Hematology & Immunology Anemia: Low RBCs, Hgb, or volume of RBCs Etiology: Inadequate RBC production Increased RBC destruction Acute or Chronic Blood Loss Iron, Folate, or vitamin B12 deficiency Chronic kidney disease Bone marrow suppression or infiltration Radiation therapy to bones Hematopoietic stem cell transplant Medications Hemolytic anemias RBC membrane defects Trauma, surgery Coagulopathy Complication of anticoagulation GI bleed Frequent diagnostic blood draws Signs & Symptoms o Fatigue o Dyspnea o Activity intolerance o Altered mental status o Headache o Pallor o Possible jaundice or hepatosplenomegaly o Tachycardia o Hypotension o Syncope Lab Values o Hgb < 12 g/dL (women) or 14 g/dL (men) o Urine – can test + for blood o Stool – can test + for blood Patient Management Goals of Care Interventions Improved O2 delivery to tissues and organs Absence of hypovolemia due to bleeding Tolerable level of fatigue Supplemental O2 Elevate HOB for SOB Assess patient’s ability to tolerate anemia Administer PRBCs as ordered Adequate rest periods Diet supplements Admin erythropoietin as ordered Patient education re: diet Potential Complications o Hemorrhagic Shock o Respiratory Failure (risk due to decreased oxygen carrying capacity) o Weakness and Fatigue (due to decrease in oxygen availability to cells)
Transcript
Hematology & Immunology
Anemia: Low RBCs, Hgb, or volume of RBCs
Etiology:
Inadequate RBC production Increased RBC destruction Acute or Chronic Blood Loss
Iron, Folate, or vitamin B12 deficiency
Chronic kidney disease Bone marrow suppression
or infiltration Radiation therapy to bones Hematopoietic stem cell
transplant Medications
Hemolytic anemias RBC membrane defects
Trauma, surgery Coagulopathy Complication of
anticoagulation GI bleed Frequent diagnostic blood
draws
Signs & Symptoms
o Fatigue
o Dyspnea
o Activity intolerance
o Altered mental status
o Headache
o Pallor
o Possible jaundice or hepatosplenomegaly
o Tachycardia
o Hypotension
o Syncope
Lab Values
o Hgb < 12 g/dL (women) or 14 g/dL (men)
o Urine – can test + for blood
o Stool – can test + for blood
Patient Management
Goals of Care Interventions
Improved O2 delivery to tissues and organs
Absence of hypovolemia due to bleeding Tolerable level of fatigue
Supplemental O2 Elevate HOB for SOB Assess patient’s ability to tolerate anemia Administer PRBCs as ordered Adequate rest periods Diet supplements Admin erythropoietin as ordered Patient education re: diet
Potential Complications
o Hemorrhagic Shock
o Respiratory Failure (risk due to decreased oxygen carrying capacity)
o Weakness and Fatigue (due to decrease in oxygen availability to cells)
Thrombocytopenia: Platelet count < 150,000 (increased risk of bleeding)
Causes:
o Decreased platelet production (cancers, antineoplastic agents)
o Platelets < 50,000/mm3 (or at least 50% drop from baseline)
o aPTT > 40 sec
o D‐dimer > 250 ng/mL
o Fibrinogen < 100 mg/dL
Medical Management – PREVENTION
o Slow consumption of coagulation factors
o Maintain organ perfusion
Nursing Management
o Assessment
o Monitoring
Blood and Blood Products
Transfusion Considerations
Blood admin via large bore IV and standard blood tubing with filter
PRBC should be infused within 4 hours
Patients receiving multiple products (units):
o Warm products
o IV calcium admin (citrate added to banked blood leads to hypocalcemia)
Observe for adverse reactions to transfusions
o If an adverse reaction: stop blood and report problem to provider/blood bank
Transfusion Reactions & Complications
Review Questions:
A 45‐year‐old woman is admitted with deep venous thrombosis and pulmonary emboli. She has received
a heparin bolus and was on a continuous heparin drip. The heparin was discontinued because of the
occurrence of heparin‐induced thrombocytopenia. The patient now is scheduled for insertion of a
Greenfield filter to protect the lungs from future emboli from the deep veins in her legs. Her
preoperative laboratory results show a platelet count of 25,000/mm3. Which nursing action is
indicated?
a) No action is necessary
b) Start an extra IV with large‐gauge catheter
c) Notify the surgeon
d) Monitor neurologic status carefully
A 45‐year‐old woman is admitted with deep venous thrombosis and pulmonary embolism. She has
received a heparin bolus and has been on a continuous heparin drip for 3 days. If the patient develops
heparin‐induced thrombocytopenia (HIT), what clinical sign would the nurse expect to see first?
a) Surface bleeding from wounds and IV sites
b) Hematuria
c) Petechiae
d) Bleeding from gums
A patient is admitted with urinary tract sepsis and septic shock. Within 24 hours, hematuria, hemoptysis,
petechiae and purpura, and oozing from IV sites and wounds are noted. Disseminated intravascular
coagulation (DIC) is suspected. Bleeding in DIC results from:
a) Platelet malfunction and malformation
b) Consumption of clotting factors
c) Hereditary absence of clotting factors
d) Interference in the clotting pathways by toxins
A patient with chronic kidney disease asks why he is anemic. The explanation to this patient should be
that anemia is the result of:
a) Loss of blood in the urine
b) Inadequate production of a hormone that stimulates production of red blood cells
c) Deficiency of iron needed for production of red blood cells
d) Development of a gastric ulcer and blood loss as a result of the ulcer
A patient is admitted with urinary tract sepsis and septic shock. Within 24 hours, hematuria, hemoptysis,
petechiae and purpura, and oozing from IV sites and wounds are noted. Disseminated intravascular
coagulation (DIC) is suspected. The laboratory findings most specifically indicative of DIC as the cause of
this bleeding are:
a) Prolonged prothrombin time, activated partial thromboplastin time, and bleeding times
b) Decreased platelet count
c) Elevated fibrin degradation products, especially D‐Dimer
d) Presence of schistocytes
A 52‐year‐old man returns to the hospital 2 weeks after being discharged from an admission for upper
gastrointestinal bleed. He has been vomiting bright red blood for the past 24 hours. Laboratory
parameters reveal a hemoglobin of 6 g/dL and a hematocrit of 20%. Vital signs are blood pressure 90/60
mm Hg; heart rate 120 beats/min and regular; and respiratory rate 22 breaths/min and shallow. He has
received two units of red blood cells (RBCs) in the emergency department. The physician has ordered
four more units of RBCs.
a) Calcium & Potassium
b) Blood Urea Nitrogen and Creatinine
c) Bilirubin and Amylase
d) Sodium and Magnesium
A 52‐year‐old patient with a history of alcoholism is admitted with massive esophageal bleeding. After
infusion of several liters of normal saline, the crossmatched blood is now available. A nursing action that
can prevent a transfusion reaction is to:
a) Obtain a detailed transfusion history
b) Monitor vital signs 15 minutes after starting the transfusion
c) Administer antihistamines before initiating the blood transfusion
d) Check the patient’s identification and blood type with the blood identification and type carefully
A 52‐year‐old patient with a history of alcoholism is admitted with massive esophageal bleeding.
Crossmatched blood is now available. The first action to take if a transfusion reaction is suspected is to:
a) Notify the doctor and blood bank
b) Stop the transfusion and infuse normal saline at a KVO rate
c) Check vital signs and order a new type and crossmatch
d) Obtain blood and urine specimens and send them to the lab
Thrombocytopenia may develop as the result of :
a) a drug reaction
b) a congenital problem
c) an allergic reaction
d) all of the above
Which of the following assessment information would be consistent for a low platelet count from HIT:
a) the presence of metabolic acidosis
b) the presence of acute thrombosis development
c) elevation in ALT and AST
d) decrease in neutrophils
A patient with traumatic brain injury is suspected to be going into disseminative intravascular
coagulopathy. Laboratory results consistent with this diagnosis would be:
a) low PT and aPTT, high platelet count, high fibrinogen
b) low BT, low hemoglobin, high PT and high aPTT
c) low platelet count, low fibrinogen, high PT, high aPTT
d) low fibrinogen, low FSP, high platelet count, high hemoglobin
A patient is admitted with urinary tract sepsis and septic shock. Within 24 hours, hematuria, hemoptysis,
petechiae and purpura, and oozing from IV sites and wounds are noted. Disseminated intravascular
coagulation (DIC) is suspected. Heparin may be used in the course of DIC because it:
a) Decreases circulating platelets and their aggregation ability
b) Neutralizes circulating thrombin
c) Reduces blood viscosity and the need for blood administration
d) Neutralizes circulating plasmin
A 52‐year‐old patient with a history of alcoholism is admitted with massive esophageal bleeding. The
patient is given a blood transfusion. The most common cause of a fatal transfusion reaction is:
a) Immune‐compromised recipient
b) Mismatched blood transfusion
c) Volume overload
d) Electrolyte imbalance
Shock
Definition of Shock
“Complex syndrome of decreased blood flow to body tissues resulting in cellular dysfunction and eventually leading to organ failure” (Rice, 1991)
A state of imbalance of oxygen supply and oxygen demand to the tissues at the cellular level
Clinical syndrome characterized by inadequate tissue perfusion that results in impaired cellular metabolism
SHOCK is Not Low Blood Pressure An Abnormal Hemodynamic State characterized By An Acute Reduction in Blood Flow
Followed By Tissue Hypoxia or Anoxia a process that causes the eventual shutdown of all body systems in a systematic order.
