High incidence of unexpected defibrillation coilretention during orthotopic heart transplantation
Pal Abraham, MD, Kadir Caliskan, MD, andTamas Szili-Torok, MD, PhD
From the Department of Cardiology, Thoraxcenter, ErasmusMedical Center, Rotterdam, the Netherlands
Implantation of a cardioverter-defibrillator (ICD) is areasonable choice for non-hospitalized patients awaitingorthotopic heart transplantation (OHTx) to prevent arrhyth-mic death.1 Malfunction or failure of ICD leads can occurby several mechanisms, and some of them may be attributedto lead design.2,3 Surgical removal of the entire ICD systemis part of the OHTx procedure and is usually accomplishedwithout complications.4
We wanted to explore the incidence and cause of ICD
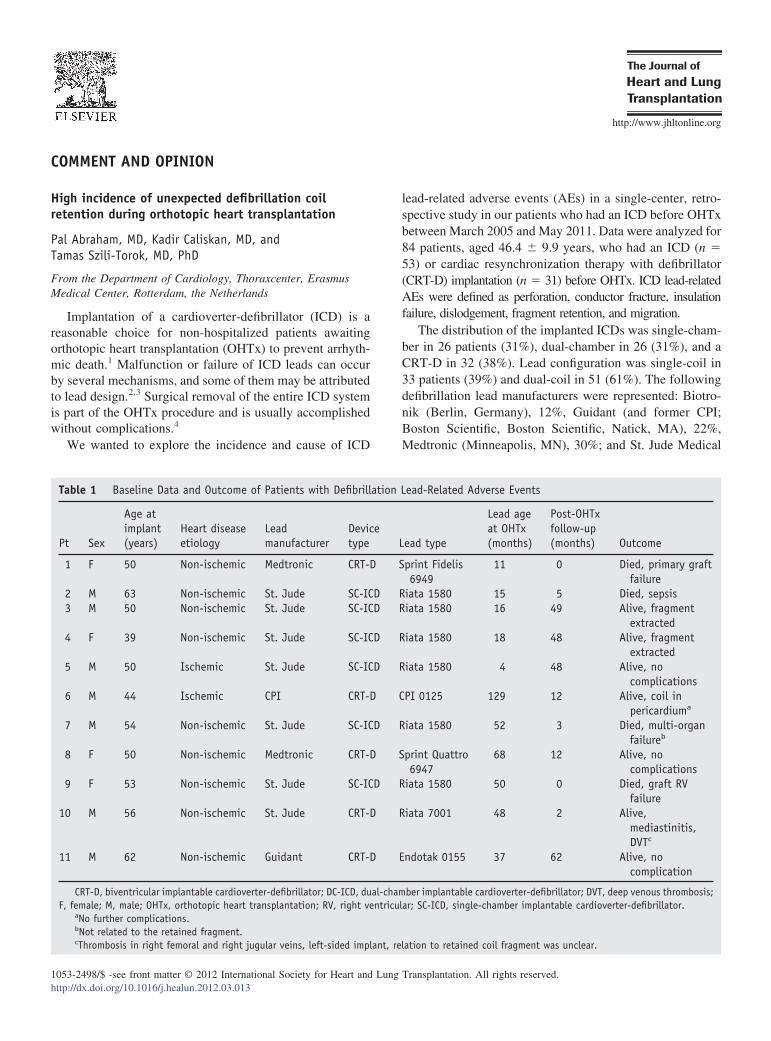
Table 1 Baseline Data and Outcome of Patients with Defibrill
Pt Sex
Age atimplant Heart disease
etiologyLeadmanufacturer
Devictype(years)
1 F 50 Non-ischemic Medtronic CRT-D
2 M 63 Non-ischemic St. Jude SC-IC3 M 50 Non-ischemic St. Jude SC-IC
4 F 39 Non-ischemic St. Jude SC-IC
5 M 50 Ischemic St. Jude SC-IC
6 M 44 Ischemic CPI CRT-D
7 M 54 Non-ischemic St. Jude SC-IC
8 F 50 Non-ischemic Medtronic CRT-D
9 F 53 Non-ischemic St. Jude SC-IC
10 M 56 Non-ischemic St. Jude CRT-D
11 M 62 Non-ischemic Guidant CRT-D
CRT-D, biventricular implantable cardioverter-defibrillator; DC-ICD, duF, female; M, male; OHTx, orthotopic heart transplantation; RV, right ve
aNo further complications.bNot related to the retained fragment.
cThrombosis in right femoral and right jugular veins, left-sided implant, rel
lead-related adverse events (AEs) in a single-center, retro-spective study in our patients who had an ICD before OHTxbetween March 2005 and May 2011. Data were analyzed for84 patients, aged 46.4 � 9.9 years, who had an ICD (n �53) or cardiac resynchronization therapy with defibrillator(CRT-D) implantation (n � 31) before OHTx. ICD lead-relatedAEs were defined as perforation, conductor fracture, insulationfailure, dislodgement, fragment retention, and migration.
