32
Highligts Tandem Meetings 2018 – Neoplasias mieloproliferativas Prof. Dra. Vaneuza A.M.Funke Responsavel Técnico STMO Adulto HC - UFPR
| Date post: | 03-Dec-2018 |
| Category: |
Documents |
| Upload: | trinhthuan |
| View: | 214 times |
| Download: | 0 times |

Highligts Tandem Meetings 2018 – Neoplasias mieloproliferativas
Prof. Dra. Vaneuza A.M.Funke
Responsavel Técnico STMO Adulto
HC-UFPR
JAK Inhibitors Prior to Allogeneic Stem Cell
Transplant for Patients with Myelofibrosis: A
Prospective Study
Methods:
• single center phase II prospective study of JAK inhibitor
therapy followed by myeloablative or reduced intensity HCT
in 22 patients with primary (n = 15) and secondary (n = 7)
MF.
• Patients were given a JAK inhibitor for at least 8 weeks
(median 7.5 months; range 2 - 30 months) prior to HCT,
which was tapered over 1-2 weeks through Day - 4 of
conditioning.
Salit R et al (FHCRC)
JAK Inhibitors Prior to Allogeneic Stem Cell
Transplant for Patients with Myelofibrosis: A
Prospective Study
Salit R et al (FHCRC)
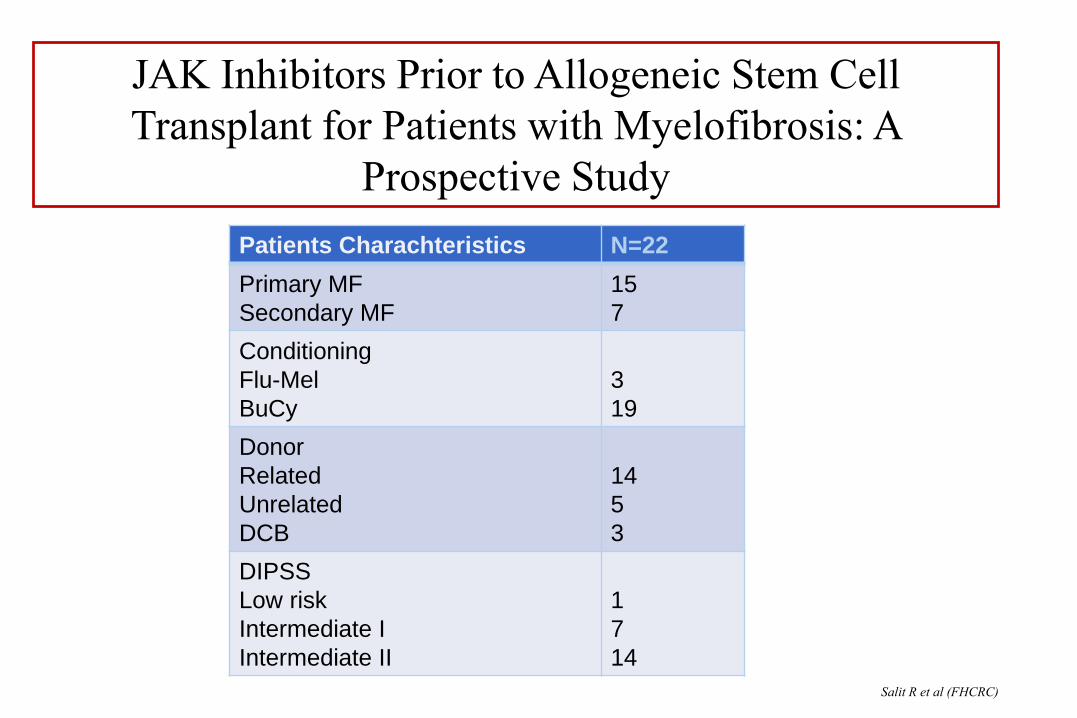
Patients Charachteristics N=22
Primary MF
Secondary MF
15
7
Conditioning
Flu-Mel
BuCy
3
19
Donor
Related
Unrelated
DCB
14
5
3
DIPSS
Low risk
Intermediate I
Intermediate II
1
7
14
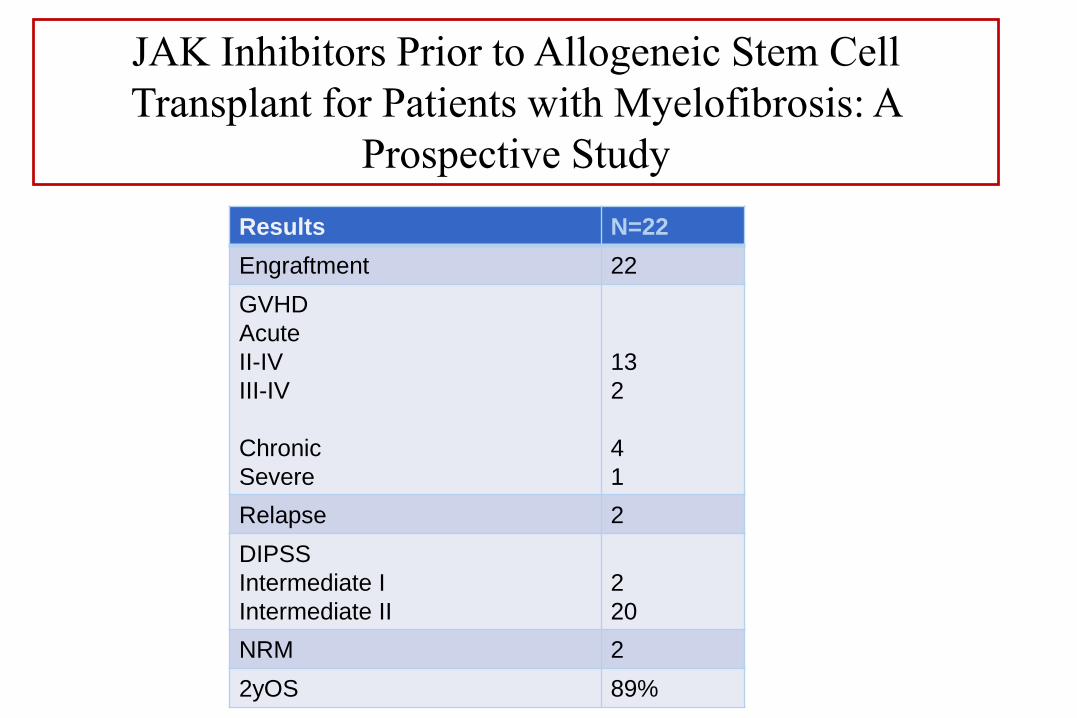
Results N=22
Engraftment 22
GVHD
Acute
II-IV
III-IV
Chronic
Severe
13
2
4
1
Relapse 2
DIPSS
Intermediate I
Intermediate II
2
20
NRM 2
2yOS 89%
JAK Inhibitors Prior to Allogeneic Stem Cell
Transplant for Patients with Myelofibrosis: A
Prospective Study

