28
HELIOS Klinikum Erfurt HELIOS Klinikum Erfurt LINC 2015 Embolization treatment for acute gastrointestinal bleeding S. Basche

HELIOS Klinikum Erfurt
HELIOS Klinikum Erfurt
LINC 2015
Embolization treatment for
acute gastrointestinal
bleeding
S. Basche

HELIOS Klinikum Erfurt LINC 2015
GIB
Upper GIB
Ulcus
Varicosis
Mallory-Weiss-S
Cancer
Oesophagus
Gaster
Duodenum

HELIOS Klinikum Erfurt LINC 2015
GIB
Prognosis
- 80% of GI- bleedings suspend spontaneous
- 20% recidivate within 3 days after therapy
- Emergency operation up to 50 % (Mortality)

HELIOS Klinikum Erfurt LINC 2015
GIB
Category Activity of bleeding
Rezidiv bleeding
I Ia Ib II IIa IIb IIc III
Acute hemorrhage Spurting hemorrhage Oozing hemmorrhage Recent hemorrhage Visible vessel Adherent clot Hemantin on ulcer base Lesions without signs of
recent hemorrhage
90% 30%
50 – 100% 20 – 50%
< 5%
< 5%
Forrest classification

HELIOS Klinikum Erfurt LINC 2015
Recurrence bleeding (high risk)
• Depending on:
– Forrest Ia/Ib 55%
– Forrest II 14 - 36%
– ulceration size > 1cm
– Localisation (posterior wall)
– Age
– Comorbidities and drugs (anticoagulation)

HELIOS Klinikum Erfurt LINC 2015
Upper GIB
23 Pat. with duodenal bleeding
I. Langner et al. Emerg Radiolog. 2008
Coiling operativ
Ulcus duodenale 8 10
Pancreatitis 1 2
Unknown 2 0
secondary hemorrhage 3 2
Ischemia 0 0
Mortality 3 2

HELIOS Klinikum Erfurt LINC 2015
GIB
n 69
Vessel n Coil Glue C + G Recurrence Comp.
A.
gastroduo.
56 32 9 15 6 0
SMA 4 0 4 0 0 1
A. lienalis 8 4 0 4 0 0
A. gastrica 1 0 1 0 0 0
Personal results, 2012

HELIOS Klinikum Erfurt LINC 2015
„blind TAE“
• It means:
– Patient after endoscopic therapy and high risk
for recurrence bleeding
– 28 patients
– technical success 100 %
– recurrence bleeding 2/28
Dr.med. Juliane Huber (2014)

