47
Hemodynamic disturbances Dr .Sura Aldewachi Department of Pathology Ninavah College of Medicine

Hemodynamic disturbances
Dr .Sura Aldewachi
Department of Pathology
Ninavah College of Medicine

OdemaApproximately 60% of body weight is water, of which 2/3 is intracellular, 1/3extracellular(mainly interstitial) only 5% of total body water is in blood plasma.
Odema means increased fluid in the interstitial tissue spaces.
Pathogenesis:
There are 2 opposing factors which govern the movement of the fluid between vascular &interstitial spaces:
1. Hydrostatic pressure i.e. capillary blood pressure encouraging the passage of fluid through the capillary wall to the extra vascular compartment =35mmHg .
2. Oncotic pressure (op) i.e. .the plasma protein encourages the↑ retention of fluid in the capillaries to maintain osmotic equilibrium, this pressure Is equivalent to 25mmHg.

At the arterial end the hydrostatic Pr is greater than theOP→ fluid is forced out the capillaries of themicrocirculation. The reverse occurs at the venous end &thefluid is attracted into the vessels.
A small amount of fluid enters the lymphatics.

Odema may be localized to a part of the body or generalized
Localized odema:
1. Acute inflammation: odema due to local effects of
inflammatory mediators---increase vascular permeability.→
accumulation of protein rich fluid (exudates) in the interstitial
spaces.
2. Hypersensitivity(allergic)odema due to increase ↑vascular
permeability.
3. Venous obstruction →venous congestion →↑capill. perm.
→transudation of fluid e.g. in the legs during pregnancy due
to pressure on the veins by the gravid uterus. Impaired
venous out flow e.g. secondary to deep venous thrombosis
(DVT) in the lower extremities →oedema restricted to the
affected leg .

4. Lymphatic :
due to obstruction of lymphatic drainage e.g. by tumor
cells ,trauma ,by radiation or by inflammation or injury
e.g. Filariasis →fibrosis of lymphatic vessels & L.N. of
the inguinal region →odema of lower limbs
(elephantiasis).In carcinoma of breast →infiltration
&obstruction of superficial lymphatics → odema of
overlying skin →"peau d orange". also after surgery or
irradiation of breast cancer →sever odema of the arm.

Generalized Odema
Either due to:
1. Increased hydrostatic pressure: most commonly in
congestive heart failure affecting the right ventriclular
cardiac function.
2. Reduced plasma oncotic pressure:
Hypoalbuminaemia ,this result from
1. excessive loss of albumin. an important cause of albumin loss is nephrotic syndrome characterized by → excessive loss of protein (albuminurea)→ generalized odema.
2. Reduced albumin synthesis: e.g. in diffuse liver diseases as in cirrhosis , or as consequence of protein malnutrition ,protein –loosing enteropathy .
Morphology:
Odema is most easily recognized grossly .
Microscopically →oedema fluid generally manifested as clearing &separation of the extracellular matrix elements.
Pathophysiology:
oedema results from;
1. Increased hydrostatic pressure,
2. Reduced plasma osmotic pressure,
3. Lymphatic obstruction.
4. Sodium and water retention.
Pulmonary odema:
is common clinical problem & frequently follow Left side heart failure & The lungs are typically 2-3 times their normal wt..
On sectioning frothy &sometimes blood-tinged fluid representing a mixture of air and oedema fluid and extravasated RBCs.

Pitting edema of the ankle joint

Lymphadema : non pitting edema of the legs

Hyperemia and congestion Both terms indicate a local increased volume of blood in a
particular tissue
Hyperemia is an active process, the affected tissue is
red, resulting from sympathetic stimulation which causes
arteriolar dilatation &local redness produced owing to the
engorgement of oxygenated blood
e.g. pathological as in acute inflammation
physiological as in exercise
Congestion is a passive process, which could be
localized or generalized, and the affected tissue is red-
blue (cyanosis). congestion is a passive dilatation of
veins as a result of partial obstruction to the venous
return ,this will cause bluish coloration due to
accumulation of deoxygenated blood .

