95
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | ancy-das |
| View: | 399 times |
| Download: | 0 times |


A N C Y M DA S2 N D Y R M S C N S G
J I P M E R
HISTORICAL DEVELOPMENT, TRENDS AND ISSUES IN THE FIELD OF
CARDIOLOGY. ETHICAL AND LEGAL ISSUES

THE HISTORY OF CARDIOVASCULAR MEDICINE
THE HISTORY OF CARDIOVASCULAR MEDICINE
1. The beginning
The conception
The birth
The early years
Cardiac catheterization

1. The beginning
1. The conception
‘Huang Ti Na-Ching Su Wen’, China's Yellow Emperor's Classic on Medicine, published circa 2600 BC, was aware of the heart and circulation, writing: ‘The blood current flows continuously in a circle and never stops’.
The importance of the heart to the sustenance of life was appreciated by the ancient Egyptians as early as 2000 BC.
In London, William Harvey conducted the first hypothesis-driven experiments in biology.

1. The beginning The conception…
In 1628, decades before Isaac Newton, Harvey published his monumental book De motu cordis, in which he described the circulation and the function of the heart.
Heberden - classic description of angina pectoris in 1772
In 1785, Withering, a British physician, described foxglove (digitalis), its use in ‘dropsy’ (oedema), and in strengthening and slowing the heart.
Brunton described the use of amyl nitrite in the treatment of angina.
1. The beginning The conception…
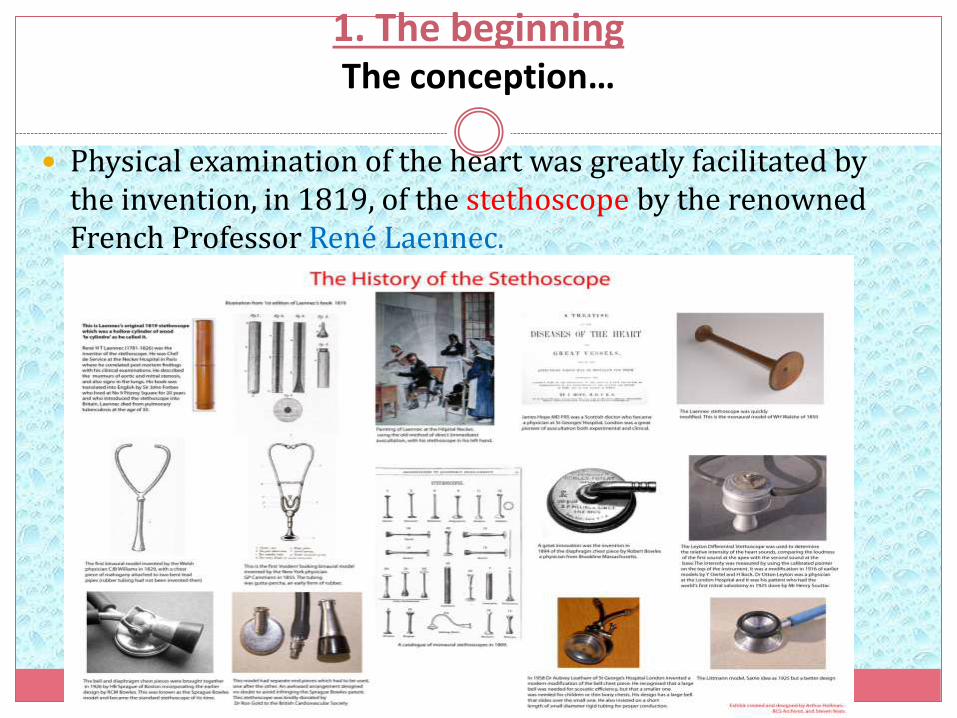
Physical examination of the heart was greatly facilitated by the invention, in 1819, of the stethoscope by the renowned French Professor René Laennec.

The beginning 2. The birth
A technical revolution swept over the medical world at the turn of the twentieth century with three discoveries, each of which contributed importantly to the birth of cardiology.
The first of these, in 1895, was diagnostic X-ray by Wilhelm Roentgen, a German physicist who received the first Nobel prize in physics for this accomplishment.

The beginning 2. The birth…
The second was a practical, non-invasive measurement of blood pressure made possible by the twin developments of the blood pressure cuff by Riva Rocciin Turin, Italy in 1896, and its use in the auscultatorymeasurement of blood pressure by Korotkoff in St. Petersburg, Russia in 1905.