Salit R et al (FHCRC)
Results:
• All patients engrafted at a median of 18 (range 14-27) days. There were
no graft failures and no incidences of cytokine release syndrome.
• Median day 80 chimerism was 88% CD3 and 100% CD33
• At a median follow up of 16.9 months, 20 of the 22 patients are alive
for a 2 year survival of 89%.
JAK Inhibitors Prior to Allogeneic Stem Cell
Transplant for Patients with Myelofibrosis: A
Prospective Study

Conclusions:
• JAK inhibitor therapy pre-HCT is safe and the strategy of
overlapping a JAK inhibitor with conditioning chemotherapy
prevented cytokine release syndrome.
• Survival at 2-years in this cohort is 89% compared with 54% in
our closely matched historical cohort of intermediate-2 patients
who did not receive a pre-transplant JAK inhibitor.
• Both Grades III-IV acute and severe chronic GVHD were
encouragingly infrequent.
JAK Inhibitors Prior to Allogeneic Stem Cell
Transplant for Patients with Myelofibrosis: A
Prospective Study

Immunosuppression Withdrawal
Is an Effective Treatment of Relapse after
Allogeneic Stem Cell Transplant for Myelofibrosis
• January 2005 and July 2015; 92 patients with primary or secondary MF who
underwent first allo-SCT at MDACC.
• All patients with disease relapse (morphologic and/or molecular) or MM
(defined as less than 95% of donor cells origin) and who had
immunosuppression reduction/withdrawal as primary therapeutic
intervention were included.
• A total of 25 patients with a median age of 59 years were eligible for the final
analysis.
• All patients were on tacrolimus as their primary GVHD prophylaxis, but none
had active GVHD at time of relapse.
• Median time from allo-SCT to relapse/MM was 106 days (31-349) and
median time from relapse to immunotherapy reduction was 11 days (0-76).
• None of the patients received additional simultaneous treatment.
Samer A. Srour, et al

