Heart Failure Care in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis Thomas Callender 1 , Mark Woodward 1,2 , Gregory Roth 3 , Farshad Farzadfar 4,5 , Jean-Christophe Lemarie 6 , Ste ´ phanie Gicquel 6 , John Atherton 7 , Shadi Rahimzadeh 4,8 , Mehdi Ghaziani 4,5 , Maaz Shaikh 1,9 , Derrick Bennett 10 , Anushka Patel 2 , Carolyn S. P. Lam 11 , Karen Sliwa 12 , Antonio Barretto 13 , Bambang Budi Siswanto 14 , Alejandro Diaz 15 , Daniel Herpin 16 , Henry Krum 17 , Thomas Eliasz 1 , Anna Forbes 1 , Alastair Kiszely 1 , Rajit Khosla 1 , Tatjana Petrinic 18 , Devarsetty Praveen 2,9 , Roohi Shrivastava 1 , Du Xin 19 , Stephen MacMahon 1,2 , John McMurray 20 , Kazem Rahimi 1 * 1 The George Institute for Global Health, University of Oxford, Oxford, United Kingdom, 2 The George Institute for Global Health, University of Sydney, Sydney, Australia, 3 Institute for Health Metrics and Evaluation, University of Washington, Seattle, Washington, United States of America, 4 Non-Communicable Diseases Research Centre, Tehran University of Medical Sciences, Tehran, Iran, 5 Endocrinology and Metabolism Research Centre, Tehran University of Medical Sciences, Tehran, Iran, 6 Effi-Stat, Paris, France, 7 Department of Cardiology, Royal Brisbane and Women’s Children Hospital and University of Queensland School of Medicine, Brisbane, Australia, 8 Department of Epidemiology, Shahid Beheshti University of Medical Sciences, Tehran, Iran, 9 The George Institute for Global Health, Hyderabad, India, 10 Clinical Trials Service Unit, University of Oxford, Oxford, United Kingdom, 11 National University of Singapore, Singapore, 12 Hatter Institute for Cardiovascular Research in Africa, University of Cape Town, Cape Town, South Africa, 13 Faculdade de Medicina da Universidade de Sa ˜o Paulo, Sa ˜o Paulo, Brazil, 14 National Cardiovascular Centre University Indonesia, Jakarta, Indonesia, 15 Universidad Nacional del Centro de la Provincia de Buenos Aires, Buenos Aires, Argentina, 16 Centre Hospitalier Universitaire de Poitiers, Poitiers Cedex, France, 17 Centre of Cardiovascular Research & Education in Therapeutics, Monash University, Melbourne, Australia, 18 Bodleian Healthcare Libraries, University of Oxford, Oxford, United Kingdom, 19 The George Institute for Global Health, Peking University, Beijing, China, 20 University of Glasgow, Glasgow, United Kingdom Abstract Background: Heart failure places a significant burden on patients and health systems in high-income countries. However, information about its burden in low- and middle-income countries (LMICs) is scant. We thus set out to review both published and unpublished information on the presentation, causes, management, and outcomes of heart failure in LMICs. Methods and Findings: Medline, Embase, Global Health Database, and World Health Organization regional databases were searched for studies from LMICs published between 1 January 1995 and 30 March 2014. Additional unpublished data were requested from investigators and international heart failure experts. We identified 42 studies that provided relevant information on acute hospital care (25 LMICs; 232,550 patients) and 11 studies on the management of chronic heart failure in primary care or outpatient settings (14 LMICs; 5,358 patients). The mean age of patients studied ranged from 42 y in Cameroon and Ghana to 75 y in Argentina, and mean age in studies largely correlated with the human development index of the country in which they were conducted (r = 0.71, p,0.001). Overall, ischaemic heart disease was the main reported cause of heart failure in all regions except Africa and the Americas, where hypertension was predominant. Taking both those managed acutely in hospital and those in non- acute outpatient or community settings together, 57% (95% confidence interval [CI]: 49%–64%) of patients were treated with angiotensin-converting enzyme inhibitors, 34% (95% CI: 28%–41%) with beta-blockers, and 32% (95% CI: 25%–39%) with mineralocorticoid receptor antagonists. Mean inpatient stay was 10 d, ranging from 3 d in India to 23 d in China. Acute heart failure accounted for 2.2% (range: 0.3%–7.7%) of total hospital admissions, and mean in-hospital mortality was 8% (95% CI: 6%–10%). There was substantial variation between studies ( p,0.001 across all variables), and most data were from urban tertiary referral centres. Only one population-based study assessing incidence and/or prevalence of heart failure was identified. Conclusions: The presentation, underlying causes, management, and outcomes of heart failure vary substantially across LMICs. On average, the use of evidence-based medications tends to be suboptimal. Better strategies for heart failure surveillance and management in LMICs are needed. Please see later in the article for the Editors’ Summary. Citation: Callender T, Woodward M, Roth G, Farzadfar F, Lemarie J-C, et al. (2014) Heart Failure Care in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLoS Med 11(8): e1001699. doi:10.1371/journal.pmed.1001699 Academic Editor: Peter Byass, Umea ˚ Centre for Global Health Research, Umea ˚ University, Sweden Received December 19, 2013; Accepted June 24, 2014; Published August 12, 2014 Copyright: ß 2014 Callender et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Data Availability: The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper and its Supporting Information files. Raw data extractions are available for sharing to other researchers upon request. Funding: This work was supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre Programme and NIHR Career Development Fellowship. KR and SM are supported by the Oxford Martin School and the George Institute for Global Health. The researchers conducted this study totally independently of the funding bodies. No funding bodies had any role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Competing Interests: CL is funded by a Clinician Scientist Award from the National Medical Research Council of Singapore; receives research grants from Boston scientific, Medtronic, and Vifor Pharma; and serves as a consultant for Bayer and Novartis. JML is employed by the contract research organization Effi-Stat, which receives funding from pharmaceutical and biotechnology companies. In 2009 and 2010 Effi-Stat received financial support from Sanofi-Aventis for providing statistical analysis and programming for the I-Prefer study included in this review (reference [70]). SG is employed by the contract research organization Effi-Stat, which receives research funding from pharmaceutical and biotechnology companies. AP is a member of the Editorial Board of PLOS Medicine. PLOS Medicine | www.plosmedicine.org 1 August 2014 | Volume 11 | Issue 8 | e1001699
Transcript
Heart Failure Care in Low- and Middle-Income Countries:A Systematic Review and Meta-AnalysisThomas Callender1, Mark Woodward1,2, Gregory Roth3, Farshad Farzadfar4,5, Jean-Christophe Lemarie6,
Stephanie Gicquel6, John Atherton7, Shadi Rahimzadeh4,8, Mehdi Ghaziani4,5, Maaz Shaikh1,9,
Derrick Bennett10, Anushka Patel2, Carolyn S. P. Lam11, Karen Sliwa12, Antonio Barretto13, Bambang
Budi Siswanto14, Alejandro Diaz15, Daniel Herpin16, Henry Krum17, Thomas Eliasz1, Anna Forbes1,
Alastair Kiszely1, Rajit Khosla1, Tatjana Petrinic18, Devarsetty Praveen2,9, Roohi Shrivastava1, Du Xin19,
Stephen MacMahon1,2, John McMurray20, Kazem Rahimi1*1 The George Institute for Global Health, University of Oxford, Oxford, United Kingdom, 2 The George Institute for Global Health, University of Sydney, Sydney, Australia,
3 Institute for Health Metrics and Evaluation, University of Washington, Seattle, Washington, United States of America, 4 Non-Communicable Diseases Research Centre, Tehran
University of Medical Sciences, Tehran, Iran, 5 Endocrinology and Metabolism Research Centre, Tehran University of Medical Sciences, Tehran, Iran, 6 Effi-Stat, Paris, France,
7 Department of Cardiology, Royal Brisbane and Women’s Children Hospital and University of Queensland School of Medicine, Brisbane, Australia, 8 Department of
Epidemiology, Shahid Beheshti University of Medical Sciences, Tehran, Iran, 9 The George Institute for Global Health, Hyderabad, India, 10 Clinical Trials Service Unit, University
of Oxford, Oxford, United Kingdom, 11 National University of Singapore, Singapore, 12 Hatter Institute for Cardiovascular Research in Africa, University of Cape Town, Cape
Town, South Africa, 13 Faculdade de Medicina da Universidade de Sao Paulo, Sao Paulo, Brazil, 14 National Cardiovascular Centre University Indonesia, Jakarta, Indonesia,
15 Universidad Nacional del Centro de la Provincia de Buenos Aires, Buenos Aires, Argentina, 16 Centre Hospitalier Universitaire de Poitiers, Poitiers Cedex, France, 17 Centre of
Cardiovascular Research & Education in Therapeutics, Monash University, Melbourne, Australia, 18 Bodleian Healthcare Libraries, University of Oxford, Oxford, United Kingdom,
19 The George Institute for Global Health, Peking University, Beijing, China, 20 University of Glasgow, Glasgow, United Kingdom
Abstract
Background: Heart failure places a significant burden on patients and health systems in high-income countries. However,information about its burden in low- and middle-income countries (LMICs) is scant. We thus set out to review bothpublished and unpublished information on the presentation, causes, management, and outcomes of heart failure in LMICs.
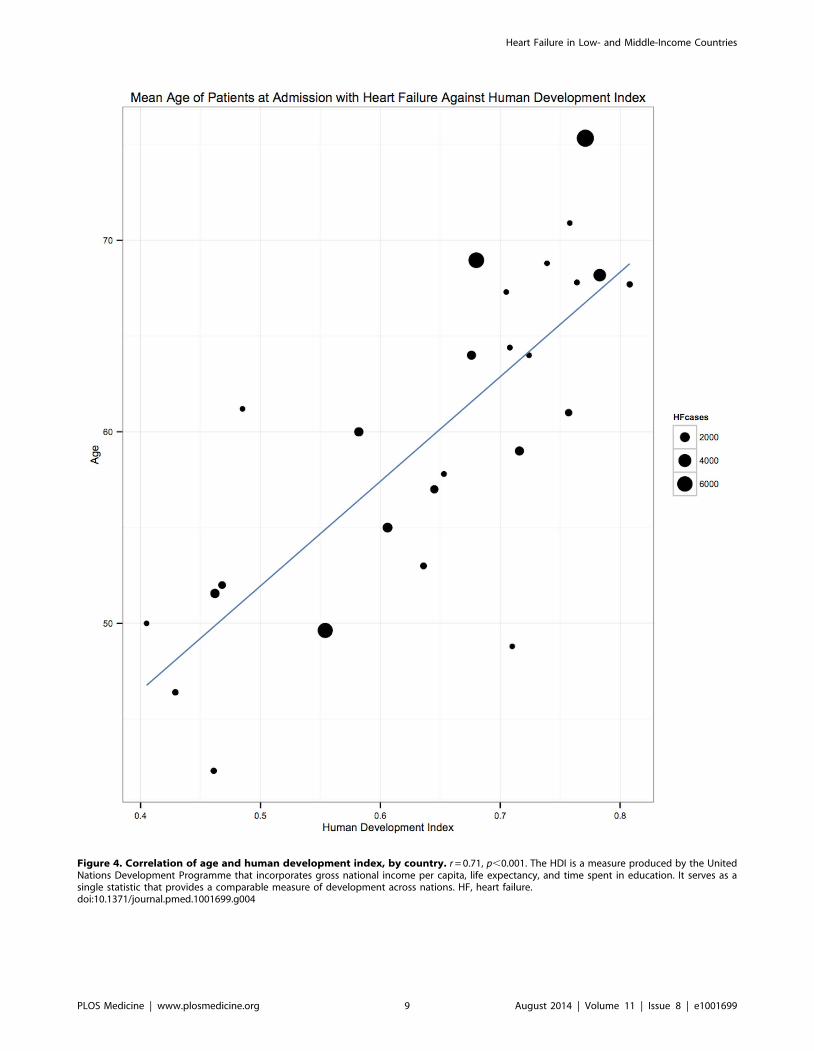
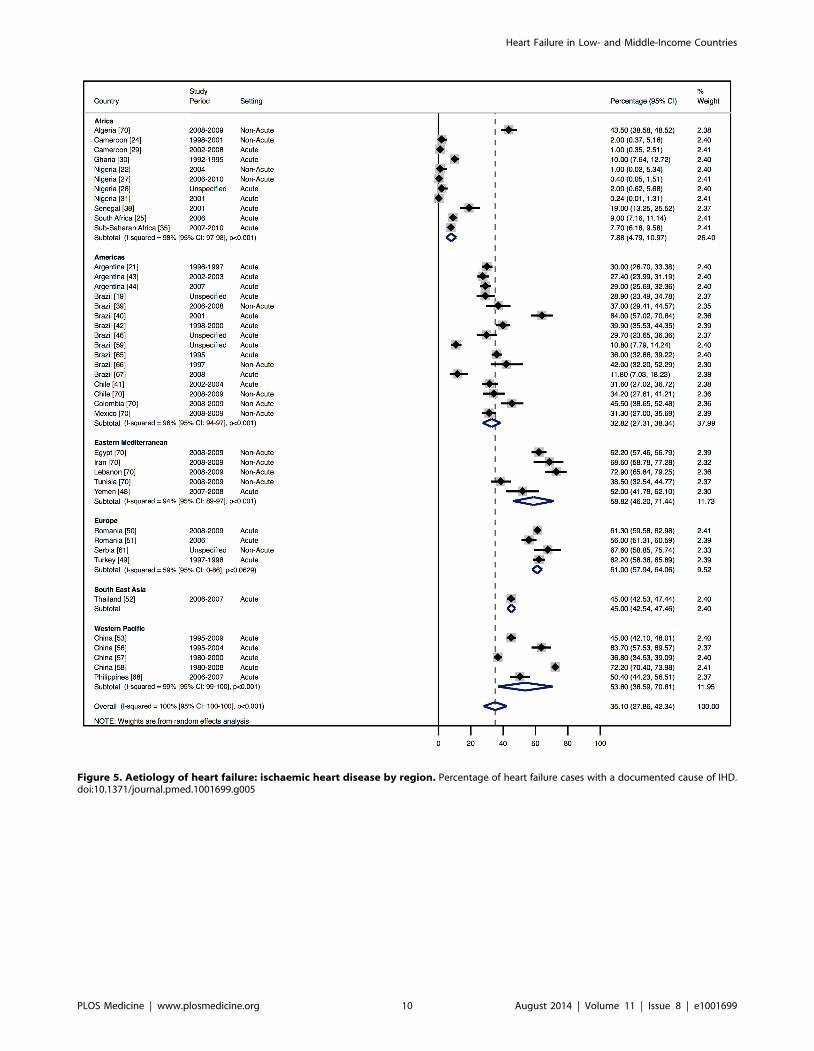
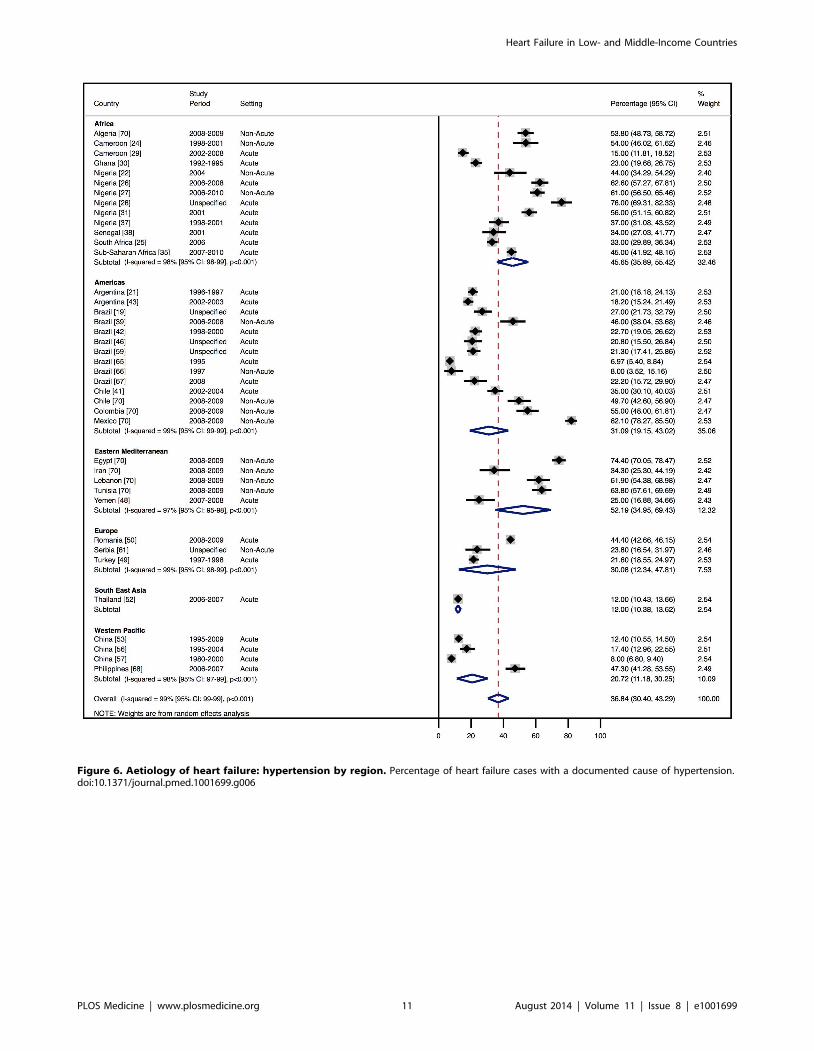
Methods and Findings: Medline, Embase, Global Health Database, and World Health Organization regional databases weresearched for studies from LMICs published between 1 January 1995 and 30 March 2014. Additional unpublished data wererequested from investigators and international heart failure experts. We identified 42 studies that provided relevant information onacute hospital care (25 LMICs; 232,550 patients) and 11 studies on the management of chronic heart failure in primary care oroutpatient settings (14 LMICs; 5,358 patients). The mean age of patients studied ranged from 42 y in Cameroon and Ghana to 75 yin Argentina, and mean age in studies largely correlated with the human development index of the country in which they wereconducted (r = 0.71, p,0.001). Overall, ischaemic heart disease was the main reported cause of heart failure in all regions exceptAfrica and the Americas, where hypertension was predominant. Taking both those managed acutely in hospital and those in non-acute outpatient or community settings together, 57% (95% confidence interval [CI]: 49%–64%) of patients were treated withangiotensin-converting enzyme inhibitors, 34% (95% CI: 28%–41%) with beta-blockers, and 32% (95% CI: 25%–39%) withmineralocorticoid receptor antagonists. Mean inpatient stay was 10 d, ranging from 3 d in India to 23 d in China. Acute heart failureaccounted for 2.2% (range: 0.3%–7.7%) of total hospital admissions, and mean in-hospital mortality was 8% (95% CI: 6%–10%). Therewas substantial variation between studies (p,0.001 across all variables), and most data were from urban tertiary referral centres.Only one population-based study assessing incidence and/or prevalence of heart failure was identified.
