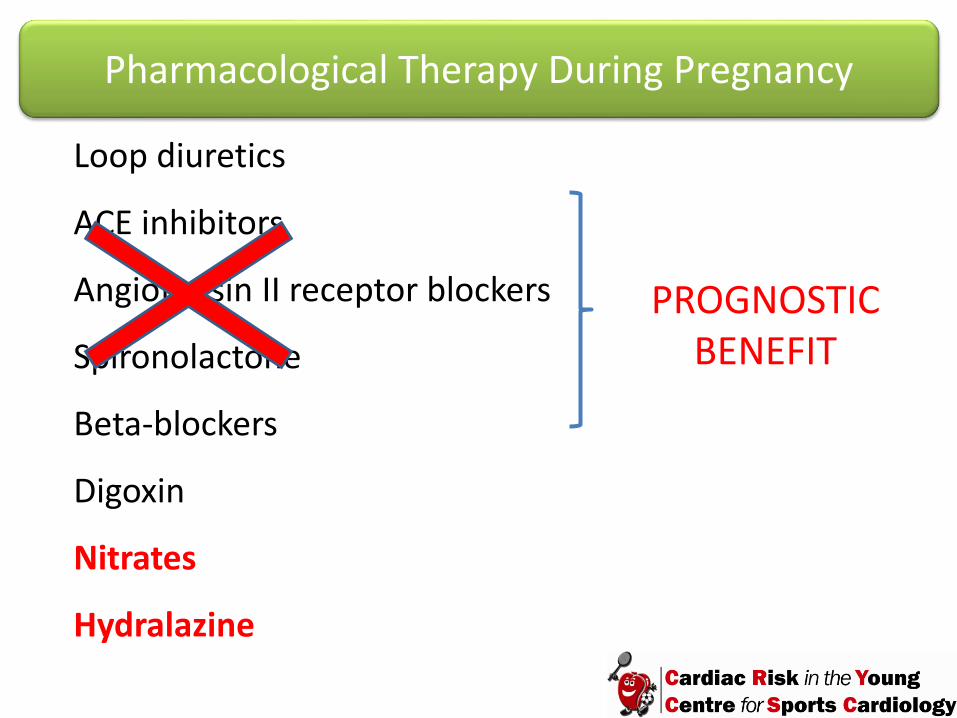
Loop diuretics
ACE inhibitors
Angiotensin II receptor blockers
Spironolactone
Beta-blockers
Digoxin
Nitrates
Hydralazine
PROGNOSTIC BENEFIT
Pharmacological Therapy During Pregnancy
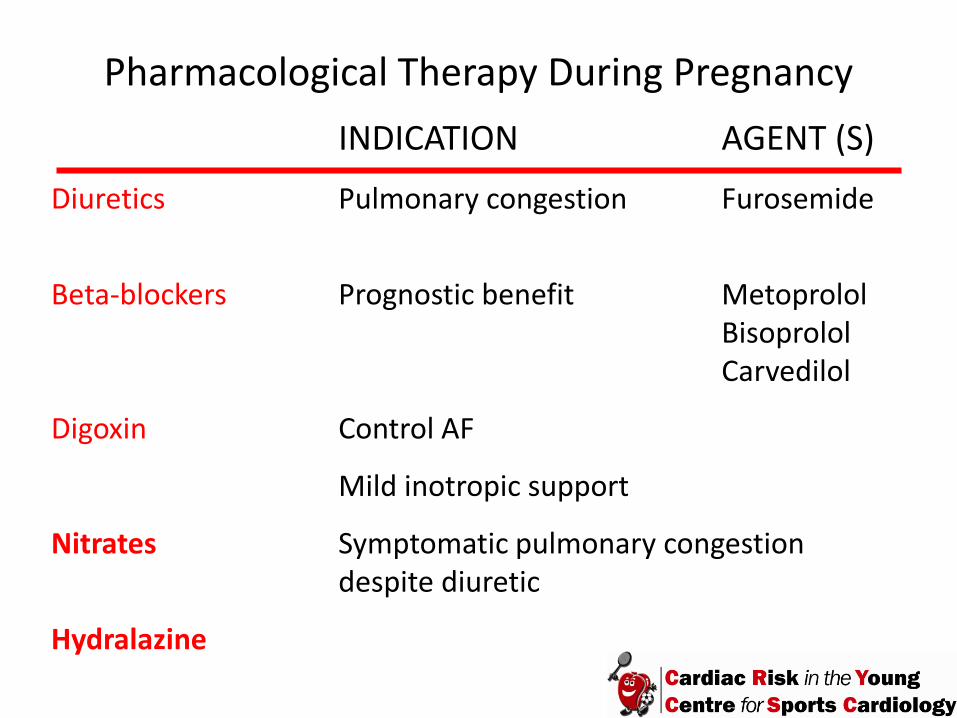
Pharmacological Therapy During Pregnancy
INDICATION AGENT (S)
Diuretics Pulmonary congestion Furosemide
Beta-blockers Prognostic benefit Metoprolol Bisoprolol Carvedilol
Digoxin Control AF
Mild inotropic support
Nitrates Symptomatic pulmonary congestion despite diuretic
Hydralazine