o Time varies from person to person o Process speeds up with progression of the disorder o Circulatory failure leads to cell hypoxia and eventually - death
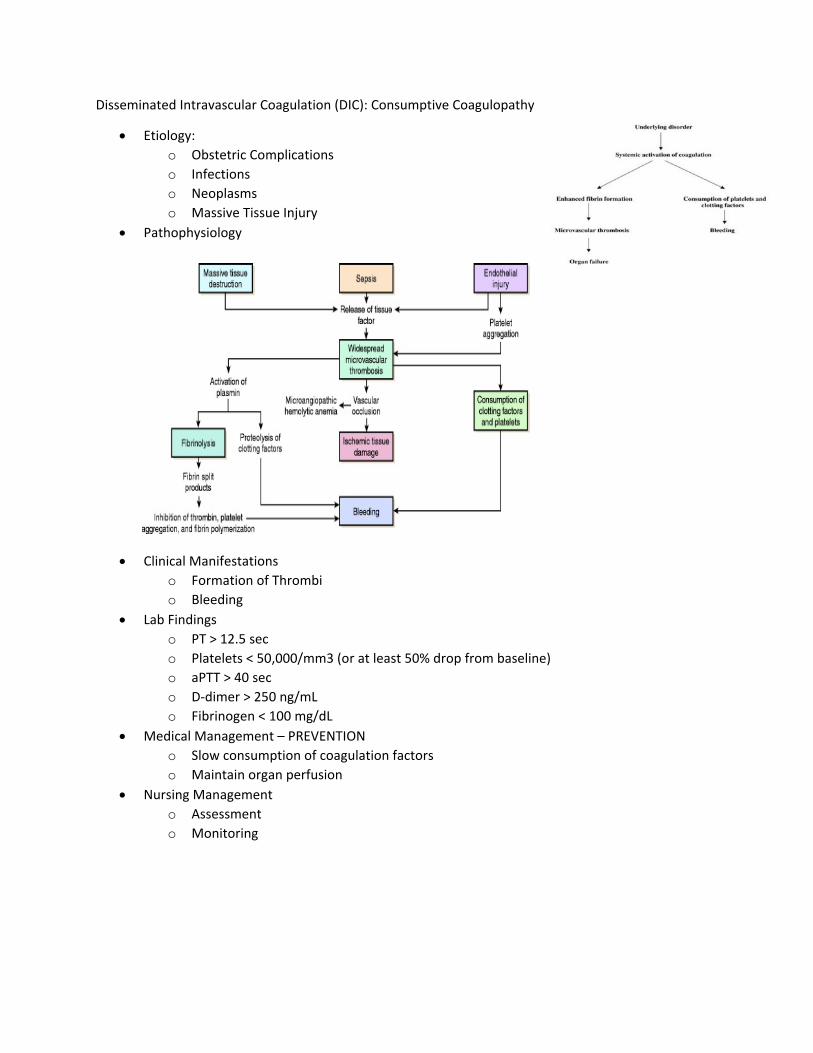
Pathophysiology of Shock
Aerobic Metabolism o In a normal cell – oxygen is used by the mitochondria to convert adenosine
diphospate (ADP) to adenosine triphosphate (ATP) through a process called oxidative phosphorylation in the Krebs cycle
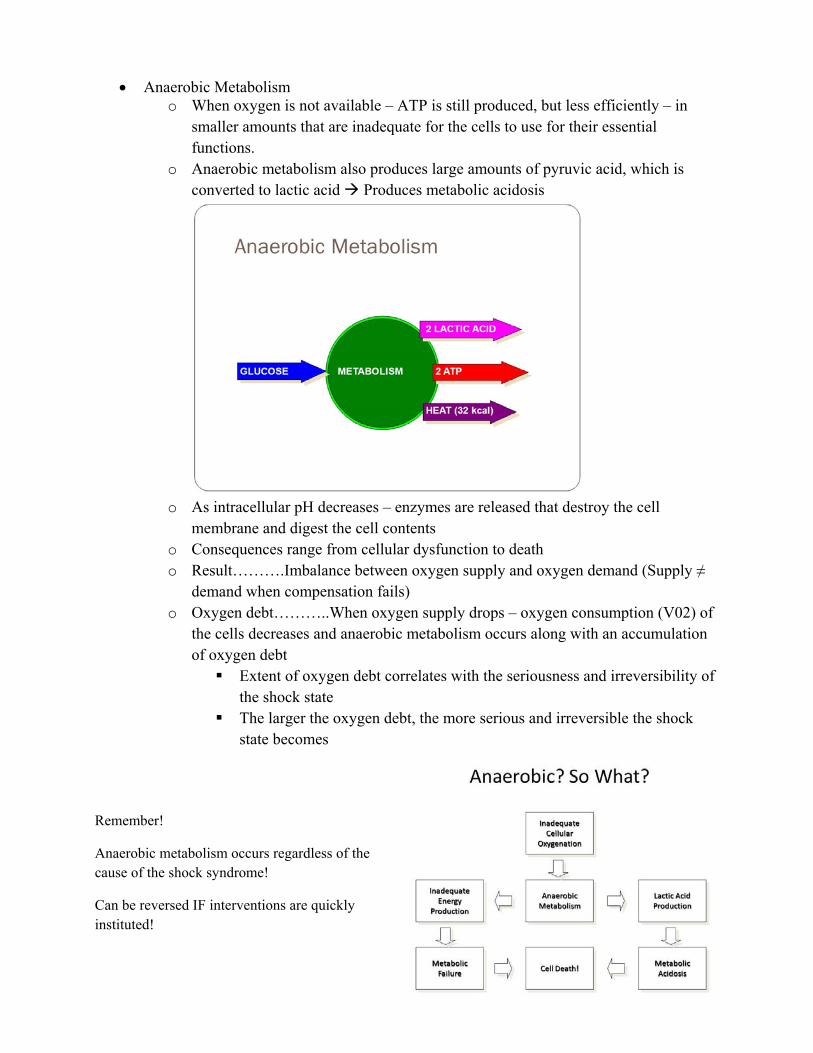
Anaerobic Metabolism o When oxygen is not available – ATP is still produced, but less efficiently – in
smaller amounts that are inadequate for the cells to use for their essential functions.
o Anaerobic metabolism also produces large amounts of pyruvic acid, which is converted to lactic acid Produces metabolic acidosis
o As intracellular pH decreases – enzymes are released that destroy the cell
membrane and digest the cell contents o Consequences range from cellular dysfunction to death o Result……….Imbalance between oxygen supply and oxygen demand (Supply ≠
demand when compensation fails) o Oxygen debt………..When oxygen supply drops – oxygen consumption (V02) of
the cells decreases and anaerobic metabolism occurs along with an accumulation of oxygen debt Extent of oxygen debt correlates with the seriousness and irreversibility of
the shock state The larger the oxygen debt, the more serious and irreversible the shock
state becomes
Remember!
Anaerobic metabolism occurs regardless of the cause of the shock syndrome!
Can be reversed IF interventions are quickly instituted!
Stages of Shock: Compensatory • Progressive • Irreversible Compensatory
Decreased cardiac output compensatory mechanisms Activation of the autonomic nervous system Activation of the renin-angiotensin system Increased rate and depth of respirations
Compensatory Shock - Clinical Findings Normal BP, narrow pulse pressure Sinus tachycardia Fast, deep respirations Decreased urinary output Increased urine specific gravity
Cool, clammy skin Decreased LOC Dilated pupils Increased blood sugar Respiratory alkalosis with hypoxemia
Progressive
Decreased oxygen delivery to cells Shift to anaerobic metabolism Decreased production ATP Production of lactic acid results in metabolic acidosis Failure of the Na+/K+ pump Arrhythmias Alteration of capillary fluid dynamics Further decrease in cardiac output DIC
Progressive Shock – Clinical Findings
Decreased BP with narrow pulse pressure Continued tachycardia Acute renal failure Continued decreasing LOC Interstitial pulmonary edema Peripheral edema Metabolic and respiratory acidosis with hypoxemia
Irreversible
Microvascular and organ damage are now irreversible (untreatable) There is often a "last ditch" effort from the ischemic midbrain with an enormous
discharge of endogenous catecholamines and this can create a last spike of sinus tachycardia
Major Classifications of Shock States Hypovolemic Shock Cardiogenic Shock Obstructive Shock Distributive Shock
Hypovolemic Shock Due to a decrease in circulatory volume
o a decreased venous return. Can result when the fluid in the intravascular space has decreased or the size of the intravascular space has increased in proportion to the fluid volume
Etiology o Hemorrhage o Dehydration o Burns o Third-spacing (such as during a bowel resection)
Clinical presentation o Decreased BP o Increased HR o Increased RR o Decreased urine output o Normal temperature o Cool, pale skin o Decreased CO, CI, PA pressures, PCWP o Increased SVR o Decreased mixed venous oxygen saturation
Treatment of Shock o The primary goals of treatment are:
Early identification of patients at risk for shock Optimize oxygen delivery Identify and treat the underlying cause of shock Decrease oxygen consumption
o Treatment Goal, ABC’s o Restoration of fluid status o Identify and control source of fluid loss o Fluid resuscitation, crystalloids or colloids o Blood products if indicated o Vasoconstrictive agents to maintain perfusion o Monitor lab values o Use large bore IV or CVL o Send blood for CBC, Electrolytes, BUN, CR, DIC, liver function, type and cross o Place NG tube if cause is R/O UGI bleed o Monitor and report patient response to treatment o Collaborative Management o Correcting the cause of volume depletion o Surgical correction o Replacing blood o Anti-emetics; anti-diarrheals o Restoring the intravascular volume o Isotonic fluid/Colloids/Blood Products
Signs and symptoms may also be related to the period of time over
which fluid loss has occurred
Patients may tolerate gradual fluid loses better than sudden shifts or
losses in fluid
Cardiogenic Shock Occurs when the heart fails to function as a pump Severe dysfunction of the right or left ventricle that results in inadequate pumping Causes
o Large myocardial infarction or several small infarctions Affects 20-40% of all individuals who suffer a myocardial infarction
o End-stage cardiomyopathy o Papillary muscle dysfunction o Ventricular septal defect o Arrhythmia o Cardiac Contusion
Pumping action of the heart fails related to injury of cardiac muscle cells 80% mortality rate
Clinical Presentation
o Decreased BP, may be normal initially o Increased HR o Increased RR o Decreased urine output o Normal temperature
o Cool, pale skin o Decreased CO, CI o Increased PCWP, PA pressures o Decreased mixed venous oxygen
saturation
Pathophysiology Impaired pumping ability of the left ventricle Decreased stroke volume Decreased cardiac output Decreased blood pressure Decreased tissue perfusion Inadequate systolic emptying Elevated left ventricular filling pressure Increased left atrial pressure Increased pulmonary venous pressure Pulmonary interstitial edema or
Intraalveolar edema
Collaborative Management o Limiting or reducing myocardial damage during an acute MI
Rapid interventions with thrombolytics, angioplasty, coronary revascularizations
Nitroglycerin, oxygen, pain control, rest o Improving the effectiveness of the pumping action of the heart
o Hemodynamic support Right Sided Failure Left Sided Failure o Volume expansion o Keep CVP between 10 and
15mm/Hg o Vasodilators may be used to
reduce afterload o Positive inotropes may be used
o Venodilators and diuretics as indicated
o Afterload reducers o Inotropes o IABP o Ventricular assist device
Obstructive Shock States Emboli resulting from a venous thrombosis can occlude a major pulmonary artery Tension pneumothorax – can impede venous return Cardiac tamponade – is caused by bleeding into the pericardial sac impairing ventricular
filling and decreasing cardiac output Distributive (Vasogenic)
Abnormality in the vascular system that produces a maldistribution of blood flow, includes neurogenic, anaphylactic and septic
Occurs when blood vessels dilate without subsequent increase in volume Related to poor vascular tone causing vasodilation Volume is adequate – vascular bed is too large Blood pools in the periphery Decreased venous return causes insufficient filling of the ventricle Leads to
inadequate ventricular pumping Decreased cardiac output Tissue hypoxia and cell death
Immune system overreaction that results in a host of vasoactive reactions Causes: Repeated exposure to an antigen (antibiotics, other drugs, contrast media, food,
insect stings, snake bites) Allergic reaction Fatal if untreated Antigen binds to immunoglobulin causing a release of chemicals including histamine,
kallikrein, and platelet-activating factor.
Pathophysiology: Massive vasodilation and increased capillary permeability Antigen + Antibody = Antigen/Antibody Reaction Release of vasoactive mediators Massive vasodilation (veins & arterioles) & Increased capillary permeability (leads to interstitial edema and relative hypovolemia)
Clinical manifestations o Urticaria o Pruritis o “Sense of impending doom” o Bronchoconstriction (wheezing,
cyanosis)
o Increased capillary permeability (fluid shifts to interstitial spaces)
o Decreased CO as a result of massive peripheral vasodilation Increased HR, RR
o Decreased PA pressures, PCWP
Treatment goal, ABC’s o Identify and remove causative agent o Fluids o Epinephrine o Antihistamines o Corticosteroids o Bronchodilators o Patient education
Neurogenic Shock Results from the loss of normal sympathetic nervous system response Etiology
o Brain injury that results in depression of the vasomotor center o Spinal cord injury (above mid-thoracic region) o High spinal anesthesia o Drug overdose
Pathophysiology: o Caused by stimulation of the autonomic nervous system = parasympathetic
system is unchallenged or sympathetic nervous system is blocked results in massive vasodilation, decreased venous return, and decreased cardiac output
Clinical Manifestations: o Decreased preload, SV, CO and blood pressure o Bradycardia develops – inhibited baroreceptor response o Loss of reflex tachycardia further compromises cardiac output and tissue
perfusion o Neurogenic shock develops within 60 minutes after spinal cord injury
Can continue for several weeks o Hypotension, heart rate less than 60, warm, dry skin, hypothermia o Additional signs of hypoperfusion
Treatment goal, ABC’s o Maintain stability of the spine o Provide for cardiovascular stability o Fluid resuscitation o Vasoconstrictors to improve BP o Atropine
Septic Shock A systemic response to massive infection Adequate tissue perfusion is maintained by an adequate circulating blood volume and the
adequacy of circulating volume depends on the condition of the heart, vascular tone and actual blood volume.
Patients at risk o Fever o Host-related o Malignancy o Extremes of age o Malnutrition
o Immune deficiency o Chronic illness o Treatment Related o Chemotherapy o Radiation
o Antibiotics o Skin Breakdown o Invasive procedures o Prolonged hospitalization o Translocation of Bacteria
Caused by infection
o Initial inflammatory response results in an elevation of blood flow and vascular permeability at the infectious site
o Mediators are released causing further alterations in the vascular bed o Severe infections cause the release of endotoxins and exotoxins which are
powerful vasodilators o Results in decreased venous return and decreased cardiac output
Pathophysiology
o Too much inflammation o Hypercoagulability o Decreased fibrinolysis
Clinical presentation
o Early (Hyperdynamic) Signs of sympathetic stimulation Increased heart rate, respiratory rate, myocardial contractility, cardiac
output Increased oxygen consumption by tissues and cells Increased minute ventilation Blood vessels dilate – decrease SVR Warm, flushed skin, changes in LOC, fever and chills, hypoxemia, rapid
bounding peripheral pulses o Late (Hypodynamic) – the body can no longer meet the oxygen demands of the
tissues Decreased cardiac output Severe hypotension Weak, rapid thready pulses Hypothermia Cold, clammy , mottled skin Multiple organ failure
o Decreased BP o Increased HR, RR o Urine output increased then decrease o Temperature
o Skin: warm then cool o Color: flushed then pale o CO, CI increase then decrease o PA pressures, PCWP, SVR decrease then increase o Mixed venous oxygen saturation increase then decrease
Treatment Goals
o Optimize Oxygen Delivery Supplemental oxygen Administration of IV fluids Positive inotropes Vasoactive drugs Trendelenburg position modified
o Fluid administration, followed by appropriate vasopressor o Antibiotic therapy o Blood cultures o Anti-endotoxins o Septic Shock o Early recognition and removal of source of infection o Appropriate antibiotic therapy o Hemodynamic support o Nutritional support o Handwashing o Universal precautions o Measures to prevent nosocomial infection
Review
Shock is NOT JUST LOW BP Despite physician’s orders-drug titration is NOT about blood pressure, but tissue
perfusion. Hypovolemic shock requires fluid RX Cardiogenic shock requires inotropic and dilator RX Vasogenic shock requires fluid,Vasopressors and possibly inotropic RX Prevention is the single most important intervention!