Venous congestion can be either general or local.
General venous congestion:
Where the whole venous return is impaired by chronic obstructions e.g.
Pulmonary congestion: in cases of left sided heart failure as in mitral stenosis →raised pressure in the pulmonary veins →alveolar capillaries become tortous &distended with red cells →break down of RBCs &phagocytosis of intra-alveolar red cell debris leading to accumulation of (hemosidrin –laden macrophages) (heart failure cells) with transudate in the alveolar spaces esp the posterior &basal lobes of the lungs).
Morphology
grossly, the cut surface is hemorrhagic and wet.
Microscopically, there is engorgement of capillaries by blood.

Pulmonary congestion with dilated capillaries and leakage of blood into alveolar
spaces leads to an increase in hemosiderin-laden macrophages,
as seen here.

Congestion of the liver
usually follows right sided heart failure →liver moderately enlarged &tender.
Micro:red cells accumulate in the sinusoids around the central veins surrounded by the peripheral hepatocytes which are better oxygenated because of their proximity to hepatic arterioles so they are less hypoxic &may only develop fatty changes giving it an appearance called "nut meg liver".
Local venous congestion: follows mechanical interference with the venous drainage from an organ
e.g. limbs in DVT caused by Venous thrombosis .
compression of a vein by tumor or bandage.
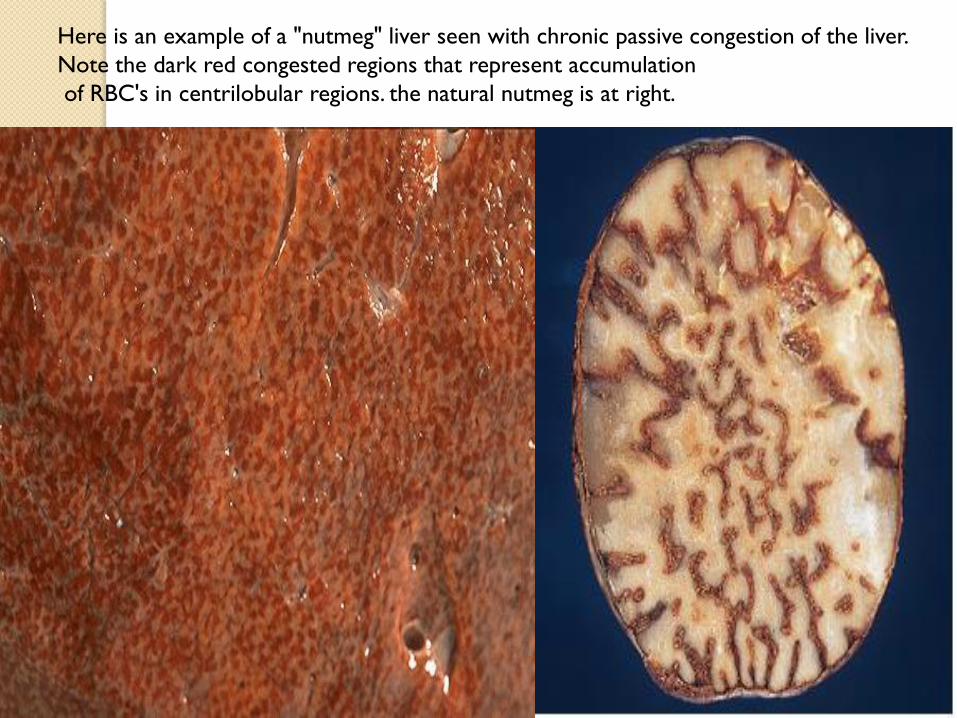
Here is an example of a "nutmeg" liver seen with chronic passive congestion of the liver.
Note the dark red congested regions that represent accumulation
of RBC's in centrilobular regions. the natural nutmeg is at right.

Microscopically, the nutmeg pattern results from congestion around
the central veins, as seen here. This is usually due to a "right sided"
heart failure.

Hemostasis and thrombosisNormal hemostasis means
1. Maintaining blood in a fluid, clot-free state in normal vessels.
2. Rapid localized plug at a site of vascular injury.
Thrombosis, is the pathologic opposite to hemostasis, and it means an inappropriate activation of normal hemostatic process.
the general sequence of events AFTER INITIAL INJURY include:
1. Brief period of arteriolar vasoconstriction.
2. Primary hemostasis (transient platelet plug).
3. Secondary hemostasis (activation of coagulation cascade).
4. Permanent plug.

