25
HEENT EMERGENCIES
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | nigel-cross |
| View: | 219 times |
| Download: | 3 times |

HEENT EMERGENCIES

A 52yo M presents w/ nasal bleeding for 4hrs. PMHx is HTN. There is no clear source of bleeding, and an anterior pack does not stop
the bleeding. BP=160/90. What is the most appropriate management?
• Insert a posterior pack & d/c the pt w/ close follow-up
• Keep the anterior packing in place and discharge on antibiotics. Arrange close follow-up
• Pack posteriorly, and if bleeding is controlled admit to ICU. Arrange urgent ENT consultation
• Lower her blood pressure to 120 mmHg systolic in order to control this bleeding

What is the most common organism causing acute otitis media in a 10 year old?
• Moraxella catarrhalis
• Haemophilus influenza
• Staphylococcus aureus
• Streptococcus pneumoniae

A 14yo F complains of R ear pain after being slapped on the side of her head. Exam reveals a perforation
of the anterior aspect of the TM. There is no bleeding. Which of the following is true?
• Topical abx should be prescribed to prevent middle ear infection
• Emergent ENT consultation should be obtained
• The pt should be advised to keep water out of the ear
• Daily cleansing of the ear w/ H2O2 drops & a cotton swab should be performed

A 67yo male w/ IDDM presents w/ swelling, pain, & drainage from his R ear. He presented 6d earlier w/ similar complaints & was started on antibiotic ear drops. He has a T 39C, & states his ear pain & drainage are worse. The best course of action is:• Admit with ENT consultation, along with steroid ear drops
• Admit with urgent ENT consultation, as well as begin IV antibiotics active against Pseudomonas
• Encourage outpatient follow-up while continuing the ear drops
• Switch to another abx drop, add PO abx & follow-up w/ ENT in wk

A 50yo M presents w/ pain & tenderness in the R submandibular area and is able to feel a small "bump" on the floor of his mouth. A small stone can be palpated in the area of the duct. Which of the following is true concerning the tx?
• Salivary gland secretions should be minimized with a bland diet
• X-rays are of rare value• Elder patients present with this most frequently
• Attempts should be made to “milk” the stone out of the duct. If this is unsuccessful, refer to the ENT office for incision or dilation of the duct
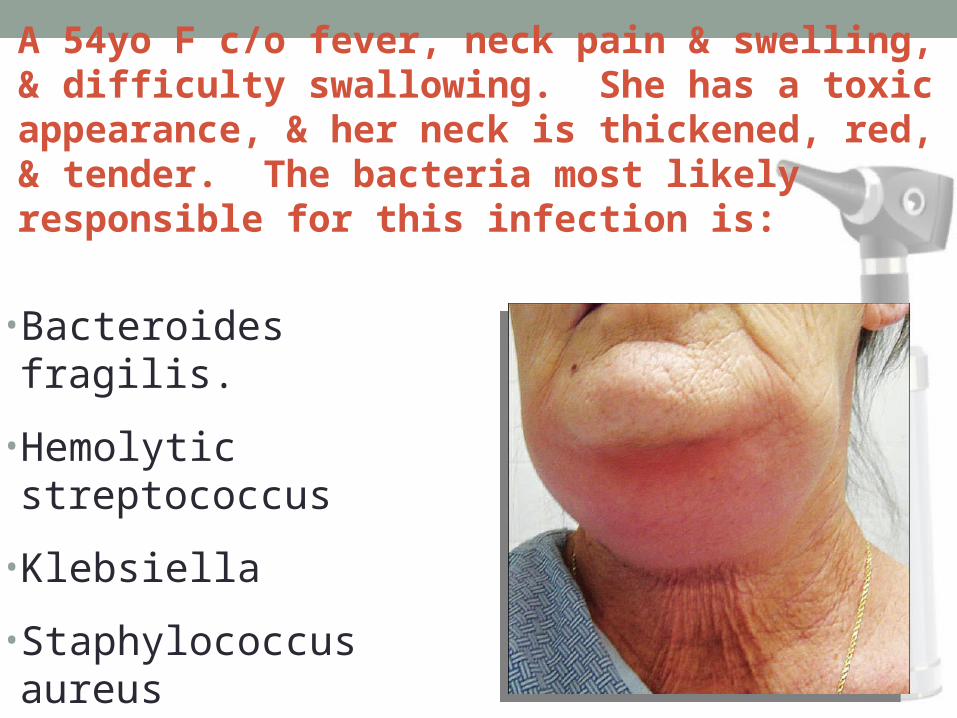
A 54yo F c/o fever, neck pain & swelling, & difficulty swallowing. She has a toxic appearance, & her neck is thickened, red, & tender. The bacteria most likely responsible for this infection is:
• Bacteroides fragilis.
• Hemolytic streptococcus
• Klebsiella
• Staphylococcus aureus