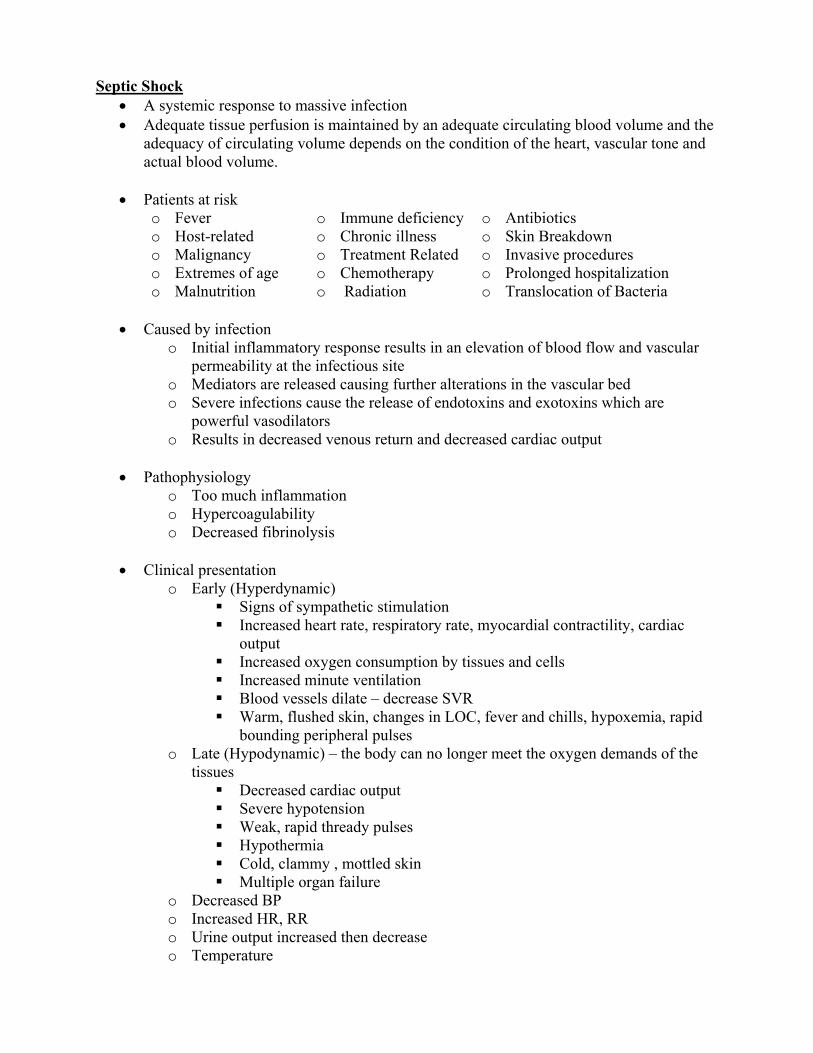
Review of Shock Types
Shock Type CVP PAWP SVR C.O. HR Comments
Hypovolemic ↓ ↓ ↑ ↓ ↑
Cardiogenic ↑ ↑ ↑ ↓ ↑
Neurogenic ↓ ↓ ↓ ↑ ↓
Septic ↓ ↓ ↓ ↑ ↑
Anaphylactic ↓ ↓ ↓ ↑ ↑
Respiratory Monitoring and Beyond: ABGs, SPO2, & ETCO2 Description • Arterial blood gases are used to measure the amount of oxygen, carbon dioxide, and
bicarbonate in the blood, as well as the pH. • ABGs provide information regarding physiologic phenomena
Acids • Substances capable of releasing a hydrogen ion (H+) into solution. • Volatile acids
▫ excreted through the lungs (CO2) • Fixed or nonvolatile acids
▫ excreted by the kidneys (ketoacids and lactic acid) Bases • Substances capable of combining with H+ in solution. • Bicarbonate (HCO3)
▫ Most important base in the blood ▫ regulated by the kidneys
• Hemoglobin and plasma proteins. • Bases are reflected in the ABGs as the HCO
3 and the base excess or base deficit.
Elements of ABGs: Normal Values
Element Description Normal Value pH • Represents a combined effect of metabolic and respiratory
factors • Low pH = acidosis • High pH = alkalosis
7.35-7.45 (7.4)
PCO2 • Measure of the partial pressure of carbon dioxide dissolved in the plasma
• Byproduct of metabolism • CO2 is excreted by the lungs and is a measure of the adequacy
of ventilation • CO2 functions as an acid because it combines with water to
produce carbonic acid (H2CO3)
35-45 mmHg
HCO3 • Bicarbonate ion is a base regulated by the kidneys • It may be adjusted to compensate for respiratory acid-base
imbalance, or may be altered by other factors such as kidney disease or metabolic alterations
22-26 mEq/L
PaO2 • Partial pressure of oxygen dissolved in arterial plasma • Only about 1% of total oxygen content is carried in this state • Indicates how well oxygen is being taken up in the lungs
80-100 mmHg
SaO2 • Represents the percentage of total hemoglobin which is saturated with oxygen
• Vast majority of oxygen is carried in this state • Usually well-correlated with PaO2 (oxyhemoglobin
dissocation curve), some conditions (i.e. pH, temp) can influence the relationship
95-98%
Base Excess (BE)
• Represents the combined effects of HCO3 and other bases – plasma proteins, hemoglobin, and others
• A negative base excess is sometimes referred to as a base deficit
▫ Elevated (acidotic), decreased (alkalotic), or normal 3. Check HCO3 (metabolic parameter)
▫ Elevated (alkalotic), decreased (acidotic), or normal 4. If abnormalities exist, determine which of the major acid/base imbalances is present 5. Determine whether any compensation mechanisms are involved 6. Check PO2 and O2 saturation
▫ normal, elevated, or decreased 7. Observe patient (evaluate vital signs and physical parameters)
▫ Evaluate why patient presents any abnormal values which are present and implement appropriate actions to correct the acid/base imbalance
Respiratory Acidosis (Elevated PaCO2) • Caused by hypoventilation of any etiology
▫ COPD ▫ Oversedation, head trauma, anesthesia, or reduced function of respiratory center. ▫ Neuromuscular disease ▫ Inappropriate mechanical ventilation ▫ Other causes of hypoventilation (sleep apnea)
Respiratory Alkalosis (Low PaCO2) • Caused by hyperventilation
▫ Hypoxemia ▫ Nervousness and anxiety ▫ Pulmonary Embolus ▫ Pregnancy ▫ Inappropriate mechanical ventilation ▫ Compensation for metabolic acidosis
Metabolic Alkalosis (Elevated HCO3) • Caused by a loss of nonvolatile acid or increase in HCO3 • Gastric loss of acid • HCO3 during cardiac arrest • Baking soda • Massive blood transfusion – citrate – lactate - bicarbonate • Increased excretion of H+, K+, and Cl - due to :
• No increase in immeasurable anions: ▫ Diarrhea ▫ Drainage of pancreatic juice ▫ Treatment with diamox ▫ Treatment with ammonium chloride ▫ Renal tubular Acidosis
Clinical Signs of Acidosis/Alkalosis
Acidosis (CNS Depression) Alkalosis (CNS Excitation) • Depressed thought processes • Delayed reaction times • Slurred speech • Somnolence • Uncoordination • Confusion • Semi-coma • Death
• The anion gap refers to a difference in the routinely measured cations (positively charged particles, such as Na+ , Ca++, and Mg++ ) and anions (negatively charged particles , such as HCO3- and Cl-)
• The formula for the anion gap is: ▫ AG= Na+ - (HCO3- + Cl-)
• The normal anion gap is 8-16 mEq/L • Practice: Na 138, HCO3 11, Cl 99, = Anion Gap of ______
Anion Gap – why do we care? • Assists in differential diagnosis of the type of metabolic acidosis • An elevated anion gap acidosis suggests an increase in plasma level of unmeasured
cations (accumulation of acids is not adequately buffered by a base) • A nonelevated anion gap acidosis reflects the loss of bicarbonate, rather than an
increase in acid production or a decrease in acid excretion.
Respiratory Acidosis (pH is low, PaCO2 is high)
pH 7.30 PCO2 65 PO2 90 HCO3 26 BE 0 SaO2 95%
Respiratory Alkalosis (pH is high, PaCO2 is low)
pH 7.5 PCO2 30 PO2 90 HCO3 26 BE 0 SaO2 95%
Metabolic Acidosis (pH is low, HCO3/BE is low)
pH 7.30 PCO2 35 PO2 92 HCO3 18 BE -3 SaO2 97%
Metabolic Alkalosis (pH is high, HCO3/BE is high)
pH 7.50 PCO2 40 PO2 95 HCO3 35 BE +3 SaO2 96%
Compensation • Body’s ability to regulate pH by adjusting either the rate of ventilation (excretion of
CO2) or the renal excretion of HCO3) • Mechanism by which an abnormal PaCO2 or HCO3 may be accompanied by a normal or
near-normal pH • In other words, it is the body’s attempt to normalize pH. • Common compensatory mechanisms involve regulating the amount of CO2 (respiratory
compensation-fast response) or the amount of HCO3- (metabolic compensation-slower response)
HOW? • Respiratory acidosis due to increased PaCO2
▫ Compensation: Kidneys excrete more acid and less HCO3- resulting in increased HCO3-
• Respiratory alkalosis due to decreased PaCO2 ▫ Compensation: Kidneys excrete HCO3-
• Metabolic acidosis due to decreased HCO3- ▫ Compensation: Hyperventilation to decrease PaCO2
• Metabolic alkalosis due to increased HCO3- ▫ Compensation: Hypoventilation to increase PaCO2
Rate & depth of respirations increase eliminates additional CO2
↓ pH ↓ HCO3 ↓ PaCO2
Metabolic Alkalosis
• Bicarbonate excess Rate & depth of respirations decrease retaining CO2
↑ pH ↑ HCO3 ↑ PaCO2
Respiratory Acidosis
• Retained CO2 & excess carbonic acid
Kidneys conserve bicarbonate to restore carbonic acid : bicarbonate ratio 1:20
↓ pH ↑ PaCO2 ↑ HCO3
Respiratory Alkalosis
• Loss of CO2 & deficient carbonic acid
Kidneys excrete bicarbonate and conserve H+ to restore carbonic acid : bicarbonate ratio
↑ pH ↓ PaCO2 ↓ HCO3
There are two types of compensation • Partial Compensation
▫ pH, pC02, and Bicarb are all abnormal • Full Compenstion
▫ pH is normal, pC02 and Bicarb are abnormal
Assessment of Acid-Base Balance • Look at the pH, and determine if it is low (acidotic), normal, or high (alkalotic) • Look at the CO2 and HCO3 and determine if these values “match” the pH.
▫ For example, you would expect a normal pH to go along with a normal CO2 and HCO3-. A normal pH with abnormal CO2 and HCO3 indicates compensation.
Physiologic Phenomena - Oxygenation • Ability of the lungs to deliver fresh O2 to the blood in the pulmonary capillary beds • Reflected in the partial pressure of oxygen (PaO2) and the percent saturation of oxygen
(SaO2) in the arterial blood • Oxygenation Definition
▫ Amount of oxygen carried in the arterial blood that is bound to the hemoglobin molecule.