• 48% (12 of 25) responded to tacrolimus reduction as primary intervention
and achieved CR (MM, n=6; molecular/morphologic relapse, n=6).
• Among the responders, 3 died of GVHD complications and 9 remain alive
requiring no subsequent treatment.
• All responders developed GVHD, with liver GVHD universal to all patients
(100%).
• Tacrolimus was resumed (or dose increased) in all patients, and systemic
steroids ± photophoresis were used in 7 patients, with no notable negative
impact on graft-versus-tumor (GVT) effects.
Samer A. Srour, et al
Immunosuppression Withdrawal
Is an Effective Treatment of Relapse after
Allogeneic Stem Cell Transplant for Myelofibrosis

• Among the non-responders (n=13; MM, n=6; molecular/morphologic
relapse, n=7), 8 died (6 of persistent/recurrent disease, and 2 of GVHD) and
5 remain alive at last follow-up. Of these 5 patients, 4 had a second allo-SCT
and one patient received DLI.
• Only 4 (31%) of the nonresponding patients developed GVHD.
• With a median follow up of 52 months, the median OS was not reached for
all patients and the 5-year OS rates were 73% and 37% among responders
to tacrolimus withdrawal versus the nonresponders, respectively (Figure).
Samer A. Srour, et al
Immunosuppression Withdrawal
Is an Effective Treatment of Relapse after
Allogeneic Stem Cell Transplant for Myelofibrosis

Immunosuppression Withdrawal
Is an Effective Treatment of Relapse after
Allogeneic Stem Cell Transplant for Myelofibrosis

Views on Bone Marrow Transplant: A Survey of
Patients with Myelofibrosis
Methods:
• A survey for MPN patients was posted on multiple websites, including MPN Forum, MPN
Advocacy, MPN Research Foundation, and MPN Education foundation.
Results:
• There were 366 respondents. 129 patients indicated that they had MF: 62 had primary MF (PMF),
and 67 had secondary MF.
• Median age of respondents was 61 (31-84), and 80 (62%) were female.
• The majority identified themselves as “white” 125 (97%). 118 (91%) patients had at least some
college, 63 (49%) of patients indicated they had private insurance, and 45 (35%) had
medicare/medicaid. 65 (50%) are currently receiving ruxolitinib.
• Of these patients 49 (41%) had been referred for a bone marrow transplant consult, 41 of those
patients went to the consult. The majority of the patients felt that they received the information
they needed at the consult (n=35, 85%).
• 10 (25%) of patients plan to undergo a transplant in the near future, 6 (15%) at some point in the
future, and 24 (60%) do not plan on undergoing a transplant.
• Of those who were not going to transplant, there were a variety of concerns expressed (Table
1). Of the 16 patients who planned on proceeding with transplant, 14 provided reasons including
the belief that it will improve survival, the desire to be around for family, and fear of dying.
Jeanne Palmer et al

Concern Not important Important*
Worried about the financial impact it will have on my family 13 11
Worried about the financial impact it will have on me 12 12
I do not want my family to have to take care of me 10 14
I do not want to get sick 6 18
I would rather enjoy the time I have left 5 19
I do not want to spend a long time in the hospital setting during the
transplant
5 18
I do not believe it will dramatically improve my life expectancy 4 20
I feel my quality of life will be worse with transplant 3 21
I am worried about graft versus host disease 2 22
I am worried about dying from the transplant 2 22
Views on Bone Marrow Transplant: A Survey of
Patients with Myelofibrosis

Transplant Outcomes for Patients with Secondary Acute Myeloid Leukemia
(AML) Arising from Myeloproliferative Neoplasms (MPN).
METHODS
• All patients with AML arising from MPN who underwent SCT at
MD Anderson Cancer Center (Jan 2001-Feb 2017) were
included.
• 54 patients that underwent SCT, 5 underwent SCT twice. Only
the data for the first SCT was included. Patients receiving cord
blood or haploidentical SCT (n=11) were excluded. Finally, 43
unique SCT events were included in the study.
Mithun Vinod Shah,et al

Characteristics Value (N=43)
Age in years, median (range) 59 (14-72)
Sex, N (%)
Female
Male
12 (28)
31 (72)
Pre-SCT % blasts, median (range)
Bone marrow
Peripheral
5 (0-86)
1.5 (0-68)
Pre-SCT line of chemotherapy, median (range) 1 (0-5)
Donor Type, N (%)
Matched related
Matched unrelated
17 (40)
26 (60)
Cell Source, N (%)
BM
PB
9 (21)
34 (79)
HCT-CI, median (range)
≤4
>4
4 (0-11)
29 (67)
14 (33)
Melphalan in conditioning regimen, N (%)
Yes
No
14 (33)
29 (67)
Pre SCT, N (%)
7+3
Ara-C
JAK2i
HMA
29 (67)
7 (16)
9 (21)
10 (23)
Treatment with JAK2i/HMA pre-SCT, N (%)
No/ No
Yes / No
No / Yes
Yes / Yes
31 (72)
2 (5)
3 (7)
Transplant Outcomes for Patients with Secondary Acute Myeloid Leukemia
(AML) Arising from Myeloproliferative Neoplasms (MPN).

