Hepatobiliary & Pancreatic Diseases International xxx (xxxx) xxx
Contents lists available at ScienceDirect
Hepatobiliary & Pancreatic Diseases International
journal homepage: www.elsevier.com/locate/hbpd
Original Article/Liver
Potential application of ultrasound-guided thermal ablation in rare
liver tumors
Li-Li Wu
a , Jia-Xin Chen
a , Kai Li a , Zhong-Zhen Su
b , Ying-Lin Long
a , Li-Ping Luo
a , Er-Jiao Xu
a , ∗, Rong-Qin Zheng
a
a Department of Medical Ultrasonics, Third Affiliated Hospital of Sun Yat-sen University, Guangdong Key Laboratory of Liver Disease Research, Guangzhou
510630, China b Department of Medical Ultrasonics, Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai 5190 0 0, China
a r t i c l e i n f o
Article history:
Received 4 May 2018
Accepted 15 October 2018
Available online xxx
Keywords:
Contrast-enhanced ultrasound
Thermal ablation
Rare liver tumor
Fusion imaging
a b s t r a c t
Background: With the advances of imaging techniques, the detection rate of rare liver tumor is increased.
However, the therapeutic strategies of the rare liver tumors remain limited.
Methods: We analyzed twelve pathologically confirmed rare liver tumors in 8 patients. All of the pa-
tients underwent ultrasound (US) guided biopsy and subsequent thermal ablation. The tumors were ab-
lated according to the preoperative plans and monitored by real-time US. CT/MRI fused with contrast
enhanced US (CEUS) or three-dimensional (3D) US-CEUS images were used to guide and assess the abla-
tion zone more accurately during thermal ablation. The rate of technical efficacy was assessed based on
the contrast-enhance CT/MRI (CECT/MRI) results one month after ablation. Local tumor progression (LTP),
recurrence and complications were followed up and recorded.
Results: Among these twelve nodules, nine were subject to US-guided thermal ablation, whereas
the other three inconspicuous nodules were subject to CEUS-guided thermal ablation. Intra-procedure