Conclusions: The presentation, underlying causes, management, and outcomes of heart failure vary substantially across LMICs. Onaverage, the use of evidence-based medications tends to be suboptimal. Better strategies for heart failure surveillance andmanagement in LMICs are needed.Please see later in the article for the Editors’ Summary.
Citation: Callender T, Woodward M, Roth G, Farzadfar F, Lemarie J-C, et al. (2014) Heart Failure Care in Low- and Middle-Income Countries: A Systematic Reviewand Meta-Analysis. PLoS Med 11(8): e1001699. doi:10.1371/journal.pmed.1001699
Academic Editor: Peter Byass, Umea Centre for Global Health Research, Umea University, Sweden
Received December 19, 2013; Accepted June 24, 2014; Published August 12, 2014
Copyright: � 2014 Callender et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper and itsSupporting Information files. Raw data extractions are available for sharing to other researchers upon request.
Funding: This work was supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre Programme and NIHR Career DevelopmentFellowship. KR and SM are supported by the Oxford Martin School and the George Institute for Global Health. The researchers conducted this study totally independentlyof the funding bodies. No funding bodies had any role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: CL is funded by a Clinician Scientist Award from the National Medical Research Council of Singapore; receives research grants fromBoston scientific, Medtronic, and Vifor Pharma; and serves as a consultant for Bayer and Novartis. JML is employed by the contract research organization Effi-Stat,which receives funding from pharmaceutical and biotechnology companies. In 2009 and 2010 Effi-Stat received financial support from Sanofi-Aventis forproviding statistical analysis and programming for the I-Prefer study included in this review (reference [70]). SG is employed by the contract research organizationEffi-Stat, which receives research funding from pharmaceutical and biotechnology companies. AP is a member of the Editorial Board of PLOS Medicine.
PLOS Medicine | www.plosmedicine.org 1 August 2014 | Volume 11 | Issue 8 | e1001699
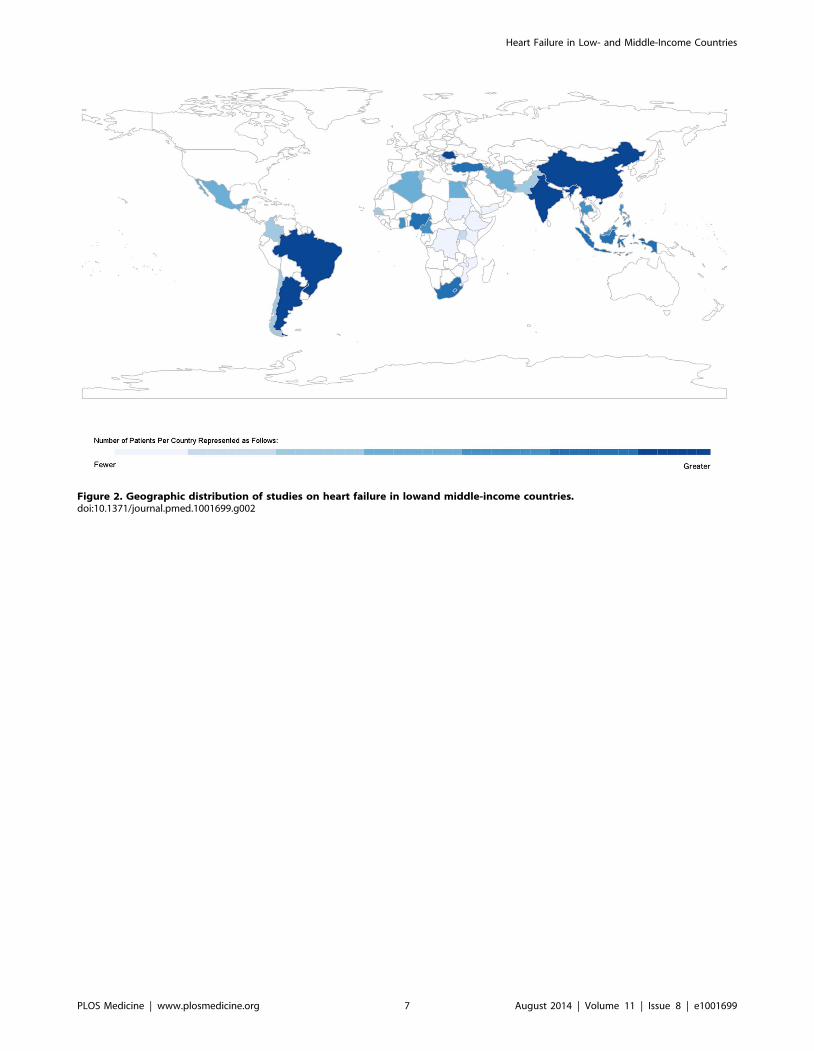
Figure 2. Geographic distribution of studies on heart failure in lowand middle-income countries.doi:10.1371/journal.pmed.1001699.g002
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 7 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 3. Male patients by region.doi:10.1371/journal.pmed.1001699.g003
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 8 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 4. Correlation of age and human development index, by country. r = 0.71, p,0.001. The HDI is a measure produced by the UnitedNations Development Programme that incorporates gross national income per capita, life expectancy, and time spent in education. It serves as asingle statistic that provides a comparable measure of development across nations. HF, heart failure.doi:10.1371/journal.pmed.1001699.g004
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 9 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 5. Aetiology of heart failure: ischaemic heart disease by region. Percentage of heart failure cases with a documented cause of IHD.doi:10.1371/journal.pmed.1001699.g005
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 10 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 6. Aetiology of heart failure: hypertension by region. Percentage of heart failure cases with a documented cause of hypertension.doi:10.1371/journal.pmed.1001699.g006
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 11 August 2014 | Volume 11 | Issue 8 | e1001699
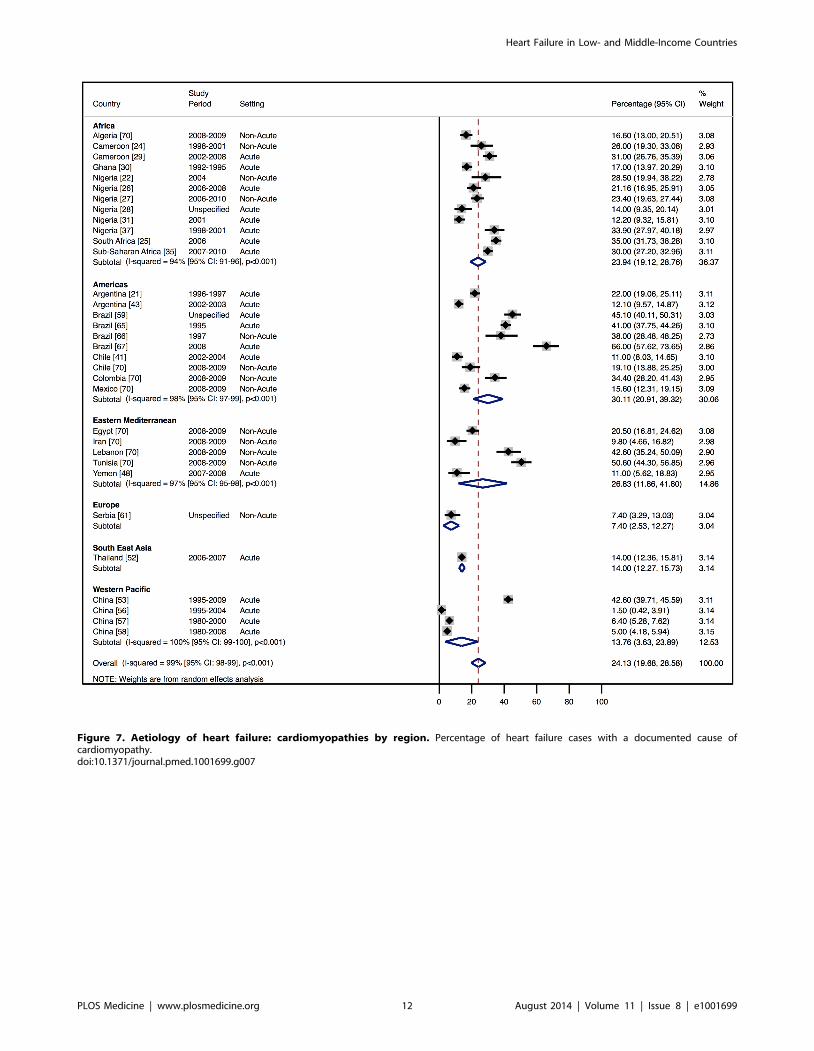
Figure 7. Aetiology of heart failure: cardiomyopathies by region. Percentage of heart failure cases with a documented cause ofcardiomyopathy.doi:10.1371/journal.pmed.1001699.g007
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 12 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 8. Aetiology of heart failure: valvular heart disease by region. Percentage of heart failure cases with a documented cause of valvularheart disease.doi:10.1371/journal.pmed.1001699.g008
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 13 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 9. Diuretic use by region. Loop and/or thiazide diuretics. ‘Rahimzadeh S, Farzadfar F, Ghaziani M (2013) Iranian hospital data project(unpublished data).doi:10.1371/journal.pmed.1001699.g009
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 14 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 10. Angiotensin-converting enzyme inhibitor use by region. ‘Rahimzadeh S, Farzadfar F, Ghaziani M (2013) Iranian hospital dataproject (unpublished data).doi:10.1371/journal.pmed.1001699.g010
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 15 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 11. Beta-blocker use by region. ‘Rahimzadeh S, Farzadfar F, Ghaziani M (2013) Iranian hospital data project (unpublished data).doi:10.1371/journal.pmed.1001699.g011
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 16 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 12. Mineralocorticoid receptor antagonist use by region. ‘Rahimzadeh S, Farzadfar F, Ghaziani M (2013) Iranian hospital data project(unpublished data).doi:10.1371/journal.pmed.1001699.g012
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 17 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 13. In-hospital mortality rates by region. ‘Rahimzadeh S, Farzadfar F, Ghaziani M (2013) Iranian hospital data project (unpublished data).doi:10.1371/journal.pmed.1001699.g013
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 18 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 14. Meta-regression of hypertension against study period.doi:10.1371/journal.pmed.1001699.g014
Figure 15. Meta-regression of ischaemic heart disease against study period.doi:10.1371/journal.pmed.1001699.g015
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 19 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 16. Meta-regression of cardiomyopathies against study period.doi:10.1371/journal.pmed.1001699.g016
Figure 17. Meta-regression of valvular heart disease against study period.doi:10.1371/journal.pmed.1001699.g017
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 20 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 18. Meta-regression of beta-blocker use against study period.doi:10.1371/journal.pmed.1001699.g018
Figure 19. Meta-regression of angiotensin-converting enzyme inhibitor use against study period.doi:10.1371/journal.pmed.1001699.g019
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 21 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 20. Meta-regression of mineralocorticoid receptor antagonist use against study period.doi:10.1371/journal.pmed.1001699.g020
Figure 21. Meta-regression of diuretic use against study period.doi:10.1371/journal.pmed.1001699.g021
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 22 August 2014 | Volume 11 | Issue 8 | e1001699
Figure 22. Meta-regression of in-hospital mortality rates against study period.doi:10.1371/journal.pmed.1001699.g022
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 23 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
1.
Ch
arac
teri
stic
so
fA
fric
are
gio
nst
ud
ies
and
dat
abas
es
incl
ud
ed
.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Alg
eri
a[7
0]‘
Pro
spe
ctiv
e2
00
8–
20
09
All
ou
tpat
ien
ts$
21
yo
fag
ew
ith
eit
he
ra
pre
vio
us
or
ne
wd
iag
no
sis
of
he
art
failu
re.
Excl
usi
on
:p
atie
nts
wit
hac
ute
de
com
pe
nsa
ted
he
art
failu
re,
or
tho
sein
ano
the
rcl
inic
tria
l.
Clin
ical
dia
gn
osi
so
nth
eb
asis
of
the
Fram
ing
ham
crit
eri
a.[7
1].
91
%o
fp
arti
cip
ants
had
ane
cho
card
iog
ram
.
40
0T
he
sed
ata
com
efr
om
the
IP
REF
ERre
gis
try.
Stre
ng
ths:
.1
0ce
ntr
es.
Site
sw
ere
ran
do
mly
sele
cte
d,
and
all
card
iolo
gis
tsw
ith
inth
eco
un
try
con
sid
ere
de
ligib
le.
Mis
sin
gd
ata
and
loss
tofo
llow
-up
tran
spar
en
t.P
rosp
ect
ive
tria
lw
ith
ina
spe
cifi
ed
recr
uit
me
nt
pe
rio
d.