RESULTS
• Four (9.3%) patients had early death, and 38 (88.4%) patients
engrafted.
• Twenty eight patients died with AML recurrence being the most
common cause of death (n=17, 61%).
• The median follow up in patients alive was 41 months (5-170).
• The median PFS and OS were 6 and 15 months respectively.
• At 4 years:
• PFS: 31%,
• OS:38%
• Non-relapse mortality:24%
• Progression:43%
Mithun Vinod Shah,et al
Transplant Outcomes for Patients with Secondary Acute Myeloid Leukemia
(AML) Arising from Myeloproliferative Neoplasms (MPN).
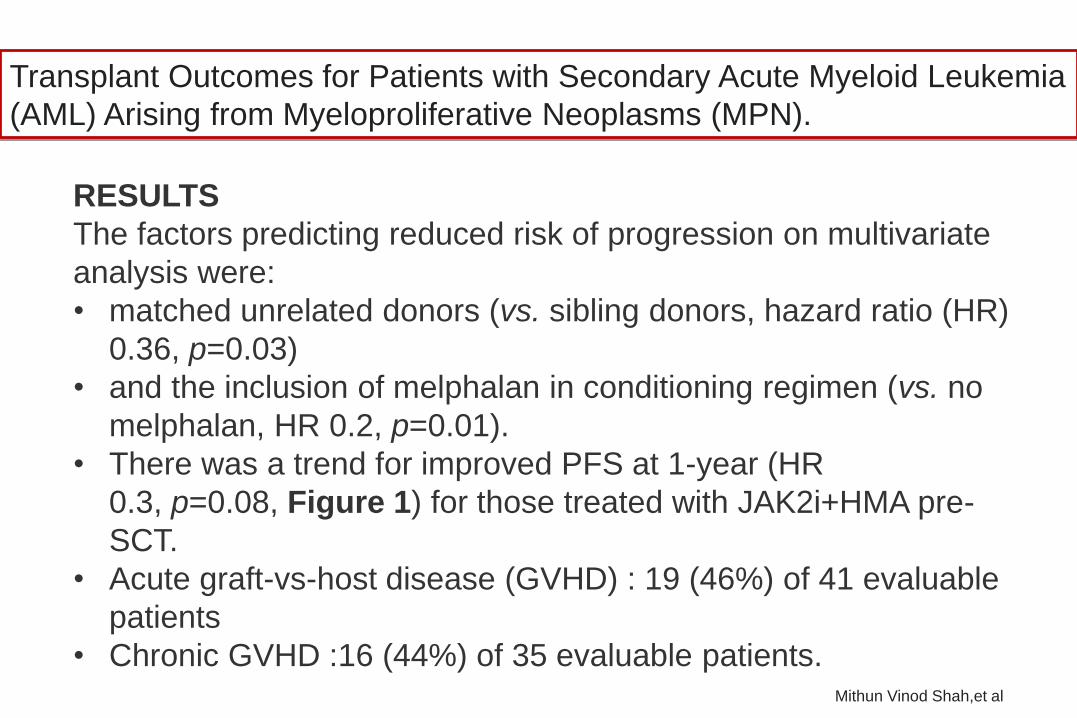
RESULTS
The factors predicting reduced risk of progression on multivariate
analysis were:
• matched unrelated donors (vs. sibling donors, hazard ratio (HR)
0.36, p=0.03)
• and the inclusion of melphalan in conditioning regimen (vs. no
melphalan, HR 0.2, p=0.01).
• There was a trend for improved PFS at 1-year (HR
0.3, p=0.08, Figure 1) for those treated with JAK2i+HMA pre-
SCT.
• Acute graft-vs-host disease (GVHD) : 19 (46%) of 41 evaluable
patients
• Chronic GVHD :16 (44%) of 35 evaluable patients.Mithun Vinod Shah,et al
Transplant Outcomes for Patients with Secondary Acute Myeloid Leukemia
(AML) Arising from Myeloproliferative Neoplasms (MPN).