CT/MRI-CEUS or 3D US-CEUS fusion imaging assessments demonstrated that the ablation zone sufficiently
covered the original tumor, and no immediate supplementary ablation was required. Additionally, no ma-
jor complications were observed during the follow-up period. The postoperative CECT/MRI confirmed that
the technique success rate was 100%. Within the surveillance period of 13 months, no LTP or recurrence
was noted.
Conclusions: US-guided thermal ablation was feasible and safe for rare liver tumors. The use of fusion
imaging technique might make US-guided thermal ablation as effective as surgical resection, and this
technique might serve as a potential therapeutic modality for rare liver tumors in the future.
L.-L. Wu, J.-X. Chen and K. Li et al. / Hepatobiliary & Pancreatic Diseases International xxx (xxxx) xxx 3
ARTICLE IN PRESS
JID: HBPD [m5G; November 6, 2018;13:49 ]
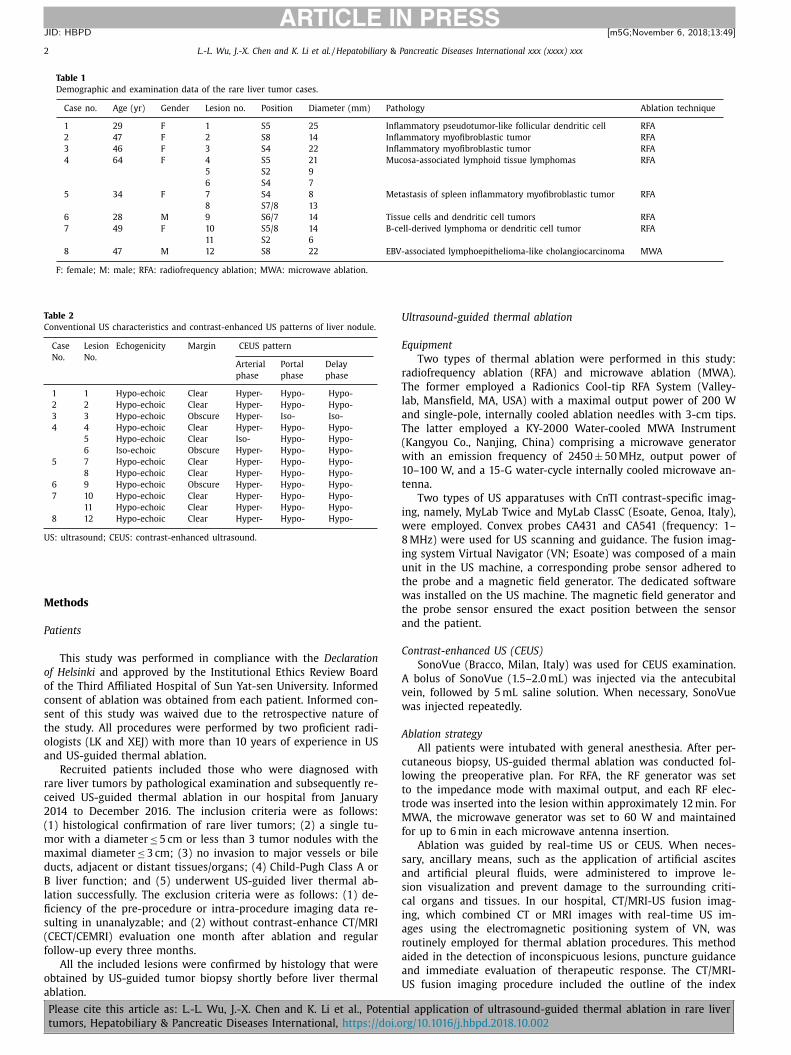
Fig. 1. A 47-year-old female patient with inflammatory myofibroblastic tumor. A –C : The contrast enhanced ultrasound (CEUS) images demonstrating the hyper-enhancement
in arterial phase and hypo-enhancement in portal phase; D –F : Preoperative MRI images demonstrating the hyper-enhancement in arterial phase and hypo-enhancement in
portal and venous phase; G : The 3D US-CEUS fusion imaging evaluation carried out immediately after the radiofrequency ablation showing the non-enhanced zone of CEUS
covered the blue ring of index tumor and the red ring of preset ablative margin, which indicated the tumor and its 5 mm ablative margin were completely ablated except
the adjacent large vessels; H : One month post-operatively, contrast enhanced MRI image showing the completely necrosis of the index tumor.
l
t
d
I
c
t
i
z
b
s
s
a
s
a
a
a
i
w
P
2
t
a
e
w
I
t
esion and its ablative margins on CT/MRI images, registration of
wo sets of images, alignment by fine-tuning and navigation. The
etails of the procedure were described in our previous report [8] .
