18
HEPATIC ENCEPHALOPATHY HEPATIC ENCEPHALOPATHY Dr. Bindu Mohandas Dr. Bindu Mohandas M-5 unit M-5 unit
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | julie-cross |
| View: | 223 times |
| Download: | 1 times |
HEPATIC HEPATIC ENCEPHALOPATHYENCEPHALOPATHY
Dr. Bindu MohandasDr. Bindu Mohandas
M-5 unitM-5 unit
SYNONYMSSYNONYMS
Portosystemic encephalophathyPortosystemic encephalophathy
Hepatic coma Hepatic coma
Incidence: 71% in cirrhosisIncidence: 71% in cirrhosis
DEFINITIONDEFINITION
Hepatic Encephalopathy is a Hepatic Encephalopathy is a neuropsychatric syndrome caused by liver neuropsychatric syndrome caused by liver disease, characterised by disturbances in disease, characterised by disturbances in conciousness level & behaviour, personality conciousness level & behaviour, personality changes, fluctuating neurological signs, changes, fluctuating neurological signs, asterixis & distinctive EEG changes.asterixis & distinctive EEG changes.
TYPESTYPES
Acute/ Subacute Acute/ Subacute Reversible Reversible
ChronicChronic Progressive Progressive leading to irreversible leading to irreversible coma & coma & death death
Factors Precipitating Factors Precipitating hepatic encephalopathyhepatic encephalopathy
Increased Protein Load (nitrogen) – Increased Protein Load (nitrogen) – GI bleeding, excessive dietary GI bleeding, excessive dietary protein, uremia, constipationprotein, uremia, constipation
Drugs – Sedatives, AntidepressantsDrugs – Sedatives, Antidepressants Dehydration – Diuretics, paracentesis Dehydration – Diuretics, paracentesis Trauma – including surgeryTrauma – including surgery Electrolyte imbalance – hypokalemia, Electrolyte imbalance – hypokalemia,
alkalosis, hypovolemiaalkalosis, hypovolemia Large binge of alcoholLarge binge of alcohol
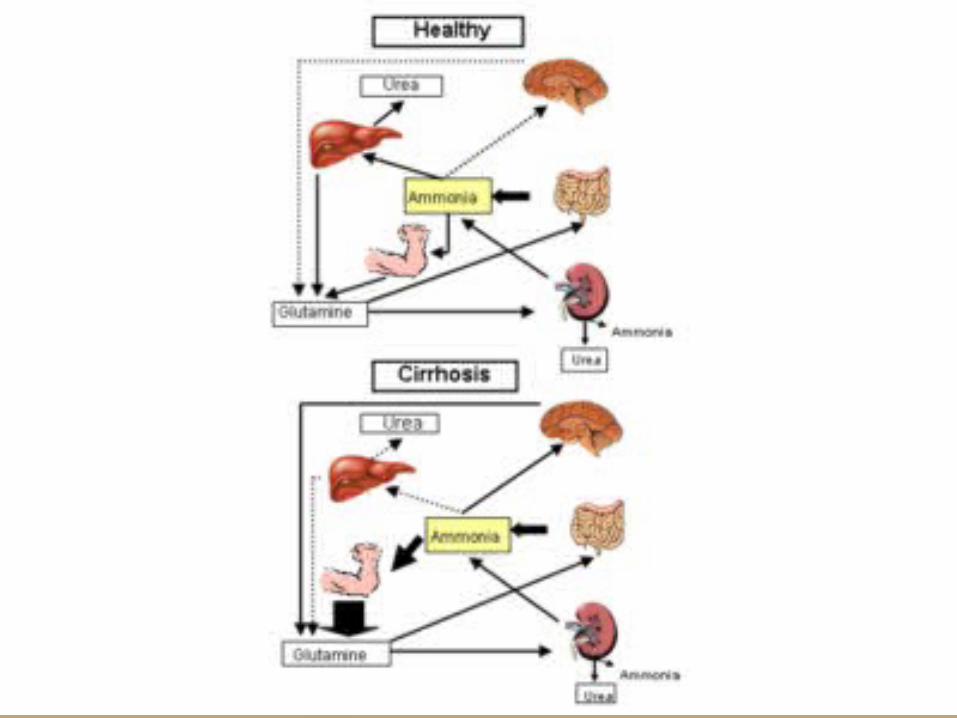
ETIOPATHOGENESISETIOPATHOGENESISAbnormality in nitrogen metabolism by urease producing bacteria in Abnormality in nitrogen metabolism by urease producing bacteria in
bowel.bowel.
Accumulation of ammonia, octapamine aminoacid, fatty acid, mercaptans.Accumulation of ammonia, octapamine aminoacid, fatty acid, mercaptans.
Carried to liver by portal circulation.Carried to liver by portal circulation.