Transplant Outcomes for Patients with Secondary Acute Myeloid Leukemia
(AML) Arising from Myeloproliferative Neoplasms (MPN).

Haploidentical Transplantation Outcomes for
Secondary Acute Myeloid Leukemia –
on Behalf of the ALWP of the EBMT
• 166 pts with sAML who received Haplo-HCT between 2006-2016 (prior
MDS/MPN=128; OMHD=15; solid tumor=17; BMFS=6) were studied.
• Median age at Haplo-HCT was 60 years and time from diagnosis to Haplo-HCT 5
months.
• Median follow-up of surviving pts was 24 months. At transplantation, 77 pts were in
CR1 while 89 had active disease.
• 63 pts received ablative (MAC) and 103 reduced-intensity conditioning (RIC)
regimen.
• MAC conditioning was mostly with thiotepa, busulfan, and fludarabine (TBF) in 34
pts (54%) and RIC with TBF and fludarabine-TBI in 28 (27%) and 35 (34%) pts,
respectively.
• 35 pts received ATG, 119 received post-transplant cyclophosphamide (PTCy), and
12 received both.
.
Zhuoyan Li, et al

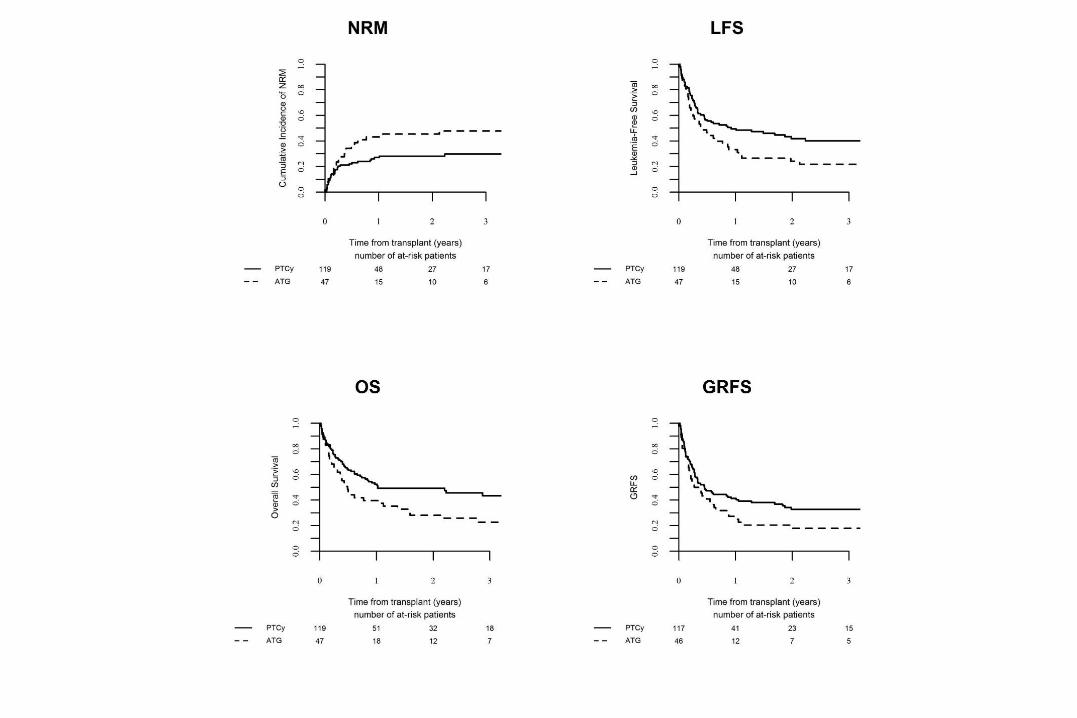
Haploidentical Transplantation Outcomes for Secondary Acute Myeloid Leukemia – on Behalf of the ALWP of the EBMT-
• Myeloid engraftment was achieved in 146 (88%) pts.
• 39 (25%) developed acute GVHD (grade II-IV) by day 100.
• The 2-year cumulative incidence of chronic GVHD: 25.5% , relapse
(RI): 30.3% and non-relapse mortality (NRM): 33.3%.
• 2 y Overall survival (OS): 42.5%, leukemia free survival (LFS):
36.4% and GVHD-free/relapse free survival (GRFS) 28.3%.
• Multivariate analysis:
• Active disease resulted in higher RI and inferior LFS, OS, and
GRFS compared with patients in CR1 at time of Haplo-HCT.
• PTCy was associated with lower NRM and superior LFS, OS,
and GRFS compared to ATG (HR 2.25, 2.01, 2.16, and 1.73,
respectively with p values <0.05; Figure 1) and a trend for
higher RI (HR=2.02, p=0.052).
Zhuoyan Li, et al
Haploidentical Transplantation Outcomes for
Secondary Acute Myeloid Leukemia –
on Behalf of the ALWP of the EBMT