f the index lesion was inconspicuous, CT/MRI-US fusion imaging
ould be used to locate the lesion and guide the subsequent punc-
ure. After the thermal ablation procedure, CT/MRI-CEUS fusion
maging was generally employed to assess whether the ablated
one covered the index lesion and its ablative margin. If possi-
le, 5 mm ablative margin was required during intraoperative as-
essment unless the lesion was adjacent to the major hepatic ves-
els or liver capsule. Moreover, 3D US-CEUS fusion imaging was
lso used for the immediate evaluation of therapeutic response in
ome other patients if the lesions were conspicuous on US im-
ges. Briefly, 3D US-US fusion imaging fused the real-time US im-
ges with the 3D US images that were acquired before ablation
a
Please cite this article as: L.-L. Wu, J.-X. Chen and K. Li et al., Potentia
4 L.-L. Wu, J.-X. Chen and K. Li et al. / Hepatobiliary & Pancreatic Diseases International xxx (xxxx) xxx
ARTICLE IN PRESS
JID: HBPD [m5G; November 6, 2018;13:49 ]
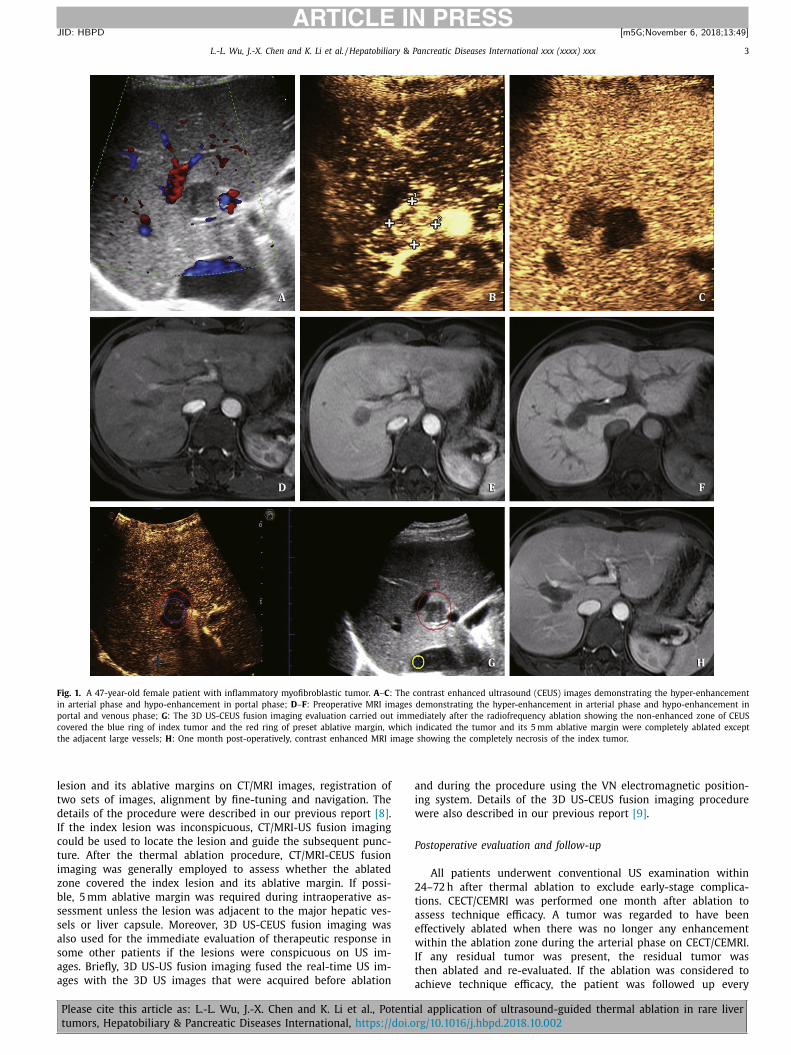
Fig. 2. A 49-year-old female patient with B-cell-derived lymphoma or dendritic cell tumor. A–C: The preoperative MRI images demonstrating the hyper-enhancement in arte-
rial phase and hypo-enhancement in the portal and venous phase of the lesion; D –F : The contrast enhanced ultrasound (CEUS) images demonstrating the hyper-enhancement
in arterial phase and hypo-enhancement in the portal phase; G : The 3D US-CEUS fusion imaging evaluation carried out immediately after the radiofrequency ablation show-
ing the non-enhanced zone of CEUS covered the index tumor and the yellow ring of preset ablative margin, which indicated the tumor and its 5-mm ablative margin were
completely ablated; H : One month post-operatively, contrast enhanced MRI image showing the completely necrosis of the index tumor.
R
D
s
a
n
h
s
e
s
i
three months after thermal ablation to evaluate recurrence and
complications.
Local tumor progression (LTP) was defined as the appearance of
new tumor foci one month after intervention at the edge of the ab-
lation zone, which was often characterized as hyper-enhancement
during arterial phase with hypo-enhancement in the portal venous
system or the delayed phase on CECT/CEMRI images.
Statistical analysis
All statistical analyses were performed using SPSS software
(Version 22.0, SPSS Inc., Chicago, IL, USA). Quantitative and qualita-
tive data were presented as the median (range) and number (per-
centage), respectively.