Special Precautions with Drugs
Loop Diuretic Reduce placental perfusion Beta-blockers Fetal bradycardia Intra-uterine growth retardation Apnoeic episodes Hypoglycaemia MONITOR NEWBORNS FOR 24-48 h

Indications for Anticoagulation
Intramural thrombus Systemic thromboembolism Paroxysmal or persistent AF in females with DCM Left ventricular ejection fraction < 35% Concomitant use of Bromocriptine
Anticoagulation in Heart Failure Patients
Warfarin Avoid in first trimester and last 4-8 weeks of pregnancy Maintain INR ≥ 2
Low Molecular Weight Heparin Enoxaparin and Dalteparin SC Dose adjusted Give as a twice daily regime Monitor weekly 4 h post dose Anti Xa levels (0.8-1.2)

Anticoagulation in Heart Failure Patients
Stop LMWT Heparin once contractions have started. Don’t recommence anticoagulation until all bleeding has stopped after delivery. Warfarin can be resumed after delivery. Anticoagulate for 6 months in PPCM.

Pharmacological Therapy After Delivery
ACE I Enalapril, Captopril, Bezapril Beta-blockers Bisoprolol, Metoprolol, Carvedilol Aldo antagonist Spironolactone Nitrates Hydralazine Diuretics Furosemide Digoxin Warfarin