You are examining a 4 yo F who knocked out her two upper central incisors in a fall. She is visiting friends, who do not know whether these are her primary teeth. You know that:
• Normal primary dentition consists of 12 mandibular & 12 maxillary teeth.
• The upper central incisors are the first teeth to erupt at approximately 10 months of age
• All primary teeth should be present by 3 years of age.
• Permanent dentition doesn’t begin to erupt until 7yrs of age.

A 19yo F c/o severe mouth pain 4d after removal of 2 impacted mandibular molars. She looks very uncomfortable, but has normal vital signs. Her exam shows probable dry sockets. You can offer her best relief by:
•packing the socket with gauze impregnated with penicillin.•packing the socket with gauze soaked in 4% lidocaine.•packing the socket with gauze soaked in eugenol (oil of cloves).•suturing the gum over the exposed socket.

A 10yo M was struck in the mouth and has a chipped tooth. The missing fragment is soaking in milk. You examine the fragment & see a central drop of blood. You should now:
• arrange urgent follow-up with dentist or endodontist.
• pack the pocket with gauze soaked in 4% lidocaine.
• pack the pocket with gauze soaked in eugenol (oil of cloves).
• glue the fragment back into place using cyanoacrylate glue.
A 29yo camper avulsed his upper medial incisor 2 hrs ago. He put his teeth into his pocket, and drove to see you. You need to:• gently rinse the teeth and
reimplant them, as there is an excellent chance they will take
• gently rinse the teeth & reimplant them, but refer to an endodontist & warn him that the teeth will probably not survive
• scrub the teeth to remove contaminants, then reimplant them
• soak the teeth in a sterilizing solution and call the dentist

The most common complication of acute otitis media is:
•bacteremia•hearing loss•mastoiditis•meninigitis