.9
0%
had
con
firm
atio
no
fh
ear
tfa
ilure
thro
ug
he
cho
card
iog
rap
hy.
Lim
itat
ion
s:R
ep
rese
nta
tive
on
lyo
fth
ose
atte
nd
ing
ou
tpat
ien
tca
rdio
log
yse
rvic
es,
exc
lud
ing
the
acu
tese
cto
ro
rth
ose
pat
ien
tsin
pri
mar
yca
rew
ith
he
art
failu
ren
ot
un
de
rjo
int
care
of
aca
rdio
log
ist.
Cam
ero
on
[24
]P
rosp
ect
ive
and
retr
osp
ect
ive
ele
me
nts
19
98
–2
00
1C
on
secu
tive
pat
ien
ts$
15
yo
fag
ead
mit
ted
toth
eca
rdio
log
ycl
inic
and
/or
the
me
dic
alw
ard
so
fY
aou
nd
eG
en
era
lH
osp
ital
.T
ho
sew
ho
had
no
th
adan
ech
oca
rdio
gra
mw
ere
exc
lud
ed
.A
pro
spe
ctiv
ep
has
ew
asca
rrie
do
ut
be
twe
en
Sep
tem
be
ran
dN
ove
mb
er
20
01
,w
he
real
lp
atie
nts
wit
hsu
spe
cte
dh
ear
tfa
ilure
we
rein
clu
de
d(3
9p
atie
nts
).A
retr
osp
ect
ive
ph
ase
invo
lve
dth
eu
seo
fca
sen
ote
so
fth
ose
wit
hh
ear
tfa
ilure
adm
itte
dto
the
ho
spit
alan
du
nd
erg
oin
ge
cho
card
iog
rap
hy
be
twe
en
19
98
and
Sep
tem
be
r2
00
1(1
28
pat
ien
ts).
Clin
ical
dia
gn
osi
so
nth
eb
asis
of
the
Fram
ing
ham
crit
eri
a[7
1].
All
pat
ien
tsh
adan
ech
oca
rdio
gra
m.
16
7St
ren
gth
s:A
llp
atie
nts
had
ech
oca
rdio
gra
ph
icas
sess
me
nt.
Lim
itat
ion
s:T
his
isa
stu
dy
of
asi
ng
lere
gio
nal
tert
iary
refe
rral
cen
tre
set
ina
rura
lar
ea
that
may
no
tb
ere
pre
sen
tati
veo
fth
eb
road
er
po
pu
lati
on
.P
atie
nts
wh
oh
adn
ot
had
ane
cho
card
iog
ram
we
ree
xclu
de
d,
bu
tit
isu
ncl
ear
ho
wm
any
pat
ien
tsw
ith
acl
inic
ald
iag
no
sis
of
he
art
failu
rew
ere
thu
se
xclu
de
dan
dto
wh
ate
xte
nt
this
red
uce
sth
eg
en
era
lizab
ility
of
the
stu
dy
fin
din
gs.
Mis
sin
gd
ata
un
rep
ort
ed
.
Cam
ero
on
[29
]P
rosp
ect
ive
20
02
–2
00
8A
llco
nse
cuti
vep
atie
nts
dia
gn
ose
dw
ith
con
ge
stiv
eca
rdia
cfa
ilure
refe
rre
dto
the
card
iac
cen
tre
of
St.
Eliz
abe
thC
ath
olic
Ge
ne
ral
Ho
spit
al,
Shis
on
g,
Cam
ero
on
.
Clin
ical
dia
gn
osi
so
nth
eb
asis
of
the
Fram
ing
ham
crit
eri
a.Ec
ho
card
iog
rap
hy
use
d,
bu
tn
oin
dic
atio
nif
all
pat
ien
tsu
nd
erw
en
tth
isin
vest
igat
ion
.
46
2St
ren
gth
s:C
om
pre
he
nsi
vep
rosp
ect
ive
stu
dy
en
com
pas
sin
gal
lp
atie
nts
dia
gn
ose
dw
ith
inth
est
ud
yp
eri
od
.Lo
ssto
follo
w-u
pd
ocu
me
nte
d.
Lim
itat
ion
s:T
his
isa
stu
dy
of
asi
ng
lere
gio
nal
card
iolo
gy
refe
rral
cen
tre
that
may
no
tb
ere
pre
sen
tati
veo
fth
eb
road
er
po
pu
lati
on
.M
issi
ng
dat
an
ot
tran
spar
en
tly
acco
un
ted
for.
De
mo
crat
icR
ep
ub
lico
fth
eC
on
go
[32
]
Pro
spe
ctiv
e2
00
3–
20
04
Eve
ryfo
urt
hp
atie
nt
adm
itte
dw
ith
he
art
failu
reas
anin
pat
ien
th
avin
gb
ee
nse
en
atth
eca
rdio
log
ycl
inic
of
the
Lom
oM
ed
ical
Ce
ntr
eo
fth
eH
ear
to
fA
fric
aC
ard
iova
scu
lar
Ce
ntr
ein
Kin
shas
a.
Ech
oca
rdio
gra
ph
y.1
00
Stre
ng
ths:
All
pat
ien
tsh
ade
cho
card
iog
rap
hic
asse
ssm
en
t.Li
mit
atio
ns:
Th
isis
ast
ud
yo
fa
sin
gle
urb
ano
utp
atie
nt
card
iolo
gy
refe
rral
cen
tre
that
may
no
tb
ere
pre
sen
tati
veo
fth
eb
road
er
po
pu
lati
on
.M
issi
ng
dat
an
ot
tran
spar
en
tly
acco
un
ted
for.
Gh
ana
[30
]P
rosp
ect
ive
19
92
–1
99
5C
on
secu
tive
pat
ien
tsw
ith
he
art
failu
rere
ferr
ed
toth
eN
atio
nal
Car
dio
tho
raci
cC
en
tre
,A
ccra
,o
ver
4y.
Fram
ing
ham
crit
eri
a.A
llp
atie
nts
had
ane
cho
card
iog
ram
pe
rfo
rme
d.
57
2St
ren
gth
s:T
his
cen
tre
rece
ive
sre
ferr
als
fro
mal
lh
osp
ital
sac
ross
the
cou
ntr
y,in
cre
asin
gth
eg
en
era
lizab
ility
of
the
resu
lts.
All
pat
ien
tsh
ade
cho
card
iog
rap
hy.
Lim
itat
ion
s:A
ckn
ow
led
ge
dp
ote
nti
alfo
rre
ferr
alb
ias
asp
atie
nts
atth
issi
ng
leu
rban
tert
iary
spe
cial
ist
cen
tre
may
no
tb
ere
pre
sen
tati
veo
fh
ear
tfa
ilure
man
age
me
nt
els
ew
he
re.
Un
cle
arif
the
rew
ere
mis
sin
gd
ata,
and
ho
wth
ey
we
reac
cou
nte
dfo
r.
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 24 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
1.
Co
nt.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Nig
eri
a[3
6]
Re
tro
spe
ctiv
e1
99
5–
20
05
Th
eca
sen
ote
so
f2
02
pat
ien
tsw
ith
he
art
failu
rew
ere
ran
do
mly
sele
cte
dfr
om
the
ou
tpat
ien
tan
din
pat
ien
td
ep
artm
en
tso
fU
niv
ers
ity
Co
lleg
eH
osp
ital
,Ib
adan
.
Ne
wY
ork
He
art
Ass
oci
atio
ncl
assi
fica
tio
n.
20
2Li
mit
atio
ns:
Re
tro
spe
ctiv
est
ud
yw
ith
un
cert
ain
dia
gn
ost
icac
cura
cy.
Inp
atie
nt
and
ou
tpat
ien
tm
anag
em
en
tw
ere
no
tse
par
ate
d.
Th
isis
ast
ud
yo
fa
sin
gle
urb
ante
rtia
ryre
ferr
alce
ntr
eth
atm
ayn
ot
be
rep
rese
nta
tive
of
the
bro
ade
rp
op
ula
tio
n.
Mis
sin
gd
ata
no
ttr
ansp
are
ntl
yac
cou
nte
dfo
r.
Nig
eri
a[3
4]
Re
tro
spe
ctiv
e1
99
6–
20
05
All
pat
ien
tsre
cord
ed
ash
avin
ga
dia
gn
osi
so
fh
ear
tfa
ilure
fro
mth
em
ort
alit
yre
cord
so
fth
eU
niv
ers
ity
of
Ilori
nT
eac
hin
gH
osp
ital
No
tsp
eci
fie
d.
22
8St
ren
gth
s:C
om
pre
he
nsi
vere
vie
wo
fal
ld
eat
hs
and
the
irre
spe
ctiv
eca
sen
ote
sfr
om
the
ho
spit
al,
limit
ing
sele
ctio
nb
ias.
Lim
itat
ion
s:U
nce
rtai
nd
iag
no
stic
accu
racy
.T
his
isa
sin
gle
urb
ante
ach
ing
ho
spit
alp
rovi
din
gse
rvic
es
ton
ort
h-c
en
tral
Nig
eri
a.A
lth
ou
gh
the
ho
spit
alco
vers
ala
rge
catc
hm
en
tar
ea,
the
pat
ien
tsm
ayn
on
eth
ele
ssn
ot
be
rep
rese
nta
tive
of
the
bro
ade
rp
op
ula
tio
n.
Nig
eri
a[3
3]
Pro
spe
ctiv
e1
99
7–
20
01
Re
cord
so
fal
lp
atie
nts
adm
itte
dw
ith
card
iova
scu
lar
dis
eas
eto
the
Ob
afe
mi
Aw
olo
wo
Un
ive
rsit
yT
eac
hin
gH
osp
ital
sC
om
ple
xin
Ife
,N
ige
ria.
No
tsp
eci
fie
d.
38
6St
ren
gth
s:Si
ng
lete
rtia
ryre
ferr
alce
ntr
ep
rovi
din
gse
rvic
es
to1
0m
illio
nin
div
idu
als
inth
eso
uth
we
sto
fN
ige
ria,
incr
eas
ing
the
stu
dy’
sg
en
era
lizab
ility
.Li
mit
atio
ns:
Sin
gle
cen
tre
,th
ou
gh
wit
ha
larg
eca
tch
me
nt
are
a,m
ayn
ot
be
rep
rese
nta
tive
of
the
bro
ade
rp
op
ula
tio
n.
No
stan
dar
dis
ed
dia
gn
ost
iccr
ite
ria
use
d.
Nig
eri
a[3
7]
Re
tro
spe
ctiv
e1
99
8–
20
01
All
pat
ien
tsad
mit
ted
toth
em
ed
ical
war
ds
of
the
Un
ive
rsit
yo
fU
yoT
eac
hin
gH
osp
ital
inso
uth
ern
Nig
eri
aw
ith
he
art
failu
red
uri
ng
the
dry
seas
on
sw
ith
inth
est
ud
yp
eri
od
.Ex
clu
sio
n:
Pat
ien
tsw
ith
ren
ald
ise
ase
or
susp
ect
ed
coro
nar
yar
tery
dis
eas
e.
Clin
ical
feat
ure
sw
ith
the
aid
of
blo
od
resu
lts,
che
stra
dio
gra
ph
y,e
lect
roca
rdio
gra
ph
y,an
de
cho
card
iog
rap
hy.
Th
ep
rop
ort
ion
rece
ivin
gad
dit
ion
alin
vest
igat
ion
sis
un
kno
wn
.
24
5St
ren
gth
s:C
om
pre
he
nsi
veas
sess
me
nt
of
pat
ien
tsw
ith
he
art
failu
reas
cod
ed
for
by
this
ho
spit
al.
Lim
itat
ion
s:Si
ng
lete
rtia
ryre
ferr
alce
ntr
em
ayn
ot
be
rep
rese
nta
tive
of
the
bro
ade
rp
op
ula
tio
n.S
tud
yw
asa
retr
osp
ect
ive
stu
dy
of
case
no
tes;
con
seq
ue
ntl
y,d
iag
no
stic
accu
racy
isu
nce
rtai
n.
Pro
po
rtio
ns
rece
ivin
gad
dit
ion
alg
old
-sta
nd
ard
inve
stig
atio
ns,
such
ase
cho
card
iog
rap
hy,
no
td
ocu
me
nte
d.
Nig
eri
a[3
1]
Re
tro
spe
ctiv
e2
00
1–
20
05
All
adu
lts
$1
8y
wit
hco
ng
est
ive
card
iac
failu
read
mit
ted
toth
em
ed
ical
war
ds
of
the
Un
ive
rsit
yo
fP
ort
Har
cou
rtT
eac
hin
gH
osp
ital
.Ex
clu
sio
n:
pat
ien
tsw
ho
seco
nd
itio
nd
idn
ot
me
et
the
Fram
ing
ham
crit
eri
ao
rw
ho
die
dw
ith
in2
4h
of
adm
issi
on
.
Fram
ing
ham
crit
eri
a.4
23
Stre
ng
ths:
Cle
ard
iag
no
stic
crit
eri
a.C
om
pre
he
nsi
veas
sess
me
nt
of
pat
ien
tsw
ith
he
art
failu
re.
Lim
itat
ion
s:Si
ng
lete
rtia
ryre
ferr
alce
ntr
em
ayn
ot
be
rep
rese
nta
tive
of
the
bro
ade
rp
op
ula
tio
n.
Re
tro
spe
ctiv
eas
sess
me
nt
wit
hu
nce
rtai
nac
cura
cyo
fth
eae
tio
log
yo
fh
ear
tfa
ilure
.U
ncl
ear
wh
atp
rop
ort
ion
rece
ive
dad
dit
ion
alin
vest
igat
ion
ssu
chas
ech
oca
rdio
gra
ph
y.U
ncl
ear
ho
wm
issi
ng
dat
aw
ere
acco
un
ted
for.
Nig
eri
a[2
2]
Pro
spe
ctiv
eM
ay–
Jun
e2
00
4C
on
secu
tive
pat
ien
ts$
18
yw
ith
susp
ect
ed
he
art
failu
rep
rese
nti
ng
too
utp
atie
nt
de
par
tme
nt,
war
ds,
or
the
casu
alty
un
ito
fJo
sU
niv
ers
ity
Te
ach
ing
Ho
spit
al.
Fram
ing
ham
crit
eri
a.1
02
Stre
ng
ths:
Co
nse
cuti
vep
atie
nts
incl
ud
ed
,lim
itin
gp
ote
nti
alfo
rse
lect
ion
bia
s.C
lear
do
cum
en
tati
on
of
rati
on
ale
be
hin
dsa
mp
lesi
ze.
Stan
dar
dis
ed
dia
gn
osi
scr
ite
ria
use
d.
Ack
no
wle
dg
ed
limit
atio
ns.
Lim
itat
ion
s:Si
ng
lete
rtia
ryre
ferr
alce
ntr
em
ayn
ot
be
rep
rese
nta
tive
of
the
bro
ade
rp
op
ula
tio
n.
Inp
atie
nt
and
ou
tpat
ien
tsa
mp
len
ot
sep
arat
ed
.A
eti
olo
gy
of
he
art
failu
reas
cert
ain
ed
by
case
no
tes
and
clin
ical
fin
din
gs
on
exa
min
atio
nra
the
rth
ang
old
-sta
nd
ard
inve
stig
atio
n.
Ech
oca
rdio
gra
ph
yn
ot
avai
lab
leto
all
pat
ien
ts.
Nig
eri
a[2
6]
Pro
spe
ctiv
e2
00
6–
20
08
Co
nse
cuti
vep
atie
nts
$1
5y
wit
hh
ear
tfa
ilure
pre
sen
tin
gto
the
Un
ive
rsit
yo
fA
bu
jaT
eac
hin
gH
osp
ital
.