The distribution of the implanted ICDs was single-cham-ber in 26 patients (31%), dual-chamber in 26 (31%), and aCRT-D in 32 (38%). Lead configuration was single-coil in33 patients (39%) and dual-coil in 51 (61%). The followingdefibrillation lead manufacturers were represented: Biotro-nik (Berlin, Germany), 12%, Guidant (and former CPI;Boston Scientific, Boston Scientific, Natick, MA), 22%,Medtronic (Minneapolis, MN), 30%; and St. Jude Medical
910 The Journal of Heart and Lung Transplantation, Vol 31, No 8, August 2012
(St. Paul, MN), 36%. The mean time from ICD lead im-plantation to OHTx was 36 � 30 months. Patients in thesingle-coil group were younger, but sex, ischemic etiology,duration of OHTx procedure, and lead age did not differsignificantly.
No lead-related AEs occurred in the single-coil group,but 11 (22%) ICD lead-related AEs were documented in thedual-coil group immediately after OHTx. All AEs wereretained proximal coil fragments of ICD leads. Details andoutcome of the patients with an AE are listed in Table 1.Nine heart surgeons were involved in the OHTx procedures,all with ample experience. There was no difference in thedistribution of surgeons regarding the incidence of leadfragmentation. The failed ICD leads came from the St. JudeMedical Riata family in 7 of 11 patients; whereas 2 patients
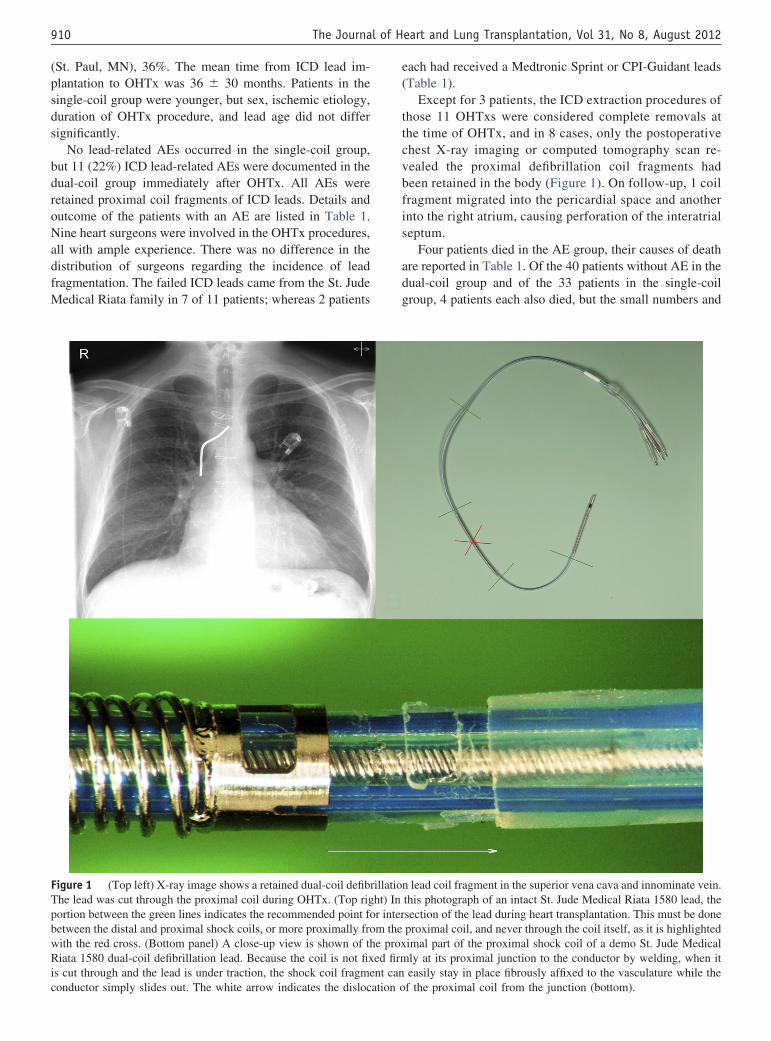
Figure 1 (Top left) X-ray image shows a retained dual-coil defibThe lead was cut through the proximal coil during OHTx. (Top rigportion between the green lines indicates the recommended point fobetween the distal and proximal shock coils, or more proximally frowith the red cross. (Bottom panel) A close-up view is shown of thRiata 1580 dual-coil defibrillation lead. Because the coil is not fixis cut through and the lead is under traction, the shock coil fragme
conductor simply slides out. The white arrow indicates the dislocation o
each had received a Medtronic Sprint or CPI-Guidant leads(Table 1).