Both hemostasis and thrombosis are regulated by;
1. Vascular wall:(Anti-platelet, anticoagulant ,fibrinolytic
properties and pro-coagulant effects).
2. Platelets: play a central role in hemostasis, (adhesion,
secretion, aggregation).
3. Coagulation cascade.
is essentially a series of enzymatic conversions, turning
inactive pro-enzymes into active enzymes and culminating
in thrombin formation.
Thrombin converts soluble fibrinogen into insoluble fibrin.
Beside inducing coagulation, activation of the clotting
cascade also sets into motion a fibrinolytic cascade that
limits the size of the final clot.

Thrombosis, Virchow triad
Three primary influences predispose to thrombus formation (Virchow triad);
1. Endothelial injury, leading to;
Exposure of sub-endothelial extracellular matrix.
Adhesion of platelets
2. Stasis or turbulence of blood flow, by causing;
a. Endothelial injury .
b. Disruption of laminar flow.
c. Preventing dilution of activated clotting factors by fresh blood.
d. Retarding the inflow of clotting factor inhibitors.
3. Blood hypercoagulability
Morphology, thrombi may develop anywhere in thecardiovascular system.
Grossly and microscopically have apparent laminations(lines of Zahn), produced by alternating pale layers ofplatelets admixed with some fibrin and darker layerscontaining more red cells.
Arterial thrombi are usually occlusive, are firmly attachedto the wall, and are gray-white and friable.
Venous thrombi are almost invariably occlusive, areless firmly attached to the wall, and are red.
Postmortem clots are gelatinous, dark red, usually notattached to the wall, and lack lines of Zahn.
Mural thrombi, are those attached to the wall of aspacious cavity.
Vegetations, are thrombi formed on heart valves.

Fate of the thrombus, include
1. Propagation.
2. Embolization.
3. Dissolution.
4. Organization and re-canalization.
Thrombi are significant because;
1. They cause obstruction of vessels.
2. They are possible sources of emboli.

Mural thrombi of the heart
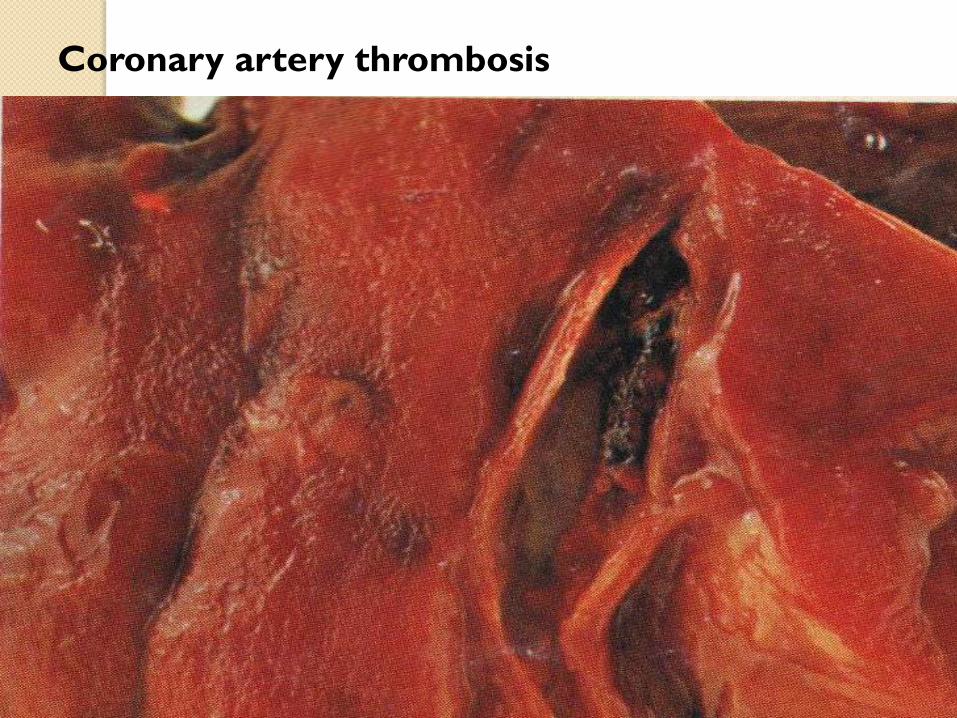
Coronary artery thrombosis

Cross section through the coronary artery showing the thrombus
obstructing the whole lumen.