Euro
pe
anSo
cie
tyo
fC
ard
iolo
gy
gu
ide
line
s.Ec
ho
card
iog
rap
hy
avai
lab
lefo
ral
lp
atie
nts
.
34
0St
ren
gth
s:La
rge
catc
hm
en
tar
ea
for
this
refe
rral
cen
tre
,im
pro
vin
gg
en
era
lizab
ility
.A
llp
atie
nts
had
ech
oca
rdio
gra
ph
icas
sess
me
nt,
imp
rovi
ng
ove
rall
dia
gn
ost
icac
cura
cyan
dth
ato
fas
sig
ne
du
nd
erl
yin
gae
tio
log
ies
of
he
art
failu
re.
Lim
itat
ion
s:Si
ng
lete
rtia
ryre
ferr
alce
ntr
em
ayre
fle
ctm
ore
seve
reca
ses
or
tho
seo
fu
nce
rtai
nd
iag
no
sis,
the
refo
ren
ot
refl
ect
ing
pra
ctic
ein
the
bro
ade
rh
eal
thse
rvic
e.
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 25 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
1.
Co
nt.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Nig
eri
a[2
7]
Pro
spe
ctiv
e2
00
6–
20
10
Clin
ical
reg
istr
yo
fco
nse
cuti
vein
div
idu
als
refe
rre
dfo
rth
efi
rst
tim
eto
the
card
iolo
gy
clin
ico
fth
eU
niv
ers
ity
of
Ab
uja
Te
ach
ing
Ho
spit
al.
Excl
usi
on
:th
ose
wit
hm
usc
ulo
ske
leta
lch
est
pai
no
rh
ep
atic
or
ren
alfa
ilure
.
Euro
pe
anSo
cie
tyo
fC
ard
iolo
gy
gu
ide
line
s.Ec
ho
card
iog
rap
hy
avai
lab
lefr
om
.9
5%
of
pat
ien
ts.
47
5St
ren
gth
s:C
on
secu
tive
pat
ien
ts,
red
uci
ng
the
risk
of
sele
ctio
nb
ias.
Cle
ar,s
tan
dar
dis
ed
,dia
gn
ost
iccr
ite
ria.
Do
cum
en
ted
use
of
the
STR
OB
Eg
uid
elin
es
[16
]fo
rth
ere
po
rtin
go
fo
bse
rvat
ion
alst
ud
ies.
Lim
itat
ion
s:Si
ng
lete
rtia
ryre
ferr
alce
ntr
em
ayre
fle
ctm
ore
seve
reca
ses
or
tho
seo
fu
nce
rtai
nd
iag
no
sis,
the
refo
ren
ot
refl
ect
ing
pra
ctic
ein
the
bro
ade
rh
eal
thse
rvic
e.
Nig
eri
a[2
8]
Pro
spe
ctiv
eU
nkn
ow
n(p
ub
lish
ed
20
09
)
17
7co
nse
cuti
vein
div
idu
als
wit
hh
ear
tfa
ilure
pre
sen
tin
gto
the
Un
ive
rsit
yC
olle
ge
Ho
spit
al,
Ibad
an.
Fram
ing
ham
crit
eri
a.A
llp
atie
nts
un
de
rwe
nt
ane
cho
card
iog
ram
.
17
7St
ren
gth
s:C
lear
,st
and
ard
ise
d,
dia
gn
ost
iccr
ite
ria.
All
pat
ien
tsh
adan
ech
oca
rdio
gra
m,i
mp
rovi
ng
the
accu
racy
of
he
art
failu
red
iag
no
sis
and
that
of
un
de
rlyi
ng
aeti
olo
gy.
Cat
chm
en
tar
ea
of
gre
ate
rth
an3
mill
ion
ind
ivid
ual
s,im
pro
vin
gth
eg
en
era
lizab
ility
of
the
resu
lts.
Cle
are
xpla
nat
ion
of
stat
isti
cal
me
tho
ds
use
d.
Lim
itat
ion
s:Si
ng
lete
rtia
ryre
ferr
alce
ntr
em
ayre
fle
ctm
ore
seve
reca
ses
or
tho
seo
fu
nce
rtai
nd
iag
no
sis,
the
refo
ren
ot
refl
ect
ing
pra
ctic
ein
the
bro
ade
rh
eal
thse
rvic
e.
Sen
eg
al[3
8]
Pro
spe
ctiv
eJa
nu
ary–
Jun
e2
00
1Se
lect
ion
crit
eri
an
ot
spe
cifi
ed
.U
rban
ho
spit
alin
Dak
ar.
Clin
ical
dia
gn
osi
s.A
llp
atie
nts
un
de
rwe
nt
ech
oca
rdio
gra
ph
y.
17
0St
ren
gth
s:A
llp
atie
nts
un
de
rwe
nt
ech
oca
rdio
gra
ph
y,im
pro
vin
gth
elik
ely
accu
racy
of
the
dia
gn
osi
so
fh
ear
tfa
ilure
and
of
assi
gn
ed
aeti
olo
gy.
Lim
itat
ion
s:Si
ng
leu
rban
ho
spit
alin
the
cap
ital
may
no
tre
fle
ctb
road
er
po
pu
lati
on
wit
hh
ear
tfa
ilure
.U
ncl
ear
sele
ctio
ncr
ite
ria.
Sou
thA
fric
a[2
5]
Pro
spe
ctiv
e2
00
6A
llp
atie
nts
wit
hca
rdio
vasc
ula
rd
ise
ase
or
pre
sen
tin
gto
the
card
iolo
gy
un
it.
Th
ose
wit
ha
de
no
vop
rese
nta
tio
nw
ith
he
art
failu
rew
ere
incl
ud
ed
.Ex
clu
sio
n:
tho
sew
ith
acu
teis
chae
mic
aeti
olo
gy.
Bas
ed
on
Euro
pe
anSo
cie
tyo
fC
ard
iolo
gy
gu
ide
line
s.A
llp
atie
nts
had
ane
cho
card
iog
ram
.
84
4St
ren
gth
s:So
leca
rdio
vasc
ula
rce
ntr
efo
ra
po
pu
lati
on
of
1.1
mill
ion
ind
ivid
ual
s,in
cre
asin
gth
eg
en
era
lizab
ility
of
fin
din
gs.
All
pat
ien
tsu
nd
erw
en
te
cho
card
iog
rap
hic
asse
ssm
en
t,im
pro
vin
glik
ely
accu
racy
of
dia
gn
osi
san
do
fu
nd
erl
yin
gae
tio
log
yo
fe
ach
pat
ien
t’s
he
art
failu
re.
Cle
ard
ocu
me
nta
tio
no
fd
ata
avai
lab
ility
and
crit
eri
aap
plie
d.
Lim
itat
ion
s:Ex
clu
sio
no
fth
ose
wit
han
isch
aem
icae
tio
log
ym
ayu
nd
ere
stim
ate
the
pro
po
rtio
no
fth
ose
wit
hh
ear
tfa
ilure
du
eto
IHD
.U
rban
ho
spit
alse
ttin
gm
ayn
ot
refl
ect
the
bro
ade
rp
op
ula
tio
n.
Sub
-Sah
aran
Afr
ica
[35
]P
rosp
ect
ive
20
07
–2
01
0P
atie
nts
$1
2y
wit
hac
ute
he
art
failu
reco
nfi
rme
db
ye
cho
card
iog
rap
hy
we
rein
clu
de
d.
Th
est
ud
yw
asco
nd
uct
ed
inth
efo
llow
ing
cou
ntr
ies:
Sud
an,
Eth
iop
ia,
Ke
nya
,U
gan
da,
Mo
zam
biq
ue
,So
uth
Afr
ica,
Cam
ero
on
,N
ige
ria,
Sen
eg
al.
Excl
usi
on
:th
ose
wit
hac
ute
ST-
ele
vati
on
myo
card
ial
infa
rcti
on
,kn
ow
nse
vere
ren
alfa
ilure
,h
ep
atic
failu
re,
or
ano
the
rca
use
of
hyp
oal
bu
min
em
ia.
Un
spe
cifi
ed
sig
ns
and
sym
pto
ms
of
he
art
failu
re.
All
pat
ien
tsh
adan
ech
oca
rdio
gra
m.
1,0
06
Stre
ng
ths:
All
pat
ien
tsh
ade
cho
card
iog
rap
hic
asse
ssm
en
t,im
pro
vin
gd
iag
no
stic
accu
racy
.C
lear
do
cum
en
tati
on
of
mis
sin
gd
ata
and
loss
tofo
llow
-up
asw
ell
ash
ow
this
was
acco
un
ted
for
inan
alys
es.
Firs
tp
ub
lish
ed
dat
ao
nh
ear
tfa
ilure
fro
ma
nu
mb
er
of
Afr
ican
cou
ntr
ies.
Lim
itat
ion
s:U
rban
sin
gle
ho
spit
alce
ntr
es
incl
ud
ed
.In
div
idu
alst
ud
ysi
tes
oft
en
had
very
few
pat
ien
tse
nro
lled
(ran
ge
fro
m1
0to
20
0).
Excl
usi
on
crit
eri
am
ayle
adto
the
un
de
rest
imat
ion
of
IHD
asa
cau
seo
fh
ear
tfa
ilure
.
‘P
revi
ou
sly
un
pu
blis
he
dd
ata.
do
i:10
.13
71
/jo
urn
al.p
me
d.1
00
16
99
.t0
01
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 26 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
2.
Ch
arac
teri
stic
so
fA
me
rica
sre
gio
nst
ud
ies
and
dat
abas
es
incl
ud
ed
.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Arg
en
tin
a[2
3]
Re
tro
spe
ctiv
e1
99
2–
19
99
All
pat
ien
tsd
iag
no
sed
wit
hco
ng
est
ive
he
art
failu
re,
de
com
pe
nsa
ted
he
art
failu
re,
or
acu
tep
ulm
on
ary
oe
de
ma
asre
cord
ed
inth
ee
lect
ron
icvi
tal
stat
isti
cso
fa
com
mu
nit
yh
osp
ital
of
Mar
de
lP
lata
,A
rge
nti
na.
No
tsp
eci
fie
d.
6,3
68
Stre
ng
ths:
Co
mp
reh
en
sive
stu
dy
wit
hlim
ite
dse
lect
ion
bia
s.Li
mit
atio
ns:
Sin
gle
com
mu
nit
yh
osp
ital
that
may
no
tb
ere
fle
ctiv
eo
fb
road
er
pat
tern
so
fh
ear
tfa
ilure
pre
vale
nce
.N
ost
and
ard
ise
dm
eth
od
for
dia
gn
osi
ng
he
art
failu
re,
rely
ing
on
dis
char
ge
rep
ort
s.
Arg
en
tin
a[2
1]
Pro
spe
ctiv
e1
99
6–
19
97
Pat
ien
tsad
mit
ted
tob
oth
the
ge
ne
ral
me
dic
alan
dca
rdio
log
yw
ard
sw
ith
de
com
pe
nsa
ted
chro
nic
he
art
failu
re.
Pat
ien
tsm
ust
hav
eh
adh
ear
tfa
ilure
,as
dia
gn
ose
db
yth
eFr
amin
gh
amcl
inic
alcr
ite
ria,
for
30
do
rm
ore
.Ex
clu
sio
n:
acu
teh
ear
tfa
ilure
du
eto
anis
chae
mic
eve
nt,
tho
selo
stto
follo
w-u
p,
and
tho
sew
ith
ou
tan
ele
ctro
card
iog
ram
and
che
stra
dio
gra
ph
.
Fram
ing
ham
crit
eri
a.U
nsp
eci
fie
dp
rop
ort
ion
rece
ive
de
cho
card
iog
rap
hy.
75
1St
ren
gth
s:3
1ce
ntr
es
fro
mac
ross
Arg
en
tin
a,4
2%
of
wh
ich
we
rein
Bu
en
os
Air
es.
Stan
dar
dis
ed
dia
gn
ost
iccr
ite
ria.
Cle
arst
atis
tica
lme
tho
ds
do
cum
en
ted
.Li
mit
atio
ns:
Ce
ntr
es
we
rein
vite
dto
take
par
tra
the
rth
anra
nd
om
ise
d.
Un
cert
ain
pro
po
rtio
nre
ceiv
ed
ech
oca
rdio
gra
ph
icco
nfi
rmat
ion
.Ex
clu
sio
ncr
ite
ria
may
lead
tou
nd
ere
stim
atio
no
fIH
Das
anae
tio
log
yo
fh
ear
tfa
ilure
.
Arg
en
tin
a[4
3]
Pro
spe
ctiv
e2
00
2–
20
03
All
pat
ien
ts.
18
yh
osp
ital
ise
dfo
rd
eco
mp
en
sate
dch
ron
ich
ear
tfa
ilure
.Ex
clu
sio
n:
he
art
failu
rese
con
dar
yto
am
yoca
rdia
lin
farc
tio
no
rp
ost
-op
era
tive
ly.
Inve
stig
ato
r’s
dis
cre
tio
n.
61
5St
ren
gth
s:3
6ce
ntr
es
pre
do
min
antl
yb
ase
dar
ou
nd
Bu
en
os
Air
es
or
ne
igh
bo
uri
ng
reg
ion
s.C
om
pre
he
nsi
veas
sess
me
nt
of
all
pat
ien
tsw
ith
like
lylo
wse
lect
ion
bia
s.Li
mit
atio
ns:
Ce
ntr
es
we
ren
ot
ran
do
mis
ed
,ra
the
rin
vite
d.
Co
nse
qu
en
tly,
resu
lts
may
no
tre
fle
ctth
eb
road
er
man
age
me
nt
of
he
art
failu
ream
on
gst
ph
ysic
ian
sw
ith
less
of
anin
tere
stin
he
art
failu
re.
No
stan
dar
dd
iag
no
stic
crit
eri
a.Ex
clu
sio
ncr
ite
ria
may
lead
tou
nd
ere
stim
atio
no
fIH
Das
anae
tio
log
yo
fh
ear
tfa
ilure
.U
nce
rtai
nad
just
me
nt
for
tho
sew
ith
mis
sin
gd
ata.
Arg
en
tin
a[4
4]
Pro
spe
ctiv
e2
00
7A
llp
atie
nts
.1
8y
of
age
we
rein
clu
de
dif
ho
spit
alis
ed
for
de
com
pe
nsa
ted
chro
nic
he
art
failu
re.
Excl
usi
on
:h
ear
tfa
ilure
asa
com
plic
atio
no
fa
myo
card
ial
infa
rcti
on
or
po
st-o
pe
rati
vely
.
Inve
stig
ato
r’s
dis
cre
tio
n.
73
6St
ren
gth
s:3
6ce
ntr
es
fro
mac
ross
Arg
en
tin
a.Li
mit
atio
ns:
Ce
ntr
es
invi
ted
tota
kep
art
rath
er
than
ran
do
mis
ed
,an
dth
ose
that
did
may
refl
ect
clin
icia
ns
wit
han
inte
rest
inh
ear
tfa
ilure
,af
fect
ing
the
bro
ade
rg
en
era
lizab
ility
of
resu
lts.
Excl
usi
on
crit
eri
am
ayle
adto
un
de
rest
imat
ion
of
IHD
asan
aeti
olo
gy
of
he
art
failu
re.
No
stan
dar
dd
iag
no
stic
crit
eri
a.U
nce
rtai
nad
just
me
nt
for
tho
sew
ith
mis
sin
gd
ata
or
lost
tofo
llow
-up
.N
ost
and
ard
dia
gn
ost
iccr
ite
ria
for
he
art
failu
re.
