Heather A. Flynn, PhD Associate Professor & Vice Chair for Research Department of Behavioral Sciences and Social Medicine FSU College of Medicine Adjunct Associate Professor, University of Michigan Medical School Department of Psychiatry
Transcript
Heather A. Flynn, PhD Associate Professor & Vice Chair for Research
Department of Behavioral Sciences and Social Medicine FSU College of Medicine
Adjunct Associate Professor, University of Michigan Medical School Department of Psychiatry
Not treating perinatal depression in the US is not an option
Burden and costs of depression and treatment What do we know about effective interventions? Gaps in the field What do we know about what works?
Cause DALYs
1. HIV / AIDS 32,871
2. Unipolar Depressive Disorders 30,086
3. Cataracts 9,295
4. Tuberculosis 9,163
total US economic burden of depression in 2000 has been estimated to be $83.1 billion Due to cost associated with medical care, direct
depression treatment, suicide costs and workplace costs (>$12 billion for health care costs to employers)
Full remission of depression has been associated with drastic improvement in Quality Adjusted Life Years
Equal to an estimate of $19,564 to $39,128 per quality-adjusted life year gained.
One study found that patients are willing to pay more
than the actual care of depression treatment and about the same as other medical conditions.
Components of Collaborative Care: a) accompanied by organizational enhancements of care, b) involving clinician education, c) support from case managers or a collaborative care approach between specialists and primary care physicians, d) systematic monitoring / follow up of outcome
Depression is a chronic, recurrent illness: Life course - untreated
(Stressors designated by arrows)
Meets criteria for Major Depressive Disorder
Ages: Child-Adolescent Adult Older
Most individuals with depression in the world are female: Depression is twice as common in women worldwide; 1 in 4 will be depressed over the lifespan; up to 80% remain untreated; accounts for more disability worldwide than most other illnesses
Reasons for sex differences in prevalence are not known Improved understanding of, detection and intervention
for women across the lifespan will impact the illness for men and women: Depression around childbearing is a high risk period for the mother as well as high risk for male and female offspring – Key prevention opportunity for reducing burden of depression
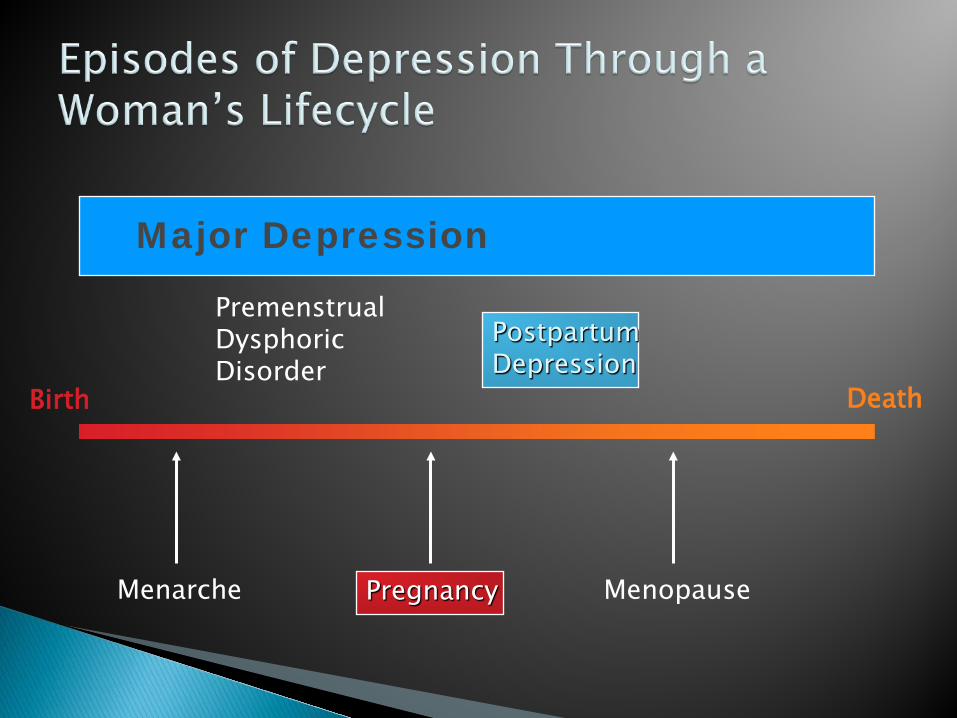
Menarche Pregnancy Menopause