▫ It is reflected as SaO2 (the percent of hemoglobin in saturated with oxygen) ▫ The driving force for SaO2 is the PaO2 (partial pressure of dissolved oxygen in
the blood) • Assess Oxygenation
▫ Look at the PaO2, which is a good indicator of O2 uptake in the lungs. ▫ Assess the SaO2 as an indicator of O2 content (CaO2) ▫ While PO2 and SaO2 are related, the vast majority of the total O2 content is
reflected in the SaO2 ▫ Consider the hemoglobin content of the blood
• Ventilation ▫ Ability of the body to rid itself of carbon dioxide (CO) ▫ Reflected in ABGs as partial pressure of CO (PaCO)
• Assess Oxygen Delivery ▫ The ‘bottom line’ of respiration is the delivery of O2 to the body’s cells and
removal of carbon dioxide ▫ For this to occur, the oxygenated blood must be delivered to the tissues and
deoxygenated blood returned to the heart • Two ways to Assess O2 Delivery
▫ Oxygen delivery and uptake by tissues can be measured using a properly equipped pulmonary artery catheter
▫ Basic physical assessment cues: • Short of breath or hyperventilating • Blood pressure, pulse rate and rhythm, skin temperature and color • Distention of the neck veins, Auscultation of a gallop or murmur • Crackles at the bases of the lungs
ETCO2 – ventilation vital sign ETCO2 monitoring determines the CO2 concentration of exhaled gases Photo detector measures the amount of infrared light absorbed by airway gases during
inspiration and expiration o CO2 molecules absorb specific wavelengths of infrared light energy o Light absorption increases directly with CO2 concentration
A monitor converts this data to a CO2 value and a corresponding waveform (capnograph)
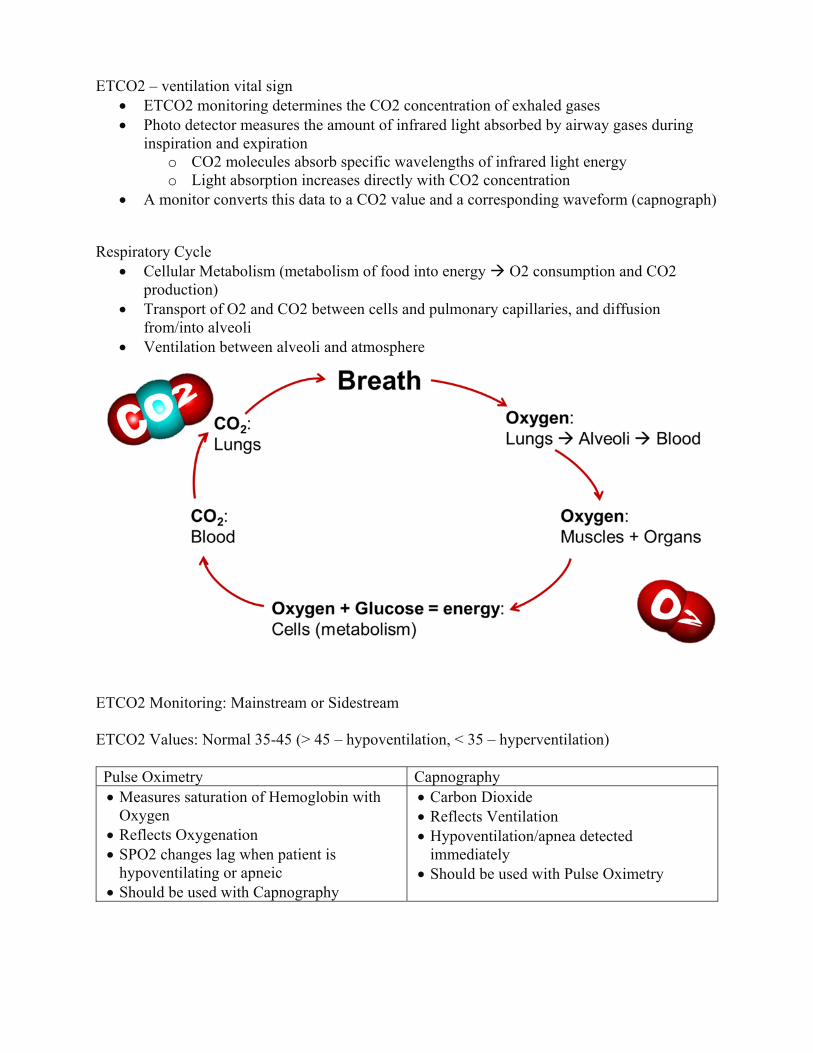
Respiratory Cycle Cellular Metabolism (metabolism of food into energy O2 consumption and CO2
production) Transport of O2 and CO2 between cells and pulmonary capillaries, and diffusion
from/into alveoli Ventilation between alveoli and atmosphere
ETCO2 Monitoring: Mainstream or Sidestream ETCO2 Values: Normal 35-45 (> 45 – hypoventilation, < 35 – hyperventilation) Pulse Oximetry Capnography Measures saturation of Hemoglobin with
Oxygen Reflects Oxygenation SPO2 changes lag when patient is
hypoventilating or apneic Should be used with Capnography
Which of the following ABG values would be most indicative of a diagnosis of acute respiratory failure?
pH pCO2 pO2 HCO3
A. 7.18 70 54 26
B. 7.18 80 63 42 C. 7.26 55 80 24
D. 7.34 45 65 23
Which of the following is a correct statement about a shift of the oxyhemoglobin dissociation curve to the right?
A. It can result from an increase in blood pH B. It can result from an increase in body temperature C. It results in less oxygen being unloaded from hemoglobin molecules D. It results in 100% saturation of hemoglobin
Which of the following best defines hypoventilation?
A. An RR less than 10 B. A pCO2 greater than 45 C. A pO2 less than 75 D. An arterial pH greater than 7.35
An ABG sample obtained while a patient is breathing room air reveals the following: pH 7.18, pCO2 80, pO2 35, HCO3 29 The ABG indicates:
A. Respiratory acidosis with mild hypoxemia B. Respiratory acidosis with severe hypoxemia C. Combined respiratory and metabolic acidosis with mild hypoxemia D. Combined respiratory and metabolic acidosis
A patient is admitted to the MICU with the following arterial blood gas results pH 7.55, CO2 28 mmHg, PaO2 88 mmHg, HCO3 26 mEq/L What is the interpretation?
A. Respiratory Acidosis B. Compensated Metabolic Alkalosis C. Non-compensated Respiratory Alkalosis D. Metabolic Alkalosis
Which of the following is a complication of mechanical ventilation and peak end expiratory pressure (PEEP) therapy?
A. Atelectasis B. Oxygen toxicity C. Reduced cardiac output D. Acute Respiratory Distress Syndrome
5/26/2020
1
VENTILATION STRATEGIESBeth Brown, BSN, RN, CCRN‐K
CONTENT
Modes of Mechanical Ventilation
Prone positioning
Noninvasive Ventilation
Mechanical Ventilation Prevention of Complications Therapeutic Interventions
Tracheostomy
Therapeutic Gases Nitric Oxide Heliox
LUNG VOLUMES/CAPACITIES DEFINITIONS
Total Lung Capacity (TLC): Volume of gas contained in the lung at the end of maximal inspiration
Vital Capacity (VC): Maximal volume of gas that can be expelled from the lungs following a maximal inspiration
Inspiratory Capacity (IC): Maximal volume of gas that can be inspired from the resting expiratory level
Functional Residual Capacity (FRC): Volume of gas remaining in the lungs at resting end expiration
COMMON BASIC VENTILATOR SETTINGS
FiO2 ‐ fraction of inspired Oxygen (21% ‐ 100%).
Tidal Volume ‐ amt of air that the ventilator has been set to deliver to the patient with each breath. Healthy Lungs: 6‐8 ml/kg ALI/ARDS: 5‐6 ml/kg
Respiratory rate‐Number of positive pressure breaths the ventilator delivers per minute.
5/26/2020
2
PEEP
Lets the patient exhale while maintaining a preset positive pressure at the end of expiration.
Allows for greater gas exchange before the next breath. It is the application of positive pressure to the airway at end expiration.
First used early in the 1970s as a treatment for Respiratory distress syndrome in newborns
Auto‐PEEP: occurs when expiration is not long enough to empty the lungs
INSPIRATORY TIME: EXPIRATORY TIME RELATIONSHIP (I:E RATIO)
During spontaneous breathing, the normal I:E ratio is 1:2, indicating that for normal patients the exhalation time is about twice as long as inhalation time.
If exhalation time is too short “breath stacking” occurs resulting in an increase in end‐expiratory pressure also called auto‐PEEP.
Depending on the disease process, such as in ARDS, the I:E ratio can be changed to improve ventilation
PRESSURES
PEAK Airway Pressures Measured at airway opening Norm: < 40
PLATEAU Pressures Measured at end of inspiration Norm: < 30
CONVENTIONAL MODES OF MECHANICAL VENTILATION
Ventilation Modes considerations: Trigger: What controls the tidal breath? Pressure or Volume
Limit: What determines the size of the breath?
Cycle: What actually ends the breath? Usually time
5/26/2020
3
CONVENTIONAL MODES OF MECHANICAL VENTILATION –VOLUME MODES
Tidal volume and minute ventilation are ensured Volume is preset Pressure varies with patient compliance and resistance
Assist‐Control Ventilation (ACV) CMV All breaths (patient initiated and pre‐set) are same volume
Synchronized Intermittent Mandatory Ventilation (SIMV) Pre‐set breaths are set volume, patient‐initiated volume determined by patient Vent synchronizes the mandatory breaths with patient’s own breaths
CONVENTIONAL MODES OF MECHANICAL VENTILATION – PRESSURE MODES
Tidal volume is determined by the selected pressure level, airway resistance, and lung compliance Pressure is preset Volume varies
Pressure Controlled Ventilation (PCV) Does not allow for patient‐initiated breaths Applies constant pressure for a preset time Variable tidal volumes (flow depends on lung resistance, lung compliance, and patient effort) Used in ARDS to reduce barotrauma
Pressure Support Ventilation (PSV) Patient determines inflation volume and respiratory rate Used to augment spontaneous breathing
CONVENTIONAL MODES OF MECHANICAL VENTILATION – PRESSURE MODES CONTINUED
Airway Pressure Release Ventilation (APRV) Bi‐level mode providing 2 levels of CPAP with an inverse ratio (very short expiration time – inverse ratio) Requires increased amounts of sedation Considered Rescue Method for patients with lung compliance and oxygenation issues Helps prevent alveolar collapse and maintain recruitment
Risks: Pneumothorax Ventilator trauma
CONVENTIONAL MODES OF MECHANICAL VENTILATION – DUAL MODES
Pressure Regulated Volume Control (PRVC) A control mode, which delivers a set tidal volume with each breath at the lowest possible peak pressure. Delivers the breath with a decelerating flow pattern that is thought to be less injurious to the lung…… “the guided hand”.