Bra
zil
[45
]R
etr
osp
ect
ive
19
92
to2
01
0P
atie
nts
adm
itte
dto
pu
blic
ho
spit
als
inSa
oP
aulo
wit
hh
ear
tfa
ilure
.N
ot
spe
cifi
ed
.1
94
,09
8St
ren
gth
s:Fr
om
the
Dat
asu
sre
gis
try,
pro
vid
ing
ho
spit
ale
pis
od
est
atis
tics
for
the
en
tire
pu
blic
he
alth
syst
em
of
Sao
Pau
lo.
Lim
itat
ion
s:U
nce
rtai
nd
iag
no
stic
crit
eri
ab
ase
do
nin
div
idu
alp
hys
icia
n’s
dis
cre
tio
n.
Bra
zil
[42
]P
rosp
ect
ive
19
98
–2
00
0C
on
secu
tive
pat
ien
tsad
mit
ted
toh
osp
ital
wit
hw
ors
en
ing
sym
pto
ms
of
he
art
failu
re(N
YH
Afu
nct
ion
alcl
asse
sIII
or
IV).
Excl
usi
on
:p
atie
nts
wit
hh
ear
tfa
ilure
du
eto
valv
ula
rh
ear
td
ise
ase
s,th
yro
toxi
cosi
s,h
ypo
thyr
oid
ism
,se
vere
anae
mia
,am
ylo
ido
sis,
ne
op
lasi
a,ch
ron
icn
on
-car
dio
ge
nic
pu
lmo
nar
yd
ise
ase
s,p
revi
ou
sh
ear
ttr
ansp
lan
tati
on
,ch
ron
ich
aem
od
ialy
sis,
or
par
tici
pat
ion
ind
rug
pro
toco
ls.
Clin
ical
dia
gn
osi
sb
ase
do
nth
eFr
amin
gh
amcr
ite
ria.
49
4St
ren
gth
s:St
and
ard
ise
dd
iag
no
stic
crit
eri
a.Li
mit
atio
ns:
Un
ive
rsit
yT
eac
hin
gH
osp
ital
inSa
oP
aulo
de
dic
ate
dto
card
iolo
gy.
Excl
usi
on
crit
eri
am
ayfu
rth
er
hin
de
rg
en
era
lizab
ility
.O
nly
pat
ien
tsw
ith
NY
HA
fun
ctio
nal
clas
sIII
or
IV,
som
ayn
ot
be
ge
ne
raliz
able
toth
ose
wit
hm
ilde
rsy
mp
tom
s.T
he
exc
lusi
on
of
pat
ien
tsw
ith
valv
ula
rh
ear
td
ise
ase
may
imp
act
on
the
assi
gn
me
nt
of
aeti
olo
gie
so
fh
ear
tfa
ilure
.U
ncl
ear
ho
wlo
ssto
follo
wu
pan
dm
issi
ng
dat
aw
ere
acco
un
ted
for.
Bra
zil
[40
]P
rosp
ect
ive
20
01
98
con
secu
tive
pat
ien
tsad
mit
ted
top
arti
cip
atin
gp
ub
lich
osp
ital
san
d1
05
con
secu
tive
pat
ien
tsad
mit
ted
top
arti
cip
atin
gp
riva
teh
osp
ital
sw
ith
inth
e3
-mo
stu
dy
pe
rio
din
the
city
of
Nit
ero
iw
ith
aB
ost
on
crit
eri
asc
ore
of
8o
rm
ore
.
Bo
sto
ncr
ite
ria
sco
re$
8.
20
3St
ren
gth
s:M
ult
iple
ho
spit
als
wit
hin
Nit
ero
i,im
pro
vin
gg
en
era
lizab
ility
.C
lear
stat
isti
cal
me
tho
ds
rep
ort
ed
.Ju
stu
nd
er
hal
fo
fp
atie
nts
we
refr
om
the
pri
vate
sect
or,
the
rem
ain
ing
fro
mth
ep
ub
licse
cto
r,al
low
ing
dir
ect
com
par
iso
nb
etw
ee
nth
ese
two
gro
up
san
dre
pre
sen
tati
on
fro
ma
bro
ade
rsw
ath
eo
fso
cie
ty.
Lim
itat
ion
s:T
he
me
tho
ds
use
dto
sele
ctth
ep
arti
cip
atin
gh
osp
ital
sar
eu
ncl
ear
,as
isth
efi
nal
nu
mb
er
of
site
sin
clu
de
d.
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 27 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
2.
Co
nt.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Bra
zil
[19
]P
rosp
ect
ive
20
05
–2
00
6C
on
secu
tive
pat
ien
tsad
mit
ted
wit
hh
ear
tfa
ilure
and
syst
olic
dys
fun
ctio
n.
Clin
ical
dia
gn
osi
sw
ith
ech
oca
rdio
-g
rap
hic
con
firm
atio
n.
26
3Li
mit
atio
ns:
Sin
gle
urb
ance
ntr
eth
atm
ayn
ot
be
rep
rese
nta
tive
of
the
pat
tern
so
fca
reat
the
nat
ion
alle
vel.
Un
cle
arh
ow
mis
sin
gd
ata
and
loss
tofo
llow
-up
we
reac
cou
nte
dfo
r.U
nce
rtai
nd
iag
no
stic
crit
eri
ao
rp
rop
ort
ion
rece
ivin
ge
cho
card
iog
rap
hy.
On
lyp
atie
nts
wit
hsy
sto
licd
ysfu
nct
ion
we
rein
clu
de
d,
po
ssib
lyre
du
cin
gth
eg
en
era
lizab
ility
of
resu
lts.
Bra
zil
[39
]P
rosp
ect
ive
20
06
–2
00
8C
on
secu
tive
pat
ien
ts$
18
yre
ferr
ed
toh
ear
tfa
ilure
clin
icw
ith
aB
ost
on
sco
reo
f$
7.
Ind
ivid
ual
sw
ere
all
clas
sed
asliv
ing
inru
ral
are
asas
pe
rth
eB
razi
lian
Inst
itu
teo
fG
eo
gra
ph
yan
dSt
atis
tics
.
Bo
sto
ncr
ite
ria
sco
re$
7.
All
pat
ien
tsu
nd
erw
en
te
cho
card
iog
rap
hy.
16
6St
ren
gth
s:A
llp
atie
nts
had
ech
oca
rdio
gra
ph
icas
sess
me
nt.
Stan
dar
dd
iag
no
stic
crit
eri
a.Li
mit
atio
ns:
Sin
gle
cen
tre
stu
dy
that
may
no
tb
ere
pre
sen
tati
veo
fth
ep
atte
rns
of
care
atth
en
atio
nal
leve
l.
Bra
zil
[46
]P
rosp
ect
ive
Un
kno
wn
(pu
blis
he
d2
00
8)
Pat
ien
tsco
nse
cuti
vely
adm
itte
dto
the
em
erg
en
cyd
ep
artm
en
to
fth
eIn
stit
uto
do
Co
raca
od
oH
osp
ital
das
Clın
icas
da
Facu
ldad
ed
eM
ed
icin
ad
aU
niv
ers
idad
ed
eSa
oP
aulo
ove
ra
pe
rio
do
f1
50
dw
ith
the
dia
gn
osi
so
fd
eco
mp
en
sate
dh
ear
tfa
ilure
.1
00
ou
to
fth
e2
12
pat
ien
tsin
itia
llyas
sess
ed
we
rere
tro
spe
ctiv
ely
sele
cte
d,
for
wh
om
furt
he
rd
eta
ilsw
ere
colle
cte
d.
No
tsp
eci
fie
d.
10
0St
ren
gth
s:A
lth
ou
gh
the
rew
ere
no
stan
dar
dd
iag
no
stic
crit
eri
afo
rh
ear
tfa
ilure
itse
lf,t
he
rew
ere
stan
dar
dcr
ite
ria
for
assi
gn
ing
aeti
olo
gie
so
fh
ear
tfa
ilure
.Li
mit
atio
ns:
Sin
gle
urb
ante
rtia
ryre
ferr
alce
ntr
eth
atm
ayn
ot
be
rep
rese
nta
tive
of
the
pat
tern
so
fca
reat
the
nat
ion
alle
vel.
No
stan
dar
dd
iag
no
stic
crit
eri
au
sed
.M
eth
od
of
sele
ctio
no
fth
e1
00
pat
ien
tsfo
rw
ho
mm
ore
de
taile
dan
alys
isw
asp
erf
orm
ed
un
cle
ar.
Bra
zil
[59
]P
rosp
ect
ive
16
un
spe
cifi
ed
mo
nth
s(p
ub
lish
ed
20
12
).
Te
rtia
ryce
ntr
ein
Salv
ado
r,B
ahia
,B
razi
l.C
on
secu
tive
pat
ien
tsw
ith
ad
iag
no
sis
of
he
art
failu
rew
ho
had
had
ech
oca
rdio
gra
ph
y.
Ech
oca
rdio
gra
ph
y.3
83
Stre
ng
ths:
All
pat
ien
tsh
ade
cho
card
iog
rap
hic
asse
ssm
en
t.St
and
ard
crit
eri
afo
rth
eas
sig
nm
en
to
fae
tio
log
ies.
Lim
itat
ion
s:Si
ng
leu
rban
tert
iary
refe
rral
cen
tre
that
may
no
tb
ere
pre
sen
tati
veo
fth
ep
atte
rns
of
care
atth
en
atio
nal
leve
l.O
nly
tho
sep
atie
nts
wh
oh
adal
read
yh
ade
cho
card
iog
rap
hy
we
rein
clu
de
d.
End
em
iczo
ne
for
Ch
agas
dis
eas
e,
wh
ich
may
hin
de
rth
eg
en
era
lizab
ility
of
the
stu
dy.
Bra
zil
[67
]R
etr
osp
ect
ive
20
08
All
pat
ien
tsw
ith
con
ge
stiv
eh
ear
tfa
ilure
tre
ate
dat
the
ou
tpat
ien
tcl
inic
of
Ho
spit
ald
asC
lınic
aso
fth
eFe
de
ral
Un
ive
rsit
yo
fG
oia
s.Ex
clu
sio
n:
tho
sew
ho
die
din
20
08
(th
eir
me
dic
alre
cord
sw
ere
inco
mp
lete
)o
rw
ho
we
ren
ot
fro
mth
est
ate
of
Go
ias.
No
tsp
eci
fie
d.
14
4St
ren
gth
s:U
nb
iase
dca
sese
lect
ion
.Li
mit
atio
ns:
Re
tro
spe
ctiv
eu
seo
fca
sen
ote
sw
ith
ou
tsp
eci
fie
dd
iag
no
stic
crit
eri
a.Si
ng
leu
rban
cen
tre
that
may
no
tb
ere
pre
sen
tati
veo
fth
ep
atte
rns
of
care
atth
en
atio
nal
leve
l.P
atie
nts
wh
od
ied
wit
hin
the
tim
efr
ame
of
the
stu
dy
we
ree
xclu
de
d,
limit
ing
the
stu
dy
top
atie
nts
wit
hle
ssse
vere
form
so
fh
ear
tfa
ilure
.
Bra
zil
[65
]P
rosp
ect
ive
19
97
10
0p
atie
nts
we
rera
nd
om
lyse
lect
ed
fro
mth
eo
utp
atie
nt
de
par
tme
nt
of
the
Ho
spit
ald
asC
linic
as,
ate
rtia
ryre
ferr
alce
ntr
ein
Sao
Pau
lo.
Pat
ien
tsw
ere
incl
ud
ed
ifth
ey
we
refo
un
do
ne
cho
card
iog
rap
hy
toh
ave
aLV
EFo
f,
60
%.
Ech
oca
rdio
gra
ph
y.1
00
Stre
ng
ths:
All
pat
ien
tsh
ade
cho
card
iog
rap
hy
pe
rfo
rme
d,
aid
ing
wit
hth
eac
cura
cyo
fd
iag
no
sis.
Lim
itat
ion
s:Si
ng
leu
rban
tert
iary
refe
rral
cen
tre
that
may
no
tb
ere
pre
sen
tati
veo
fth
eb
road
er
po
pu
lati
on
.
Bra
zil
[66
]R
etr
osp
ect
ive
19
95
An
alys
iso
fth
ose
pat
ien
tsad
mit
ted
wit
hh
ear
tfa
ilure
toth
eH
ear
tIn
stit
ute
of
Sao
Pau
lou
sin
gth
eP
RO
DES
Pre
gis
try.
No
tsp
eci
fie
d.
90
3St
ren
gth
s:D
atas
et
of
all
pat
ien
tsad
mit
ted
ove
rth
eco
urs
eo
f1
99
5w
ith
he
art
failu
reto
this
ho
spit
al.
Lim
itat
ion
s:Sp
eci
alis
th
ear
tfa
ilure
urb
anh
osp
ital
,w
ho
sep
atie
nts
may
no
tb
eg
en
era
lizab
le.
No
form
alst
and
ard
for
the
dia
gn
osi
so
fh
ear
tfa
ilure
isd
ocu
me
nte
d.
Ch
ile[4
1]
Pro
spe
ctiv
e2
00
2–
20
04
37
2p
atie
nts
wit
hN
YH
Acl
ass
IIIo
rIV
he
art
failu
refr
om
14
cen
tre
sin
Ch
ilew
ere
incl
ud
ed
.Ex
clu
sio
n:
pri
nci
pal
reas
on
for
ho
spit
alis
atio
nw
asn
ot
he
art
failu
reo
rn
ew
-on
set
he
art
failu
reo
rca
rdio
ge
nic
sho
ckse
con
dar
yto
am
yoca
rdia
lin
farc
tio
n.
Clin
ical
dia
gn
osi
su
sin
gEu
rop
ean
Soci
ety
of
Car
dio
log
yd
iag
no
stic
crit
eri
a.In
case
so
fd
ou
bt
resp
on
seto
tre
atm
en
tw
asu
sed
.5
2%
un
de
rwe
nt
ech
oca
rdio
gra
ph
y.
37
2St
ren
gth
s:N
atio
nal
Re
gis
try
of
He
art
Failu
reo
fC
hile
,1
4ce
ntr
es.
Cle
ard
iag
no
stic
crit
eri
a.Li
mit
atio
ns:
Ch
oic
eo
fp
arti
cip
atin
gce
ntr
es
no
td
esc
rib
ed
.Ex
clu
sio
no
fp
atie
nts
wit
hh
ear
tfa
ilure
afte
ra
myo
card
ial
infa
rcti
on
may
lead
toar
tifi
cial
lylo
wra
tes
of
IHD
asth
eat
trib
ute
dca
use
of
he
art
failu
re.
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 28 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
2.
Co
nt.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Ch
ile[7
0]‘
Pro
spe
ctiv
e2
00
8–
20
09
All
ou
tpat
ien
ts$
21
yo
fag
ew
ith
ne
wo
rp
revi
ou
sly
dia
gn
ose
dh
ear
tfa
ilure
.Ex
clu
sio
n:
pat
ien
tsw
ith
acu
ted
eco
mp
en
sate
dh
ear
tfa
ilure
.
Fram
ing
ham
crit
eri
a.7
8%
had
ane
cho
card
iog
ram
.
19
9T
he
sed
ata
com
efr
om
the
IP
REF
ERre
gis
try.
Stre
ng
ths:
.1
0ce
ntr
es.
Site
sw
ere
ran
do
mly
sele
cte
d,
and
all
card
iolo
gis
tsw
ith
inth
eco
un
try
con
sid
ere
de
ligib
le.
Mis
sin
gd
ata
and
loss
tofo
llow
-up
tran
spar
en
t.P
rosp
ect
ive
tria
lw
ith
ina
spe
cifi
ed
recr
uit
me
nt
pe
rio
d.
78
%h
adco
nfi
rmat
ion
of
he
art
failu
reth
rou
gh
ech
oca
rdio
gra
ph
y.Li
mit
atio
ns:
Re
pre
sen
tati
veo
nly
of
tho
seat
ten
din
go
utp
atie
nt
card
iolo
gy
serv
ice
s,e
xclu
din
gth
eac
ute
sect
or
or
tho
sep
atie
nts
inp
rim
ary
care
wit
hh
ear
tfa
ilure
no
tu
nd
er
join
tca
reo
fa
card
iolo
gis
t.