Hematopoietic stem cell
transplantation in myelofibrosis: a
comparison between myeloablative and
reduced intensity conditioning
Funke VAM; Furtado VF; Santos GR; Sinamura LA;
Fagundes T; Nunes EC; Sola CB; Medeiros LA;
Pasquini R; Malvezzi M
Asbmt 2012

Instituições Participantes
• UFPR
• HNSG
• JAU
• INCA
• UFMG
• UNICAMP
• Einstein
• UFRGS
• USP-RP
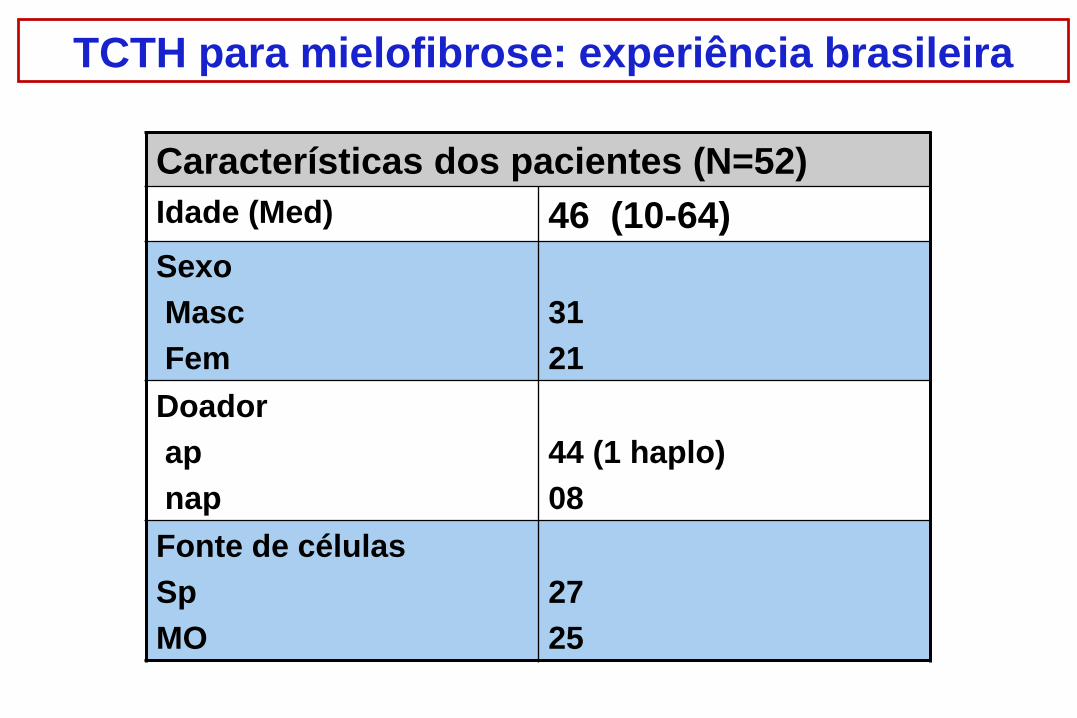
TCTH para mielofibrose: experiência brasileira
Características dos pacientes (N=52)