The beginning 2. The birth…
The third was the string galvanometer for
recording cardiac potentials on the surface of the body, the electrocardiograph, which was described by Einthoven in 1902; he, too, was rewarded with a Nobel Prize.
Physicians who used all three of these new tools in addition to clinical findings to study their patients became identified as the first ‘heart specialists’, i.e. cardiologists

The beginning 2. The birth…
In 1901, Krehl, a Viennese physician, appears to have been the first to report that coronary occlusion in patients is associated with chest pain, that it causes acute myocardial infarction (AMI), and that it is not uniformly fatal.
In 1910, Obratzov and Strazhenko in Kiev, described five patients with AMI. They reported that unusually heavy exertion and intense emotion could be precipitants.
Herrick, a Chicago physician, who alerted the English speaking world to AMI and was also the first to describe electrocardiographic changes in this condition.

The beginning 2. The birth…
Biochemistry and experimental pathology were the next sciences to exert important impacts on cardiology.
In 1910, Adolf Windhaus, the Nobel Prize-winning German organic chemist, described the presence of cholesterol in human aortic plaques
And in 1913, two young Russians, Anitschkov and Chalatow, carried out one of the most important experiments in the early history of cardiology which gave rise to the lipid theory of atherogenesis.
Thus, modern cardiology was born in Europe and it then spread rapidly to the rest of the world.

The beginning 3. The early years
Cardiology quickly developed its own journals and societies, both of which are features of a separate medical specialty.
In 1908, both the Archives des Maladies du Coeur in France and the Zentralblattfur Herzkrankheiten in Germany commenced publication.
In 1909, Heart, the first English language journal, was started.
In Italy, Malatti du cuore began publication in 1916 and the American Heart Journal in 1925.
Reflecting continental and global interests, the European Heart Journal was begun in 1980 and the International Journal of Cardiology in 1981.
At the present time, 114 print cardiology journals are listed in the Index Medicus, and the number of online-only journals is growing rapidly.

The beginning 3. The early years…
The British Cardiac Club was founded in 1922 and became the British Cardiac Society in 1937.
The American Heart Association was begun in 1924.
The Belgian, Italian, French and Swiss Cardiac Societies were formed in 1934, 1935, 1937 and 1948, respectively.
In the US, a second important organization, the American College of Cardiology was established in 1949.
National governments also began to support cardiac research.
In the United States, the National Heart Institute (now the National Heart, Lung and Blood Institute) was established in 1948.

The beginning 4.Cardiac catheterization
In 1929 Werner Forssmann, a resident in urologic surgery in Eberswalde, Germany, carried out the first cardiac catheterization, and on himself!
His goal was to develop a method of injecting drugs into the heart.
Cardiac catheterization, first as a research, and later as a diagnostic tool, was begun in 1941 at Columbia University/Bellevue Hospital in New York by Andre Cournand (formerly a French pulmonary physiologist) and Dickinson Richards, who systematically investigated the haemodynamics in every important cardiac condition.
They and Forssmann shared a Nobel Prize.
By the 1960s, cardiac catheterization had spread to most large hospitals in the industrialized world and had become an indispensible cardiac diagnostic procedure.

The beginning 4.Cardiac catheterization…
Catheter-based treatments of arrhythmias, including pacemakers and internal cardioverter defibrillators followed and catheter-based replacement of the aortic valve.
Coronary arteriography, first carried out accidentally and then developed by Sones in Cleveland in 1958.
Coronary arteriography allowed the diagnosis and aided in the management of patients with ischaemic heart disease.


The beginning 4.Cardiac catheterization…
Gruntzig and coworkers in Zurich, developed transluminal coronary angioplasty; which was followed by the development of stents and other refinements of percutaneous coronary intervention.

2. Milestones in the evolution of cardiology
Treatment of acute myocardial infarction
Acute coronary syndromes
Imaging
Cardiac surgery
Arrhythmias
Valvular heart disease
Heart failure
Prevention

1. Treatment of acute myocardial infarction
In his classic 1912 paper on AMI, Herrick stated ‘the importance of absolute rest in bed … is clear’and for five decades bed rest was the cornerstone of therapy
Practice gradually changed; ambulation was accelerated and convalescence shortened.
The development of the coronary care unit (CCU) was one of a pair of signal advances in the treatment of AMI. The idea of the CCU was proposed in 1961 by Julian, then a medical registrar at the Royal Infirmary, Edinburgh.

Treatment of acute myocardial infarction…
Four separate concepts made the CCU possible:
(i) aggregating patients into a single area of the hospital where trained personnel, equipment and drugs are all available;
(ii) continuous monitoring of the ECG;
(iii) development of closed-chest cardiac resuscitation for ventricular fibrillation; and
(iv) delegation of the immediate treatment of ventricular fibrillation and other life-threatening arrhythmias to trained nurses, in the absence of a physician.