Co
lom
bia
[70
]‘P
rosp
ect
ive
20
08
–2
00
9A
llo
utp
atie
nts
$2
1y
of
age
wit
hn
ew
or
pre
vio
usl
yd
iag
no
sed
he
art
failu
re.
Excl
usi
on
:p
atie
nts
wit
hac
ute
de
com
pe
nsa
ted
he
art
failu
re.
Fram
ing
ham
crit
eri
a.7
2%
had
ane
cho
card
iog
ram
.
21
1T
he
sed
ata
com
efr
om
the
IP
REF
ERre
gis
try.
Stre
ng
ths:
.1
0ce
ntr
es.
Site
sw
ere
ran
do
mly
sele
cte
d,
and
all
card
iolo
gis
tsw
ith
inth
eco
un
try
con
sid
ere
de
ligib
le.
Mis
sin
gd
ata
and
loss
tofo
llow
-up
tran
spar
en
t.P
rosp
ect
ive
tria
lw
ith
ina
spe
cifi
ed
recr
uit
me
nt
pe
rio
d.
.7
0%
had
con
firm
atio
no
fh
ear
tfa
ilure
thro
ug
he
cho
card
iog
rap
hy.
Lim
itat
ion
s:R
ep
rese
nta
tive
on
lyo
fth
ose
atte
nd
ing
ou
tpat
ien
tca
rdio
log
yse
rvic
es,
exc
lud
ing
the
acu
tese
cto
ro
rth
ose
pat
ien
tsin
pri
mar
yca
rew
ith
he
art
failu
ren
ot
un
de
rjo
int
care
of
aca
rdio
log
ist.
Me
xico
[70
]‘P
rosp
ect
ive
20
08
–2
00
9A
llo
utp
atie
nts
$2
1y
of
age
wit
hn
ew
or
pre
vio
usl
yd
iag
no
sed
he
art
failu
re.
Excl
usi
on
:p
atie
nts
wit
hac
ute
de
com
pe
nsa
ted
he
art
failu
re.
Fram
ing
ham
crit
eri
a.7
5%
had
ane
cho
card
iog
ram
.
45
8T
he
sed
ata
com
efr
om
the
IP
REF
ERre
gis
try.
Stre
ng
ths:
.1
0ce
ntr
es.
Site
sw
ere
ran
do
mly
sele
cte
d,
and
all
card
iolo
gis
tsw
ith
inth
eco
un
try
con
sid
ere
de
ligib
le.
Mis
sin
gd
ata
and
loss
tofo
llow
-up
tran
spar
en
t.P
rosp
ect
ive
tria
lw
ith
ina
spe
cifi
ed
recr
uit
me
nt
pe
rio
d.
75
%h
adco
nfi
rmat
ion
of
he
art
failu
reth
rou
gh
ech
oca
rdio
gra
ph
y.Li
mit
atio
ns:
Re
pre
sen
tati
veo
nly
of
tho
seat
ten
din
go
utp
atie
nt
card
iolo
gy
serv
ice
s,e
xclu
din
gth
eac
ute
sect
or
or
tho
sep
atie
nts
inp
rim
ary
care
wit
hh
ear
tfa
ilure
no
tu
nd
er
join
tca
reo
fa
card
iolo
gis
t.
‘P
revi
ou
sly
un
pu
blis
he
dd
ata.
NY
HA
,N
ew
Yo
rkH
ear
tA
sso
ciat
ion
.d
oi:1
0.1
37
1/j
ou
rnal
.pm
ed
.10
01
69
9.t
00
2
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 29 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
3.
Ch
arac
teri
stic
so
fEa
ste
rnM
ed
ite
rran
ean
reg
ion
stu
die
san
dd
atab
ase
sin
clu
de
d.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Egyp
t[7
0]‘
Pro
spe
ctiv
e2
00
8–
20
09
All
ou
tpat
ien
ts$
21
yo
fag
ew
ith
ne
wo
rp
revi
ou
sly
dia
gn
ose
dh
ear
tfa
ilure
.Ex
clu
sio
n:
pat
ien
tsw
ith
acu
ted
eco
mp
en
sate
dh
ear
tfa
ilure
.
Fram
ing
ham
crit
eri
a.7
3%
had
ane
cho
card
iog
ram
.4
34
Th
ese
dat
aco
me
fro
mth
eI
PR
EFER
reg
istr
y.St
ren
gth
s:.
10
cen
tre
s.Si
tes
we
rera
nd
om
lyse
lect
ed
,an
dal
lca
rdio
log
ists
wit
hin
the
cou
ntr
yco
nsi
de
red
elig
ible
.M
issi
ng
dat
aan
dlo
ssto
follo
w-u
ptr
ansp
are
nt.
Pro
spe
ctiv
etr
ial
wit
hin
asp
eci
fie
dre
cru
itm
en
tp
eri
od
..
90
%h
adco
nfi
rmat
ion
of
he
art
failu
reth
rou
gh
ech
oca
rdio
gra
ph
y.Li
mit
atio
ns:
Re
pre
sen
tati
veo
nly
of
tho
seat
ten
din
go
utp
atie
nt
card
iolo
gy
serv
ice
s,e
xclu
din
gth
eac
ute
sect
or
or
tho
sep
atie
nts
inp
rim
ary
care
wit
hh
ear
tfa
ilure
no
tu
nd
er
join
tca
reo
fa
card
iolo
gis
t.
Iran
#,‘
Re
tro
spe
ctiv
e1
99
8–
20
12
All
27
7p
atie
nts
wit
hh
ear
tfa
ilure
fro
ma
dat
ase
to
f8
3,8
95
ho
spit
alis
ed
pat
ien
tsin
Iran
.U
np
ub
lish
ed
dat
ase
t.
No
tsp
eci
fie
d.
27
7St
ren
gth
s:M
ult
i-ce
ntr
est
ud
y.Li
mit
atio
ns:
No
n-r
and
om
sele
ctio
no
fh
osp
ital
s.D
iag
no
stic
crit
eri
au
sed
un
spe
cifi
ed
.
Iran
[70
]‘P
rosp
ect
ive
20
08
–2
00
9A
llo
utp
atie
nts
$2
1y
of
age
wit
hn
ew
or
pre
vio
usl
yd
iag
no
sed
he
art
failu
re.
Excl
usi
on
:p
atie
nts
wit
hac
ute
de
com
pe
nsa
ted
he
art
failu
re.
Fram
ing
ham
crit
eri
a.9
5%
had
ane
cho
card
iog
ram
.1
05
Th
ese
dat
aco
me
fro
mth
eI
PR
EFER
reg
istr
y.St
ren
gth
s:.
10
cen
tre
s.Si
tes
we
rera
nd
om
lyse
lect
ed
,an
dal
lca
rdio
log
ists
wit
hin
the
cou
ntr
yco
nsi
de
red
elig
ible
.M
issi
ng
dat
aan
dlo
ssto
follo
w-u
ptr
ansp
are
nt.
Pro
spe
ctiv
etr
ial
wit
hin
asp
eci
fie
dre
cru
itm
en
tp
eri
od
..
90
%h
adco
nfi
rmat
ion
of
he
art
failu
reth
rou
gh
ech
oca
rdio
gra
ph
y.Li
mit
atio
ns:
Re
pre
sen
tati
veo
nly
of
tho
seat
ten
din
go
utp
atie
nt
card
iolo
gy
serv
ice
s,e
xclu
din
gth
eac
ute
sect
or
or
tho
sep
atie
nts
inp
rim
ary
care
wit
hh
ear
tfa
ilure
no
tu
nd
er
join
tca
reo
fa
card
iolo
gis
t.
Leb
ano
n[7
0]‘
Pro
spe
ctiv
e2
00
8–
20
09
All
ou
tpat
ien
ts$
21
yo
fag
ew
ith
ne
wo
rp
revi
ou
sly
dia
gn
ose
dh
ear
tfa
ilure
.Ex
clu
sio
n:
pat
ien
tsw
ith
acu
ted
eco
mp
en
sate
dh
ear
tfa
ilure
.
Fram
ing
ham
crit
eri
a.8
3%
had
ane
cho
card
iog
ram
.1
81
Th
ese
dat
aco
me
fro
mth
eI
PR
EFER
reg
istr
y.St
ren
gth
s:.
10
cen
tre
s.Si
tes
we
rera
nd
om
lyse
lect
ed
,an
dal
lca
rdio
log
ists
wit
hin
the
cou
ntr
yco
nsi
de
red
elig
ible
.M
issi
ng
dat
aan
dlo
ssto
follo
w-u
ptr
ansp
are
nt.
Pro
spe
ctiv
etr
ial
wit
hin
asp
eci
fie
dre
cru
itm
en
tp
eri
od
..
80
%h
adco
nfi
rmat
ion
of
he
art
failu
reth
rou
gh
ech
oca
rdio
gra
ph
y.Li
mit
atio
ns:
Re
pre
sen
tati
veo
nly
of
tho
seat
ten
din
go
utp
atie
nt
card
iolo
gy
serv
ice
s,e
xclu
din
gth
eac
ute
sect
or
or
tho
sep
atie
nts
inp
rim
ary
care
wit
hh
ear
tfa
ilure
no
tu
nd
er
join
tca
reo
fa
card
iolo
gis
t.
Pak
ista
n[4
7]
Re
tro
spe
ctiv
e2
00
2–
20
03
Firs
tp
rese
nta
tio
nto
Ag
ha
Kh
anU
niv
ers
ity
Ho
spit
alin
Kar
ach
iw
ith
the
dia
gn
osi
so
fn
ew
-on
set
con
ge
stiv
eh
ear
tfa
ilure
that
me
tth
eB
ost
on
crit
eri
a.Ex
clu
sio
n:
LVEF
$4
0%
,p
rio
rd
iag
no
sis
of
syst
olic
he
art
failu
red
atin
gb
ack
3m
o,
un
de
rlyi
ng
dis
eas
ew
ith
exp
ect
ed
surv
ival
of
less
than
6m
on
ths,
kno
wn
pri
mar
yva
lvu
lar
he
art
dis
eas
e(r
he
um
atic
or
no
nrh
eu
mat
ic),
pat
ien
td
ied
in-h
osp
ital
,o
rn
ofo
llow
-up
avai
lab
leaf
ter
dis
char
ge
.
Clin
ical
dia
gn
osi
sb
ase
do
nB
ost
on
crit
eri
a.A
llp
atie
nts
rece
ive
de
cho
card
iog
rap
hy.
19
6St
ren
gth
s:A
llp
atie
nts
had
ech
oca
rdio
gra
ph
icas
sess
me
nt.
Lim
itat
ion
s:Si
ng
lete
rtia
ryre
ferr
alce
ntr
ein
Kar
ach
im
ayn
ot
be
ge
ne
raliz
able
toth
eb
road
er
po
pu
lati
on
.Th
ee
xclu
sio
no
fva
lvu
lar
he
art
dis
eas
em
ayim
pac
to
nth
eae
tio
log
ies
ascr
ibe
dto
case
so
fh
ear
tfa
ilure
.Sim
ilarl
y,th
ee
xclu
sio
no
fth
ose
wh
od
ied
inh
osp
ital
may
affe
ctth
eg
en
era
lizab
ility
of
the
fin
din
gs.
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 30 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
3.
Co
nt.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Tu
nis
ia[7
0]‘
Pro
spe
ctiv
e2
00
8–
20
09
All
ou
tpat
ien
ts$
21
yo
fag
ew
ith
ne
wo
rp
revi
ou
sly
dia
gn
ose
dh
ear
tfa
ilure
.Ex
clu
sio
n:
pat
ien
tsw
ith
acu
ted
eco
mp
en
sate
dh
ear
tfa
ilure
.
Fram
ing
ham
crit
eri
a.7
1%
had
ane
cho
card
iog
ram
.2
57
Th
ese
dat
aco
me
fro
mth
eI
PR
EFER
reg
istr
y.St
ren
gth
s:.
10
cen
tre
s.Si
tes
we
rera
nd
om
lyse
lect
ed
,an
dal
lca
rdio
log
ists
wit
hin
the
cou
ntr
yco
nsi
de
red
elig
ible
.M
issi
ng
dat
aan
dlo
ssto
follo
w-u
ptr
ansp
are
nt.
Pro
spe
ctiv
etr
ial
wit
hin
asp
eci
fie
dre
cru
itm
en
tp
eri
od
.7
1%
had
con
firm
atio
no
fh
ear
tfa
ilure
thro
ug
he
cho
card
iog
rap
hy.
Lim
itat
ion
s:R
ep
rese
nta
tive
on
lyo
fth
ose
atte
nd
ing
ou
tpat
ien
tca
rdio
log
yse
rvic
es,
exc
lud
ing
the
acu
tese
cto
ro
rth
ose
pat
ien
tsin
pri
mar
yca
rew
ith
he
art
failu
ren
ot
un
de
rjo
int
care
of
aca
rdio
log
ist.
Ye
me
n[4
8]
Pro
spe
ctiv
e2
00
7–
20
08
Firs
t1
00
con
secu
tive
pat
ien
tsad
mit
ted
toIb
nSe
en
aC
en
tral
Ho
spit
al,
Mu
kalla
,w
ith
he
art
failu
re.
All
pat
ien
tsw
ere
req
uir
ed
toh
ave
blo
od
test
s,e
lect
roca
rdio
gra
m,
ech
oca
rdio
gra
m,
and
che
stra
dio
gra
m.
Excl
usi
on
:al
lp
atie
nts
wh
ofo
ran
yre
aso
nd
rop
pe
dfr
om
follo
w-u
pb
efo
rein
vest
igat
ion
was
com
ple
ted
(die
d,
tran
sfe
rre
d,
dis
char
ge
d)
Fram
ing
ham
crit
eri
a.A
llp
atie
nts
un
de
rwe
nt
ech
oca
rdio
gra
ph
y.
10
0St
ren
gth
s:C
lear
dia
gn
ost
iccr
ite
ria
for
un
de
rlyi
ng
aeti
olo
gie
s.A
llp
atie
nts
had
ech
oca
rdio
gra
ph
icas
sess
me
nt.
Re
ferr
alce
ntr
efo
ra
larg
eca
tch
me
nt
are
a.Li
mit
atio
ns:
Sin
gle
urb
ante
rtia
ryre
ferr
alce
ntr
em
ayn
ot
be
rep
rese
nta
tive
of
the
bro
ade
rp
op
ula
tio
no
fp
atie
nts
wit
hh
ear
tfa
ilure
.
‘P
revi
ou
sly
un
pu
blis
he
dd
ata.
#S.
Rah
imza
de
h,
F.Fa
rzad
far
F,an
dM
.G
haz
ian
i,u
np
ub
lish
ed
dat
a.d
oi:1
0.1
37
1/j
ou
rnal
.pm
ed
.10
01
69
9.t
00
3
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 31 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
4.
Ch
arac
teri
stic
so
fEu
rop
ere
gio
nst
ud
ies
and
dat
abas
es
incl
ud
ed
.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Ro
man
ia[5
1]
Re
tro
spe
ctiv
e2
00
64
59
con
secu
tive
lyad
mit
ted
pat
ien
tsb
etw
ee
nJa
nu
ary
and
De
cem
be
r2
00
6to
the
card
iolo
gy
de
par
tme
nt
wit
ha
dis
char
ge
dia
gn
osi
so
fch
ron
ich
ear
tfa
ilure
.
No
tsp
eci
fie
d.
45
9Li
mit
atio
ns:
Sin
gle
urb
ang
en
era
lh
osp
ital
may
no
tb
ere
pre
sen
tati
veo
fth
eb
road
er
po
pu
lati
on
of
pat
ien
tsw
ith
he
art
failu
re.