5/26/2020
4
VENTILATOR MODES
MODE FUNCTION CLINICAL USE Assist‐Control Ventilation (A/C) Delivers breath in response to patient effort and if
patient fails to do so within preset amount of timeUsually used for spontaneously breathing patients with weakened respiratory muscles
Ventilator breaths are synchronized with patient’s respiratory effort
Usually used to wean patients from mechanical ventilation
Pressure Controlled Ventilation (PCV)
Pressure limited ventilation; can be combined with inverse ratio (watch for auto‐PEEP)
Pressure Support Ventilation (PSV) Preset pressure that augments the patient’s inspiratory effort and decreases breathing work
Often used with SIMV during weaning
Airway Pressure Release Ventilation (APRV)
Biphasic ventilation with short expiratory time
Pressure Regulated Volume Control (PRVC)
NON‐CONVENTIONAL MODES OF MECHANICAL VENTILATION
High Frequency Oscillatory Ventilation (HFO) Used for refractory hypoxemia Oscillates the lung around a constant mean airway pressure higher than conventional ventilation Delivers breaths at high frequencies and low tidal volumes Hertz (Hz): 1 Hz = 60 breaths
Disadvantages: Require heavy sedation/neuromuscular blockade Cannot transport patient Cannot auscultate breath/heart/bowel sounds
PRONE POSITIONING
Redistributes pulmonary blood flow
7 trials All showed improvement in oxygenation 6/7 did not show improvement in mortality
Intact airway protective mechanism (needed for extubation)
WEANING
Definitions Rapid Shallow Breathing index (RSBI): respiratory rate divided by tidal volume. Most studied of the weaning parameters The faster you breathe with small volumes the higher the number
Negative Inspiratory Force (NIF): (or MIP –maximal inspiratory pressure) Global assessment of strength of respiratory muscles
Minute Ventilation: respiratory rate x tidal volume Estimates demand on the respiratory system. Normal is 5‐6L/min in healthy adults. Increased CO2 production from fever, hypermetabolic state, hypoxemia, etc will increase minute ventilation
5/26/2020
8
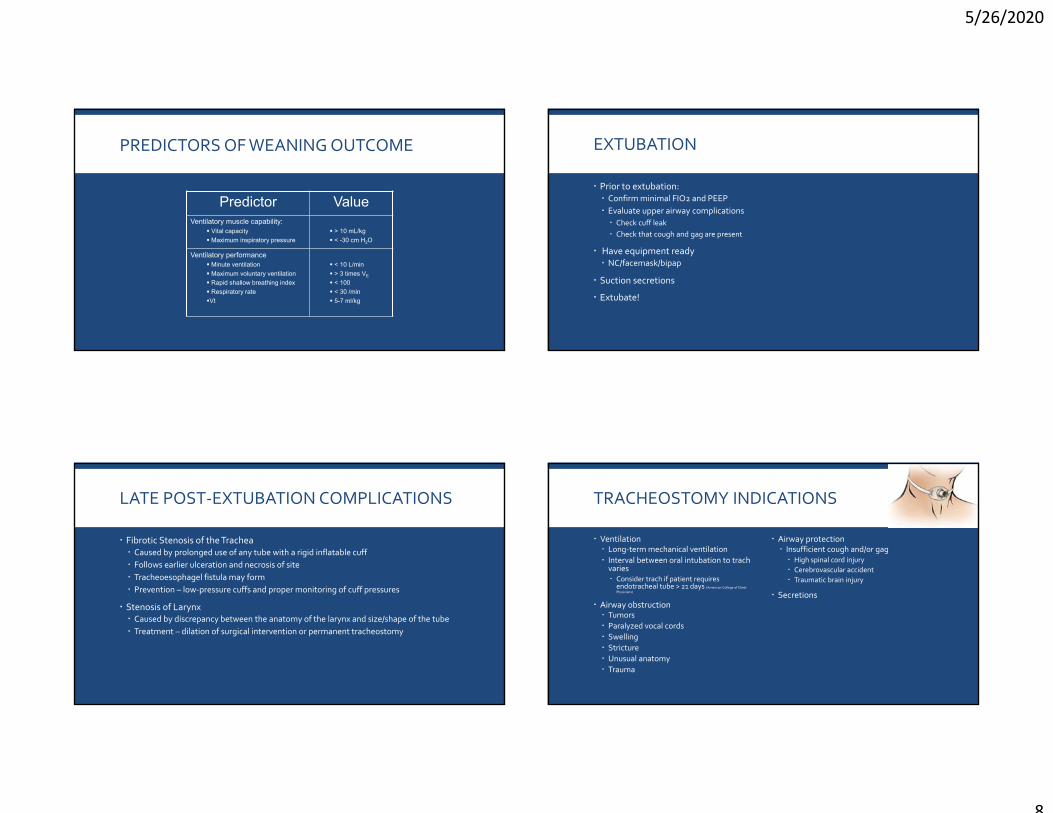
PREDICTORS OF WEANING OUTCOME
Predictor ValueVentilatory muscle capability:
Vital capacity
Maximum inspiratory pressure
> 10 mL/kg
< -30 cm H2O
Ventilatory performance Minute ventilation
Maximum voluntary ventilation
Rapid shallow breathing index
Respiratory rate
Vt
< 10 L/min
> 3 times VE
< 100
< 30 /min
5-7 ml/kg
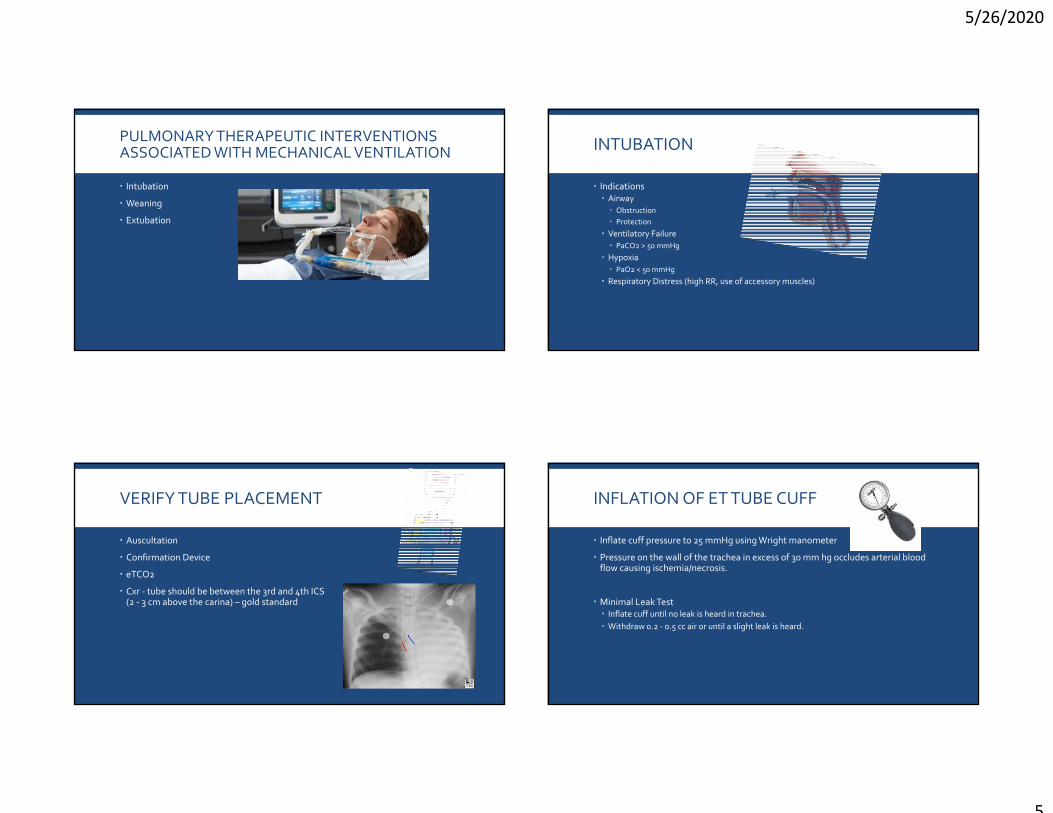
EXTUBATION
Prior to extubation: Confirm minimal FIO2 and PEEP Evaluate upper airway complications Check cuff leak Check that cough and gag are present
Have equipment ready NC/facemask/bipap
Suction secretions
Extubate!
LATE POST‐EXTUBATION COMPLICATIONS
Fibrotic Stenosis of the Trachea Caused by prolonged use of any tube with a rigid inflatable cuff Follows earlier ulceration and necrosis of site Tracheoesophagel fistula may form Prevention – low‐pressure cuffs and proper monitoring of cuff pressures
Stenosis of Larynx Caused by discrepancy between the anatomy of the larynx and size/shape of the tube Treatment – dilation of surgical intervention or permanent tracheostomy
TRACHEOSTOMY INDICATIONS
Ventilation Long‐term mechanical ventilation Interval between oral intubation to trachvaries Consider trach if patient requires endotracheal tube > 21 days (American College of Chest Physicians)
Modes of Mechanical Ventilation https://www.openanesthesia.org/modes_of_mechanical_ventilation/
Henderson, Griesdale, Dominelli et al. (2014). Does prone positioning improve oxygenation and reduce mortality in patients with acute respiratory distress syndrome? Canadian Respiratory Journal 21(4).
Hartjes, TM. (2006). AACN Core Curriculum for High Acuity, Progressive, and Critical Care Nursing 7th Edition.
WHICH OF THE FOLLOWING IS A COMPLICATION OF MECHANICAL VENTILATION AND PEAK END EXPIRATORY PRESSURE (PEEP) THERAPY?
A. Atelectasis
B. Oxygen toxicity
C. Reduced cardiac output
D. Acute Respiratory Distress Syndrome
Fluid & Electrolytes Study Guide
An electrolyte is a term for salts, or ions and is expressed as millequivalents/L
When immersed in water, electrolytes dissociate into charged particles, either (+) charged ions
(cation) or as a (‐) charged ion (anion)
In normal circumstances total cations = total anions (if not, a “gap” occurs)
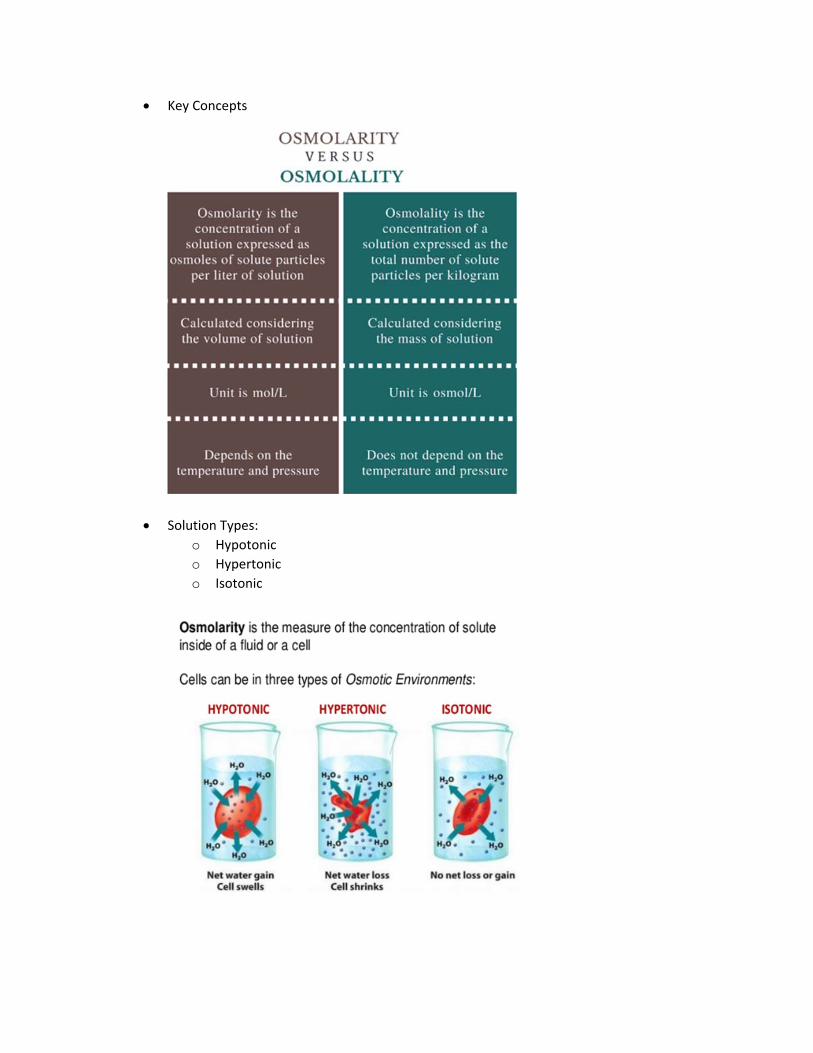
Key Concepts:
o Electrolytes and body fluids are interdependent
o Found in all fluid compartments body secretions and wastes
o Measure electrolytes in the extracellular fluid or vascular compartment
o Major Body Fluid/Electrolyte Compartments
Intracellular
Fluid within the cells, including RBC’s and WBC’s
Largest compartment
Contains 2/3 of the total body weight (approx. 25 liters in a 70 kg
adult)
Extracellular
Fluid outside the cells
Make up 1/3 total body weight
3 compartments
o Intravascular – fluid within the blood vessel (plasma)
o Interstitial – fluid that surrounds the cells
o Trans‐cellular – includes CSF, pericardial, pleural, digestive,
Isotonic Same Osmolarity as serum and body fluids Expands the intravascular compartment without effecting the intracellular or interstitial compartments
LR NS D5W*
Hypotonic Lowers serum osmolarity and causes fluid shifts from intravascular into intracellular compartments Hydrates the cells Depletes fluid within the intravascular compartment
0.45% NS 0.33% NS
Hypertonic Raises the serum osmolarity Shifts fluid from the intracellular/interstitial compartments into the intravascular compartment Shrinks the cells Volume expanders
D5 ½ NS 3% NS D5LR
Potassium – Normal 3.5‐5.5 (MEq/L)
Action in Body:
Maintains cellular osmolarity
Necessary for transmission of nerve impulses and for muscle contraction
Assists with reassembling amino acids into proteins
Maintains acid‐base balance
Regulated By: Kidney through glomerular filtration rate, aldosterone
Comments:
Kidney cannot conserve K+, so it must be consumed daily.