Treatment of acute myocardial infarction…
In the 1970s, the Soviet cardiologist Chazov and coworkers gave birth to the modern era of management of AMI with the second signal advance in the care of patients with AMI, i.e. reperfusion of the ischaemic myocardium by infusion of streptokinase directly into the thrombotically occluded coronary artery in an effort to limit infarct size.
Chazov's paper was not translated and had little impact outside the Soviet Union. In 1979, Rentrop et al. introduced this treatment to the rest of the world.
Thus, limiting infarct size and thereby reducing mortality had moved from the experimental laboratory to the hospital emergency room.

2.Acute coronary syndromes
In the first half of the twentieth century, ischaemia was clearly divided into two separate categories, transient ischaemia, which caused chronic angina and prolonged ischaemia at rest which was responsible for AMI.
In the late-1930s, clinicians began to identify a third syndrome, having some characteristics of both of these conditions. This condition, ultimately named unstable angina, was considered to be severe angina occurring at rest.
it has become apparent that the majority of cases of unstable angina are, in fact, small non-ST segment elevation AMIs (NSTEMI).
In these patients, coronary arteriography often shows multi-vessel obstructive coronary artery disease without recent total occlusion and are not helped by fibrinolytic therapy and those that are at high risk require prompt, coronary revascularization.

3. Imaging
Until the end of the nineteenth century, the disordered structure and function of the heart could not be ascertained in living humans.
The first approaches to cardiac imaging, radiography and fluoroscopy, followed by peripheral angiocardiography and then selective angiocardiography, have overcome this barrier.
we now have various modes of echocardiographyavailable, a technique first described in 1954 by Edler and Hertz in Sweden, computed X-ray tomography, magnetic resonance imaging and spectroscopy, radionuclide imaging, and positron emission tomography.

4. Cardiac surgery
The modern era of cardiac surgery began in the early 1950s with the development of open heart surgery using cardiopulmonary bypass, which was necessary for the successful repair of most congenital and many acquired cardiac disorders.
This ushered in a series of spectacular collaborations between surgeons and engineers. The development of prosthetic heart valves led to astounding benefits in the lives of patients with severe valvular heart disease.
Coronary artery bypass grafting, begun by DeBakey et al. in Houston in 1964 provides relief from angina pectoris that is refractory to medical management, and has improved the survival of patients, such as those with left main coronary artery disease and three-vessel disease.

5. Arrhythmias
Serious bradyarrhythmias—particularly advanced atrioventricularblock—was the first arrhythmia to be controlled, initially by an external pacemaker by Zoll in Boston in 1952 and then an implanted cardiac pacemaker, developed by Elmqvist and Senning in Stockholm in 1958.
This was followed by the development of external cardioversion of ventricular fibrillation, ventricular tachycardia, and atrial fibrillation.
The development of implantable cardioverter-defibrillators by Mirowski et al. has proved to be life-saving in patients having ventricular fibrillation and sudden cardiac death.
Progressive improvements in electrophysiological testing and endocardialelectrical mapping have led to the abolition of a number of arrhythmias, including paroxysmal supraventricular and ventricular tachycardias.

6. Heart failure
Although heart failure was recognized as a clinical entity in the eighteenth century, the causes were obscure; no effective therapies other than digitalis were available, and the prognosis was dismal.
Mercurial diuretics were introduced in the 1920s, but these drugs were only of modest efficacy and required painful, deep intramuscular injections.
Development of effective oral diuretics; the benzothiadiazines in 1957, the aldosterone inhibitors in 1959, and the powerful ‘loop diuretics’ in 1962.
The next important step was vasodilator therapy, which was first administered intravenously in acute heart failure

6. Heart failure…
Cohn et al. then led a multicentre trial, the VHEFT trial, which showed improved survival in patients with chronic heart failure who received the combination of hydralazine and a long-acting nitrate.
Next came the application of neurohormonal blockers—angiotensin-converting enzyme inhibitors, beta-adrenergic receptor blockers, and aldosterone inhibitors—each of which was shown to improve prognosis.
Cardiac transplantation, introduced in 1967, is effective in prolonging life by about 10 years in end-stage heart failure, but because of a donor shortage, it is available only to a small fraction of patients who could benefit.

7. Prevention
Up to the middle of the twentieth century, the practice of cardiology focused on the treatment of patients with established, often advanced, cardiovascular disease and most treatment were symptomatic.
Prevention of cardiovascular disease was not deemed possible, and rarely mentioned.
At mid-century, the occurrence of an AMI was usually totally unexpected. Most commonly it struck down apparently healthy persons in their most productive years.
However, by 1961, investigators in the Framingham Heart Study had shown that overtly healthy subjects with hypertension and hypercholesterolaemia were at higher risk of developing AMI ; they coined the term ‘coronary risk factors’.
7. Prevention
An array of additional coronary risk factors is now recognized which include age, gender, family history, cigarette smoking, low HDL-cholesterol, elevated lipoprotein, diabetes, inflammation, and chronic kidney disease.
The identification of these risk factors has provided the basis for prevention of atherosclerotic vascular disease.
Healthy lifestyles, weight control, cessation of smoking, reduction of low-density lipoprotein cholesterol, and control of blood pressure have substantially reduced the incidence and recurrence of AMI, acute coronary syndromes, stroke, and coronary deaths.