Premenstrual Dysphoric Disorder
Postpartum Depression
Major Depression
Birth Death
Proper Detection
Receipt of patient-centered, effective treatment
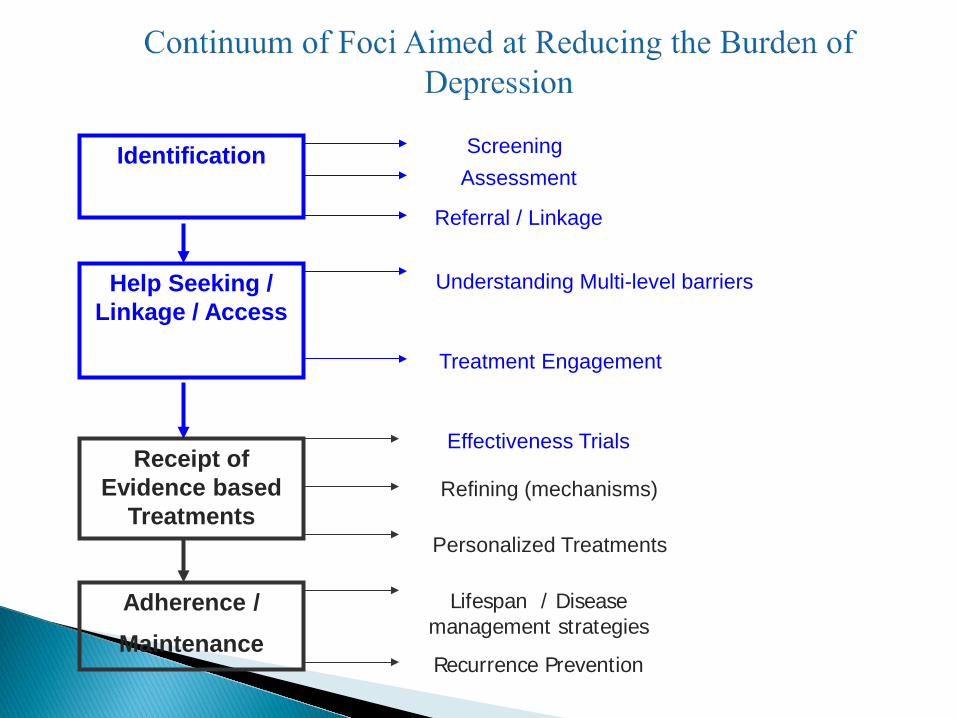
Identification
Help Seeking / Linkage / Access
Receipt of Evidence based
Treatments
Adherence / Maintenance
Screening Assessment
Referral / Linkage
Understanding Multi-level barriers
Treatment Engagement
Effectiveness Trials
Personalized Treatments
Lifespan / Disease management strategies
Recurrence Prevention
Refining (mechanisms)
Depression and related disorders are highly prevalent around time of childbearing
Considered the most common complication of pregnancy
Maternal depression, stress, trauma linked to poor infant and child outcomes in multiple domains – Key Prevention opportunity
Most women in the US seek prenatal care; most depressed individuals do not seek specialty mental health / psychiatry care
Depression in Pregnancy 14%1 Postpartum Depression 10%-15%,
cross-culturally2 Postpartum Blues 50%-85%3 Postpartum Psychosis 1-2/10003
1. Evans J, et al. BMJ. 2001;323:257-260; 2. O’Hara M, Swain A. Int Rev Psychiatry. 1996;8(1):37-54. 3.Gale & Harlow. J Psychosom Obstet Gynaecol. 2003;24(4):257-66
Anxiety, obsessiveness regarding infant safety, dystonic thoughts of infant harm, fear of returning to work
No different from age matched non-childbearing women (O’Hara et al., 1990; AHQR, 2005)
13% cross-culturally (O’Hara & Swain, 1996) Higher rates found using: ◦ Self-report symptom measures ◦ Longer assessment periods (12 month period prevalence
= 30%) ◦ Lower SES women - 25% (structured interviews) to 47%
(self report)
Perinatal depression persists into the PP period, even up to 4 years
It is particularly debilitating for the infant health and development in the first year postpartum
Women with perinatal depression have been found to use greater medical care services than non-depressed women
Some studies found higher use of pediatric emergency services and less well child care thank non depressed women (Flynn et al, 2004)
One study of 817 new mothers showed that depressed women incurred 90% health care expenditures as compared to non-depressed women (Dagher et al. 2012).
Improvement of Depression Care has been shown to be related to significantly improved functioning, less absenteeism and greater work productivity
Pregnancy and the Intrauterine environment are crucial for risk of development of hypertension, diabetes, coronary heart disease, metabolic disorders, pulmonary, renal and mental illnesses lifelong for the child.