HELIOS Klinikum Erfurt LINC 2015
GIB
Lower GIB
Tumor
Polyposis
Meckel - Divertikel
Divertikulitis
Morbus Crohn
Colitis Ulcerosa
Angiodysplasie
Infarct / Embolie
Duodenum
Jejunum
Ileum
Colon
Rectum
HELIOS Klinikum Erfurt LINC 2015
GIB
Symptoms
Haematemesis
Melaena
Haematochezie
HELIOS Klinikum Erfurt LINC 2015
Lower GIB
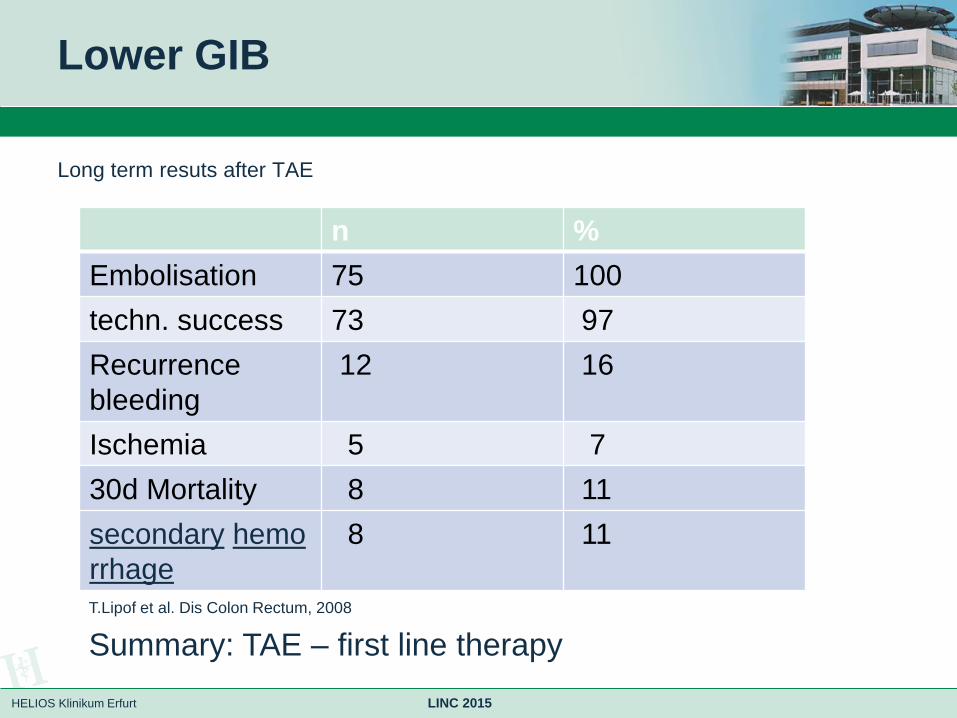
Long term resuts after TAE
n %
Embolisation 75 100
techn. success 73 97
Recurrence
bleeding
12 16
Ischemia 5 7
30d Mortality 8 11
secondary hemo
rrhage
8 11
T.Lipof et al. Dis Colon Rectum, 2008
Summary: TAE – first line therapy

HELIOS Klinikum Erfurt LINC 2015
Case 1
Patient: f; 75 y
• severe GIB after clipping in duodenal ulcer
• Therapy:
Embolisation with Histoacryl / Lipiodol

HELIOS Klinikum Erfurt LINC 2015
Case 1

HELIOS Klinikum Erfurt LINC 2015
Case 2
Patient: m ; 64 y
• chronic repeated pancreatitis
• Tumor of pancreatic head
• severe GIB
• Therapy:
Coil- Embolisation