Fail to get detoxified due to hepatocellular disease/ Porto systemic Fail to get detoxified due to hepatocellular disease/ Porto systemic shunting of blood.shunting of blood.
Enters the systemic circulation.Enters the systemic circulation.
Crosses the blood brain barrier.Crosses the blood brain barrier.
Accumulates in brain.Accumulates in brain.
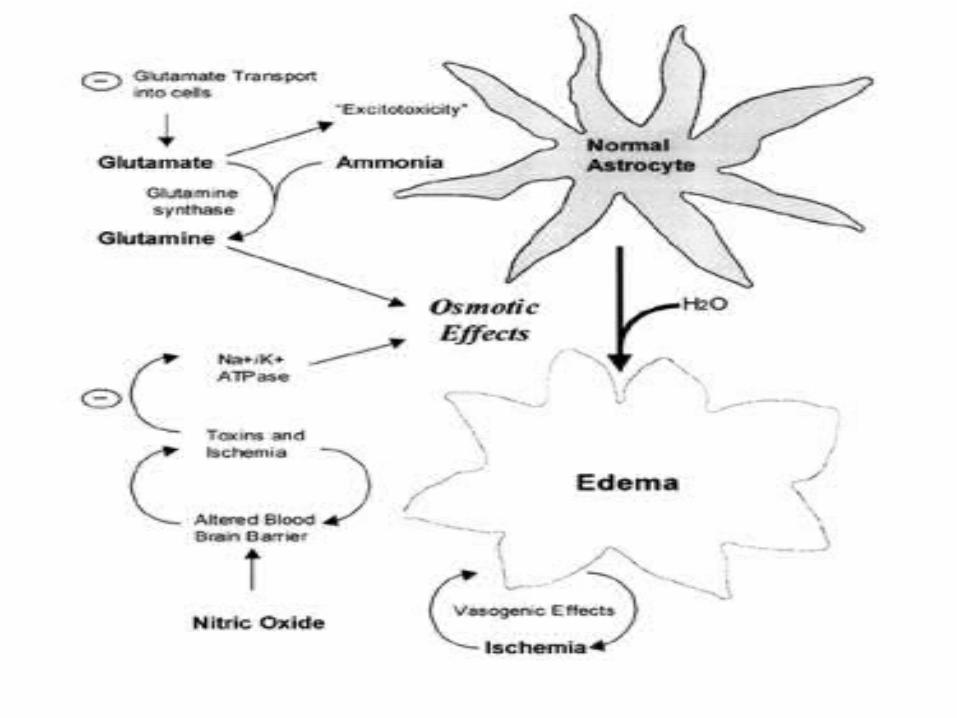
Ammonia induced alteration in astrocyte glutamine & glutamate Ammonia induced alteration in astrocyte glutamine & glutamate concentrations.concentrations.
Altered neurotransmission & cerebral oedema. Altered neurotransmission & cerebral oedema.
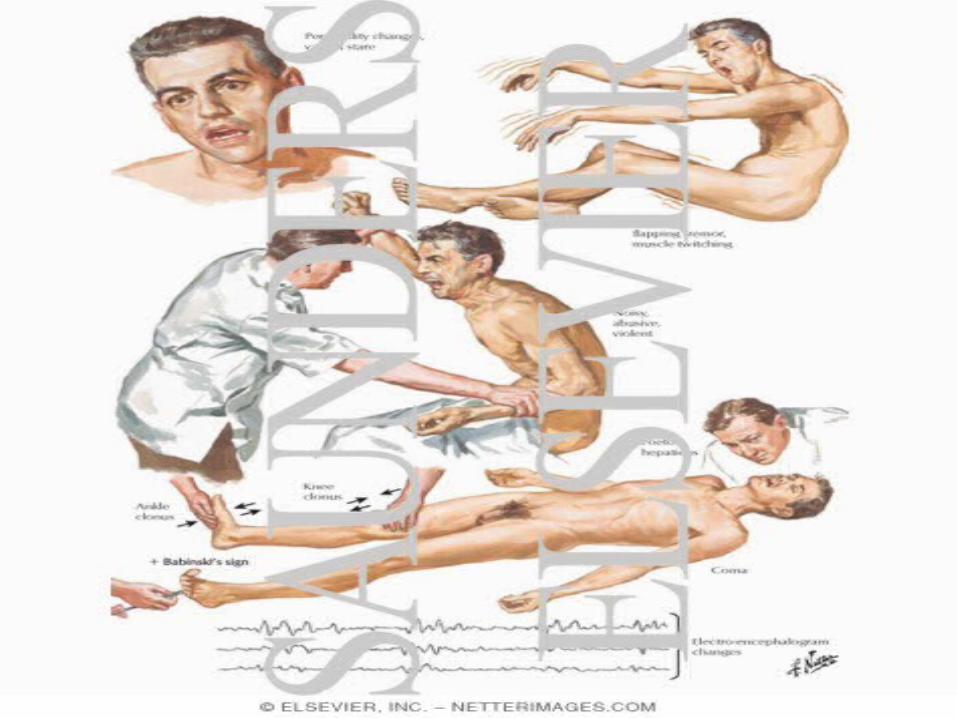
CLINICAL FEATURESCLINICAL FEATURES
Apathy, inability to concentrate, confusion, Apathy, inability to concentrate, confusion, disorientation, drowsiness, slurring of speech disorientation, drowsiness, slurring of speech derangement of conciousnessderangement of conciousnessAltered sleep rhythmAltered sleep rhythmIncreased psychomotor activityIncreased psychomotor activityProgressive drowsiness, stupor & comaProgressive drowsiness, stupor & comaFocal / generalised seizuresFocal / generalised seizuresExaggeration of DTRExaggeration of DTRAsterixisAsterixisConstructional aparaxiaConstructional aparaxiaFetor hepaticusFetor hepaticusInability to perform simple arithmatic tasks & Inability to perform simple arithmatic tasks & change in handwriting.change in handwriting.