Except for 3 patients, the ICD extraction procedures ofthose 11 OHTxs were considered complete removals atthe time of OHTx, and in 8 cases, only the postoperativechest X-ray imaging or computed tomography scan re-vealed the proximal defibrillation coil fragments hadbeen retained in the body (Figure 1). On follow-up, 1 coilfragment migrated into the pericardial space and anotherinto the right atrium, causing perforation of the interatrialseptum.
Four patients died in the AE group, their causes of deathare reported in Table 1. Of the 40 patients without AE in thedual-coil group and of the 33 patients in the single-coilgroup, 4 patients each also died, but the small numbers and
n lead coil fragment in the superior vena cava and innominate vein.this photograph of an intact St. Jude Medical Riata 1580 lead, thesection of the lead during heart transplantation. This must be doneproximal coil, and never through the coil itself, as it is highlightedimal part of the proximal shock coil of a demo St. Jude Medically at its proximal junction to the conductor by welding, when iteasily stay in place fibrously affixed to the vasculature while the
rillatioht) Inr interm thee proxed firmnt can
f the proximal coil from the junction (bottom).
911Abraham et al. Comment and Opinion
absence of any relation of the deaths to the retained frag-ments makes any comparison meaningless. Two patientsunderwent an uncomplicated femoral transvenous lead frag-ment extraction 19 and 56 days after transplantation. In therest of the patients, including the patient with the coil in thepericardium, we left the fragments in place after individu-ally weighing risks vs benefits of removal.
Incomplete removal of defibrillation coils at the time ofOHTx is a clinically relevant problem that affected 22% of ourdual-coil lead cohort but not the single-coil cohort. The com-plications are suggestive of a specific, lead-related problem.We could only address here the specific lead design problem ofthe St. Jude Riata 1580 dual-coil defibrillation lead, becausethe problems with the other lead types remain to be elucidated.This lead, which is no longer sold, used to be manufactureddifferently than others.2 The proximal end of the proximal coilin this lead is not welded to the conductor, and only the distalend of the proximal coil has electrical connection and firmfixation to the conductor by welding. When the coil is cutthrough and the lead is under traction from the pocket, thedefibrillation coil can easily stay in place, fibrously affixed tothe vasculature, while the conductor can slide out (Figure 1).We suggest that the intersection of the ICD lead should not bedone through the coil; instead, the lead should be cut throughbetween the 2 coils (Figure 1). This will prevent the retentionof coil remnants in the vasculature.
The importance of removal of all the abandoned hard-ware at the time of OHTx is obvious because the risk of
infection is high during life-long immunosuppressive ther-
apy. The use of single-coil defibrillation leads in candidatesto OHTx is suggested to prevent such complications.
Disclosure statementThe authors acknowledge Attila Kardos, MD, PhD, DominicA. M. J. Theuns, PhD (research support from Biotronik, BostonScientific, and St. Jude Medical), Alexander P. W. M. Maat, MD,PhD, Aggie H. M. M. Balk, MD, PhD, and Luc J. L. M. Jordaens,MD, PhD (consultant for St. Jude Medical, Biotronik, and Sorin)for their contribution to this article.
Pal Abraham, MD, Kadir Caliskan, MD, and Tamas Szili-Torok, MD, PhD have no related conflicts of interest to disclose.None of the authors has a financial relationship with a commercialentity that has an interest in the subject of the presented manuscriptor other conflicts of interest to disclose. No funding was receivedfor this work from any external sources.
References
1. Sandner SE, Wieselthaler G, Zuckermann A, et al. Survival benefit ofthe implantable cardioverter-defibrillator in patients on the waiting listfor cardiac transplantation. Circulation 2001;104:I171-6.
2. Porterfield JG, Porterfield LM, Kuck KH, et al. Clinical performance ofthe St. Jude Medical Riata defibrillation lead in a large patient popula-tion. J Cardiovasc Electrophysiol 2009;21:551-6.
3. Kleemann T, Becker T, Doenges K, et al. Annual rate of transvenousdefibrillation lead defects in implantable cardioverter-defibrillators overa period of �10 years. Circulation 2007;115:2474-80.
4. Smith MC, Love CJ. Extraction of transvenous pacing and ICD leads.