Please cite this article as: L.-L. Wu, J.-X. Chen and K. Li et al., Potentia
L.-L. Wu, J.-X. Chen and K. Li et al. / Hepatobiliary & Pancreatic Diseases International xxx (xxxx) xxx 5
ARTICLE IN PRESS
JID: HBPD [m5G; November 6, 2018;13:49 ]
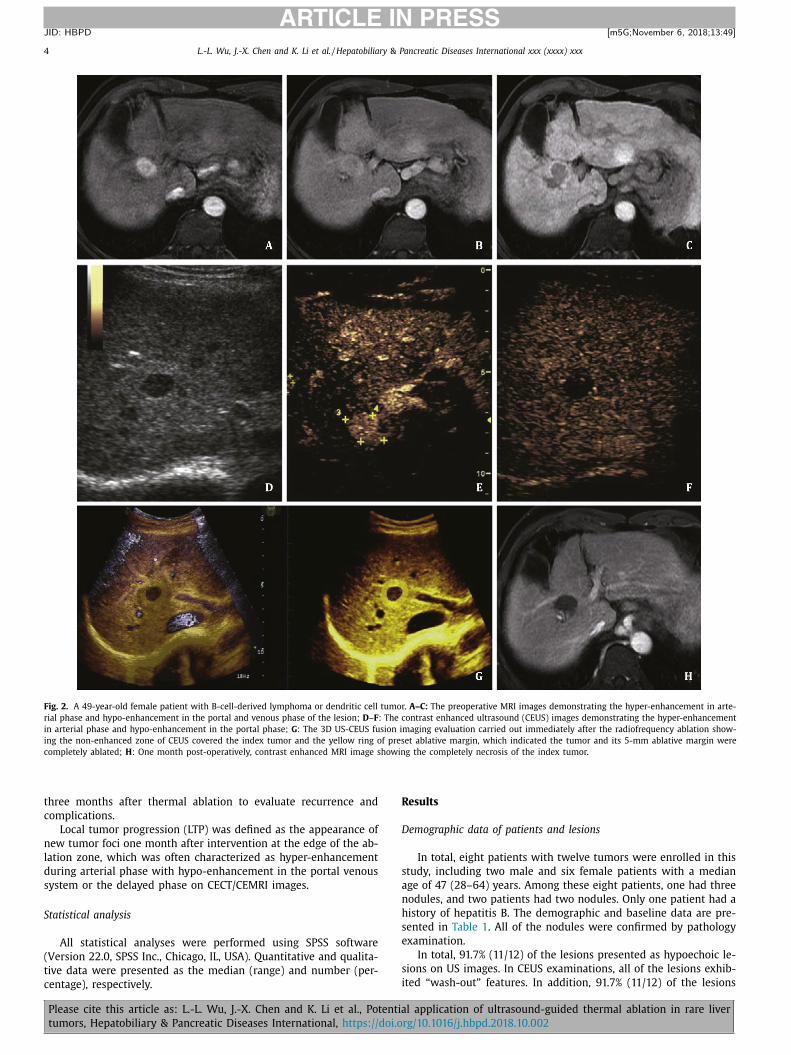
Fig. 3. A 46-year-old female patient with recurrent inflammatory myofibroblastic tumor. A –C : Preoperative MRI image of the index tumor; D : MRI-US fusion imaging located
the index tumor which was inconspicuous on US images before radiofrequency ablation; E : After the radiofrequency ablation, MRI-CEUS fusion imaging was employed to
evaluate the therapeutic effect immediately. The CEUS images showing the non-enhanced zone already covered the blue ring of index tumor and the red ring of preset
ablative margin, which indicated the tumor and 5-mm ablative margin were completely ablated; F : One month post-operatively, contrast enhanced MRI image showing the
completely necrosis of the index tumor.
e
e
U
r
P
a
w
s
(
l
t
n
m
t
c
T
o
F
fi
t
u
d
t
r
a
r
r
o
c
xhibited hyper-enhancement during the arterial phase and hypo-
nhancement during the portal phase or late phase.