HELIOS Klinikum Erfurt LINC 2015
Case 2

HELIOS Klinikum Erfurt LINC 2015
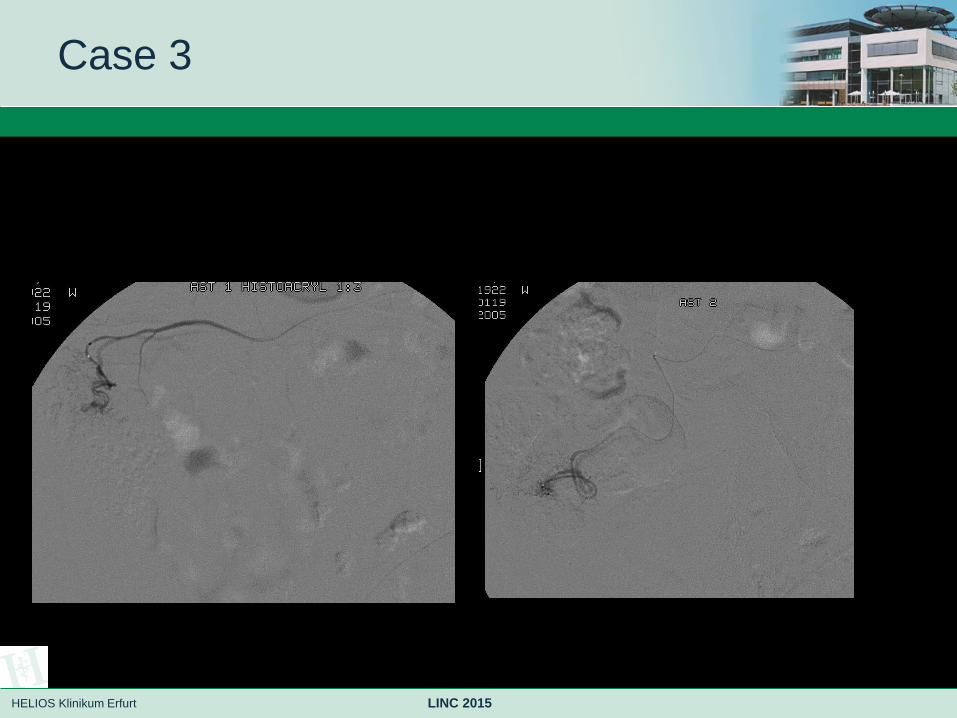
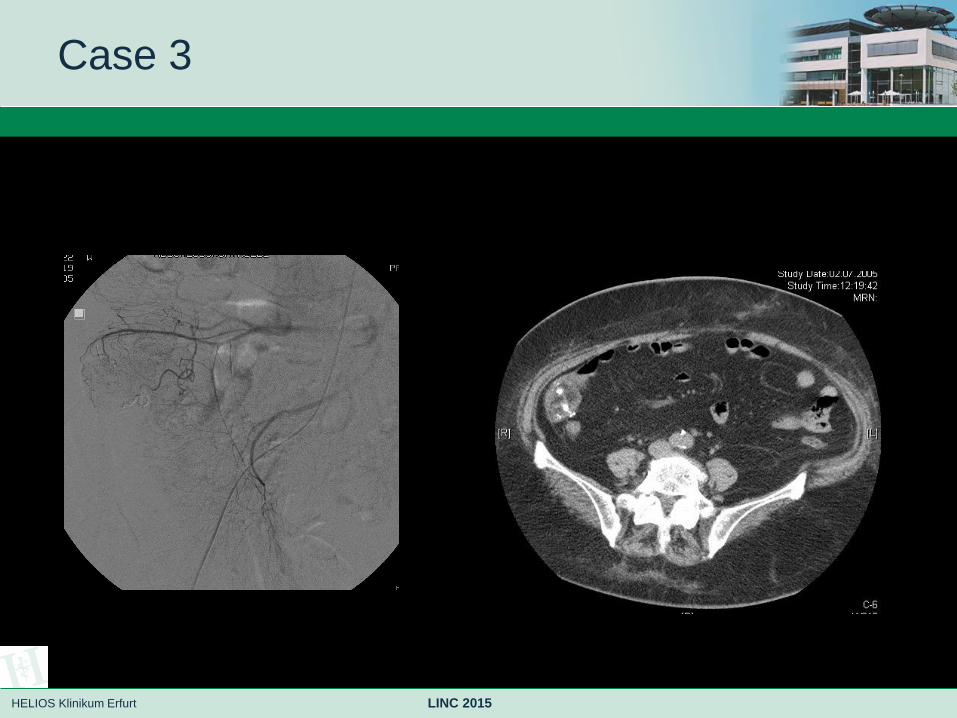
Case 3
Patient: f ; 83 y
• repeated severe GIB
• Angiodysplasie of Colon
• Therapy:
Embolisation of four Feederarteries with glue

HELIOS Klinikum Erfurt LINC 2015
Case 3
HELIOS Klinikum Erfurt LINC 2015
Case 3
HELIOS Klinikum Erfurt LINC 2015
Case 3