Role of Bromocriptine
Oxidative stress Activates Cathepsin D
Cleaves Prolactin to a 16 kDa fragment
Angiostatic Pro-apoptotic
Bromocriptine prevents onset of PPCM in a mouse model
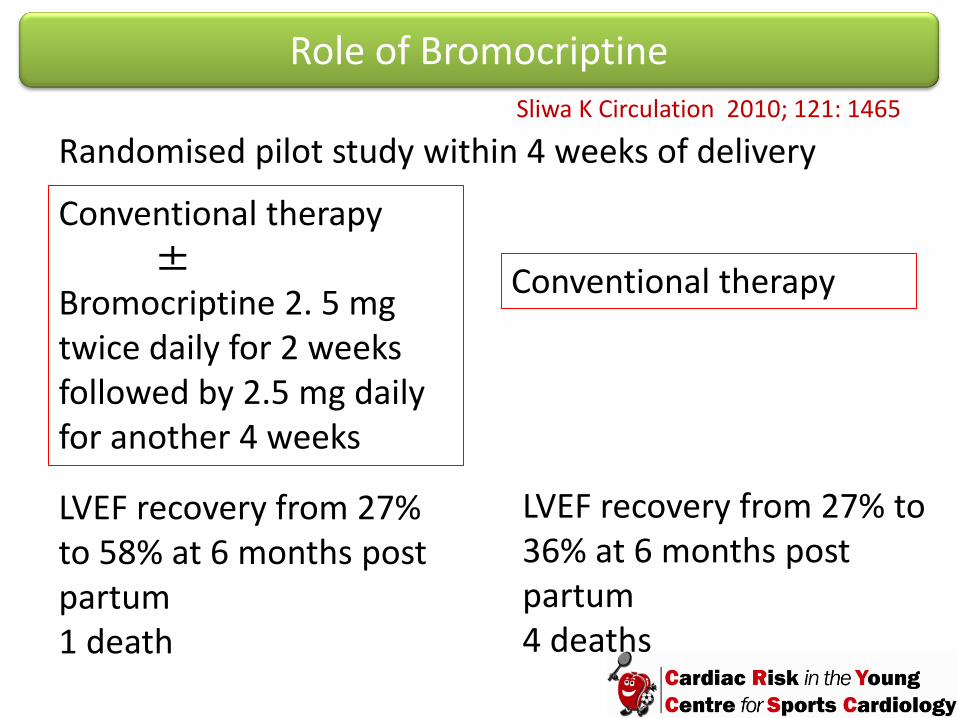
Role of Bromocriptine
Randomised pilot study within 4 weeks of delivery
Conventional therapy ± Bromocriptine 2. 5 mg twice daily for 2 weeks followed by 2.5 mg daily for another 4 weeks
Conventional therapy
LVEF recovery from 27% to 58% at 6 months post partum 1 death
LVEF recovery from 27% to 36% at 6 months post partum 4 deaths
Sliwa K Circulation 2010; 121: 1465
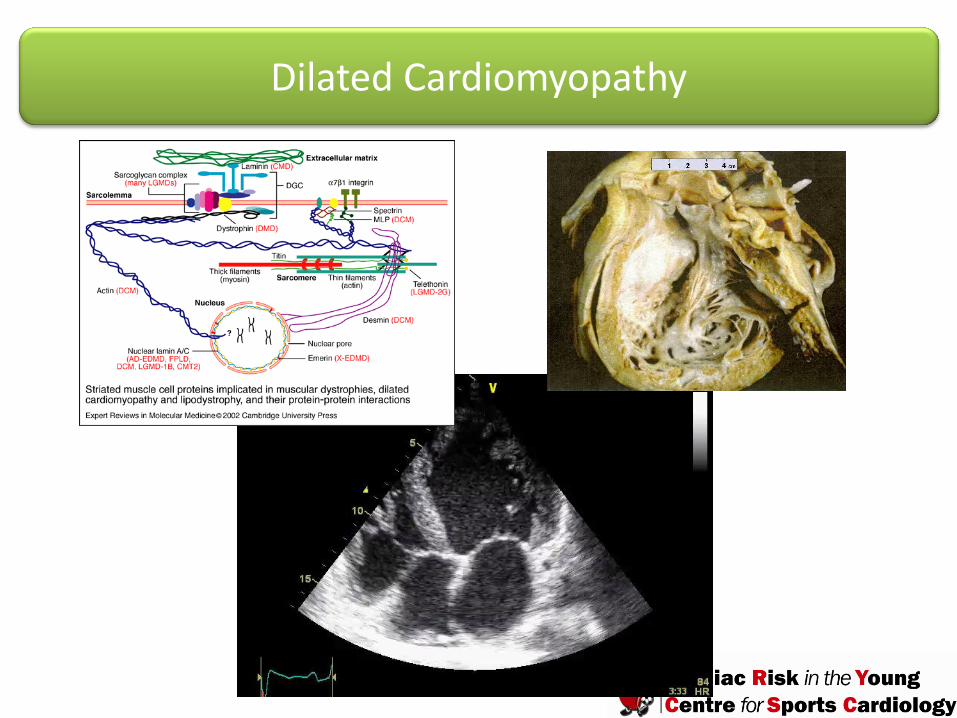
Dilated Cardiomyopathy

Dilated Cardiomyopathy - Management
Counselled about the risks of pregnancy. Same as conventional heart failure. Avoid ACEI, A2RB and aldosterone antagonists during pregnancy. Anticoagulation (guidelines as with PPCM) IV furosemide 20-40 mg during third stage to reduce risk of pulmonary oedema from auto-transfusion secondary to involution of the uterus.