S guidance and intra-procedure assessment of thermal ablation of
are liver tumors
rocedure of liver tumor thermal ablation
All the tumors included in this study were ablated precisely
t the designated regions. Among these twelve nodules, nine
ere subject to US-guided thermal ablation, whereas three incon-
picuous nodules were subject to CEUS-guided thermal ablation
Table 2 ). Artificial ascites was administered in one case to improve
esion visualization and prevent damages to the adjacent gastroin-
estinal tract.
According to the immediate evaluation of fusion imaging, the
on-perfusion zones covered the target lesions. Besides, at least 5-
m ablative margins were achieved unless the lesion was adjacent
o the major hepatic vessels or liver capsule. All the lesions were
Please cite this article as: L.-L. Wu, J.-X. Chen and K. Li et al., Potentia
WLL, CJX and XEJ conceived, designed and performed the exper-
ments, analyzed the data, wrote the paper, and reviewed drafts of
he paper. LK, SZZ and ZRQ reviewed drafts of the paper. LYL and
LP collected the data. All the authors have read and approved this
ubmission. WLL and CJX contributed equally to this work. XEJ is
he guarantor.
unding
This study was supported by grants from National Key R&D Pro-
ram of China ( 2017YFC01120 0 0 ), National Natural Science Foun-
ation of China ( 81430038 and 81401434 ), Science and Technol-
gy Planning Project of Guangdong Province ( 2015A020214009 ,
016A020215072 , and 2017A020215082 ); and Natural Science
oundation of Guangdong Province ( 2016A030313205 ).
thical approval
This study was approved by the Institutional Ethics Review
oard of the Third Affiliated Hospital of Sun Yat-sen University.
ompeting interest
No benefits in any form have been received or will be received
rom a commercial party related directly or indirectly to the sub-
ect of this article.
eferences
[1] Bruix J , Sherman M American Association for the Study of Liver Dis-
eases. Management of hepatocellular carcinoma: an update. Hepatology2011;53:1020–1022 .
[2] Chen W , Zheng R , Baade PD , Zhang S , Zeng H , Bray F , et al. Cancer statistics in
China, 2015. CA Cancer J Clin 2016;66:115–132 . [3] Parisi A , Desiderio J , Trastulli S , Castellani E , Pasquale R , Cirocchi R ,
et al. Liver resection versus radiofrequency ablation in the treatment of cir-rhotic patients with hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int
2013;12:270–277 . [4] Lee DH , Lee JM . Primary malignant tumours in the non-cirrhotic liver. Eur J
Radiol 2017;95:349–361 .
[5] Feng K , Yan J , Li X , Xia F , Ma K , Wang S , et al. A randomized controlled trial ofradiofrequency ablation and surgical resection in the treatment of small hepa-
tocellular carcinoma. J Hepatol 2012;57:794–802 . [6] Lau WY , Lau SH . The current role of radiofrequency ablation in the treat-
ment of hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int 2017;16:122–126 .
[7] Kudo M , Matsui O , Izumi N , Iijima H , Kadoya M , Imai Y , et al. JSH consen-
sus-based clinical practice guidelines for the management of hepatocellularcarcinoma: 2014 update by the liver cancer study group of Japan. Liver Cancer
2014;3:458–468 . [8] Li K , Su ZZ , Xu EJ , Ju JX , Meng XC , Zheng RQ . Improvement of ablative mar-
gins by the intraoperative use of CEUS-CT/MR image fusion in hepatocellularcarcinoma. BMC Cancer 2016;16:277 .
[9] Xu EJ , Lv SM , Li K , Long YL , Zeng QJ , Su ZZ , et al. Immediate evalua-
tion and guidance of liver cancer thermal ablation by three-dimensional ul-trasound/contrast-enhanced ultrasound fusion imaging. Int J Hyperthermia
2018;34:870–876 . [10] An C , Rakhmonova G , Choi JY , Kim MJ . Liver imaging reporting and data sys-
tem (LI-RADS) version 2014: understanding and application of the diagnosticalgorithm. Clin Mol Hepatol 2016;22:296–307 .