Microscopic appearance of thrombus' the line of Zahn’ These lines represent
layers of red cells, platelets, and fibrin which are laid down in the vessel as
the thrombus form.

Fates of thrombus : propagation, resolution, organization,
recanalization & embolization.
Note the organization & the recanalization of the
thrombus in these two slides.

Atheroma with organized thrombus: the
thrombus here is replaced by granulation tissue.
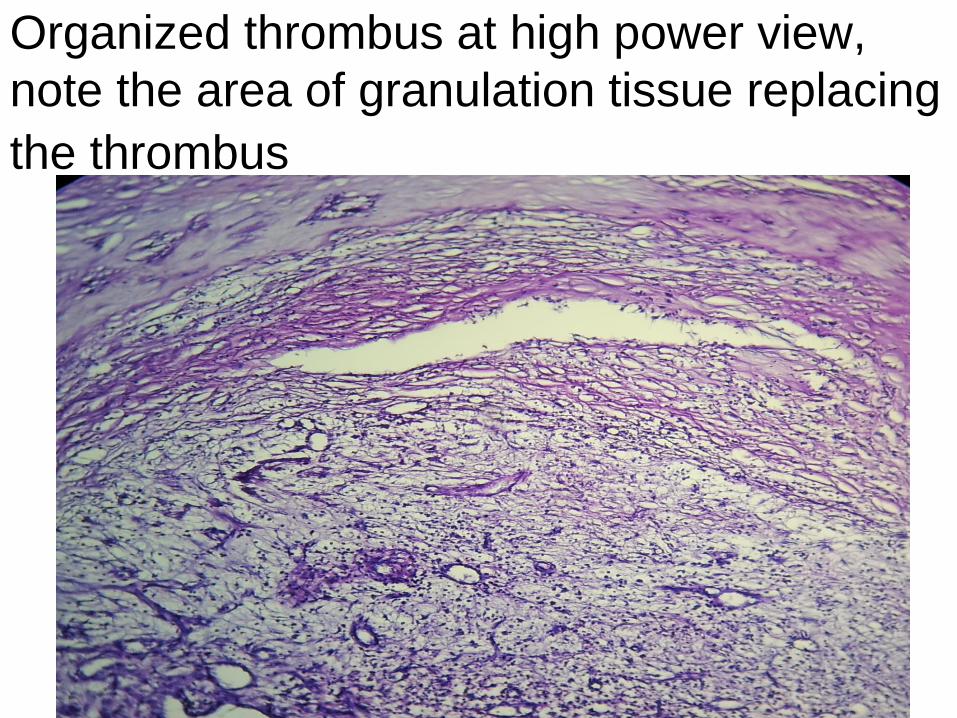
Organized thrombus at high power view,
note the area of granulation tissue replacing
the thrombus

Embolism
is a detached intravascular solid, liquid, or gaseous mass that is carried by the blood to a site distant from its point of origin.
There are many types of emboli;
1. Thrombo-emboli.
2. Fat.
3. Gas (air, nitrogen).
4. Atheroma -emboli.
5. Tumor fragments.
6. Bone marrow.
7. Foreign body (bullet).
The potential effect of embolism is ischemic necrosis (infarction)

Pulmonary thrombo-embolismin more than 95% of instances, venous emboli ,,,deep leg
vein thrombi, are the source.
Depending on the size of the embolus;
1. It may occlude the main pulmonary artery.
2. Impact across the bifurcation (saddle embolus).
3. Or pass out into the smaller branching arterioles.
4. Rarely, an embolus may pass through an inter-atrial or inter-ventricular defect to gain access to the systemic circulation (paradoxical embolism).
Clinical consequences1. Most pulmonary emboli are silent.2. Sudden death (acute corpulmonale).3. Obstruction of medium-sized arteries may result in pulmonary hemorrhage.4. Obstruction of small end-arterioles result in infarction.5. Multiple emboli over time may cause chronic corpulmonale.