Depression and anxiety in pregnancy are among the most common and impactful
Low birth weight, premature delivery, and small for gestational age infants (Steer et al., 1992; Kelly et al. 2002, Hoffman et al., 2000)
Weight loss associated with depression-fetal growth (Wisner et al. 1999)
Pre-eclampsia (Kurki et al, 2000) Elevated cortisol, reduced dopamine in neonates
(Lundy et al., 1999) Increased fetal activity and infant
neurobehavioral dysregulation (Field et al., 2006; Dieter et al., 2001)
Inadequate prenatal care (Kelly et al., 1999) Risk for postpartum depression (Beck, 2001)
less affectionate and responsive to infant cues (Broth, Goodman, Hall, Raynor, 2004)
problems with breastfeeding (Field, Hernandez-Reif, & Feijo, 2002)
infant irritability (Zuckerman et al., 1990)
delayed linguistic and cognitive development (Alpern & Lyons-Ruth, 1993; Leadbeater & Bishop, 1994)
inadequate preventive care (Leiferman, 2002) greater use of Pediatric ED and missed
outpatient pediatric appointments (Flynn et al, 2004)
High incidence, peak prevalence Opportunity for prevention of risk to next
generation Often early or first episode Identifiable risk factors ◦ prior history of mood disorder, socioeconomic
disadvantages, inadequate social support, high levels of stress / anxiety
Prime time for contact with medical care system and (?) openness to health-related information
National Academy of Science (NAS) and Institute of Medicine (IOM) report: Depression in Parents, Parenting, and Children
American Psychiatric Association and American College of Obstetricians and Gynecologists – Report on Management of Depression in Pregnancy
National Institute of Health – Office of Research on Women’s Health; NIMH Perinatal Research Strategic Plan; Report of Neurodevelopment
Surgeon General’s Women’s Mental Health Project Perinatal Depression Information Network Health Resources and Services Administration Bright Futures
Project State and Federal Law and Policy focused on Addressing
Postpartum Depression
Medications Psychotherapy (CBT, IPT) adapted for perinatal and
home visitation Mindfulness and Yoga Circadian (light), Sleep and exercise Centering / Peer support
RISK OF UNTREATED MATERNAL
ILLNESS
RISK OF FETAL
EXPOSURE
CASE-BY-CASE DECISION
Two major goals: Depression / distress symptom remission Improve interpersonal functioning
Resolving acute interpersonal crisis Increasing social support
12-16 Sessions (Initial, Middle and End/ Transition Phases)
Complicated Grief Interpersonal Role Conflict / Dispute Interpersonal Role Transition Interpersonal sensitivity
(CBT) targets negative (depression maintaining) thoughts and behaviors that tend to worsen depressed mood and teaches ways of thinking and behaving that work better.
CBT is structured and involves weekly homework Work is focused on the link between depression
maintaining thoughts, mood and behavior
Overall purpose of BA 1) determine patterns of behaving and coping that worsen depression and 2)develop plan for increasing access to more “reinforcing” experiences
Among more severely depressed patients, behavioral activation comparable to antidepressant medication, and to cognitive therapy (Dimidjian et al., 2006)
How do we detect, intervene and improve outcomes? Engagement is key
Most persons with depression do not present to Mental Health – but to primary care (ob/gyn)
Physicians CANNOT typically tell by looking at
someone and asking a few questions if they have MDD Many women do not “act” depressed Screening tools greatly improve detection accuracy but
are not perfect – follow up assessment is necessary
Several user-friendly measures: ◦ Edinburgh Postnatal Depression Scale (EPDS)1 10-items, range 0-30, 3min ◦ Beck Depression Inventory (BDI-II) 2 21-items, range 0-63, 6min ◦ Postpartum Depression Screening Scale (PDSS)3
35-items, range 1-175, 10min
Cox JL, et al. Br J Psychiatry. 1987;150:782-786; 2. Beck, A. T., Steer, R. A., & Brown, G. K. (1996). BDI-II manual. San Antonio: The Psychological Corporation. 3. Beck, C. T., Gable, R. K. Nursing Research. 2000:49, 272–282.
Approximately 75% of women with known or likely depression are not detected or treated
Spitzer et al. 2000 – 3,000 with PRIME MD Kelly et al., 2001 – 186 with PRIME MD Marcus et al., 2003 – 3,472 with CESD > 16 Flynn et al., 2005 –276 with CESD > 16 Smith et al, 2004 – 387 with PRIME and MINI
24% depression risk and interviewed (n=274)
78% of high risk = no treatment
17% current MDD (n=46)
48% (n=22) of MDD any treatment
Of MDD treated, 13% (n=6) receiving “adequate” treatment
Flynn et al., 2006
Engagement
Detection
Diagnosis
Treatment
Symptom improvement
Improved outcomes (e.g. function, parenting, well-being, quality of life, health,
Not able to address key questions from the literature review: Few high-quality studies comparing screening to no screening Lack of evidence for any benefit associated with detecting
symptoms of depression that together do not meet criteria for a diagnosis of major depression
Patient characteristics in studies which do not reflect the diversity of the U.S. population of pregnant and postpartum women
Lack of evidence for an impact of screening and treatment of depression on longer term maternal and infant outcomes
Biggest barriers to synthesizing this literature is the diversity in research methods, definitions, and analytic tools used.