Dia
gn
ost
iccr
ite
ria
no
tcl
ear
.D
ata
reco
rde
dfr
om
ho
spit
alfi
les.
Un
cle
arh
ow
mis
sin
gd
ata
we
reac
cou
nte
dfo
r.
Ro
man
ia[5
0]
Pro
spe
ctiv
e2
00
8–
20
09
All
con
secu
tive
pat
ien
tsh
osp
ital
ise
dw
ith
ap
rim
ary
dia
gn
osi
so
fac
ute
he
art
failu
resy
nd
rom
es.
Excl
usi
on
:p
atie
nts
wit
hh
igh
-ou
tpu
th
ear
tfa
ilure
.
Euro
pe
anSo
cie
tyo
fC
ard
iolo
gy
gu
ide
line
s.8
0%
of
pat
ien
tsh
adan
ech
oca
rdio
gra
m.
3,2
24
Stre
ng
ths:
Nat
ion
alre
gis
try
invo
lvin
g1
3si
tes,
incr
eas
ing
the
ge
ne
raliz
abili
tyo
fit
sre
sult
s.A
larg
em
ajo
rity
of
pat
ien
tsh
ade
cho
card
iog
rap
hic
asse
ssm
en
t.B
oth
tert
iary
acad
em
icce
ntr
es
and
ge
ne
ral
ho
spit
als
we
rein
clu
de
d,
incr
eas
ing
ge
ne
raliz
abili
ty.
Lim
itat
ion
s:U
ncl
ear
ho
wm
issi
ng
dat
aw
ere
acco
un
ted
for,
alth
ou
gh
this
issu
eis
ackn
ow
led
ge
din
the
irlim
itat
ion
sse
ctio
n.
Serb
ia[6
1]
Cro
ss-s
ect
ion
alU
nkn
ow
nP
atie
nts
wit
hch
ron
ich
ear
tfa
ilure
we
rere
cru
ite
dfr
om
ano
utp
atie
nt
card
iolo
gy
clin
icat
the
Clin
icfo
rC
ard
iova
scu
lar
Dis
eas
es,
Clin
ical
Ce
nte
rN
is.
Excl
usi
on
:th
ose
wh
oh
adh
ada
wo
rse
nin
go
fsy
mp
tom
so
rch
ang
es
intr
eat
me
nt
inth
ep
rece
din
g2
wk.
Euro
pe
anSo
cie
tyo
fC
ard
iolo
gy
and
ech
oca
rdio
gra
ph
y.1
27
Stre
ng
ths:
All
pat
ien
tsu
nd
erw
en
te
cho
card
iog
rap
hy.
Stan
dar
dis
ed
dia
gn
ost
iccr
ite
ria.
Lim
itat
ion
s:Si
ng
leu
rban
cen
tre
may
no
tb
ere
pre
sen
tati
veo
fth
eb
road
er
po
pu
lati
on
.U
ncl
ear
me
tho
do
fca
seas
cert
ain
me
nt.
Tu
rke
y[4
9]
Re
tro
spe
ctiv
e1
99
7–
19
98
Me
dic
alre
cord
so
fco
nse
cuti
vep
atie
nts
adm
itte
dfo
rco
ng
est
ive
he
art
failu
reat
16
acad
em
ich
osp
ital
sw
ere
sele
cte
dfo
rre
vie
w:
‘‘Th
em
ost
rece
nt,
inav
era
ge
,5
0p
atie
nts
fro
me
ach
cen
tre
wit
hsu
ffic
ien
td
ata
for
CH
F[c
on
ge
stiv
eh
ear
tfa
ilure
]in
the
irfi
les
we
rein
clu
de
d’’.
Am
eri
can
He
art
Ass
oci
atio
ng
uid
elin
es.
81
%h
adan
ech
oca
rdio
gra
m.
66
1St
ren
gth
s:1
6ce
ntr
es
fro
mac
ross
the
cou
ntr
y.A
larg
em
ajo
rity
of
ind
ivid
ual
sh
ade
cho
card
iog
rap
hic
asse
ssm
en
t.Li
mit
atio
ns:
Re
sult
sfr
om
acad
em
ich
osp
ital
sm
ayn
ot
be
ge
ne
raliz
able
toth
eb
road
er
he
alth
syst
em
.M
eth
od
of
case
asce
rtai
nm
en
tm
ayle
adto
sele
ctio
nb
ias.
Un
cle
arh
ow
mis
sin
gd
ata
we
reac
cou
nte
dfo
r.
Tu
rke
y[6
4]
Pro
spe
ctiv
e1
99
9–
20
00
Asu
rve
yw
asco
nd
uct
ed
of
ara
nd
om
sam
ple
of
11
7p
rim
ary
care
ph
ysic
ian
sfr
om
acro
ssT
urk
ey
wh
olo
gg
ed
all
pat
ien
tsth
ey
saw
wit
hh
ear
tfa
ilure
.
No
tsp
eci
fie
d.
87
6St
ren
gth
s:R
eal
-wo
rld
pra
ctic
eta
ken
fro
ma
ran
do
msa
mp
leo
f1
17
pri
mar
yca
rep
hys
icia
ns
fro
mac
ross
Tu
rke
y.Li
mit
atio
ns:
Dia
gn
osi
so
fh
ear
tfa
ilure
left
toth
ecl
inic
ian
s.
Tu
rke
y[6
3]
Pro
spe
ctiv
e2
00
5A
sam
ple
of
4,6
50
ran
do
mly
sele
cte
din
div
idu
als
had
the
irh
eig
ht,
we
igh
t,b
loo
dp
ress
ure
me
asu
red
asw
ell
asan
ECG
and
blo
od
take
nfo
rN
T-p
roB
NP
leve
l.A
ny
of
the
sam
ple
wit
ha
card
iac
his
tory
,ab
no
rmal
ECG
,o
rN
T-p
roB
NP
$1
20
pg
/ml
was
furt
he
rin
vest
igat
ed
wit
he
cho
card
iog
rap
hy.
Ech
oca
rdio
gra
ph
y.3
20
Stre
ng
ths:
Po
pu
lati
on
-bas
ed
ran
do
msa
mp
leo
fin
div
idu
als
may
pro
vid
eg
en
era
lizab
lein
form
atio
no
np
reva
len
ceo
fh
ear
tfa
ilure
.
ECG
,e
lect
roca
rdio
gra
m.
do
i:10
.13
71
/jo
urn
al.p
me
d.1
00
16
99
.t0
04
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 32 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
5.
Ch
arac
teri
stic
so
fSo
uth
East
Asi
are
gio
nst
ud
ies
and
dat
abas
es
incl
ud
ed
.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Ind
ia[6
9]‘
Re
tro
spe
ctiv
e2
00
8–
20
12
Bill
ing
cod
es
fro
mh
osp
ital
use
dto
ide
nti
fyp
atie
nts
wit
hh
ear
tfa
ilure
inA
nd
hra
Pra
de
sh.
No
tsp
eci
fie
d.
5,7
58
Stre
ng
ths:
Th
isst
ud
yo
fb
illin
gd
ata
isfr
om
ala
rge
sam
ple
of
ove
r1
.5m
illio
nh
osp
ital
isat
ion
s.Li
mit
atio
ns:
Bill
ing
dat
are
lyo
ncl
inic
alco
din
g,
and
con
seq
ue
ntl
yth
ere
are
no
stan
dar
dis
ed
dia
gn
ost
iccr
ite
ria
avai
lab
le.
Ind
on
esi
a[2
0]
Pro
spe
ctiv
e2
00
6C
on
secu
tive
lyh
osp
ital
ise
dp
atie
nts
$1
8y
infi
veh
osp
ital
s.P
atie
nts
wit
hh
ear
tfa
ilure
pri
mar
ilyb
ein
gtr
eat
ed
asa
co-m
orb
idra
the
rth
anp
rim
ary
con
dit
ion
.Ex
clu
sio
n:
tho
sew
ith
ou
tan
acce
ssib
lem
ed
ical
reco
rd,
tho
sew
ith
ou
tac
ute
de
com
pe
nsa
ted
he
art
failu
re.
No
tsp
eci
fie
d.
1,6
87
Ind
on
esi
anar
mo
fA
DH
ERE-
Inte
rnat
ion
al.
Stre
ng
ths:
Five
ho
spit
als,
imp
rovi
ng
the
po
ten
tial
ge
ne
raliz
abili
tyo
fre
sult
s.M
issi
ng
dat
atr
ansp
are
ntl
yac
cou
nte
dfo
r.Ec
ho
card
iog
rap
hic
asse
ssm
en
tin
37
.9%
of
pat
ien
ts.
Lim
itat
ion
s:D
isch
arg
ed
ata
wit
hla
cko
fst
and
ard
isat
ion
inth
ed
iag
no
sis
of
he
art
failu
re,
wh
ich
may
lead
tose
lect
ion
bia
s.
Th
aila
nd
[52
]R
etr
osp
ect
ive
20
06
–2
00
7C
on
secu
tive
lyh
osp
ital
ise
dp
atie
nts
age
mo
reth
an1
8y
at1
8ca
rdio
vasc
ula
rce
ntr
es.
Pat
ien
tsw
ith
he
art
failu
rep
rim
arily
be
ing
tre
ate
das
aco
-mo
rbid
rath
er
than
pri
mar
yco
nd
itio
n.
Excl
usi
on
:th
ose
wit
ho
ut
anac
cess
ible
me
dic
alre
cord
,p
atie
nts
wit
hca
rdio
ge
nic
sho
ck,
and
pe
rio
pe
rati
veh
ear
tfa
ilure
.
No
tsp
eci
fie
d.
1,6
12
Th
aiar
mo
fA
DH
ERE-
Inte
rnat
ion
al.
Stre
ng
ths:
18
card
iova
scu
lar
cen
tre
sfr
om
acro
ssth
eco
un
try,
con
seq
ue
ntl
yg
reat
er
ge
ne
raliz
abili
tyo
fth
ere
sult
s.6
0.4
%h
ade
cho
card
iog
rap
hic
asse
ssm
en
t.Li
mit
atio
ns:
Dis
char
ge
dat
aw
ith
lack
of
stan
dar
dis
atio
nin
the
dia
gn
osi
so
fh
ear
tfa
ilure
,w
hic
hm
ayle
adto
sele
ctio
nb
ias.
‘P
revi
ou
sly
un
pu
blis
he
dd
ata.
do
i:10
.13
71
/jo
urn
al.p
me
d.1
00
16
99
.t0
05
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 33 August 2014 | Volume 11 | Issue 8 | e1001699
Ta
ble
6.
Ch
arac
teri
stic
so
fW
est
ern
Pac
ific
reg
ion
stu
die
san
dd
atab
ase
sin
clu
de
d.
Co
un
try
of
Ori
gin
Stu
dy
De
sig
nR
ecr
uit
me
nt
Pe
rio
dS
ele
ctio
nC
rite
ria
He
art
Fa
ilu
reD
efi
nit
ion
Ca
ses
of
He
art
Fa
ilu
reS
tre
ng
ths
an
dL
imit
ati
on
s
Ch
ina
[57
]R
etr
osp
ect
ive
19
80
–2
00
0P
atie
nts
adm
itte
dw
ith
he
art
failu
reto
par
tici
pat
ing
ho
spit
als.
No
tsp
eci
fie
d.
1,7
56
Stre
ng
ths:
Mu
lti-
cen
tre
stu
dy
may
incr
eas
eg
en
era
lizab
ility
of
resu
lts.
Lon
gst
ud
yti
me
pe
rio
de
nab
ling
anal
ysis
of
tre
nd
sac
ross
tim
e.
Lim
itat
ion
s:R
etr
osp
ect
ive
use
of
case
no
tes,
wit
hco
nse
qu
en
tla
cko
fst
and
ard
ise
dd
iag
no
stic
crit
eri
a,m
ayin
cre
ase
sele
ctio
nan
dre
po
rtin
gb
ias.
Ch
ina
[58
]R
etr
osp
ect
ive
19
80
–2
00
8P
atie
nts
adm
itte
dto
the
me
dic
alw
ard
sd
uri
ng
the
stu
dy
pe
rio
d.
No
tsp
eci
fie
d.
2,4
58
Stre
ng
ths:
Lon
gti
me
pe
rio
do
fst
ud
yal
low
ed
the
anal
ysis
of
me
dic
atio
np
resc
rip
tio
nch
ang
es
ove
rti
me
.Li
mit
atio
ns:
Urb
ansi
ng
le-c
en
tre
stu
dy
may
no
tb
eg
en
era
lizab
leto
bro
ade
rh
eal
thse
rvic
e.
Re
tro
spe
ctiv
eu
seo
fca
sen
ote
sw
ith
ou
tst
and
ard
ise
dd
iag
no
stic
crit
eri
afo
rh
ear
tfa
ilure
may
incr
eas
ere
po
rtin
gan
dse
lect
ion
bia
s.
Ch
ina
[56
]R
etr
osp
ect
ive
19
95
–2
00
4P
atie
nts
adm
itte
dw
ith
he
art
failu
re.
No
tsp
eci
fie
d.
25
9Li
mit
atio
ns:
Dia
gn
ost
iccr
ite
ria
no
tst
and
ard
ise
d,
lead
ing
top
ote
nti
alfo
rre
po
rtin
gan
dse
lect
ion
bia
s.
Ch
ina
[53
]R
etr
osp
ect
ive
19
95
–2
00
9P
atie
nts
adm
itte
dw
ith
he
art
failu
reto
thre
eu
niv
ers
ity
ho
spit
als.
Am
eri
can
He
art
Ass
oci
atio
n2
00
5g
uid
elin
es.
1,1
19
Stre
ng
ths:
Mu
lti-
cen
tre
coh
ort
stu
dy.
Lim
itat
ion
s:A
cad
em
icce
ntr
es
may
no
tre
fle
ctth
eb
road
er
he
alth
serv
ice
.
Ch
ina
[55
]R
etr
osp
ect
ive
20
07
Pat
ien
tsad
mit
ted
wit
hh
ear
tfa
ilure
.Fr
amin
gh
amcr
ite
ria.
47
8Li
mit
atio
ns:
Ru
ral
sin
gle
-ce
ntr
est
ud
yth
atm
ayn
ot
be
ge
ne
raliz
able
toth
eb
road
er
he
alth
serv
ice
.R
etr
osp
ect
ive
anal
ysis
of
case
no
tes
op
en
tore
po
rtin
gb
ias.
Ch
ina
[54
]R
etr
osp
ect
ive
20
08
–2
00
9P
atie
nts
adm
itte
dw
ith
he
art
failu
re.
Euro
pe
anSo
cie
tyo
fC
ard
iolo
gy
20
05
gu
ide
line
s2
06
Lim
itat
ion
s:U
rban
sin
gle
-ce
ntr
est
ud
yth
atm
ayn
ot
be
ge
ne
raliz
able
toth
eb
road
er
he
alth
serv
ice
.
Ch
ina
[60
]P
rosp
ect
ive
Un
kno
wn
(pu
blis
he
d2
01
2)
Ind
ivid
ual
sad
mit
ted
toth
eP
eo
ple
’sLi
be
rati
on
Arm
yG
en
era
lH
osp
ital
,B
eiji
ng
,o
ver
the
age
of
60
yw
ith
ad
iag
no
sis
of
chro
nic
he
art
failu
re.
Excl
usi
on
:th
ose
wit
hse
vere
aort
icst
en
osi
s,an
tici
pat
ed
card
iac
tran
spla
nta
tio
n,
or
ale
ftve
ntr
icu
lar
assi
std
evi
ce.