3. The present
Evidence-based cardiological practice
The rise of global cardiology
The growth of cardiovascular centres

4.The future
The near term future, i.e. approximately the next decade, is likely to see an increasing prevalence of atherosclerotic disease worldwide, with the ageing of the population and the rise in obesity and diabetes.
Efforts will be intensified to start preventive therapy, such as changes in diet and the use of statins, progressively earlier in life.
Perhaps, inexpensive ‘polypills’ containing aspirin, an angiotensin-converting enzyme inhibitor, a thiazide diuretic and a statin, or some variation thereof, will prove to be of value for primary and secondary prevention in selected persons in developing nations.
Successful use of stem-cell therapy in the prevention and treatment of heart failure following AMI and in some forms of chronic heart failure is likely.
Pluripotent stem cells derived from the patient's own cell types, including fibroblasts, are particularly interesting.

4.The future…
There will be enormous advances and rapidly growing use of smaller, more reliable, safer, and less-expensive implanted ventricular assist pumps as ‘destination therapy’.
When all else fails, gene therapy may be employed .
It will be necessary to set up new, specialized clinics to care for patients who receive cell-based, device-based, and combination therapy for heart failure and AMI.
MILESTONES IN CARDIOLOGY
1628 : William Harvey, an English physician, first described blood circulation.
1706 : Raymond de Vieussens, a French anatomy professor, first describes the structure of the hearts chamber and vessels.
1733 : Stephen Hales, an English clergyman and scientist, first measured blood pressure.
1801 : Francisco Romero ,a Spanish surgeon done the first cardiac surgery known as Open Pericardiostomy
MILESTONES IN CARDIOLOGY…
1816 : Rene T.H. Laennec, a French physician, invents the stethoscope.
1896 : Dr. Ludwig Rehn, a German Surgeon Performed first successful heart surgery on human being without any complications; he stitched a wound on the heart of German soldier.
1899: Two Swiss physiologists introduces the process of defibrillation on dogs heart
MILESTONES IN CARDIOLOGY…
1903 :Willem Einthoven, a Dutch physiologist, develops the electrocardiograph.
1912 : James B. Herrick, an American physician, first describes heart disease resulting from hardening of the arteries.
1938 :Robert E. Gross, an American surgeon, performs first open heart surgery.
1947: Defibrillator was first time used on human being during the open heart surgery by Dr. Claude Beck(Prof. Surgeon at Western Reserve University)

MILESTONES IN CARDIOLOGY…
1951 :Charles Hufnagel, an American surgeon, develops a plastic valve to repair an aortic valve.
1952 : F. John Lewis, an American surgeon performs first successful open heart surgery.
1952 : Dr. John F. Lewis, an American Surgeon used hypothermia to temporarily slow down the heart beat making it accessible to lengthen the time of Open Heart Surgery.
1953 :Jhon H. Gibbon, an American surgeon, first uses a mechanical heart and blood purifier.

MILESTONES IN CARDIOLOGY…
1954 : First cross circulation operation was performed by Dr. C. Walton Lillihie(American Surgeon)
1961: J.R.Jude, an American cardiologist, leads a team performing the first external cardiac massage to restart a heart.
1964: Dr. James D. Hardy of the University of Mississippi, attempted the first heart transplant from a nonhuman primate – a chimpanzee named Bino -- into a human. The patient was 68-year-old Boyd Rush. After only 90minutes, the heart stopped functioning because it was too small to maintain circulation on its own .

MILESTONES IN CARDIOLOGY…
1965 :Micheal DeBakey and Adrian Kantrowitz, American surgeons, implanted mechanical devices to help a diseased heart.
1967: Dr. Rene Favaloro , an American Surgeon used a vein from the leg to bypass a blocked coronary artery. This procedure, known as coronary artery bypass surgery .
1967 :Christian Barnard , a South African surgeon, performs the whole heart transplant from one person to another.