Systemic thrombo-embolism
they may originate from;
1. Intra-cardiac mural thrombi, (about 80% of emboli).
2. Aortic aneurysm.
3. Thrombi on ulcerated atherosclerotic plaques.
4. Fragmentation of a valvular vegetation.
5. Paradoxical emboli.
6. Up to 15% of emboli are of unknown origin.
The main sites involved are
1. Lower extremities (75%).
2. Brain (10%).
3. Intestines.
4. Kidneys.
5. Spleen.
6. Upper extremities
Fat embolism
it may result from;
1. Fractures of long bones (most common).
2. Soft tissue trauma and burns (rare).
Gas embolism
air may enter the circulation during;
1. Obstetric procedures.
2. Chest wall injury.
In excess of 100 cc is required to have a clinical effect.
The bubbles produce physical obstruction to vessels,
and may lead to infarction.

Amniotic fluid embolism
it is an uncommon complication of labor.
The underlying cause is the infusion of amniotic fluid or
fetal tissue into the maternal circulation via a tear in the
placental membranes or rupture of uterine veins.
1. Sudden severe dyspnea.
2. Cyanosis.
3. Hypotensive shock.
4. Seizure and coma.
5. If the patient survives, pulmonary edema and DIC
develop.

Pulmonary embolus obstructing the main pulmonary
artery
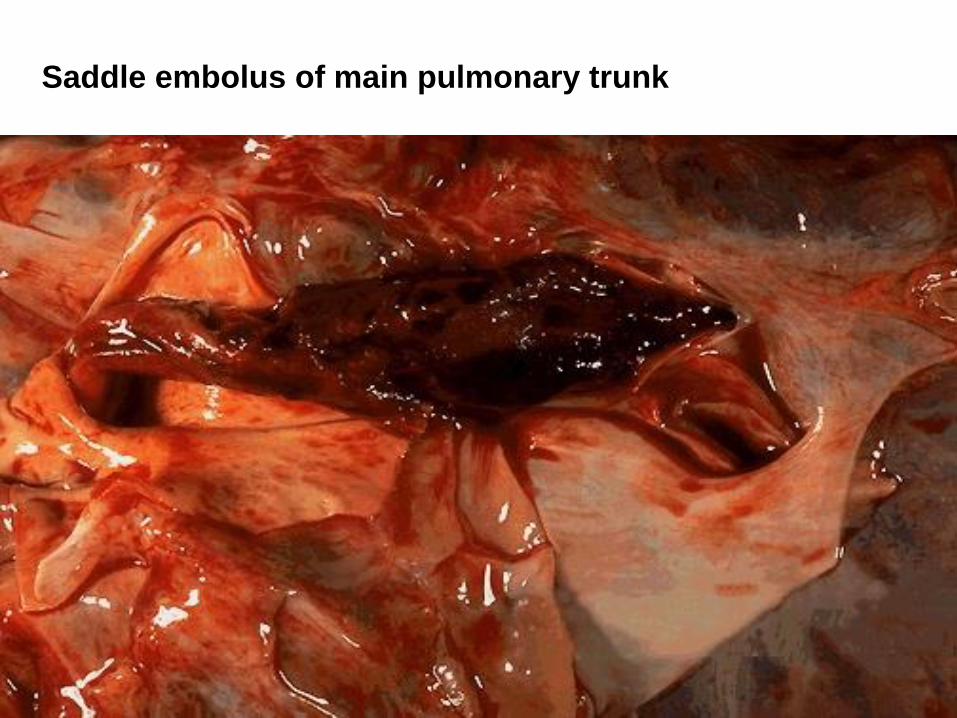
Saddle embolus of main pulmonary trunk

This is the microscopic appearance of a pulmonary thromboembolus in a large
pulmonary artery. There are interdigitating areas of pale pink and red that form the
"lines of Zahn" characteristic for a thrombus .

Paradoxical embolus through a patent foramen ovale

Infarction :
It is an ischemic necrosis caused by occlusion of either the
arterial supply or the venous drainage.
Causes, include;
1. Thrombosis or embolism (99%).
2. Local vasospasm.
3. Expansion of atheroma.
4. Extrinsic compression of a vessel (tumor, twisting, edema,
hernia).
5. Traumatic rupture.
Morphology
infarcts are classified
1. On the basis of their color; red (hemorrhagic)&white
(anemic)
2. On the basis of presence or absence of infection;
septic& sterile.