K+ and H+ move together in the kidney.
If cellular K+ is lowered, Na+ enters the cell, making it more irritable.
Hyperkalemia: > 5.5 MEq/L
Causes Symptoms Treatment
Injured cells
Early burns
Hemolysis
Renal disease
Adrenal insufficiency
Low cardiac output syndrome
Certain drugs
Too much intake of K+
Intestinal colic
Diarrhea
Irritability
Nausea
Dizziness
Muscle weakness
Cramps and pain
flaccid muscle paralysis
high peaked T‐waves on EKG, wide QRS
Reducing K+ intake
Giving oral or IV hydrating solutions
Giving dextrose and insulin infusions (20% dextrose solution with 1 unit of insulin for each 2gm of dextrose).
Using extrarenal dialysis
Giving binding resins (e.g., Kayexalate)
Giving osmotic diarrheal (Sorbitol)
Albuterol 10‐20 mg
Hypokalemia: < 3.5 MEq/L
Causes Symptoms Treatment
Alkalosis: K+ shifts into cell
Severe stress: K+ shifts into the cell
Diuretic therapy
Abnormal GI losses
Starvation or malnutrition
Metabolic disease
Increased adrenal corticosteroid secretion or corticosteroid therapy
Essential for blood clotting, for normal functioning of the central nervous system, and for muscle contraction and neuromuscular stability.
Stabilizes cell membranes.
Regulated By: Parathyroid hormone, thyrocalcitonin, vitamin D, kidney function
Comments:
Major concentration is in the bone.
50% of serum Ca2+ is bound to protein.
Normal gastric acidity is necessary for absorption of Ca2+ in the gut.
Acts as a sedative on body.
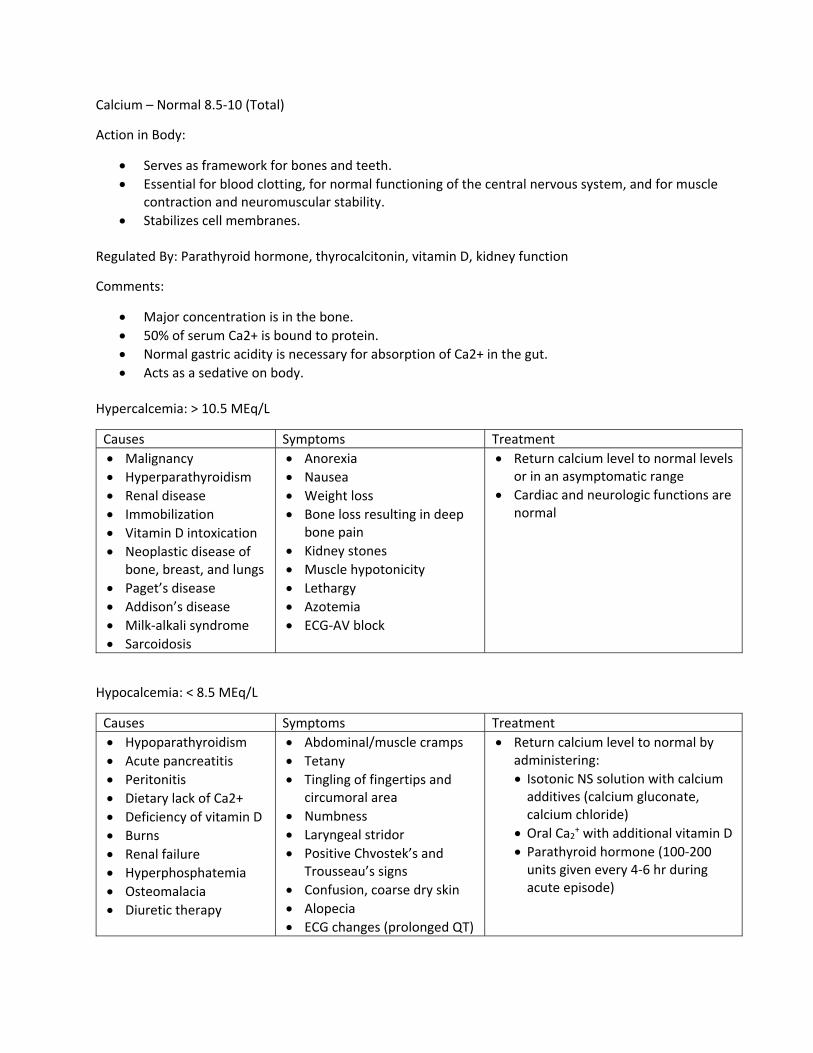
Hypercalcemia: > 10.5 MEq/L
Causes Symptoms Treatment
Malignancy
Hyperparathyroidism
Renal disease
Immobilization
Vitamin D intoxication
Neoplastic disease of bone, breast, and lungs
Paget’s disease
Addison’s disease
Milk‐alkali syndrome
Sarcoidosis
Anorexia
Nausea
Weight loss
Bone loss resulting in deep bone pain
Kidney stones
Muscle hypotonicity
Lethargy
Azotemia
ECG‐AV block
Return calcium level to normal levels or in an asymptomatic range
Cardiac and neurologic functions are normal
Hypocalcemia: < 8.5 MEq/L
Causes Symptoms Treatment
Hypoparathyroidism
Acute pancreatitis
Peritonitis
Dietary lack of Ca2+
Deficiency of vitamin D
Burns
Renal failure
Hyperphosphatemia
Osteomalacia
Diuretic therapy
Abdominal/muscle cramps
Tetany
Tingling of fingertips and circumoral area
Numbness
Laryngeal stridor
Positive Chvostek’s and Trousseau’s signs
Confusion, coarse dry skin
Alopecia
ECG changes (prolonged QT)
Return calcium level to normal by administering:
Isotonic NS solution with calcium additives (calcium gluconate, calcium chloride)
Oral Ca2+ with additional vitamin D
Parathyroid hormone (100‐200 units given every 4‐6 hr during acute episode)
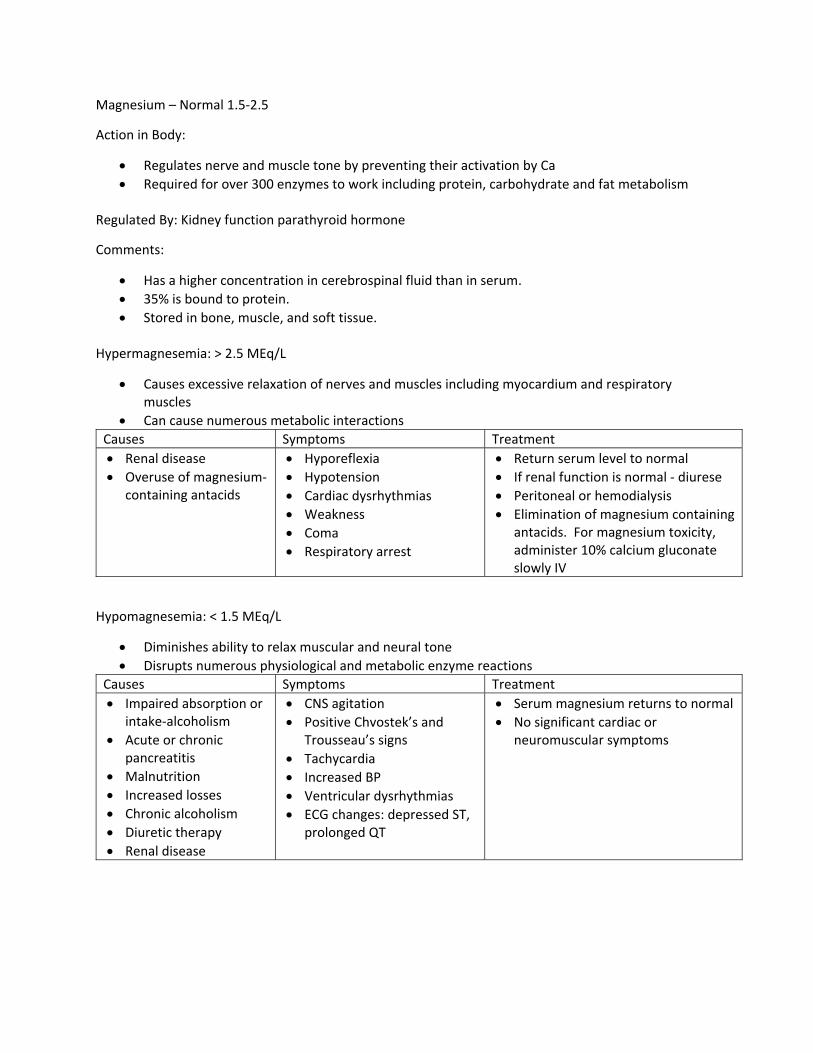
Magnesium – Normal 1.5‐2.5
Action in Body:
Regulates nerve and muscle tone by preventing their activation by Ca
Required for over 300 enzymes to work including protein, carbohydrate and fat metabolism
Regulated By: Kidney function parathyroid hormone
Comments:
Has a higher concentration in cerebrospinal fluid than in serum.
35% is bound to protein.
Stored in bone, muscle, and soft tissue.
Hypermagnesemia: > 2.5 MEq/L
Causes excessive relaxation of nerves and muscles including myocardium and respiratory muscles
Can cause numerous metabolic interactions
Causes Symptoms Treatment
Renal disease
Overuse of magnesium‐containing antacids
Hyporeflexia
Hypotension
Cardiac dysrhythmias
Weakness
Coma
Respiratory arrest
Return serum level to normal
If renal function is normal ‐ diurese
Peritoneal or hemodialysis
Elimination of magnesium containing antacids. For magnesium toxicity, administer 10% calcium gluconate slowly IV
Hypomagnesemia: < 1.5 MEq/L
Diminishes ability to relax muscular and neural tone
Disrupts numerous physiological and metabolic enzyme reactions
Causes Symptoms Treatment
Impaired absorption or intake‐alcoholism
Acute or chronic pancreatitis
Malnutrition
Increased losses
Chronic alcoholism
Diuretic therapy
Renal disease
CNS agitation
Positive Chvostek’s and Trousseau’s signs
Tachycardia
Increased BP
Ventricular dysrhythmias
ECG changes: depressed ST, prolonged QT
Serum magnesium returns to normal
No significant cardiac or neuromuscular symptoms
Phosphorus – Normal 2.7‐4.6 Mg/dL
Contained in the body as phosphate
85% found in teeth & bones
Function o component of cell membrane o muscle function o neuro function o carb, fat, protein metabolism o Ingredient in compound found in RBCs o Buffers acids and bases o Promotes energy transfer through formation of ATP o WBC phagocytosis o Platelet function
Electrolyte Disturbances and ECG Changes
• p flat ‐ hyperkalemia
• pr prolonged – hyperkalemia, hypermagnesemia
• qrs widened – hyperkalemia, hypermagnesemia
• qt prolonged – hypocalcemia
• st prolonged – hypocalcemia
• st shortened – hypercalcemia
• st depressed – hypokalemia, hypomagnesemia
• t widened – hypercalcemia
• t tall – hyperkalemia, hypomagnesemia
• t inverted – hypokalemia
• shallow, flat T ‐ Hypokalemia
• u prominent ‐ hypokalemia
5/26/2020
1
Respiratory Failure
By
Beth Brown, BSN, RN, CCRN-K
Respiratory System
Respiratory system includes:>CNS (Medulla / chemoreceptors)>Peripheral nervous system (phrenic nerve)>Respiratory muscles>Chest wall>Lungs>Upper airway>Bronchial tree>Alveoli>Pulmonary vasculature>Heart
Alveolar Gas Exchange
Type I epithelial cells Gas exchange90% of alveolar lining
Type II epithelial cellsSurfactant production10% of alveolar lining
Respiratory Failure
Definition: A syndrome in which the respiratory system fails in one or more of its gas exchange functions
or
“inability of the lungs to meet the metabolic demands of the body. This can be from failure of tissue oxygenation and/or failure of CO2 homeostasis.”