MILESTONES IN CARDIOLOGY…
1974: Andreas Gruentzig performed the first peripheral human balloon angioplasty.
1980 : Michel Mirowski , a Polish Cardiologist, the first ICD (Implantable Cardioverter Defibrillators) --weighing 9 ounces and about the size of a deck of cards –was implanted into a human patient.
1982 : Willem DeVries, an American surgeon, implants a permanent artificial heart, designed by Robert Jarvik, an American physician, into a patient.
CARDIOLOGY'S 10 GREATEST DISCOVERIES OF THE
20TH CENTURY
1. Electrocardiography
2. Preventive Cardiology and the
Framingham Study
3. “Lipid Hypotheses” and Atherosclerosis
4. Coronary Care Units
5. Echocardiography
CARDIOLOGY'S 10 GREATEST DISCOVERIES OF THE 20TH
CENTURY…
6. Thrombolytic Therapy
7. Cardiac Catheterization and Coronary
Angiography
8. Open-Heart Surgery
9. Automatic Implantable Cardiac
Defibrillators
10. Coronary Angioplasty

RECENT ADVANCES AND FUTURE TRENDS IN CARDIOLOGY
Clinical Cardiology
Interventional Cardiology
Stem Cell Therapy
Cardiac Imaging
X-ray imaging Computed Tomography (CT) Magnetic Resonance (MR) imaging Nuclear Medicine imaging Ultrasound

Clinical Cardiology
Clinical cardiology is never static and lot of effort is put on development of better drugs.
The most recent has been the approval and availability of newer thenopyridine prasugrel which is used in treatment of acute coronary syndromes for those proceeding to percutaneous interventions.
For management of angina we have newer drugs ivabridine and ranolazine as add on therapy.

Clinical Cardiology…
Dabigatran an oral anticoagulant is a very exciting addition in stroke and embolism prevention in patients with atrialfibrillation.
it does not require INR monitoring as compared to warfarin
superior to warfarin in reducing stroke or peripheral embolic events.
Less risk of hemorrhage is an added attraction.
Newer antiarrhythmics have become available which includes drugs like dronedarone which is indicated in prevention of recurrence of atrial fibrillation.
Compared to amiodarone the incidence of pulmonary, hepatic and thyroid related side effects is almost negligible.

Interventional Cardiology
There have been exciting developments in the field of interventional cardiology too.
On catheterization table, assessment of lesion severity using Fractional Flow Reserve (FFR) has gained prominence lately.
FFR represents the maximum achievable blood flow after challenge with adenosine to myocardium supplied by stenotic artery as a fraction of normal maximum value.
A value of less than 0.75 identifies stenosis with inducible ischemia.
This has made multi vessel disease angioplasty much more evidence based and unnecessary stenting in physiologically normal lesions is avoided.
Interventional Cardiology…
Recently lot of interest has been generated by concept of thrombus aspiration in primary percutaneousintervention.
In a Bayesian meta-analysis, adjunctive thrombectomyimproves early markers of reperfusion but does not substantially effect 30-day post-MI mortality, reinfarction, and stroke.
Thrombectomy is one of the rare effective preventive measures against no-reflow.
Interventional Cardiology…
Local drug delivery viz Drug Eluting Balloons (DEB) have generated lots of interest lately.
Rationale for the development of DEB derives mainly from the limitations of Drug Eluting Stents (DES).
DEB may be used in subsets of lesions where DES cannot be delivered or where DES do not perform well, such as in tortuous vessels, small vessels, or long diffuse calcified lesions, which can result in stent fracture
The most appealing indication for paclitaxel eluting balloons would be for the treatment of ISR.

Advantages of DEB…
Additional potential advantages include (a) homogenous drug transfer to the entire vessel wall;
(b) rapid release of high concentrations of the drug sustained in the vessel wall no longer than a week, with little impact on long term healing;
(c) absence of polymer could decrease chronic inflammation and the trigger for late thrombosis;
(d) absence of a stent allows the artery’s original anatomy to remain intact, notably in cases of bifurcation or small vessels, thereby diminishing abnormal flow patterns; and
(e) with local drug delivery, overdependence on antiplatelet therapy could be curtailed.

Interventional Cardiology…
Percutaneous coronary intervention (PCI) with bioabsorbablestents has created interest recently.
The need for mechanical support for the healing artery is temporary, and beyond the first few months there are potential disadvantages of a permanent metallic prosthesis.
Biodegradable stents contain a biodegradable polymer or are completely biodegradable.

Interventional Cardiology…
Till now management of valvular heart disease was mostly a surgical domain.
Recently, the potential for less invasively replicating these successful surgical procedures without the need for thoracotomy or cardiopulmonary bypass has generated considerable interest.
The Mitraclip device has proven relatively safe and often effective.
Using a multiaxial transeptal catheter system, a metallic clip is used to grasp and approximate the free edges of the 2 leaflets

Interventional Cardiology…
Balloon aortic valvuloplasty replacing Surgical aortic valve replacement for patients with symptomatic severe aortic valve stenosis.
Percutaneous aortic valve replacement (PAVR) using stent-based prostheses has emerged as a promising new option in recent years

Stem Cell Therapy
Stem cell therapy as applied to cardiology has shown partial progress.
The angina in so called end stage coronary artery disease is refractory to conventional medical therapy.
Laboratory and preclinical studies have provided evidence for the safety and potential efficacy of autologous CD34+ stem cell therapies as treatment for angina.
Stem Cell Therapy
Clinical studies investigating intramyocardialtransplantation of autologous CD34+ stem cells by catheter injection for patients with refractory angina show that this is safe and feasible.
Role of stem cells in heart failure is also under evaluation.
There appeared to be a significant decrease in long-term mortality in the stem-cell-treated patients.