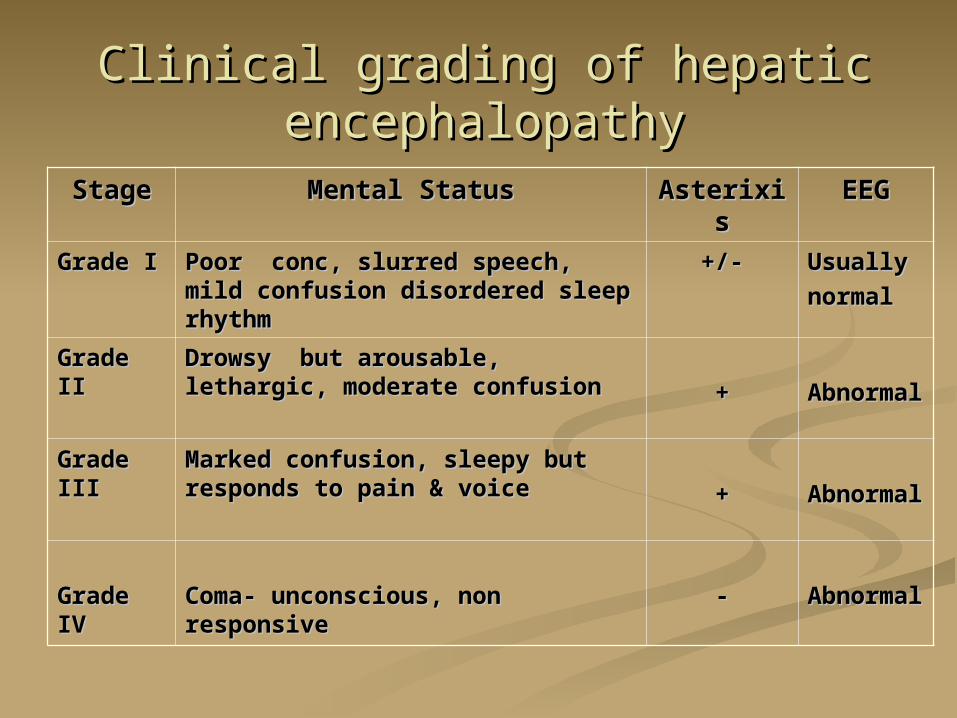
Clinical grading of hepatic Clinical grading of hepatic encephalopathyencephalopathy
StageStage Mental StatusMental Status AsterixisAsterixis EEGEEG
Grade IGrade I Poor conc, slurred speech, mild Poor conc, slurred speech, mild confusion disordered sleep confusion disordered sleep rhythmrhythm
+/-+/- UsuallyUsually
normalnormal
Grade IIGrade II Drowsy but arousable, lethargic, Drowsy but arousable, lethargic, moderate confusionmoderate confusion ++ AbnormAbnorm
alal
Grade Grade IIIIII
Marked confusion, sleepy but Marked confusion, sleepy but responds to pain & voiceresponds to pain & voice ++ AbnormAbnorm
alal
Grade Grade IVIV
Coma- unconscious, non Coma- unconscious, non responsiveresponsive
-- AbnormAbnormalal
INVESTIGATIONSINVESTIGATIONS
EEG – Shows high voltage, slow wave EEG – Shows high voltage, slow wave forms reduced alpha rhythm & forms reduced alpha rhythm & increased delta activity.increased delta activity.