5/26/2020
2
V/Q mismatch—
normal: (4L vent/ 5L perf) normal V/Q ratio of 0.8 responsive to oxygen therapy – contact
between air and blood
Intrapulmonary shunt—
a lung unit that is not ventilated, but continues to be perfused
alveoli collapsed / filled with mucus or fluid
clinical effect “refractory hypoxemia” not responsive to oxygen therapy –
altered contact between air and blood
Classifications
Type I -Hypoxemic respiratory failureMost common PO2 <60From lung diseases involving fluid filling or
collapse of alveoli
Type II -Hypercapneic resp failure Inadequate airflow / hypoventilation
syndromePCO2 > 50 (in non-chronic pt)Diseases of muscle weakness, respiratory
center, or lung disease
Classifications
Type I failure PneumoniaARDSPulmonary edema/
CHFAtelectasis Interstitial diseases/
fibrosis
Type II failureCOPDDrug ODNeuromuscular
diseasesChest wall
abnormalitiesHead or spinal cord
injury
5/26/2020
3
Classifications Type III – Perioperative respiratory failure –
increased atelectasis due to low FRC in the setting of abnormal wall mechanics
Type IV – Shock – patients who are intubated and ventilated in the process of resuscitation of shock
Acute vs ChronicAcuteDevelops over
minutes to hourspH is less likely to
be compensated
ChronicDevelops over
several days or longerAllows time for
renal compensation, so pH can be normal
Diagnosis of Respiratory FailureClinical picture – air hunger signs, hypoxia,
DiagnosisAcute onset (6 hrs to 1 week after event)Bilateral infiltrates on CXRGround glass opacities on CTP/F ratio (PO2/FIO2 in decimal) –Measurement
of how well lungs are oxygenating blood
200-300 - mild ARDS 100-200 - moderate ARDS
<100 – severe ARDS
5/26/2020
8
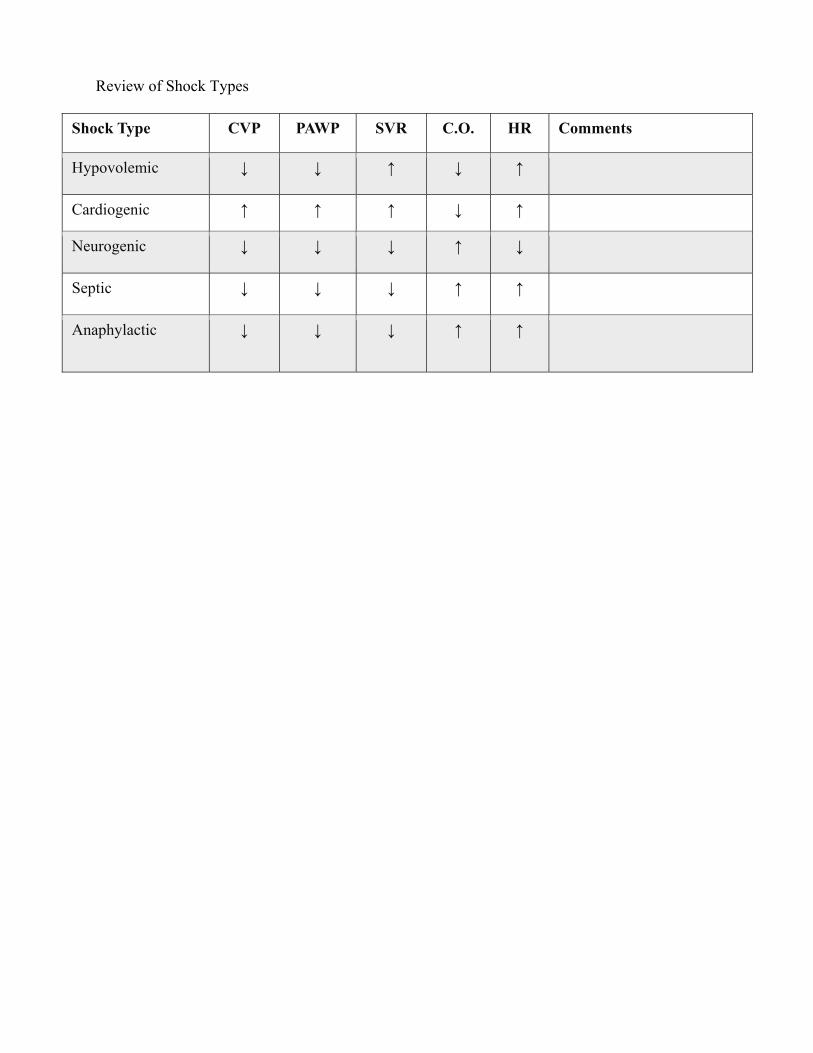
A screenshot of chest radiographs of a man suspected to have COVID-19. (Obtained by ProPublica via the Radiological Society of North America, cited in the paper “Severe Acute Respiratory Disease in a Huanan Seafood Market Worker: Images of an Early Casualty” by Lijuan Qian, JieYu and Heshui Shi.)
ManagementLow tidal volume ventilation (LTVV)
>protects from alveolar over-distention>Based on predicted body weight (PBW)>Target tidal volume 4-6 ml/kg with ARDS>Increase set rate to keep up minute
ventilation>Plateau pressure goal <30
5/26/2020
9
Predicted Body WeightMales
50kg + 2.3(height in inches-60)
Females45.5kg +2.3 (height in inches-60)
Management, cont…
PEEP>may use in higher levels >reduces atelectasis>reduces shear force injury>maintains alveolar recruitment>decreases release of inflammatory
PRONE POSITIONINGPROSEVA study 2013 showed promising
results for select population in severe ARDSP/F ratio < 150, FIO2 >.60, Peep >5Applied early (<36 hrs after intubation)Mean time of 17 hrs per day in proneAverage of 73% of time in ICU in prone
position
> Showed reduction in 28 day mortality(16% vs 33%)
> Showed reduction in 90 day mortality (24% vs 41%)
5/26/2020
11
Neuromuscular Blockade (NMB) Paralytic drug to decrease O2 demand To prevent patient-ventilator dyssynchrony For short term use, typically less than 48 hoursCan cause myopathy, increased rehabilitation
timeMUST use with sedationOften needed with alternate modes of
Steroids – data conflicting –depends on cause - use early if done (<14 days from onset.) More trials ongoing
Macrolide antibiotics (Azithromycin)-LARMA trial showed lower 180 day mortality - antimicrobial / anti –inflammatory effects. Warrants clinical trial.
Vitamin D – PETAL network – trial underway
Conservative fluid management – preferred unless can’t do –i.e. hypotension / poor organ perfusion.
5/26/2020
1
Pulmonary Disorders
B E T H B R O W N , B S N , R N , C C R N - K
Pneumonia
Inflammatory process of the lung parenchyma, including alveolar spaces and interstitial tissue
Produced by an infectious agent
Inflammatory exudate fills alveoli
Produces consolidation Second most common
cause of hospitalization Most common infectious
cause of death
Pneumonia Risk Factors
Older age (>65) ~ 3 x higher risk than general population Chronic co-morbidities COPD, bronchiectasis, asthma, cystic fibrosis Chronic Heart disease Stroke Diabetes, malnutrition Immunocompromised
Influenza A & B Coronaviruses Rhinoviruses Adenoviruses RSV (Respiratory Syncytial Virus) Human Metapneumovirus Human bocaviruses Hantavirus
Fungi (seen more in immunocompromised pts) Cryptococcus Histoplasmosis Coccidioides Blastomyces Aspergillus Pneumocystis jirovecii
CAP Bioterrorism agents Bacillus anthracis (Anthrax) Yersinia pestis (plague) Francisella tularensis (tularemia) C. burnetii (Q fever) Ricin
5/26/2020
3
HAP/VAP Increased incident of antimicrobial resistance MDR- multi-drug resistant - nonsusceptibility to at least one
agent in three different classes XDR- extensively drug resistant - nonsusceptibility to at least
one agent in all but 2 classes PDR – pan-drug resistant – nonsusceptibility to all
antimicrobial agents that can be used for treatment Most HAP occurs in non-ventilated patients VAP rates on steady decline in US VAP prolongs ventilation days from 7.6 to 11.5 on
average, and LOS from 11.5 to 13.1 days VAP excess cost approximately $40,000 per pt.
HAP/VAP Related to number and virulence of micro-organisms
entering lower respiratory tract Aspiration of gastric contents (pneumonitis / infection) Microaspiration of colonized OP tract organisms ETT - facilitates aspiration Hospitalized pts often colonized with microorganisms
from hospital environment Possibly from contaminated reservoirs, respiratory
devices, equipment Contaminated hands of healthcare personnel Questionable adverse effect of PUD prophylaxis ?
Suspicion for pseudomonas or recent hospitalization / antibiotics Antipseudomonal Beta lactam (i.e. zosyn, meropenem) +
fluoroquinolone
Suspicion / known MRSA – add Vancomycin or linezolid
Glucocorticoids – controversial – maybe for exaggerated inflammatory response
Procalcitonin levels to help guide antibiotic discontinuation
5/26/2020
5
HAP/ VAP Prevention
Hand hygiene HOB elevated Oral care (chlorhexidine) / brush teeth Subglottic suctioning Judicious use of PUD prophylaxis Antimicrobial stewardship Weaning / extubation as early as possible Daily awakening trials Assess weaning appropriateness – RSBI, spontaneous trials
Avoid saline lavages Patient position changes
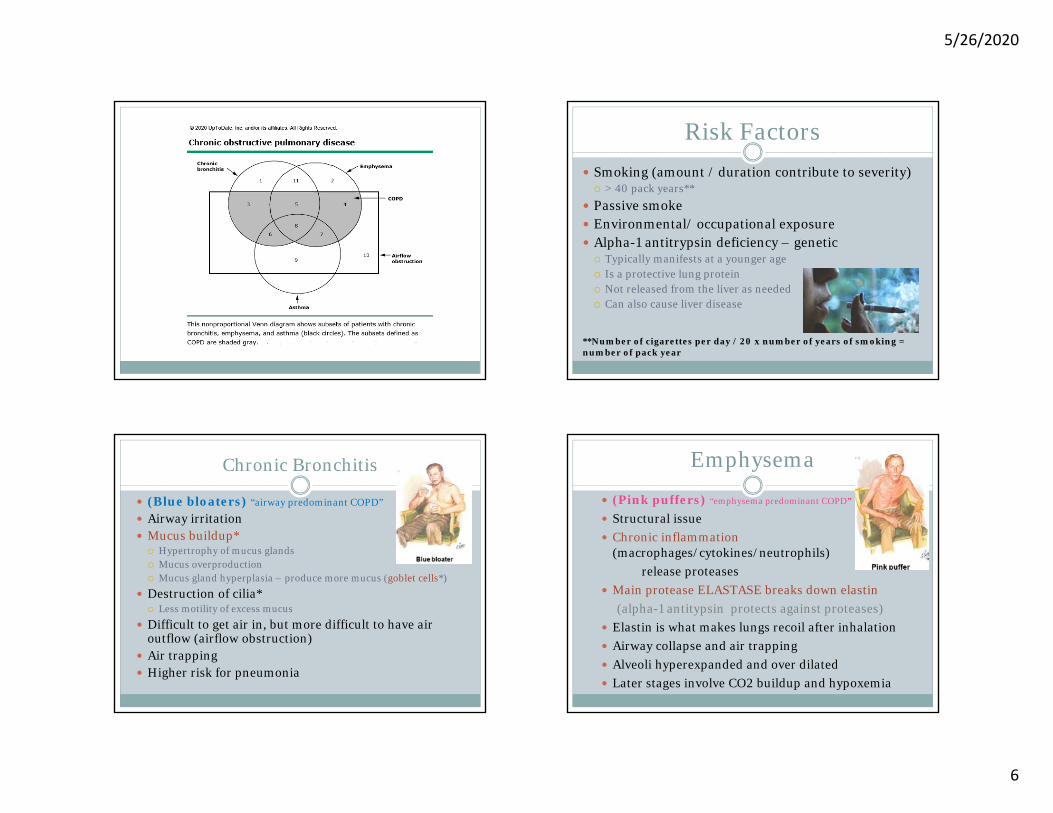
COPD / SubtypesChronic BronchitisEmphysemaChronic obstructive asthma *asthma with
reversible airflow obstruction is NOT considered COPD
“COPD is a common, preventable, and treatable disease characterized by persistent respiratory symptoms and airflowlimitation that is due to airway and/or alveolar abnormalities
usually caused by significant exposure to noxious particlesor gases.”