Cardiac Imaging
X-ray imaging
Computed Tomography (CT)
Magnetic Resonance (MR) imaging
Nuclear Medicine imaging
Ultrasound
RECENT ADVANCES AND FUTURE TRENDS IN CARDIOLOGY…
Minimally Invasive Heart Surgery.
Types of Minimally Invasive Heart Surgeries
Minimally Invasive Valve Surgery
Minimally Invasive CABG Surgery
Off-pump/beating heart bypass surgery

RECENT ADVANCES AND FUTURE TRENDS IN CARDIOLOGY…
Benefits of minimally invasive surgical techniques
Small incisions.
Small scars.
Shorter hospital stay after surgery .
Low risk of infection.
Low risk of bleeding and blood transfusion .
Shorter recovery time and faster return to normal activities/work.
Division of the sternum is not needed for robotically assisted heart surgery

RECENT ADVANCES AND FUTURE TRENDS IN CARDIOLOGY…
Robotically Assisted Heart Surgery
Types of Robotically Assisted Heart Surgeries
Robotically Assisted Valve Surgery.
Robotically Assisted Bypass Surgery.
Robotically Assisted ASD .
Robotically Assisted Removal of Cardiac Tumors .

ISSUES OF CARDIOLOGY
CARDIOVASCULAR DISEASES
Coronary artery disease (CAD)
Congestive heart failure (CHF)
Arrhythmias

CARDIOVASCULAR DISEASES
Coronary artery disease (CAD) is still the major cardiovascular pathology, and is expected to remain so for the foreseeable future.
However, improved treatment of CAD has resulted in an increased survival rate, so that there is an increasing incidence of patients with severe myocardial scars caused by previous infarction.
These weakened hearts will lead to an increase in the number of patients suffering from congestive heart failure (CHF), who will form an increasingly important group.

CARDIOVASCULAR DISEASES….
A third group of patients that is expected to become increasingly important is that of patients with cardiac arrythmias.
While the number of congenital arrythmias will remain more-or-less constant,
the aging population will increase the incidence of atrialfibrillation, and the increased number of heart attack survivors will result in an increase in the incidence of ischemic ventricular tachycardia and the related risks of sudden death.

LEGAL AND ETHICAL ISSUES IN
CARDIOVASCULAR MEDICINE

LEGAL AND ETHICAL ISSUES IN CARDIOVASCULAR MEDICINE
Clinical ethics “provides a structured approach for identifying, analyzing, and resolving” moral problems and ethical dilemmas that arise while caring for patients.
Four ethics principles address most of these problems—
beneficence,
nonmaleficence,
respect for patient autonomy, and
justice.
Ethics principles
Beneficence refers to the clinician's duty to promote the best interests of patients.
Nonmaleficence refers to the duty to prevent or avoid doing harm to patients.
Respect for patient autonomy refers to the duty to respect patients’ values, goals, and rights of self-determination.
Justice refers to the duty to treat patients fairly (i.e., based on medical need, not on patient characteristics such as ethnicity and gender).
Common Ethical Dilemmas InCardiovascular Medicine
1. Promoting Beneficence Beneficence requires that clinicians promote the interests of
patients, which take precedence over the clinicians’ self-interests.
Beneficent clinicians maintain clinical competence and strive for quality, safety, and continuous improvement in clinical practice.
Beneficence requires that clinicians completely and clearly share their assessments and recommendations with patients and ensure that patients understand them.
Recommendations should not be presented as a menu of choices, but as a hierarchy of options based on efficacy, safety, and patients’ health care–related values, preferences and goals.

Common Ethical Dilemmas In Cardiovascular Medicine…
2. Preventing and Avoiding Harm to Patients
The ethics principle of nonmaleficence is closely coupled with the principle of beneficence.
Weighing the potential benefits versus the potential harms of a diagnostic or therapeutic intervention is common in clinical practice.
Needless to say, clinicians should prevent or minimize harms associated with any intervention.
Nonmaleficence also requires that clinicians not abandon patients.
conflicts of interests should not compromise clinicians’ nonmaleficence duties

Common Ethical Dilemmas In Cardiovascular Medicine…
3. Ensuring Informed Consent and Informed Refusal
Consent problems arises because patients experiencing acute, life threatening illness that interfere with their ability to make decisions on treatment/ participation in clinical research.
The informed consent is based on the principle of autonomy.
Consent denotes voluntary agreement, permission or compliance.