Hypertrophic Cardiomyopathy

Pulmonary Congestion
Outflow obstruction Arrhythmias
Hypertrophic Cardiomyopathy- Management During Pregnancy
Beta-blockers when maximal wall thickness > 15 mm, LV outflow gradient > 30 mm Hg or ventricular arrhythmias. Verapamil also effective in reducing LV obstruction. Close monitoring of females with high risk profile. Anticoagulation in females with paroxysmal or persistent AF. Consider DC cardioversion in acute symptomatic AF. Cautious use of diuretics.
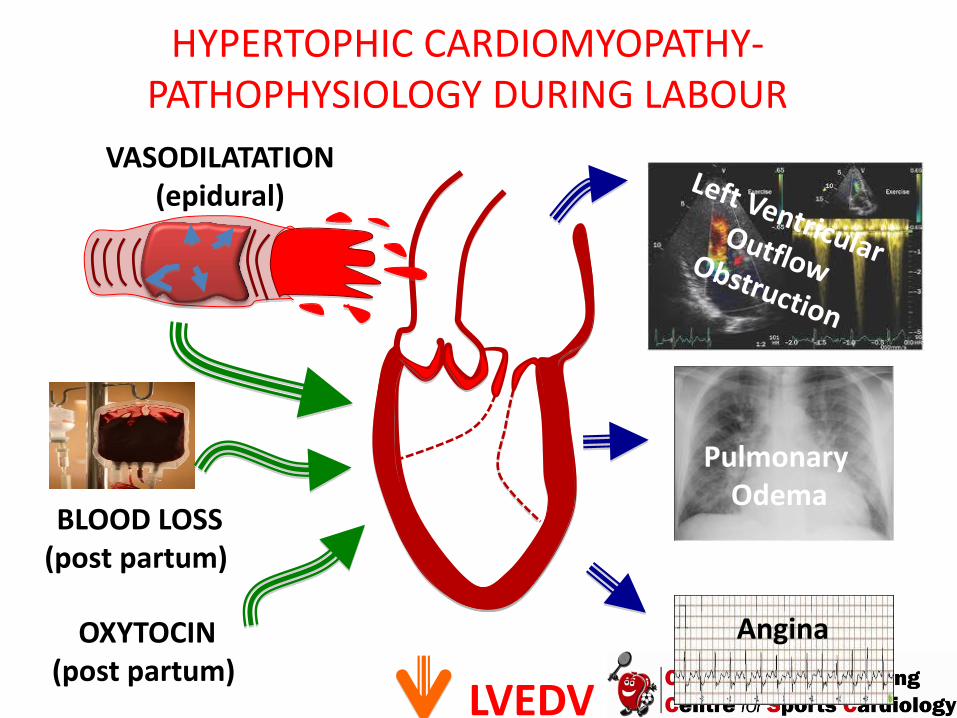
VASODILATATION (epidural)
BLOOD LOSS (post partum)
Pulmonary Odema
Angina
LVEDV
HYPERTOPHIC CARDIOMYOPATHY- PATHOPHYSIOLOGY DURING LABOUR
OXYTOCIN (post partum)
Hypertrophic Cardiomyopathy- Management During Labour
Aim for vaginal delivery Careful BP monitoring with epidural anaesthesia Replenish blood loss rapidly Judicious care with IV fluids Oxytocin infusion in the third stage of labour

Cardiomyopathies are amongst the commonest causes of maternal death in pregnancy in the Western World. Care should be provided in specialised joint obstetric/cardiac units.

