HELIOS Klinikum Erfurt LINC 2015
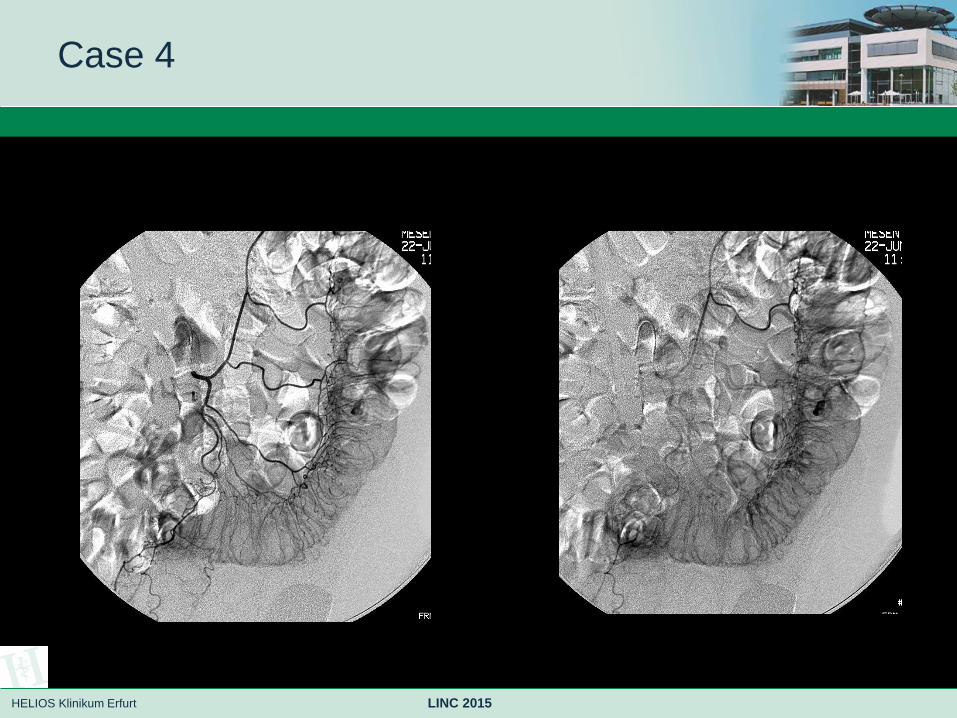
Case 4
Patient: m ; 66 y
• after 2/3 Resektion in gastric cancer
• insufficient Anastomosis
• severe GIB out of sigmoid,
• coloskopic Therapy on diverticulosis not possible
• Therapy:
Embolisation of one Feederartery with glue
HELIOS Klinikum Erfurt LINC 2015
Case 4

HELIOS Klinikum Erfurt LINC 2015
Case 4

HELIOS Klinikum Erfurt LINC 2015
Case 4

HELIOS Klinikum Erfurt LINC 2015
Case 5
Patient: m ; 68 y
• acute pancreatitis
• acute abdominal pain
• respiratory insufficiency
• AMI
symptomatically growing aneurysm of A.lienalis
• Therapy:
Coil and glue embolisation

HELIOS Klinikum Erfurt LINC 2015
Case 5

HELIOS Klinikum Erfurt LINC 2015
Summary (Material)
• Coil (larger vessels)
• Glue (smaller vessels, target restriction)
• Covered stent
• Beads
• All together ?
• Whats the best???
• Your own experience

HELIOS Klinikum Erfurt LINC 2015
Conclusion
CONCLUSIO: endovascular at first
Endovaskular therapies of GIB
„questions“ - answers
Rekanalisation after Coiling ? Low risk of occluding procedures
Downer 2008,
Organ-Ischemia liver/ splenic/ pancreas ? Target restriction!
Sessa 2004, Chiesa 2005
Stent-Grafts in septic Aneurysm ? Unlimited indication
Sachdev 2006, Tulsyan 2007, deFreitas 2007, Rossi 2008
Long time patency of Stent-Grafts ? Sufficient evidence based
Kasirajan 2001, Gabelmann 2002, Sessa 2004, Rossi 2008
Secondary Aneurysma-Expansion (inflammatoric No valid data
etiology) ?

HELIOS Klinikum Erfurt
HELIOS Klinikum Erfurt
LINC 2015
Embolization treatment for
acute gastrointestinal
bleeding
S. Basche

