(GOLD definition- Global Initiative for Chronic ObstructiveLung Disease)
Passive smoke Environmental/ occupational exposure Alpha-1 antitrypsin deficiency – genetic Typically manifests at a younger age Is a protective lung protein Not released from the liver as needed Can also cause liver disease
**Number of cigarettes per day / 20 x number of years of smoking = number of pack year
Chronic Bronchitis
(Blue bloaters) “airway predominant COPD”
Airway irritation Mucus buildup* Hypertrophy of mucus glands Mucus overproduction Mucus gland hyperplasia – produce more mucus (goblet cells*)
Destruction of cilia* Less motility of excess mucus
Difficult to get air in, but more difficult to have air outflow (airflow obstruction)
Main protease ELASTASE breaks down elastin(alpha-1 antitypsin protects against proteases)
Elastin is what makes lungs recoil after inhalation Airway collapse and air trapping Alveoli hyperexpanded and over dilated Later stages involve CO2 buildup and hypoxemia
Centriacinar (centrilobular) – dilation or destruction of the respiratory bronchiole (center portion of acinar
Panacinar – enlargement or destruction of all parts of the acinus (most commonly seen with alpha-1 antitrypsin deficiency)
Distal acinar (paraseptal) – alveolar ducts predominantly affected (air pockets very distal “blebs”– near pleura- high risk for pneumothorax)
ACINUS=collectively refers to bronchiole, alveolar ducts, alveolar sacs, and alveoliPARENCHYMA=above plus capillaries, and instersititum
COPD symptoms
Dyspnea (initially may be only with exertion)
Accessory muscle use Chronic cough Insidious onset of sputum production Gradual decline in activity – easily fatigued Morning is the worst time of day for them
5/26/2020
8
Heart Effects
Group 3 Pulmonary HTN (groups based on etiology) Chronic lung disorders (COPD, ILD, overlap syndromes, OSA,
etc.
Defined as mean PA pressure > 20 mmHg at rest > 35 considered severe
Cor pulmonale Complication of PH PH induced structural changes (hypertrophy or dilatation) or
impaired function of RV associated with chronic lung disease &/or hypoxemia
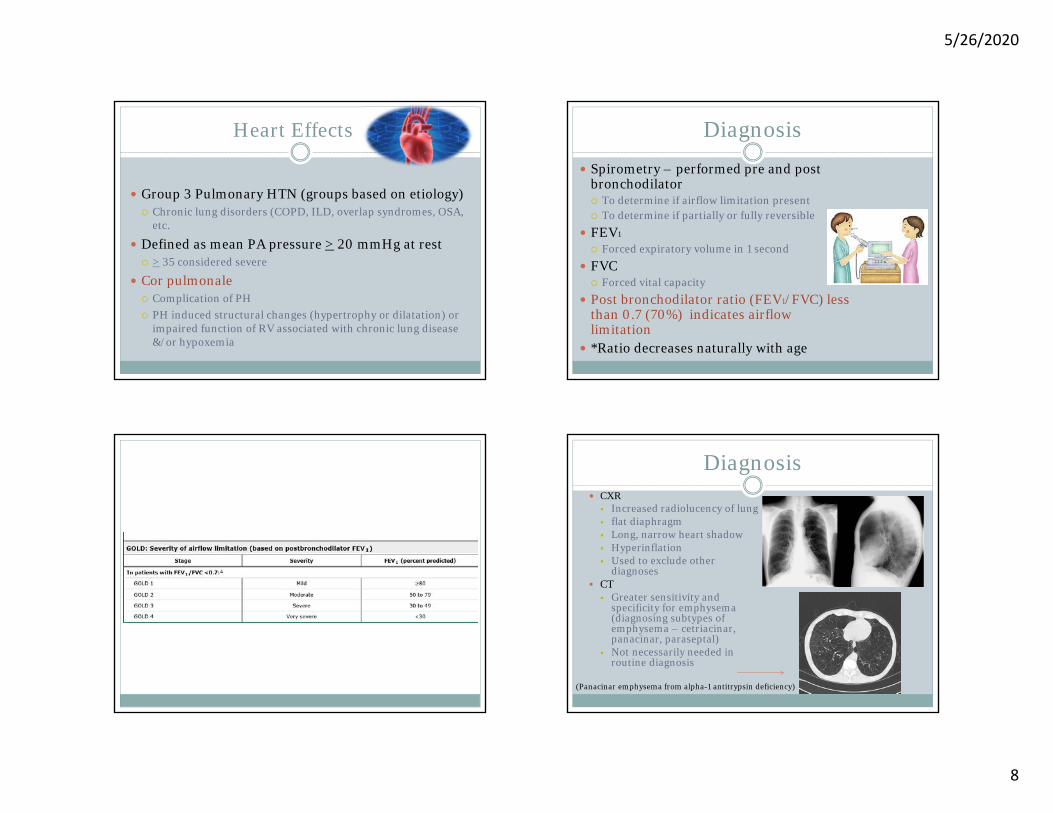
Diagnosis
Spirometry – performed pre and post bronchodilator To determine if airflow limitation present To determine if partially or fully reversible
FEV1
Forced expiratory volume in 1 second
FVC Forced vital capacity
Post bronchodilator ratio (FEV1/FVC) less than 0.7 (70%) indicates airflow limitation
*Ratio decreases naturally with age
Diagnosis CXR Increased radiolucency of lung flat diaphragm Long, narrow heart shadow Hyperinflation Used to exclude other
diagnoses CT Greater sensitivity and
specificity for emphysema (diagnosing subtypes of emphysema – cetriacinar, panacinar, paraseptal)
Not necessarily needed in routine diagnosis
(Panacinar emphysema from alpha-1 antitrypsin deficiency)
5/26/2020
9
Exacerbations
Worsening of chronic condition Increase in dyspnea Increase in productive cough Hypoxemia Respiratory acidosis Respiratory failure
shown beyond standard treatment + associated with n/v, tremor, arrhythmias
Nebulized magnesium- no effect on FEV1 in COPD exacerbation
Chest physiotherapy (percussion, vibration, IPPB, postural drainage, etc) – not beneficial and may provoke bronchoconstriction
5/26/2020
10
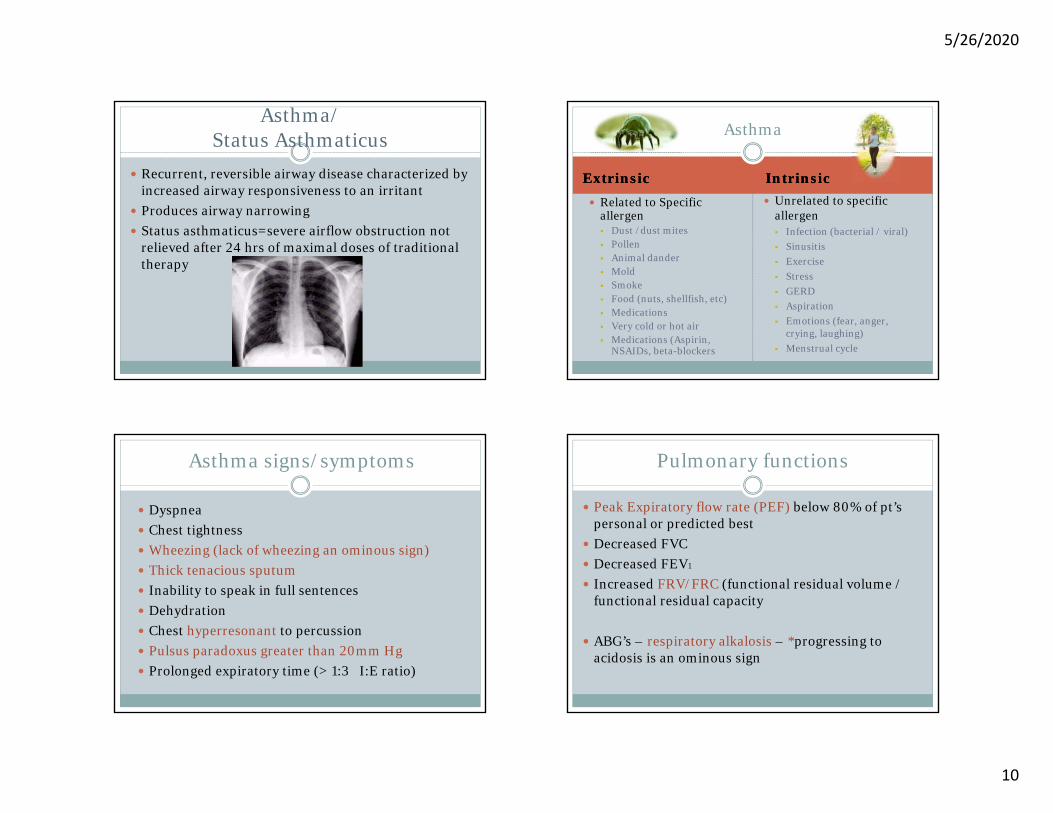
Asthma/Status Asthmaticus
Recurrent, reversible airway disease characterized by increased airway responsiveness to an irritant
Produces airway narrowing Status asthmaticus=severe airflow obstruction not
relieved after 24 hrs of maximal doses of traditional therapy
Asthma
ExtrinsicExtrinsic IntrinsicIntrinsic Related to Specific
allergen Dust /dust mites Pollen Animal dander Mold Smoke Food (nuts, shellfish, etc) Medications Very cold or hot air Medications (Aspirin,
NSAIDs, beta-blockers
Unrelated to specific allergen Infection (bacterial / viral) Sinusitis Exercise Stress GERD Aspiration Emotions (fear, anger,
crying, laughing) Menstrual cycle
Asthma signs/symptoms
Dyspnea Chest tightness Wheezing (lack of wheezing an ominous sign) Thick tenacious sputum Inability to speak in full sentences Dehydration Chest hyperresonant to percussion Pulsus paradoxus greater than 20mm Hg Prolonged expiratory time (> 1:3 I:E ratio)
Pulmonary functions
Peak Expiratory flow rate (PEF) below 80% of pt’spersonal or predicted best
Sub-Massive Hemodynamically stable Sudden onset of dyspnea at
reset or with exertion Chest discomfort / pleuritic
pain Flu-like symptoms Fever, scattered crackles Restlessness, apprehension Tachypnea / tachycardia Cough (hemoptysis) Orthopnea Can be asymptomatic
Massive Hemodynamically unstable Drop in SBP < 90mm/Hg or
> 40mm/Hg drop from baseline
Shock / hypotension Impending doom Severe dyspnea Hemoptysis Perspiration Tachycardia JVD Sudden death
Factors for Increased Mortality
RV dysfunction Elevated BNP PE with co-existing DVT RV thrombus Elevated serum troponin Hyponatremia
5/26/2020
14
Diagnosing PE
Pulmonary angiography – definitive, but also invasive
CT Angio (PE protocol) – definitive and non-invasive
Diagnosing PE
VQ scan – non-invasive, suggestive, not definitive Venous doppler – not definitive - tells if DVT is present. D-dimer elevated– not definitive – tells if by-products of a clot
are present Echo – dilated RV – massive PE (McConnell’s Sign) EKG – S1Q3T3 sign or new RBBB, a-fib/flutter, right axis shift,
sinus tach, T wave inversions inV1-V4 (RV strain pattern)
68 yo woman with new onset dyspnea on exertion
Prominent S in lead IQ wave /inverted T in lead III
DOACs Rivaroxaban (Xarelto) Apixaban (Eliquis) Dabigatran (Pradaxa) Warfarin (Coumadin) - Vit K antagonist
Fat embolus
From long bone, sternal, pelvic fracture From major soft tissue trauma Fat Embolus Syndrome (FES) Triad: Respiratory compromise – hypoxemia, dyspnea,
tachypnea Neurologic abnormalities – confusion, MS changes,
seizures Petechial rash – in 20-50% of cases – usually found in
nondependent regions of the body, i.e. head, neck, anterior thorax, axillae, and sub-conjunctiva
Treatment of Fat Embolus
Corticosteroids – give within 12 hrs of injury to prevent fat embolus
O2 Anticoagulation IVC filter for high risk patients
5/26/2020
16
Air Embolus
Usually enter via venous system (lower pressure) At risk with surgical wound > 5 cm above right atrium Neurological and ENT procedures Vascular catheters (insertion or removal) Blunt or penetrating trauma to chest Positive pressure ventilation Rapid ascent in scuba divers
Treatment Position head down, left side Hyperbaric oxygen chamber High FIO2 (reabsorbs faster) Supportive






































































![HISK 10 ANemia HEMOLITIK.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/course/download/1110000096-hematology-and-immunology... · Autoimmune hemolytic anemia caused byAutoimmune hemolytic](https://static.documents.pub/doc/80x56/5c7c94c409d3f23a2a8b4fbf/hisk-10-anemia-read-only-ocwusuacidocwusuacidcoursedownload1110000096-hematology-and-immunology.jpg)