Which of the following is true regarding epistaxis?
• Anterior epistaxis accounts for 25% of cases
• Anterior epistaxis usually arises from a posterior branch of the sphenopalatine artery
• The incidence decreases with age
• It is more common in warmer seasons and southern climates
If a permanent tooth cannot be immediately reimplanted, the best transport medium is:
• a. Saliva
• b. Milk
• c. Water
• d. Hank’s solution
For Sale: Tooth pouch for over the top parents
The sources for most causes of posterior epistaxis is:
• Sphenopalatine artery
• Anterior ethmoidal artery
• Posterior ethmoidal artery
• Kiesselbach’s plexus
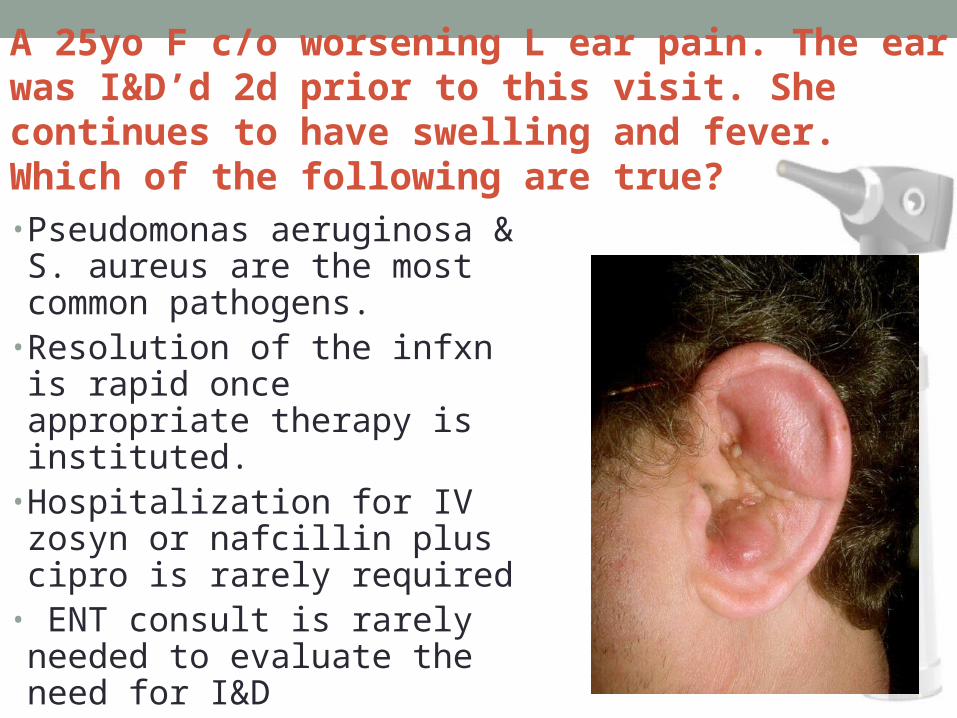
A 25yo F c/o worsening L ear pain. The ear was I&D’d 2d prior to this visit. She continues to have swelling and fever. Which of the following are true?
• Pseudomonas aeruginosa & S. aureus are the most common pathogens.
• Resolution of the infxn is rapid once appropriate therapy is instituted.
• Hospitalization for IV zosyn or nafcillin plus cipro is rarely required
• ENT consult is rarely needed to evaluate the need for I&D
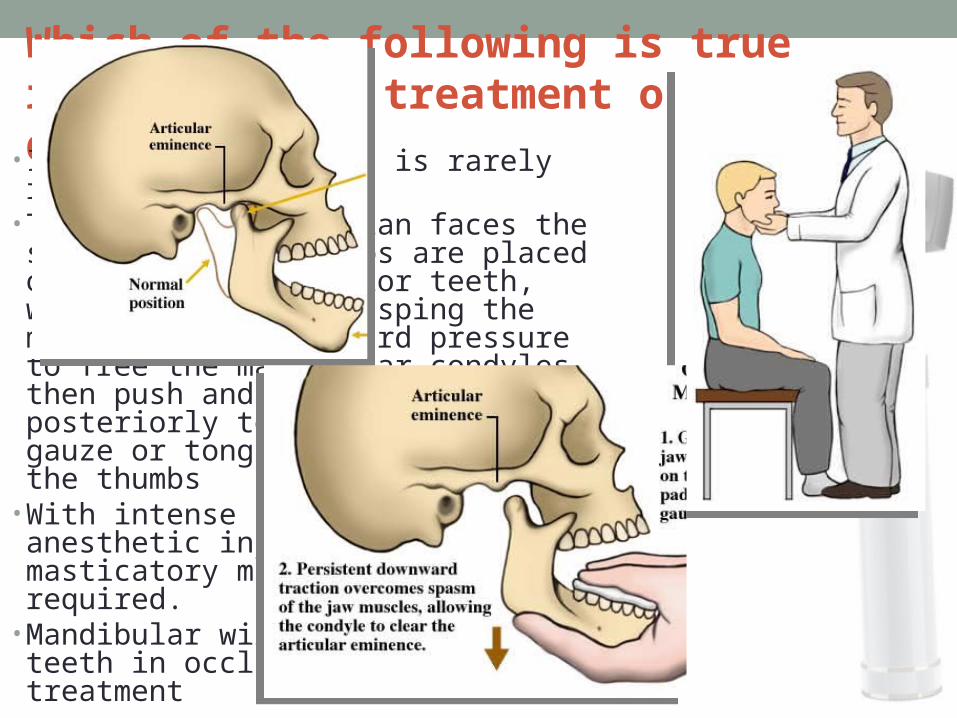
Which of the following is true regarding the treatment of TMJ dislocation:
• Intravenous sedation is rarely required• The standing physician faces the seated pt; the thumbs are placed on the lower posterior teeth, with the fingers grasping the mandible. Use downward pressure to free the mandibular condyles, then push and rotate the mandible posteriorly to reduce it. Use gauze or tongue blades to protect the thumbs
• With intense spasm, local anesthetic injection of the masticatory muscles may be required.
• Mandibular wiring to hold the teeth in occlusion is definitive treatment

In infants less than 12wks old w/ otitis media & conjunctivitis or afebrile pneumonia, consider __ as the cause.
• Mycoplasma
• C. trachomatis
• S. pneumoniae
• S. aureus or gram-negative enteric organisms