Legal and Ethical Issues; Informed Consent
It implies to permission by the patient to perform an act on his body either for diagnosis or therapeutic procedure.
The four elements of consent are;
voluntariness
capacity
knowledge
Decision making

Points to be considered in consent…
Consent must be given voluntarily
If patient is not mentally capable (critical patients) informed consent should be obtained from surrogate or legal next of kin.
It should be given by a person of sound mind & above the age of 18 years.
Requires the disclosure of basic information considered necessary for decision making
Patients providing consent should be free from pain & depression.

Consent obtained from a minor
Consent given under fear, fraud or misrepresentation
Consent obtained from the person who is not fit
Consent obtained in language not understood by the person
Consent obtained from person under sedation, intoxication or semiconscious
Consent obtained without providing adequate information on the possible risks are invalid under law.

Common Ethical Dilemmas In Cardiovascular Medicine
4. Handling Medical Errors
The ethical rationale for disclosing errors to patients is strong.
First, clinicians should act in the best interests of the patient. Nondisclosure does not serve the patient and damages trust because many patients eventually learn of errors.
Second, respect for patient autonomy requires that clinicians disclose errors to patients to allow for informed decision-making.

Common Ethical Dilemmas In Cardiovascular Medicine…
Handling Medical Errors….
Third, justice requires that patients be given what is due to them, including information about their medical condition and compensation if appropriate (e.g., for injury).
Finally, clinicians should participate in efforts to prevent errors.
Handling Medical Errors….
Clinicians may feel uncomfortable disclosing errors to patients. The following steps can lessen this burden:
Disclosure should be done in private; the patient's loved ones and essential members of the health care team should be present. Interruptions should be avoided.
Before disclosing the error, the clinician should discern the patient's perception of the problem.

Handling Medical Errors….
When disclosing the error, the clinician should speak clearly and check for comprehension (e.g., “May I clarify anything?”).
After disclosing the error, the clinician should sincerely apologize and inform the patient that the clinician and organization will act to prevent future errors. The clinician should avoid attributing blame to others (e.g., “The nurse must have forgotten to tell me about your allergy.”).
The clinician should acknowledge the patient's response to the disclosure by using empathic statements (e.g., “I can see that you are upset by this news.”).
The clinician should describe a treatment and follow-up plan.
The clinician should document the discussion in writing.

Common Ethical Dilemmas In Cardiovascular Medicine…
5. Addressing Refusals of and Requests for Withdrawal of Life-Sustaining Treatments
Respect for patient autonomy is the ethics principle that underlies a patient's right to refuse or request the withdrawal of medical treatments
A patient also has the right to refuse previously consented treatments if their health care–related values, preferences, and goals have changed.
5. Addressing Refusals of and Requests for Withdrawal of Life-Sustaining Treatments…
Regardless of the clinician's intent, beginning or continuing a treatment that a patient has refused may be viewed from a legal standpoint as battery.
Dying patients (or their surrogates) may refuse or request the withdrawal of life-sustaining treatments (e.g., mechanical ventilation, hemodialysis, artificially administered hydration and nutrition, device therapies) that are perceived by the patients (or surrogates) as burdensome.
Withdrawal of life-sustaining treatments from dying patients who no longer want the treatment is widely practiced.

Common Ethical Dilemmas In Cardiovascular Medicine…
6. Fostering Advance Care Planning
Respect for patient autonomy is the ethics principle that underlies advance care planning.
Advance care planning is a process in which patients, working with their clinicians and loved ones, articulate their values, preferences, and goals regarding future health care decisions
One form of advance care planning is the do not resuscitate (DNR) order.
In general, cardiopulmonary resuscitation (CPR) is the default standard of care for cardiac arrest unless a DNR order has been written for the patient.

6. Fostering Advance Care Planning…
Advance care planning also includes completion of an advance directive.
ADs are health care instructions used when a patient lacks decision-making capacity.
The AD should be regarded as an extension of the autonomous patient.
Common types of ADs are the health care power of attorney, in which a patient designates another person for making future health care decisions, the living will, in which a patient lists preferences about future treatments, and the combined AD, which has features of both a health care power of attorney and a living will.

Common Ethical Dilemmas In Cardiovascular Medicine…
7. Ensuring Appropriate Surrogate Decision Making
Patients who lack decision-making capacity are incapable of being autonomous.
For these patients, clinicians must rely on surrogate decision-makers to make decisions for patients.
If the patient's AD names a surrogate, this choice should be honored.
If the patient does not have an AD, the ideal surrogate is one who best understands the patient's health care values, preferences, and goals.