Perinatal depression treatment studies show high attrition (up to 2/3)
Miranda et al., 2003 - psychologists spoke with patients a mean (SD) of 10.2 (12.2) times before they attended a psychotherapy visit
One year outcomes: 36% assigned to psychotherapy received 6 or more CBT sessions (Miranda et al., 2006)
The common referral process of providing a listing of contact information for mental health services, necessitating women to navigate insurance coverage and therapist availability, presents multiple obstacles.
lack of knowledge about depression, need for normalization of symptoms, stigma/trust issues and logistical barriers are important influences on perinatal depression treatment
A tailored, active referral process with ongoing monitoring may be more effective. An integrated care model with mental health clinicians available for individualized,
brief consultation on site may serve to facilitate treatment. Contemplating treatment for depression is a complex, emotionally taxing process
that may threaten their views of themselves as mothers. Therefore, the process of communicating normalizing, non-stigmatizing
depression information, using the patients own language initially in a way that emphasizes positive benefits to both mother and infant may be critical in determining whether women will follow through with treatment referrals or not.
Flynn et al., GHP, 2010
Can this person
help me?
Feeling heard
(non-judgmental, autonomy)
Trust Clinician
Clear Communication about treatment
Perception of Expertise
Anticipation, normalization and individualized planning for follow up challenges (unable to reach, missed visits) ◦ Alleviated anxiety of outreach staff
• Use of Motivational Interviewing at first contact
o elicitation of importance of treating depression, participant articulation of commitment to follow through, including strategies to keep appointments (Flynn, CBP 2009)
• Dedicated outreach staff making regular contact with participants at regular intervals. Offers to assist with selected needs (such as connecting with ob clinic staff).
• Several additional contacts and permissions • Ongoing communication with and use of prenatal care setting
Engaging low income women with MDD in psychotherapy is complex and challenging
Canceled and rescheduled sessions are the norm ◦ “Frontload” engagement, alliance and psychotherapy in
session 1-4 Treatment focus must be clearly relevant to the
woman in the face of multiple competing demands and psychosocial stressors and barriers – maintain focus on symptoms and functioning
Dedicated outreach staff, coordination with obstetrics is critical
Combination medication is probably needed, but high levels of patient (and clinician? ) ambivalence; Recurrent MDD requires higher intensity treatment
Screening Feedback and Referral (Standard Care?) Psychoeducation and addressing barriers Motivational Interviewing ◦ Hundreds of studies showing improved engagement and
adherence ◦ Highly patient-centered with attention to values, and the
language / communication within the patient-clinician interaction ◦ Can be done very briefly ◦ Requires training
Effective training, attention to work flow processes, and available consultation (Miller et al., 2009)
Explaining the diagnosis in culturally congruent, easy to understand language; Explaining treatment options and recommendations; Eliciting and addressing patients’ reactions, concerns, treatment preferences; Delivering and explaining self-care kits; Introducing an on-site behavioral health specialist (Miller et al., 2012)
“Arguments regarding expanded access to effective mental health treatment have often been framed in terms of cost savings or cost offset. Unfortunately, this argument often cloaks a discriminatory assumption that effective mental health care is justifiable only if it reduces overall health care expenditures. We do not believe that expenditures for treatment of other major health conditions are held to such a standard. When judged by a more appropriate yardstick that includes improvements in health as well as dollars spent, improved depression treatment compares favorably with other uses of health care resources.”
AHRQ review (2005, 2013) Hewitt & Gilbody, 2009 Primarily due to the poor quality and
methodological inconsistencies between and among studies
But >15 years of analogous work in PC has shown clear benefit.
Not treating depression in pregnancy or postpartum is not an option!
Most women receive inadequate treatment Treatment adherence and outcomes are poor
Integrated care ◦ Mental health providers are linked with primary care providers via co-
location, common medical records, team meetings, etc. Collaborative care ◦ Patient is cared for by a multidisciplinary team; each team member has a
specific role Stepped care ◦ Matches intensity of treatment and resources to severity and complexity
of illness Self care ◦ Actively engages patient in managing illness and maintaining health
Meta-analysis1 shows that these models improve ◦ quality of care ◦ patient and provider satisfaction ◦ clinical outcomes
1. Neumayer-Gromen et al: Med Care 42:1211-1221, 2004
Screening – Figure out how to optimize effectiveness (properly designed studies)
Assessment – training for front line professionals in psychiatric assessment
Attention to clinician communication style best suited to each individual patient
Patient education about illness and treatment (if needed) Menu of intervention and treatment options Assessment of motivation and follow through influences Planned monitoring and support All of the above must be customized to communities and
cultures Must be cost effective for sustainability