The most reliable sign of acute otitis media is :
• Retraction of the tympanic membrane
• Purulence behind the tympanic membrane
• Loss of TM mobility
• Bulging of the tympanic membrane
Antibiotic options for AOM that cover beta-lactamase producing H. influenzae and B. catarrhalis include all of the following EXCEPT:
• A. TMP/SMX, 8 and 40 mg/kg divided BID
• B. Pediazole (erythro + sulfisoxazole), 50 mg/kg divided QID to a max of 2 g/day
• C. Dicloxacillin, 40 mg/kg divided TID
• D. Augmentin, 45 mg/kg/day BID

Which of the following must be ruled out in a 2yo child with edematous, bluish-red gingivae?
• Dilantin hyperplasia• Leukemia• Pyogenic granuloma• Systemic lupus erythematosus
(SLE)• Thrombotic thrombocytopenic
purpura (TTP)
Gums of a child with leukemia after atomic bomb explosion

From medial to lateral or distal, all of the following are the correct type & # of teeth in each quadrant of the adult mouth EXCEPT:
• 1 central incisor• 1 lateral incisor• 1 canine or cuspid• 1 premolar• 3 molars (3rd molar is known as the "wisdom tooth" &
commonly doesn't erupt until adulthood.)
There are 2 premolars per quadrant
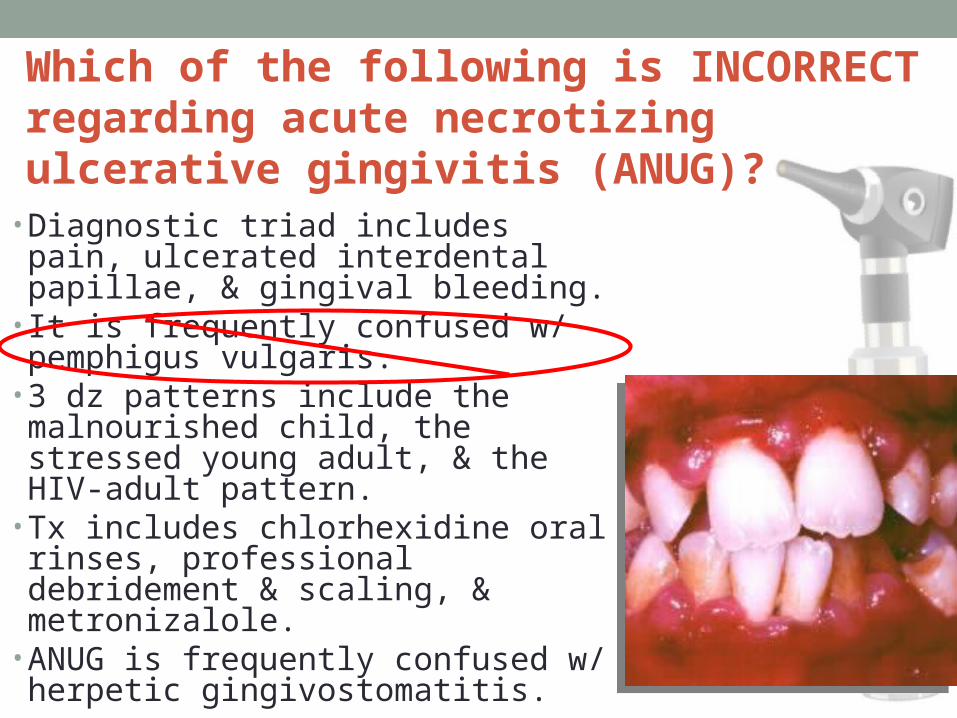
Which of the following is INCORRECT regarding acute necrotizing ulcerative gingivitis (ANUG)?
• Diagnostic triad includes pain, ulcerated interdental papillae, & gingival bleeding.
• It is frequently confused w/ pemphigus vulgaris.
• 3 dz patterns include the malnourished child, the stressed young adult, & the HIV-adult pattern.
• Tx includes chlorhexidine oral rinses, professional debridement & scaling, & metronizalole.
• ANUG is frequently confused w/ herpetic gingivostomatitis.
A 19 yo M involved in a fight has suffered a 3 cm gaping intraoral lac. All of the following are true regarding management EXCEPT:
• Irrigate, debride, & close any mucosal lacs using 4-0 absorbable sutures.
• With through-&-through injuries, repair the intraoral aspect first, then use a new sterile setup to do the outside.
• All puncture wounds should be repaired.• Repair of dental & bony structures should precede soft tissue repair.
• Tetanus prophylaxis

The End

