[11] Giorgio A , Montesarchio L , Gatti P , Amendola F , Matteucci P , Santoro B ,
et al. Contrast-enhanced ultrasound: a simple and effective tool in defining arapid diagnostic work-up for small nodules detected in cirrhotic patients dur-
ing surveillance. J Gastrointest Liver Dis 2016;25:205–211 . [12] Konopke R , Bunk A , Kersting S . The role of contrast-enhanced ultra-
sound for focal liver lesion detection: an overview. Ultrasound Med Biol2007;33:1515–1526 .
[13] Claudon M , Dietrich CF , Choi BI , Cosgrove DO , Kudo M , Nolsøe CP , et al. Guide-lines and good clinical practice recommendations for contrast enhanced ul-
trasound (CEUS) in the liver - update 2012: a WFUMB-EFSUMB initiative in
cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS.Ultrasound Med Biol 2013;39:187–210 .
[14] Tominaga K , Kamimura K , Sakamaki A , Terai S . Intraductal papillary neoplasmof the bile duct: a rare liver tumor complicated by malignancy. Hepatology
2017;66:1695–1697 .
l application of ultrasound-guided thermal ablation in rare liver
L.-L. Wu, J.-X. Chen and K. Li et al. / Hepatobiliary & Pancreatic Diseases International xxx (xxxx) xxx 7
ARTICLE IN PRESS
JID: HBPD [m5G; November 6, 2018;13:49 ]
[
[15] Liu LN , Xu HX , Zheng SG , Sun LP , Guo LH , Zhang YF , et al. Ultrasound findingsof intraductal papillary neoplasm in bile duct and the added value of con-
trast-enhanced ultrasound. Ultraschall Med 2015;36:594–602 . [16] Piscaglia F , Wilson SR , Lyshchik A , Cosgrove D , Dietrich CF , Jang HJ , et al. Amer-
ican college of radiology contrast enhanced ultrasound liver imaging reportingand data system (CEUS LI-RADS) for the diagnosis of hepatocellular carcinoma:
a pictorial essay. Ultraschall Med 2017;38:320–324 . [17] Ismail H , Dembowska-Bagi ́nska B , Broniszczak D , Kalici ́nski P , Maruszewski P ,
Kluge P , et al. Treatment of undifferentiated embryonal sarcoma of the liver in
children–single center experience. J Pediatr Surg 2013;48:2202–2206 .
Please cite this article as: L.-L. Wu, J.-X. Chen and K. Li et al., Potentia
[18] Lei JY , Wang WT , Yan LN , Wen TF , Li B . Radiofrequency ablation versus surgicalresection for small unifocal hepatocellular carcinomas. Medicine (Baltimore)
2014;93:e271 . [19] Cho YK , Kim JK , Kim WT , Chung JW . Hepatic resection versus radiofrequency
ablation for very early stage hepatocellular carcinoma: a Markov model analy-sis. Hepatology 2010;51:1284–1290 .
20] Li K , Su Z , Xu E , Huang Q , Zeng Q , Zheng R . Evaluation of the ablation mar-gin of hepatocellular carcinoma using CEUS-CT/MR image fusion in a phantom
model and in patients. BMC Cancer 2017;17:61 .
l application of ultrasound-guided thermal ablation in rare liver





![Hepatobiliary diseases in buffalo ( Bubalus bubalis ... · diseases of internal organs, including hepatic diseases in buffalo under field conditions [3,5]. A complete ultrasonographic](https://static.documents.pub/doc/80x56/5eb4d20a1ae6da71cd66ea30/hepatobiliary-diseases-in-buffalo-bubalus-bubalis-diseases-of-internal-organs.jpg)