Euro
pe
anSo
cie
tyo
fC
ard
iolo
gy
20
08
gu
ide
line
s.3
27
Lim
itat
ion
s:Si
ng
le-c
en
tre
arm
yg
en
era
lh
osp
ital
inth
eca
pit
alw
ith
ah
igh
pro
po
rtio
no
fm
ale
pat
ien
ts(7
8%
of
this
coh
ort
)m
ayn
ot
be
bro
adly
ge
ne
raliz
able
.
Ch
ina
[62
]P
rosp
ect
ive
Un
kno
wn
(pu
blis
he
d2
00
9)
Clu
ste
rra
nd
om
ise
dsa
mp
leo
fad
ult
sin
pri
mar
yca
refa
cilit
ies
wit
hco
ng
est
ive
he
art
failu
rein
six
cou
nti
es
of
Liao
nin
gP
rovi
nce
.
Fram
ing
ham
crit
eri
a.5
29
Stre
ng
ths:
Clu
ste
rra
nd
om
isat
ion
of
pri
mar
yca
refa
cilit
ies,
red
uci
ng
po
ten
tial
for
bia
s.R
ep
rese
nta
tio
nfr
om
six
cou
nti
es
of
Liao
nin
gP
rovi
nce
may
imp
rove
reg
ion
alg
en
era
lizab
ility
of
the
resu
lts.
Lim
itat
ion
s:U
nce
rtai
nd
iag
no
stic
crit
eri
aan
dp
atie
nt
po
ol.
Mal
aysi
a[6
8]‘
Re
tro
spe
ctiv
e2
00
7–
20
08
Co
nse
cuti
vein
div
idu
als
wit
ha
pri
nci
pal
dis
char
ge
dia
gn
osi
so
fh
ear
tfa
ilure
,u
sin
gth
ere
leva
nt
Inte
rnat
ion
alC
lass
ific
atio
no
fD
ise
ase
-9co
de
s.P
atie
nts
wit
hh
ear
tfa
ilure
pri
mar
ilyb
ein
gtr
eat
ed
asa
co-m
orb
idra
the
rth
anp
rim
ary
con
dit
ion
.Ex
clu
sio
n:
pat
ien
ts,
18
y,th
ose
wit
ho
ut
anac
cess
ible
me
dic
alre
cord
,th
ose
wit
ho
ut
acu
ted
eco
mp
en
sate
dh
ear
tfa
ilure
.
No
tsp
eci
fie
d.
90
7M
alay
sian
arm
of
AD
HER
E-In
tern
atio
na
l.St
ren
gth
s:M
ult
i-ce
ntr
etr
ial,
imp
rovi
ng
the
po
ten
tial
ge
ne
raliz
abili
tyo
fre
sult
s.A
llq
ue
stio
ns
on
the
ele
ctro
nic
case
rep
ort
we
rere
qu
ire
dto
be
com
ple
ted
,e
limin
atin
gre
po
rtin
gb
ias
du
eto
mis
sin
gd
ata.
Lim
itat
ion
s:D
isch
arg
ed
ata
wit
hla
cko
fst
and
ard
isat
ion
inth
ed
iag
no
sis
of
he
art
failu
re,
wh
ich
may
lead
tose
lect
ion
bia
s.
Ph
ilip
pin
es
[68
]‘
Re
tro
spe
ctiv
e2
00
6–
20
07
All
con
secu
tive
ind
ivid
ual
sad
mit
ted
wit
han
Inte
rnat
ion
alC
lass
ific
atio
no
fD
ise
ase
-9co
de
for
he
art
failu
re.
Pat
ien
tsw
ith
he
art
failu
rep
rim
arily
be
ing
tre
ate
das
aco
-mo
rbid
rath
er
than
pri
mar
yco
nd
itio
n.
Excl
usi
on
:P
atie
nts
,1
8y,
tho
sew
ith
ou
tan
acce
ssib
lem
ed
ical
reco
rd,
and
tho
sew
ith
ou
tac
ute
de
com
pe
nsa
ted
he
art
failu
re.
No
tsp
eci
fie
d.
26
1P
hili
pp
ine
sar
mo
fA
DH
ERE-
Inte
rnat
ion
al.
Stre
ng
ths:
Mu
lti-
cen
tre
tria
l,im
pro
vin
gth
ep
ote
nti
alg
en
era
lizab
ility
of
resu
lts.
All
qu
est
ion
so
nth
ee
lect
ron
icca
sere
po
rtw
ere
req
uir
ed
tob
eco
mp
lete
d,
elim
inat
ing
rep
ort
ing
bia
sd
ue
tom
issi
ng
dat
a.Li
mit
atio
ns:
Dis
char
ge
dat
aw
ith
lack
of
stan
dar
dis
atio
nin
the
dia
gn
osi
so
fh
ear
tfa
ilure
,w
hic
hm
ayle
adto
sele
ctio
nb
ias.
‘P
revi
ou
sly
un
pu
blis
he
dd
ata.
do
i:10
.13
71
/jo
urn
al.p
me
d.1
00
16
99
.t0
06
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 34 August 2014 | Volume 11 | Issue 8 | e1001699
Table 7. Included countries grouped by World Health Organization region.
Africa Americas Eastern Mediterranean Europe South East Asia Western Pacific
Algeria Argentina Egypt Romania India China
Cameroon Brazil Iran Turkey Indonesia Malaysia
DRC Chile Lebanon Serbia Thailand Philippines
Ethiopia Colombia Pakistan
Ghana Mexico Tunisia
Kenya Yemen
Mozambique
Nigeria
Senegal
South Africa
Uganda
DRC, Democratic Republic of the Congo.doi:10.1371/journal.pmed.1001699.t007
*Weighted by study size.doi:10.1371/journal.pmed.1001699.t008
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 35 August 2014 | Volume 11 | Issue 8 | e1001699
Table 9. Characteristics of patients, by country.
Region and Country Recruitment PeriodHeart FailureCases
Mean Age(Years)
Male(Percent)
Mean Lengthof Stay (Days)
Mean LVEF(Percent)
Africa
Algeria [70]‘ 2008–2009 400 64 60% — 49%
Cameroon [24] 1998–2001 167 57 59% — 23%
Cameroon [29] 2002–2008 462 43 57% 13
Democratic Republic of theCongo [32]
2003–2004 100 57 48% —
Ghana [30] 1992–1995 572 42 55% —
Nigeria [26] 2006–2008 340 51 51% — 42%
Nigeria [27] 2006–2010 475 49 50% —
Nigeria [22] 2004 102 45 31% —
Nigeria [28] Unspecified 177 52 51% — 45%
Nigeria [31] 2001–2005 423 54 57% —
Nigeria [36] 1995–2005 202 56 54% —
Senegal [38] 2001 170 50 — 11
South Africa [25] 2006 844 55 43% — 45%
Sub-Saharan Africa [35] 2007–2010 1,006 52 49% 9 40%
Americas
Argentina [21] 1996–1997 751 66 41% —
Argentina [43] 2002–2003 615 70 55% —
Argentina [44] 2007 736 — 59% —
Argentina [23] 1992–1999 6,368 77 65%‘ 5
Brazil [39] 2006–2008 166 61 51% — 49%
Brazil [40] 2001 203 67 50% 8*
Brazil [42] 1998–2000 494 58 70% — 34%
Brazil [45] 1992–2010 194,098 — 51% 10
Brazil [46] Unspecified 100 59 56% 9 46%
Brazil [19] 2005–2006 263 60 63% 25 27%
Brazil [59] Unspecified 383 54 53% —
Brazil [66] 1997 100 57 76% — 43%
Brazil [67] 2008 144 61 54% —
Brazil [65] 1995 903 53 60% —
Chile [41] 2002–2004 372 69 59% 11 35%
Chile [70]‘ 2008–2009 199 65 55% — 42%
Colombia [70]‘ 2008–2009 211 70 86% — 46%
Mexico [70]‘ 2008–2009 458 68 43% — 54%
Eastern Mediterranean
Egypt [70]‘ 2008–2009 434 58 66% — 55%
Iran#,‘ 1998–2012 277 67 — 5
Iran [70]‘ 2008–2009 105 57 77% — 34%
Lebanon [70]‘ 2008–2009 181 69 61% — 43%
Pakistan [47] 2002–2003 196 61 65% —
Tunisia [70]‘ 2008–2009 257 67 51% — 53%
Yemen [48] 2007–2008 100 58 65% —
Europe
Romania [50] 2008–2009 3,224 69 56% — 38%
Romania [51] 2006 459 61 86% —
Serbia [61] Unspecified 127 71 73% — 40%
Turkey [49] 1997–1998 661 61 64% — 38%
Turkey [63] 2005 320 — 40% —
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 36 August 2014 | Volume 11 | Issue 8 | e1001699
Table 9. Cont.
Region and Country Recruitment PeriodHeart FailureCases
Mean Age(Years)
Male(Percent)
Mean Lengthof Stay (Days)
Mean LVEF(Percent)
Turkey [64] 1998–2000 876 64 48% —
South East Asia
India [69]‘ 2008–2012 5,758 50 66% 3
Indonesia [20] 2006 1,687 60 65% — 33%
Thailand [52] 2006–2007 1,612 64 50% —
Western Pacific
China [53] 1995–2009 1,119 65 71% — 38%
China [54] 2008–2009 206 74 56% —
China [55] 2007 478 69 47% —
China [56] 1995–2004 259 70 63% 29
China [57] 1980–2000 1,756 68 56% 35
China [58] 1980–2008 2,458 71 52% 13
China [60] Unspecified 327 — 78% — 57%
China [62] 2008 529 — 30% —
Malaysia [68]‘ 2007–2008 907 61 69% —
Philippines [68]‘ 2006–2007 725 53 55% —
‘Previously unpublished dataset.*Contributed by author.#S. Rahimzadeh, F. Farzadfar F, and M. Ghaziani, unpublished data.doi:10.1371/journal.pmed.1001699.t009
Table 10. Reported causes of heart failure, by region.
PLOS Medicine | www.plosmedicine.org 39 August 2014 | Volume 11 | Issue 8 | e1001699
73. Moscavitch S-D, Garcia JL, Rosa LF, Pestana PR, Moraes LV, et al. (2009)
Insuficiencia cardıaca: estarao as diretrizes incorporadas na rede de cuidadosprimarios? Rev Port Cardiol 28: 683–696.
74. Brazil Minister of Health (2014) Datasus [database]. Available: http://www2.
datasus.gov.br/DATASUS/index.php. Accessed 7 December 2013.75. Sliwa K, Wilkinson D, Hansen C, Ntyintyane L, Tibazarwa K, et al. (2008)
Spectrum of heart disease and risk factors in a black urban population in SouthAfrica (the Heart of Soweto Study): a cohort study. Lancet 371: 915–922.
(2005) Characteristics and outcomes of patients hospitalized for heart failure in
the United States: rationale, design, and preliminary observations from the first100,000 cases in the Acute Decompensated Heart Failure National Registry
(ADHERE). Am Heart J 149: 209–216. doi:10.1016/j.ahj.2004.08.00578. Khatibzadeh S, Farzadfar F, Oliver J, Ezzati M, Moran A (2012) Worldwide risk
factors for heart failure: A systematic review and pooled analysis. Int J Cardiol
168: 1186–1194. doi:10.1016/j.ijcard.2012.11.065
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 40 August 2014 | Volume 11 | Issue 8 | e1001699
Background. A healthy heart pumps about 23,000 liters ofblood around the body every day. This blood deliversoxygen and nutrients to the rest of the body and carriescarbon dioxide and waste products away from the tissuesand organs. A healthy heart is therefore essential for life.Unfortunately, many people (particularly elderly people)develop heart failure, a life-threatening condition in whichthe heart no longer pumps enough blood to meet all thebody’s needs because it has become too weak or too stiff towork properly. Heart failure can affect the left, right, or bothsides of the heart, and it can develop slowly (chronic heartfailure) or quickly (acute heart failure). Its symptoms includeswelling (edema) of the feet, ankles, and legs, tiredness, andshortness of breath. Heart failure, which is most commonlycaused by coronary heart disease (blockage with fattydeposits of the blood vessels that supply the heart) or highblood pressure (hypertension), cannot be cured. However,lifestyle changes (for example, losing weight and avoidingsalty food) and various medications can control heart failureand improve the quality of life of patients.
Why Was This Study Done? In high-income countries(HICs), heart failure is a common condition that typicallyconsumes 1%–2% of healthcare resources. Experts believethat heart failure may soon become a major public healthissue in low- and middle-income countries (LMICs) becausefewer people are dying of infectious diseases in thesecountries than in the past. LMICs need to plan for thiseventuality, but little is known about the current burden ofheart failure in LMICs. Here, the researchers undertake asystematic review and meta-analysis of published andunpublished information on the presentation, causes, man-agement, and outcomes of heart failure in LMICs. Asystematic review uses predefined criteria to identify all theresearch on a given topic; a meta-analysis uses statisticalapproaches to combine the results of several studies.
What Did the Researchers Do and Find? The researchersidentified 49 published studies and four unpublisheddatabases that provided information on nearly 240,000hospitalizations for acute and chronic heart failure in 31LMICs. Across these LMICs, the average age of patientsadmitted to hospital for heart failure was 63 years, more thanten years younger than the average admission age in HICs.Differences in mean age at presentation, which ranged from42 years in Cameroon and Ghana to 75 years in Argentina,largely correlated with the human development index (ameasure of national well-being) of individual LMICs. Notably,acute heart failure accounted for 2.2% of all hospitaladmissions in the LMICs for which data were available.Hypertension was the main cause of heart failure in Africaand the Americas, whereas ischemic heart disease was themain cause in all other regions. More than two-thirds ofpatients were prescribed diuretics for heart failure, whereasonly 57% of patients were treated with angiotensin-
converting enzyme inhibitors, only 34% were treated withbeta-blockers, and only 32% were treated with mineralocor-ticoid receptor antagonists, the three treatments currentlyrecommended in guidelines for managing heart failure.Finally, on average, patients admitted to hospital for heartfailure in LMICs spent ten days in hospital, and 8.3% of themdied in hospital (compared to 6.7% and 4% of similarpatients across Europe and the US, respectively).
What Do These Findings Mean? These findings showthat the presentation, causes, management, and outcomesof heart failure vary substantially across LMICs. Importantly,however, these findings reveal that heart failure is already amajor burden in LMICs and that the use of recommendedmedications for heart failure is currently suboptimal in thesecountries. Because the studies included in this systematicreview and meta-analysis set out to answer different researchquestions and used different methods to diagnose heartfailure, the estimates of the burden of heart failure in LMICsprovided here may not be completely accurate. Moreover,because the data were derived mainly from urban tertiaryreferral hospitals, these findings may not reflect the broaderpicture of heart failure in the community in LMICs. However,although additional studies are needed to completely assessthe burden of heart failure in LMICs, the present findingsnevertheless highlight the need to implement betterstrategies for the management of heart failure in LMICs.
Additional Information. Please access these websites viathe online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1001699.
N This study is further discussed in a PLOS MedicinePerspective by Druin Burch
N The US National Heart, Lung, and Blood Institute providesinformation for patients about heart failure
N The UK National Health Service Choices website providesinformation about all aspects of heart failure
N The American Heart Association, a not-for-profit organiza-tion, also provides detailed information about heart failurefor patients and their carers
N The British Heart Foundation, a not-for-profit organization,provides additional information about heart failure,including a personal story about heart failure; furtherpersonal stories about heart failure are provided by thenot-for-profit organization Healthtalkonline
N Heart Failure Matters provides practical information aboutheart failure for patients, families, and caregivers in severallanguages; its website includes an animated journeythrough heart failure and several personal stories aboutthe condition
N MedlinePlus provides links to further resources about heartfailure (in English and Spanish)
Heart Failure in Low- and Middle-Income Countries
PLOS Medicine | www.plosmedicine.org 41 August 2014 | Volume 11 | Issue 8 | e1001699