Idade (Med) 46 (10-64)
Sexo
Masc
Fem
31
21
Doador
ap
nap
44 (1 haplo)
08
Fonte de células
Sp
MO
27
25
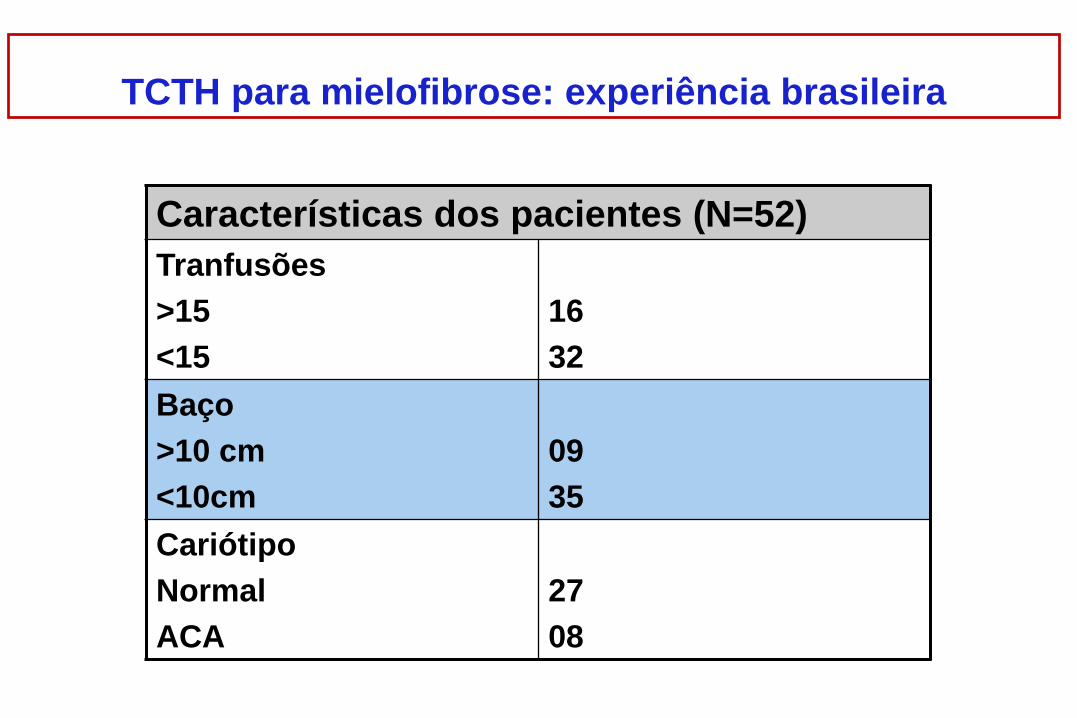
TCTH para mielofibrose: experiência brasileira
Características dos pacientes (N=52)
Tranfusões
>15
<15
16
32
Baço
>10 cm
<10cm
09
35
Cariótipo
Normal
ACA
27
08
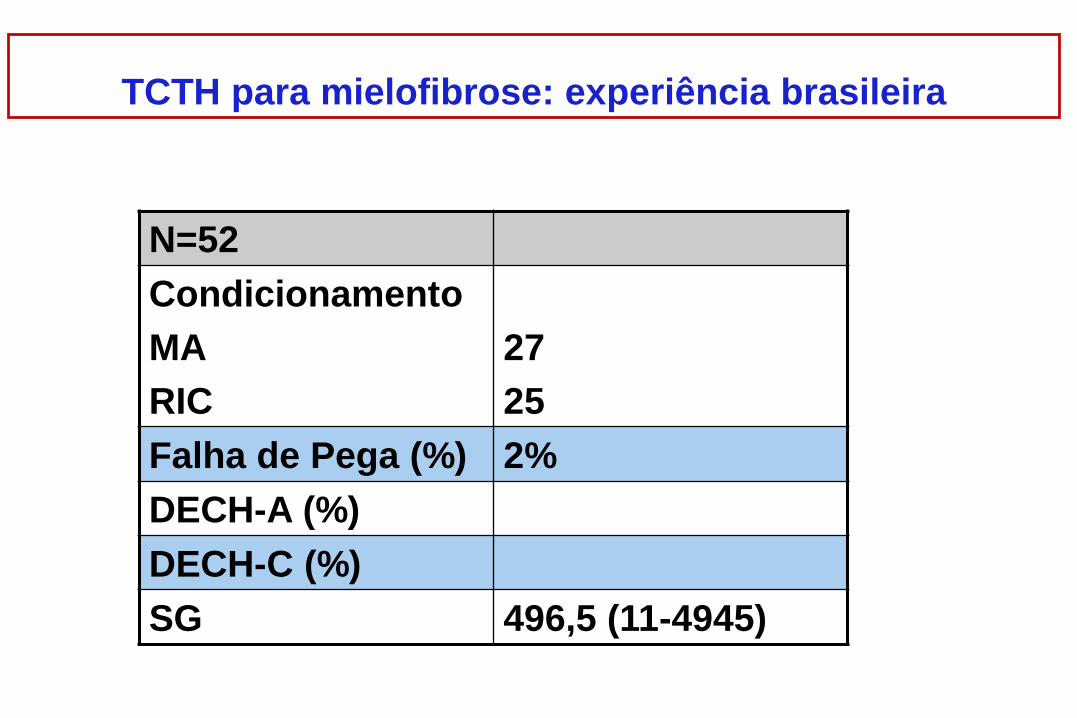
N=52
Condicionamento
MA
RIC
27
25
Falha de Pega (%) 2%
DECH-A (%)
DECH-C (%)
SG 496,5 (11-4945)
TCTH para mielofibrose: experiência brasileira