Red infarcts occur in the following situations;
1. Venous occlusion (testis, ovary).
2. Loose tissue.
3. Tissues with dual circulation.
4. Previously congested tissues.
5. Re-established blood flow
White infarcts
occur in arterial occlusion in solid organs with end-arterial circulation.
Most infarcts tend to be wedge-shaped, with the occluded vessel at the apex and the periphery of the organ forming the base.
At the outset, all infarcts are poorly defined and slightly hemorrhagic. Over the course of few days, they become more firm and brown. Most infarcts are replaced by scar tissue.
In septic infarcts, abscess is produced.
Clinical correlation
The consequences of a vascular occlusion can range
from no or minimal effect, to death of a tissue or
even the individual.
The factors that influence the outcome include;
1. Nature of the vascular supply.
2. Rate of development of occlusion.
3. Vulnerability to hypoxia.
4. Oxygen content of blood

Pulmonary infarction produced by a medium-sized thromboembolus
to the lung. This infarction forms a wedge- shaped area & has begun
to organize at the margins.

Infarctions of the spleen produce wedge –shaped pale areas
And caused by obstruction of spleenic artery

Shock :
Also called cardio-vascular collapse, is defined as systemic hypo-perfusion caused by reduction either in cardiac output or in the effective circulating blood volume. The end results are;
1. Hypotension.
2. Impaired tissue perfusion.
3. Cellular hypoxia.
Initially, cellular injury is reversible, followed in sustained shock by cell death.
Shock is categorized into;
1. Cardiogenic.
2. Hypovolemic.
3. Septic.
4. Neurogenic.
5. Anaphylactic.

cardiogenic shock
myocardial pump failure: which may be caused by :myocardial infarction ,ventricular rupture, arrhythmias ,cardiac temponade ,pulmonary embolism, open heart surgery………
Principle mechanism is failure of myocardial pump →sudden fall in C.O.
Hypovolemic shock
result from:
loss of blood or plasma volume e.g. hemorrhage ,
fluid loss as in vomiting &diarrhea ,burns or trauma.
Principle mechanism :inadequate blood or plasma
volume→ low Cardiac Output

septic shock
is caused by systemic microbial infections (endotoxic shock)
& it can occur after gm+ bacteria septicemia or even
fungal sepsis.
The toxins produced by these bacteria causes arteriolar
vasodilatation &pooling of blood.
neurogenic shock
in severe pain following fracture bone.
Anaphylactic shock
Initiated by type 1 hypersensitivity reaction →systemic vasodilatation & ↑vascular permeability

Stages of shockUnless the insult is massive and rapidly lethal, shock tends to evolve through 3 phases;1. Initial non-progressive phase during which reflex
compensatory mechanisms are activated &perfusion of vital organs is maintained which include: neurohumoralmechanisms help to maintain the C.O.& blood pressure.
These mechanisms include: baroreceptors reflexes release of catecholamines activation of rennin –angiotensin axis release of antidiuretic hormone ADH &generalized sympathetic stimulation
The net effect is:
tachycardia
,renal conservation of fluid .
Cutaneous vasoconstricon is responsible for coolness &pallor of skin in shock .

coronary &cerebral vessels are less sensitive to the sympathetic response & thus maintain relatively normal caliber , blood flow →oxygen delivery to the vital organs .
septic shock ------vasodilatation. Of skin →skin feel warm &flushed.
2--progressive stage
characterized by tissue hypoperfusion &worsening of circulatory &metabolic imbalance .
if tissue hypoxia is persistent →intracellular aerobic respiration is replaced by anaerobic glycolysis .→increase production of lactic acid →lactic acidosis →↓tissue pH→ blunts the vasomotor response →pooling of bd in the microcirculation →worsen the C.O.
With this wide tissue hypoxia ,vital organs begin to fail ;clinically the patient may become confused &urinary output declines.
3-irreversible stage
cellular &tissue injury is so severe that even if the hemodynamic defects are corrected ,survival is not possible .the patient has complete renal shutdown due to acute tubular necrosis
Morphology, the changes are those of hypoxic injury. Most
particularly involved organs are;
Brain. Heart. Lungs. Kidneys. Adrenals. Gastro-intestinal tract.
Clinical features, they depend on the precipitating insult.
In hypovolemic and cardiogenic shock, the patient presents
with hypotension; weak, rapid pulse; and cool, cyanotic skin.
In septic shock, the skin initially is warm and flushed.
The prognosis varies with the origin of shock and its duration.
The best is in a young patient with hypovolemic shock, and the
worst is in an old patient with cardiogenic shock and that with
septic shock.

