Elevation of serum ammoniaElevation of serum ammonia
No pathognomonic liver function No pathognomonic liver function abnormalityabnormality
CT Brain & CSF analysis – NormalCT Brain & CSF analysis – Normal
USG AbdomenUSG Abdomen
MRI scan in stage IV shows cerebral MRI scan in stage IV shows cerebral oedemaoedema
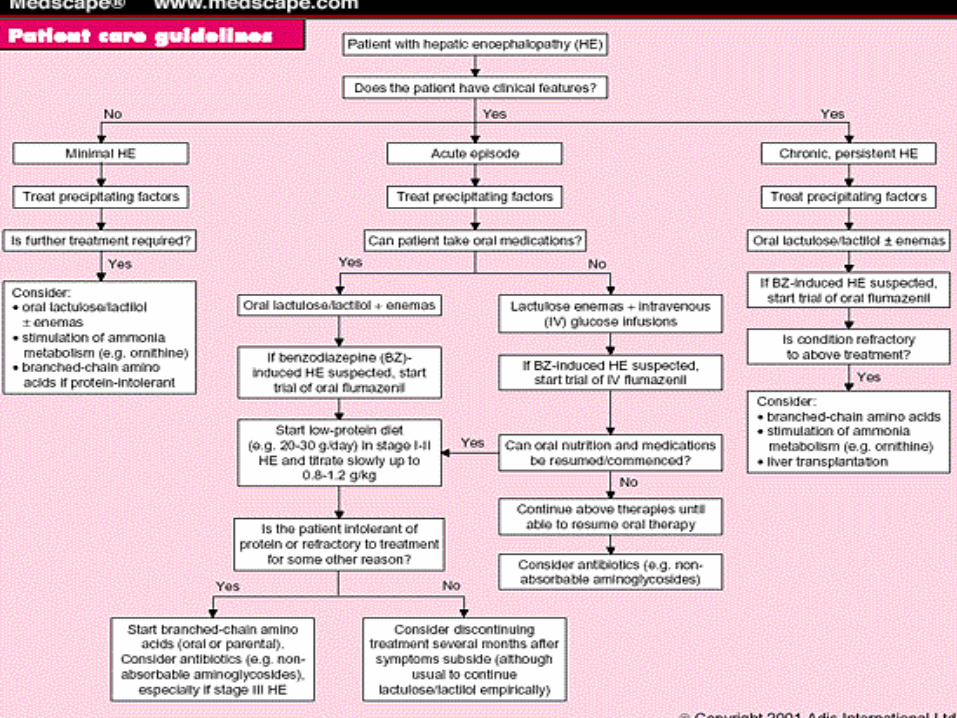
MANAGEMENTMANAGEMENT
Treat/Remove the precipitating causesTreat/Remove the precipitating causesDietary protein restrictionDietary protein restrictionLactulose (15-30ml 8Lactulose (15-30ml 8thth hourly) or Lactitol hourly) or LactitolNeomycin (1-4g 4-6 hourly) or Ampicillin Neomycin (1-4g 4-6 hourly) or Ampicillin i.v mannitoli.v mannitolAvoid drugs – sedatives, diureticsAvoid drugs – sedatives, diureticsLiver transplantation – defenite RxLiver transplantation – defenite RxThe use of levodopa, bromocriptine, The use of levodopa, bromocriptine, ketoanalogues of aminoacid ketoanalogues of aminoacid & i-v infusion of aminoacids, & i-v infusion of aminoacids, haemoperfusionhaemoperfusion – role is unclear.– role is unclear.

PROGNOSISPROGNOSIS
** Hepatic encephalopathy is associated with Hepatic encephalopathy is associated with short survival in cirrhotic patients short survival in cirrhotic patients
** Factors worsening the prognosis areFactors worsening the prognosis are
11. . male sexmale sex
22. . Increased levels of S. bilirubin, alkaline Increased levels of S. bilirubin, alkaline phosphatase, Potassium, BUNphosphatase, Potassium, BUN
33. . Reduced albumin and prothrombin activityReduced albumin and prothrombin activity. .
DIFFERENTIAL DIFFERENTIAL DIAGNOSISDIAGNOSIS
Subdural haematomaSubdural haematoma
Drug or alcohol intoxicationDrug or alcohol intoxication
Delirium tremensDelirium tremens
Wernicke’s encephalopathyWernicke’s encephalopathy
Primary psychiatric disordersPrimary psychiatric disorders
HypoglycemiaHypoglycemia
Neurological Wilson’s diseaseNeurological Wilson’s disease
SOURCE OF SOURCE OF INFORMATIONINFORMATION
www.google.comwww.google.com
www.pubmed.comwww.pubmed.com
Harrison’s internal medicineHarrison’s internal medicine
Davidson’s Principle of MedicineDavidson’s Principle of Medicine
Alagappan’s practical manual Alagappan’s practical manual

TTHHAANNKKYYOOUU

