Sobrevida Global
0 2 0 0 0 4 0 0 0 6 0 0 0
0
2 0
4 0
6 0
8 0
1 0 0
T im e
Pe
rc
en
t s
urv
iva
l
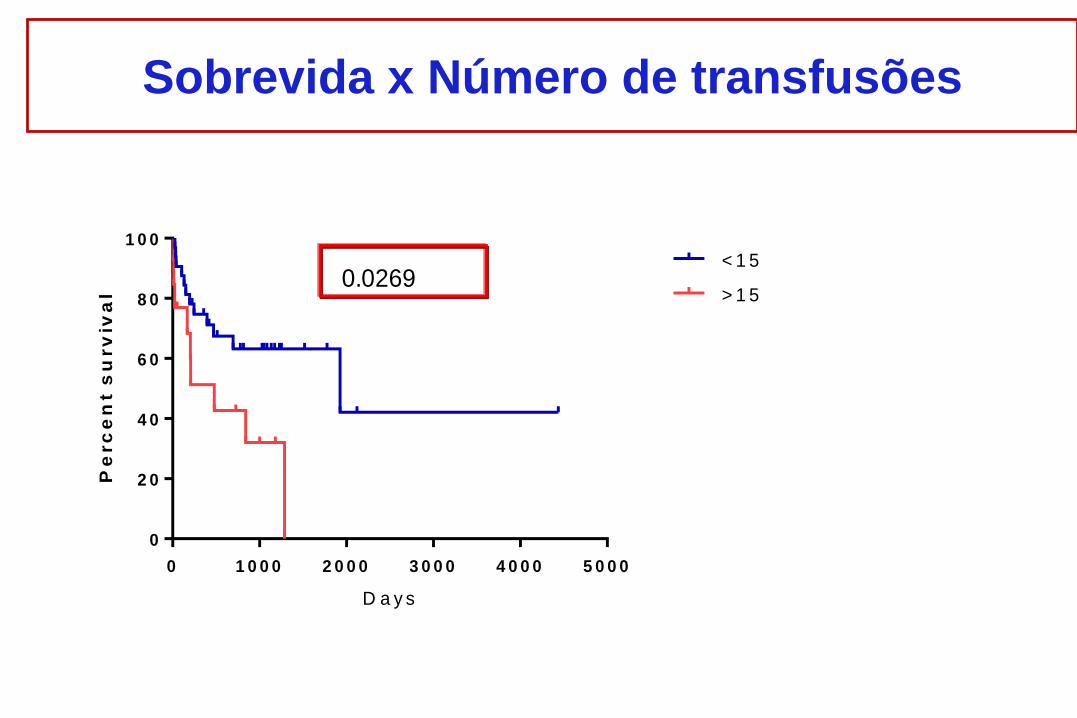
Sobrevida x Número de transfusões
0 1 0 0 0 2 0 0 0 3 0 0 0 4 0 0 0 5 0 0 0
0
2 0
4 0
6 0
8 0
1 0 0
D a y s
Pe
rc
en
t s
urv
iva
l
< 1 5
> 1 50.0269

Tipo de doador
0 2 0 0 0 4 0 0 0 6 0 0 0
0
2 0
4 0
6 0
8 0
1 0 0
S u rv iva l
Pe
rc
en
t s
urv
iva
l
a p
n a
0.0057

Sobrevida x esplenomegalia
P= 0,0187
0 1 0 0 0 2 0 0 0 3 0 0 0 4 0 0 0
0
2 0
4 0
6 0
8 0
1 0 0
S u rv iva l
Pe
rc
en
t s
urv
iva
l
b a c o < 2 0
B a c o > 2 0

Irradiacao esplenica como parte do condicionamento de
pacientes com Mielofibrose submetidos a HSCT
•Vaneuza A.M. Funke (Resp. Técnico STMO Adulto UFPR)
•Nelson Hamerschlak ( Hospital Albert Einstein)
•Mary Evelyn Flowers (FHCRC)

Proposta
• Estudo Piloto
• N= 10
• Endpoint primario : pega do enxerto
• Cond : Flu 150+ Bu 10-16 + ATG
• CTP
• Irradiacao esplenica 4 Gy -8 e -7

Agradecimentos
• Marco Bitencourt
• Daniela Setubal
• Caroline Bonamin
• Michel Oliveira
• Samir Nabhan
• Ricardo Pasquini

