Common Ethical Dilemmas In Cardiovascular Medicine…
8. Addressing Requests for Interventions
Many patients (or their surrogates) make requests for specific diagnostic and therapeutic interventions.
Many requests are reasonable and within standards of care; clinicians generally should grant these requests.
However, clinicians are not obligated to grant requests for interventions that are ineffective or violate their consciences.
Common Ethical Dilemmas In Cardiovascular Medicine…
9. Maintaining Patient Confidentiality
The ethics principle of respect for patient autonomy requires that clinicians maintain patient confidentiality.
Clinicians need access to patients’ medical information, ask sensitive questions and conduct thorough physical examinations to assess and treat patients properly.
Patients should trust that their personal and medical information will be kept confidential.

Common Ethical Dilemmas In Cardiovascular Medicine…
10. Bedside Allocation of Health Care Resources
The ethics principle of justice requires that clinicians treat patients fairly.
Injustice occurs when health care–related decisions are based on patient-specific factors such as gender, ethnicity, and religion, not on medical need.

THE HISTORY OF CARDIAC NURSING
The 1960s
first coronary care unit was founded at the Royal Infirmary in Edinburgh, Scotland, by Dr. Desmond G. Julian
cardiopulmonary resuscitation
The 1970s
cardiac care units and departments
more trained cardiac nurses skilled in CPR, cardiac monitoring and the administration of cardiac medicines.

THE HISTORY OF CARDIAC NURSING…
The 1980s Cardiac nursing as an established nursing specialty.
The Society for Peripheral Vascular Nursing (SPVN), founded in Boston in 1982 and renamed the Society for Vascular Nursing (SVN) in 1990
The American Association of Cardiovascular and Pulmonary Rehabilitation was founded in 1985
Association provides education and training for cardiac nurses

THE HISTORY OF CARDIAC NURSING…
The 1990s
The Preventive Cardiovascular Nurses Association (PCNA) was founded in the United States as the Lipid Nurse Task Force (LNTF) in 1992
evidence-based study of a wider array of cardiovascular disorders

THE HISTORY OF CARDIAC NURSING…
The 21st Century
The American Nurses Credentialing Center (ANCC) is the world's largest nurse credentialing organization, and a subsidiary of the American Nurses Association (ANA).
The first Cardiac and Vascular Nurse examinations were administered by the PCNA in May 2001 in conjunction with the ANCC.

The 21st Century….
The PCNA continues to offer the certification exams as well as continuing education courses online and live seminars and training events.
In addition to the ANCC Cardiac/Vascular Nurse Certification, the PCNA supports the Accreditation Council for Clinical Lipidology (ACCL) certification examination.
Cardiac nursing continues to grow as nursing becomes more specialized.

THEORY APPLICATION
PEPLAU’S THEORY OF IPR

PEPLAU’S THEORY OF IPR..
Four Levels of Anxiety:
1.Mild anxiety is a positive state of heightened awareness and sharpened senses, allowing the person to learn new behaviors and solve problems. The person can take in all available stimuli (perceptual field).
2. Moderate anxiety involves a decreased perceptual field (focus on immediate task only); the person can learn new behavior or solve problems only with assistance. Another person can redirect the person to the task.

Four Levels of Anxiety…
3. Severe anxiety involves feelings of dread and terror. The person cannot be redirected to a task; he or she focuses only on scattered details and has physiologic symptoms of tachycardia, diaphoresis, and chest pain.
4. Panic anxiety can involve loss of rational thought, delusions, hallucinations, and complete physical immobility and muteness. The person may bolt and run aimlessly, often exposing himself or herself to injury.

JOURNAL ARTICLE
Journal; Recent Advances in Preventive Cardiology and Lifestyle Medicine
Barry A. Franklin, PhD; Mary Cushman, MD, MSc
A Cardioprotective Polypill: Need for a Fully Powered Trial?
Wald and Law proposed a theoretical cardioprotective polypill, on the basis of a review of the scientific literature, as a population strategy to combat CVD.
The daily formulation would include a statin, 3 blood pressure–lowering drugs, folic acid, and aspirin, and could theoretically reduce coronary events by 88% and stroke by 80%.
REFERENCES
Kaul,U.,Arora,P., Recent Advances And Future Trends In Cardiology’ , JIMSA,2012.Vol.25.,No.3
Rasche,V., Gishers,G., ‘Cardiology; trends and developments’ Mediamundi 47/2., 2003.
Bonow etal., Braunwailds Heart Disease, A text book of cardiovascular medicine’ 9th edition.,2012
Jonsen,a,r., Siegler,M., Clionical Ethics; A practical approach to decision making., 5th ed., Newyork,2011



















